Embed Size (px)
Citation preview

J. clin. Path. (1955), 8, 1.
VISCERO-CUTANEOUS COLLAGENOSISA STUDY OF THE INTERMEDIATE FORMS OF DERMATOMYOSITIS,SCLERODERMA, AND DISSEMINATED LUPUS ERYTHEMATOSUS
BY
WALTER PAGEL AND C. S. TREIPFrom the Department of Morbid Anatomy and Histology, Central Middlesex Hospital, London
(RECEIVED FOR PUBLICATION SEPTEMBER 14, 1954)
It has been known for some time that dermato-myositis and scleroderma are closely related (Freu-denthal, 1940; Dowling and Freudenthal, 1938)and that intermediate forms exist between thesetwo entities. In the present paper further materialwill be presented in support of this idea.
It was pointed out in a previous paper (Pagel,Woolf, and Asher, 1949) that profound visceralchanges, probably ischaemic, resulting from vas-
cular lesions, are often found in dermatomyositissimultaneously with the skin and muscle changes.In scleroderma concomitant visceral and skinlesions have long been known and extensively re-
corded-so much so that the demand has nowbeen made for the abolition of the name " sclero-derma" and the substitution in its place of theterm " progressive diffuse sclerosis " (Goetz, 1945;Beigelman, Goldner, and Bayles, 1953), a clumsierbut more precisely descriptive name. Some of thechanges seen resemble those observed in dissemi-nated lupus erythematosus. It would thus appearthat overlapping features are not limited to sclero-derma and dermatomyositis, but include membersof the group of so-called collagen diseases. It istherefore suggested that an even more general termshould be used for these overlapping syndromes,"viscero-cutaneous collagenosis."
ILLUSTRATIVE CASESIn the present paper, based on illustrative cases,
the following points are discussed in detail. (1)Transition of dermatomyositis to progressivediffuse sclerosis; (2) the histological changes innail cuticle in dermatomyositis and disseminatedlupus erythematosus, and their possible diagnosticsignificance; (3) suprarenal changes in progressivediffuse sclerosis and dermatomyositis, suggestingnodular fibrosis developing from focal fibrinoidnecrosis; (4) transitional renal and muscularchanges; (5) the muscular changes in dermato-myositis compared with myositis induced experi-mentally with muscular extracts.
A
Transition of Dermatomyositis to ProgressiveDiffuse Sclerosis
Case 1.-The patient, a woman aged 36, wasoriginally described as Case 3 by Pagel, Woolf, andAsher. She developed dermatomyositis 11 yearsbefore death, and five years before death both legshad to be amputated, as severe chronic and atrophicsclerodermatous lesions had rendered them ankylosedand useless. For three years after the amputationsshe had intermittent acute attacks of urinary infection,for which she was admitted on several occasions,responding each time to chemotherapy. Four yearsafter operation a radiograph of the chest showedlarge "cysts" in the lungs. She was admitted onJanuary 19, 1953, with a history of acute left-sidedpyelitis. She was dehydrated and drowsy and herblood pressure was 80 mm. Hg systolic. The bloodurea was 163 mg. per 100 ml. Two days after ad-mission she became cyanosed and shocked, developedrapid respirations, and died the following day.Necropsy (No. 53 /40).-The body was that of a
woman looking older than her age, with scarringand pigmentation of the skin, particularly roundthe breasts and sites of amputation. The right lunggave a gross impression of pulmo lobatus, i.e., therewere irregular deep fissures in both upper and lowerlobes (Fig. 1) and on the cut surface a number ofwell-defined, grey, fibrosed areas, measuring about2.5 x 1.5 cm., chiefly in the cortico-pleural, infra-clavicular, and hilar areas. These contained systemsof bullae up to 2 cm. in diameter (Figs. 2 and 3).The left lung was not adherent and contained one ortwo small, fibrous areas. Both lungs showed basaloedema and congestion. There were a few fine peri-cardial adhesions. The heart showed no appreciablechanges.The liver weighed 1,080 g. and was firm. The cut
surface showed a fine reticular fibrosis throughout.with a loss of. lobular pattern. The spleen weighed225 g., the pulp was soft and purplish, with obscureMalpighian bodies. The kidneys were small, veryirregularly scarred, with pale, mottled subcapsularsurfaces, from- which the capsule stripped easily.The cut surfaces showed good cortico-medullary
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

WALTER PAGEL and C. S. TREIP
FIc. 2
FIo. l.-Case 1: " Pulmo lobatus," pleural surface ofright lung.
FIG. 2.-Case 1: Cut surface of right lung, showing aninfra-clavicular area of fibrosis. Inset: A similararea in the lower, more dorsal portion of the rightupper lobe, with cyst formation.
FIG. 3.-Case 1: another cut surface of right lung,showing pleural thickening, including interlobarfissures and apical and cortico-pleural areas offibrosis with cyst formation.
FIG. 4.-Case 1: histological section through lung.Fibrinoid lining of dilated alveolar ducts (arrows)( x 80). Inset: close-up of fibrinoid lining (haemat-oxylin and eosin, x 300).
FIG. 5.-Case 1: histological section of skin. Thinningof epidermis with sub-epitheLial oedema and lymph-orrhagia in the cutis (haematoxylin and eosin, x 80).
FIG. 6.-Case 1: liver. Histological section showingmultilobular liver cirrhosis (haematoxylin and eosin,x 80).
2
- -z
-Z
-4
*-.Z=
0-
P-- w
W =
FIG. I
--So X-
------ -.-i--
- t-ita
- se1^---. S.i .-|di .. l......... . I-e Ns. ... .. .X-- X . i* ^.X . I.
e-E
.... E
FiG. 3
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

FIG. 4
- \ T-.W :
4*4
ar sI _ _
p ''A.
Fio. S
FIG. 6
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

WALTER PAGEL and C. S. TREIP
demarcation, but the cortical thickness was reducedto 0.5 cm. The pelves contained purulent urine.Cortical lipoid in the suprarenals was reduced.
Histology.-In the lungs, sections through the tri-angular fibrous foci and the multiple subpleural scarsshowed the uniform picture of collapse-indurationwith compensatory emphysema. In the fibrous tissue.curly hyperplastic elastic fibres were seen in largenumbers forming plaques, chiefly subpleurally butalso evenly distributed throughout the collagenousareas. Additional features were fibrinoid lining ofdilated alveolar ducts (Fig. 4), collapsed bronchioli.crystalline foreign bodies with foreign-body giant cellsin collapsed alveoli, and concentric intimal thickening,with elastic reduplication, of the pulmonary arterialbranches.The skin from various parts of the bodv was
markedly thinned in the epidermis with sub-epidermaloedema and conglutination of collagen. Some of thesections Fhowed focal lymphorrhagia (Fig. 5). Irregu-lar clumps and plaques of fragmented elastic fibre,were scattered throughout the dermis, especially inthe foci of conglutinated collagen.The liver showed a multilobular portal cirrhosis
with collections of lymphocytes in the periportalsepta around hyperplastic bile capillaries (Fig. 6).There was a marked capsular fibrosis, containing bilecapillaries. The parenchymal cells showed littlechange.
In the kidneys there were areas of hyalinizedglomeruli with some tubular atrophy and markedfocal lymphocytic collections in these places. Someof the glomeruli showed partially lamellated hyalinedeposits, the rest of the Malpighian corpuscles beingencrusted with nummular crystalline material. Therewere also marked eccentric and concentric intimalthickenings of arterioles with elastic reduplication(Fig. 7). Exceptionally, a small gap in the elasticawas seen (Fig. 7). Some of the atrophic and dilatedtubules contained granular and homogeneous casts.One isolated but very definite area of fibrinoidnecrosis was seen in the stroma between a hyalinizedglomerulus and some normal tubules. This area wasstrongly positive with the fibrin and periodic acidstains, and failed to stain with elastic-van-Giesonstain (Fig. 8).The skeletal muscles showed (a) fibrous scars inti-
mately woven with muscle to give an appearance ofparcelling and sometimes of interruption of musclefibres (Fig. 9A), (b) lymphorrhagia in the long axis ofthe muscle fibres (Fig. 9B). (c) oedema of the septa.and (d) haemorrhages.
In the oesophagus there was some thickening of thefibrous septa in the muscular layers. The thyroidshowed marked thickening of the septa and someperivascular lymphocytic collections. The tonsilshowed a small rim of lymphocytic tissue followedby grossly thickened and oedematous, almost hyalin-ized, fibrous tissue. This tissue contained markedlvhvalinized small arteries, with an uninterrupted, some-what thickened, internal elastic lamella.
The Diagnostic Sigiificance of the HistologicalChanges in the Nail Cuticle
Case 2. A widow, aged 55, two to three weeksbefore the onset of symptoms was stung by a beeon the left upper arm, which swelled up and waspainful for two weeks. The main illness began sixweeks before admission to hospital, when the fingersof both hands swelled up and became blue and pain-ful on movement. There was also a dark brownswelling round the cuticles of the nails, and the pulpsof the fingers were tender. Both wrists becameswollen and painful at the same time. Three weekslater the ankles swelled and the thighs became pain-ful anteriorly. A week later, pain, particularly onmovement, spread to the shoulders and upper arms.but improved later. Some puffiness of the eyelids wasobserved on waking one week before admission, anda pleuritic pain was felt substernally and in the leftaxilla. The previous history contributed nothing.apart from attacks of "bronchial asthma."
She was admitted to the Central Middlesex Hos-pital on November 24, 1953. On examination she waspale and tired-looking, with angular stomatitis. Thctemperature was 100.5°. Blood pressure 190/120mm. Hg. Respiratory movements were poor, andthere was some dullness of percussion at both bases.The fundi showed bilateral soft exudates. No otherabnormal neurological signs were found.The cutaneous changes were brown crusts around
the cuticles of all the nails of both hands. The smalljoints of the hands and the wrists were stiff, the leftbeing worse than the right. Weakness led to diffi-culty in sitting up. Dermatomyositis was diagnosedclinically on account of weakness and the nailchanges.
Investigations showed an E.S.R. of 40 mm. in onehour. Serum proteins were 5.5 g. per 100 ml. (albu-min 3.2 g., globulin 2.3 g.). The 24-hour creatinineand creatine excretions were 830 mg. and 119 mg.respectively (within normal limits). The blood urealevel was 28 mg. per 100 ml., and the serum potassium(two days before death) 4.5 mEq/l. (17.5 per 100 ml.).A skin and muscle biopsy of the right deltoid on
December 4 showed slightly flattened papillae withoedema of the dermis. Pieces of muscle showed noinflammatory reaction or vascular changes and noevidence of dermatomvositis.
Radiography of the chest showed patchy consolida-tion and collapse at the right base. Three blood cul-tures were sterile.
Despite the negative biopsy and normal creatinemetabolism. A.C.T.H. therapy was begun on Decem-ber 8 with 50 mg. A.C.T.H. b.d. intramuscularly,reduced later to 20 mg. b.d. Little change wasnoticeable, apart from a fall in temperature to nor-mal and changes in the radiograph suggesting pul-monary oedema. On December 20 she became muchworse, with cyanosis and dyspnoea, a temperature of100° F.. and signs of left basal pneumonia. She diedon December 23, 10 weeks after the onset ofsymptoms.
4
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

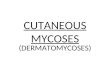
FIG. 8.-Case 1: kidney. Area of fibrinoidnecrosis in the stroma (arrow) (haemat-oxylin and eosin, x 300). Inset: thesame, stained for fibrin (P.T.A.H.,x 300).
FIG. 7.-Case 1: kidney. Elastic van G.eson section, showing arterywith reduplication of internal elastic. Another artery (arrow)shows a gap in the internal elastic membrane (x 80).
)cAI
IVt .:
r.; --U - ,1*4 i WWA*. vtt
~~~: .~~~.FIG. 9.-Case I: skeletal muscle. A, Haematoxylin and eosin sec-
tion showing fibrous scars (x 160). B, Haematoxylin and eosinsection showing lymphorrhagia ( x 300). ,,= x
*:,1it..,-.I
: .......
B3
,...;'r
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

WALTER PAGEL and C. S. TREIP
FIG. IO.-Case 2: histological section through nail bedshowing intra-epidermal bulla filled with fibrin andcapillary haemorrhage in the core (haematoxylinand eosin, x 160).
FIG. 12.-Case 2: nail bed. Section showing capillary thrombosis(arrows) (haematoxylin and eosin, 300). Inset: the same,fibrin preparation (arrows) ( x 3001.
^ J.l IiA
FIG. 1 l.-Case 2: nail bed. Section through intra-epidermal bulla, filled with fibrin and fibrinoid
material (haematoxylin and eosin, x 300). Inset: the same. Fibrin preparation (P.T.A.H., x 300).
6
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

VISCERO-CUTANEOUS COLLAGENOSIS
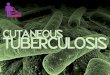
FIG. 13.-Case 3: peripheral muscle. Waxydegeneration with syncytia and calcification(haematoxylin and eosin, x 300). Inset:close-up of calcified degenerated musclefibres (x 700).
FIG. 14.-Case 3: peripheral muscle. Venousthrombosis with haemorrhage. Fibrin stain(P.T.A.H., x 300). Inset: the same (haemat-oxylin and eosin, x 160).
Necropsy (No. 53/561).-The bodywas that of a middle-aged obesewoman. There were no obvious skinchanges apart from some rougheningand swelling of the cuticles of thefinger-nails. All lobes of .the lungswere consolidated, with some rightbasal adhesions. The heart weighed440 g. with considerable left ventricu-lar hypertrophy but no gross lesions.The alimentary system appeared nor-mal. The kidneys showed a normalpattern. The thyroid weighed 90 g.,9with a pale, fleshy cut surface. Theskeletal muscles appeared grosslynormal.Histology.-The skin of the nail
bed showed marked subpapillarycongestion, capillary haemorrhages,and oedema (Fig. 10). In one areathere were deposits of fibrin (verifiedby phosphotungstic acid haematoxylinstaining) and fibrinoid material in thetips of three dermal papillae (Fig. 11).This material lay extravascularly andw as distinct from fibrin in the der-mal capillaries, which showed somethrombus more proximally (Fig. 12).There was some disorganization of the basal layer ofthe epidermis, which gave the impression of theformation of a small "bulla " containing fibrin atthe dermo-epidermal junction (Fig. 10).
In the skin of the arm the papillary body wasflattened with subpapillary oedema.There was congestion of the lung with chronic
atelectasis and carnification with occasional squamousmetaplasia. Collagen, but no elastic fibres, was
- )+..........'......... It - ...
_ a , *P *1
¢_~~~~~~1- %
present in the carnified areas (Weigert-Van-Giesonstain).
In the kidney a fair number of glomeruli showedfibrinoid necrosis as well as hyalinization of afferentarterioles. There was some reduplication of arteriolarinternal elastic laminae.Oedema and central cortical congestion were seen
in the suprarenal, with areas of fine fat droplets inthe zona fasciculata.
7
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

IDg9 . '
i~~4 1 -. .~
W~~~~~~~~~~~~~~~~~~i;v a'- Tt L s ,..-t
+~ ~~ ~~ ~~ ~~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~*
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

of acute haemorrhagic infarction. In some of theveins the intima was thickened and incipient throm-bosis with intramural haemorrhage (Fig. 14) was seen.One artery showed an intimal cushion, with fibrinousexudation into it.The skin of the eyelid had a thin epidermis with a
slight but definite horny layer, and oedema of thecutis with a marked "cap-like" deposition of fibrin(confirmed by fibrin stain-Fig. 15, inset A) oncollagen fibres (Fig. 15).A combined van Gieson and Wilder stain (Fig. 15,
inset B) revealed argentaffine fibres throughout theyellow-staining, fibrinoid ground substance of the"caps." The "caps " are periodic acid positive.The skin of the toe had a thin epidermis with a
thick, horny layer, conspicuous oedema of the cutis,and occasional deposition of fibrin.The suprarenals showed large, well-defined fibrous
plaques up to 0.4 cm. in diameter in the stainedsection, replacing most of the parenchyma (Fig. 16).They did not contain amyloid, and were of collagen,fairly well vascularized. The capsule was thickened,oedematous, and hyaline. There were no appreciable'vascular changes.The tongue had a rough surface with sub-epidermal
lymphocytic collections. The muscle showed slight,but definite, degenerative changes.The aorta showed atheroma and round-celled
collections round the vasa vasorum. The adven-titial vessels showed concentric intimal thickening.The liver showed some thickening of the peri-
pheral portal septa.
Progressive Diffuse Sclerosis with FocalFibrinoid Necrosis in the Suprarenals
Case 4.-A woman aged 50 was admitted complain-ing of blueness, coldness, and pain in the feet andhands, progressing for the past 20 years. For sixvears she had suffered from arthritis. Examinationshowed an emaciated woman, with atrophic, shinyskin over the whole body, erythematous blotches onthe face, and cyanosis of fingers and toes, with
FIG. 17.-Case 4: kidney. I F -A, Glomerulus with Xthrombosis of afferent .'vessels (haematoxylin 'and eosin, x 375). B, . ; 4Glomerulus with fib-rinoid necrosis of capil- Ilaries of the tufts (hae-matoxylin and eosin,x 340). C, Artery withsmall remnants of elasticfibres (Van Gieson elas- .tic preparation, x 300). -
C
incipient gangrene and ulceration of the fingers. Shealso had signs of congestive heart failure, in whichshe died.Necropsy (46/270).-The tonsils were dark red,
ulcerated, and necrotic. There were some lightpleural adhesions. The lungs had the consistencyof consolidation in the lower lobe, but the cut sur-face showed no actual consolidation, only manyhaemorrhagic areas up to 2 x 2 cm. in diameter.The appearances resembled those of " rheumatic "
lung. The pulmonary arteries appeared normal. Theheart showed mitral stenosis with mural thrombus inthe apical portion of the interventricular septum.There was also a haemorrhagic area in the posteriorpart of the septum, 3 x I cm. in diameter. The lowerparts of the oesophagus and cardia were almost blackand oedematous. The kidneys showed a regulargranulation, with many sub- and intra-capsularhaemorrhages. The cut surface showed a variegatedpicture of small haemorrhages and yellow flecks.Histology.-The papillae of the skin of the chest
wall were flattened, with marked oedema of the cutisbeneath.
In the kidney there were some small corticalinfarcts with central haemorrhages and intra- andextra-tubular collections of lymphocytes. The intimaof medium-sized arteries was thickened concentric-ally. Some glomeruli showed thrombosis of afferentvessels and others fibrinoid necrosis of capillaries ofthe tuft (Fig. 17A and B), the latter change beingrarer. Elastic stains showed that in some arterioles
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

WALTER PAGEL and C. S. TREIP
FIG. 18.-A, Tonsil. Focus of fibrinoid necrosis (haematoxylin and eosin, x 360). B, Suprarenal. Similar focus of fibrinoid necrosis ( x 300).
there were gaps in the elastic laminae similar to thoseseen in the kidney of Case 1 (Fig. 17C).The tonsils showed sub-epithelial areas of fibrinoid
necrosis around congested capillaries, in which theblood appeared to be static (Fig. 18A).
In the suprarenal there were ill-defined foci offibrinoid necrosis scattered through the cortex (Fig.18B). A few lymphorrhages were present.
In the tongue there was an oedematous conglutina-tion of the connective tissue between the papillae andthe muscle with lymphocytes. In addition, haemor-rhages were seen round post-capillary veins.The oesophagus showed a picture similar to that inthe tongue. The myocardium showed sub-endo-cardial haemorrhagic infarction. In the lungs therewas intra-alveolar oedema and an exudate of lympho-cytes into the bronchi. The liver showed severe
passive congestion and the spleen marked oedema.
Transitional Renal and Muscular Changes
Case 5.-A man aged 46 was well until the onsetof rheumatoid arthritis in the feet, shoulders, andknees in 1950. Butazolidin, begun in October, 1953,relieved most of his symptoms. He developed clini-cal signs of lesions of the fifth, ninth, and tenthcranial nerves on the right side in January, 1954.The spleen became palpable. Investigations revealeda blood pressure of 190/100 mm. Hg with papill-oedema and retinal exudates. The urine containedprotein. The globulin content of the blood was
6.12 g. per 100 ml., albumin 2.88 g. per 100 ml.,zinc sulphate turbidity 42 units per 100 ml., and a
blood urea level (terminally) of 240 mg. per 100 ml.(One month before the blood urea had been 32 mg.
per 100 ml.) The blood showed a leucoc tosis of18,000 per. c.mm. with 670% neutrophils. The maxi-mum erythrocyte sedimentation rate was 105 mm.in one hour. Bone marrow biopsy showed onedoubtful lupus erythematosus cell. The clinicaldiagnosis was considered to lie between acute dis-seminated lupus erythematosuis and polyarteritisnodosa. The patient died in uraemia within twoweeks of admission.Necropsy (54/204). The body was that of a well-
nourished man. The brain appeared normal extern-ally. The lungs showed some grey hepatization, andthere was some fibrinous pleurisy. The heart showedhypertrophy of the left ventricular wall. The caecumshowed a small mucosal slough. The kidneys weighed215 (right) and 275 (left) g. respectively. The capsulesstripped easily, leaving smooth surfaces showing occa-sional petechiae and some yellowish flecks. The cutsurface was of brownish red, and the cortico-medullary pattern was almost completely lost, withoutfocal infiltrations or haemorrhages and withoutarterial prominence. The pancreas weighed 160 g.and had a firm nodular consistency. Two areas ofnecrosis were present, the larger, measuring 3 x 2 x
0.5 cm., being in the head; it was sharply defined,with a yellowish homogeneous surface and an adja-cent area of haemorrhagic necrosis which seemedgrossly to contain a thrombosed artery. The smallerinfarct measured 1.5 x 1 x 1 cm. and was situated atthe junction of the left and middle thirds; it showeda similar cut surface, without haemorrhage. Therewas no adjacent fat necrosis. The skeletal musclesand other major viscera showed no gross abnor-malities.
lo
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

VISCERO-CUTANEOUS COLLAGENOSIS
A
D
FIG. 19.-Case 6: peripheral muscle. A, Waxy degeneration of muscle fibres with sarcolemmal cell reaction (haematoxylin and eosin, x 300).B. The same. Sarcolemmal cells occupy deep lacunae in the dissolving muscle bundles (haematoxylin and eosin, x 300). C, Part ofsarcolemmal tube filled by sarcolemmal cells mixed with some polymorphs (haematoxylin and eosin, x 300). D, The same. Thickeningand oedema of stroma (haematoxylin and eosin, x 160).
Histology.-In the glomeruli the most strikingchange was a focal fibrinoid necrosis of the tufts,with occasional "wire-loop" formations due to pick-ing out of the basement membranes. Proliferativeglomerulitis and capsulitis were not seen. There werea few hyalinized glomeruli. The tubules showedpatchy necrosis, often severe and hyaline in appear-ance, occasionally with a collection of neutrophils.The lumina contained casts which were often brightlyeosinophilic and positive for fibrin (P.T.A.H. stain-ing). The vessels showed various lesions, the mostconspicuous change being a fibrinoid necrosis ofafferent glomerular and larger arterioles, with whicha thrombosis was sometimes associated. In theperiphery extensive hyaline and thrombotic lesionswere often associated with subcapsular acute infarcts.The larger arteries showed hyperplastic intimal andmedial sclerosis. There was moderate interstitialoedema with occasional lymphocytic collections.Staining for amyloid was negative.
Large areas of recent infarction, with peripheralneutrophil reaction, were seen in the pancreas. Therewere areas of haemorrhage with necrosed vessels, oneof which contained thrombus. Arteritis was not seen.Many vessels showed hypertensive changes.Some of the sections of peripheral muscle showed
degeneration and fragmentation of muscle fibres, withcellular ingestion of fragments in the sarcolemmaltubes. There was a general increase of sarcolemmalnuclei and also some focal lymphorrhages with a fewplasma cells.Fibrinous pleurisy, with an organizing oedema and
incipient bronchopneumonia in the parenchyma, wasfound. Many siderophores were present in the alveoli.The caecum showed an infarcted mucosa associated
with thrombosed vessels. Serosal vessels showed verysevere intimal sclerosis.
Sections of the bone marrow, liver, spleen, thyroid,small intestine, suprarenal gland, and retina showed
11
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

WALTER PAGEL and C. S. TREIP
no significant changes apart from those of hyper-tension. The Gasserian ganglia showed focaldemyelination.
Dermatomydoitic Changes ResemblingExpeainental Fnins
Case 6.-A woman aged 37 was admitted to anotherhospital with an obscure pyrexia, thought to be dueto pneumonia. Soon after admission solid sub-cutaneous oedema of the arms and thighs was noted.A clinical diagnosis of dermatomyositis was made andcortisone was given, with rapid improvement. Abiopsy of the skin and biceps was sent to us foropinion.
Histology.-The sections showed a variety ofcharacteristic changes.There was waxy degeneration of muscle bundles.The sarcolemmal tubes were filled with fairly large
polygonal cells with somewhat hyperchromatic, round,elliptic, or spindly nuclei. These cells had engulfed orclustered round fragments of necrotic muscle (Fig.19A). Sometimes they seemed to lie in de.ep lacunaeor else form round muscle bundles (Fig. 19B). Besidesthese there were peripheral remnants of muscle tissueadherent to the sarcolemmal wall, leaving a centralspace (" pseudo-vessels ").
Syncytia, mostly forming seams along degeneratingmuscle fibres, were found.
Polymorphs, including a few eosinophils, formedmicro-abscesses replacing parts of muscle bundleswithin the confines of the sarcolemma (Fig. 19C).The stroma, which contained a few plasma cells,
some capillary haemorrhages, a few polymorphs, andsomewhat juicy fibroblasts (Fig. 19D), was thickenedand oedematous.The papillary body, with marked oedema of the
cutis, was flattened.
CLINICAL AND HISTOLOGICALCONCLUSIONS
DiagnosisLooking back at the descriptions of these cases,
the first point to be discussed is diagnosis.In Case 1 the patient, developing dermatomyositis
11 years before death, died of a disease whichaccords with the descriptions of generalized sclero-derma or progressive diffuse sclerosis.
In Case 2 the diagnosis was doubtful. Theclinical picture could equally well have fitted acase of acute disseminated lupus erythematosus,a rash often being absent in this condition. Clinic-ally the parallel is close; in both disseminatederythematosus and dermatomyositis there is fever,muscular weakness, oedema of the eyelids, andlesions around the cuticles of the nails. Pleurisy isperhaps more in favour of lupus erythematosus,
while the absence of anaemia and leucopenia andthe normal serum proteins are against it. It isunfortunate that lupus erythematosus cells werenot searched for.
In Cases 3 and 6 the clinical diagnosis was con-sistent with subacute dermatomyositis, which wasconfirmed by biopsy.
Case 4 was clinically one of scleroderma.In Case 5 the clinical diagnosis of polyarteritis
nodosa was not borne out by the histological find-ings. These included " wire loop " glomeruli andcapillary and arteriolar thromboses in the kidney,changes suggestive of disseminated lupus erythe-matosus. It should be added that a doubtful lupuserythematosus cell was found in the bone marrow,but lupus erythematosus cells have been observedby Cohen (1954) in rheumatoid arthritis and cantherefore not be considered diagnostic. Finally,the striking reversal of the albumin: globulin ratio,such as in this case, is not normally seen in poly-arteritis nodosa, and supports the diagnosis of dis-seminated lupus erythematosus.
Histology of the Affected Organsngs.-These were affected principally in Case
1. According to Ellman and Cudkowicz (1954) andEvans and Parker (1954) the pulmonary changesrecorded in scleroderma are diffuse fibrosis, finenodulation, cyst formation, and pleural fibrosis.Getzowa (1945), who gives a detailed descriptionof these changes, shows a photograph of the cysticlesions, resembling a " honeycomb " lung. Otherauthors lay stress on the diffuse fibrosis withoutmacroscopic changes (Weiss, Stead,. Warren, andBailey, 1943). The appearance of the right lungin the present case differs considerably from thosealready described-a picture of thick, fibrousbands with large fibrous plaques obliterating mostof the parenchyma. Histologically, the strikingfeature is the presence of .much elastic tissue inthe fibrous areas, in contrast to Getzowa's cases,in which elastic fibres had disappeared from thefibrous areas, indicating a probable sequence ofcollapse followed by fibrosis. The small cysts areproduced by a compensatory emphysema. Thefibrinoid lining of the alveoli was described byGetzowa and resembles that seen sometimes in theso-called rheumatic lung (Hadfield, 1938). It hasbeen pointed out since that these membrants arenot specific of rheumatic aetiology. We observedseveral classical examfiples in cases with acute termi-nal circulatory failure, e.g., after thoracoplasty.Nevertheless, the frequency of such changes inacute rheumatic diseases, especially when com-bining with organizing changes (" Masson's
12
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

VISCERO-CUTANEOUS COLLAGENOSIS
bodies "), remains impressive (Neubuerger, Geever,and Rutledge, 1944).Kidney.-The main question in respect of this
organ is the incidence and specificity of arteriolarfibrinoid necrosis in scleroderma, as described byMoore and Sheehan (1952), of " wire loop"glomeruli in disseminated lupus erythematosus, asdescribed by Klemperer, Pollack, and Baehr (1941),and of gaps in the elastic lamellae as seen in burnt-out polyarteritis nodosa (Pagel, 1951).The " scleroderma " change was absent in Case 1,
present in Cases 2 and 4. Whereas Case 1, in spiteof its absence, was a typical example of diffusescleroderma (" visceral sclerosis "), Case 2, inwhich it was present, was not. The " L.E.D."change was found in Case 5 only, in which itestablished the diagnosis of disseminated lupuserythematosus, against the clinical diagnosis ofpolyarteritis nodosa, as it can for practical pur-poses be considered characteristic of disseminatedlupus erythematosus (Allen, 1951).The " polyarteritis nodosa " change occurred in
Cases 1 and 4, which were both of scleroderma.Two other less characteristic vascular changes
were capillary and arteriolar thromboses, as seenin Case 5.Of non-vascular kidney changes, the area of
fibrinoid necrosis in the stroma is of interest, forsuch extravascular renal foci do not seem to havebeen observed previously in scleroderma, althoughthey are well recognized in the skin (see Case 3).
Liver and Pancreas.-The liver was grosslychanged in Case 1 only (a case of scleroderma).Beerman (1948) remarks that little has appearedin the recent literature on hepatic involvement inscleroderma. This remark still holds good. Brock(1934) noted in his Case 4 an increase of peri-portal connective tissue. Perdomo de Fernandez,Ravera, and Piovano (1951) performed a liverbiopsy on a man aged 43 with scleroderma,whose liver was palpable two fingerbreadths belowthe costal margin. He comments that few casesof scleroderma have hepatic symptoms and thatthe abdomen is often difficult to palpate becauseof the rigidity of the wall. Histological examina-tion showed foci of sclerosis consisting of whorlsof collagen fibres showing some hyaline degenera-tion. There were also some collections of roundcells and fibroblasts. Both lesions were accom-panied by discrete hepatocellular degenerativelesions-fatty changes, with bile pigment deposits.Harvier and Bonduelle's case (1947), a womanaged 43, showed radiologically calcification of thehepatic capsule. Biopsy was not performed. Goetzdescribes the " deposition of a peculiar amorphous
material in a cirrhotic liver of an unusual type,"but gives no further details of these cases. Beigel-man et al. (1953) describe centrilobular hepaticfibrosis in their Case 9. The findings in the pre-sent case seem to correspond fairly closely withthose of Perdomo de Fernandez et al., the portalchanges being more advanced with little parenchy-mal damage. In Harvier and Bonduelle's casethere was probably a similar capsular fibrosis, inwhich calcium deposits had been laid down. Itseems then that the tendency to fibrosis extends tothe portal tract and capsule of the liver in somecases.The pancreas was involved in Case 5, in which
there was evidence of malignant hypertension.Pancreatic necrosis due to arterial thrombosis inmalignant hypertension has been reported (Pageland Woolf, 1948) and we have also seen recana-lized thrombosis without necrosis of the pancreasin a case of malignant hypertension. The lesionin the caecum in the present case was probablyof a similar nature.
Skin.-Lesions of scleroderma were found inCase 1 (scleroderma), in Case 2 (a transitionalcase between dermatomyositis and disseminatedlupus erythematosus), in Case 3 (dermatomyositis),and in Case 4 (dermatomyositis).
Nail bed changes were seen in Case 2 (tran-sitional between dermatomyositis and disseminatedlupus erythematosus).
Lesions of the nail cuticles in dermatomyositisare well recognized (Keil, 1942) and may be anearly symptom. Searching through the cases re-ferred to by Keil and through subsequent litera-ture, we have been unable to find any account ofthe histological appearance of these lesions and soare unable to compare our own findings with any
FIG. 20.-Case 2A: naked-eye appearances of nail bed changes inlupus erythematosus disseminatus. Splinter haemorrhages innails, in addition to multiple petechiae, swelling, and blisteringof nail cuticulae.
13
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

WALTER PAGEL and C. S. TREIP
I
WN
* *4
A
AL ;sS
4--ysts
others. The cases of Pick (1935) and Engelhardt(1935) seem to correspond clinically to our own,
but no histological report was given. The picturewe found does, however, demonstrate that ubi-quitous hall-mark of the "collagen " diseases,fibrinoid necrosis. The " bulla " seems to be theresult of epidermolysis. Liquefactive degenerationof the basal epidermal cells is also a feature oflupus erythematosus (Klemperer et al., 1941;Lever, 1949). The changes in this case have a
particular point of interest because they show a
combination of capillary thrombosis with extra-vascular fibrinoid necrosis. Such a combinationis not normally seen. Usually we have either thepicture of acronecrosis with capillary thrombosis,as seen in thrombocytopenic purpura (Moschcowitz,1925; Baehr, Klemperer, and Schifrin, 1936) or insubacute bacterial endocarditis (Pagel, 1949) andthrombotic micro-angiopathy (Symmers, 1952), or
FIG.' 21.-Case 2A: fibrin thrombi(arrows) in capillaries of the cutis.Thinning of epidermis with epi-dermolysis (arrows). (Haematoxylin
else that of extravascularfibrinoid necrosis as seen incollagen disease (dissemi-nated lupus erythematosus,dermatomyositis). In poly-arteritis nodosa, the classi-cal collagen disease of bloodvessels, no evidence ofprimary thrombosis can befound and sub-endothelialhyaline deposition, said top r e c e d e acrothrombosis(Gore, 1950), differs from
~ tX t-^>-K4 the early polyarteritic9>'; changes (Pagel, 1951).*t8 .Thrombosis observed in
it the same area is not inci-dental, however. This is
a@^;>b zJ- .w shown by its occurrence ina similar setting in the skinchanges of disseminatedlupus erythematosus. Asan example the case may be
...'-t_tf-briefly described of a man
-xS*~) aged 62 years (Case 2A),*- a -* i who died after a five
months' illness suggestive ofA4101W
< disseminated lupuserythematosus - erythemat-ous rash, joint pains, andprogressive loss of weight.No lupus erythematosus cells
were found in the bone marrow and a skin biopsywas not helpful. Terminally the rash became bul-lous and there were swelling, cyanosis, and epi-dermolysis of the nail folds (Fig. 20). There wasno response to treatment with A.C.T.H. and corti-sone. The post-mortem examination (P.M. 54 /265)showed grossly only a basal bronchopneumoniaand a diffluent splenic pulp. Significant histo-logical changes were restricted to the skin andnail fold, and were similar at both sites. Theepidermis was flattened and atrophic, more so inthe skin than in the nail fold, with liquefactiondegeneration of the basal layer (Fig. 21). Thecorium was markedly oedematous with capillarycongestion. Some of the dilated capillaries con-tained fibrin thrombi (Fig. 21). Small haemor-rhages had occurred in some of the papillae. Inaddition, there was fibrinoid degeneration in thedeeper corium. There was a moderate lympho-
14
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

VISCERO-CUTANEOUS COLLAGENOSIS
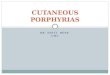
FIG. 22.-Rabbit muscle. Intramuscularinjection of 0.1 ml. of a specific anti-muscular anti-serum. Three aspects ofthe histological changes, experimentalanaphylactic myositis (Kall6s and Pagel,unpublished). Fragments of musclesurrounded by " sarcolytes." Topleft, x 50. Top right, x 200. Bottom,> 300.
cytic infiltration of the corium, sometimes localizedround the appendages.These changes are fairly characteristic of acute
lupus erythematosus, in which we would like toinclude capillary thrombosis, although Klempereret al. (1941) on the basis of a much more exten-sive material considered thrombosis to be uncom-
mon in this disease. We regard the thrombosisto be independent of vascular damage, which was
absent in the walls of thrombosed vessels.It should be mentioned, however, that it is the
combination of capillary thrombosis and fibrinoidnecrosis rather than their occurrence singly whichseems to be characteristic. For, in one of threecontrol nail beds selected from random post-mortem material (Nos. 54/182, 54/183, 54/184),a case of coronary thrombosis in a male aged 74,a small fresh, fibrin thrombus was seen in an intra-papillary vessel, whereas no appreciable changeswere seen in the two other control cases.
In connexion with the acrothrombosis andcapillary haemorrhages seen in the present case,it should be noted that, according to Keil, grosshaemorrhages may occur in the nail beds indisseminated lupus erythematosus, and splinter
w-t
p.tAf DC~~~~~~~~~~~A
haemorrhages in the nail beds are a feature ofdermatomyositis.A feature worthy of comment is the fibrinoid
".caps" lining bundles of collagen fibres in theeyelid. A combined van Gieson-Wilder stainshows that the " caps " consist not of fibrin alonebut of a non-collagen ground substance in whichargentaffine fibres are present. It is tempting toassume that this ground substance was originallycollagen in a state of fibrinoid degeneration, andto compare the presence of argentaffine fibreswith that typically observed in rheumatic and para-rheumatic conditions (Klinge, 1933 ; Pagel, 1951).
Muscle.-Muscle changes were absent in Cases 2(transitional case) and 4 (scleroderma).Of the others, Case 5 (disseminated lupus
erythematosus) showed myositic changes whichwill be discussed in the final,comment. In con-nexion with this case, it should be rememberedthat lesions of striped muscle are not uncommonin rheumatoid arthritis (Cruickshank, 1952).The classical myositic changes were seen in
Cases 1, 3, and 6. The changes in Case 6 indicateacute episodes superimposed on a more protracted.
15
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

WALTER PAGEL anid C. S. TREIP
though extensive, destruction of muscle. The acutechanges are shown by micro-abscesses replacingplarts of necrotic muscle bundles and by the pern-mysial haemorrhages. Chronic changes are shownby extensive collections of cells engulfing smallfragments of necrotic muscle within the confinesof the sarcolemmal tubes. The first impression isof inflammatory cells in vessels, but a closer studysoon shows that the spaces are really sarcolemmaltubes, partly empty, partly filled with special cells,namely the sarcolytes described by Glucksmann(1934) in the metamorphosis of amphibia. Thesecells should be regarded as the associates, or per-haps the precursors, of the syncytia, the well-knownproducts of muscular regeneration. Apart from thepolymorphs, the inflammatory cells, notably plasmacells and macrophages, are rare though presenthere and there in the stroma. These pictures invitea comparison with the experimental findings byKall6s and Pagel (1937) produced by injecting amuscular antiserum into rabbit muscle. Here, too,fragments of muscle, often within the sarcolemmatubes, were found. These formed, together withdistinctly eosinophilic sarcolytes, small granulo-mata and syncytia comparable to those seen inthe present case (Fig. 22).Suprarenals. and Tonsils.-The extensive focal
fibrosis of the suprarenal cortex seen in Case 3seems to be a noteworthy feature. From the soft,oedematous nature of the fibrous tissue we wouldsuggest that the change is related to the diseaseand is not accidental or congenital. In view ofthe suprarenal changes found in Case 4 foci offibrinoid necrosis it is not unlikely that the focalfibrosis represents the terminal stages of suchnecrotic foci. In Case 4 areas of focal fibrinoidnecrosis were also found in the tonsil.
DISCUSSIONIt can be seen from the discussion of the cases
that the differential diagnosis of dermatomyositis,progressive diffuse sclerosis, and disseminatedlupus erythematosus can be a matter of the utmostdifficulty. Case 3 is the most straightforward andone can with fair confidence diagnose it as a sub-acute dermatomyositis, both clinically and histo-logically. With Case 1, however, we encounterdifficulty. Are we to call it chronic dermato-myositis with visceral changes or progressivediffuse sclerosis supervening upon a former attackof dermatomyositis ? The continuity of thedisease since the original onset 11 years beforedeath would favour the former diagnosis, but thevisceral lesions were certainly those of a progres-sive diffuse sclerosis. Nor is histology helpful.
Brock states that the late stages of the two diseasescan be distinguished because in dermatomyositisinflammatory infiltrations and a variety of de-
generations of the parenchyma of muscles are out-standing features to the end." From his descrip-tion, it seems he is referring to the round-celledinfiltrations of muscle now known as "lymphor-rhagia." They are also now known to be non-specific (Cruickshank, 1952 Russell, 1953). Freu-denthal (1940) was able to demonstrate lymphor-rhages in muscle in a case of scleroderma andconcluded that "the histological changes in skinand muscle in generalized scleroderma anddermatomyositis show no essential difference."With this latter view we agree. We also feel thateither chronic dermatomyositis has the viscerallesions of progressive diffuse sclerosis or thatdermatomyositis merges imperceptibly into it. Wetherefore conclude that Case 1 is an instance ofdermatomyositis termin ating in progressive sclerosis.Where then does Case 2 stand diagnostically '.
Clinically it appeared to be a case of dermato-myositis, but no muscular changes were foundeither during life or after death when the onlyrelevant change was in the nail bed. Reports inthe literature indicate the difficulties of otherauthors (Bradley, Drake, and Mack, 1951:Madden, 1950). Out of 21 biopsies in Madden'scases of disseminated lupus erythematosus. sixshowed nodular myositis. Fifty per cent. ofthem showed lupus erythematosus cells inmarrow examination. He concluded that the"muscle changes in dermatomyositis and dis-seminated lupus erythematosus are not specific"and even discourages muscle biopsy as a majorprocedure for a very ill patient, recommendingrather the examination for lupus erythematosuscells, despite the low incidence of positive resultsin the latter investigation. Histological evidenceof the non-specific character of the muscularchanges in dermatomyositis had already beenadduced by Pagel et al. (1949). Degos, Garnier.Darnis, and Vissian (1949) described a case ofsubacute lupus erythematosus with dermato-myositis. Of Spuhler and Morandi's (1949) twocases, the first showed diffuse scleroderma withRaynaud's syndrome, clinical dermatomyositis.and a Libman-Sacks endocarditis. They con-cluded that disseminated lupus erythematosus,dermatomyositis, and scleroderma are differingforms of reaction to a non-specific infection. InClein's (1953) case of acute dermatomyositis themuscle biopsy (reported by us) was negative, butthis was not considered to exclude dermatomyositis.The case bore a close resemblance clinically to
16
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

VlSCERO-CUTANEOUS COLLAGENOSIS
our Case 2, but showed no cuticular changes andhad an erythematous rash. Retrospectively it isdifficult to exclude also the possibility of an acutedisseminated lupus erythematosus in Clein's case,which responded to cortisone. Later the patientdeveloped a condition resembling rheumatoidarthritis. We suggest therefore that our Case 2combines clinical features of dermatomyositis withhistological features of progressive diffuse sclerosisand disseminated lupus erythematosus.
Case 5 illustrates a further aspect of the clinicaldiagnostic difficulty. Polyarteritis nodosa was con-sidered here because the one possible lupus ery-thematosus cell seen was thought to be a " tart "cell rather than a true lupus erythematosus cell (theingested nuclear fragment was sharply defined andretained a recognizable chromatin pattern) and wastherefore disregarded. As the " tart " cell is sup-posed to be a precursor of the lupus erythematosuscell and as neither of these cells occurs in poly-arteritis nodosa, this disregard seems to have beenunjustified. The histological findings quite defi-nitely excluded polyarteritis nodosa. Many of thechanges found, necrotizing arteriolitis, capillarythrombosis, pancreatic necrosis, and myositis, arealso found in other syndromes, and we are left withthe distinctive " wire-loop " phenomenon. Thiscase had features in common with progressivediffuse sclerosis, dermatomyositis, and disseminatedlupus erythematosus.
Case 6 shows that dermatomyositis is primarilya degenerative and not an inflammatory lesion ofmuscle. The majority of the cells seen are youngmyogenic elements, probably sarcolemma cells,which engulf and cluster around fragments ofnecrotic muscle. They seem to be related to thesyncytia seen in a similar site, at or lining, thesarcolemma and fragments of necrotic muscle.Inflammatory cells are secondary invaders; in thepresent case, polymorphs, including some eosino-phils, form an addition somewhat unusual indermatomyositis, whereas plasma cells, a con-spicuous feature in some cases, are very scarce.Lymphocytes commonly seen in the form of"lymphorrhagia " are also scanty.
In none of these cases were the haematoxophilbodies said to be characteristic of disseminatedlupus erythematosus (Klemperer, Gueft, Lee,Leuchtenberger, and Pollister, 1950) found. Theywere, however, present in a case previously re-ported by Pagel (1951, Fig. 7). The latter caseshowed a clinical picture of polyarteritis nodosawith consistently high eosinophilia, polyneuritis,and fleeting pulmonary infiltrations. An excisedskin nodule showed extensive deposition of
B
granules with intense affinity for haematoxylin-the picture of haematoxophil bodies. An addi-tional feature was the distinct foreign-body re-action of tuberculoid type which they elicited.This observation of haematoxophil bodies in acase of polyarteritis nodosa confirms the findingsof Worken and Pearson (1953) that these bodiesneed not be invariably associated with dissemi-nated lupus erythematosus.The distinctive features of the present series are
summarized in Table I.
TABLE ISUMMARY OF HISTOLOGICAL
SERIESCHANGES IN PRESENT
Lesion Case Case Case Case Case CaseLeSiOn ~~1 2 3 4 S 6
Muscle changes resemb-ling dermatomyositis + 0 + 0 - +
Muscle changes resemb-ling experimentalmyositis 0 0 0 0 0
Skin changes resemblingdermatomyositis . . + + 0
Skin changes resemblingscleroderma.. . + + + 0 +
Visceral changes resemb-ling progressive dif- Notfuse sclerosis - 0 + known
Visceral changes resemb-ling disseminated lupuserythematosus .. + 0 0 + +
It would appear, then, from the increasingnumber of reports in the literature and from ourown experience, that the clear-cut diagnosis ofdiseases of the collagen group (notably acutedermatomyositis and disseminated lupus erythema-tosus) is becoming progressively tindermined, fromboth the clinical and histological points of view.
SUMMARYThe clinical and histological features of dermato-
myositis, progressive diffuse sclerosis, and dis-seminated lupus erythematosus may overlap suffi-ciently to render differential diagnosis impossiblein some cases. We suggest that such intermediateforms be grouped under the name of "viscero-cutaneous collagenosis."From the material presented, the view that
dermatomyositis and4scleroderma are stages of thesame disease is confirmed.The changes in the nail fold, clinically regarded
as characteristic of disseminated lupus erythema-tosus and dermatomyositis, are a clearly recogniz-able histological entity, consisting of patchy extra-vascular fibrinoid necrosis associated with capillarythrombosis-an unusual combination of collagendisease and acronecrosis.
17
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from

WALTER PAGEL atnd C. S. TREIP
One of the cases of dermatomyositis presentedshows muscular changes strikingly similar to thosereproduced experimentally by means of an anti-muscular serum.
Focal necrosis and focal fibrosis in the supra-renal are thought to represent the early and endstages of a process which can be associated withdermatomyositis.
We are indebted to Dr. Josephine Roth, Dr. HerbertLevy, and Dr. R. Aidin for material and opportunitiesfor clinical pathological discussion, to Mr. L. G. Spainand Miss Marjorie Webb for technical assistance, andto Miss Yvonne Vincent for assistance with photo-graphy.
REFERENCESAllen, A. C. (1951). The Kidney, p. 170. Grune and Stratton, New
York.Baehr, G., Klemperer, P., and Schifrin, A. (1936). T-ans. Ass. Anmer.
Phys., 51, 43.Beerman, H. (1948). Amer. J. med. Sci., 216, 458.Beigelman, P. M., Goldner, F., Jr., and Bayles, T.IB. (1953).] New
Engl. J. Med., 249, 45.Bradley, J. E., Drake, M. E., and Mack, H. P. (1951). Amer. J.
Child., 81, 403.Brock, W. G. (1934). Arch. Derm. Syph., Chicago, 30, 227.Clein, L. (1953). Brit. med. J., 2, 1357.Cohen, H. (1954). John Tate Memorial Lecture. Unpublished.Cruickshank, B. (1952). J. Path. Bact., 64, 21.Degos, R., Garnier, G., Darnis, F., and Vissian, L. (1949). Bull.
Soc. franC. Derm. Syph., 56, 114.Dowling, G. B., and Freudenthal, W. (1938). Brit. J. Derit., 50, 519.Ellman, P., and Cudkowicz, L. (1954). Thorax, 9, 46.
Engelhardt (1935). Zbl. Haut. u. GeschlKr., 52, 69.Evans, M., and Parker, R. A. (1954). Thorax, 9, 154.Freudenthal, W. (1940). Brit. J. Derm., 52, 289.Getzowa, S. (1945). Arch. Path., Chicago, 40, 99.Glucksmann, A. (1934). Z. Anat. EntwGesch., 103. 303.Goetz, R. H. (1945). Clin. Proc., 4, 337.Gore. 1. (1950). Amer. J. Path., 26, 155.Hadfield, G. (1938). Lancet, 2, 710.Harvier, P., and Bonduelle, M. (1947). Presse med., 55. 369.Kall6s, P., and Pagel, W. (1937). Acta med. scand., 91, 292. Quoted
from Kall6s, P., and Kall6s-Deffner, L. (1937). Ergebn. Hyg.Bakt., 19, 178; and Pagel, W. (1939) in Fortschritte der Allergie-lehre, ed. Kall6s, P., p. 73. Karger, Basel.
Keil, H. (1942). Ann. intern. Med., 16, 828.Klemperer. P., Gueft, B., Lee, S. L., Leuchtepberger, C., and
Pollister, A. W. (1950). Arch. Path., Chicago, 49, 503.Pollack, A., and Baehr, G. (1941). Ibid., 32, 569.
Klinge, F. (1933). Ergebn. allg. Path. path. Anat., 27, 1.Lever, W. F. (1949). Histopathslogv of the Skin, p. 252. Lippincott,
Philadelphia.Madden, J. F. (1950). Arch. Derm. Syph., Chicago, 62, 192.Moore, H. C., and Sheehan. H. L. (1952). Lancet, 1, 68.Moschcowitz, E. (1925). Arch. intern. Med., 36, 89.Neubuerger, K. T., Geever, E. F., and Rutledge, F. K. (1944). .4rclt.
Path., Chicago, 37, 1.Pagel, W. (1949). Amer. J. m"e.d. Sci., 218, 425.--(1951). Journal of Clinical Pathology, 4, 137.
and Woolf, A. L. (1948). Brit. ined. J., 1, 442.Woolf, A. L., and Asher, R. (1949). J. Path. Bact., 61, 403.
Perdomo de Fernandez, C., Ravera, J. J., and Piovano, S. (1951). Arch.urug. Med., 38, 361.
Pick, W. (1935). Arch. Derm. Syph., Berl., 173, 302.Russell, D. S. (1953). J. Path. Bact., 65. 279.Spuhler, O., and Morandi, L. (1949). Helt. med. .4cta, 16, 147.Symmers, W. St. C. (1952). Brit. med. J., 2, 897.Weiss, S., Stead, E. A., Warret, J. V., and Bailey, 0. T. (1943).
Arch. intern. med., 71, 749.Worken, B., and Pearson, R. D. (1953). Arch. Path., Chicago, 56
293.
18
on April 13, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.8.1.1 on 1 February 1955. D
ownloaded from