Embed Size (px)
Citation preview

Thank you for selecting Lotus Path Wellness Center as your care provider. I offer optimum health naturally through Oriental and Functional Medicine practices.
Your first session with me will last an hour and a half. Since a full 90 minutes is setaside for you, please advise us as soon as possible if you find that you are not able to keep the appointment. Additional appointments take 30 –60 minutes, based on your needs.
Please print the forms below that need to be completed. Some forms are straightforward and some may require that you think about the answers. We find that many of our patients are amazed at how quickly their situation changes for the better, and sometimes it is good to be reminded of how you felt before you started your path to optimal wellness.
Please bring these completed forms to your first appointment:1. Patient Registration Form/Personal History
5. Metabolic Assessment Form Key
2. Patient Informed Consent 6. Supplements and Pharmaceuticals List3. Agreement to Abide by Office Policies 7. Seven Day Diet Log4. Patient History
If you are taking a multi-nutrient supplement, include the amount of each individual nutrient contained in each capsule. If it is easier, simply bring the bottles in with you at the time of your visit. Also, if you have had recent lab reports or medical records that are pertinent to your current situation, please bring copies of those with you.
I will act as a coach/consultant in your healthcare, offering alternatives thatconventional medicine may not consider. Should you have any questions, please call us at 964-0847. We request that you honor the 24-hour cancellation policy as a courtesy to those waiting for an appointment. If 24 hours' notice isn't given, you will be charged $50. We look forward to working with you.
Sincerely,Dr. Maria BelluccioLotus Path Wellness Center

______________________________________________________________________Patient’s Agreement to Abide by
OFFICE POLICIES____________________________________________________________
GENERAL INFORMATIONLotus Path Wellness Center office hours are from 9:00 a.m. to 5:00 p.m. Monday through Wednesday. We are closed on Thursday and Fridays. Our practice covers a wide variety of medical and health related issues to aid in creating balance and wellness through Oriental and functional medicine.
POLICIESOffice visits are made by appointment only. The nature of this practice is to provide you with the best possible care and service so that you acquire optimum health in natural ways. Therefore, you may experience unexpected delays in being seen. Please be assured that you will be attended to as promptly as possible and be given the same careful attention as those who came before you.
Full payment is expected at the time of service. You may pay with credit card, debit card, check, or cash. We accept Visa, MasterCard, and Discover only. A 24-hour notice is required for cancellation; otherwise you WILL BE billed a $50 fee for the appointment time.
Nutritional supplements may be offered to patients based on their individual needs.Supplements, once opened, cannot be returned.
I have read and understand the above office policies, and I agree to them as a condition for being seen by Dr. Maria Belluccio.
________________________________________________________ Date_______________________________Patient (or Guardian) Signature
PATIENT REGISTRATION FORMTo my patients: the information collected is confidential and will help me determine if the treatment offered here will help you. If I do not sincerely believe that your condition will respond satisfactorily, I will not accept your case. In order that I understand your condition properly, please be as accurate and legible as possible with completing the enclosed forms.
NAME___________________________________Gender________ Marital Status___________

Date of Birth_____________________________ SS Number_____________________________
Address____________________________________City_______________State____Zip______
Home Phone___________________ Cell phone__________________ Other________________
Email address___________________________________________________________________
Employer______________________________________Occupation______________________
Business Address________________________________Bus.Phone_______________________
Family Physician________________________________Phone #_________________________
Emergency contact____________________________Relationship_______________________
Phone#______________________________________________________________________
Who referred you to my practice?__________________________________________________

I, _________________________________________________, hereby request and consent to the performance of acupuncture and related modalities on me (or on the patient listed below for whom I am legally responsible) administered by the acupuncture physician listed below and/or other licensed acupuncturists who now or in the future may treat me while employed by, working or associated with, or serving as back-up for the acupuncture physician named hereunder, whether the treatment is performed at the clinic whchi may be listed below or at some other location.I understand that the methods of treatment may include, but are not limited to acupuncture, electro-acupuncture, moxibustion, vasopneumatic cupping, electro-therapy, Tui-na (oriental massage), western massage, applied kinesiology and natural internal medicines, which may include herbs, minerals, animal by-product, homeopathic dilutions and nutritional supplements, which may be administered for oral consumption or topical application and may be in the form of teas, pills, powders, tinctures or sterile injectable. I understand that certain herbal teas may need to be cooked or otherwise prepared by me according to the instructions provided by the acupuncture physician. I also understand that certain teas may have an unpleasant smell or taste. I understand that it is my responsibility to notify a member of the clinical staff of any unanticipated or disturbing effects associated with the consumptions of these medicines. I understand that it is my responsibility to inform my physician of any and all other medications that I am taking so that any untoward interactions can be avoided. Although negative interactions are rare, I do understand that the correct medial knowledge concerning interactions of prescription pharmaceuticals with herbs and other natural supplements is incomplete.I have been informed that acupuncture and its related modalities is a safe method of treatment with few and infrequent side effects. The side effects may include bruising, temporary numbness or tingling near the needle sites, temporary lightheadedness which may last for an hour or more, or fainting due to “needle shock”. Significant bruising is a common side effect of cupping and scraping modalities. Burns and/or scarring are unlikely potential risks of moxibustion treatment. Rare and unusual risks of acupuncture treatment include spontaneous miscarriage, nerve damage, organ injury and pneumothorax. Infection is another rare, yet possible risk of acupuncture. My practice complies with the highest industry standards and legal requirements by using only pre-sterilized disposable needles and maintaining a clean and safe working environment. I understand that this document describes only the known major risks and possible side effects of acupuncture and related treatments. The herbs and other nutritional supplements that are used in my practice are considered safe but may be toxic if consumed in large doses. Some supplements may be contraindicated during pregnancy. I understand that I must carefully follow the acupuncture physician’s instructions regarding dosage and other usage parameters. I further understand that I must inform my acupuncture physician if I am or if I become pregnant.I understand that positive results of treatment are not guaranteed. I understand that all my medical records will be kept confidential and will not be copied or view by others without my express written consent, except as may be required by legal mandate.By voluntarily signing this form, I am indicating that I have read (or had read to me) this “Consent to Treatment” and have had the opportunity to ask questions about any concerns. I intend this consent to cover the entire course of treatments for my present condition and for any future conditions for which I might seek treatment from this acupuncture physician.

PATIENT’S NAME: _________________________________________________________ Date: ________________________________________ Please print name.
Patient Signature: ________________________________________________________ Relationship to patient: ______________________________ (or legal representative)
MARIA E. BELLUCCIO, R.N, A.P., D.O.M.

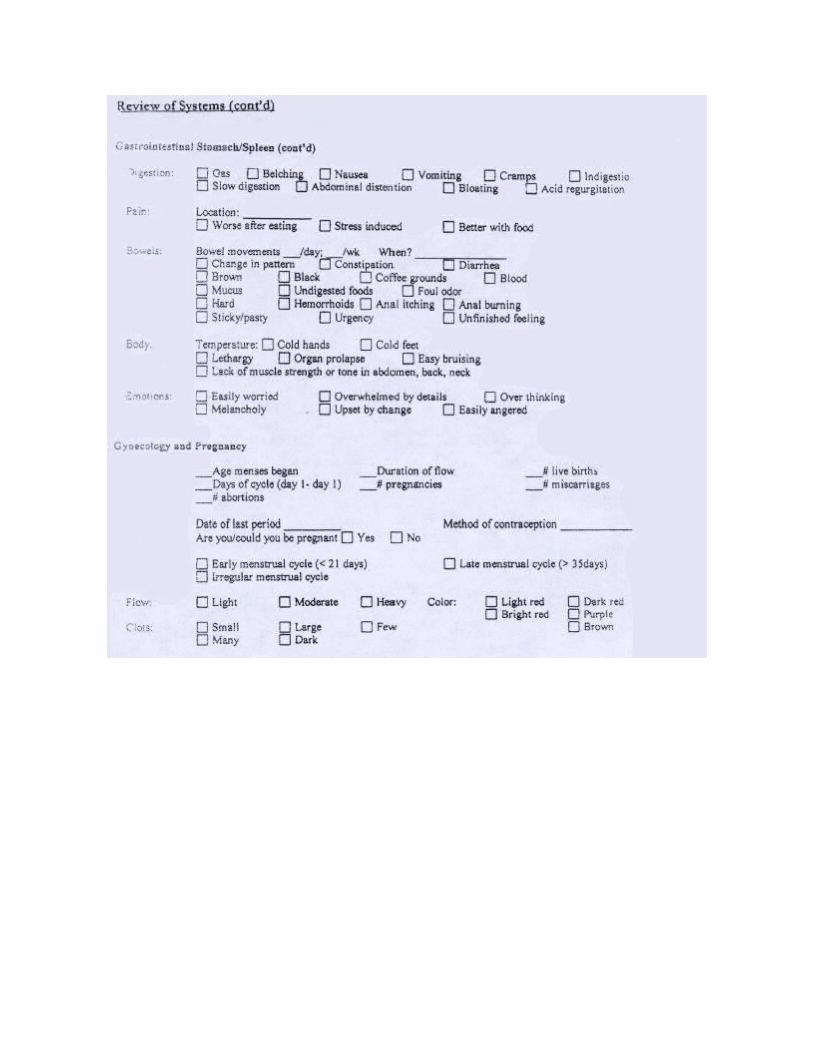
PATIENT HISTORY




HIPAA Compliance Document-Concerning Your Protected Health Information
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
The covered entity is required by law to maintain the privacy of protected health information and to provide individuals with notice of its legal and privacy practices with respect to protected health
information;
For purposes of this notice, the term “covered entity” refers to Lotus Path Wellness Center, Dr. Maria Belluccio, and office staff.
Dear Patient: You have rights concerning your private health information, your access to this information and to know how this information is used by our office. You also have rights related to our ability to contact you concerning your activity in our practice, such as recall reminders, billing, and other matters related to how we communicate with you and others on your behalf. Please understand that this office and each and all of its employees and associates make every effort possible to keep confidential your private medical information at all times and with your consent only, will such information ever be shared with others.
A. The covered entity may contact the individual to provide appointment reminders or information about treatment alternatives or other health-related benefits and services that may be of interest to the individual.B. Your information will not be shared with any third party without your express written consent.C. Your records are available to you for your review, copying or corrections by appointment and you will not be denied access to your personal health information. Any changes you request to your personal health information must be supplied to this office in writing and you will be advised within 30 days of any objection to the correction, or that the correction has been made.D. With respect to other providers requesting your personal health information, we will require a written authorization for the release of medical records signed by you, detailing the name, address and phone number of the requesting physician or facility. Under no circumstance will we discuss your personal health information with anyone without your express permission in writing. (This will of course exclude any office staff that has necessary access to your record)
I have received a copy of this Privacy Notice
Patient Signature__________________________________ Date___________________
Print Your Name _______________________________________




![media.razoo.com€¦ · Web viewWe can’t wait to celebrate the difference your generosity will make. Sincerely, (Your name) ... If you love [Mission aka “rescuing animals”],](https://img.dokumen.tips/doc/110x75/5af9d63d7f8b9a2d5d8d715a/mediarazoocom-web-viewwe-cant-wait-to-celebrate-the-difference-your-generosity.jpg)



























