Embed Size (px)
Citation preview

Training & Testing266
Kirkeberg JM et al. Protocols for Verifying VO 2max … Int J Sports Med 2011; 32: 266 – 270
accepted after revision November 18, 2010
Bibliography DOI http://dx.doi.org/ 10.1055/s-0030-1269914 Published online: January 26, 2011 Int J Sports Med 2011; 32: 266 – 270 © Georg Thieme Verlag KG Stuttgart · New York ISSN 0172-4622
Correspondence Dr. Robert W. Pettitt Department of Human Performance Minnesota State University Mankato Mankato, MN 56001 Tel.: + 1 / 507 / 389 1811 Fax: + 1 / 507 / 389 5618 [email protected]
Key words ● ▶ graded exercise ● ▶ oxygen uptake ● ▶ treadmill ● ▶ verifi cation bout
Validity of 3 Protocols for Verifying VO 2max
[23] . Poole et al. [27] observed that such criteria were often surpassed well prior to attainment of VO 2max and exercise intolerance and recom-mended abandonment of such secondary crite-ria. Instead, these authors recommended use of a verifi cation bout. The verifi cation bout subsequent to a GXT has emerged as a technique for identifying ‘ true ’ VO 2max [21] . Some researchers have performed verifi cation bouts on separate days [3, 27] ; how-ever, such protocols require 2 visits which adds time and technician cost. Conversely, others [8, 22] have conducted verifi cation bouts subse-quent to a GXT during a single visit and have reported valid observations of ‘ true ’ VO 2max . Unfortunately, authors of these studies neglected to report validity data of these measures that take into account individual subject variations, which can be problematic in measurement research [14] . A second concern is that most studies utilized supra-maximal intensities for their verifi cation bouts [3, 8, 11, 22] . Too high of an intensity for the verifi cation bout may result in too short of an exercise duration for VO 2 to achieve maximum consistently between subjects [22] . Therefore, we examined the consistency of VO 2max values derived from 3 diff erent GXT dura-
Introduction ▼ Maximal volume of oxygen uptake (VO 2max ) rep-resents the limit to which oxygen delivery and uptake within exercising muscles can occur [19] . The VO 2max represents maximal aerobic capacity and its measurement is used to appraise health and performance as well as develop exercise pre-scriptions. Hill and Lupton [12] introduced the aerobic capacity concept in 1923, although whether these researchers implied that a fi nite measure of VO 2max was characterized by a pla-teau in VO 2 relative to increased work rate has been questioned [24] . Indeed, contemporary researchers have suggested a ‘ true ’ VO 2max can be demonstrated without a plateau phenomenon [7, 29] . Traditionally, a graded exercise test (GXT) dura-tion of 8 – 12 min was suggested as optimum [6] ; however, this dogma has been questioned [20] . Howley et al. [15] originally summarized a host of secondary criteria for verifying attainment of VO 2max obtained during a GXT. The most prev-alent of these criteria actually reported in research studies are a respiratory exchange ratio (RER) above 1.10 and attainment within 10 bpm of age-predicted heart rate maximum (HR max )
Authors J. M. Kirkeberg 1 , 2 , L. C. Dalleck 1 , 3 , C. S. Kamphoff 1 , R. W. Pettitt 1
Affi liations 1 Department of Human Performance, Minnesota State University, Mankato, Mankato, United States 2 Cardiopulmonary Rehabilitation, Havasu Regional Medical Center, Lake Havasu City, United States 3 Department of Sport and Exercise Science, University of Auckland, Auckland, New Zealand
Abstract ▼ The verifi cation bout has emerged as a technique for confi rming ‘ true ’ VO 2max ; however, validity during a single visit is unknown. We evaluated 3 diff erent GXT durations with severe intensity verifi cation bouts. On 3 separate days, in coun-terbalanced order, 12 recreational-trained men completed short (9 ± 1 min), middle (11 ± 1 min), and long (13 ± 2 min) duration GXTs followed by exhaustive, sine wave verifi cation bouts during the same visit. Intensities for verifi cation were set at speeds equivalent to 2-stages minus end-GXT speed. No diff erences (p < 0.05) in VO 2max
(mL / kg / min) were observed between short (49.1), middle (48.2), and long (48.8) protocols. In addi-tion, no diff erences in verifi cation bout duration occurred between protocols (3 ± 1 min). Validity of VO 2max was strongest for the middle duration protocol (ICC α = 0.97; typical error = 1 mL / kg / min; CV = 2 % ). A small, but signifi cantly higher HR max ( ~ 1 – 2 bpm) was observed for the long protocol. Maximum respiratory exchange ratios were inconsistent (ICC α ranged 0.58 – 0.68). Our fi ndings indicate GXT-verifi cation bout testing during a single visit is a valid means of measur-ing ‘ true ’ VO 2max . The 10 min target for GXT dura-tion was the optimum.
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

Training & Testing 267
Kirkeberg JM et al. Protocols for Verifying VO 2max … Int J Sports Med 2011; 32: 266 – 270
mounting with the aid of arm rails and straddling the treadmill belt at the point of intolerance. Speed was decreased from the end speed (S end ) to an intensity of 0.50 (S end – 134 m / min) + 134 m / min for a 3 min cool-down exercise period, as per our pilot work (refer to discussion for details on cool-down intensity). Follow-ing the cool-down period, the subject began an exhaustive, sine wave verifi cation bout (i. e., constant speed). Intensity for the verifi cation bout was equivalent to S end minus 2 stages, where stages were derived using equation c . Prior to commencing the study, pilot testing on recovery durations and intensities, along with verifi cation bout intensities were examined. Although prior investigators [8, 11, 22] have used a supramaximal intensity for the verifi cation bout, our pilot testing revealed our protocol was more suitable for permitting at least a 2 min verifi cation bout subsequent to the 3 GXT durations tested. As subjects indicated their desire to terminate exercise with a thumb up gesture, in both the GXT and verifi cation bouts, they were asked to rate their level of perceived exertion (RPE ranging 6 – 20) by pointing to a chart [5] .
Statistical analyses Separate one way analyses of variance (ANOVA) with repeated measures and Bonferroni adjustment for post hoc analysis were used to test for duration diff erences. Separate 2-way ANOVAs with repeated measures were used to compare VO 2max , RER max , and HR max between the 3 GXT durations and corresponding verifi ca-tion bouts. Relative validity between the GXT and verifi cation bout for each physiological measurement was determined using intraclass correlations (ICC α ). Typical error (or standard error of measurement), both average variation and coeffi cient of variation (CV), were determined using the techniques described by Hop-kins [14] . Alpha for all inferential statistics was set at 0.05.
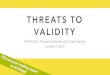
Results ▼ Exercise durations and VO 2max Short, middle, and long GXT durations were achieved using the procedures expressed in equations a through c ( ● ▶ Table 1 , left column). ● ▶ Fig. 1 illustrates a representative subject in each of the 3 protocols. Diff erences in GXT durations (p < 0.05), along with S end ( ● ▶ Table 1 , middle column), did not evoke appreciably diff erent durations of the verifi cation bouts (p = 0.13) ( ● ▶ Table 1 , right column). GXT-verifi cation mean VO 2max values (mL / kg / min) for the short, middle, and long durations were 49.1, 48.2, and 48.8, respectively. VO 2max values did not diff er between the GXT durations (p = 0.22) nor between any of the GXTs and verifi -cation bouts (p = 0.19) ( ● ▶ Table 2 ). Validity analyses indicated that the middle duration yielded more consistent GXT and veri-fi cation maximum values for VO 2 and HR ( ● ▶ Table 3 ). Finally, no diff erence (p = 0.73) in VO 2max values was observed between test days, a fi nding indicating that our subjects did not experience an order-eff ect with the metabolic testing.
tions and subsequent submaximal, severe intensity [13] verifi -cation bouts. Our hypothesis was that the 10 min target duration (middle) would yield more consistent VO 2max values in compari-son to 8 min (short) or 14 min (long) target durations. We also examined the secondary criteria of RER above 1.10 and HR max for each protocol, as these are the most commonly reported sec-ondary criteria for confi rming VO 2max [23] .
Materials and Methods ▼ Subjects 12 recreational-trained men (age: 29 ± 7 years; body mass: 90 ± 13 kg; height: 181 ± 8 cm) volunteered to engage in 3 exer-cise trials on 3 separate days. Exclusion criteria included pre-existing medical conditions aff ecting metabolism (e. g., diabetes, renal disease, etc.) along with a history of musculoskeletal inju-ries or surgeries that might aff ect running performance. Subjects affi rmed verbally that they avoided food and beverages contain-ing alcohol, non-prescription drugs, caff eine, or supplements along with refraining from strenuous exercise 24 h preceding each test day. Testing for each subject was conducted approxi-mately 1 week apart at the same time of day. Written informed consent was obtained and all procedures were pre-approved by the host university institutional review board, in accordance with ethical standards of the International Journal of Sports Medicine [10] .
Experimental procedures Upon entering the laboratory, each subject ’ s height and mass were measured directly. These data along with their response to a question on their physical activity rating [9] , scaled from 0 to 10, were inserted into a non-exercise VO 2max prediction equation [16] . Treadmill speed required to evoke VO 2max (S peak ) at a 3 % grade was calculated by the following metabolic equations [1] : [a] W peak (m / min) = (Relative VO 2max – 3.5) / 0.2 [b] 3 % Grade S peak = S peak – (S peak * 0.027) Where 3.5 represents resting VO 2 , 0.2 assumes an additional mL O 2 / kg / min for each m / min rise in running speed, and 0.027 rep-resents the correction factor for grade. In counterbalanced fashion, subjects completed one of 3 GXT protocols at a 3 % grade whereby speed began at 134 m / min and advanced to a specifi c speed (rounded to the nearest 2.68 m / min, the limit of the treadmill used). A 2 min warm-up of walking at 67 m / min preceded each protocol. Speed increments for each minute were calculated for short (8 min), middle (10 min), and long (14 min) target durations using: [c] Increment = [(3 % Grade S peak – 134) / (target duration)] Where 1.34 m / min is starting speed and the speed evoking the target duration commences 1 min prior to the expected VO 2 response. For example, if 10 min is the target duration for evok-ing the predicted VO 2max , S peak would be set at 9 min. A heart rate strap (Polar Instruments, Oulu, Finland) was affi xed to the tho-rax and heart rate was recorded telemetrically by a metabolic analyzer (Parvomedics TrueOne, Sandy, UT). The analyzer also recorded expired VO 2 and VCO 2 , on a breath by breath basis; however, the data were averaged to 30 s time samples, as 30 s time-sampling is the most commonly reported technique [28] . Flow and gas calibration was performed prior to each test as per the manufacturer ’ s guidelines. Subjects were given strong verbal encouragement for each test. Termination of the GXT was determined by the subject dis-
Table 1 Peak exercise durations (M ± SD) for the 3 protocols.
Protocol GXT Duration
(min)
End Speed
(m / min)
Verifi cation
Duration (min)
short 9.22 ± 1.21 224 ± 17 2.78 ± 0.46 middle 10.78 ± 1.31 a 213 ± 16 a 3.08 ± 0.80 long 13.06 ± 2.25 a,b 206 ± 18 a,b 3.45 ± 1.01 a Diff erent from short; b diff erent from middle (p < 0.05)
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

Training & Testing268
Kirkeberg JM et al. Protocols for Verifying VO 2max … Int J Sports Med 2011; 32: 266 – 270
Secondary criteria RER was lower in the verifi cation bouts vs. the GXT protocols (main eff ect, p < 0.05) and was lower for the long vs. the short or middle durations (interaction, p < 0.05). As such, RER max consis-tency between the GXT and verifi cation bout was weak ( ● ▶ Table 3 ). Summarized in ● ▶ Table 2 , the long duration GXT
evoked the highest HR max values (p < 0.05) both subsequent to the GXT and verifi cation bouts, respectively. Nearly all subjects (11 of 12) achieved within 10 bpm of age-predicted HR max , as estimated using 220 minus age. Most subjects achieved an RER above 1.10 in the short (7 of 12) and middle (9 of 12) GXT proto-cols; however, the frequency of this criterion decreased for the long (3 of 12) protocol.
Discussion ▼ Our study is the fi rst to demonstrate high test-retest consistency between the GXT-verifi cation bouts for same day testing using intensities below the S end . Correlation coeffi cient values in our study exceed those reported by Astorino et al. (r = 0.89) [3] , who performed their verifi cation bouts on a separate day from the GXT. The CV for our middle duration (2.1 % ) was less than the variability reported by Midgley et al. [22] (3.5 and 3.9 % ) and Hawkins et al. [11] (3.2 and 4.3 % ). Thus, equal if not superior verifi cation bouts can be accomplished during a single testing session. One criticism raised by Noakes [25] is when researchers con-clude ‘ true ’ VO 2max exists when grouped means between 2 tests do not diff er signifi cantly from each other. Specifi cally, he argued that one or more subjects may diff er substantially on 2 tests but not render 2 sets of observations statistically diff erent. The issue of how to judge whether individual subjects vary on repeated measures of a test was addressed eloquently by Hopkins [14] . He recommended absolute measures of consistency (i. e., typical error and CV) are the appropriate statistics that help the exercise scientist judge how robust a measurement technique is from a practical standpoint. In our middle duration protocol (10 min target GXT), variability was ~ 1 mL / kg / min (CV of 2 % ) between the GXT and verifi cation bout ( ● ▶ Table 3 ). This variability is nearly one half that of the absolute variability values reported by prior studies using verifi cation bouts. Thus, our fi ndings are both signifi cant and practically relevant. Smaller increment GXTs (longer target durations) resulted in lower S end values, a fi nding consistent with others [2, 6, 30] . Despite using diff erent intensities for the 3 constant-speed veri-fi cation bouts, based on S end , no diff erences in verifi cation dura-tions were observed ( ● ▶ Table 1 ). Such a fi nding refutes the possible notion that diff erences in GXT duration infl uence exer-cise tolerance during a verifi cation bout that commences shortly following the termination of a GXT. Similar verifi cation bout
Short
60
50
40
30
20
10
0
60
50
40
30
20
10
0
60
50
40
30
20
10
0
0 5 10
Middle
Long
Time (min)
15 20
0 5 10 15 20
0 5 10 15 20
VO2
(mL/
kg/m
in)
VO2
(mL/
kg/m
in)
VO2
(mL/
kg/m
in)
Fig. 1 Representative mean VO 2max (mL / kg / min) values during the short (50.8), middle (51.7), and long (50.3) protocols for 23-year-old subject.
Table 2 Physiological variables (M ± SD) from the 3 protocols.
GXT Verifi cation Bout
VO 2max (mL / kg / min) short 49.24 ± 5.31 48.97 ± 5.95 middle 48.90 ± 5.08 47.45 ± 4.48 long 49.07 ± 4.70 48.44 ± 5.02 RER max short 1.11 ± 5.23 1.00 ± 4.99 c middle 1.10 ± 4.14 1.01 ± 4.59 c long 1.07 ± 3.13 b 1.00 ± 3.44 c HR max (bpm) short 187.7 ± 9.6 185.3 ± 9.6 middle 186.5 ± 9.7 185.8 ± 9.2 long 188.8 ± 7.1 a 188.7 ± 6.6 a a Higher than middle and short; b Lower than short and middle; c Lower than GXT (p < 0.05)
Table 3 Intraclass correlation ( α ), typical error, coeffi cient of variation ( % ) for the 3 duration GXTs and corresponding verifi cation bouts.
ICC Typical Error Coeffi cient of Variation
VO 2max α mL / kg / min % short 0.89 1.87 3.8 middle 0.95 1.04 2.1 long 0.91 1.44 3.0 HR max α bpm % short 0.95 2.1 1.1 middle 0.97 1.6 0.9 long 0.96 1.4 0.8 RER max α L · L −1 % short 0.58 0.03 3.1 middle 0.58 0.03 2.7 long 0.68 0.02 1.8
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

Training & Testing 269
Kirkeberg JM et al. Protocols for Verifying VO 2max … Int J Sports Med 2011; 32: 266 – 270
durations occurred conceivably because aggregate energy expenditures (i. e., aerobic contribution and depletion of anaero-bic capacity) were similar between the 3 GXTs as a function of the power-duration relationship; however, direct methods to quantify total expenditure in the present study were not made. In the present study, we observed lower CV measures for our GXT and verifi cation bouts in comparison to prior groups [11, 22] . Less variability in our study may be explained by the fact that these research groups used supramaximal intensities for verifi cation stages whereas our protocol was below S end . 2 other groups [7, 29] have reported submaximal loads success-fully verifi ed VO 2max ; however, neither reported absolute mea-sures of variability making comparisons diffi cult. Use of submaximal intensities may provide better verifi cation mea-sures of VO 2max in that too high of an intensity during the verifi -cation bout may prohibit attainment of a valid VO 2max (e. g., verifi cation bouts lasting only 1 – 2 min) [21] . Hill et al. [13] described that attainment of VO 2max during constant-load, severe exercise conforms to the same hyperbolic relationship existing between power and exercise tolerance (i. e., intensities above the critical power (CP) which evoke a slow component of VO 2 approaching maximum at a faster rate). Indeed, small increases in intensity above the CP increases the rates at which metabo-lites such as H + and P i accumulate within the exercising muscle [17] . Hill et al. [13] referred to this concern as the fourth exercise domain; an intensity above CP in which local fatigue results in too short of an exercise duration for attaining VO 2max . In an eff ort to prescribe a severe intensity for our verifi cation bouts but not encroach the fourth exercise domain (NB, a greater concern for our short target duration), we assigned our verifi cation intensi-ties using 2-stages preceding S end , a decision based on pilot work. Such a protocol permitted our sample of recreational-trained men to exercise a suitable duration for each verifi cation bout ( ● ▶ Table 1 ). A second diff erence with our study, observing lower CV mea-sures between GXT and verifi cation bouts, in comparison to prior groups [11, 22] , was our use of a custom GXT protocol. Hawkins et al. [11] used the same % grade increment increase, for men and women; however, these authors did not report GXT durations which would expectantly be diff erent based on diff er-ences in aerobic capacity. Conversely, Midgley et al. [22] used a custom protocol that netted a GXT duration of ~ 12 min. Although prior data suggest GXT duration is less relevant for yielding sim-ilar VO 2max values [20] ; the eff ect of GXT duration on a subse-quent, same day verifi cation bout has not been reported. At the onset of the study, we applied a regression technique [9, 16] we deemed appropriate for our sample of recreational-trained sub-jects, to derive an expected GXT duration. The ability to validly prescribe GXT durations, with non-exercise regression equations, on highly-trained athletes is an area in need of further analysis. Also based on pilot work, we selected 50 % of the diff erence in starting speed and S end to serve as the intensity for our active recovery. We speculated this would minimize risk of syncope subsequent to the GXT; yet, be low enough of an intensity to eliminate reliance on the fast glycolytic energy pathway (i. e., lactate production). Indeed, cool-down exercise at intensities below threshold can augment clearance of blood lactate and increase hepatic production of blood glucose along with muscle glycogen synthesis [4] . Postexercise VO 2 values preceding com-mencement of the verifi cation bout decreased below 50 % of the diff erence in VO 2max during the GXT and VO 2 values at the start of the verifi cation bout (see ● ▶ Fig. 1 for representative). Other
investigators have used extremely low intensities for their cool-down exercise period [8, 22] . One reservation for using too low of a cool-down intensity is that the verifi cation bout is too abrupt [22] . Conversely, use of a moderate intensity (below threshold) may help better maintain circulation of oxygen and regulatory hormones along with metabolic inertia within the engaged skel-etal muscles [26] . Achievement of a RER above 1.10 has been suggested as a sec-ondary criterion for verifying VO 2max [15] . Poole et al. [27] rec-ommended abandoning this criterion based on the observation that many of their subjects surpassed a RER of 1.10 well prior to attaining VO 2max . In the present study, RER max values for the verifi cation bouts were lower than the GXTs for each protocol we examined. Rossiter et al. [29] reported similar trends for RER, when same-day GXTs were performed, for both their submaxi-mal and supramaximal verifi cation trials. The likely cause for lower RER values during same day verifi cation is a diminished non-metabolic CO 2 production (i. e., VO 2 between the GXT and verifi cation were similar, see ● ▶ Table 2 ). We also noted that RER max fl uctuated frequently between test days, was inconsist-ent between the GXTs and verifi cation bouts ( ● ▶ Table 3 ), and that many of our subjects failed to achieve the 1.10 criterion for their GXT. As such, our fi ndings concur with Poole et al. that RER fails to serve as a valuable metric for VO 2max testing. Similar to the above 1.10 RER criterion, attaining within 10 bpm of age-predicted HR max has also been suggested for verifying attainment of VO 2max [15] ; however, this criterion has also been criticized [27] . Midgley et al. [22] argued that age-predicted HR max may infl ate estimates on athletes who routinely experi-ence trained-induced decreases in HR max . Alternatively, these authors suggested a comparison of HR max from the GXT and ver-ifi cation bout may serve as a more useful secondary criterion due to the improbability of voluntarily replicating 2 submaximal HR max values from incremental and constant-load exercise bouts carried out to intolerance. Interestingly, our data actually dem-onstrates this is possible ( ● ▶ Table 2 ). Specifi cally, we observed a small, but signifi cant increase in HR max for the long duration GXT and subsequent verifi cation bout, although most subjects achieved 10 bpm of age-predicted HR max for each protocol. Achievement of this slightly higher HR max ( ~ 1 – 2 bpm) during the long protocol was consistent among subjects ( ● ▶ Table 3 ) and occurred despite observations that slightly lower HR max values were observed between the shorter GXT and verifi cation bouts. We are confi dent subjects gave a maximal eff ort based on rat-ings of perceived exertion. Therefore, our only explanation for this fi nding is the diff erence in total duration between protocols. At very high intensities, HR is mediated by circulating catecho-lamine concentrations [18] . The long protocol perhaps permit-ted better humoral activation of cardiac pacing cells. When target GXT durations were estimated for 8, 10, and 14 min, using equations a – c , subjects achieved VO 2max in GXT durations comparable to those targets ( ● ▶ Table 1 ). Should a practitioner desire to achieve GXT durations between 8 and 12 min, our rec-ommendation is to select 10 min as the target. Albeit longer pro-tocols (e. g., 13-min) may evoke higher and ‘ true ’ HR max values ( ● ▶ Table 2 ), the expense of such is a compromise of less consist-ent verifi cation of VO 2max ( ● ▶ Table 3 ). Although longer duration GXTs may be equally valid [20] , the spirit of the original study by Buchfuhrer et al. [6] was to demonstrate that a valid measure of VO 2max may be gained in a shorter duration. Our fi ndings indi-cate that 10 min is the optimum GXT duration to strive for when attempting GXT-verifi cation bouts within the same session. Such
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

Training & Testing270
Kirkeberg JM et al. Protocols for Verifying VO 2max … Int J Sports Med 2011; 32: 266 – 270
a hypothesis, however, should be explored using women, on subjects with diff erent fi tness levels, and using diff erent modes of exercise. The non-signifi cant mean diff erences between GXT and verifi ca-tion bouts ( ● ▶ Table 2 ), combined with the high level of consist-ency in measurement ( ● ▶ Table 3 ) begs the question, why administer a verifi cation bout if it yields the same result? The answer is implied in the name of the technique: to verify the GXT result. Such a procedure is useful particularly when indi-viduals fail to experience a plateau in VO 2 despite an encouraged best eff ort, which is reportedly common [7] . Thus, concerning the verifi cation bout, the more relevant question is what diff er-ence between the GXT and verifi cation VO 2 tests is acceptable for concluding ‘ true ’ VO 2max has been measured? Midgley et al. [21] suggested that ~ 2 % diff erence would be acceptable; how-ever, their recommendation was derived on the error of the metabolic device without consideration for normal biological variation. Thus, such a criterion may be too conservative. If 30 s sampling is used, we recommend ‘ true ’ VO 2max on recreational-trained men is verifi ed when GXT and verifi cation measures dif-fer less than 3 % . Using typical errors of the present study, that criterion would approximate to a relative VO 2 criterion of less than 1.5 mL / kg / min. Clearly, such standards would vary for dif-ferent sampling rates and diff erent fi tness levels. Thus, more research is needed in this regard. In summary, the ability to measure ‘ true ’ VO 2max has implica-tions for monitoring aerobic capacity in response to training and for prescribing exercise intensities [19] . We compared VO 2max values between GXTs and severe intensity verifi cation bouts car-ried out for 3 separate test durations in recreational-trained men. Albeit, small but signifi cantly higher HR max values were observed in the long protocol, the 10 min target duration yielded the most consistent results for VO 2max verifi cation. The severe intensity verifi cation bout (below S end ) provides better consist-ency of VO 2max measurements in comparison to previous studies utilizing supramaximal intensities (i. e., above S end ). The verifi ca-tion bout subsequent to a GXT during a single visit is a promis-ing technique for determining ‘ true ’ VO 2max . Therefore, future research on same day GXT-verifi cation protocols is warranted.
References 1 ACSM’s Guidelines for Exercise Testing and Prescription . Baltimore: Lip-
picott, Williams & Wilkins ; 2010 2 Astorino TA , Rietschel JC , Tam PA , Taylor K , Johnson SM , Freedman TP ,
Sakarya CE . Reinvestigation of optimum duration of VO 2max testing . J Exerc Physiol 2004 ; 7 : 1 – 8
3 Astorino TA , White AC , Dalleck LC . Supramaximal testing to confi rm attainment of VO 2max in sedentary men and women . Int J Sports Med 2009 ; 30 : 279 – 284
4 Belcastro AN , Bonen A . Lactic acid removal rates during controlled and uncontrolled recovery exercise . J Appl Physiol 1975 ; 39 : 932 – 936
5 Borg GAV . Borg’s Perceived Exertion and Pain Scales . Champaign, IL: Human Kinetics ; 1998
6 Buchfuhrer MJ , Hansen JE , Robinson TE , Sue DY , Wasserman K , Whipp BJ . Optimizing the exercise protocol for cardiopulmonary assessment . J Appl Physiol 1983 ; 55 : 1558 – 1564
7 Day JR , Rossiter HB , Coats EM , Skasick A , Whipp BJ . The maximally attainable VO 2 during exercise in humans: the peak vs. maximum issue . J Appl Physiol 2003 ; 95 : 1901 – 1907
8 Foster C , Kuff el E , Bradley N , Battista RA , Wright G , Porcari JP , Lucia A , deKoning JJ . VO 2max during successive maximal eff orts . Eur J Appl Physiol 2007 ; 102 : 67 – 72
9 George JD , Stone WJ , Burkett LN . Non-exercise VO 2max estimation for physically active college students . Med Sci Sports Exerc 1997 ; 29 : 415 – 423
10 Harriss DJ , Atkinson G . International Journal of Sports Medicine – Eth-ical Standards in Sport and Exercise Science Research . Int J Sports Med 2009 ; 30 : 701 – 702
11 Hawkins MN , Raven PB , Snell PG , Stray-Gundersen J , Levine BD . Maxi-mal oxygen uptake as a parametric measure of cardiorespiratory capacity . Med Sci Sports Exerc 2007 ; 39 : 103 – 107
12 Hill AV , Lupton H . Muscular exercise, lactic acid, and the supply and utilization of oxygen . Q J M 1923 ; 16 : 135 – 171
13 Hill DW , Poole DC , Smith JC . The relationship between power and the time to achieve. VO 2max . Med Sci Sports Exerc 2002 ; 34 : 709 – 714
14 Hopkins WG . Measures of reliability in sports medicine and science . Sports Med 2000 ; 30 : 1 – 15
15 Howley ET , Bassett DR Jr , Welch HG . Criteria for maximal oxygen uptake: review and commentary . Med Sci Sports Exerc 1995 ; 27 : 1292 – 1301
16 Jackson AS , Blair SN , Mahar MT , Wier LT , Ross RM , Stutesville JE . Predic-tion of functional aerobic capacity without exercise testing . Med Sci Sports Exerc 1990 ; 22 : 863 – 870
17 Jones AM , Wilkerson DP , DiMenna F , Fulford J , Poole DC . Muscle meta-bolic responses to exercise above and below the “ critical power ” assessed using 31P-MRS . Am J Physiol 2008 ; 294 : R585 – R593
18 Laughlin MH . Cardiovascular response to exercise . Am J Physiol 1999 ; 277 : S244 – S259
19 Levine BD . VO 2max : what do we know, and what do we still need to know? J Physiol 2008 ; 586 : 25 – 34
20 Midgley AW , Bentley DJ , Luttikholt H , McNaughton LR , Millet GP . Chal-lenging a dogma of exercise physiology: does an incremental exercise test for valid VO 2max determination really need to last between 8 and 12 min? Sports Med 2008 ; 38 : 441 – 447
21 Midgley AW , Carroll S . Emergence of the verifi cation phase procedure for confi rming ‘ true ’ VO 2max . Scand J Med Sci Sports 2009 ; 19 : 313 – 322
22 Midgley AW , McNaughton LR , Carroll S . Verifi cation phase as a useful tool in the determination of the maximal oxygen uptake of distance runners . Appl Physiol Nutr Metab 2006 ; 31 : 541 – 548
23 Midgley AW , McNaughton LR , Polman R , Marchant D . Criteria for deter-mination of maximal oxygen uptake: a brief critique and recommen-dations for future research . Sports Med 2007 ; 37 : 1019 – 1028
24 Noakes TD . How did A V Hill understand the VO 2max and the “ plateau phenomenon? ” Still no clarity? Br J Sports Med 2008 ; 42 : 574 – 580
25 Noakes TD . Maximal oxygen uptake as a parametric measure of cardi-orespiratory capacity: comment . Med Sci Sports Exerc 2008 ; 40 : 585
26 Perrey S , Scott J , Mourot L , Rouillon JD . Cardiovascular and oxygen uptake kinetics during sequential heavy cycling exercises . Can J Appl Physiol 2003 ; 28 : 283 – 298
27 Poole DC , Wilkerson DP , Jones AM . Validity of criteria for establishing maximal O 2 uptake during ramp exercise tests . Eur J Appl Physiol 2008 ; 102 : 403 – 410
28 Robergs RA , Dwyer D , Astorino T . Recommendations for improved data processing from expired gas analysis indirect calorimetry . Sports Med 2010 ; 40 : 95 – 111
29 Rossiter HB , Kowalchuk JM , Whipp BJ . A test to establish maximum O 2 uptake despite no plateau in the O 2 uptake response to ramp incre-mental exercise . J Appl Physiol 2006 ; 100 : 764 – 770
30 Yoon BK , Kravitz L , Robergs R . VO 2max , protocol duration, and the VO 2 plateau . Med Sci Sports Exerc 2007 ; 39 : 1186 – 1192
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.