Embed Size (px)
Citation preview

Eye & Contact Lens
Ultraviolet A and Riboflavin Therapy as an Adjunct in Corneal Ulcer Refractory to Medical TreatmentAyhan Sağlk, M.D., Ömür Ö. Uçakhan, M.D., Ayfer Kanpolat, M.D.DisclosuresEye Contact Lens. 2013;39(6):413-415.
Abstract and Introduction
Abstract
Objective: To present a case of corneal ulcer unresponsive to medical treatment, successfully treated with the use of ultraviolet (UV) A and riboflavin collagen crosslinking (CXL) administered twice.
Methods: A 68-year-old diabetic male patient was diagnosed with unilateral severe corneal ulcer. Gram and Giemsa stains and corneal culture results were performed twice, but no specific pathogen could be detected. The clinical presentation suggested fungal infection. The ulcer was unresponsive to extensive medical treatment administered for 10 days. There was an initial response to topical and intrastromal voriconazole administration; however, this was followed by reactivation. Therefore, UVA-riboflavin treatment was performed when the patient was still on medical therapy.
Results: The stromal infiltrate appeared inactive 1 week after UVA-riboflavin CXL treatment. However, reactivation was noticed on the second week, and a second UVA-riboflavin treatment was planned and performed 3 weeks after the first one. The epithelial defect disappeared, and the stromal infiltrate stayed inactive starting from the first week of the second UVA-riboflavin treatment until the last follow-up examination at month 6.
Conclusion: The UVA-riboflavin CXL may be considered in the management of corneal ulcers unresponsive to medical management.

Introduction
Riboflavin and ultraviolet (UV) A collagen crosslinking (CXL) of the cornea was first introduced by Wollensak et al.[1] in 2003 for the treatment of keratoconus. This method has a stiffening effect on the corneal stroma, which increases its biomechanical strength, thus enabling the arrest of the progression of the disease.
Recent clinical and in vitro studies have suggested that UVA-riboflavin CXL may be effective in the treatment of corneal ulcers.[2–8] A number of publications have described successful treatment of therapy-resistant infectious ulcers and the arrest of corneal melting with UVA-activated riboflavin.[2,4–6]
We present herein a case of presumed infectious corneal ulcer unresponsive to medical treatment, which was effectively treated with two successive adjuvant UVA-riboflavin CXL therapies.
Case Report
A 68-year-old insulin-dependent diabetic male patient presented with progressive pain, redness, photophobia, tearing, and decreased vision of 1-month duration in his left eye. He had history of cataract extraction and intraocular lens placement 5 years ago on his right eye. On examination, the visual acuities were counting fingers (CF)@3 ft in the right eye and CF@2 ft in the left eye, with no improvement on manifest refraction. The right eye was pseudophakic and had geographic atrophy because of age-related macular degeneration on fundus examination. On the left eye, the patient had conjunctival congestion and hyperemia, a central 2- × 2-mm corneal epithelial defect with deep stromal infiltration, endothelial plaque, moderate anterior chamber reaction, and vascularization extending from the limbus to the corneal infiltrate at 5-o'clock position (Fig. 1A). There was also a prominent nuclear opacification preventing ophthalmoscopy in the left eye. However, ultrasound examination revealed no pathology.
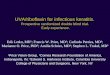
Figure 1.
Slitlamp photograph of the patient (A) showing a 2- · 2-mm central corneal epithelial defect with surrounding stromal infiltrate and conjunctival injection at initial presentation; (B) 2 weeks after the first ultraviolet (UV) A-riboflavin crosslinking (CXL) showing persistence of active infiltration of the stroma with stromal thinning next to the epithelial defect; (C) 1 week after the second UVA-riboflavin

CXL showing resolution of the stromal infiltration; and (D) 6 months after the second UVA-riboflavin CXL showing complete central corneal scarring with no active infiltration or inflammation.
Corneal scrapings were performed twice for Gram and Giemsa staining and cultures; however, laboratory results were negative. The ulcer was unresponsive to extensive medical treatment with gentamicin gtt (14 mg/mL every hour (qs)), cefazolin gtt (50 mg/mL qs), fluconazole gtt (2 mg/mL qs), amphotericin B gtt (0.15 mg/mL qs), and ketoconazole (2 × 200 mg orally) administered for 10 days. Because the clinical appearance suggested fungal infection with a prominent ulceration, deep infiltrate, and an endothelial plaque, with no response to fortified therapy administered for 10 days, the patient was started a new regimen with topical voriconazole (0.01 mg/mL qs); amphotericin B and fluconazole drops were stopped. Intrastromal voriconazole (0.5 mg/mL) injection was performed once. A positive clinical response was noted on the fifth day of voriconazole treatment. However, the ulceration and infiltration was active again on the seventh day of voriconazole treatment, and stromal thinning was noted temporal to the deep stromal infiltrate.
Therefore, UVA-riboflavin CXL treatment was planned and performed as described by Wollensak et al.[1]Briefly, the periocular area was cleaned with povidone-iodine solution. Proparacaine hydrochloride (0.5%) drops were administered, and an eye speculum was inserted. After topical anesthesia, the loose epithelium was removed. Ultrasound pachymetry was attempted to be performed; however, no measurement could be obtained. Riboflavin (Medio-Cross riboflavin/dextran solution, 0.1%) was topically administered for a period 30 minutes at an interval of 2 minutes. The cornea was then illuminated using a UV-X lamp (Peschke Meditrade GmbH, Huenenberg, Switzerland), UVA 365 nm, with an irradiance of 3.0 mW/cm2 and a total dose of 5.4 J/cm2. Riboflavin was continued to be administrated to the cornea during UVA illumination.
Antifungal agents were continued after the UVA-riboflavin CXL therapy. The stromal infiltrate appeared inactive at 1-week follow-up examination, and the patient reported the improvement of his symptoms. However, reactivation was noticed again on the second week (Fig. 1B). A second UVA-riboflavin treatment was planned and performed 3 weeks after the first one. After the second treatment, the epithelial defect disappeared on day 7 (Fig. 1C), stromal infiltrate was inactive, corneal vascularization was distinctive, and the ulcer healed with a scar and prominent vascularization. The antimicrobial agents were tapered and stopped in 3 months. No

activation of the ulcer was noted until the last follow-up examination at month 6, at which time the visual acuity was CF@4 ft, and there was complete scarring of the lesion (Fig. 1D).
Discussion
The combined use of UVA and riboflavin causes photooxidative reactions leading to the development of more collagen crosslinks between the stromal collagen fibers. This changes the intrinsic biomechanical properties of the cornea, increasing its biomechanical strength. This increase in corneal strength has been shown to arrest the progression of keratoconus.[1,9]In addition to keratoconus, the photochemical interaction of UVA and riboflavin used in corneal collagen crosslinking has been applied in the treatment of postlaser in situ keratomileusis corneal ectasia, pseudophakic bullous keratopathy,[10] Fuchs endothelial dystrophy,[11] and, more recently, in infectious keratitis.
In infective keratitis, microbial inactivation occurs via the by-products of riboflavin after UVA exposure. Nucleic acids are damaged by direct electron transfer, production of singlet oxygen, and generation of hydrogen peroxide with the formation of hydroxyl radicals.[12] Photoactivation of riboflavin damages the RNA and DNA of microorganisms by oxidation processes, causing lesions in chromosomal strands.[2] Part of the therapeutic effect of UVA-riboflavin therapy was suggested to be because of the decreased susceptibility of the corneal stroma to proteolytic enzymes produced by the pathogenic bacteria.[13]
Until now, UVA-riboflavin CXL has been shown to effectively treat severe infectious corneal ulcers of various causative factors including bacterial, fungal, and parasitic ulcers, in addition to culture-negative infectious keratitis.[2–6,14] In all but two patients with Acanthamoeba keratitis, the ulcers were reported to show favorable resolution after one UVA-riboflavin CXL therapy.
Direct fungicidal effect of CXL alone has not been proven so far. In vitro studies demonstrated that UVA-riboflavin treatment did not have any effect against Candida albicans,[7] Aspergillus fumigatus, andFusarium sp.[15] However, Sauer et al.[15] showed significant in vitro inhibition growth of test isolates using combined UVA-riboflavin treatment and amphotericin B. The therapeutic effect of combined CXL and antifungal medication has also been shown in previous case studies. Anwar et

al.[6] first showed successful resolution of a culture-proven fungal keratitis (Aspergillus spp.) with UVA-riboflavin CXL, along with antifungal treatment in a human eye. In an animal study, Galperin et al.[3] showed UVA-riboflavin treatment to be useful as a coadjuvant to the medical treatment in resistant Fusarium solanikeratitis infection on rabbit eyes.
Another concern with fungal keratitis is that, in approximately 50% of cases, deep fungal penetration develops,[16] whereas UVA-riboflavin therapy only effects down to about 300 μm from the surface. This fact is another reason why UVA-riboflavin therapy should be considered as an adjunct to antifungal treatment in keratomycosis.
In the case presented herein, although the culture results were negative twice, the clinical presentation suggested fungal etiology. A positive clinical response was noted on the fifth day of voriconazole treatment, again, suggesting fungal etiology. However, reactivation of the stromal infiltration on seventh day of voriconazole treatment, with accompanying stromal melting, tempted us to consider UVA-riboflavin CXL. Initial resolution following CXL was followed by reactivation again, and a second UVA-riboflavin CXL was performed 3 weeks after the first one. This second procedure was successful in arresting the progression of the infiltration and inflammation with favorable clinical resolution. To our knowledge, this is the only case of presumed fungal keratitis treated with two successive UVA-riboflavin CXL applications. The severity of the infection and its central location were the causes of the final limited visual acuity achieved. The UVA-riboflavin CXL obviated the need for therapeutic-penetrating keratoplasty and allowed us to delay keratoplasty to later date when it can be performed in a more controlled manner with a possibly lower risk of subsequent graft failure.
In conclusion, UVA-riboflavin CXL, in combination with antimicrobial therapy, seems to be a promising new technique in the treatment of keratitis. However, the photosensitization protocol used herein may not be the most favorable one for the treatment of corneal ulcers. In addition, the repetition of the procedure should be applied with caution to prevent excessive keratocyte apoptosis and endothelial damage. Further research is required to establish the appropriate photosensitization protocol in keratitis, and until more data are available, CXL should only be considered in therapy-refractive keratitis.

References1. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-A-induced collagen
crosslinking for the treatment of keratoconus. Am J Ophthalmol 2003;135:620–627.2. Khan YA, Kashiwabuchi RT, Martins SA, et al. Riboflavin and ultraviolet light a
therapy as an adjuvant treatment for medically refractive Acanthamoeba keratitis: Report of 3 cases. Ophthalmology 2011;118:324–331.
3. Galperin G, Berra M, Tau J, et al. Treatment of fungal keratitis from Fusarium infection by corneal cross-linking.Cornea 2012;31:176–180.
4. Makdoumi K, Mortensen J, Sorkhabi O, et al. UVA-riboflavin photochemical therapy of bacterial keratitis: A pilot study. Graefes Arch Clin ExpOphthalmol 2012;250:95–102.
5. Morén H, Malmsjö M, Mortensen J, et al. Riboflavin and ultraviolet a collagen crosslinking of the cornea for the treatment of keratitis. Cornea 2010;29:102–104.
6. Anwar HM, El-Danasoury AM, Hashem AN. Corneal collagen crosslinking in the treatment of infectious keratitis.Clin Ophthalmol 2011;5:1277–1280.
7. Martins SA, Combs JC, Noguera G, et al. Antimicrobial efficacy of riboflavin/UVA combination (365 nm) in vitro for bacterial and fungal isolates: A potential new treatment for infectious keratitis. Invest Ophthalmol Vis Sci2008;49:3402–3408.
8. Wollensak G. Corneal collagen crosslinking: New horizons. Exp Rev Ophthalmol 2010;5: 201–215.
9. Wollensak G, Spoerl E, Seiler T. Stress-strain measurements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking. J CataractRefract Surg 2003;29:1780–1785.
10. Ghanem RC, Santhiago MR, Berti TB, et al. Collagen crosslinking with riboflavin and ultraviolet-A in eyes with pseudophakic bullous keratopathy. J Cataract Refract Surg 2010;36:273–276.
11. Hafezi F, Dejica P, Majo F. Modified corneal collagen crosslinking reduces corneal oedema and diurnal visual fluctuations in Fuchs dystrophy. Br JOphthalmol 2010;94:660–661.
12. Baier J, Maisch T, Maier M. Singlet oxygen generation by UVA light exposure of endogenous photosensitizers.Biophys J 2006;91:1452–1459.
13. Spoerl E, Wollensak G, Seiler T. Increased resistance of crosslinked cornea against enzymatic digestion. Curr Eye Res 2004;29:35–40.
14. del Buey MA, Cristóbal JA, Casas P, et al. Evaluation of in vitro efficacy of combined riboflavin and ultraviolet a for Acanthamoeba isolates. Am JOphthalmol 2012;153:399–404.
15. Sauer A, Letscher-Bru V, Speeg-Schatz C, et al. In vitro efficacy of antifungal treatment using riboflavin/UV-A (365 nm) combination and amphotericin B. Invest Ophthalmol Vis Sci 2010;51:3950–3953.
16. Vemuganti GK, Garg P, Gopinathan U, et al. Evaluation of agent and host factors in progression of mycotic keratitis: A histologic and microbiologic study of 167 corneal buttons. Ophthalmology 2002;109:1538–1546.
http://www.medscape.com/viewarticle/814172_2