Embed Size (px)
Citation preview

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Systematic reviews of imaging gynecological and gastrointestinal malignancies for developingevidence-based guidelines
Bipat, S.
Link to publication
Citation for published version (APA):Bipat, S. (2007). Systematic reviews of imaging gynecological and gastrointestinal malignancies for developingevidence-based guidelines. Amsterdam: Shandra Bipat.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 13 Jul 2020

Systematic reviews of imaging gynecological
and gastrointestinal malignancies for
developing evidence-based guidelines
�

� �� �
Thesis: Systematic reviews of imaging gynecological and gastrointestinal malignancies for developing evidence-based guidelinesCopyright: 2007, Shandra Bipat, Amsterdam, The Netherlands
This thesis was prepared at the Department of Radiology, Academic Medical Center, University of Amsterdam, The Netherlands. Part of the research was financially supported by the Dutch Order of Medical Specialists.
Cover by: Shandra Bipat and Jaap StokerLayout: Chris Bor, Medical Photography and Illustration, Academic Medical Center, Amsterdam and Buijten & Schipperheijn, Amsterdam. Printed by: Buijten & Schipperheijn, Amsterdam, The NetherlandsISBN: 978-90-9021715-4

� �� �
Systematic reviews of imaging gynecological
and gastrointestinal malignancies for
developing evidence-based guidelines
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctor
aan de Universiteit van Amsterdam
op gezag van de Rector Magnificus
prof.dr. J.W. Zwemmer
ten overstaan van een door het college voor promoties ingestelde
commissie, in het openbaar te verdedigen in de Aula der Universiteit
op vrijdag 30 maart 2007, te 10:00 uur
door
Shandra Bipat
geboren te Nickerie, Suriname

� �� �
Promotiecommissie
Promotoren: Prof. dr. J.Stoker
Prof. dr. P.M.M. Bossuyt
Co-promotor: Prof. dr. A.H. Zwinderman
Overige leden: Prof. dr. J.S. Laméris
Prof. dr. M.P.M. Burger
Prof. dr. D.J. Gouma
Prof. dr. M.G.M. Hunink
Prof. dr. W.P.Th. M. Mali
Prof. dr. H.C.W. de Vet
Faculteit der Geneeskunde

� �� �
Table of ConTenTs
Chapter 1 General introduction and Outline of the thesis 6
Chapter 2 Is there a role for magnetic resonance imaging in the evaluation of 14
inguinal lymph node metastases in patients with vulva carcinoma?
Chapter 3 Computed tomography and magnetic resonance imaging in staging of 28
uterine cervical carcinoma: a systematic review
Chapter 4 Rectal cancer: local staging and assessment of lymph node involvement 42
with endoluminal US, CT, and MR imaging: a meta-analysis
Chapter 5 Ultrasonography, computed tomography and magnetic resonance imaging 68
for diagnosis and determining resectability of pancreatic adenocarcinoma:
a meta-analysis
Chapter 6 Imaging and treatment of patients with colorectal liver metastases in the 86
Netherlands: a survey
Chapter 7 Colorectal liver metastases: CT, MR imaging, and PET for diagnosis. 98
Meta-analysis
Chapter 8 Evidence-based guideline on management of colorectal liver metastases 120
in the Netherlands
Chapter 9 Multivariate random-effects approach: for meta-analysis of cancer staging 142
studies
Summary and Conclusions 166
Samenvatting en Conclusies 176
List of Publications 188
Dankwoord en Curriculum Vitae 192

1C h a p t e r

General introduction and Outline of the thesis

�
Chapter 1
GeneRal InTRoDUCTIon
Radiological modalities are playing a major role in the management of patients with abdominal
and pelvic malignancies. Improvements in radiological techniques during the last fifteen years, such
a launching of spiral computed tomography, magnetic resonance imaging, and contrast agents,
have led to an increasing use of these modalities for accurate diagnosis and staging of pelvic and
abdominal malignancies [1-6]. For several areas in diagnosis and staging of abdominal and pelvic
malignancies, a large body of scientific evidence is available. The findings in all these studies are not
always univocal, which may account for some of the substantial practice variation in the use of these
techniques.
Clinical guidelines are systematically developed statements to support decision-making. They
can reduce variability in practice, improve the process and outcomes of health care, and optimize
resource utilization. For the development of guidelines for diagnosis and staging, the evidence-
based approach has been put forward, which relies on a combination of the best available evidence
with clinical expertise [7-10]. The more recent development of methods for performing systematic
reviews of diagnostic accuracy studies has further increased the ability to synthesize the available
evidence.
All systematic reviews involve a number of key stages that set them apart from the more tradi-
tional narrative reviews: they start from a well defined clinical question, they rely on comprehensive
literature searching to identify all potentially relevant studies, use explicit selection criteria to include
eligible studies, assess the methodological quality of included studies, explore heterogeneity and its
likely sources and, if possible, to synthesize study results, and arrive at valid and precise summary
estimates (meta-analysis) [11-14].
Meta-analysis is a set of statistical techniques to quantitatively summarize the results obtained at a
systematic review [15-17]. The benefits of meta-analysis over individual trials include increased preci-
sion and statistical power and the ability to identify and explore heterogeneity in the results from
individual studies. The results of well-conducted systematic reviews and meta-analysis can provide
guideline developers and decision makers the highest quality of scientific information.
The overall goal of a systematic review is to combine results of previous studies to arrive at sum-
mary estimates for the relevant study question. In radiology, systematic reviews and meta-analyses
are most often used to estimate the summary diagnostic accuracy of an imaging test, such as
ultrasonography, computed tomography or magnetic resonance imaging [18-25].
Another possible aim of a systematic review can be the identification and explanation of inconsis-
tencies in the results of primary studies [26]. Systematic reviews can help practitioners keep abreast
of the medical literature by summarizing large bodies of evidence and helping to explain differences
among studies on the same question. Systematic reviews can also help in identifying gaps in the
evidence and may provide a quantitative basis for new research initiatives [27].
Systematic reviews are usually time consuming and can therefore be expensive. The use of meta-
analyses to synthesize the evidence from randomized controlled trials is growing in popularity and
the methodology has well advanced. In contrast, the statistical methodology for meta-analyses of
diagnostic accuracy studies is still developing but important steps have been made [28-31].

General introduction and outline of the thesis
�
oUTlIne of THe THesIs
Diagnostic accuracy studies express the level of agreement between the results of a test and the
results of the reference standard. For several pelvic and abdominal malignancies, including rectal
cancer, colorectal liver metastases, pancreatic cancer, uterine cervical cancer, a substantial body of
evidence is available. It may therefore be very relevant to summarize and explore this in a systematic
way, and when feasible, to perform a meta-analysis.
For some clinical questions, the evidence is more limited, to the extent that performing systematic
reviews or meta-analysis will not be helpful for developing clinical guidelines. In these cases, appropri-
ate diagnostic studies of sufficient methodological quality can be helpful in providing the evidence to
support decision making.
This thesis summarizes the diagnostic accuracies of several imaging modalities, such as ultraso-
nography (US), computed tomography (CT), magnetic resonance imaging (MRI), and positron emis-
sion tomography with 18-fluorodeoxyglucose (FDG-PET) in the evaluation of rectal cancer, colorectal
liver metastases, pancreatic cancer, uterine cervical cancer and vulva carcinoma either by means of
systematic reviews or by performing an appropriate diagnostic study. In addition, several parts are
used to develop guideline and this is also presented in this thesis.
Chapter 2 of this thesis focuses on the impact of MRI for lymph node detection in patients with
vulva carcinoma. The goal of the study was to retrospectively determine the accuracy of MRI for
lymph node detection in patients with vulva carcinoma by comparing the MRI findings with histo-
pathological findings obtained by sentinel node procedure or surgery.
In chapter 3 we systematically review the available evidence on the diagnostic accuracy of CT
and MRI in staging uterine cervical carcinoma. The aim of this study was to obtain precise and valid
estimates of the diagnostic performance of CT and MRI in the evaluation of parametrial invasion,
bladder and rectum invasion, and lymph node involvement.
Chapter 4 reports results of a meta-analysis comparing endoluminal US (EUS), CT, and MRI in
local staging (T-staging) and assessment of lymph node involvement in patients with rectal cancer.
The aim of this study was to obtain summary estimates of the accuracy of EUS, CT, and MRI for
correct identification of the T-stages and malignant lymph nodes.
In chapter 5 the results of a meta-analysis comparing US, CT, and MRI for the diagnosis and for
determining resectability of pancreatic adenocarcinoma are reported. Our aim was to obtain sum-
mary estimates of the accuracy of conventional CT, helical CT, MRI, and US.
In chapter 6 we summarize the findings of a survey performed on the management of patients
with colorectal liver metastases in the Netherlands. The survey documented the extent of variation
in the diagnosis and treatment strategies. A second aim was to obtain relevant background informa-
tion for developing and implementing evidence-based guidelines.
In chapter 7 the results of a meta-analysis on the diagnostic accuracy of CT, MRI, and FDG-PET for
the detection of colorectal liver metastases are summarized. In the systematic review we collected
studies on the diagnostic accuracy of CT, MRI, and FDG-PET for the detection of colorectal liver
metastases on a per-patient and on a per-lesion basis.

�0
Chapter 1
A large section of the results summarized in this chapter was used to develop a Dutch evidence-
based guideline for diagnosis and treatment of patients with colorectal liver metastases. This evi-
dence-based guideline is summarized in chapter 8.
The clinical care of cancer patients relies not only on the differentiation between disease and
non-disease but also on correct staging, understaging and overstaging by imaging modalities. In the
meta-analytic approaches used in chapters 3, 4, 5, and 7, we needed thresholds to construct 2 x 2
tables for the calculation of sensitivity, specificity or the diagnostic odds ratio. By defining the thresh-
olds, inevitably information was lost. In chapter 9 an alternative approach is presented to deal with
this type of data sets. The aim of this approach is to report results on correct staging, understaging
and overstaging of tumor.
Finally, the results of this thesis are summarized and implications are made.

General introduction and outline of the thesis
��
References
1. Chang JM, Lee JM, Lee MW, et al. Superparamagnetic iron oxide-enhanced liver magnetic resonance im-aging: comparison of 1.5 T and 3.0 T imaging for detection of focal malignant liver lesions. Invest Radiol 2006;41:168-174.
2. Choi HJ, Roh JW, Seo SS, et al. Comparison of the accuracy of magnetic resonance imaging and positron emis-sion tomography/computed tomography in the presurgical detection of lymph node metastases in patients with uterine cervical carcinoma: a prospective study. Cancer 2006;106:914-922.
3. Gearhart SL, Frassica D, Rosen R, Choti M, Schulick R, Wahl R. Improved staging with pretreatment positron emission tomography/computed tomography in low rectal cancer. Ann Surg Oncol 2006;13:397-404.
4. Imbriaco M, Smeraldo D, Liuzzi R, et al. Multislice CT with single-phase technique in patients with suspected pancreatic cancer. Radiol Med (Torino) 2006;111:159-166
5. Karabulut N, Elmas N. Contrast agents used in MR imaging of the liver. Diagn Interv Radiol 2006;12:22-30
6. Tatli S, Mortele KJ, Breen EL, Bleday R, Silverman SG. Local staging of rectal cancer using combined pelvic phased-array and endorectal coil MRI. J Magn Reson Imaging 2006; 23:534-540
7. McArthur J. The systematic review: an essential element of an evidence based approach to nursing. Nurs Prax N Z 1997;12:10-15.
8. Craig JC, Irwig LM, Stockler MR. Evidence-based medicine: useful tools for decision making. Med J Aust 2001;174:248-253.
9. Manser R, Walters EH. What is evidence-based medicine and the role of the systematic review: the revolution coming your way. Monaldi Arch Chest Dis 2001;56:33-38.
10. Hess DR. What is evidence-based medicine and why should I care? Respir Care 2004;49:730-741.
11. Deville WL, Buntinx F, van der Windt DA, et al. Didactic Guidelines for conducting systematic reviews of stud-ies evaluating the accuracy of diagnostic tests. 2001. Knottnerus JA, editor. The evidence Base of diagnosis. London: BMJ Publishing Group.
12. Deville WL, Buntinx F, Bouter LM, et al. Conducting systematic reviews of diagnostic studies: didactic guide-lines. BMC Med Res Methodol 2002;2:9.
13. Khan KS, Dinnes J, Kleijnen J. Systematic reviews to evaluate diagnostic tests. Eur J Obstet Gynecol Reprod Biol 2001;95:6-11.
14. Khan KS. Systematic reviews of diagnostic tests: a guide to methods and application. Best Pract Res Clin Obstet Gynaecol 2005;19:37-46.
15. Acton GJ. Meta-analysis: a tool for evidence-based practice. AACN Clin Issues 2001; 12:539-545.
16. Gallagher EJ. Systematic reviews: a logical methodological extension of evidence- based medicine. Acad Emerg Med 1999;6:1255-1260.
17. Imperiale TF. Meta-analysis: when and how. Hepatology 1999;29:26S-31S.
18. Bipat S, Glas AS, Slors FJ, Zwinderman AH, Bossuyt PM, Stoker J. Rectal cancer: local staging and assess-ment of lymph node involvement with endoluminal US, CT, and MR imaging--a meta-analysis. Radiology 2004;232:773-783.
19. Koelemay MJW, Nederkoorn PJ, Reitsma JB, Majoie CB. Systematic review of computed tomographic angiog-raphy for assessment of carotid artery disease. Stroke 2004;35:2306-2312.
20. Terasawa T, Blackmore CC, Bent S, Kohlwes RJ. Systematic review: computed tomography and ultrasonogra-phy to detect acute appendicitis in adults and adolescents. Ann Intern Med 2004;141:537-546.
21. Visser K, Hunink MG. Peripheral arterial disease: gadolinium-enhanced MR angiography versus color-guided duplex US--a meta-analysis. Radiology 2000;216:67-77.
22. Oei EH, Nikken JJ, Verstijnen AC, Ginai AZ, Myriam Hunink MG. MR imaging of the menisci and cruciate liga-ments: a systematic review. Radiology 2003;226:837-848.
23. Midgette AS, Stukel TA, Littenberg B. A meta-analytic method for summarizing diagnostic test performances: receiver-operating-characteristic-summary point estimates. Med Decis Making 1993;13:253-257.

Chapter 1
�� ��
24. Nelemans PJ, Leiner T, de Vet HC, van Engelshoven JM. Peripheral arterial disease: meta-analysis of the diag-nostic performance of MR angiography. Radiology 2000;217:105-114
25. Fraquelli M, Colli A, Casazza G, et al. Role of US in detection of Crohn disease: meta-analysis. Radiology 2005; 236:95-101.
26. Nelson EA. The value of systematic reviews in research. Prof Nurse 1998;14:24-28
27. Cooper NJ, Jones DR, Sutton AJ. The use of systematic reviews when designing studies. Clin Trials 2005;2:260-264.
28. Gatsonis CA. Random-effects models for diagnostic accuracy data. Acad Radiol 1995; 2 Suppl 1:S14-S21
29. Moses LE, Shapiro D, Littenberg B. Combining independent studies of a diagnostic test into a summary ROC curve: data-analytic approaches and some additional considerations. Stat Med 1993;12:1293-1316.
30. Reitsma JB, Glas AS, Rutjes AW, Scholten RJ, Bossuyt PM, Zwinderman AH. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J Clin Epidemiol 2005;58:982-990.
31. Walter SD. Properties of the summary receiver operating characteristic (SROC) curve for diagnostic test data. Stat Med 2002;21:1237-1256
��

�� ��

2C h a p t e r

Is there a role for magnetic resonance imaging in the evaluation of inguinal lymph node metastases in patients with vulva carcinoma?
Shandra BipatGerwin A. FransenAnje M. SpijkerboerJacobus van der VeldenPatrick M. M. BossuytAeilko H. ZwindermanJaap Stoker
Gynecologic Oncology 2006;103:1001-1006

�6
Chapter 2
absTRaCT
Objective: To study the accuracy of magnetic resonance imaging (MRI) in lymph node detection in
patients with vulva carcinoma.
Methods: Sixty patients with diagnosed vulva carcinoma underwent MRI examination for preop-
erative evaluation of lymph nodes. MR images were read independently and retrospectively by
two radiologists, both unaware of physical examination and surgery findings. The following char-
acteristics of each lymph node with a short-axis diameter of ≥ 8 mm were recorded: size (axial,
sagittal, and coronal); aspect (homogeneous, with fatty center or partial fat); margin (smooth,
lobulated/speculated or indistinct); shape (round, ovoid or elongated). Based on these charac-
teristics, each lymph node was classified as malignant or benign, and subsequently each groin
was classified as malignant or benign. Histopathology obtained at sentinel node procedure or by
inguinofemoral lymphadenectomy was used as reference standard. Per groin sensitivity, specific-
ity, positive and negative predictive values were calculated. Kappa statistics on per groin basis
were calculated to express interobserver agreement.
Results: Onehundred nineteen groins were examined either by sentinel node procedure or surgery,
of which 23 groins were malignant. Sensitivity, specificity, positive, and negative predictive values
were 52%, 85%, 46%, and 87% for observer 1 and 52% 89%, 52% and 89% for observer 2. The
interobserver agreement was 104/119 (kappa 0.62), representing good agreement.
Conclusion: At this stage there is no role for standard MRI in evaluating lymph node involvement
in patients with vulva carcinoma.

Role of MRI in evaluating lymph nodes in patients with vulva carcinoma
�7
InTRoDUCTIon
Cancer of the vulva accounts for 3 to 5% of primary gynecologic malignancies [1, 2]. For
several decades, the standard treatment has been radical vulvectomy with unilateral or bilateral
inguinofemoral lymphadenectomy through separate incisions. Despite modifications of the surgical
treatment, this operation still results in considerable morbidity. Wound breakdown (17%) and/or
infection (39%) of the groin, lymphatic cyst formation (40%), and lymph edema (28%) all can occur
after standard treatment [3]. Moreover, 10 to 25% of patients in early stage disease have node
involvement and thus between 75% and 90% of patients have unnecessary nodal surgery and the
associated morbidity [4].
Over the last decades investigators tried to identify the patients in which they could predict the
status of the lymph nodes in order to plan groin surgery. Unfortunately it has been proven very
difficult to define such groups. One of the main problems is the lack of the clinical assessment of
nodal disease. In a recent study the negative predictive value of groin palpation was found to be only
77% [5].
The sentinel node procedure is a promising technique that has recently emerged with the poten-
tial to identify those patients with groin node metastases. This technique is becoming increasingly
accepted in the management of cutaneous melanoma and breast cancer [6-9]. Several studies have
shown promising results in vulva cancer [10-12] reporting a negative predictive value close to 100%.
A disadvantage of this technique is that the drainage pathway can sometimes be blocked because of
lymph nodes totally replaced by tumor. In these cases metastatic lymph nodes will not be recognized
[13, 14].
Magnetic Resonance Imaging (MRI) is a non-invasive method, being used more often in the
diagnostic work up of gynecologic malignancy to stage both the primary tumor and regional lymph
nodes [15, 16]. The role of imaging in staging the primary vulva tumor is limited, as the manage-
ment primary depends on the size of the primary tumor which can be accurately assessed clinically.
Patients with tumor less than 4 cm in diameter and clinically non-suspicious groin nodes (cN0) will
undergo radical excision of the tumor in combination with sentinel node procedure. Patients with
tumor larger than 4 cm in diameter and with suspected groin nodes will undergo radical excision
and lymphadenectomy. Only malignant lymph nodes will alter the management to perform either
sentinel node procedure or lymphadenectomy.
In two pilot studies, MRI has been evaluated for lymph node detection in patients with vulva
carcinoma. In a study of Sohaib et al [17], evaluating 22 patients, sensitivity and specificity of respec-
tively 50% and 100% were obtained, while in a study of Hawnaur et al [18], evaluating 10 patients,
sensitivity and specificity of 89% and 91% were obtained.
As lymphatic spread remains an important prognostic factor in patients with vulva carcinoma
and no uniform results are described in the literature, concerning the value of MRI in lymph node
detection, we retrospectively analyzed the accuracy of MRI in lymph node detection in 60 patients
with vulva carcinoma. The results of MRI were compared with the pathological results of the sentinel
node or lymphadenectomy specimen. In addition, we evaluated interobserver variability of MRI for
this purpose.

��
Chapter 2
MaTeRIals anD MeTHoDs
PatientsBetween January 2002 and October 2005, 63 patients were referred in the Academic Medical
Center in Amsterdam for MRI examination for the preoperative evaluation of lymph nodes in pa-
tients with diagnosed vulva carcinoma. All patients were diagnosed as having vulva cancer based
on signs and symptoms, including vulvar pain, itching, bleeding and detection of a palpable mass
at physical examination by gynecological oncologists and by histopathology (squamous carcinoma,
melanoma).
Magnetic Resonance Imaging MRI was performed on a 1.5 T unit (Signa Horizon EchoSpeed, General Electric Medical Systems,
Milwaukee, Wisconsin, USA) using a phased array multicoil. All patients had fasted (4 hr) prior to
examination. To reduce bowel peristalsis, 20 mg butyl scopalaminebromide (Buscopan, Boehringer,
Ingelheim, Germany) was administrated intramuscularly. The following sequences were performed:
(a) Coronal three-dimensional T1-weighted gradient sequence (TR/TE: 11.5/4.2 ms) with 2.8 mm
slice thickness, field of view (FOV) of 35 cm and matrix of 192 x 256; (b) Axial and sagittal fast
spin echo 2500/70 ms T2-weighted with 4 mm section thickness, 4 mm slice gap, 30 cm FOV and
512 x 256 matrix; (c) Coronal fast spin echo 600/10 ms T1-weighted with fat saturation and after
administration of Magnevist® (Schering AG, Berlin, Germany), with 4 mm section thickness, 4 mm
slice gap, 30 cm FOV and 256 x 256 matrix; and (d) For the upper abdomen, an axial Half-Fourier
acquisition single shot turbo SE (HASTE) (TR/TE;964/60 ms) with 7.0 mm slice thickness, FOV of 40
cm and matrix of 256 x 160.
Image analysisMR images were read independently and retrospectively by an experienced abdominal radiologist
(10 year experience CT and MRI of the abdomen) and independently by a radiologist (6 year experi-
ence of which five years as resident). Both were unaware of the findings at previous reading, of the
results of the physical examination (except for the presence of a vulva tumor) and the findings from
surgery and histopathology.
MRI examination quality
The following characteristics of MRI examination were recorded: (a) the quality of MRI examination:
classified as good, moderate or poor (non-diagnostic); (b) presence and type (e.g. movement and
peristalsis) of artifacts; and (c) whether all regions (inguinal right, inguinal left, iliacal right, iliacal left)
could be evaluated. In addition, both observers recorded the review times.
Lymph node assessment
Each observer recorded independently the following characteristics of all lymph nodes with a
minimal short-axis diameter of at least 8 mm depicted on MR images: (a) size: in axial, sagittal,
and coronal plane; (b) localization: lymph nodes at the groin were subdivided into two groups:

Role of MRI in evaluating lymph nodes in patients with vulva carcinoma
��
superficial inguinal lymph nodes and femoral lymph nodes. Superficial inguinal lymph nodes are
located in the superficial fascia parallel to the inguinal ligament and along the terminal part of the
greater saphenous vein. Femoral lymph nodes are located along the medial side of the femoral
vessels (figures 1 and 2); (c) aspect: homogeneous lymph node, lymph node with fatty center or
partial fat in nodes; (d) margin: smooth, lobulated/speculated or indistinct as defined by Kim et
al [19]; (e) shape: round (ratio of long/short-axis diameter of 1); ovoid (ratio of long/short-axis
diameter between 1 and 1.5) or elongated (ratio of long/short-axis diameter larger than 1.5);
and (f) diagnosis: an overall expression based on the above mentioned characteristics was used
to classify each lymph node as malignant or benign.
Reference standardHistopathology was used as the reference standard, either obtained at sentinel node procedure or
at operation (inguinofemoral lymphadenectomy). Patients with tumors less than 4 cm in diameter
and clinically non-suspicious groin nodes (cN0) were included in a sentinel node study after giving
consent [20]. The details of the sentinel lymph node procedure are published elsewhere [10, 21-23].
After removal of the first sentinel lymph node, the groin was re-examined for radioactivity and if
radioactivity was detected at a level greater than 10% of the first excised sentinel lymph node, the
dissection was continued in search of additional sentinel lymph nodes. The removed sentinel lymph
nodes were examined by the pathologist at frozen sections.
Patients with a negative sentinel node had no further surgery of groin nodes. All other patients,
including patients with positive frozen sentinel nodes, were treated by a local radical excision and an
ipsilateral (in case of a unilateral tumor) or bilateral inguinofemoral lymph node dissection. Both the
primary tumor and lymphadenectomy specimens were sent to the pathologist separately for routine
histopathologic examination.
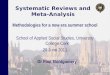
Figure 1. A 78-year old woman with vulva carcinoma and left superficial lymph node metastases.(a) Axial T2-weighted fast spin echo MRI image shows enlarged lymph node with a short-axis of 10 mm node (arrow). (b) Coronal T1-weighted gradient echo image showing the same lymph node (arrow).

�0
Chapter 2
StatisticsQuality assessment
Data on the quality of MRI examination, on the presence of artifacts, and on the evaluation of the
different regions (inguinal right, inguinal left, iliacal right, and iliacal left) were summarized for
each observer. Differences between observers with respect to quality of MRI examinations, pres-
ence of artifacts and non-evaluable regions were analyzed with the McNemar test. Differences in
review times between observers were assessed by Wilcoxon signed ranks test.
Quantity assessment: per groin or per lymph node
Per groin analysis: Each groin was classified as either negative or positive based on MRI data and
separately based on pathology report. Sensitivity, specificity, positive predictive and negative
predictive values per groin were calculated for each observer. For this purpose both superficial
inguinal and femoral lymph nodes were analyzed jointly, due to the low prevalence of malignant
lymph nodes. Kappa statistics on per groin basis to express interobserver agreement were calcu-
lated.
Per lymph node analysis: The number of malignant and benign nodes (superficial inguinal and femo-
ral nodes) depicted on MRI were summarized for each observer. In addition association between the
type of nodes (malignant vs. benign) and characteristics were evaluated by means of Chi-square test
statistic. Short-axis diameters between malignant and benign nodes were compared by independent
Student t-test.
Finally, the number of malignant nodes depicted on histology per groin was also compared
with the number of malignant lymph nodes depicted on MR images in the corresponding groin by
both observers. This was done to obtain an expression of either under or overestimation of MRI.
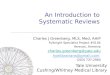
Figure 2. A 76-year old woman with vulva carcinoma and right femoral lymph node metastases. (a) Axial T2-weighted fast spin echo MRI image shows adjacent to femoral vessels a 14 mm (short-axis) lymph node (arrow). (b) Coronal T1-weighted gradient echo image showing the same lymph node (arrow). The lymph node is hypo-intense at T1 indicating that the hyper-intensity on the T2 image does not represent fat.

Role of MRI in evaluating lymph nodes in patients with vulva carcinoma
��
Data were analyzed using SPSS software (Version 9.0 for Windows, SPSS, Inc, Chicago, IL). P
values of less than 0.05 were considered to indicate statistical significance results.
ResUlTs
PatientsThree of the 63 patients, did not undergo either sentinel node procedure or inguinofemoral lymph-
adenectomy and were excluded form the study; one patient due to cardiac problems, one did
undergo vulvectomy only and the third patient was planned for radiation therapy. The demographic
characteristics of patients are listed in table 1. Fifty-seven patients had squamous cell carcinoma and
the other three had melanoma.
Table 1. Demographic characteristics of patients undergoing MRI
Mean age (range) 69 (36-92)
Clinical stage
Squamous cell carcinomas (57)
T1N0M0
T2N0M0
T3N0M0
T1N1Mx
T2N1Mx
T3N1Mx
Melanoma (3)
Breslow II
Breslow III
21
26
3
1
4
2
2
1
Size of tumor (mm) a
≤ 20 mm
20-40 mm
≥ 40 mm
30
18
19
Site of tumor
Median
Unilateral
Bilateral
15
44
8
Final pathological stage
Malignant lymph nodes present
Malignant lymph nodes absent
16
44
x: M-stage unknown. a 7 patients had two lesions

��
Chapter 2
Reference standardA sentinel node procedure was performed in 36 patients. Of the 72 groins examined, 61 showed
radioactivity. A total of 108 sentinel lymph nodes were excised (33 groins with 1 node, 15 with 2, 11
with 3, and 2 groins with 6 nodes) as well as 8 non-sentinel nodes. Frozen section showed metastatic
disease in 7 groins in 4 patients. These patients and the remaining 24 patients, in whom no sentinel
procedure was performed, did undergo either bilateral or unilateral resection of inguinal lymph
nodes (27 bilateral and 1 unilateral resection). A total of 119 groins were examined either by sentinel
node procedure or surgery of which 23 groins (16 patients) were positive and 96 were negative.
MRI findings Quality assessment
The results of the quality assessment for both observers are listed in table 2. Both observers
agreed on the quality of MRI examinations in 53 (88%) patients (52 good, 1 moderate); in the
other 7 MRI examinations discrepancies were found. Artifact were reported in 4 and 10 MRI ex-
aminations by observer 1 and observer 2, respectively (P = 0.031) (table 2). Two (2/240) regions
in 2 patients and 21 regions (21/240) in 11 patients were not evaluable according to observer
1 and observer 2 (P < 0.0001) respectively. Observer 2 scored more regions as non-evaluable,
due to incomplete imaging in 10 patients; however no influence on lymph node evaluation was
recorded.
The review time for observer 1 ranged between 4 and 25 minutes (modus: 7 minutes) and for
observer 2 between 5 and 20 minutes (modus 5 minutes), with significantly lower review times
for observer 2 (P = 0.02).
Table 2. Results of the quality assessment for both observers
Quality of assessment Observer 1 Observer 2
Quality MRI examinations
Poor
Moderate, either
Good
0
1
59
1
7
52
Presence of artifacts
Movements/Peristalsis
Hip prosthesis
Inadequate imaging
1
3
0
5
3
4 a
a 1 patient had also movement/peristalsis artifacts and 1 patient had a hip prosthesis.
Per groin analysis
Of the 23 positive groins, both observers detected 12 (sensitivity 52%). Of the 96 negative groins, 14
and 11 were scored as positive by observers 1 and 2, respectively (specificity of 85% and 89% respec-

Role of MRI in evaluating lymph nodes in patients with vulva carcinoma
��
tively). Positive and negative predictive values for observer 1 were 46% and 87% and for observer 2,
52% and 89%, respectively. Sensitivity, specificity, positive predictive and negative predictive values
for both observers were comparable. The interobserver agreement was 104/119, producing a kappa
of 0.62, and therefore representing good agreement.
Per lymph node analysis
In total 33 and 28 malignant lymph nodes and 100 and 86 benign lymph nodes were identified on
MRI, by observer 1 and 2, respectively. Table 3 presents the MRI characteristics of the malignant
nodes and benign nodes as scored by both observers, independent of the histological findings.
Malignant nodes had larger short-axis compared to benign nodes, according to both observers.
However, only observer 2 showed a significant difference in the short-axes between malignant and
benign nodes, respectively 10.6 and 9.1 mm (P < 0.0001). According to both observers, malignant
nodes were associated with homogenous aspect, while benign nodes were associated with fatty
center or partial fat in the nodes (P < 0.0001). Smooth margin was associated with benign nodes
(P < 0.0001). Finally oval and elongated shapes were associated with benign nodes (P values of
respectively 0.004 and 0.01 for observer 1 and 2).
On histopathology, 38 malignant lymph nodes were found in 23 groins. The number of malignant
lymph nodes depicted on MR images in the corresponding 23 groins is presented in figure 3. Ob-
Table 3. Characteristics of malignant and benign lymph nodes assessed by both observers based on MRI features
MRI characteristics Observer 1 Observer 2
33 malignant 100 benign 28 malignant 86 benign
Short-axis diameter (mm) (mean ± SE)
10.1 ± 0.38 9.8 ± 0.16 10.6 ± 0.36 9.1 ± 0.17
Aspect
Homogeneous 19 1 14 8
Fatty center 1 70 0 46
Partial fat 8 23 10 32
Other 5 0 4 0
Margin
Smooth 4 91 5 66
Lobulated/speculated 25 9 16 20
Indistinct 4 0 7 0
Ratio long to short- axis
Round (ratio 1) 4 3 8 6
Oval (ratio1-1.5) 26 62 11 42
Elongated (ratio > 1.5) 3 35 9 38

��
Chapter 2
server 1 underestimated the number of positive lymph nodes in 14 groins and overestimated the
number of positive lymph nodes in 3 groins, while observer 2 underestimated the number of positive
lymph nodes in 15 groins and overestimated the number of lymph nodes in 1 groin.
In addition, observer 1 falsely identified 17 lymph nodes as malignant in 14 groins and observer
2 falsely identified 13 lymph nodes as malignant in 11 groins.
DIsCUssIon
This is the largest to date study evaluating a large number of groins in patients with vulvar cancer
undergoing MRI for preoperative work-up. On per groin analysis, MRI has low sensitivity and positive
predictive values compared to the reference standard (sentinel node procedure or inguinofemoral
lymph node dissection and subsequent histopathology). Specificity values were 85% and 88% for
observer 1 and observer 2 respectively. Positive predictive values for observer 1 were 88% and 89%
respectively. On per lymph node analysis, the observers either underestimated or overestimated
(false positives) the number of malignant lymph nodes.
Although several associations between nodes characteristics and the type of nodes obtained on
MRI were found. Malignant nodes had larger short-axis compared to benign nodes and were associ-
ated with homogenous aspect, while benign nodes were associated with fatty center or partial fat in
the nodes. However, no recommendation could be made, as the diagnostic value of MRI was limited
(sensitivity and positive predictive value).
A previous study of Sohaib et al, evaluating 22 patients (9 positive groins) and reported similar
results: high specificity values for the identification of superficial inguinal nodes (97%) and deep
inguinal lymph nodes (100%), low sensitivity of 40% and 50%, respectively [17]. In their study
each lymph node was assessed as either benign or malignant, without predefined criteria. A study
of Hawnaur et al [18], evaluating 10 patients reported a sensitivity of 89% (8 positive groins) and
0
1
2
3
4
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Groin
Num
ber o
f mal
igna
nt ly
mph
no
des Reference standard
MRI by observer 1
MRI by observer 2
Malignant lymph nodes
Figure 3. Number of malignant nodes observed by both observers on MRI compared with the number of malignant nodes obtained by histopathology in the positive groins.

Role of MRI in evaluating lymph nodes in patients with vulva carcinoma
��
specificity of 91%. In the latter study the following criteria were considered as malignant: long axis
diameter > 21 mm, short-axis > 10 mm, long/short-axis > 1.5, irregular margin, cystic aspect of lymph
nodes. The prevalence (9/10) of positive lymph nodes in the groins in this study was higher than in a
general patient population with vulvar cancer; in addition 5 of the 10 patients had locally advanced
diseases (Stage III or IV).
The study of Sohaib et al reported a sensitivity of 40% and a specificity of 97% for the de-
tection of malignant superficial inguinal nodes, if short-axis exceeded 10 mm. For detection of
malignant deep inguinal nodes the sensitivity and specificity were 50% and 100% respectively if
short-axis > 8 mm. In our study therefore all lymph nodes with a minimal short-axis of at least 8
mm depicted on MR images were recorded by both observers independently. We attempted to
study superficial inguinal lymph nodes and the femoral lymph nodes separately as performed by
Sohaib et al; yet the low number of malignant lymph nodes limited the accuracy and relevance of
such separate analysis.
Although the sensitivity and prevalence of malignant groins were low, the observers showed
good agreement in assessing lymph nodes (kappa 0.62).
One limitation of this study was the retrospective design, however, all imaging protocols were
comparable and the management (sentinel node or lymphadenectomy) was not based on MRI find-
ings, but on the clinical findings and therefore this retrospective design could not influence clinical
management and thus the reference standard. Another limitation of this study is the lack of a node
by node analysis. However, given the poor results per groin, these results can be expected even to
be inferior to the per groin results.
In the light of high negative predictive values (approaching 100%) of the sentinel node procedure
it is clear that MRI with 85% and 89% negative predictive values does not play a major role in the
decision to perform lymphadenectomy in patients with vulvar cancer. Theoretically, MRI could play
a role in triaging patients for sentinel node procedures; when a positive lymph node is suspected on
MRI and confirmed by fine-needle aspiration (FNA), these patients could be saved from a sentinel
node procedure. However due to the low positive predictive values (approximately 50%), half of the
patients will undergo unnecessary FNA procedures.
Moreover, ultrasonography combined with fine-needle aspiration (FNA) is an alternative imaging
technique to assess inguinal lymph nodes with sensitivity and specificity values up to 93% and 100%
respectively [24, 25]. When a positive lymph node is found with the combination of ultrasound and
FNA this may prevent unnecessary sentinel node procedure in a much cost effective way compared
to MRI.
Recent advantages on lymph node specific MRI contrast agents have shown improvements in the
differentiation between benign and malignant lymph nodes in pelvic cancer. Sensitivity values for the
detection of malignant pelvic lymph nodes are reported up to 100% [26-31]. To our knowledge, no
research has been performed or is being performed on the evaluation of ultrasmall paramagnetic
iron oxide (USPIO) in patients with vulva carcinoma.
At this stage there is no role for routine MRI in evaluating lymph node involvement in patients
with vulva carcinoma. Assessing lymph node involvement remains a major challenge for current im-
aging modalities and needs to be improved as lymphatic spread is an important prognostic factor.

�6
Chapter 2
References
1. Podratz KC, Symmonds RE, Taylor WF, Williams TJ. Carcinoma of the vulva: analysis of treatment and survival. Obstet Gynecol 1983; 61:63-74.
2. Wharton JT, Gallager S, Rutledge FN. Microinvasive carcinoma of the vulva. Am J Obstet Gynecol 1974; 118:159-162.
3. Gaarenstroom KN, Kenter GG, Trimbos JB, et al. Postoperative complications after vulvectomy and inguino-femoral lymphadenectomy using separate groin incisions. Int J Gynecol Cancer 2003; 13:522-527.
4. Cavanagh D, Hoffman MS. Controversies in the management of vulvar carcinoma. Br J Obstet Gynaecol 1996; 103:293-300.
5. Bosquet JG, Kinney WK, Russell AH, Gaffey TA, Magrina JF, Podratz KC. Risk of occult inguinofemoral lymph node metastasis from squamous carcinoma of the vulva. International Journal of Radiation Oncology Biology Physics 2003; 57:419-424.
6. Essner R. The role of lymphoscintigraphy and sentinel node mapping in assessing patient risk in melanoma. Semin Oncol 1997; 24:S8-10.
7. Giuliano AE, Kirgan DM, Guenther JM, Morton DL. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg 1994; 220:391-398.
8. Krag DN, Weaver DL, Alex JC, Fairbank JT. Surgical resection and radiolocalization of the sentinel lymph node in breast cancer using a gamma probe. Surg Oncol 1993; 2:335-339.
9. Nieweg OE, Jansen L, Valdes Olmos RA, et al. Lymphatic mapping and sentinel lymph node biopsy in breast cancer. Eur J Nucl Med 1999; 26:S11-S16.
10. de Hullu JA, Hollema H, Piers DA, et al. Sentinel lymph node procedure is highly accurate in squamous cell carcinoma of the vulva. J Clin Oncol 2000; 18:2811-2816.
11. Decesare SL, Fiorica JV, Roberts WS, et al. A pilot study utilizing intraoperative lymphoscintigraphy for identi-fication of the sentinel lymph nodes in vulvar cancer. Gynecol Oncol 1997; 66:425-428.
12. Levenback C, Coleman RL, Burke TW, Bodurka-Bevers D, Wolf JK, Gershenson DM. Intraoperative lymphatic mapping and sentinel node identification with blue dye in patients with vulvar cancer. Gynecol Oncol 2001; 83:276-281.
13. de Hullu JA, Oonk MH, Ansink AC, Hollema H, Jager PL, van der Zee AG. Pitfalls in the sentinel lymph node procedure in vulvar cancer. Gynecol Oncol 2004; 94:10-15.
14. Fons G, ter RB, Sloof G, de Hullu J, van der Velden J. Failure in the detection of the sentinel lymph node with a combined technique of radioactive tracer and blue dye in a patient with cancer of the vulva and a single positive lymph node. Gynecol Oncol 2004; 92:981-984.
15. Ascher SM, Imaoka I, Hricak H. Diagnostic imaging techniques in gynecologic oncology. In Hoskins WJ, Perez CA, Young RC, eds. Principles of Gynecologic Oncology, Philadelphia: Lippincott Williams & Wilkins, 2000: 629.
16. Togashi K, Nishimura K, Sagoh T, et al. Carcinoma of the cervix: staging with MR imaging. Radiology 1989; 171:245-251.
17. Sohaib SA, Richards PS, Ind T, et al. MR imaging of carcinoma of the vulva. AJR Am J Roentgenol 2002; 178:373-377.
18. Hawnaur JM, Reynolds K, Wilson G, Hillier V, Kitchener HC. Identification of inguinal lymph node metastases from vulval carcinoma by magnetic resonance imaging: an initial report. Clin Radiol 2002; 57:995-1000.
19. Kim JY, Harisinghani MG. MR imaging staging of pelvic lymph nodes. Magn Reson Imaging Clin N Am 2004; 12:581-586.
20. de Hullu JA, Oonk MH, van der Zee AG. Modern management of vulvar cancer. Curr Opin Obstet Gynecol 2004; 16:65-72.
21. de Hullu JA, Doting E, Piers DA, et al. Sentinel lymph node identification with technetium-99m-labeled nanocol-loid in squamous cell cancer of the vulva. J Nucl Med 1998; 39:1381-1385.

Role of MRI in evaluating lymph nodes in patients with vulva carcinoma
�7
22. de Hullu JA, van der Zee AG. Sentinel node techniques in cancer of the vulva. Curr Womens Health Rep 2003; 3:19-26.
23. de Hullu JA, van der Zee AG. Groin surgery and the sentinel lymph node. Best Pract Res Clin Obstet Gynaecol 2003; 17:571-589.
24. Hall TB, Barton DP, Trott PA, et al. The role of ultrasound-guided cytology of groin lymph nodes in the manage-ment of squamous cell carcinoma of the vulva: 5-year experience in 44 patients. Clin Radiol 2003; 58:367-371.
25. Moskovic EC, Shepherd JH, Barton DP, Trott PA, Nasiri N, Thomas JM. The role of high resolution ultrasound with guided cytology of groin lymph nodes in the management of squamous cell carcinoma of the vulva: a pilot study. Br J Obstet Gynaecol 1999; 106:863-867.
26. Bellin MF, Lebleu L, Meric JB. Evaluation of retroperitoneal and pelvic lymph node metastases with MRI and MR lymphangiography. Abdom Imaging 2003; 28:155-163.
27. Harisinghani MG, Saini S, Weissleder R, et al. MR lymphangiography using ultrasmall superparamagnetic iron oxide in patients with primary abdominal and pelvic malignancies: radiographic-pathologic correlation. AJR Am J Roentgenol 1999; 172:1347-1351.
28. Keller TM, Michel SC, Frohlich J, et al. USPIO-enhanced MRI for preoperative staging of gynecological pelvic tumors: preliminary results. Eur Radiol 2004; 14:937-944.
29. Kim JH, Beets GL, Kim MJ, Kessels AG, Beets-Tan RG. High-resolution MR imaging for nodal staging in rectal cancer: are there any criteria in addition to the size? Eur J Radiol 2004; 52:78-83.
30. Koh DM, Brown G, Temple L, et al. Rectal cancer: mesorectal lymph nodes at MR imaging with USPIO versus histopathologic findings--initial observations. Radiology 2004; 231:91-99.
31. Rockall AG, Sohaib SA, Harisinghani MG, et al. Diagnostic performance of nanoparticle-enhanced magnetic resonance imaging in the diagnosis of lymph node metastases in patients with endometrial and cervical cancer. J Clin Oncol 2005; 23:2813-2821.

3C h a p t e r

Computed tomography and magnetic resonance imaging in staging of uterine cervical carcinoma: a systematic review
Shandra BipatAfina S. GlasJacobus van der VeldenAeilko H. ZwindermanPatrick M. M. BossuytJaap Stoker
Gynecologic Oncology 2003;91:59-66.

�0 ��
Chapter 3
�0 ��
absTRaCT
Objective: The goal of this article is to systematically review the available evidence on the diag-
nostic performance of computed tomography (CT) and magnetic resonance imaging (MRI) in
staging of cervical carcinoma.
Methods: A comprehensive computer literature search was performed in MEDLINE and EMBASE
databases from January 1985 to May 2002. Two reviewers independently scored method-
ological quality of included studies and extracted relevant data for data analysis. A bivariate
random-effects approach was used to summarize estimates of sensitivity and specificity values.
Covariates were added to this model to study the influence of sample size, publication year,
methodological criteria, and MRI techniques on summary estimates.
Results: Fifty-seven articles were included. In 49 articles one imaging modality was evaluated
(MRI, 38; CT, 11), and in 8 articles, both. Inclusion criteria were: minimum of 10 patients includ-
ed, histopathology as reference standard, sufficient data presented to construct 2 × 2 tables.
The exclusion criterion was: data reported elsewhere in more detail. Sensitivity estimates for
parametrial invasion were 74% (95% CI: 68%-79%) for MRI and 55% (95% CI: 44%–66%) for
CT and for lymph node involvement 60% (95% CI: 52%-68%), and 43% (95% CI: 37%-57%),
respectively. MRI and CT had comparable specificities for parametrial invasion and lymph node
involvement. For bladder invasion and rectum invasion the sensitivities for MRI were respec-
tively 75% (95% CI: 66%-83%) and 71% (95% CI: 53%-83%), higher compared with CT. The
specificity in evaluating bladder invasion for MRI was significantly higher compared with CT:
91% (95% CI: 83%-95%) for MRI and 73% (95% CI: 52%-87%) for CT. The specificities for
rectum invasion were comparable. Differences in patient sample size, publication year, meth-
odological criteria and MRI techniques had no effect on the summary estimates.
Conclusion: For overall staging of cervical carcinoma, MRI is more accurate than CT.

�0 ��
CT and MRI in staging uterine cervical carcinoma: systematic review
�0 ��
InTRoDUCTIon
Cervical carcinoma is one of the most common cancers in developing countries, accounting for
6% of all malignancies in women (estimated 470,000 cases in 2000) and is associated with a high
mortality (approximately 233,000 worldwide) [1]. Most patients with cervical cancer are detected
through symptoms, such as abnormal vaginal bleeding and vaginal discharge. Investigation of an
abnormal cervical smear followed by histopathology usually establishes the diagnosis.
The Federation Internationale de Gynecologie et d’Obstetrique (FIGO) staging system is used
worldwide for the clinical staging of cervical carcinoma and does not include evaluation of lymph
node involvement. However, the prognosis of patients with cervical cancer depends heavily on
lymph node involvement [2].
The choice to perform surgery (radical hysterectomy with bilateral pelvic lymphadenectomy
for stages IA, IB, and IIA) or (chemo) radiotherapy (intracavitary and external-beam radiotherapy
for stages IIB, III, and IV) depends on both the FIGO stage of the disease and the lymph node
involvement. The clinical staging system relies primarily on findings at physical examination (gyne-
cological examination) and basic imaging techniques such as chest film, intravenous urography,
barium enema, cystoscopy, and sigmoidoscopy. Discrepancies of approximately 25% (in early
stage ≤ IIA) and 65–90% (in advanced stages ≥ IIB) between clinical and surgical staging have
been reported [3-6]. Furthermore little or no information on lymph node involvement is obtained
by clinical examination and basic imaging techniques [7].
In the search for more accurate diagnostic tools, cross-sectional imaging modalities such as
computed tomography (CT) and magnetic resonance imaging (MRI) [8-18] have been proposed.
Despite extensive research efforts on the diagnostic performance of these modalities in staging of
cervical carcinoma, no uniform approach has emerged. The decision to use one of these imaging
modalities should be based on reliable evidence of their diagnostic performance.
The purpose of the study was to summarize the available evidence and to obtain precise and
valid estimates of the diagnostic performance of CT and MRI in the evaluation of parametrial inva-
sion, bladder and rectum invasion, and lymph node involvement. For this purpose, we conducted
a systematic review in which we also studied to what degree differences in techniques and differ-
ences in study design could account for the variability in results on diagnostic accuracy.
MaTeRIals anD MeTHoDs
Data sources A comprehensive computer literature search of English and German language studies in human
subjects was performed to identify articles on the diagnostic performance of CT and MRI in stag-
ing of cervical carcinoma compared with histopathology as reference standard.
The MEDLINE and EMBASE databases from January 1985 to May 2002 were searched for
the following terms: “cervix neoplasms, tomography/X-ray computed/or magnetic resonance

�� ��
Chapter 3
�� ��
imaging/or nuclear magnetic resonance” as medical subject headings (MeSH) and “specificity/or
false negative/or accuracy” as text words [19-23].
The list of articles was supplemented by extensive cross-checking of the reference lists.
Review articles, letters, comments, case reports, and articles not presenting raw data were not
selected.
Study selectionStudies were included when all of the following inclusion criteria were met: (1) minimum sample
size of 10 patients; (2) histopathology of specimens obtained by surgery, laparotomy, postmor-
tem, biopsy, or fine-needle aspiration as reference standard: (3) sufficient data to construct a 2
× 2 contingency table in which the findings from the imaging technique can be compared with
those from the reference standard (cells labeled as true positives, false positives, true negatives,
and false negatives). The exclusion criterion was data reported elsewhere in more detail (dupli-
cate publication).
Data extractionTwo observers independently performed data extraction using a standard form. Discrepancies in
judgment were solved by the independent judgment of a third reviewer. For each study sensitivity
and specificity were calculated from the 2 × 2 tables for detection of parametrial invasion, blad-
der invasion, rectal invasion, and lymph node involvement. We also recorded whether data were
analyzed per patient or per site analysis (e.g. per parametrium for parametrial invasion and per
site/node for lymph node metastases).
In addition, the following items were extracted: (a) year of publication; (b) CT technique: type
of scanner (conventional, spiral/helical CT), use of contrast (oral, rectal, intravenous), and slice
thickness; (c) MRI technique: magnetic field, type of coil (body, phased array, surface, endorec-
tal coil), type of sequences, and use of intravenous contrast medium (gadolinium); and (d) total
sample size.
The following methodological design criteria were scored for all included studies [23-26]: (a)
patient selection (consecutive or non-consecutive); (b) interpretation of results (blinded or not
blinded); (c) method of verification (partial verification or complete); (d) method of data collec-
tion (prospective, retrospective and unknown); and (e) description of study population, diagnostic
test(s), and reference test (sufficient or insufficient).
The reference test (histopathology of specimens obtained by surgery, laparotomy, post-
mortem, biopsy, or fine-needle aspiration) and the diagnostic test, CT and/or MRI, had to be
described with sufficient detail to allow for replication, validation, and generalization of the study.
Descriptions of these tests were scored as sufficient if clear definitions of positive and negative
test results were mentioned in the text. Description of the study population was judged to be suf-
ficient if at least the following characteristics were described: age of participants and distribution
of symptoms (FIGO classification).

�� ��
CT and MRI in staging uterine cervical carcinoma: systematic review
�� ��
Data analysisBecause of the anticipated heterogeneity of sensitivity and specificity between studies we used a
bivariate random-effects approach to analyze the data [27, 28]. We assumed a bivariate normal
distribution for the logit-transformed sensitivity and specificity values, taking into account both
the estimation error of the sensitivity and specificity values in each study as well as heterogeneity
between studies due to differences in patient population and study design.
Using this model we obtained estimates of the mean logit-transformed sensitivity and specific-
ity values across studies. Summary estimates of sensitivity and specificity with confidence intervals
were calculated after antilogarithm transformation of these logit estimates.
Covariate adjustmentTo determine whether results were significantly affected by heterogeneity between individual
studies, the influence of the following covariates was analyzed: sample size (> 50 vs. ≤ 50)
and publication period (1985–1991 vs. 1992–1997 vs. 1998–2002). We also evaluated whether
shortcomings in methodology (patient selection, unblinded interpretation of test results, verifica-
tion bias, and retrospective collection of data), had an effect on diagnostic accuracy.
For this purpose we adjusted for these criteria by adding covariates simultaneously to the
bivariate approach.
Subgroup analysisSubgroup analysis compared MRI techniques: (a) T2-weighted with Gd-enhanced T1-weighted
sequences; (b) Body coil with body and additional coil (e.g., surface, endorectal coil, or phased
array coil); and (c) Low to medium magnetic field strength (< 1.5 T) with high field magnetic field
strength (≥ 1.5 T).
Subgroup analysis was not possible for different MRI sequences (e.g., fast spin echo, gradient
echo, turbo spin echo) and technical CT factors (e.g. scan thickness, use of contrast, and type of
scanner) due to the diversity, and small number of data.
The z test was used to test for differences between subgroups. A P value of 0.05 or less was
considered statistically significant. Calculations and analysis were performed with Microsoft Excel
2000 (Microsoft, Seattle, WA, USA), SPSS 10.0 for Windows (SSPS, Chicago, IL, USA) and the SAS
statistical software version 8.02 (SAS Institute Inc., NC, USA).
ResUlTs
Literature search and study selectionWith the computer search and extensive cross-checking of the reference lists, 111 articles could
be identified. In this set 87 papers were found to be eligible after reading the abstract. Of the 87
potentially eligible articles, 61 fulfilled all inclusion criteria. Four studies had to be excluded due to
publication in more detail elsewhere, resulting in 57 articles. In 49 articles, one imaging modality

�� ��
Chapter 3
�� ��Figure 1. Result of individual studies plotted in Receiver Operating Characteristics (ROC) spaces
Methodological quality elements Score N*
Patient selection Consecutive 25
Non-consecutive 32
Interpretation of test results Blinded 29
Not blinded 28
Method of verification Complete 43
Partial 14
Description of study population Sufficient 34
Insufficient 23
Description of diagnostic test(s) Sufficient 54
Insufficient 3
Description of reference test Sufficient 25
Insufficient 32Method of data collection Prospective 30
Retrospective 14
Unknown 13* Number of articles
Table 1. Results of the assessment of methodological quality elements

�� ��
CT and MRI in staging uterine cervical carcinoma: systematic review
�� ��
alone was evaluated (MRI: 38, CT: 11), and in 8 articles both imaging modalities were evaluated.
Table 1 lists the results of the methodological quality assessment of these articles. Many
studies suffered from selective patient sampling, suboptimal interpretation of results, incomplete
verification methods, and poor description of study population and of reference test. A list of all
included articles with relevant characteristics is available on request from the authors.
Data analysisFigure 1 shows the distribution of sensitivity and specificity between studies. Sensitivity as well
as specificity in the evaluation of parametrial invasion was heterogeneous for MRI; for CT a small
number of data sets were included. For lymph node involvement, heterogeneity was observed
mainly in the sensitivity values, for both CT and MRI. Only a small number of studies evaluated
invasion into the bladder and rectum.
Results of the bivariate data analysis on the diagnostic values of CT and MRI in the detection
of parametrial, bladder and rectum invasion, and lymph node involvement are summarized in
figure 2.
The results of the bivariate approach show a significantly higher sensitivity in the evaluation of
parametrial invasion by MRI compared with CT: 74% (95% CI: 68%–79%) for MRI and 55% (95%
CI: 44%–66%) for CT (P = 0.0027). The sensitivity for lymph node involvement by MRI was also
found to be significantly higher compared with CT: 60% (95% CI: 52%–68%) for MRI and 43%
(95% CI: 37%–57%) for CT (P = 0.047). The specificities in the evaluation of parametrial invasion
and lymph node involvement for MRI and CT were comparable.
Figure 2. Sensitivity and specificity estimates (with confidence intervals) of CT and MRI for staging of cervix carcinoma. n = number of data sets included. *Significant difference when compared with CT (sensitivity esti-mates), P < 0.05. **Significant difference when compared with CT (specificity estimates).

�6 �7
Chapter 3
�6 �7
Figure 4. Results of the bivariate approach with covariates for evaluation of lymph node involvement by MRI. Summary sensitivity and specificity values are represented with confidence intervals.
Figure 3. Results of the bivariate approach with covariates for evaluation of parametrial invasion by MRI. Summary sensitivity and specificity values are represented with confidence intervals.

�6 �7
CT and MRI in staging uterine cervical carcinoma: systematic review
�6 �7
The sensitivity for bladder invasion and rectum invasion by MRI were higher compared with CT:
respectively 75% (95% CI: 66%–83%) and 71% (95% CI: 53%–83%) for MRI compared with
64% (95% CI: 39%–82%) and 45% (95% CI: 20%–73%) for CT. These differences were not sta-
tistically significant. The specificity in the evaluation of bladder invasion for MRI was significantly
higher compared with CT: 91% (95% CI: 83%–95%) for MRI and 73% (95% CI: 52%–87%) for
CT (P = 0.0324). The specificities for rectum invasion were comparable.
Covariate adjustmentCovariate adjustment (size of patient population and year of publication) and subgroup analysis
(for MRI techniques) was possible only in the MRI data sets obtained for parametrial invasion
and lymph node involvement. Population size (>50 vs. ≤ 50) and publication period (1985–1991
vs. 1992–1997 vs. 1998–2002) had no influence on both the sensitivity and specificity estimates
(Figure 3 and Figure 4).
Shortcomings in methodology (patient selection, unblinded interpretation of test results, verifi-
cation bias, and retrospective collection of data) also had no effect on diagnostic accuracy.
Subgroup analysisNo differences were observed in subgroups comparing MRI techniques; T2-weighted vs. Gd-
enhanced T1-weighted sequences, body coil vs. body and additional coil, and low to medium
magnetic field strength (< 1.5 T) vs. high field magnetic field strength (≥ 1.5 T) (Figure 3 and
Figure 4).
DIsCUssIon
The aim of this systematic review was twofold: (1) to summarize the available evidence and to
obtain valid and precise summary estimates of the diagnostic performance of CT and MRI for
staging of cervical carcinoma, and (2) to explore potential sources of heterogeneity in findings
between studies.
In this analysis of 17 years of published literature we found many studies, with MRI being the
most extensively evaluated procedure. We found a significantly higher sensitivity for the evalua-
tion of parametrial invasion and lymph node involvement by MRI compared with CT. Sensitivity
for MRI in the evaluation of bladder invasion and rectum invasion was also higher compared with
values for CT, but these differences were not statistically significant. The specificity estimates in
the evaluation of parametrial invasion, lymph node involvement, and rectum invasion for MRI and
CT were comparable. The specificity estimate for bladder invasion by MRI was significantly higher
than that by CT. For the staging of cervical carcinoma, the clinical (FIGO) staging is used world-
wide and proposed to be the official staging method. The inherent limitations of this staging
system concerning invasion outside the cervix and presence of lymph node metastases are espe-
cially prominent in advanced disease (higher prevalence).

�� ��
Chapter 3
�� ��
Because of these limitations of the clinical staging system, we studied the two currently used cross-
sectional imaging modalities, CT and MRI, in evaluating all factors influencing treatment modality
and prognosis: parametrial, bladder and rectum invasion, and lymph node involvement.
Additionally, we scored methodological quality features to test whether shortcomings in meth-
odology affected diagnostic accuracy. Most studies suffered from methodological weaknesses
(see table 1) such as insufficient description of the reference standard, non-consecutive patient
selection, unblinded interpretation of data, verification bias, and retrospective collection of data,
which can cause over- and underestimation of diagnostic accuracies [25]. Arrive et al. [24], using
another scale for the assessment of methodological criteria in radiological studies, also showed
the methodological weaknesses of most radiological studies. These results imply that only a small
minority of the available data can be used in clinical practice, as shortcomings in study design
characteristics can affect the diagnostic accuracy [25, 29-31]. We feel that investigators in the
field of radiology should be aware of optimal designs of their studies and readers should be aware
of weaknesses in design when interpreting the results.
Furthermore, we made an attempt to minimize some of the well-known limitations of meta-
analysis. If primary studies suffer from inadequate scientific quality, combining them in an analytic
approach will yield poor results. We attempted to minimize this problem by (1) applying inclusion
criteria, (2) combining results in a bivariate random-effects approach, which accounts for varia-
tion in results, and (3) using covariate adjustment to explore heterogeneity based on study design
characteristics.
This bivariate random-effects approach [27, 28] is more convenient than the model described
by Moses and colleagues [32, 33], which focuses on the summary receiver operating characteris-
tic (SROC) curve. The bivariate approach produces summary estimates of sensitivity and specificity
as outcomes, which are more familiar to clinicians. Summary estimates of sensitivity and specific-
ity can also be estimated from the SROC curve but this is not clear-cut, since many different pairs
of sensitivity and specificity can be chosen along the SROC curve. One other advantage of this
bivariate random is that both the error of estimation of the sensitivity and specificity values in
each study and the heterogeneity between studies due to different population or threshold set-
tings are taken into account. With this model it is also possible to evaluate the effects of study
characteristics on sensitivity and specificity separately.
One meta-analysis [34] evaluated CT and MRI in the detection of lymph node involvement. In
that study, CT and MRI were found to be comparable in the detection of lymph node metastases
from cervical carcinoma. However, the analysis addressed only a subset of methodological quality
criteria and did not include more recent studies with current technology and data were combined
in a SROC. Moreover, the analysis evaluated only lymph node involvement, whereas the present
analysis focused on the overall staging (FIGO and lymph node involvement).
What are the shortcomings of our systematic review? By including only published data, we
cannot exclude publication bias, which tends to cause overestimation of diagnostic performance
because of the greater likelihood of publication of positive rather than negative results [35].
Another limitation of this study is that we were not able to categorize patients for subgroup
analysis, due to variations in the staging obtained by pathology.

�� ��
CT and MRI in staging uterine cervical carcinoma: systematic review
�� ��
Despite our attempt to explore the heterogeneity, a considerable variation in accuracy between
the included studies remained unexplained. It cannot be excluded that other factors such as dif-
ferences in CT and MRI equipment, institutions, or patient population (spectrum of disease) have
a systematic impact on the diagnostic accuracy.
CT and MRI are limited as it is impossible to differentiate metastatic nodes from non-meta-
static hyperplastic nodes of similar size and shape; the only CT and MRI criteria that are generally
accepted in the evaluation of pelvic node metastases are the size and shape of the node. In the
past decade, a 1-cm diameter has become the preferred criterion, as either the maximum or
minimum transverse diameter. By using this criterion, the reported sensitivity values for CT and
MRI were low, whereas the specificity values were high.
On the basis of our meta-analysis of imaging findings, the following clinical practice guidelines
can be formulated for staging cervical carcinoma. In clinically early-stage cancer, the prevalence
of spread of disease outside the cervix is low and therefore the additional value of MRI is limited.
In more advanced disease, MRI can play an important role as clinical staging has significant limita-
tions in advanced disease. Costs of CT and MRI are difficult to evaluate.
Preoperative MRI has been shown to be cost minimizing, as using MRI as initial imaging exami-
nation requires fewer tests and fewer procedures compared with the standard workup including
CT [36]. However, more MRI studies satisfying all methodological criteria are needed to fully
evaluate MRI techniques and protocols, and to obtain a uniform MRI strategy.

�0 ��
Chapter 3
�0 ��
References
1. World Health Organisation Globoscan 2000, Cancer incidence, mortality and prevalence worldwide, Version 1.0. IARC Cancer Base No. 5. , IARC Press, Lyon (2001).
2. Tanaka Y, Sawada S and Murata T. Relationship between lymph node metastases and prognosis in patients irradiated postoperatively for carcinoma of the uterine cervix. Acta Radiol Oncol 1994;23:455–459.
3. Subak LL, Hricak H, Powell CB, Azizi L, Stern JL. Cervical carcinoma: computed tomography and magnetic resonance imaging for preoperative staging. Obstet Gynecol 1995;86: 43–50.
4. Averette HE, Ford, JH Jr, Dudan RC, Girtanner RE, Hoskins WJ, Lutz MH. Staging of cervical cancer. Clin Obstet Gynecol 1975;18:215–232.
5. Lagasse LD, Creasman WT, Shingleton HM, Ford JH, Blessing JA. Results and complications of operative staging in cervical cancer: experience of the Gynecologic Oncology Group. Gynecol Oncol 1980;9:90–98.
6. Van NJ Jr, Roddick JW, Lowin DM. The staging of cervical cancer: inevitable discrepancies between clinical staging and pathologic findings. Am J Obstet Gynecol 1971;110: 973–978.
7. Lanza A, Re A, D’Addato F, Morino M, Wierdis T, Caldarola B, Ferraris G. Lymph nodal metastases and the clinical stage of cervix carcinoma. Eur J Gynaecol Oncol 1987;8: 61–67.
8. Bandy LC, Clarke-Pearson DL, Silverman PM, Creasman WT. Computed tomography in evaluation of extra-pelvic lymphadenopathy in carcinoma of the cervix. Obstet Gynecol 1985;65:73–76.
9. Angel C, Beecham JB, Rubens DJ, Thornbury JR, Stoler MH. Magnetic resonance imaging and pathologic correlation in stage IB cervix cancers. Gynecol Oncol 1987;27: 357–367.
10. Botsis D, Gregoriou O, Kalovidouris A, Tsarouchis K, Zourlas PA. The value of computed tomography in staging cervical carcinoma. Int J Gynaecol Obstet 1988;27:213–218.
11. Abe Y, Yamashita Y, Namimoto T, Takahashi M, Katabuchi H, Tanaka N, Okamura H. Carcinoma of the uterine cervix: high-resolution turbo spin-echo MR imaging with contrast-enhanced dynamic scanning and T2-weighting. Acta Radiol 1998;39:322–326.
12. deSouza NM, Whittle M, Williams AD, et al. Magnetic resonance imaging of the primary site in stage I cervical carcinoma: a comparison of endovaginal coil with external phased array coil techniques at 0.5T. J Magn Reson Imaging 2000;12:1020–1026.
13. Fujiwara K, Yoden E, Asakawa T, et al. Role of magnetic resonance imaging (MRI) in early cervical cancer. Gan To Kagaku Ryoho 2000;27 suppl 2:576–581.
14. Oellinger JJ, Blohmer JU, Michniewicz K, et al. Pre-operative staging of cervical cancer: comparison of magnetic resonance imaging (MRI) and computed tomography (CT) with histologic results. Zentralbl Gynakol 2000;122:82–91.
15. Sheu MH, Chang CY, Wang JH, Yen MS. Cervical carcinoma: assessment of parametrial invasion and lymph node metastasis with magnetic resonance imaging. Chung Hua I Hsueh Tsa Chih (Taipei) 2000;63:634–640.
16. Yang WT, Lam WW, Yu MY, Cheung TH, Metreweli C. Comparison of dynamic helical CT and dynamic MR imaging in the evaluation of pelvic lymph nodes in cervical carcinoma. AJR Am J Roentgenol 2000;175:759–766.
17. Ascher SM, Takahama J, Jha RC. Staging of gynecologic malignancies. Top Magn Reson Imaging 2001;12:105–129.
18. Pannu HK, Corl FM, Fishman EK. CT evaluation of cervical cancer: spectrum of disease. Radiographics 2001;21:1155–1168.
19. Deville WL, Bezemer PD, Bouter LM. Publications on diagnostic test evaluation in family medicine journals: an optimal search strategy. J Clin Epidemiol 2000;53:65–69.

�0 ��
CT and MRI in staging uterine cervical carcinoma: systematic review
�0 ��
20. Deville WL, Buntinx F, van der Windt DA, et al. Didactic guidelines for conducting systematic reviews of studies evaluating the accuracy of diagnistic tests. In: J.A. Knottnerus, Editor, The evidence base of diag-nosis, BMJ Publishing Group, London (2001).
21. Deeks JJ. Systematic reviews in health care: systematic reviews of evaluations of diagnostic and screening tests. BMJ 2001;323:157–162.
22. Assendelft WJ, van Tulder MW, Scholten RJ, Bouter LM. [The practice of systematic reviews. II. Searching and selection of studies]. De praktijk van systematische reviews. II. Zoeken en selecteren van literatuur. Ned Tijdschr Geneeskd 1999;143: 656–661.
23. van der Windt DA, Zeegers MP, Kemper HC, Assendelft WJ, Scholten RJ. [Practice of systematic reviews. VI. Searching, selection and methodological evaluation of etiological research]. De praktijk van systema-tische reviews. VI. Zoeken, selecteren en methodologisch beoordelen van etiologisch onderzoek. Ned Tijdschr Geneeskd 2000;144:1210–1214.
24. Arrive L, Renard R, Carrat F, et al. A scale of methodological quality for clinical studies of radiologic exami-nations. Radiology 2000;217:69–74.
25. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999;282:1061–1066.
26. Assendelft WJ, Scholten RJ, van Eijk JT, Bouter LM. [The practice of systematic reviews. III. Evaluation of methodological quality of research studies] De praktijk van systematische reviews. III. Methodologische beoordeling van onderzoeken. Ned Tijdschr Geneeskd 1999;143:714–719.
27. Van Houwelingen HC, Zwinderman KH,. Stijnen T. A bivariate approach to meta-analysis. Stat Med 1993;12:2273–2284.
28. Van Houwelingen HC, Arends LR, Stijnen T. Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med 2002;21:589–624.
29. Khan KS, Daya S, Jadad A. The importance of quality of primary studies in producing unbiased systematic reviews. Arch Intern Med 1996;156:661–666.
30. Panzer RJ, Suchman AL, Griner PF. Workup bias in prediction research. Med Decis Making 1987;7:115–119.
31. Ransohoff DF and Feinstein AR. Problems of spectrum and bias in evaluating the efficacy of diagnostic tests. N Engl J Med 1978;299:926–930.
32. Littenberg B and Moses LE. Estimating diagnostic accuracy from multiple conflicting reports: a new meta-analytic method. Med Decis Making 1993;13:313–321.
33. Moses LE, Shapiro D, Littenberg B. Combining independent studies of a diagnostic test into a summa-ry ROC curve: data-analytic approaches and some additional considerations. Stat Med 1993;12:1293–1316.
34. Scheidler J, Hricak H, Yu KK, Subak L, Segal MR. Radiological evaluation of lymph node metastases in patients with cervical cancer: a meta-analysis. JAMA 1997;278:1096–1101.
35. Irwig L, Macaskill P, Glasziou P, Fahey M. Meta-analytic methods for diagnostic test accuracy. J Clin Epide-miol 1995;48:119–130.
36. Hricak H, Powell CB, Yu KK, Washington E, Subak LL, Stern JL et al. Invasive cervical carcinoma: role of MR imaging in pretreatment workup: cost minimization and diagnostic efficacy analysis. Radiology 1996;198: 403–409.

4C h a p t e r

Rectal cancer: local staging and assessment of lymph node involvement with endoluminal US, CT and MR imaging: a meta-analysis
Shandra BipatAfina S. GlasFrederik J. M. SlorsAeilko H, ZwindermanPatrick M. M. BossuytJaap Stoker
Radiology 2004:232:773-783

��
Chapter 4
absTRaCT
Purpose: To perform a meta-analysis to compare endoluminal ultrasonography (EUS), computed
tomography (CT), and magnetic resonance imaging (MRI) in rectal cancer staging.
Methods: Relevant articles published between 1985 and 2002 were included if more than 20
patients were studied, histopathologic findings were the reference standard, and data were
presented for 2 x 2 tables; articles were excluded if data were reported elsewhere in more de-
tail. Two reviewers independently extracted data on study characteristics and results. Bivariate
random-effects approach was used to obtain summary estimates of sensitivity and specificity
for invasion of muscularis propria, perirectal tissue, and adjacent organs, and for lymph node
involvement. Summary receiver operating characteristic (ROC) curves were fitted for perirectal
tissue invasion and lymph node involvement.
Results: Ninety articles fulfilled all inclusion criteria. For muscularis propria invasion, EUS and
MRI had similar sensitivities; specificity of EUS (86% [95% CI: 80%-90%]) was significantly
higher than that of MRI (69% [95% CI: 52%-82%]) (P = 0.02). For perirectal tissue invasion,
sensitivity of EUS (90% [95% CI: 88%-92%]) was significantly higher than that of CT (79%
[95% CI: 74%-84%]) (P < 0.001) and MRI (82% [95% CI: 74%-87%]) (P= 0.003); specificities
were comparable. For adjacent organ invasion and lymph node involvement, estimates for
EUS, CT, and MRI were comparable. Summary ROC curve for EUS of perirectal tissue invasion
showed better diagnostic accuracy than that of CT and MRI. Summary ROC curves for lymph
node involvement showed no differences in accuracy.
Conclusion: For local invasion, EUS was most accurate and can be helpful in screening patients
for available therapeutic strategies.

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
��
InTRoDUCTIon
Rectal cancer is a common cancer and a major cause of mortality in Western countries. The diag-
nosis is usually established by means of clinical examination (rectal digital examination), endoscopy
(sigmoidoscopy and colonoscopy), double-contrast enema examination, and histologic confirma-
tion, supplemented by biochemistry (e.g. blood carcinoembryonic antigen measurement). All of
these techniques are poor indicators of the depth of invasion and lymph node involvement, which
are both important features for prognosis [1-5].
Accurate preoperative assessment of these prognostic factors is an important first step in
assigning patients to one of the available treatment strategies, which include transanal local
excision, transanal endoscopic microsurgery, total mesorectal excision, preoperative irradiation,
and preoperative chemotherapy. From the clinical point of view, it is important to select patients
for local therapy, such as transanal local excision or transanal endoscopic microsurgery (mainly
stage T1 or lower) [6-9]; total mesorectal excision (mainly stages T2 and T3); and a long course of
preoperative (chemotherapeutic) radiation therapy, aimed at downsizing and downstaging the
tumor(s) (mainly stage T4) [10-12].
In patients considered suitable for total mesorectal excision, the spread of tumor to the me-
sorectal fascia is the second important feature that needs to be assessed [13-15]. This relation
determines if a patient can be treated directly with or without a short course of preoperative
radiation therapy or whether the patient should be considered to have a locally advanced tumor
necessitating a long course of chemotherapeutic radiation therapy. This is an important next step
in the selection of patients for the proper treatment strategy. The identification and the role of
mesorectal fascia are still under investigation, however; therefore, the assessment of the depth
of cancer invasion (T stage) remains the primary and most important feature in the treatment
of patients with rectal cancer. The presence of lymph node involvement is relevant for clinical
decision making in two circumstances: (1) if local excision in the absence of lymphadenopathy
is performed and (2) if lymph node metastases are present outside the endopelvic envelope, in
which case the tumor is considered to be locally advanced.
Non-invasive radiologic modalities such as endoluminal ultrasonography (EUS), computed to-
mography (CT), and magnetic resonance imaging (MRI) have proved to be important and have
been widely used diagnostic tools in the assessment of depth of cancer invasion and/or lymph
node involvement. Extensive research on the diagnostic performance of these modalities in the
staging of rectal cancer has been performed [16-20], yet studies on the evaluation of all three
imaging modalities within the same patient population are limited.
Furthermore, a wide variation in study design, patient population, imaging techniques, and
results exists. These factors make it difficult for workers in this field to know the diagnostic per-
formance of these imaging modalities.
A meta-analysis of diagnostic tests represents a powerful tool to summarize findings in the
literature by taking into account and enabling analysis of differences between studies [21, 22].
Thus, the purpose of our study was to perform a meta-analysis to compare EUS, CT, and MRI in
the staging of rectal cancer.

�6
Chapter 4
MaTeRIals anD MeTHoDs
Literature SearchA comprehensive computerized systematic literature search [23] was performed (S.B.) to identify
abstracts of English-language articles from studies involving human subjects. Relevant studies on
the diagnostic performance of EUS, CT, and MRI in the staging of rectal cancer were identified.
The MEDLINE database from January 1985 to December 2002 was searched with the follow-
ing keywords: (a) “rectal neoplasms” (medical subject heading, or MeSH) and (b) “magnetic reso-
nance imaging” (MeSH) or “tomography, x-ray computed” (MeSH) or “ultrasonography” (MeSH)
and (c) “specificity” or “false negative” or “accuracy” as text words.
The EMBASE, Cochrane, and CANCERLIT databases were also checked for relevant articles by
using (a) “rectal cancer” and (b) “magnetic resonance imaging” or “computed tomography” or
“ultrasonography” and (c) “specificity” or “false negative” or “accuracy” as text words. To identify
additional relevant references, the reference lists of the articles retrieved were checked manually.
After reading the abstracts, one reviewer (S.B.) examined all potentially eligible articles in
which EUS, CT, and/or MRI were evaluated. Reviews, letters, comments, case reports, and articles
that did not present raw data were excluded.
Study SelectionStudies were selected if they fulfilled all of the following inclusion criteria: (1) more than 20
patients had histologically proved rectal adenocarcinoma or carcinoma and were not treated with
preoperative chemotherapy and/or radiation therapy; (2) histopathologic findings (specimens
obtained at surgery, laparoscopy, laparotomy, lymph node biopsy) were used as the reference
standard; (3) sufficient data were presented to construct a 2 x 2 contingency table (either raw 2 x
2 data or sensitivity and/or specificity with absolute numbers of positive and negative findings or
the standard errors) of the imaging modalities compared with the reference standard for invasion
of the submucosa, muscularis propria, perirectal tissue, or adjacent organs or lymph node involve-
ment (perirectal or distant lymph nodes).
Studies were excluded if data were reported elsewhere in more detail. When data were pub-
lished more than once, the study with the most details or the most patients was included.
Data ExtractionTwo reviewers (S.B., F.J.M.S.) independently extracted relevant data from each article, including
study characteristics and test results, by using a standardized data extraction form. The reviewers
were not blinded to authors, journal name, or year of publication. Both reviewers extracted data
from all articles. In cases of discrepancies, a third blinded reviewer assessed all discrepant items,
and majority opinion was used for analysis.
Study CharacteristicsThe following study design characteristics were scored: (a) patient selection: consecutive or non-
consecutive; (b) interpretation of test results: blinded or not blinded; (c) verification: complete or

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
�7
partial—in cases in which more than 10% of the study group was not subjected to the reference
test, the study was scored as applying partial verification; all other cases were scored as complete
verification; (d) methods of data collection: prospective, retrospective, or unknown—data collec-
tion was categorized as either prospective or retrospective; in case of doubt, the method of data
collection was scored as unknown; (e) reporting of study population: sufficient or insufficient—a
description of the study population was judged to be sufficient if at least the age of participants
and male-to-female ratio were included; (f) reporting of diagnostic test(s): sufficient or insuf-
ficient; and (g) reporting of reference test: sufficient or insufficient.
In a study of diagnostic accuracy, both the reference test and the diagnostic test(s) should be
described with sufficient detail to allow for replication, validation, and generalization of the study.
Descriptions of the tests were scored as sufficient if clear definitions of positive and negative test
results were mentioned in the text.
Additionally, the following study characteristics were recorded for each article: (a) year of
publication; (b) sample size (number of patients); and (c) mean age of patients.
Examination ResultsThe following imaging techniques were recorded in the assessment of retrieved articles: for EUS,
type of probe and frequency of transducer; for CT, type of contrast material (oral, rectal, or
intravenous), section thickness, and use of spiral mode; and for MRI, magnetic field strength,
sequence, intravenous contrast material (used or not used), and type of coil used (body coil with
or without additional coil [e.g. phased-array or endorectal coil]).
For local staging, 2 x 2 tables were extracted or reconstructed from reported sensitivity and
specificity values and absolute numbers of positive and negative findings as follows:
(a) For invasion of muscularis propria, stage T2 or higher versus stage T1.
(b) For invasion of perirectal tissue, stage T3 or higher versus stage T2 or lower.
(c) For invasion of adjacent organs, stage T4 versus stage T3 or lower.
For invasion of the submucosa, no 2 x 2 tables could be extracted or reconstructed because of
the limited data on negative results (T0 and Tis). We extracted or reconstructed 2 x 2 tables for
lymph node involvement (perirectal, iliac, or mesenteric lymph nodes). Cut-off values for positive
lymph nodes were also extracted.
To avoid selection of data sets, in articles in which investigators tabulated the results for dif-
ferent readers (interobserver), for multiple observations per reader (intraobserver), for multiple
MRI systems, and for multiple MRI sequences, all tabulated results (2 x 2 tables) were considered
separate data sets.
Statistical AnalysisA bivariate random-effects model [24, 25] was used to obtain summary estimates of sensitivity
and specificity and to fit summary receiver operating characteristic (ROC) curves that correspond-
ed to the observed ranges of sensitivity and specificity values.

��
Chapter 4
Bivariate Random-Effects AnalysisIn this model, we assumed that the true values of sensitivity and specificity followed a bivariate
normal distribution around some common mean value of logit-transformed sensitivity (logit-sens)
and logit-transformed specificity (logit-spec) with a variance matrix Σ (σA and σB describe the vari-
ance among studies in logit-sens and logit-spec, respectively, and σAB is the covariance between
logit-sens and logit-spec).
Covariance
Logit-sens and logit-spec were calculated as follows: logit-sens = ln[sens/(1 – sens)] and logit-spec
= ln[spec/(1 – spec)], where ln is the natural logarithm, sens is sensitivity, and spec is specificity.
Because of this transformation of sensitivity and specificity into logit-sens and logit-spec, these
values will be approximately normally distributed with squared standard error 1/[nx(1 – x)], where
n is the number of cases or control subjects and x is sensitivity or specificity.
The random-effects model produces estimates of the mean logit-sens and logit-spec with their
standard errors. Sensitivity and specificity estimates with their 95% confidence intervals (CIs) were
calculated after anti–logit transformation of the mean logit-sens and logit-spec. The random-ef-
fects model also produces the associated variances (σA and σB) and the covariance (σAB).
To display summary ROC curves, we estimated the intercept (α) and slope (β) of the linear
regression line: logit-sens = α + (β*logit-spec) [26]. The slope (β) of this regression line equals the
covariance between logit-sens and logit-spec (σAB) divided by the variance of logit-spec (σB): β =
σAB / σB.
After calculation of the slope, the intercept (α) was calculated by solving the regression equa-
tion between the mean values of logit-sens and logit-spec. After anti–logit transformation of the
regression line, a summary ROC curve was obtained.
Bivariate Analysis with CovariatesTo determine whether results were significantly affected by heterogeneity between individual
studies, the following covariates were added to the bivariate random-effects model for modality:
year of publication (continuous variable: 2000 was set to 0, 1999 to –1, 1998 to –2, 1997 to
–3, etc), sample size (> 50 vs. ≤ 50 patients), interpretation of results (blinded vs. not blinded),
verification (complete vs. partial), patient selection (consecutive vs. non-consecutive), and method
of data collection (prospective vs. retrospective or unknown). Year 2000 was chosen as the refer-
ence year because of the low number of publications after 2000.
We considered variables to be explanatory if their regression coefficients were statistically
significant (P < 0.05). Subsequently, we performed bivariate regression analysis with multiple
covariates for each stage per modality. In this analysis, previously identified explanatory variables
were analyzed with a backward elimination procedure, where the variable with the highest P-
value was excluded first. Variables were considered statistically significant if P < 0.1.

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
��
Summary ROC CurvesFor each modality, a model was obtained that was adjusted for significant variables that were set
to 1, indicating the ideal design versus 0, as appropriate. The intercept and slope were estimated
for the regression line (logit-sens = α + [β*logit-spec]), and a summary ROC curve was fitted after
anti-logit transformation of this regression line.
The position of the summary ROC curve indicates the difference in diagnostic performance
among the imaging modalities. A summary ROC curve located near the upper left corner indicates
the better diagnostic modality.
Summary Estimates of Sensitivity and SpecificityTo compare the estimates for EUS, CT, and MRI, a final model was obtained that was adjusted for
variables that significantly affected the estimates of the imaging modalities (set to 1, indicating
the ideal design vs. 0), as appropriate.
Since tabulated results for different readers (interobserver), for multiple observations per read-
er (intraobserver), for multiple MRI systems, and for multiple MRI sequences were considered
to be separate data sets, correlations were taken into account. For this approach, the empirical
standard error calculated by means of the “sandwich estimator” was used, which is possible with
the SAS software (version 8.02; SAS Institute, Cary, NC) procedure mixed [27]. This approach
was also used for intramodality intrapatient correlation (in some studies, different modalities were
compared in the same patient population).
Studying the histograms of the residuals and the random-effects estimates confirmed the
goodness of fit of the model. To evaluate the difference between estimates for EUS, CT, and
MRI, we included in our model a factor that indicated type of diagnostic modality; a P value of
less than 0.05 of the regression coefficient of this factor was considered to indicate a significant
difference.
Subgroup AnalysisOnly the groups of studies on MRI and EUS contained sufficient numbers to allow subgroup
analysis of technical differences, although the numbers did not allow an analysis of the effects
of covariates. We compared the following MRI techniques: (a) use of body coil versus surface
and/or phased-array and/or endorectal coil; (b) unenhanced MRI (T1- and T2-weighted imaging)
versus gadolinium-enhanced T1-weighted MRI; and (c) magnetic field strength used (< 1.5 T vs.
≥ 1.5 T). In a subgroup analysis of the EUS techniques, low-frequency probes (< 7.5 MHz) versus
high-frequency probes (≥ 7.5 Mhz) were compared.
All analyses were performed by using Microsoft Excel 2000 (Microsoft, Seattle, Wash), SPSS
10.0 for Windows (SSPS, Chicago, Ill), and SAS statistical software (SAS Institute).

�0
Chapter 4
ResUlTs
Search Results and Study SelectionAfter the computerized search was performed and reference lists were extensively cross-checked,
357 articles were identified. We found 146 articles to be potentially eligible after reading the
abstract, of which 90 fulfilled the criteria for inclusion. Reasons for not including studies were
the following: less than 20 patients studied (n = 31); lack of reference standard (histopathologic
findings obtained at surgery, laparotomy, laparoscopy, or lymph node biopsy) (n = 1); incomplete
or inconclusive data to allow calculation of true-positive, false-positive, true-negative, and false-
negative findings (n = 19); and data reported elsewhere in more detail (n = 5).
Table 1. Study and patient characteristics of included data sets for each cancer stage
Stage No of Data Sets
No of Patients/Prevalence (%)
Years of Publication
References
T2-stage
EUS 39 2881/ 73.1% 1985-2002 16, 17, 20, 28-57
CT 2 65/96.9% 1986,1994 31, 41
MRI 13 630/83.5% 1993-2002 16, 17, 20, 45, 58-65
T3-stage
EUS 61 3904/52.7% 1985-2002 16, 17, 20, 28-41, 44-57, 66-89
CT 18 994/61.1% 1985-2002 18, 19, 31, 42, 66, 67, 72, 74, 75 78, 84, 89-94
MRI 17 746/58.2% 1993-2002 16, 17, 20, 45, 58-65, 82, 83, 95, 96
T4-stage
EUS 37 2686/7.4% 1985-2002 17, 20, 28-41, 44, 47-53, 56, 57, 68, 69, 73, 75, 81, 83, 87, 97
CT 9 397/6.6% 1985-2002 18, 19, 31, 39, 75, 83, 98
MRI 11 537/8.4% 1993-2002 17, 20, 40, 58, 60-65
N-stage
EUS 55 3879/39.9% 1986-2002 16, 33, 35-38, 40, 42, 44-48, 51, 52, 53, 55, 67-69, 71, 72, 74, 76-79, 81, 82, 84-88, 97, 99-107
CT 18 1123/40.8% 1985-2002 18, 19, 67, 72, 74, 78, 83, 84, 89-91, 93, 94, 100, 106, 108
MRI 19 1003/32.5% 1986-2002 16, 20, 45, 58-60, 64, 65, 82, 83, 95, 96, 106, 108-110

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
��
Data ExtractionFrom the 90 articles included, 299 data sets were retrieved. Most data sets suffered from selec-
tive patient sampling (64%), suboptimal interpretation of results (77%), and poor description of
the reference standard (73%). The other study design characteristics were distributed as follows:
complete verification of results (90%), sufficient description of patient populations (66%), suf-
ficient description of diagnostic tests (89%), and prospective collection of data (50%). For each
cancer stage and imaging modality, included data sets with corresponding numbers of patients,
years of publication, and references are presented in table 1.
A full list of all included articles with all relevant study characteristics and complete examination
results (for each stage and imaging modality) is available from the authors upon request.
Table 2. Predictors identified by means of backward regression analysis for each stage
Variable Regression coefficient P value
Muscularis propria invasion by EUS (39 data sets) Year of publication* Size of patient population (> 50)‡
0.08 (0.004, 0.15)†
1.16 (0.46, 1.85)0.040.001
Perirectal tissue invasion by EUS (61 data sets) Patient selection (consecutive)‡ -0.43 (-0.84, -0.01) 0.04
Perirectal tissue invasion by CT (18 data sets) Year of publication‡ -0.07 (-0.11, -0.04)† < 0.001
Perirectal tissue invasion by MRI (17 data sets) Method of data collection (prospective)‡ 0.92 (0.006, 1.85) 0.05
Adjacent organs invasion by EUS (37 data sets) Year of publication* Size of patient population (> 50)*
Size of patient population (> 50)‡
0.06 (0.02, 0.09)†
0.59 (0.15, 1.03)0.59 (0.08, 1.09)
0.0050.0080.02
Adjacent organs invasion by MRI (11 data sets) Year of publication‡ -0.31(-0.44, -0.17)† < 0.001
Lymph node involvement by EUS (55 data sets) Year of publication‡
Method of data collection (prospective)‡ 0.04 (0.002, 0.08)†
0.48 (0.06, 0.89)0.060.03
Lymph node involvement by CT (18 data sets) Verification of results (complete)‡ -1.81 (-2.12, -1,51) < 0.001
Lymph node involvement by MRI (19 data sets) Year of publication‡
Interpretation of results (blind)‡0.15 (0.02, 0.28)†
0.80 (0.15, 1.45)0.030.01
Note.—Numbers in parentheses are 95% confidence intervals. A positive regression coefficient indicates better discriminatory power of the imaging modality in studies with that characteristic than in studies without the corresponding characteristics. A negative regression coefficient indicates reduced diagnostic performance in studies with that characteristic. * Effect on sensitivity;† Value is change per year (year 2000 was coded as 0, 1999 as –1, 1998 as –2, 1997 as –3, etc); ‡ Effect on specificity.

��
Chapter 4
Data AnalysisAfter backward stepwise regression analysis was performed, several variables were identified as
significant predictors of the diagnostic performance of EUS, CT, and MRI for evaluation of inva-
sion of the muscularis propria, perirectal tissue, and adjacent organs and lymph node involvement
from rectal cancer (table 2).
Summary ROC CurvesWith the regression models, intercepts and slopes of the summary ROC curves for EUS, CT, and
MRI were calculated. Summary ROC curves could be fitted for data on perirectal tissue invasion
and lymph node involvement. For invasion in the muscularis propria and adjacent organs, no
intercepts and slopes could be defined because of the homogeneity of either the sensitivity or
specificity values.
The summary ROC curves for perirectal tissue invasion have different positions in ROC space
(figure 1); indicating differences in diagnostic performance between the imaging modalities, with
the summary ROC curve for EUS located nearest to the upper left corner. The summary ROC
curves for lymph node involvement have similar positioning in ROC space, indicating no differ-
ences in diagnostic performance of the imaging modalities.
0
0,2
0,4
0,6
0,8
1
0 0,2 0,4 0,6 0,8 1
False positive rate
Tru
e p
osit
ive
rate
EUS results
sROC EUS
CT results
sROC CT
MRI results
sROC MRI0
0,2
0,4
0,6
0,8
1
0 0,2 0,4 0,6 0,8 1
False positive rate
Tru
e p
osit
ive
rate
EUS results
sROC EUS
CT results
sROC CT
MRI results
sROC MRI
Lymph node involvementPerirectal tissue invasion
Figure 1. Summary ROC curves based on the final regression model for evaluation of perirectal tissue inva-sion and lymph node involvement with EUS, CT, and MRI and results of individual data sets. Left: Summary ROC curves for perirectal tissue invasion included consecutive patient selection for EUS, publication year for CT, and prospective data collection for MRI. Right: Summary ROC curves for lymph node involvement included publication year and prospective data collection for EUS, complete verification of results for CT, and publica-tion year and blinded interpretation of results for MRI. Year 2000 was chosen as the reference year. A summary ROC curve located near the upper left corner indicates better diagnostic modality. Curves for perirectal tis-sue invasion indicate differences in diagnostic performance among imaging modalities, with summary ROC curve for EUS located nearest to the upper left corner. Curves for lymph node involvement indicate no differences in diagnostic performance of imaging modalities.

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
��
Summary Estimates of Sensitivity and SpecificityMuscularis propria invasion.
In the final model, publication year and sample size (> 50 patients) were included as covariates
for EUS. Because of the few CT data sets available for evaluation, no data analysis was performed
for this aspect. No significant variables were identified for MRI (table 2). EUS and MRI have similar
sensitivity estimates of 94%. The specificity value for EUS (86%) was significantly higher (P = 0.02)
than that for MRI (69%), indicating overstaging of T1 (or lower) tumors with MRI (table 3).
Perirectal tissue invasion
The final model included consecutive patient selection for EUS, publication year for CT and pro-
spective data collection for MRI as covariates. The sensitivity estimates for EUS, CT, and MRI were
90%, 79%, and 82%, respectively, with a significantly higher sensitivity estimate for EUS than for
CT (P < 0.001) and MRI (P = 0.003), indicating understaging of T3 (or higher) tumors with CT
and MRI. The specificity estimates for EUS, CT, and MRI were comparable: 75%, 78%, and 76%,
respectively (table 3).
Adjacent organ invasion
The model included year of publication and sample size (> 50 patients) for EUS and publication
year for MRI as covariates. No significant predictors were found for the diagnostic performance
of CT. Sensitivity estimates of all imaging modalities were comparable: 70% for EUS, 72% for
CT, and 74% for MRI. Specificity estimates were also comparable: 97% for EUS, 96% for CT, and
96% for MRI (table 3).
Lymph node involvement
Year of publication and prospective data collection for EUS, complete verification for CT, year of
publication, and blind interpretation of results for MRI were included as covariates in the final
model. Sensitivity estimates for EUS, CT, and MRI were comparably low: 67%, 55%, and 66%,
respectively. Specificity values were also comparable: 78% for EUS, 74% for CT, and 76% for MRI
(table 3).
In all models in which publication year was included as the covariate, year 2000 was chosen as the
reference year because in some data sets, only one data set was available for publications after
2000. For invasion of muscularis propria and adjacent organs and for lymph node involvement,
more significant variables were found for EUS than for CT and MRI (table 2). Adjustment of the
models for EUS with more variables and the models for CT and MRI with fewer variables could
lead to overestimation of the EUS estimates and underestimation of the CT and MRI estimates.
To evaluate this, models were also studied in which all variables that significantly affected the
estimates of EUS, CT or MRI were included simultaneously. The results of these models were
comparable to the results of the models in which adjustment per modality was performed. To
avoid repetition, these results are not presented.

��
Chapter 4
Subgroup AnalysisSince there was a sufficient number of data sets for perirectal tissue invasion, subgroup analysis
could be performed for this stage.
The results of the subgroup analysis for MRI techniques (use of a body coil vs. a body coil with
an additional coil, unenhanced MRI vs. gadolinium-enhanced MRI, and low vs. high magnetic field
strength) and EUS techniques (low vs. high frequency) are presented in table 4. Summary ROC
curves are presented in figure 2.
No significant differences were found between the techniques, as shown by the summary
estimates and the summary ROC curves.
Table 3. Summary estimates of sensitivity and specificity for EUS, CT, and MRI in the staging of rectal cancer
Stage Imaging Modality Sensitivity (%) Specificity (%)
Muscularis propria invasion EUS 94 (90-97) 86 (80-90)
CT N.A N.A
MRI 94 (89-97) *69 (52-82)*
Perirectal tissue invasion EUS 90 (88-92) 75 (69-81)
CT *79 (74-84)* 78 (73-83)
MRI *82 (74-87)* 76 (65-84)
Adjacent organs invasion EUS 70 (62-77) 97 (96-98)
CT 72 (64-79) 96 (95-97)
MRI 74 (63-83) 96 (95-97)
Lymph node involvement EUS 67 (60-73) 78 (71-84)
CT 55 (43-67) 74 (67-80)
MRI 66 (54-76) 76 (59-87)
Note.—Numbers in parentheses are 95% confidence intervals. EUS = endoluminal US, NA = not applicable. * Significantly lower than EUS.
Table 4. Subgroup analysis on MRI and EUS techniques for perirectal tissue invasion
Imaging Modality and Technique Sensitivity (%) Specificity (%)
MRI with body coil 83 (70-91) 75 (54-88)
MRI with body and additional coil 79 (68-87) 73 (57-84)
MRI without contrast material 80 (61-91) 76 (52-90)
MRI with contrast material 81 (72-87) 71 (59-81)
MRI at < 1.5 T 86 (70-94) 73 (48-89)
MRI at ≥ 1.5 T 80 (70-87) 74 (60-84)
EUS at < 7.5 MHz 91 (85-94) 79 (76-82)
EUS at ≥ 7.5 MHz 89 (85-92) 79 (71-85)
Note.—Numbers in parentheses are 95% confidence intervals

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
��
MRI coil0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
False positive rate
True
pos
itiv
e ra
te
Body coil results
sROC: body coil
Body + additional coil results
sROC: body + additional coil
MRI contrast0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
False positive rate
True
pos
itiv
e ra
te
Without contrast results
sROC: without contrast
With contrast results
sROC: with contrast
MRI magnetic �eld0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
False positive rate
True
pos
itiv
e ra
te
< 1.5 T results
sROC: < 1.5 T
≥ 1.5 T results
sROC: ≥ 1.5 T
EUS probe frequency0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
False positive rate
True
pos
itiv
e ra
te
< 7.5 Mhz results
sROC: < 7.5 Mhz
≥ 7.5 Mhz results
sROC: ≥ 7.5 Mhz
False positive rate
Figure 2. Summary ROC curves for different subgroups in the evaluation of perirectal tissue invasion and for results of individual data sets.Upper left: Summary ROC curves for MRI performed with body coil alone versus body coil with additional coil. Upper right: Summary ROC curves for unenhanced versus gadolinium-enhanced MRI. Lower left: Summary ROC curves for low magnetic field strength (< 1.5 T) versus high magnetic field strength (≥ 1.5 T). Lower right: Sum-mary ROC curves for EUS: low frequency (< 7.5 MHz) versus high frequency (≥ 7.5 MHz). Summary ROC curve located near the upper left corner indicates the better diagnostic modality. Summary ROC curves for subgroups showed similar positioning in ROC space, indicating no differences between subgroups.

�6
Chapter 4
DIsCUssIon
In this meta-analysis, we obtained summary estimates and summary ROC curves for the diagnostic
accuracy of EUS, CT, and MRI in the staging of patients with rectal cancer. EUS was found to be
the most accurate modality when compared with CT and MRI for evaluation of local invasion of
rectal cancer.
For lymph node involvement, the results were comparable, with low sensitivity values. EUS was
used to evaluate only perirectal or mesorectal lymph nodes, whereas CT and MRI were also used
to evaluate iliac and mesenteric or retroperitoneal lymph nodes. However, these data were not
presented separately. We found no significant differences between MRI and EUS techniques in a
subgroup analysis.
In our meta-analysis of literature from a 16-year period, we attempted to minimize some of
the well-known limitations of meta-analysis by applying (a) data extraction by two reviewers inde-
pendently, since differences in interpretation and extraction of data can lead to biased results; (b)
explicit inclusion criteria, such as use of histopathologic findings as the reference standard—dif-
ferential verification has been shown to lead to overestimation of results [111]; (c) exclusion of
duplicate publications—positive results are more likely to be published more than once and could
lead to overestimation of results; (d) extraction of study characteristics to study the effects on the
diagnostic performance. Lijmer et al [111] showed that bias in study design characteristics led to
either over- or underestimation of diagnostic performance; and (e) combination of results in a
bivariate random-effects approach to account for variation in results.
The outcomes of the bivariate approach are both (a) summary estimates of sensitivity and
specificity, which are more familiar to clinicians, and (b) a covariance matrix to fit summary ROC
curves. The advantage of this regression analysis over regular summary ROC analysis ln [DOR] =
α+ β*S, where DOR is the diagnostic odds ratio and S is sum [112] (Appendix), is that this model
accounts not only for the heterogeneity between studies due to different threshold settings but
also for the error of estimation of the sensitivity and specificity values in each study. This random
model also accounts for the residual heterogeneity that may remain even after adjusting for study
characteristics and imaging techniques [113].
To avoid missing important articles, additional databases such as EMBASE, Cochrane, and
CANCERLIT were checked. In addition, the reference lists of original articles and reviews, retrieved
by means of electronic search in the MEDLINE database, were checked manually to identify rel-
evant articles. To avoid exclusion of relevant articles, the literature search was performed for the
years 1985–2002. The question arises whether techniques used in the earlier period represent
outdated technology with inferior results. We therefore performed a subgroup analysis for differ-
ent techniques. No significant differences could be observed. We performed covariate adjustment
for publication year. The year of publication had different effects (increased or decreased) on the
diagnostic accuracy. This may be explained not only by technical developments and different tech-
niques employed over the years, but also by variation in training and expertise of the investigators.
Until now, the latter has rarely been reported in the literature.

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
�7
An important problem in the performance of meta-analysis is the possibility of publication bias.
However, we attempted to study the aspect of publication bias by evaluating whether the size of
studies affected the diagnostic accuracy. In particular, small studies with optimistic results may be
published more easily than small studies with unfavorable results. Larger studies with optimistic
results may also be published more easily than larger studies with unfavorable results, but this
difference will be smaller. The evaluation of the effect of sample size did not show a better diag-
nostic performance of smaller studies compared with larger studies in all data sets. Funnel plot
analysis was not performed, since the limited number of data points for some data sets could
have decreased the power of detecting publication bias. We also did not quantify the number of
unpublished studies, since authors are reluctant to provide information on unpublished studies.
One other limitation is the consideration of 2 x 2 tables for different readers, for multiple
observations per reader, and for multiple MRI sequences as separate data sets. This has been
performed to avoid selection bias. We are aware of the dependency inherent in data sets from
the same patient population. Studying this dependency is not possible with our software, since
SAS procedure mixed (SAS Institute) is only able to adjust for this potential dependency if the
same amounts of data sets are available in each study. We studied this correlation by using the
empirical standard error calculated by means of the “sandwich estimator,” which is possible in
SAS procedure mixed (SAS Institute) [27]. We also used this approach to adjust for correlations
between imaging modalities applied in the same patient population.
Another possible limitation of this meta-analysis is that a multiple backward stepwise regression
analysis was performed with six covariates, and the final model was adjusted for significant vari-
ables. In our study, more data sets were available for EUS than for CT or MRI. For some stages (mus-
cularis propria invasion, adjacent organ invasion, and lymph node involvement), more significant
predictors were found for EUS; this can be explained by the larger number of data sets for EUS. By
adjusting the CT and MRI models with fewer variables, the accuracy of CT and MRI could be under-
estimated. However, we also obtained models for each stage in which we simultaneously adjusted
for all variables that significantly affected the estimates of three imaging modalities per stage.
These results were comparable with the results of the models in which adjustment per modality was
performed and are therefore not presented in this article. Moreover, because of the few MRI stud-
ies suitable for subgroup analysis, the sensitivity and specificity values had wide 95% CIs that over-
lapped completely or partially, indicating no significant differences between several techniques.
Patient characteristics (disease stage, age, or sex distribution) are also important for diagnostic
accuracy, but variation in data presentation made it impossible to study the effect of these vari-
ables. In general, the time interval between performance of diagnostic tests and the reference
test should be short. A longer period between performance of the diagnostic test and the refer-
ence test will lead to a greater change in the disease status and decrease in the discriminatory
power of the diagnostic test. This implies that the comparison should ideally be performed on the
same day. In most of the studies, this time period was not described or was diverse; therefore,
this variable could not be analyzed. A large interval is not likely, however, given the disease under
consideration.

��
Chapter 4
Finally, positron emission tomography with fluorine 18 fluorodeoxyglucose is another imaging
modality that can add incremental information to the preoperative assessment of patients with
rectal cancer. However, data on this issue were limited [114-116] and were therefore not included
in this meta-analysis.
We are aware of one other systematic review on the diagnostic performance of these imaging
modalities in the staging of rectal cancer. Kwok and colleagues [117] reported summary sensitiv-
ity values of 93%, 78%, and 86% with specificity values of 78%, 63%, and 77%, respectively, for
EUS, CT, and MRI in the determination of wall penetration (stage T3). In the assessment of lymph
node involvement, the sensitivity of EUS, CT, and MRI was found to be 71%, 52%, and 65%
with specificity of 76%, 78%, and 80%, respectively. Kwok et al [117] also found EUS to be the
most accurate modality when compared with MRI and CT in the assessment of wall penetration.
However, when evaluating studies of MRI that included use of an endorectal coil, this technique
was found to be as effective as EUS in the assessment of wall penetration and was the most
effective technique in the assessment of nodal involvement. The conclusion was that MRI with
use of an endorectal coil offers the maximum amount of information by a single modality in the
staging of rectal cancer. The latter is not in concordance with our findings, which is most likely
caused by methodologic differences. Their analysis was based on a descriptive analysis by simply
pooling data without accounting for (a) heterogeneity between studies due to different threshold
settings (between-study variation) and (b) errors of estimation of sensitivity and specificity values
in each study (within-study variation). Moreover, no 95% CIs or P values were reported to reflect
the statistical precision of the observed differences.
Although EUS has proved to be a better imaging modality than CT and MRI in the present
study, it has several limitations: operator dependency; limitation to tumors located 8–10 cm from
the anal verge when a rigid probe is used; and no assessment of stenotic tumors. Selection of pa-
tients may therefore lead to biased results. Because of the lack of detailed information on patient
selection, we could not study whether the selection of patients for EUS was different from that
of CT and MRI; however, the prevalences per cancer stage were comparable (table 1).
Moreover, EUS is not able to depict lymph nodes that are outside the range of the transducer
and cannot discriminate between lymph nodes inside or outside the mesorectal fascia, since the
fascia is not identified at EUS. The latter is also of importance in determining the spread of stage
T3 tumors considered for total mesorectal excision. This may explain the more recent widespread
use of MRI, since these limitations do not apply to MRI with external coils. To improve the sensitiv-
ity values of MRI for lymph node detection, newer techniques, such as use of new lymph node-
specific MRI contrast agents (ultrasmall iron-based particles taken up by the lymphatic system),
may provide a more sensitive MRI method to detect lymph node involvement [118-122].
However, both the use of new lymph node-specific MRI contrast agents and the identification of
the mesorectal fascia are still under investigation.
CT has limitations in differentiating and distinguishing the different layers of the rectal wall,
demonstrating the mesorectal fascia, and depicting tumor invasion in surrounding pelvic struc-
tures. The introduction of multisection CT scanners may improve the diagnostic value of this

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
��
modality, as the assessment of local disease with improved visualization of the mesorectal fascia
can be combined with assessment of liver involvement and lung metastases [123-124].
On the basis of the results of this meta-analysis, EUS seems to be a better diagnostic imaging
test for local staging than are CT and MRI. Because of the limited information on the identification
of the mesorectal fascia with MRI [125-127] and spiral CT, at present, EUS might be helpful in
selecting patients for available therapeutic strategies. The identification of lymph nodes with EUS,
CT, and MRI remains a major point of concern.

60
Chapter 4
References
1. Harrison JC, Dean PJ, el Zeky F, Vander ZR. From Dukes through Jass: pathological prognostic indicators in rectal cancer. Hum Pathol 1994; 25:498-505.
2. Jass JR, Love SB. Prognostic value of direct spread in Dukes’ C cases of rectal cancer. Dis Colon Rectum 1989; 32:477-480.
3. Tang R, Wang JY, Chen JS, et al. Survival impact of lymph node metastasis in TNM stage III carcinoma of the colon and rectum. J Am Coll Surg 1995; 180:705-712.
4. Willett CG, Badizadegan K, Ancukiewicz M, Shellito PC. Prognostic factors in stage T3N0 rectal cancer: do all patients require postoperative pelvic irradiation and chemotherapy? Dis Colon Rectum 1999; 42:167-173.
5. Wolmark N, Fisher B, Wieand HS. The prognostic value of the modifications of the Dukes’ C class of colorectal cancer. Ann Surg 1986; 203:115-122.
6. Akasu T, Kondo H, Moriya Y, et al. Endorectal ultrasonography and treatment of early stage rectal cancer. World J Surg 2000; 24:1061-1068.
7. Blair S, Ellenhorn JD. Transanal excision for low rectal cancers is curative in early-stage disease with favor-able histology. Am Surg 2000; 66:817-820.
8. Gao JD, Shao YF, Bi JJ, Shi SS, Liang J, Hu YH. Local excision carcinoma in early stage. World J Gastroen-terol 2003; 9:871-873.
9. Langer C, Liersch T, Markus P, et al. Transanal endoscopic microsurgery (TEM) for minimally invasive resec-tion of rectal adenomas and “low-risk” carcinomas (uT1, G1–2). Z Gastroenterol 2002; 40:67-72.
10. Chen ET, Mohiuddin M, Brodovsky H, Fishbein G, Marks G. Downstaging of advanced rectal cancer fol-lowing combined preoperative chemotherapy and high dose radiation. Int J Radiat Oncol Biol Phys 1994; 30:169-175.
11. Kaminsky-Forrett MC, Conroy T, Luporsi E, et al. Prognostic implications of downstaging following pre-operative radiation therapy for operable T3–T4 rectal cancer. Int J Radiat Oncol Biol Phys 1998; 42:935-941.
12. Rau B, Wust P, Hohenberger P, et al. Preoperative hyperthermia combined with radiochemo therapy in locally advanced rectal cancer: a phase II clinical trial. Ann Surg 1998; 227:380-389.
13. Hermanek P, Hermanek P, Hohenberger W, Klimpfinger M, Kockerling F, Papadopoulos T. The pathologi-cal assessment of mesorectal excision: implications for further treatment and quality management. Int J Colorectal Dis 2003; 18:335-341.
14. Nagtegaal ID, van Krieken JH. The role of pathologists in the quality control of diagnosis and treatment of rectal cancer: an overview. Eur J Cancer 2002; 38:964-972.
15. Wiggers T, van de Velde CJ. The circumferential margin in rectal cancer: recommendations based on the Dutch Total Mesorectal Excision Study. Eur J Cancer 2002; 38:973-976.
16. Gualdi GF, Casciani E, Guadalaxara A, d’Orta C, Polettini E, Pappalardo G. Local staging of rectal cancer with transrectal ultrasound and endorectal magnetic resonance imaging: comparison with histologic find-ings. Dis Colon Rectum 2000; 43:338-345.
17. Hunerbein M, Pegios W, Rau B, Vogl TJ, Felix R, Schlag PM. Prospective comparison of endorectal ultra-sound, three-dimensional endorectal ultrasound, and endorectal MRI in the preoperative evaluation of rectal tumors: preliminary results. Surg Endosc 2000; 14:1005-1009.
18. Chiesura-Corona M, Muzzio PC, Giust G, Zuliani M, Pucciarelli S, Toppan P. Rectal cancer: CT local staging with histopathologic correlation. Abdom Imaging 2001; 26:134-138.
19. Matsuoka H, Nakamura A, Masaki T, et al. Preoperative staging by multidetector-row computed tomogra-phy in patients with rectal carcinoma. Am J Surg 2002; 184:131-135.
20. Blomqvist L, Machado M, Rubio C, et al. Rectal tumour staging: MR imaging using pelvic phased-array and endorectal coils vs endoscopic ultrasonography. Eur Radiol 2000; 10:653-660.

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
6�
21. Kinkel K, Lu Y, Both M, Warren RS, Thoeni RF. Detection of hepatic metastases from cancers of the gastrointestinal tract by using noninvasive imaging methods (US, CT, MR imaging, PET): a meta-analysis. Radiology 2002; 224:748-756.
22. Oei EH, Nikken JJ, Verstijnen AC, Ginai AZ, Myriam Hunink MG. MR imaging of the menisci and cruciate ligaments: a systematic review. Radiology 2003; 226:837-848.
23. Deville WL, Bezemer PD, Bouter LM. Publications on diagnostic test evaluation in family medicine journals: an optimal search strategy. J Clin Epidemiol 2000; 53:65-69.
24. Van Houwelingen HC, Zwinderman KH, Stijnen T. A bivariate approach to meta-analysis. Stat Med 1993; 12:2273-2284.
25. Van Houwelingen HC, Arends LR, Stijnen T. Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med 2002; 21:589-624.
26. Rao CR. Linear statistical inference and its applications 2nd ed. New York, NY: Wiley, 1973; 417-420.
27. Liang KY, Zeger SL. Regression analysis for correlated data. Annu Rev Public Health 1993;14:43-68.
28. Hildebrandt U, Feifel G. Preoperative staging of rectal cancer by intrarectal ultrasound. Dis Colon Rectum 1985; 28:42-46.
29. Konishi F, Muto T, Takahashi H, Itoh K, Kanazawa K, Morioka Y. Transrectal ultrasonography for the as-sessment of invasion of rectal carcinoma. Dis Colon Rectum 1985; 28:889-894.
30. Beynon J, Foy DM, Roe AM, Temple LN, Mortensen NJ. Endoluminal ultrasound in the assessment of local invasion in rectal cancer. Br J Surg 1986; 73:474-477.
31. Kramann B, Hildebrandt U. Computed tomography versus endosonography in the staging of rectal carci-noma: a comparative study. Int J Colorectal Dis 1986; 1:216-218.
32. Feifel G, Hildebrandt U, Dhom G. Assessment of depth of invasion in rectal cancer by endosonography. Endoscopy 1987; 19:64-67.
33. Glaser F, Schlag P, Herfarth C. Endorectal ultrasonography for the assessment of invasion of rectal tumours and lymph node involvement. Br J Surg 1990; 77:883-887.
34. Orrom WJ, Wong WD, Rothenberger DA, Jensen LL, Goldberg SM. Endorectal ultrasound in the preopera-tive staging of rectal tumors: a learning experience. Dis Colon Rectum 1990; 33:654-659.
35. Napoleon B, Pujol B, Berger F, Valette PJ, Gerard JP, Souquet JC. Accuracy of endosonography in the stag-ing of rectal cancer treated by radiotherapy. Br J Surg 1991; 78:785-788.
36. Boyce GA, Sivak MV, Jr, Lavery IC, et al. Endoscopic ultrasound in the pre-operative staging of rectal carcinoma. Gastrointest Endosc 1992; 38:468-471.
37. Derksen EJ, Cuesta MA, Meijer S. Intraluminal ultrasound of rectal tumours: a prerequisite in decision making. Surg Oncol 1992; 1:193-198.
38. Herzog U, von Flue M, Tondelli P, Schuppisser JP. How accurate is endorectal ultrasound in the preopera-tive staging of rectal cancer? Dis Colon Rectum 1993; 36:127-134.
39. Houvenaeghel G, Delpero JR, Giovannini M, et al. Staging of rectal cancer: a prospective study of digi-tal examination and endosonography before and after preoperative radiotherapy. Acta Chir Belg 1993; 93:164-168.
40. Hulsmans FJ, Tio TL, Fockens P, Bosma A, Tytgat GN. Assessment of tumor infiltration depth in rectal cancer with transrectal sonography: caution is necessary. Radiology 1994; 190:715-720.
41. Kim NK, Choi JS, Sohn SK, Min JS. Transrectal ultrasonography in preoperative staging of rectal cancer. Yonsei Med J 1994; 35:396-403.
42. Rafaelsen SR, Kronborg O, Fenger C. Digital rectal examination and transrectal ultrasonography in staging of rectal cancer: a prospective, blind study. Acta Radiol 1994; 35:300-304.
43. Adams WJ, Wong WD. Endorectal ultrasonic detection of malignancy within rectal villous lesions. Dis Colon Rectum 1995; 38:1093-1096.
44. Fedyaev EB, Volkova EA, Kuznetsova EE. Transrectal and transvaginal ultrasonography in the preoperative staging of rectal carcinoma. Eur J Radiol 1995; 20:35-38.

6�
Chapter 4
45. Starck M, Bohe M, Fork FT, Lindstrom C, Sjoberg S. Endoluminal ultrasound and low-field magnetic reso-nance imaging are superior to clinical examination in the preoperative staging of rectal cancer. Eur J Surg 1995; 161:841-845.
46. Kaneko K, Boku N, Hosokawa K, et al. Diagnostic utility of endoscopic ultrasonography for preoperative rectal cancer staging estimation. Jpn J Clin Oncol 1996; 26:30-35.
47. Nielsen MB, Qvitzau S, Pedersen JF, Christiansen J. Endosonography for preoperative staging of rectal tumours. Acta Radiol 1996; 37:799-803.
48. Akasu T, Sugihara K, Moriya Y, Fujita S. Limitations and pitfalls of transrectal ultrasonography for staging of rectal cancer. Dis Colon Rectum 1997; 40(suppl 10):S10-S15.
49. Hunerbein M, Schlag PM. Three-dimensional endosonography for staging of rectal cancer. Ann Surg 1997; 225:432-438.
50. Maier AG, Barton PP, Neuhold NR, Herbst F, Teleky BK, Lechner GL. Peritumoral tissue reaction at tran-srectal US as a possible cause of overstaging in rectal cancer: histopathologic correlation. Radiology 1997; 203:785-789.
51. Sailer M, Leppert R, Kraemer M, Fuchs KH, Thiede A. The value of endorectal ultrasound in the assessment of adenomas, T1- and T2-carcinomas. Int J Colorectal Dis 1997; 12:214-219.
52. Massari M, De Simone M, Cioffi U, Rosso L, Chiarelli M, Gabrielli F. Value and limits of endorectal ultraso-nography for preoperative staging of rectal carcinoma. Surg Laparosc Endosc 1998; 8:438-444.
53. Akahoshi K, Kondoh A, Nagaie T, et al. Preoperative staging of rectal cancer using a 7.5 MHz front-loading US probe. Gastrointest Endosc 2000; 52:529-534.
54. Carmody BJ, Otchy DP. Learning curve of transrectal ultrasound. Dis Colon Rectum 2000; 43:193-197.
55. Kim JC, Cho YK, Kim SY, Park SK, Lee MG. Comparative study of three-dimensional and conventional endorectal ultrasonography used in rectal cancer staging. Surg Endosc 2002; 16:1280- 1285.
56. Steele SR, Martin MJ, Place RJ. Flexible endorectal ultrasound for predicting pathologic stage of rectal cancers. Am J Surg 2002; 184:126-130.
57. Garcia-Aguilar J, Pollack J, Lee SH, et al. Accuracy of endorectal ultrasonography in preoperative staging of rectal tumors. Dis Colon Rectum 2002; 45:10-15.
58. Okizuka H, Sugimura K, Ishida T. Preoperative local staging of rectal carcinoma with MR imaging and a rectal balloon. J Magn Reson Imaging 1993; 3:329-335.
59. Schnall MD, Furth EE, Rosato EF, Kressel HY. Rectal tumor stage: correlation of endorectal MR imaging and pathologic findings. Radiology 1994; 190:709-714.
60. Okizuka H, Sugimura K, Yoshizako T, Kaji Y, Wada A. Rectal carcinoma: prospective comparison of con-ventional and gadopentetate dimeglumine enhanced fat-suppressed MR imaging. J Magn Reson Imaging 1996; 6:465-471.
61. Pegios W, Vogl J, Mack MG, et al. MRI diagnosis and staging of rectal carcinoma. Abdom Imaging 1996; 21:211-218.
62. Hadfield MB, Nicholson AA, MacDonald AW, et al. Preoperative staging of rectal carcinoma by magnetic resonance imaging with a pelvic phased-array coil. Br J Surg 1997; 84:529-531.
63. Vogl TJ, Pegios W, Mack MG, et al. Accuracy of staging rectal tumors with contrast-enhanced transrectal MR imaging. AJR Am J Roentgenol 1997; 168:1427-1434.
64. Drew PJ, Farouk R, Turnbull LW, Ward SC, Hartley JE, Monson JR. Preoperative magnetic resonance staging of rectal cancer with an endorectal coil and dynamic gadolinium enhancement. Br J Surg 1999; 86:250-254.
65. Kim NK, Kim MJ, Park JK, Park SI, Min JS. Preoperative staging of rectal cancer with MRI: accuracy and clinical usefulness. Ann Surg Oncol 2000; 7:732-737.
66. Beynon J, Mortensen NJ, Foy DM, Channer JL, Virjee J, Goddard P. Pre-operative assessment of local inva-sion in rectal cancer: digital examination, endoluminal sonography or computed tomography? Br J Surg 1986; 73:1015-1017.

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
6�
67. Rifkin MD, Wechsler RJ. A comparison of computed tomography and endorectal ultrasound in staging rectal cancer. Int J Colorectal Dis 1986; 1:219-223.
68. Saitoh N, Okui K, Sarashina H, Suzuki M, Arai T, Nunomura M. Evaluation of echographic diagnosis of rectal cancer using intrarectal ultrasonic examination. Dis Colon Rectum 1986; 29:234-242.
69. Alessi G, Giuliani A, Risi D, Meli C, Schillaci A, Stipa S. Intrarectal ultrasonography in the preoperative stag-ing of rectal cancer. Ital J Surg Sci 1987; 17:239-244.
70. Beynon J, Roe AM, Foy DM, Channer JL, Virjee J, Mortensen NJ. Preoperative staging of local invasion in rectal cancer using endoluminal ultrasound. J R Soc Med 1987; 80:23-24.
71. Di Candio G, Mosca F, Campatelli A, Cei A, Ferrari M, Basolo F. Endosonographic staging of rectal carci-noma. Gastrointest Radiol 1987; 12:289-295.
72. Holdsworth PJ, Johnston D, Chalmers AG, et al. Endoluminal ultrasound and computed tomography in the staging of rectal cancer. Br J Surg 1988; 75:1019-1022.
73. Salo JO, Mecklin JP, Jarvinen H, Lehtonen T. Endo-ultrasonography for preoperative staging of rectal cancer. Ann Chir Gynaecol 1988; 77:57-60.
74. Rifkin MD, Ehrlich SM, Marks G. Staging of rectal carcinoma: prospective comparison of endorectal US and CT. Radiology 1989; 170:319-322.
75. Rotte KH, Kluhs L, Kleinau H, Kriedemann E. Computed tomography and endosonography in the preopera-tive staging of rectal carcinoma. Eur J Radiol 1989; 9:187-190.
76. Dershaw DD, Enker WE, Cohen AM, Sigurdson ER. Transrectal ultrasonography of rectal carcinoma. Can-cer 1990; 66:2336-2340.
77. Jochem RJ, Reading CC, Dozois RR, Carpenter HA, Wolff BG, Charboneau JW. Endorectal ultrasonographic staging of rectal carcinoma. Mayo Clin Proc 1990; 65:1571-1577.
78. Goldman S, Arvidsson H, Norming U, Lagerstedt U, Magnusson I, Frisell J. Transrectal ultrasound and computed tomography in preoperative staging of lower rectal adenocarcinoma. Gastrointest Radiol 1991; 16:259-263.
79. Lindmark G, Elvin A, Pahlman L, Glimelius B. The value of endosonography in preoperative staging of rectal cancer. Int J Colorectal Dis 1992; 7:162-166.
80. Scialpi M, Andreatta R, Agugiaro S, Zottele F, Niccolini M, Dalla PF. Rectal carcinoma: preoperative stag-ing and detection of postoperative local recurrence with transrectal and transvaginal ultrasound. Abdom Imaging 1993; 18:381-389.
81. Nielsen MB, Pedersen JF, Christiansen J. Rectal endosonography in the evaluation of stenotic rectal tumors. Dis Colon Rectum 1993; 36:275-279.
82. Thaler W, Watzka S, Martin F, et al. Preoperative staging of rectal cancer by endoluminal ultrasound vs. magnetic resonance imaging: preliminary results of a prospective, comparative study. Dis Colon Rectum 1994; 37:1189-1193.
83. Barbaro B, Valentini V, Manfredi R. Combined modality staging of high risk rectal cancer. Rays 1995; 20:165-181.
84. Osti MF, Padovan FS, Pirolli C, et al. Comparison between transrectal ultrasonography and computed tomography with rectal inflation of gas in preoperative staging of lower rectal cancer. Eur Radiol 1997; 7:26-30.
85. Heneghan JP, Salem RR, Lange RC, Taylor KJ, Hammers LW. Transrectal sonography in staging rectal carcinoma: the role of gray-scale, color-flow, and Doppler imaging analysis. AJR Am J Roentgenol 1997; 169:1247-1252.
86. Lindmark GE, Kraaz WG, Elvin PA, Glimelius BL. Rectal cancer: evaluation of staging with endosonography. Radiology 1997; 204:533-538.
87. Barbaro B, Schulsinger A, Valentini V, Marano P, Rotman M. The accuracy of transrectal ultrasound in predicting the pathological stage of low-lying rectal cancer after preoperative chemoradiation therapy. Int J Radiat Oncol Biol Phys 1999; 43:1043-1047.

6�
Chapter 4
88. Adams DR, Blatchford GJ, Lin KM, Ternent CA, Thorson AG, Christensen MA. Use of preoperative ultra-sound staging for treatment of rectal cancer. Dis Colon Rectum 1999; 42:159-166.
89. Harewood GC, Wiersema MJ, Nelson H, et al. A prospective, blinded assessment of the impact of preop-erative staging on the management of rectal cancer. Gastroenterology 2002; 123:24-32.
90. Netri G, Coco C, Valentini V, et al. Clinical staging of rectal cancer: results of a prospective continuing study. Ital J Surg Sci 1985; 15:169-174.
91. Thompson WM, Halvorsen RA, Foster WL, Roberts L, Gibbons R. Preoperative and postoperative CT stag-ing of rectosigmoid carcinoma. AJR Am J Roentgenol 1986; 146:703-710.
92. Cellini N, Coco C, Maresca G, et al. Clinical staging of rectal cancer: a study on 126 patients. Rays 1986; 11:69-79.
93. Angelelli G, Macarini L, Lupo L, Caputi-Jambrenghi O, Pannarale O, Memeo V. Rectal carcinoma: CT stag-ing with water as contrast medium. Radiology 1990; 177:511-514.
94. Civelli EM, Gallino G, Mariani L, et al. Double-contrast barium enema and computerised tomography in the pre-operative evaluation of rectal carcinoma: are they still useful diagnostic procedures? Tumori 2000; 86:389-392.
95. Gagliardi G, Bayar S, Smith R, Salem RR. Preoperative staging of rectal cancer using magnetic resonance imaging with external phase-arrayed coils. Arch Surg 2002; 137:447-451.
96. Murano A, Sasaki F, Kido C, et al. Endoscopic MRI using 3D-spoiled GRASS (SPGR) sequence for local staging of rectal carcinoma. J Comput Assist Tomogr 1995; 19:586-591.
97. Scialpi M, Rotondo A, Angelelli G. Water enema transvaginal ultrasound for local staging of stenotic rectal carcinoma. Abdom Imaging 1999; 24:132-136.
98. Lupo L, Angelelli G, Pannarale O, Altomare D, Macarini L, Memeo V. Improved accuracy of computed tomography in local staging of rectal cancer using water enema. Int J Colorectal Dis 1996; 11:60-64.
99. Zainea GG, Lee F, McLeary RD, Siders DB, Thieme ET. Transrectal ultrasonography in the evaluation of rectal and extrarectal disease. Surg Gynecol Obstet 1989; 169:153-156.
100. Beynon J, Mortensen NJ, Foy DM, Channer JL, Rigby H, Virjee J. Preoperative assessment of mesorectal lymph node involvement in rectal cancer. Br J Surg 1989; 76:276-279.
101. Hildebrandt U, Klein T, Feifel G, Schwarz HP, Koch B, Schmitt RM. Endosonography of pararectal lymph nodes: in vitro and in vivo evaluation. Dis Colon Rectum 1990; 33:863-868.
102. Milsom JW, Graffner H. Intrarectal ultrasonography in rectal cancer staging and in the evaluation of pelvic disease: clinical uses of intrarectal ultrasound. Ann Surg 1990; 212:602-606.
103. Konishi F, Ugajin H, Ito K, Kanazawa K. Endorectal ultrasonography with a 7.5 MHz linear array scanner for the assessment of invasion of rectal carcinoma. Int J Colorectal Dis 1990; 5:15-20.
104. Milsom JW, Lavery IC, Stolfi VM, et al. The expanding utility of endoluminal ultrasonography in the man-agement of rectal cancer. Surgery 1992; 112:832- 840.
105. Spinelli P, Schiavo M, Meroni E, et al. Results of EUS in detecting perirectal lymph node metastases of rectal cancer: the pathologist makes the difference. Gastrointest Endosc 1999; 49:754-758.
106. Kim NK, Kim MJ, Yun SH, Sohn SK, Min JS. Comparative study of transrectal ultrasonography, pelvic computerized tomography, and magnetic resonance imaging in preoperative staging of rectal cancer. Dis Colon Rectum 1999; 42:770-775.
107. Tada M, Endo M. Ultrasonographic examination for lateral lymphatic spread and local recurrence of rectal cancer: preoperative detection and evaluation. Dis Colon Rectum 1995; 38:1047-1052.
108. Hodgman CG, MacCarty RL, Wolff BG, et al. Preoperative staging of rectal carcinoma by computed tomog-raphy and 0.15T magnetic resonance imaging. Preliminary report. Dis Colon Rectum 1986; 29:446-450.
109. de Lange EE, Fechner RE, Edge SB, Spaulding CA. Preoperative staging of rectal carcinoma with MR imag-ing: surgical and histopathologic correlation. Radiology 1990; 176:623-628.
110. McNicholas MM, Joyce WP, Dolan J, Gibney RG, MacErlaine DP, Hyland J. Magnetic resonance imaging of rectal carcinoma: a prospective study. Br J Surg 1994; 81:911-914.

staging of rectal cancer with endoluminal Us, CT and MRI: meta-analysis
6�
111. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999; 282:1061-1066.
112. Littenberg B, Moses LE. Estimating diagnostic accuracy from multiple conflicting reports: a new meta-analytic method. Med Decis Making 1993; 13:313-321.
113. Rutter CM, Gatsonis CA. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat Med 2001; 20:2865-2884.
114. Abdel-Nabi H, Doerr RJ, Lamonica DM, et al. Staging of primary colorectal carcinomas with fluorine-18 fluorodeoxyglucose whole-body PET: correlation with histopathologic and CT findings. Radiology 1998; 206:755-760.
115. Falk PM, Gupta NC, Thorson AG, et al. Positron emission tomography for preoperative staging of colorec-tal carcinoma. Dis Colon Rectum 1994; 37:153-156.
116. Gupta NC, Falk PM, Frank AL, Thorson AM, Frick MP, Bowman B. Pre-operative staging of colorectal carcinoma using positron emission tomography. Nebr Med J 1993; 78:30-35.
117. Kwok H, Bissett IP, Hill GL. Preoperative staging of rectal cancer. Int J Colorectal Dis 2000; 15:9-20.
118. Bellin MF, Lebleu L, Meric JB. Evaluation of retroperitoneal and pelvic lymph node metastases with MRI and MR lymphangiography. Abdom Imaging 2003; 28:155-163.
119. Bellin MF, Roy C, Kinkel K, et al. Lymph node metastases: safety and effectiveness of MR imaging with ul-trasmall superparamagnetic iron oxide particles—initial clinical experience. Radiology 1998; 207:799-808.
120. Harisinghani MG, Saini S, Weissleder R, et al. MR lymphangiography using ultrasmall superparamagnetic iron oxide in patients with primary abdominal and pelvic malignancies: radiographic-pathologic correla-tion. AJR Am J Roentgenol 1999; 172:1347-1351.
121. Hudgins PA, Anzai Y, Morris MR, Lucas MA. Ferumoxtran-10, a superparamagnetic iron oxide as a magnet-ic resonance enhancement agent for imaging lymph nodes: a phase 2 dose study. AJNR Am J Neuroradiol 2002; 23:649-656.
122. McCauley TR, Rifkin MD, Ledet CA. Pelvic lymph node visualization with MR imaging using local administra-tion of ultra-small superparamagnetic iron oxide contrast. J Magn Reson Imaging 2002; 15:492-497.
123. Laghi A, Iannaccone R, Trenna S, et al. Multislice spiral CT colonography in the evaluation of colorectal neoplasms. Radiol Med (Torino) 2002; 104:394-403.
124. Vogl TJ, Luboldt W, Herzog C, Hammerstingl R. Contrast-enhanced multislice CT in detection and evalua-tion of abdominal neoplasms. Radiologe 2002; 42:646-654. [German].
125. Beets-Tan RG, Beets GL, Vliegen RF, et al. Accuracy of magnetic resonance imaging in prediction of tumour-free resection margin in rectal cancer surgery. Lancet 2001; 357:497-504.
126. Bissett IP, Fernando CC, Hough DM, et al. Identification of the fascia propria by magnetic resonance imag-ing and its relevance to preoperative assessment of rectal cancer. Dis Colon Rectum 2001; 44:259-265.
127. Brown G, Richards CJ, Newcombe RG, et al. Rectal carcinoma: thin-section MR imaging for staging in 28 patients. Radiology 1999; 211:215-222.

Chapter 4
66 67
aPPenDIX
Littenberg and Moses [112] suggested that D = [logit (TPR) – logit (FPR)] is modulated as a linear
function of S = [logit (TPR) + logit (FPR)], where D is difference, FPR is false-positive rate (1 – speci-
ficity), TPR is true-positive rate (sensitivity), and S is sum.
Thus, they used the linear model D = α + β*S. Suppose, in a 2 x 2 table, n1 is the number of
patients with disease and n2 is the number of patients without disease.
D = [logit (TPR) – logit (FPR)]
= ln [TPR/(1-TPR)] – ln [FPR/(1-FPR)]
= ln (TP/n1)/(FN/ n1) - ln (FP/n2)/(TN/ n2)
= ln (TP/(FN) – ln (FP/TN)
= ln [(TP/(FN)/ (FP/TN)]
= ln [(TP*TN/ (FN*FP)]
= ln (odds ratio)
= ln (DOR)
where DOR is the diagnostic odds ratio, logit x = ln[x/(1 – x)], x is true-positive rate or false-posi-
tive rate, and
S= logit (TPR) + logit (FPR)
66

66 67

5C h a p t e r

Ultrasonography, computed tomography and magnetic resonance imaging for diagnosis and determining resectability of pancreatic adenocarcinoma: a meta-analysis
Shandra BipatSaffire S. K. S. PhoaOtto M. van DeldenPatrick M.M. BossuytDirk J. GoumaJohan S LamérisJaap Stoker
Journal of Computer Assisted Tomography 2005;29:438-445

70
Chapter 5
absTRaCT
Objective: To compare ultrasonography (US), computed tomography (CT), and magnetic reso-
nance imaging (MRI) in the diagnosis and determination of resectability of pancreatic adeno-
carcinoma.
Methods: Articles reporting US, CT, or MRI data of patients with known or suspected pancreatic
adenocarcinoma and at least 20 patients verified with histopathology, surgical findings, or
follow-up were included. A bivariate random-effects approach was used to calculate sensitivity
and specificity for diagnosis and resectability of pancreatic adenocarcinoma.
Results: Sixty-eight articles fulfilled all inclusion criteria. For diagnosis, sensitivities of helical CT,
conventional CT, MRI, and US were 91%, 86%, 84%, and 76% and specificities were 85%,
79%, 82%, and 75% respectively. Sensitivities for MRI and US were significantly lower com-
pared with helical CT (P = 0.04 and P = 0.0001). For determining resectability, sensitivities of
helical CT, conventional CT, MRI, and US were 81%, 82%, 82%, and 83% and specificities
were 82%, 76%, 78%, and 63% respectively. Specificity of US was significantly lower com-
pared with helical CT (P = 0.011).
Conclusion: Helical CT is preferable as an imaging modality for the diagnosis, and determination
of resectability of pancreatic adenocarcinoma.

Us, CT and MRI for diagnosis and staging pancreatic adenocarcinoma
7�
InTRoDUCTIon
The worldwide incidence of pancreatic adenocarcinoma was estimated at 216,000 in the year
2000 [1]. This disease has a poor prognosis, and resection of the tumor is the only chance of cure.
Preoperative staging should select patients with resectable tumors to undergo surgery, improv-
ing their chances of survival, and identify patients with non-resectable tumors, thus preventing
unnecessary laparotomy.
Imaging modalities used in the diagnosis and determination of resectability include ultrasonog-
raphy (US), computed tomography (CT), and magnetic resonance imaging (MRI). In some institu-
tions US is initially performed to identify patients with non-resectable tumors, mainly based on the
presence of liver metastases [2]. Helical CT is often the imaging modality of choice, whereas MRI
has been introduced more recently in the workup of patients with pancreatic adenocarcinoma.
Considerable attention has been paid to the diagnostic accuracy of these modalities, [2-7] yet
studies comparing US, CT, and MRI in the same study group are scarce; this can be attributed to
the associated costs, logistics, and patient burden. A number of narrative reviews on the radio-
logic diagnosis and staging of pancreatic adenocarcinoma have been presented [8, 9].
We performed a meta-analysis on the literature to compare US, CT, and MRI. Through a critical
appraisal of the validity of published studies and a synthesis of their results, we obtained sum-
mary estimates of helical CT, conventional CT, MRI, and US for the diagnosis and determination
of resectability of pancreatic adenocarcinoma. We also explored sources of heterogeneity in the
published research.
MaTeRIals anD MeTHoDs
Literature SearchA comprehensive computer search [10] was performed by one reviewer to retrieve all English
and German papers published between January 1990 and December 2003 that reported on the
diagnostic accuracy of US, CT, or MRI in the diagnosis and evaluation of resectability of pancreatic
adenocarcinoma.
The following databases were used: MEDLINE, EMBASE, Cochrane, and CANCERLIT. The
search terms were pancreatic neoplasms AND [magnetic resonance imaging OR nuclear mag-
netic resonance OR tomography, x-ray computed OR ultrasonography] as MESH headings AND
[specificity OR false negative OR accuracy] as text words.
Reviews articles, letters, comments, case reports, unpublished articles, and articles not pre-
senting raw data were not retrieved. Additional papers were identified by manually checking the
reference lists of review articles and of the original articles retrieved by the computer search.
Study SelectionAll retrieved articles were selected by two independent reviewers using the following inclusion
criteria: (1) data reported on US or CT or MRI; (2) patients included with known or suspected

7�
Chapter 5
pancreatic adenocarcinoma (based on specific clinical symptoms, such as laboratory results or ul-
trasound findings; (3) minimal sample size of 20 patients verified with reference standard; (4) one
or more of the following reference standards-for diagnosis, histopathology obtained by surgery/
autopsy, laparotomy/ultrasound-guided biopsy, or follow-up in patients lacking histology, and for
determining resectability, surgical findings (histopathology/intraoperative findings), autopsy, and
follow-up; and (5) sufficient data presented to construct a 2 × 2 cross-classification of the imaging
technique results and results of the reference standard for the detection of pancreatic carcinoma
and for determining resectability.
When data from the same study group were reported more than once, only the most recent
article or the article reporting a higher level of data was included.
Data ExtractionTwo observers independently extracted data from each article using a standardized form, based
on the STARD criteria [11]. Observers were not blinded with regard to information about the au-
thors, their affiliations, or the journal name, since this has been shown to be unnecessary [12]. To
resolve disagreement between the two reviewers, a third reviewer assessed all discrepant items.
Study Design Characteristics
The following study design characteristics were extracted: (a) patient selection (consecutive or
non-consecutive); (b) interpretation of test results (blinded or not blinded); (c) verification (com-
plete, partial, or unknown; papers in which more than 90% of the subgroup was subjected to the
reference standard were scored as complete verification; papers in which more than 10% of the
study group was not subjected to the reference test [histopathology, follow-up, intraoperative
findings] were scored as partial verification; and all other cases were scored as unknown); (d)
methods of data collection (prospective, retrospective, or unknown in cases of doubt); (e) report-
ing of study population (sufficient or insufficient; sufficient if all of the following characteristics
were described: spectrum of disease [e.g. clinical symptoms], age of patients, and sex distribu-
tion); (f) reporting of reference test (complete, partial, or no description; papers in which the
reference test was described in detail were scored as complete description; papers in which the
reference test was mentioned but not described in detail were scored as partial description; and
all other cases were scored as no description); and (g) reporting of diagnostic tests (sufficient or
insufficient; the diagnostic test should be described with sufficient detail to allow for replication,
validation, and generalization of the study; for US, type of probe and frequency of transducer;
for CT, type of scanning [helical or multiphase helical CT or conventional], slice thickness or col-
limation, and use of contrast; for MRI, magnetic field, type of coil, sequences, slice thickness, and
use of contrast).
Other Study Characteristics
The following characteristics were also recorded: (a) year of publication; (b) number of patients;
(c) patient characteristics such as clinical symptoms, mean age, sex distribution; and (d) depart-
ment of origin (e.g. radiology, gastroenterology, surgery, internal medicine).

Us, CT and MRI for diagnosis and staging pancreatic adenocarcinoma
7�
Examination Characteristics
We extracted data on the frequency of transducers and whether color/power Doppler was per-
formed in US imaging, the type of scanning (helical or multiphase helical CT or conventional), slice
thickness or collimation and amount of contrast for CT imaging, and the magnetic strength, type
of coil, sequences, slice thickness, and type of contrast for MRI.
Vascular invasion of the portal system (portal vein and superior mesenteric vein) is an impor-
tant determinant for non-resectability. As the CT criteria for invasion of the portal system may
differ between centers, we also extracted those from the papers.
Examination Results
The absolute numbers of true positives, false negatives, false positives, and true negatives for the
diagnosis and assessment of resectability of pancreatic carcinoma per modality were extracted
or calculated from the reported values of sensitivity and specificity. To avoid selection bias, all
tabulated results for different readers (interobserver), for multiple observations per readers (intra-
observer), for multiple MRI systems, and for multiple MRI sequences were counted as separate
data sets.
Statistical AnalysisA bivariate random-effects approach [13, 14] was used to analyze the data. In this model, we
used logit-transformed sensitivity (logit-sens) and logit-transformed specificity (logit-spec). Logit-
sens and logit-spec were calculated as follows: logit-sens = ln (sens/[1-sens]) and logit-spec = ln
(spec/[1-spec]), where ln is the natural logarithm.
Due to the transformation, these values were approximately normally distributed, and mean
logit-sens and logit-spec and their standard errors were obtained by means of a bivariate ran-
dom-effects linear regression model using the SAS proc mixed effects approach. Sensitivity and
specificity estimates with their 95% confidence intervals were back-transformed after anti-logit
transformation of the mean logit-sens and logit-spec values.
Summary Estimates of Sensitivity and SpecificityTo compare the estimates for helical CT, conventional CT, MRI, and US, we first determined
whether the logit-sens and logit-spec values depended on year of publication (continuous vari-
able: 2002 was set to 0, 2001 to -1, 2000 to -2, and so forth), sample size (≤ 50 vs. > 50), de-
partment of origin (radiology/nuclear medicine vs. others), and the study design characteristics:
patient selection (consecutive vs. non-consecutive), interpretation of test results (blinded vs. not
blinded), verification (complete verification vs. partial verification and unknown), methods of data
collection (prospective vs. retrospective and unknown), reporting of study population (sufficient
vs. insufficient), reporting of reference test (sufficient vs. insufficient and no description), and
reporting of diagnostic tests (sufficient vs. insufficient).
The year 2002 was chosen as the reference year due to the low number of publications later
than 2002. In this analysis, we considered variables as explanatory if their regression coefficients
were significant (P < 0.05).

7�
Chapter 5
Subsequently, we developed a multivariable regression model where we used a backward step-
wise algorithm to identify only the most important characteristics. Characteristics were retained
in the regression model when their P value was < 0.10.
Afterward, logit-sens and logit-spec values of the imaging techniques helical CT, conventional CT,
MRI, and US were compared with each other in this random-effects regression model, including
all variables that significantly affected the logit-sens and logit-spec values of the imaging modali-
ties as appropriate; in this final model a factor indicating the type of diagnostic modality was
included and a P value of < 0.05 of the regression coefficient of this factor was considered to
indicate a significant difference.
The fit of the final regression model was inspected graphically by studying the histograms of
the residuals and of the random-effects estimates.
CT Criteria for Invasion of Portal Vein SystemLiver metastasis, lymph nodes, vascular invasion, and extrapancreatic invasion of adjacent organs
are the important factors for excluding patients from respectability [15-18]. Invasion of the portal
system (portal vein and superior mesenteric vein) is the major factor, and different criteria exist
for invasion of the portal system.
As helical CT is the imaging modality most frequently used for the workup of patients with
pancreatic carcinoma, enough data sets on resectability were available to study whether using
encasement of more than 180 degrees, occlusion, and thrombosis as CT criteria for invasion of
the portal system showed improvements.
SubgroupsOther CT techniques such as the number of phases (eg, pancreatic phase vs. other multiphase
helical CT), slice thickness or collimation, and the use of contrast agent could not be studied due
to the heterogeneity of the studies. Also US technique (color Doppler) and MRI technical factors
such as magnetic strength, type of coil, sequence, slice thickness, matrix, and field of view could
not be studied due to the low number of data sets.
As tabulated results for different readers (interobserver), for multiple observations per readers
(intra-observer), for multiple MR systems, and for multiple MRI sequences were considered as
separate data sets, the respective correlations were taken into account. For this approach, the
empirical standard error calculated by “sandwich estimator” was used, which is possible in the
SAS proc mixed [19]. This approach was also used for intra-modality intra-patient correlation (in
some studies, different modalities were compared in the same patient population). All analyses
were performed using SPSS 11.5 for Windows (SPSS Inc, Chicago, IL) and SAS statistical software
version 8.2 (SAS institute Inc, Cary, NC).

Us, CT and MRI for diagnosis and staging pancreatic adenocarcinoma
7�
ResUlTs
Search Results and Study SelectionWith the computer search and after extensive cross-checking of reference lists, 342 articles were
identified. We found 193 articles to be potentially eligible after reading the titles and abstracts.
One hundred twenty-five articles had to be excluded because they did not report data on US,
CT or MRI (n = 49); did not include patients with known or suspected pancreatic adenocarcinoma
but patients with chronic pancreatitis, the evaluation of the duct system, or other types of pan-
creatic cancer (n = 4); evaluated fewer than 20 patients (n = 13); compared the results of US,
CT, or MRI with angiography, positron emission tomography (PET), or other imaging findings (n
= 6); did not report sufficient data on positives (true/false) and negatives (true/false) on either
diagnosis or resectability (n = 50); or reported results of overlapping patients in other languages
(n = 3). In total, 68 articles could be included in this meta-analysis [15-18, 20-83].
Data ExtractionStudy Design Characteristics
As presented in table 1, most articles suffered from bias in study design characteristics: for in-
stance, patient selection was non-consecutive in 39 articles (57%); interpretation of test results
was not blinded in 38 (56%); the method of data collection was retrospective or unknown in 35
(51%); and there was insufficient or no description of the reference test in 42 (62%).
Table 1. Study design characteristics of included studies
Study characteristics Score No. articles
Patient selection Consecutive
Non-consecutive
29
39
Interpretation of test results Blinded
Not Blinded
30
38
Verification Complete
Partial
Unknown
51
14
3
Methods of data collection Prospective
Retrospective
Unknown
33
17
18
Reporting of study population Sufficient
Insufficient
52
16
Reporting of reference test Complete
Partial
No description
26
40
2

76
Chapter 5
Other Study Characteristics
In the 68 articles, a total of 7,405 patients were evaluated with a range of median age of 39.0
to 74.0 years. In 53 articles, the male-to-female ratio was presented (3279:2478). Forty studies
were performed by departments of radiology or nuclear medicine and 28 by departments of
gastroenterology, surgery, or internal medicine.
Examination Characteristics
US was evaluated in 17 articles, with sufficient description in 10; frequencies of the transducer
ranged from 2 to 5 MHz and color/power Doppler was used in 4 studies. CT was evaluated in
55 articles, with sufficient description in 37; helical CT was used in 27 articles and slice thickness
or collimation ranged from 3 to 10 mm (depending on phases), and contrast was used in all 37
studies. MRI was evaluated in 15 articles, with sufficient description in 14; 1.5 T was used in 11
studies, 1.0 T in 4 studies, and a phased array coil in 5 studies.
Table 2. Study and patient characteristics of included data sets
Stage Data sets* Patients† Age‡ Imaging§ Department# References
Diagnosis
Helical CT 23 959 55.0-64.0 23 21 15-18, 20-29
Conventional CT 20 1473 39.0-71.0 7 9 30-46
MRI 11 583 55.1-74.0 11 7 23, 25, 31, 44, 45, 47-51
US 14 2909 39.0-64.0 7 4 30, 34-37, 39, 42 46, 52-55
Resectability
Helical CT 32 1823 54.0-66.4 29 29 15, 17, 18, 22, 25-27, 29, 56-69
Conventional CT 12 1467 57.7-67.0 5 5 35, 40, 70-79
MRI 7 516 58.0-74.0 7 4 25, 50, 51, 62, 76, 80, 81
US 6 1233 57.7-64.7 4 2 35, 58, 69, 71, 82, 83
* Number of data sets per imaging modality.† Total number of patients included in the corresponding data sets.‡ Range of the median age in data sets.§ Sufficient description of the imaging modality.# Data sets available from studies performed by radiology or nuclear medicine department.

Us, CT and MRI for diagnosis and staging pancreatic adenocarcinoma
77
Examination Results
From the 68 articles, summary data for diagnosis (23 by helical CT, 20 by conventional CT, 11 by
MRI, and 14 by US) and for resectability (32 by helical CT, 12 by conventional CT, 7 by MRI, and
6 by US) were retrieved. Table 2 presents an overview of the data sets included for diagnosis and
resectability for each imaging modality, with respective numbers of patients, their median age,
and the corresponding references and departments of origin. Figure 1 presents an overview of
sensitivity and 1—specificity values of the data sets included for diagnosis and resectability for
each imaging modality.
A complete list of all included articles with study characteristics and patient characteristics,
examination characteristics (US, CT, and MRI techniques), and examination results (absolute num-
bers of true positives, true negatives, false positives, and false negatives) is available on request
from the authors.
Data AnalysisFollowing the backward stepwise regression analysis, several variables were identified as signifi-
cant predictors of the diagnostic performance of helical CT, conventional CT, MRI, and US (table
3). Due to the low number of data sets for MRI and US in determining resectability, no covariates
were added to the models.
Summary Estimates of Sensitivity and SpecificityDiagnosis
In the final model, sufficient description of patients was included as a covariate for helical CT,
blind interpretation of results for conventional CT, and sufficient description of patient population
0,0
0,2
0,4
0,6
0,8
1,0
0,0 0,2 0,4 0,6 0,8 1,0
1-Speci�city
Sens
itivity
Helical CT
Conventional CT
MRI
US0,0
0,2
0,4
0,6
0,8
1,0
0,0 0,2 0,4 0,6 0,8 1,0
1-Speci�city
Sens
itivity
Helical CTConventional CT
MRIUS
Diagnosis Resectability
Figure 1. Receiver operating characteristics plots presenting sensitivity and 1-specificity values for diagnosis (left) and resectability (right) of helical CT, conventional CT, MRI, and US.

7�
Chapter 5
for MRI and US. The summary sensitivities for helical CT, conventional CT, MRI, and US were 91%,
86%, 84%, and 76% and the specificities were 85%, 79%, 82%, and 75% respectively. The sensi-
tivities for MRI and US were significantly lower than that of helical CT (P = 0.04 and 0.0001).
Resectability
The final model included year of publication (set to 2002), department of origin (radiology/
nuclear medicine), and sufficient description of diagnostic tests for helical CT and size of patient
population (> 50 patients) for conventional CT as covariates.
Sensitivities for helical CT, conventional CT, MRI, and US were 81%, 82%, 82%, and 83% and
specificities were 82%, 76%, 78%, and 63% respectively. Sensitivities were comparable. Specific-
ity for US was significantly lower compared with that for helical CT (P = 0.0011). The results of
the final models adjusted for significant variables are summarized in table 4.
Table 3. Predictors identified for diagnosis and determining resectabilty
Covariates Coefficient (95% CI) P value
Diagnosis helical CT (23 data sets)
Description of patient population* (sufficient)
Description of patient population† (sufficient)
1.06 (0.02, 2.10)
1.45 (0,64, 2.26)
0.046
0.0004
Diagnosis conventional CT (20 data sets)
Interpretation of results* (blind) 0.90 (0.43,1.36) 0.0002
Diagnosis MRI (11 data sets)
Description of patient population* (sufficient) -1.77(-2.83, -0.72) 0.001
Diagnosis US (14 data sets)
Description of patient population* (sufficient)
Description of patient population† (sufficient)
0.78 (0.39, 1.15)
-2.06 (-3.17, -0.95)
< 0.0001
0.0003
Resectability helical CT (32 data sets)
Year of publication (change per year)*
Department of origin* (Radiology/Nuclear Medicine)
Department of origin† (Radiology/Nuclear Medicine)
Description of diagnostic test* (sufficient)
Description of diagnostic test† (sufficient)
0.14 (0.03, 0.25 ‡
-1.16 (-1.61, -0.72)
1.36 (0.95, 1.77)
-1.76 (-2.11, -1.40)
1.18 (0.81, 1.54)
0.014
< 0.0001
< 0.0001
< 0.0001
< 0.0001
Resectability conventional CT (12 data sets)
Size of patient population* (> 50 patient) -2.35 (-4.12, 0.59) 0.009
Numbers in parentheses are 95% confidence intervals. A positive regression coefficient indicates better discriminatory power of the imaging modality in studies with that characteristic compared with that in studies without the corresponding characteristics and a negative regression coefficient indicates reduced diagnostic performance in studies with that characteristic. * effect on sensitivity; † effects on specificity; ‡ Year 2002 was coded as 0, 2001 as –1, 2000 as –2, and so fort.

Us, CT and MRI for diagnosis and staging pancreatic adenocarcinoma
7�
CT Criteria for Invasion of Portal SystemNineteen data sets evaluating 687 patients showed no improvements in sensitivity and specificity
values for predefined CT criteria compared with the overall results of helical CT. The sensitivity es-
timate was 83% (95% CI: 77%-88%) and the specificity estimate was 83% (95% CI: 77%-87%).
DIsCUssIon
In this meta-analysis we obtained summary estimates of helical CT, conventional CT, MRI, and
US for diagnosis and staging (distinguishing resectable for non-resectable tumors) of pancreatic
cancer. For diagnosis, the sensitivities of US and MRI were lower compared with helical CT. For
resectability, US had a significantly lower specificity compared with helical CT, indicating that US
falsely stages non-resectable tumors as resectable tumors, increasing the number of unnecessary
laparotomies.
The results on CT criteria for invasion of the portal system showed no improvement of the diag-
nostic accuracy. However, other factors such as liver metastases and lymph nodes also determine
resectability. Therefore, the impact of the predefined criteria could not be separately studied and
the diagnostic value could be therefore underestimated.
We tried to minimize some of the well-known limitations of meta-analysis by having two
reviewers independently extract data, using explicit inclusion criteria, and extracting study design
characteristics to evaluate their effects on diagnostic performance. Lijmer et al [84] showed that
bias in study design characteristics led either to overestimation or underestimation of the diag-
nostic performance. In our meta-analysis most studies suffered from bias in design characteristics
Table 4. Summary Estimates of Sensitivity and Specificity for US, CT, and MRI
Imaging modality Data sets/Number of patients
Sensitivity(95% CI)
Specificity(95% CI)
Diagnosis
Helical CT
Conventional CT
MRI
US
23/959
20/1473
11/583
14/2909
91% (86%-94%)
86% (81%-89%)
84% (78%-89%)*
76% (69%-82%)*
85% (76%-91%)
79% (60%-90%)
82% (67%-92%)
75% (51%-89%)
Resectability
Helical CT
Conventional CT
MRI
US
32/1823
12/1467
7/516
6/1233
81% (76%-85%)
82% (74%-88%)
82% (69%-91%)
83% (68%-91%)
82% (77%-87%)
76% (61%-86%)
78% (63%-87%)
63% (45%-79%)*
* Significant difference compared to helical CT.

�0
Chapter 5
following the STARD criteria. We therefore studied whether these characteristics had an impact
on the outcome and adjusted where indicated by means of a bivariate random-effects approach.
This bivariate random-effects approach accounts not only for the heterogeneity between studies
due to different threshold settings, as is the case in the regular sROC analysis, but also for both
the error of estimation of the sensitivity and specificity values in each study [85, 86].
We analyzed 2 × 2 tables for different readers, for multiple observations per readers, and for
multiple CT and MRI techniques, as separate data sets. To adjust for the dependency in data sets
from the same patient population, we studied this correlation by using the empirical standard
error calculated by “sandwich estimator.”
An issue in any form of meta-analysis is the possibility of publication bias. We evaluated
whether the size of studies was associated with diagnostic accuracy. In particular, small studies
with optimistic results may be published more easily than small studies with unfavorable results.
Larger studies with optimistic results may also be published more easily than larger studies with
unfavorable studies, but this difference will be smaller. There was no association between sample
size and diagnostic performance.
Patient characteristics (stage of disease, age, or sex distribution) are known to affect diagnos-
tic accuracy. Unfortunately, the variation in data presentation prevented us from studying the
effect of these variables.
The reference standard used in this meta-analysis ranged from histopathology to follow-up. In
general the time interval between diagnostic test and reference test in patients with neoplasms
should be short for comparison; therefore, in patients undergoing follow-up, the results could
be underestimated. This is a major limitation of most diagnostic studies, in which histopathology
could not be performed in all patients due to ethical considerations. However, it was not possible
to study the effect of different reference standards (histopathology, intraoperative findings, or
follow-up) on diagnostic accuracy due to insufficient and not separately reported results from
different reference standards.
Another important factor in the resection of pancreatic cancer is the variation between surgical
resection procedures (eg, whether to perform vein resection). The influence of this factor could
also not be studied due to limited description of surgical procedures; this is another limitation of
most diagnostic studies.
Therefore, the STARD initiative has been developed to improve the quality of the reporting
of diagnostic studies. The items in the checklist and the flowchart can help authors in describing
essential elements of the design and conduct of the study, the execution of tests, and the results
[11].
CT technical factors such as the number of phases (pancreatic phase vs. multiphase helical CT)
and the type of scanner (single-slice vs. multi-slice) are important features; however, either due to
the low number of studies evaluating multislice CT or the heterogeneity of studies, these features
could not be studied. Although helical CT has replaced conventional CT in the staging of pancre-
atic carcinoma, this has not led to improved results. MRI has been studied less extensively in the
workup of pancreatic cancer, and therefore the number of studies was too limited to evaluate
technical factors such as magnetic field strength, type of coil, and slice thickness. US is known as

Us, CT and MRI for diagnosis and staging pancreatic adenocarcinoma
��
an operator-dependent modality, but the experience level of the sonographer is not described in
the included papers, and moreover the definition of operator experience is a subjective param-
eter. Techniques such as color/power Doppler and the frequency of the transducer could also not
be studied due to the low number of data sets.
Two other modalities playing a role in the management of pancreatic carcinoma are FDG-PET
and endoscopic ultrasonography (EUS). FDG-PET can add incremental information to the diag-
nosis of pancreas cancer; but data on this issue were limited [15, 18, 21, 26, 27, 87, 88]. EUS is
considered the most sensitive modality in the diagnosis of pancreatic cancer and in determining
the local extent of pancreatic cancer, but it cannot reliably assess metastatic involvement in the
liver and because of its invasive character is used in patients with negative or inconclusive CT or
MRI results.
In conclusion, based on the high sensitivity estimate for diagnosis of helical CT compared
with MRI and US and the high specificity value for resectability compared with US, helical CT is
preferable as an imaging modality for the diagnosis and assessment of resectability of pancreatic
adenocarcinoma.

��
Chapter 5
References
1. Parkin DM, Bray F, Ferlay J, et al. Estimating the world cancer burden: Globocan 2000. Int J Cancer. 2001;94:153-156
2. Clarke DL, Thomson SR, Madiba TE, et al. Preoperative imaging of pancreatic cancer: a management-oriented approach. J Am Coll Surg 2003;196:119-129.
3. Del Frate C, Zanardi R, Mortele K, et al. Advances in imaging for pancreatic disease. Curr Gastroenterol Rep 2002;4:140-148.
4. Fletcher JG, Wiersema MJ, Farrell MA, et al. Pancreatic malignancy: value of arterial, pancreatic, and hepatic phase imaging with multi-detector row CT. Radiology 2003;229:81-90.
5. Johnson PT, Heath DG, Hofmann LV, et al. Multidetector-row computed tomography with three-dimen-sional volume rendering of pancreatic cancer: a complete preoperative staging tool using computed tomography angiography and volume-rendered cholangiopancreatography. J Comput Assist Tomogr 2003;27:347-353.
6. Pauls S, Sokiranski R, Schwarz M, et al. [Value of spiral CT and MRI (1.5 T) in preoperative diagnosis of tumors of the head of the pancreas]. Rontgenpraxis 2003;55:3-15.
7. Prokesch RW, Schima W, Chow LC, et al. Multidetector CT of pancreatic adenocarcinoma: diagnostic advances and therapeutic relevance. Eur Radiol 2003;13:2147-2154.
8. Ishiguchi T, Maruyama K, Fukatsu H, et al. Radiologic diagnosis and staging of pancreatic ductal adeno-carcinoma. Semin Surg Oncol 1998;15:23-32.
9. Balci NC, Semelka RC. Radiologic diagnosis of pancreatic carcinoma. Eur J Radiol 2001;38:105-112.
10. Deville WL, Bezemer PD, Bouter LM. Publications on diagnostic test evaluation in family medicine journals: an optimal search strategy. J Clin Epidemiol 2000;53:65-69.
11. Bossuyt PM, Reitsma JB, Bruns DE, et al. Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. Radiology 2003;226:24-28.
12. Berlin JA. Does blinding of readers affect the results of meta-analyses? University of Pennsylvania Meta-Analysis Blinding Study Group. Lancet 1997;350:185-186.
13. Van Houwelingen HC, Zwinderman KH, Stijnen T. A bivariate approach to meta-analysis. Stat Med 1993;12:2273-2284.
14. Van Houwelingen HC, Arends LR, Stijnen T. Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med 2002;21:589-624.
15. Diehl SJ, Lehmann KJ, Sadick M, et al. Pancreatic cancer: value of dual-phase helical CT in assessing resect-ability. Radiology 1998;206:373-378.
16. Keogan MT, McDermott VG, Paulson EK, et al. Pancreatic malignancy: effect of dual-phase helical CT in tumor detection and vascular opacification. Radiology 1997;205:513-518.
17. Legmann P, Vignaux O, Dousset B, et al. Pancreatic tumors: comparison of dual-phase helical CT and endoscopic sonography. AJR Am J Roentgenol 1998;170:1315-1322.
18. Lehmann KJ, Diehl SJ, Lachmann R, et al. [Value of dual-phase-helical CT in the preoperative diagno-sis of pancreatic cancer: a prospective study]. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 1998;168:211-216.
19. Liang KY, Zeger SL. Regression analysis for correlated data. Annu Rev Public Health 1993;14:43-68.
20. McNulty NJ, Francis IR, Platt JF, et al. Multi-detector row helical CT of the pancreas: effect of contrast-en-hanced multiphasic imaging on enhancement of the pancreas, peripancreatic vasculature, and pancreatic adenocarcinoma. Radiology 2001;220:97-102.
21. Mertz HR, Sechopoulos P, Delbeke D, et al. EUS, PET, and CT scanning for evaluation of pancreatic adeno-carcinoma. Gastrointest Endosc 2001;52:367-371.
22. Richter GM, Wunsch C, Schneider B, et al. [Hydro-CT in detection and staging of pancreatic carcinoma]. Radiologe 1998;38:279-286.
23. Rieber A, Tomczak R, Nussle K, et al. MRI with mangafodipir trisodium in the detection of pancreatic tumours: comparison with helical CT. Br J Radiol 2000;73:1165-1169.

Us, CT and MRI for diagnosis and staging pancreatic adenocarcinoma
��
24. Shoup M, Hodul P, Aranha GV, et al. Defining a role for endoscopic ultrasound in staging periampullary tumors. Am J Surg 2000;179:453-456.
25. Schima W, Fugger R, Schober E, et al. Diagnosis and staging of pancreatic cancer: comparison of man-gafodipir trisodium-enhanced MR imaging and contrast-enhanced helical hydro-CT. AJR Am J Roentgenol 2002;179:717-724.
26. Imbriaco M, Megibow AJ, Camera L, et al. Dual-phase versus single-phase helical CT to detect and assess resectability of pancreatic carcinoma. AJR Am J Roentgenol 2002;178:1473-1479.
27. Catalano C, Laghi A, Fraioli F, et al. Pancreatic carcinoma: the role of high-resolution multislice spiral CT in the diagnosis and assessment of resectability. Eur Radiol 2003;13:149-156.
28. Kalady MF, Clary BM, Clark LA, et al. Clinical utility of positron emission tomography in the diagnosis and management of periampullary neoplasms. Ann Surg Oncol 2002;9:799-806.
29. Laghi A, Iannaccone R, Catalano C, et al. Multislice spiral computed tomography in diagnosis and staging of pancreatic carcinoma: preliminary experience. Dig Liver Dis 2002;34:732-738.
30. Bares R, Klever P, Hauptmann S, et al. F-18 fluorodeoxyglucose PET in vivo evaluation of pancreatic glucose metabolism for detection of pancreatic cancer. Radiology 1994;192:79-86.
31. Fink C, Grenacher L, Hansmann HJ, et al. [Prospective study to compare high-resolution computed tomog-raphy and magnetic resonance imaging in the detection of pancreatic neoplasms: use of intravenous and oral MR contrast media]. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 2001;173:724-730.
32. Friess H, Langhans J, Ebert M, et al. Diagnosis of pancreatic cancer by 2[18F]-fluoro-2-deoxy-D-glucose positron emission tomography. Gut 1995;36:771-777.
33. Furukawa T, Tsukamoto Y, Naitoh Y, et al. Differential diagnosis between benign and malignant local-ized stenosis of the main pancreatic duct by intraductal ultrasound of the pancreas. Am J Gastroenterol 1994;89:2038-2041.
34. Inokuma T, Tamaki N, Torizuka T, et al. Evaluation of pancreatic tumors with positron emission tomogra-phy and F- 18 fluorodeoxyglucose: comparison with CT and US. Radiology 1995;195:345-352.
35. Nakaizumi A, Uehara H, Iishi H, et al. Endoscopic ultrasonography in diagnosis and staging of pancreatic cancer. Dig Dis Sci 1995;40:696-700.
36. Palazzo L, Roseau G, Gayet B, et al. Endoscopic ultrasonography in the diagnosis and staging of pancreatic adenocarcinoma. Results of a prospective study with comparison to ultrasonography and CT scan. Endos-copy 1993;25:143-150.
37. Pasanen PA, Eskelinen M, Partanen K, et al. A prospective study of the value of imaging, serum markers and their combination in the diagnosis of pancreatic carcinoma in symptomatic patients. Anticancer Res 1992;12:2309-2314.
38. Rodriguez J, Kasberg C, Nipper M, et al. CT-guided needle biopsy of the pancreas: a retrospective analysis of diagnostic accuracy. Am J Gastroenterol 1992;87:1610-1613.
39. Rosch T, Lorenz R, Braig C, et al. Endoscopic ultrasound in pancreatic tumor diagnosis. Gastrointest Endosc 1991;37:347-352.
40. Snady H, Cooperman A, Siegel J. Endoscopic ultrasonography compared with computed tomography with ERCP in patients with obstructive jaundice or small peri-pancreatic mass. Gastrointest Endosc 1992;38:27-34.
41. Stollfuss JC, Glatting G, Friess H, et al. 2-(fluorine-18)-fluoro-2-deoxy-D-glucose PET in detection of pancre-atic cancer: value of quantitative image interpretation. Radiology 1995;195:339-344.
42. DelMaschio A, Vanzulli A, Sironi S, et al. Pancreatic cancer versus chronic pancreatitis: diagnosis with CA 19-9 assessment, US, CT, and CT-guided fine-needle biopsy. Radiology 1991;178:95-99.
43. Furukawa T, Oohashi K, Yamao K, et al. Intraductal ultrasonography of the pancreas: development and clinical potential. Endoscopy 1997;29:561-569.
44. Muller MF, Meyenberger C, Bertschinger P, et al. Pancreatic tumors: evaluation with endoscopic US, CT, and MR imaging. Radiology 1994;190:745-751.
45. Vellet AD, Romano W, Bach DB, et al. Adenocarcinoma of the pancreatic ducts: comparative evaluation with CT and MR imaging at 1.5 T. Radiology 1992;183:87-95.

��
Chapter 5
46. Papas M, Takacs T, Tron L, et al. The possible role of F-18 FDG positron emission tomography in the dif-ferential diagnosis of focal pancreatic lesions. Clin Nucl Med 2002;27:197-201.
47. Adamek HE, Albert J, Breer H, et al. Pancreatic cancer detection with magnetic resonance cholangio-pancreatography and endoscopic retrograde cholangiopancreatography: a prospective controlled study. Lancet 2000;356:190-193.
48. Diehl SJ, Lehmann KJ, Gaa J, et al. [The value of magnetic resonance tomography (MRT), magnetic reso-nance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) in the diagnosis of pancreatic tumors]. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 1999;170:463-469.
49. Dobritz M, Fellner FA, Baum U, et al. [MR imaging of pancreatic lesions with Mn-DPDP. A histopathologic correlation]. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 2002;174:893-897.
50. Hochwald SN, Rofsky NM, Dobryansky M, et al. Magnetic resonance imaging with magnetic resonance cholangiopancreatography accurately predicts resectability of pancreatic carcinoma. J Gastrointest Surg 1999;3:506-511.
51. Richter A, Gaa J, Niedergethmann M, et al. [Ultrafast magnetic resonance tomography changes the standard in pancreas diagnosis]. Chirurg 2001;72:697-703.
52. Becker D, Strobel D, Bernatik T, et al. Echo-enhanced color- and power-Doppler EUS for the discrimination between focal pancreatitis and pancreatic carcinoma. Gastrointest Endosc 2001;53:784-789.
53. Karlson BM, Ekbom A, Lindgren PG, et al. Abdominal US for diagnosis of pancreatic tumor: prospective cohort analysis. Radiology 1999;213:107-111.
54. Maringhini A, Ciambra M, Raimondo M, et al. Clinical presentation and ultrasonography in the diagnosis of pancreatic cancer. Pancreas 1993;8:146-150.
55. Rickes S, Unkrodt K, Neye H, et al. Differentiation of pancreatic tumours by conventional ultrasound, un-enhanced and echo-enhanced power Doppler sonography. Scand J Gastroenterol 2002;37:1313-1320.
56. Andren-Sandberg A, Lindberg CG, Lundstedt C, et al. Computed tomography and laparoscopy in the as-sessment of the patient with pancreatic cancer. J Am Coll Surg 1998;186:35-40.
57. Bluemke DA, Cameron JL, Hruban RH, et al. Potentially resectable pancreatic adenocarcinoma: spiral CT assessment with surgical and pathologic correlation. Radiology 1995;197:381-385.
58. Bottger T, Engelman R, Seifert JK, et al. Preoperative diagnostics in pancreatic carcinoma: would less be better? Langenbecks Arch Surg 1998;383:243-248.
59. Hommeyer SC, Freeny PC, Crabo LG. Carcinoma of the head of the pancreas: evaluation of the pancreati-coduodenal veins with dynamic CT-potential for improved accuracy in staging. Radiology 1995;196:233-238.
60. Hough TJ, Raptopoulos V, Siewert B, et al. Teardrop superior mesenteric vein: CT sign for unresectable carcinoma of the pancreas. AJR Am J Roentgenol 1999;173:1509-1512.
61. Howard TJ, Chin AC, Streib EW, et al. Value of helical computed tomography, angiography, and endo-scopic ultrasound in determining resectability of periampullary carcinoma. Am J Surg 1997;174:237-241.
62. Lentschig MG, Reimer P, Rummeny E, et al. [The value of 3-phase spiral CT and magnetic resonance tomography in preoperative diagnosis of pancreatic carcinoma]. Radiologe 1996;36:406-412.
63. Lu DS, Reber HA, Krasny RM, et al. Local staging of pancreatic cancer: criteria for unresectability of major vessels as revealed by pancreatic-phase, thin-section helical CT. AJR Am J Roentgenol 1997;168:1439-1443.
64. Phoa SS, Reeders JW, Rauws EA, et al. Spiral computed tomography for preoperative staging of potentially resectable carcinoma of the pancreatic head. Br J Surg 1999;86:789-794.
65. Raptopoulos V, Steer ML, Sheiman RG, et al. The use of helical CT and CT angiography to predict vas-cular involvement from pancreatic cancer: correlation with findings at surgery. AJR Am J Roentgenol 1997;168:971-977.
66. Valls C, Andia E, Sanchez A, et al. Dual-phase helical CT of pancreatic adenocarcinoma: assessment of resectability before surgery. AJR Am J Roentgenol 2001;178:821-826.
67. Zeman RK, Cooper C, Zeiberg AS, et al. TNM staging of pancreatic carcinoma using helical CT. AJR Am J Roentgenol 1997;169:459-464.

Us, CT and MRI for diagnosis and staging pancreatic adenocarcinoma
��
68. Procacci C, Biasiutti C, Carbognin G, et al. Spiral computed tomography assessment of resectability of pancreatic ductal adenocarcinoma: analysis of results. Dig Liver Dis 2002;34:739-747.
69. Minniti S, Bruno C, Biasiutti C, et al. Sonography versus helical CT in identification and staging of pancreatic ductal adenocarcinoma. J Clin Ultrasound 2003;31:175-182.
70. Awad SS, Colletti L, Mulholland M, et al. Multimodality staging optimizes resectability in patients with pancreatic and ampullary cancer. Am Surg 1997;63:634-638.
71. Bakkevold KE, Arnesjo B, Kambestad B. Carcinoma of the pancreas and papilla of Vater-assessment of resectability and factors influencing resectability in stage I carcinomas. A prospective multicentre trial in 472 patients. Eur J Surg Oncol 1992;18:494-507.
72. Freeny PC, Traverso LW, Ryan JA. Diagnosis and staging of pancreatic adenocarcinoma with dynamic computed tomography. Am J Surg 1993;165:600-606.
73. Gress FG, Hawes RH, Savides TJ, et al. Role of EUS in the preoperative staging of pancreatic cancer: a large single-center experience. Gastrointest Endosc 1999;50:786-791.
74. Loyer EM, David CL, Dubrow RA, et al. Vascular involvement in pancreatic adenocarcinoma: reassessment by thin-section CT. Abdom Imaging 1996;21:202-206.
75. McCarthy MJ, Evans J, Sagar G, et al. Prediction of resectability of pancreatic malignancy by computed tomography. Br J Surg 1998;85:320-325.
76. Megibow AJ, Zhou XH, Rotterdam H, et al. Pancreatic adenocarcinoma: CT versus MR imaging in the evaluation of resectability-report of the Radiology Diagnostic Oncology Group. Radiology 1995;195:327-332.
77. O’Malley ME, Boland GW, Wood BJ, et al. Adenocarcinoma of the head of the pancreas: determination of surgical unresectability with thin-section pancreatic-phase helical CT. AJR Am J Roentgenol 1999;173:1513-1518.
78. Warshaw AL, Gu ZY, Wittenberg J, et al. Preoperative staging and assessment of resectability of pancreatic cancer. Arch Surg 1990;125:230-233.
79. Zeiss J, Coombs RJ, Bielke D. CT presentation and staging accuracy of pancreatic adenocarcinoma. Int J Pancreatol 1990;7:49-53.
80. Ahmad NA, Lewis JD, Siegelman ES, et al. Role of endoscopic ultrasound and magnetic resonance imaging in the preoperative staging of pancreatic adenocarcinoma. Am J Gastroenterol 2000;95:1926-1931.
81. McFarland EG, Kaufman JA, Saini S, et al. Preoperative staging of cancer of the pancreas: value of MR angiography versus conventional angiography in detecting portal venous invasion. AJR Am J Roentgenol 1996;166:37-43.
82. Angeli E, Venturini M, Vanzulli A, et al. Color Doppler imaging in the assessment of vascular involvement by pancreatic carcinoma. AJR Am J Roentgenol 1997;168:193-197.
83. Ishida H, Konno K, Hamashima Y, et al. Assessment of resectability of pancreatic carcinoma by color Dop-pler sonography. Abdom Imaging 1999;24:295-298.
84. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999;282:1061-1066.
85. Rutter CM, Gatsonis CA. Regression methods for meta-analysis of diagnostic test data. Acad Radiol 1995;(Suppl 1):S48-S56.
86. Rutter CM, Gatsonis CA. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat Med 2001;20:2865-2884.
87. Jadvar H, Fischman AJ. Evaluation of pancreatic carcinoma with FDG PET. Abdom Imaging 2001;26:254-259.
88. Keogan MT, Tyler D, Clark L, et al. Diagnosis of pancreatic carcinoma: role of FDG PET. AJR Am J Roent-genol 1998;171:1565-1570.

6C h a p t e r

Imaging and treatment of patients with colorectal liver metastases in the Netherlands: a survey
Shandra BipatMaarten S. van LeeuwenJan N.M. IJzermansPatrick M.M. BossuytJan-Willem GreveJaap Stoker
The Netherlands Journal of Medicine 2006;64:147-151

��
Chapter 6
absTRaCT
Background: Clinical experience has highlighted the absence of a uniform approach to the management of patients with colorectal liver metastases in the Netherlands.
Methods: A written survey on the diagnosis and treatment of patients with colorectal liver metastases was sent to all 107 chairmen of oncology committees in each hospital. Questions were asked concerning: specialists involved in decision-making, availability and existence of guidelines, and meetings, factors that needed to be improved, information regarding the di-agnostic work-up of liver metastases, detailed techniques of ultrasonography (US), computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET), factors influencing resectability, types of surgery performed, the use of (neo)-adjuvant chemotherapy, portal vein embolization performance, considering isolated hepatic perfusion (IHP), or local ablation as treatment options, actual performance of local ablation, and the use of systemic as well as regional chemotherapy.
Results: Response rate was 68% (73/107). Specialists involved in the management were mostly surgeons (70), medical oncologists (66), and radiologists (42). Factors that needed to be im-proved, as indicated by responders, were the absence of 1) guidelines; 2) registration of pa-tients; and 3) guidelines for radiofrequency ablation (RFA). Diagnostic work-up of synchronous liver metastases occurred in 71 hospitals, (by US in 69 and by CT in 2). For the work-up of metachronous liver metastases, US was used as initial modality in 14, CT in 2 hospitals, and 57 hospitals used one or the other (mainly US). As additional modality, CT was performed (71) and to a lesser extent MRI (38) or PET (22). Diagnostic laparoscopy and biopsy were performed incidentally. The choice for an imaging modality was mostly influenced by the literature and to a lesser extent by the availability and by costs, personnel, and waiting lists. Substantial varia-tion exists in the US, CT, MRI, and PET techniques. The absence of extrahepatic disease and the clinical condition were considered as the most important factors influencing resectability. Surgery was performed in 30 hospitals; hemihepatectomy in 25, segment resection in 27, multisegment resection in 23, wedge excision in 27, and combination of resection and RFA in 18 institutions. In 52 hospitals (neo)-adjuvant chemotherapy was administrated to improve surgical results, partly (35%) in trials. In nine hospitals portal vein embolization was performed, with the volume of the remnant liver as the most important factor. Local ablative techniques were considered as a treatment option in 48 hospitals and actually performed in 16 hospitals, without clearly defined indications. Experimental IHP was considered a treatment option by 45 (62%) responders, irrespective whether this treatment was available at their center. Patients with extensive metastases received systemic chemotherapy in all 73 hospitals and regional chemotherapy in ten hospitals.
Conclusion: This survey shows substantial variation in the diagnostic and therapeutic work-up of patients with colorectal liver metastases. This variation reflects either under- or over-utilization of diagnosis and treatment options. Evidence-based guidelines taking into account the avail-able evidence, experience and availability can solve this variation.

Management of patients with colorectal liver metastases in the netherlands
��
InTRoDUCTIon
Colorectal carcinoma is one of the commonest solid tumors and is responsible for approximately
10% of cancer-related deaths in the Western world. Liver metastasis is a common consequence
of colorectal carcinoma; 50 to 60% patients develop liver metastases.
Early and accurate diagnosis of liver metastasis is crucial for clinical decision-making. Surgery
is the only therapy that offers any possibility of cure with five-year survival rates after resection
of all detectable disease up to 40% [1-4]. Unfortunately, only 20 to 25% of patients are deemed
suitable for hepatic resection. To improve the results of surgery, a subgroup of these patients
either receive neoadjuvant or adjuvant chemotherapy. Patients not suitable for surgery, due to
extensive liver metastases or extrahepatic diseases, in general undergo systemic chemotherapy.
Several newer therapies such as cryosurgery, radiofrequency ablation (RFA), portal vein emboliza-
tion, isolated hepatic perfusion (IHP), and regional chemotherapy are being evaluated in patients
not suitable for surgery due to the number or distribution of liver metastases [5-11].
Imaging modalities such as ultrasound (US), computed tomography (CT), magnetic resonance
imaging (MRI), positron emission tomography (PET), and laparoscopy (combined with US), rep-
resent important tools in the selection of patients for the appropriate treatment [12-17]. Most
of these diagnostic and therapeutic modalities are available in the Netherlands and there are
concerns about variability in diagnosis and treatment policies.
Clinical experience has highlighted several problems: variation in diagnostic strategies, fac-
tors determining the respectability (presence of extrahepatic diseases), use of neoadjuvant or
adjuvant chemotherapy, extent of use of experimental treatment modalities (RFA, portal vein
embolization, IHP, and regional chemotherapy), and the use of different systemic chemotherapy
regimens. In addition, evidence-based guidelines concerning the diagnosis and treatment are not
available in the Netherlands at the moment.
Current policies are usually based on consensus meetings, expert opinions, results from stud-
ies, and personal and/or institutional experience and preferences, resulting in variable and incon-
sistent choices and regimens among specialists and institutions. By means of a written survey,
we evaluated the policies on the management of patients with colorectal liver metastases in the
Netherlands. The primary aim of this survey was to summarize the extent of variation in the diag-
nosis and treatment strategies. The second aim was to obtain relevant information for developing
and implementing evidence-based guidelines.
MaTeRIals anD MeTHoDs
A written survey on the management of colorectal liver metastases was sent to all Dutch hospitals
dealing with this group of patients in November 2002. A total of 107 questionnaires were sent to
chairmen of the oncology committees in each hospital. All eight academic hospitals participated
in this survey. The replies were returned in prepaid stamped envelopes and collected until June

�0
Chapter 6
2004. Due to the diversity of specialists involved in the work-up, the questionnaire was divided
into three parts:
1) In the general part, questions were asked about the presence of registration systems, the
number of patients diagnosed and/or treated, specialists involved in the treatment policy, avail-
ability of guidelines, existence of meetings, factors that needed to be improved and research on
both diagnostic and treatment field.
2) In the diagnostic part, information on the availability of modalities and the complete diag-
nostic work-up of synchronous and metachronous liver metastases was requested. This included
information on technical details of US, CT, MRI, and PET and the factors influencing the choice
between these approaches.
3) In the treatment part, questions were asked about factors influencing the choice for surgi-
cal treatment, the types of surgery performed, whether (neo)-adjuvant chemotherapy was ad-
ministrated, whether liver perfusion and local ablation were considered as treatment options ir-
respective of availability, types of local ablation performed, portal vein embolization performance
and whether systemic or regional chemotherapy was administrated. In addition, information on
schedules of the chemotherapy approaches was requested.
ResUlTs
Response rateSeventy-four (69%), 73 (68%) and 73 (68%) replies were returned for the general, diagnostic
and treatment parts of the questionnaire, respectively, (including from all eight academic institu-
tions).
GeneralSpecialists involved in the management were surgeons in 70, medical oncologists in 66, radiolo-
gists in 42, internists in 21, gastroenterologist in 17, and nuclear medicine specialists in three
hospitals. In all hospitals meetings were held frequently (once every two weeks) between special-
ists of one hospital (25), specialists of more hospitals (11), or between specialists and consulting
specialists of the Comprehensive Cancer Center in most centers (58).
Registration and guidelines
Registration of patients with colorectal liver metastases was only carried out in 26 hospitals. The
number of patients for diagnosis ranged from 10 to 150, for surgical treatment from 1 to 40
and for palliative chemotherapy from 6 to 45 patients. Practical guidelines were available in only
16 hospitals; however these guidelines were not evidence-based. In addition, most hospitals (66)
indicated they preferred national or regional evidence-based guidelines.
Factors needing improvement
The most important points of concern in the daily practice, according to the responders, were the

Management of patients with colorectal liver metastases in the netherlands
��
absence of general guidelines for diagnosis and treatment of patients with colorectal liver metas-
tases, absence of registration systems and to a lesser extent absence of guidelines for indications
and performance of radiofrequency ablation (RFA).
DiagnosisAvailability of imaging modalities
US and CT were available in all 73 hospitals, MRI in 71, and PET in 11 hospitals, respectively.
Diagnostic work-up of synchronous liver metastases occurred in 71 (97%) hospitals; in 69 mainly
by US and in two by means of CT.
Diagnostic work-up of metachronous liver metastases was performed step by step, starting
with an initial screening modality followed by an additional modality for further detection and
characterization of liver metastases. As initial modality US was used in 14 hospitals, CT in two
hospitals, while 57 hospitals used one or the other (mainly US). As additional modality for charac-
terization and determining resectability, CT was generally performed (71) and to a lesser extent
MRI (38) or PET (22).
In 33 hospitals a one-stop-shop imaging (for detection, characterization and determining re-
sectability) was performed by means of CT. Diagnostic laparoscopy and biopsy (US-guided or
CT-guided) were performed incidentally in 14 and 67 hospitals, respectively. Factors affecting the
choice for a diagnostic modality were mostly influenced by the literature, to a lesser extent by
availability and occasionally by costs, personnel and waiting lists.
The technical details on US, CT, MRI, and PET were provided by 62, 62, 60, and 7 hospitals,
respectively.
Ultrasonography (n = 62). In all hospitals a convex transducer was used for imaging; the use of
an additional linear transducer for detailed visualization of the liver surface was limited to seven
hospitals. US with ‘harmonic frequency’ in combination with conventional US was performed in
43 hospitals. The use of contrast agents for the assessment of vascularisation of focal lesions was
limited to two hospitals.
Computed tomography (n = 62). In 57 hospitals spiral CT scanners were used, including
37 multislice scanners. The number of detectors in the multislice scanners varied from 2 to 16
(modus: 4) and the slice thickness ranged from 1 tot 11 mm (modus: 5 mm). The introduction of
multislice scanners made it possible to perform scanning with lower slice thickness and therefore
to improve the detection of smaller lesions. In most institutions (36), four-phase scanning was
performed (unenhanced, arterial, portal, and late phase). In general the unenhanced and the
portal phases are used for detection of liver metastases; however, arterial and late phases are
helpful in distinguishing other lesions. The amount of iodine ranged from 24 to 72 g (modus 30
g). Detection of liver metastases is expected to improve by using large amount of iodine.
Magnetic emission tomography (n = 60). The magnetic strength of the MRI equipment was
mainly 1.0 T or 1.5 T (n = 47). The most frequently used contrast agent was non-specific gado-
linium (n = 42); to a lesser extent (n = 14) liver specific contrast agents such as Endorem®
(dextran-coated ferumoxide), Resovist® (ferucarbotran), Teslascan® (mangafodipir trisodium),

��
Chapter 6
and Multihance® (gadobenate dimeglumine) were used to increase detection of small liver me-
tastases, due to selective accumulation of contrast agent in liver parenchyma.
Positron emission tomography (n = 7). Six centers had a dedicated full-ring scanner. The
amount of fluoro-2-deoxyglucose varied from 150 to 600 MBq and the analysis was mostly
qualitatively and incidentally semi-quantitatively.
TreatmentFactors influencing resectability are summarized in table 1, with absence of extrahepatic disease
and the clinical condition considered being the most important factors.
Surgery was performed in 30 hospitals: hemihepatectomy in 25, segment resection in 27,
multisegment resection in 23, wedge excision in 27, and a combination of resection and RFA
in 18 institutions. In 52 (71%) hospitals either neoadjuvant or adjuvant chemotherapy was ad-
ministrated to improve surgical results with a substantial variation in the treatment regimens,
mostly 5-fluorouracil + leucovorin or 5-fluorouracil + leucovorin + oxalipatin, while irinotecan was
administrated less often. Approximately 35% (18) of the responders explicitly mentioned that
(neo)-adjuvant chemotherapy was administrated in trials.
Table 1. Factors influencing resectability of liver metastases
Factor Number of hospitals
Number of lesions 57 (78%)
Size of lesions 40 (55%)
Location of lesions 58 (79%)
R0 resection (clear surgical margins) 26 (36%)
Extrahepatic metastases 63 (86%)
Anatomic structure of the liver 26 (36%)
Stage and grade of the primary tumor 14 (19%)
Age of the patient 27 (37%)
Clinical condition of the patient 69 (95%)
Wish of the patient 52 (71%)
Time between primary tumor and metastases detection 24 (33%)
Response: 73 (68%) hospitals.
Portal vein embolization was only performed in nine hospitals to achieve a hypertrophy of the
remnant liver. The most important factor determining the choice for portal vein embolization was
the volume of the remnant liver.
Ablation techniques were considered treatment options in 48 hospitals (47 RFA, 19 cryoabla-
tion, 10 laser-induced interstitial thermotherapy). The actual use of these techniques was limited
to 16 hospitals (RFA in 15, cryoablation in two, and laser-induced interstitial thermotherapy in one
hospital), however without evident indications or guidelines.

Management of patients with colorectal liver metastases in the netherlands
��
Of the responders, 62% (45) indicated that they considered experimental IHP to be a treatment
option irrespective of whether this treatment was available at their center. IHP involves complete
vascular isolation of the liver to allow regional delivery of high-dose chemotherapy to the liver with
little systemic toxicity. This experimental technique is being evaluated at Leiden University Medical
Center and Erasmus Medical Center in Rotterdam.
Patients with extensive metastases are only suitable for chemotherapy, either systemic or
regional. In all 73 hospitals patients received systemic chemotherapy and in ten regional che-
motherapy were given. For systemic chemotherapy, several protocols were used: 5-fluorouracil
and leucovorin with either oxalipatin or irinotecan and the use of capecitabine (instead of 5-
fluorouracil).
DIsCUssIon
In most institutions, the strategy for diagnosis was comparable: US was used as an initial screen-
ing imaging modality to detect patients with liver metastases. Easy availability and non-invasive-
ness are some of the reasons for the widespread use of US. As additional modalities mostly
CT and to a lesser extent MRI were used; however, with a substantial variation in CT and MRI
techniques, such as the use of different phases and amount of contrast for CT and different
contrast agents for MRI.
The variation is mostly a consequence of technical developments (e.g. introduction of multislice
CT and liver specific MRI agents) [12-17] and uncertainties in the literature (different outcomes),
indicating the need for evidence-based guidelines.
In general, diagnostic laparoscopy is performed in selected cases to detect extrahepatic dis-
ease, thereby preventing unnecessary laparotomies. However, in patients selected for surgery
based on extensive imaging, the prevalence of extrahepatic disease will be low and therefore the
additional value of diagnostic laparoscopy will be limited [18-20].
There were concerns about surgery in patients with extrahepatic disease. However, most of
the responders indicated that extrahepatic disease is a major contraindicative factor for surgery.
In 52 hospitals (neo)-adjuvant chemotherapy was given to improve surgical results. Due to the
structure of the written survey, no data on the frequencies of neoadjuvant or adjuvant therapy
are available. (Neo)-adjuvant chemotherapy was also administrated in trials, explaining part of the
variation. We were aware of this variation and tried to summarize the extent of use of (neo)-ad-
juvant, without describing regimens and/or indications. In addition, the effect of (neo)-adjuvant
chemotherapy has not been significantly proven [21, 22].
Portal vein embolization was performed in nine hospitals, with the volume of the remnant liver
as the most important selection criterion.
RFA was considered as a treatment option in most hospitals; however, this technique was per-
formed in a limited number of hospitals, with no uniform indications or selection criteria. A paper
by Mutseart et al. reporting on the initial experience with RFA of malignant hepatic tumors in the
Netherlands showed recurrence in 52% of the patients [23]. In addition, there are no random-

��
Chapter 6
ized trials; RFA is being evaluated in an ongoing randomized trial comparing chemotherapy plus
local ablation with chemotherapy (CLOCC) alone. The advice of the British National Institute for
Clinical Excellence (NICE) is as follows: Current evidence of the safety and efficacy of local tumor
ablation by RFA for colorectal cancer metastases does not appear adequate to support the use of
this procedure without special arrangements for consent and for audit or research [24].
Most of the responders (62%) indicated that they considered IHP a treatment option for
selected patients with extensive liver metastases. IHP has good efficacy in terms of response rate
and duration; however, due to the high toxicity rate, the use of this technique is appropriately
limited to research protocols at dedicated centers [25-29].
The value of regional chemotherapy in patients with non-resectable tumors is unclear. A higher
response percentage is obtained compared with intravenous 5-FU; however, no improvement of
survival is shown [30]. This technique is therefore performed in limited cases in the Netherlands.
An important limitation of this survey is the suboptimal response (69%), not representing the
overall situation in the Netherlands. However, all the academic hospitals and institutions using
the experimental treatment options were included in this survey, thus indicating that the hospitals
that did not respond represent hospitals with a limited number or no patients with this disease.
Two major points of concern in the management of patients with colorectal cancer which
need to be addressed are the absence of guidelines and registration systems. Registration sys-
tems are important tools in evaluating management. The collaboration between specialists and
consulting specialists of the Comprehensive Cancer Centers will make it possible to establish a
national registry.
A national evidence-based guideline is being developed to overcome the problem concerning
the absence of guidelines.
Substantial variation exists in the diagnostic and therapeutic work-up of patients with colorec-
tal liver metastases. This can be explained by recent developments, the availability of techniques,
expertise, uncertainties in the literature (e.g. diagnostic value, effect, survival) and mostly by the
absence of guidelines. Research and evidence-based guidelines taking into account the available
evidence, experience and availability can solve this problem.

Management of patients with colorectal liver metastases in the netherlands
��
References
1. Fong Y, Cohen AM, Fortner JG, et al. Liver resection for colorectal metastases. J Clin Oncol 1997;15:938-946.
2. Hughes KS, Rosenstein RB, Songhorabodi S, et al. Resection of the liver for colorectal carcinoma metasta-ses. A multi-institutional study of longterm survivors. Dis Colon Rectum 1988;31:1-4.
3. Nordlinger B, Guiguet M, Vaillant JC, et al. Surgical resection of colorectal carcinoma metastases to the liver. A prognostic scoring system to improve case selection, based on 1568 patients. Association Francaise de Chirurgie. Cancer 1996;77:1254-1262.
4. Scheele J, Stang R, Altendorf-Hofmann A, Paul M. Resection of colorectal liver metastases. World J Surg 1995;19:59-71.
5. Adam R, Hagopian EJ, Linhares M, et al. A comparison of percutaneous cryosurgery and percutaneous radiofrequency for unresectable hepatic malignancies. Arch Surg 2002;137:1332-1339.
6. Ruers TJ, Joosten J, Jager GJ, Wobbes T. Long-term results of treating hepatic colorectal metastases with cryosurgery. Br J Surg 2001;88:844-849.
7. Shankar A, Lees WR, Gillams AR, Lederman JA, Taylor I. Treatment of recurrent colorectal liver metastases by interstitial laser photocoagulation. Br J Surg 2000;87:298-300.
8. Solbiati L, Livraghi T, Goldberg SN, et al. Percutaneous radio-frequency ablation of hepatic metastases from colorectal cancer: long-term results in 117 patients. Radiology 2001;221:159-166.
9. Vogl T, Mack M, Straub R, et al. [Thermal ablation of liver metastases. Current status and prospects]. Radiologe 2001;41:49-55.
10. Douillard JY, Cunningham D, Roth AD, et al. Irinotecan combined with fluorouracil compared with fluoro-uracil alone as first-line treatment for metastatic colorectal cancer: a multicentre randomised trial. Lancet 2000;355:1041-1047.
11. Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med 2000;343:905-914.
12. Hagspiel KD, Neidl KF, Eichenberger AC, Weder W, Marincek B. Detection of liver metastases: comparison of superparamagnetic iron oxide-enhanced and unenhanced MR imaging at 1.5 T with dynamic CT, intra-operative US, and percutaneous US. Radiology 1995:196:471-478.
13. Jang HJ, Lim HK, Lee WJ, Kim SH, Kim KA, Kim EY. Ultrasonographic evaluation of focal hepatic lesions: comparison of pulse inversion harmonic, tissue harmonic and conventional imaging techniques. J Ultra-sound Med 2000;19:293-299.
14. Lai DT, Fulham M, Stephen MS, et al. The role of whole-body positron emission tomography with [18F] fluo-rodeoxyglucose in identifying operable colorectal cancer metastases to the liver. Arch Surg 1996;131:703-707.
15. Ruers TJ, Langenhoff BS, Neeleman N, et al. Value of positron emission tomography with [F-18] fluoro-deoxyglucose in patients with colorectal liver metastases: a prospective study. J Clin Oncol 2002;20:388-395.
16. Van Etten B, van der Sijp J, Kruyt R, Oudkerk M, van der Holt B, Wiggers T. Ferumoxide-enhanced magnetic resonance imaging techniques in pre-operative assessment for colorectal liver metastases. Eur J Surg Oncol 2002;28:645-651.
17. Kopka L, Grabbe E. [Biphasic liver diagnosis with multiplanar-detector spiral CT]. Radiology 1999:39:971-978.
18. D’Angelica M, Fong Y, Weber S, et al. The role of staging laparoscopy in hepatobiliary malignancy: pro-spective analysis of 401 cases. Ann Surg Oncol 2003;10;183-189.
19. Jarnagin WR, Conlon K, Bodniewicz J, et al. A clinical scoring system predicts the yield of diagnostic laparoscopy in patients with potentially resectable hepatic colorectal metastases. Cancer 2001;91:1121-1128.

Chapter 6
�6 �7
20. Grobmyer SR, Fong Y, D’Angelica M, Dematteo RP, Blumgart LH, Jarnagin WR. Diagnostic laparoscopy prior to planned hepatic resection for colorectal metastases. Arch Surg 2004;139:1326-1330.
21. Figueras J, Valls C, Rafecas A, et al. Resection rate and effect of postoperative chemotherapy on survival after surgery for colorectal liver metastases. Br J Surg 2001;88:980-985.
22. Punt CJ. New options and old dilemmas in the treatment of patients with advanced colorectal cancer. Ann Oncol 2004;15:1453-1459.
23. Mutsaerts EL, van Coevorden F, Krause R, et al. Initial experience with radiofrequency ablation for hepatic tumours in the Netherlands. Eur J Surg Oncol 2003;29:731-734.
24. IPG092 Radiofrequency ablation for the treatment of colorectal metastases in the liver. http://www.nice.org.uk.
25. Alexander HR Jr, Bartlett DL, Libutti SK, Fraker DL, Moser T, Rosenberg SA. Isolated hepatic perfusion with tumour necrosis factor and melphalan for unresectable cancers confined to the liver. J Clin Oncol 1998;16:1479-1489.
26. Bartlett DL, Libutti SK, Figg WD, Fraker DL, Alexander HR. Isolated hepatic perfusion for unresectable hepatic metastases from colorectal cancer. Surgery 2001;129:176-187.
27. Rothbarth J, Pijl ME, Vahrmeijer AL, et al. Isolated hepatic perfusion with high-dose melphalan for the treatment of colorectal metastasis confined to the liver. Br J Surg 2003;90:1391-1397.
28. Marinelli A, de Brauw LM, Beerman H, et al. Isolated liver perfusion with mitomycin C in the treatment of colorectal cancer metastases confined to the liver. Jpn J Clin Oncol1996;26:341-350.
29. Vahrmeijer AL, van Dierendonck JH, Keizer HJ, et al. Increased local cytostatic drug exposure by isolated hepatic perfusion: a phase I clinical and pharmacologic evaluation of treatment with high dose melphalan in patients with colorectal cancer confined to the liver. Br J Cancer 2000;82:1539-1546.
30. Meta-Analysis Group in Cancer. Reappraisal of hepatic arterial infusion in the treatment of nonresectable liver metastases from colorectal cancer. J Nat Cancer Inst 1996;88:252-258.
�6

�6 �7

7C h a p t e r

Colorectal liver metastases: CT, MR imaging, and PET for diagnosis. Meta analysis
Shandra BipatMaarten S. van LeeuwenEmile F. I. ComansMilan E. J. PijlPatrick M. M. BossuytAeilko H. ZwindermanJaap Stoker
Radiology 2005;237:123-131

�00
Chapter 7
absTRaCT
Purpose: To perform a meta-analysis to obtain sensitivity estimates of computed tomography
(CT), magnetic resonance imaging (MRI), and fluorine 18 fluorodeoxyglucose positron emis-
sion tomography (FDG-PET) for detection of colorectal liver metastases on per-patient and
per-lesion bases.
Methods: MEDLINE, EMBASE, Web of Science, and CANCERLIT databases and Cochrane Data-
base of Systematic Reviews were searched for relevant original articles published from Janu-
ary 1990 to December 2003. Criteria for inclusion of articles were as follows: Articles were
reported in the English, German, or French language; CT, MRI or FDG-PET was performed to
identify and characterize colorectal liver metastases; histopathologic analysis (surgery, biopsy,
or autopsy), intraoperative observation (manual palpatation, intraoperative ultrasonography
[US]), and/or follow-up US was the reference standard; and data were sufficient for calculation
of true-positive or false-negative values. A random-effects linear regression model was used to
obtain sensitivity estimates in assessment of liver metastases.
Results: Of 165 identified relevant articles, 61 fulfilled all inclusion criteria. Sensitivity estimates
on a per-patient basis for non-helical CT, helical CT, 1.5 T MRI, and FDG-PET were 60.2%,
64.7%, 75.8%, and 94.6%, respectively; FDG-PET was the most accurate modality.
On a per-lesion basis, sensitivity estimates for non-helical CT, helical CT, 1.0 T MRI, 1.5 T MRI
and FDG-PET were 52.3%, 63.8%, 66.1%, 64.4%, and 75.9%, respectively; non-helical CT had
lowest sensitivity. Estimates of gadolinium-enhanced MRI and superparamagnetic iron oxide
(SPIO)–enhanced MRI were significantly better, compared with non-enhanced MRI (P = 0.019
and P < 0.001, respectively) and with helical CT with 45 g of iodine or less (P = 0.02 and P <
0.001, respectively). For lesions of 1 cm or larger, SPIO-enhanced MRI was the most accurate
modality (P < 0.001).
Conclusion: FDG-PET had significantly higher sensitivity on a per-patient basis, compared with
that of the other modalities, but not on a per-lesion basis. Sensitivity estimates for MRI with
contrast agent were significantly superior to those for helical CT with 45 g of iodine or less.

CT, MRI and PeT for diagnosis colorectal liver metastases: meta-analysis
�0�
InTRoDUCTIon
Colorectal cancer is the second leading cause of cancer-related deaths in the United States. Ac-
cording to the National Program of Cancer Registries, 146 940 new patients received a diagnosis
of the disease in 2004, with an estimated 56 730 deaths due to colorectal cancer in that year.
Liver metastasis is a common consequence of colorectal carcinoma; up to 70% of patients
with colorectal cancer eventually develop liver metastases. In 30%–40% of those patients, the
metastases are still confined to the liver at the time of detection, and only a limited number of
patients with colorectal metastases confined to the liver are surgical candidates because of the
larger size of the lesions, the broad distribution of the lesions, or the difficulty in assessing the
tumors or because the volume of the remaining liver is inadequate [1-5].
Preoperative selection of patients with colorectal metastases who are most likely to benefit
from surgery is necessary and challenging. The armamentarium for imaging-based preoperative
selection comprises transabdominal ultrasonography (US), computed tomography (CT), fluorine
18 fluorodeoxyglucose positron emission tomography (FDG-PET), and magnetic resonance imag-
ing (MRI) [6-12].
During the past 10 years, improvements in these imaging modalities were either introduced or
great progress has been made in their application [6, 8, 13-16]. Although extensive research has
been performed in regard to the diagnostic performance of CT, MRI, and FDG-PET for the detec-
tion of colorectal liver metastases, the optimal imaging staging strategy has not been defined.
Kinkel et al [17] performed a meta-analysis to compare current non-invasive imaging methods
such as US, CT, MRI and FDG-PET for the detection of hepatic metastases from colorectal, gastric,
and esophageal cancers. Treatment approaches for liver metastases from various cancerous ori-
gins (pancreatic or colorectal cancer), however, are different, and, therefore, the importance of
certain findings with respect to these origins differs.
Because of its non-invasive character, low cost, and widespread availability, US is a valuable
screening tool for the imaging of liver metastases. US, however, has two relative disadvantages:
US is more operator independent than are CT and MRI and parts of the liver remain non-visible
in certain patients at US. In daily practice, though, US is highly efficient in helping to distinguish
between two groups of patients with liver metastases: the group of patients with diffuse metas-
tases who are no longer eligible for curative treatment and the group with no metastases or a
very limited number of them. The patients in the latter group require CT, MRI or FDG-PET for the
selection of appropriate therapeutic approaches.
Thus, the aim of our study was to perform a meta-analysis to obtain the estimates of sensitivity
of CT, MRI, and FDG-PET for the detection of colorectal liver metastases on a per-patient and a
per-lesion basis.

�0�
Chapter 7
MaTeRIals anD MeTHoDs
Literature SearchA comprehensive computer literature search [18] of abstracts about studies in human subjects
was performed to identify articles about the diagnostic performance of CT, MRI, and FDG-PET for
the detection of liver metastases in patients with colorectal cancer compared with the diagnostic
performance of intraoperative US, surgery, follow-up US, and histopathologic analysis as the
reference standard.
The MEDLINE and EMBASE databases, from January 1990 to December 2003, were used with
the following keywords: (“Colorectal Neoplasms” [MeSH]) AND (“Liver neoplasms” [MeSH]) AND
(“Laparoscopy” [MeSH] OR “Tomography, Emission-Computed” [MeSH] OR “magnetic resonance
imaging” [MeSH] OR “Tomography, X-Ray Computed” [MeSH] AND (sensitivity and specificity
[MeSH] OR sensitivity [WORD] OR specificity [WORD] OR false negative [WORD] OR false posi-
tive [WORD] OR diagnosis [MeSH] OR diagnostic use [MeSH] OR detection [WORD] OR accuracy
[WORD]).
Other databases, such as CINAHL and SUMSEARCH, were also checked for relevant articles
with the following keywords: Colorectal Neoplasm [MeSH] AND (Liver Neoplasms [MeSH] OR
Neoplasm Metastasis [MeSH]). The databases of Web of Science and CANCERLIT and the Co-
chrane Database of Systematic Review were checked with the following words: Colorectal cancer
AND (liver metastases OR hepatic metastasis).
Review articles, letters, comments, case reports, unpublished articles, and articles that did not
include raw data were not selected. The list of articles was supplemented with extensive cross-
checking of the reference lists of all retrieved articles.
Selection of StudiesFour observers independently checked all retrieved articles for inclusion criteria. One observer
(S.B.) checked all articles. Three observers checked a subset of articles: One observer (M.S.v.L.)
checked studies that predominantly focused on evaluation of CT, another (M.E.J.P.) checked stud-
ies that predominantly focused on evaluation of MRI and another (E.F.I.C.) checked studies that
predominantly focused on evaluation of FDG-PET. Disagreements were resolved in consensus.
The inclusion criteria were as follows: (1) articles were reported in the English, German, or
French language; (2) CT, MRI or FDG-PET was used to identify and characterize colorectal liver
metastases; (3) histopathologic analysis (performed at surgery, biopsy, and autopsy), intraopera-
tive observation (e.g. manual palpation, intraoperative US) and/or follow-up US were used as the
reference standard; (4) for per-patient or per-lesion statistics, sufficient data were presented to
calculate the true-positive and false-negative values for imaging techniques; and (5) when data or
subsets of data were presented in more than one article, the article with the most details or the
most recent article was chosen.
Studies were excluded if results of different imaging modalities were presented in combination
and could not be differentiated for performance assessment of tests on an individual modality.

CT, MRI and PeT for diagnosis colorectal liver metastases: meta-analysis
�0�
Data ExtractionThe same observers independently extracted relevant data about study (design) characteristics
and examination results, which will be discussed later, from each article by using a standardized
form.
One observer (S.B.) extracted data from all articles. Three observers extracted data from a
subset of articles: One observer extracted only data from studies that predominantly focused on
evaluation of CT (M.S.v.L.), another extracted only data from studies that predominantly focused
on evaluation of MRI (M.E.J.P.), and still another extracted only data from studies that predomi-
nantly focused on evaluation of FDG-PET (E.F.I.C.). Observers were not blinded with regard to
information about the authors, the authors’ affiliation, or the journal name, since this has been
shown to be unnecessary [19]. To resolve disagreement between reviewers, a fifth reviewer (J.S.)
assessed all discrepant items, and the majority opinion was used for analysis.
Study design characteristics
The QUADAS quality assessment tool was used to extract relevant study design characteristics of
each study. This tool and the definitions of the characteristics are fully described elsewhere [20].
Other study characteristics
In addition, the following characteristics were recorded: (a) year of publication; (b) sample size
(number of patients with colorectal liver metastases); (c) description of study population, which
included disease severity (tumor stage), age, and male-female distribution; (d) description of
interpretation of diagnostic tests, which included the reporting of the characterization of lesions
as benign versus malignant or the detailed subcharacterization of lesions as cysts, hemangiomas,
or metastases and the confidence rating used for identification of lesions; and (e) description of
reference tests, which included intraoperative findings (at inspection and/or palpation), intraop-
erative US features (probe frequency), pathologic features (staining, lamination, and thickness of
slices), or follow-up characteristics (interval between examinations, frequencies [how many times
follow-up examinations were performed] and modality).
The following imaging features were extracted: (a) for CT, these features included type of scan-
ner (non-helical, single-section helical, or multisection helical), section thickness, amount of con-
trast agent, and number of phases; (b) for MRI, these features included magnetic field strength,
type of contrast agent (non-specific or liver-specific agents), sequences, type of coil (body coil or
phased-array coil), and section thickness; and (c) for FDG-PET, these features included system type
(dedicated full ring or other), amount of tracer, type of analysis (qualitative or quantitative), and
data acquisition characteristics (timing of scanning and time of scanning per table position).
Examination results
The numbers of true-positive, false-negative, and false-positive results in the detection of liver
metastases were extracted on a per-lesion basis. The numbers of true-positive, false-negative,
false-positive, and true-negative results were also extracted on a per-patient basis. All tabulated

�0�
Chapter 7
results for different readers (interobserver), for multiple observations per reader (intraobserver),
and for multiple CT and MRI systems and/or techniques were counted as separate data sets.
Data and Statistical AnalysisData were separately analyzed for non-helical CT, helical CT, MRI at 1.0 T, MRI at 1.5 T, and FDG-
PET. For each data set, we calculated sensitivity of the imaging techniques as the proportion p of
patients with liver metastases (per patient) or as the proportion of liver metastases (per lesion)
correctly recognized by the imaging modality.
In our statistical analysis, we used logit-transformed sensitivity ln {p /(1 – p)}, where ln is
the natural logarithm. Because of the transformation, these values were approximately normal
distributed, with a variance of 1/[n*p* (1 – p)], where n is the total number of patients with liver
metastases (per patient) or the number of liver metastases (per lesion).
Mean logit sensitivity and the standard error were obtained by means of a random-effects
linear regression model with a mixed-effects approach that was a procedure that was within the
software (SAS; SAS Institute, Cary, NC) [21, 22]. After antilogit transformation of the mean logit
sensitivity, sensitivity estimates with the 95% confidence intervals (CIs) were obtained.
All analyses were performed with statistical software (SPSS 11.5 for Windows, SPSS, Chicago,
Ill; SAS, version 8.02, SAS Institute).
Estimates of sensitivity
For comparison of the sensitivity estimates of the different imaging techniques, we first deter-
mined whether the logit sensitivity values depended on year of publication (1995 or earlier vs.
later than 1995), sample size (≤ 50 vs > 50 patients), and the study design characteristics (“yes”
vs “no” and “unclear” responses). In this analysis, we considered variables as explanatory if the
regression coefficient of the variables was significant (P < 0.05).
Subsequently, we developed a multivariable regression model with which we used a backward
stepwise algorithm to identify only the most important characteristics. Characteristics were re-
tained in the regression model when the P value for them was less than 0.10.
Afterward, logit sensitivity values of the imaging techniques of non-helical CT, helical CT, MRI
at 1.0 T, MRI at 1.5 T, and FDG-PET were compared with each other in this random-effects
regression model, which included all variables that significantly affected the logit sensitivity of
the imaging modalities (set to one, indicating the ideal design, vs. zero) as appropriate; in this
final model, a factor that indicated the type of diagnostic modality was included, and a P value of
less than 0.05 of the regression coefficient of this factor was considered to indicate a significant
difference.
Fit of the final regression model was inspected graphically with evaluation of the histograms
of the residuals and of the random-effects estimates.
When studies contributed two or more sensitivity values, for instance, when results of mul-
tiple readers (interobserver) or multiple observations per readers (intraobserver) were available
or when multiple CT or MRI systems or multiple MRI sequences were evaluated, each sensitivity

CT, MRI and PeT for diagnosis colorectal liver metastases: meta-analysis
�0�
value was counted as a separate data set. We accounted for the likely correlation between such
sensitivity values by calculating so-called robust standard errors, which are provided with the
random-effects linear regression model with the mixed-effects approach [23].
This approach was also used for intramodality intrapatient correlation (in some studies, differ-
ent modalities were compared in the same patient population).
Subgroup analysis 1
Enough data sets were available to perform subgroup analyses for helical CT and MRI at 1.5 T.
For helical CT, subgroup analyses were used to compare section thicknesses (5 mm or smaller
vs. larger than 5 mm), the amounts of administered iodine in the contrast agent (≤ 45 g vs. >
45 g), and the number of phases (one phase [portal phase] vs. two phases [arterial and portal
phases]). For MRI at 1.5 T, non-enhanced MRI, MRI enhanced with gadolinium-based contrast
agents, and MRI enhanced with superparamagnetic iron oxide (SPIO) were compared.
The subgroup analyses were performed only for data on a per-lesion basis, as data on a per-
patient basis were limited.
Subgroup analysis 2
In addition, data sets also were analyzed for different lesion sizes (lesions of < 1 cm vs. lesions
≥ 1 cm). With subgroup analyses, lesion size was compared for helical CT, non-enhanced MRI,
gadolinium-enhanced MRI and SPIO-enhanced MRI for 1.5 T imagers.
This analysis was performed only on a per-lesion basis, as data on a per-patient basis were not
available.
ResUlTs
Literature Search and Selection of StudiesWith the computer search and after extensive cross-checking of reference lists, 315 abstracts
were retrieved.
After reading of the abstracts was performed, 165 articles were found to be eligible. One hun-
dred four of the 165 relevant articles were excluded because (a) researchers in the articles did not
report data about the use of CT, MRI or FDG-PET for identification and characterization of colorec-
tal liver metastases (n = 18); (b) researchers in the articles did not use histopathologic analysis,
intraoperative observation, including manual palpation and intraoperative US, and/or follow-up
US as the reference standard (n = 25); (c) researchers in the articles did not report data that could
be used to construct or calculate true-positive, false-positive, true-negative, and/or false-negative
results (n = 54); or (d) researchers in the articles presented results from a combination of differ-
ent imaging modalities that could not be differentiated for assessment of single tests (n = 7).
Sixty-one articles fulfilled all inclusion criteria and were selected for data extraction and data
analysis.

�06
Chapter 7
Study Design CharacteristicsMost studies (table 1) had a suboptimal design in regard to the period between the time when the
reference standard was performed and the time when the index test was performed (67.2% for
“no” responses to question 4), the description of the execution of the reference standard (63.9%
for “no” responses to question 8b), the interpretation of the reference standard results without
knowledge of the index test results (91.2% for “no” responses to question 9b), the availability
of clinical data when test results were interpreted (70.5% for “no” responses to question 10),
reporting of uninterpretable and/or intermediate test results (98.4% for “no” responses to ques-
tion 11), and explanation of withdrawals from the study (75.4% for “no” responses to question
Table 1. Results of distribution of study design characteristics in 61 studies
Question about Study Design Characteristic Response* Yes No
1. Was the spectrum of patients representative of the patients who receive the test in practice?
50 11
2. Were selection criteria clearly described? 36 25
3. Is the reference standard likely to help correctly classify the target condi-tion?
55 6
4. Is the time period between performance of reference standard and index test short enough?
20 41
5. Did the whole sample or a random selection of the sample, receive verifi-cation using a reference standard?
52 9
6. Did patients undergo examination with the same reference standard re-gardless of the index test result?
36 25
7. Was the reference standard performed independently of the index test? 52 9
8a. Was the execution of the index test described in sufficient detail to permit replication of the test?
49 12
8b. Was the execution of the reference standard described in sufficient detail to permit replication of the test?
22 39
9a. Were the index test results interpreted without knowledge of the results of the reference standard?
36 25
9b. Were the reference standard results interpreted without knowledge of the results of the index test?
6 55
10. Were the same clinical data available when test results were interpreted as would be available in practice?
18 43
11. Were uninterpretable and/or intermediate test results reported? 1 60
12. Were withdrawals from the study explained? 15 46
13. Was the data collected after the research question defined? 36 25
* Data are the numbers of responses from the QUADAS tool. The numbers indicate how many articles were assigned as score of “yes” (for the QUADAS tool) and how many articles were assigned a score of “No”. The responses of “No” and “Unclear” were summarized together.

CT, MRI and PeT for diagnosis colorectal liver metastases: meta-analysis
�07
12). It is impossible to perform an ideal study; however, as the choice for a treatment strategy
strongly depends on the outcome of the diagnosis. The description of the execution of the refer-
ence standard remains a problem in studies of diagnostic performance of modalities.
Other Study Design CharacteristicsThe age of the patients included in the selected studies ranged from 12 to 93 years, with a
mean age of 61.0 years and a total of 3187 patients. In 57 studies, the sex distribution was
described: 1733 patients were male and 1128 patients were female. In all studies, imaging data
were presented about the identification of lesions; in only nine studies was a confidence rating
scale presented. In 31 of 61 studies, lesions were characterized (benign lesions were distinguished
from malignant lesions in 28 studies and detailed subcharacterization of lesions was included in
three studies). The reference standard was intraoperative observation (palpation) in 43 studies,
intraoperative US in 37, pathologic analysis in 54, and follow-up US in 31. The frequency of the
transducer used for intraoperative US varied from 5.0 to 7.5 MHz. In 11 of 54 studies in which
pathologic analysis was used as the reference standard, the method of analysis (e.g., staining or
lamination) and the thickness of slices were described.
Examination ResultsTable 2 presents the included data sets (per-patient basis and per-lesion basis), with correspond-
ing numbers of patients and reference numbers. A full list of all included articles with all relevant
study characteristics and complete examination results is available on request from the authors
of this article.
The range in section thickness at CT was 5–12 mm (median, 10 mm), and that for MRI, 5–10
mm (median, 10 mm). The range in the amount of iodine in the administered contrast agent dur-
ing CT (reported in 23 studies) was 30–60 g. In 15 studies, either non-specific gadolinium chelates
or liver-specific MRI contrast agents, such as SPIO and gadobenate dimeglumine, were used. In
most of the studies (15 of 21) about FDG-PET, the images were qualitatively analyzed (uptake of
FDG).
Table 2. Study characteristics of included data sets for each imaging modality
Imaging modality No. of Data setsand Articles
No. of Patientsin Study
References
Non-helical CT 58, 28 1915 10, 24-50
Helical CT 53, 15 621 51-65
1.0 T MRI 34, 5 173 57, 66-69
1.5 T MRI 102, 12 391 27, 51, 53, 54, 70-77
FDG-PET 26, 21 1058 41-50, 52, 59, 64, 77-83

�0�
Chapter 7
Sensitivity Estimates on Per-Patient BasisFollowing the backward stepwise regression analysis, several variables were identified as signifi-
cant predictors of the diagnostic performance of non-helical CT and FDG-PET for assessment of
colorectal liver metastases on a per-patient basis (table 3). No predictors were identified for helical
CT and MRI at 1.5 T. No data sets were available for MRI at 1.0 T. In the final models, all significant
variables were included as covariates.
The sensitivity estimates for non-helical CT, helical CT, MRI at 1.5 T, and FDG-PET were 60.2%
(95% CI: 55.7%-64.6%), 64.7% (95% CI: 30.4%-88.5%), 75.8% (95% CI: 55.9%-88.6%), and
94.6% (95% CI: 92.5%-96.1%), respectively (figure). FDG-PET had a significantly higher sensitivity
estimate compared with that of non-helical CT (P < 0.001), helical CT (P = 0.003), and MRI at 1.5
T (P < 0 .001).
Sensitivity Estimates on Per-Lesion BasisSeveral variables were identified as significant predictors of the diagnostic performance of non-
helical CT, helical CT, MRI at 1.0 T, and MRI at 1.5 T for assessment of colorectal liver metastases
(table 3) on a per-lesion basis. No predictors were found for FDG-PET.
Overall sensitivity estimates for non-helical CT, helical CT, MRI at 1.0 T, MRI at 1.5 T, and
FDG-PET were 52.3%, 63.8%, 66.1%, 64.4%, and 75.9% (table 4). Non-helical CT had the lowest
sensitivity estimate compared with helical CT (P < 0.017), MRI at 1.0 T (P < 0.001), MRI at 1.5 T
(P < 0.001), and FDG-PET (P < 0.003).
Sensitivity Estimates for each Imaging Modality on per-patientFigure shows sensitivity estimates of 60.2%, 64.7%, 75.8%, and 94.6% with 95% confidence intervals for non-helical CT, helical CT, MRI at 1.5 T, and FDG-PET, respectively on a per-patient basis. FDG-PET was the most accurate modality. A comparison of FDG-PET with non-helical CT, helical CT, and MRI at 1.5 T yielded three p values (P < 0.001, P = 0.003, P < 0 .001).
Non-helical CT Helical CT MRI 1.5T FDG-PET
Sensitivity
Per-patient basisPer-patient basis

CT, MRI and PeT for diagnosis colorectal liver metastases: meta-analysis
�0�
Subgroup Analysis 1For helical CT, subgroup analyses included a comparison of a section thickness of 5 mm (no data
about section thickness of < 5 mm were available) with a section thickness of larger than 5 mm, a
comparison of the amount of iodine in the contrast agent of 45 g or less with an amount of more
than 45 g, and a comparison of the number of phases (one phase [portal phase] vs. two phases
[arterial and portal phases]).
Sensitivity estimates for a section thickness of 5 mm and a section thickness of larger than 5
mm were comparable: 68.2% and 69.1%, respectively. For the amount of iodine of 45 g or less
Table 3. Predictors identified with backward regression analysis for each imaging modality
Modality Covariates Regressioncoefficient *
P value
Per Patient
Non-helical CT (19 data sets)
Reference standard helped to correctly clas-sify the target condition
–0.85(–1.37, –0.32)
< 0.002
Reference standard results were interpreted without knowledge of index test results
–0.55(–0.88, –0.21)
< 0.002
Helical CT (2 data sets)
No predictors found
1.5 T MRI (6 data sets)
No predictors found
FDG-PET (15 data sets)
Index test results were interpreted without knowledge of reference standard results
1.07(0.40, 1.75)
< 0.002
Per-lesion
Non-helical CT (22 data sets)
Execution of the index test was described in sufficient detail
0.87(0.38, 1.36)
< 0.001
Reference standard results were interpreted without knowledge of index test results
–0.61(–0.94, –0.28)
< 0.001
Helical CT (39 data sets)
Reference standard helped to correctly clas-sify the target condition
–0.78(–1.40, –0.17)
0.0124
1.0 T MRI (22 data sets)
Spectrum of patients was representative of patients in practice
0.08(0.07, 0.09)
< 0.001
Was the reference standard performed independently of the index test
–0.77(–0.89, –0.65)
< 0.001
1.5 T MRI (57 data sets)
Reference standard helped to correctly clas-sify the target condition
–1.85(–2.24, –1.46)
< 0.001
FDG-PET (9 data sets)
No predictors found
* Numbers in parentheses are 95% confidence intervals. A positive regression coefficient indicates better discrimi-natory power of the imaging modality in studies with that characteristic compared with that in studies without the corresponding characteristics and a negative regression coefficient indicates reduced diagnostic performance in studies with that characteristic.

��0
Chapter 7
and that of more than 45 g, the estimates were 61.4% and 64.0%, respectively. Although the
sensitivity estimate for the portal phase was higher (71.4%) compared with that of the portal and
arterial phases (65.7%), this difference was not significant.
For MRI at 1.5 T, non-enhanced MRI, gadolinium-enhanced MRI, and SPIO-enhanced MRI were
compared. Estimates of sensitivity for non-enhanced MRI, gadolinium-enhanced MRI, and SPIO-
enhanced MRI were 59.8%, 78.2%, and 73.2%, respectively. Sensitivity estimates for gadolinium-
enhanced MRI (P = 0.019) and SPIO-enhanced MR (P < 0.001) were significantly higher compared
with the estimate for non-enhanced MRI.
In addition, sensitivity estimates for gadolinium-enhanced MRI (P = 0.02) and SPIO-enhanced
MRI (P < 0.001) were significantly higher compared with the estimate for helical CT with 45 g or
less of iodine.
Subgroup Analysis 2Sensitivity estimates for non-helical CT, helical CT, non-enhanced MRI, gadolinium-enhanced MRI,
and SPIO-enhanced MRI for lesions smaller than 1 cm were 25.3% (95% CI: 15.9%-37.6%),
23.1% (95% CI: 7.0%-54.7%), 12.6% (95% CI: 8.0%-17.5%), 11.6% (95% CI: 9.5%-14.2%), and
29.3% (95% CI: 18.2%-43.6%), respectively. No differences were found between the imaging
modalities.
Table 4. Sensitivity Estimates for Non-helical CT, Helical CT, 1.0 T MRI, 1.5 T MRI, and FDG-PET on a Per-Lesion Basis
Modality Subgroups Sensitivity Estimates*
Non-helical CT Overall 52.3% (52.1-52.5)†
Helical CT Overall 63.8% (54.4-72.2)†
Slice thickness of 5 mm 68.2% (50.5-81.9)†
Slice thickness of > 5 mm 69.1% (59.8-77.1)†
Amount of Iodine of ≤ 45 gr 61.4% (43.5-76.6)†
Amount Iodine of > 45 gr 64.0% (55.1-72.0)†
Two phases (arterial and portal phases) 65.7% (56.8-73.7)†
One phase (portal phase only) 71.4% (57.7-82.1)†
1.0 T MRI Overall 66.1% (65.9-66.3)†
1.5 T MRI Overall 64.4% (57.8-70.5)†
Non-enhanced MRI 59.8% (49.0-69.7)†
Gadolinium-enhanced MRI 78.2% (63.0-88.3)‡
SPIO-enhanced MRI 73.2% (62.3-81.9)‡
FDG-PET Overall 75.9% (61.1-86.3)†
* Sensitivity estimates were obtained by means of a logit-transformed data analysis, and percentages were not cal-culated with raw data numbers. Numbers in parentheses are 95% confidence intervals expressed as percentages. † Significantly higher compared with non-helical CT‡ Significantly higher compared with non-enhanced MRI and amount of Iodine of 45 gr or less.

CT, MRI and PeT for diagnosis colorectal liver metastases: meta-analysis
���
Sensitivity estimates for non-helical CT, helical CT, non-enhanced MRI, gadolinium-enhanced MRI,
and SPIO-enhanced MRI for lesions of 1 cm or larger were 74.3% (95% CI: 66.5%-80.9%), 73.5%
(95% CI: 62.2%- 82.4%), 65.7% (95% CI: 56.4%-73.9%), 68.8% (95% CI: 61.9%-75.0%), and
90.2% (95% CI: 87.5%-92.4%), respectively. The sensitivity estimate for SPIO-enhanced MRI was
significantly higher (P < 0.001).
DIsCUssIon
In this meta-analysis, we found that on a per-patient basis, FDG-PET was most accurate for de-
tection of colorectal liver metastases. On a per-lesion basis, helical CT, MRI at 1.0 T, MRI at
1.5 T, and FDG-PET were comparable and significantly more accurate than was non-helical CT.
Data about subgroup analyses indicated no differences between section thicknesses, amounts of
administered iodine, and numbers of phases for helical CT. Gadolinium-enhanced MRI and SPIO-
enhanced MRI, however, were significantly better compared with non-enhanced MRI and helical
CT with an amount of iodine of 45 g or less.
As treatment policies differ for liver metastases of various cancerous origins (pancreatic cancer
or colorectal cancer), only data about colorectal cancer were extracted and analyzed.
To avoid selection bias, not only the MEDLINE database but also the CINAHL, SUMSEARCH,
Web of Science, and CANCERLIT databases and the Cochrane Database of Systematic Review
were searched for relevant articles. In addition, all reference lists were checked manually.
To minimize bias in the selection of studies and in data extraction, reviewers independently
selected articles on the basis of inclusion criteria, and scores were assigned to study design char-
acteristics and examination results by using a standardized form that was based on the QUADAS
tool. The QUADAS tool is an evidence-based quality assessment tool, which was developed for
use in systematic reviews of studies of diagnostic accuracy [20].
Data were analyzed by means of a random-effects approach, which accounts for the hetero-
geneity between studies caused by different threshold settings (as in regular summary receiver
operating characteristic curves) [84, 85], for the error of estimation of the sensitivity values in
each study that represents the size of the population, and finally for the residual heterogeneity
that may remain even after adjustment for study design characteristics [86, 87]. Lijmer et al [88]
showed that studies of diagnostic performance of modalities with methodological shortcomings
may cause overestimation of the accuracy of a diagnostic test; we, therefore, evaluated the effect
of these characteristics on diagnostic performance and made adjustments when appropriate.
During the years, substantial improvements in CT (e.g., introduction of spiral CT, multisec-
tion CT) and MRI (e.g., liver-specific agents and more widespread use of higher magnetic field
strength) have been introduced [13-16]. To account for these improvements, data for techniques
were analyzed separately, and, if possible, subgroup analyses were performed. In addition, data
were extracted and analyzed on a per-patient, as well as on a per-lesion, basis. This is important,
since the treatment policy depends not only on distinguishing patients with or without liver me-
tastases but also on the number, size, location, and surgical margin of the liver metastases in the

���
Chapter 7
first group. Thereby, the prevalence of liver metastases in patients with primary colorectal cancer
is high.
A potential limitation of any meta-analysis is the possibility of publication bias. We did not per-
form any analysis for detection of and adjustment for publication bias. A recent systematic review
conducted by the Cochrane Collaboration showed that a large number of methods have been
developed, and when the methods are compared with one another, results can provide different
estimates in terms of direction and magnitude of publication bias [89]. In addition, studies about
publication bias focus mostly on randomized trials, and these studies are registered; the registra-
tion of studies about diagnostic studies is either limited or difficult to achieve. We attempted to
examine publication bias by using an evaluation of whether the size of studies was associated
with the results for diagnostic accuracy. In particular, small studies with optimistic results may be
published more easily than small studies with unfavorable results. Larger studies with optimistic
results may also be published more easily than larger studies with unfavorable results, but this
difference usually is smaller. There was no association between sample size and diagnostic per-
formance.
Characteristics of the patients, such as the stage of disease, differentiation between synchro-
nous and metachronous liver metastases, presence of extrahepatic disease, and age or sex distri-
bution, are also important for diagnostic accuracy, but because of variation in data presentation
or incomplete reporting of data, the effect of these variables could not be examined.
The reference standard used in this systematic review ranged from histopathologic analysis
to follow-up US. It was impossible to examine the effect of each reference test on diagnostic
accuracy. As stated in the Standards for Reporting of Diagnostic Accuracy initiative, a reference
standard can be either a single method or a combination of methods to establish the presence of
the target condition [90]. The major problem, however, was the absence of critical information,
such as data about the execution of the reference test, the confidence rating, or the characteriza-
tion of lesions, and these data were insufficiently described or not described in a large subset of
articles. This has also been described by authors of other meta-analyses [91, 92]. Therefore, the
Standards for Reporting of Diagnostic Accuracy initiative was developed to improve the quality of
the reporting of diagnostic studies. The items in the checklist and the flowchart can help authors
in describing essential elements of the design and conduct of the study, the execution of tests,
and the results.
Another limitation is the consideration of 2 x 2 tables for different readers, for multiple obser-
vations per reader, and for multiple CT and MRI techniques as separate data sets. This has been
performed to avoid selection bias. We are aware of the dependency in data sets from the same
patient population. Analysis of this dependency is not possible with our software, as the random-
effects linear regression model with mixed-effects approach is able to adjust for this potential
dependency only if the same numbers of data sets in each study are available. We examined this
correlation by using the empirical standard error calculated by using the “sandwich estimator,”
which is possible with the software for the regression model with mixed-effects approach [25].
We also used this approach to adjust for correlation between imaging modalities performed in
the same patient population.

CT, MRI and PeT for diagnosis colorectal liver metastases: meta-analysis
���
A final limitation of this study was the absence of information on specificity values. On a per-
patient basis, specificity can be calculated. To minimize selection bias, we included all studies in
which data were presented about colorectal liver metastases (also other conditions) and not stud-
ies in which only colorectal liver metastases were presented. We summarized and analyzed only
data on colorectal liver metastases. The specificity can be underestimated in studies in which only
colorectal liver metastases are evaluated and overestimated in studies in which other conditions
are also evaluated.
Kinkel et al [17] also performed a meta-analysis to compare US, CT, MRI, and FDG-PET in the
detection of liver metastases. In studies with specificity higher than 85%, the sensitivity for US
was 55%, and that for CT was 72%, that for MRI was 76%, and that for FDG-PET was 90%. They,
however, analyzed hepatic metastases that originated from colorectal, gastric, and esophageal
cancers. Treatment policies and reference standards differ for liver metastases of different origins,
and, therefore, the importance of certain findings differs. In addition, the literature search was
performed only in the MEDLINE database, and some study design characteristics were used to
include studies, thereby introducing selection bias. Moreover, they combined results on a per-
patient basis and on a per-lesion basis, thereby causing overestimation of the diagnostic accuracy
of FDG-PET. In our per-patient analysis, FDG-PET had a significantly higher sensitivity estimate
(94.6%) compared with that of helical CT, non-helical CT, and MRI, although the sensitivity esti-
mate was comparable on a per-lesion basis. Analysis of combined data would, therefore, lead to
overestimation of the diagnostic accuracy of FDG-PET.
Although on a per-patient basis, FDG-PET was found to be most accurate, the treatment
policy depends not only on distinguishing patients with liver metastases from patients without
liver metastases but also mainly on the number, size, location, and surgical margin of the liver
metastases. In addition, FDG-PET mostly was performed in selected patients [10, 49] or with a
long time between CT and FDG-PET (> 4 weeks) [42, 46, 49], thereby increasing the detection of
liver metastases by using FDG-PET compared with the detection by using CT. In general, the time
between diagnostic tests should be short to avoid differences in disease status. In several studies,
scans were not corrected for attenuation with CT [46, 64, 78].
Because of its non-invasive character, low cost, and widespread availability, US can be used
to help distinguish patients with diffuse disease who are not eligible for curative treatment from
the group of patients with no liver metastases or the group with a limited number of them. The
patients in the latter group should undergo CT, MRI, or FDG-PET. On a per-lesion basis, helical
CT, MRI at 1.0 T, MRI at 1.5 T, and FDG-PET were comparable and significantly more accurate
compared with non-helical CT. In the subgroup analyses, however, SPIO-enhanced MRI and gado-
linium-enhanced MRI were significantly more accurate compared with non-enhanced MRI and
helical CT performed with a contrast agent that has 45 g or less of iodine.
The choice between portal phase helical CT performed with more than 45 g of iodine and MRI
with a gadolinium-based contrast agent or SPIO should, therefore, also depend on availability and
expertise and not on diagnostic accuracy only. The role of FDG-PET at this moment is limited and,
therefore, it will be used mainly as an additional imaging modality for detection of extrahepatic
disease.

���
Chapter 7
References
1. Jatzko GR, Lisborg PH, Stettner HM, Klimpfinger MH. Hepatic resection for metastases from colorectal carcinoma: a survival analysis. Eur J Cancer 1995;31A:41–46.
2. Castells A, Bessa X, Daniels M, et al. Value of postoperative surveillance after radical surgery for colorectal cancer: results of a cohort study. Dis Colon Rectum 1998;41:714–723.
3. Komborozos VA, Skrekas GJ, Pissiotis CA. The contribution of follow-up programs in the reduction of mortality of rectal cancer recurrences. Dig Surg 2001;18:403–408.
4. Safi F, Link KH, Beger HG. Is follow-up of colorectal cancer patients worthwhile? Dis Colon Rectum 1993;36:636–643.
5. Ketteniss M, Schutz G, Ulrich B. Costs and efficiency of a tumor follow-up program for the detection of colorectal liver metastases. Int J Colorectal Dis 2001;16:28–31.
6. Albrecht T, Blomley MJ, Burns PN, et al. Improved detection of hepatic metastases with pulse-inversion US during the liver-specific phase of SHU 508A: multicenter study. Radiology 2003;227:361–370.
7. Balfe DM. Hepatic metastases from colorectal cancer: radiologic strategies for improved selection. Radiol-ogy 1992;185:18–19.
8. Bellin MF, Zaim S, Auberton E, et al. Liver metastases: safety and efficacy of detection with superparamag-netic iron oxide in MRI. Radiology 1994;193:657–663.
9. Bernatik T, Strobel D, Hahn EG, Becker D. Detection of liver metastases: comparison of contrast-enhanced wide-band harmonic imaging with conventional ultrasonography. J Ultrasound Med 2001;20:509–515.
10. Boykin KN, Zibari GB, Lilien DL, McMillan RW, Aultman DF, McDonald JC. The use of FDG-positron emission tomography for the evaluation of colorectal metastases of the liver. Am Surg 1999;65:1183–1185.
11. Caudana R, Morana G, Pirovano GP, et al. Focal malignant hepatic lesions: MR imaging enhanced with gadolinium benzyloxypropionictetra-acetate (BOPTA)—preliminary results of phase II clinical application. Radiology 1996;199:513–520.
12. Ch’en IY, Katz DS, Jeffrey RB Jr, et al. Do arterial phase helical CT images improve detection or character-ization of colorectal liver metastases? J Comput Assist Tomogr 1997;21:391–397.
13. Kamel IR, Choti MA, Horton KM, et al. Surgically staged focal liver lesions: accuracy and reproducibility of dual-phase helical CT for detection and characterization. Radiology 2003;227:752–757.
14. Kim MJ, Kim JH, Chung JJ, Park MS, Lim JS, Oh YT. Focal hepatic lesions: detection and characteriza-tion with combination gadolinium- and superparamagnetic iron oxide–enhanced MR imaging. Radiology 2003;228:719–726.
15. Dill-Macky MJ, Burns PN, Khalili K, Wilson SR. Focal hepatic masses: enhancement patterns with SH U 508A and pulse-inversion US. Radiology 2002;222:95–102
16. Even-Sapir E, Lerman H, Figer A, et al. Role of (18)F-FDG dual-head gamma-camera coincidence imaging in recurrent or metastatic colorectal carcinoma. J Nucl Med 2002;43:603–609.
17. Kinkel K, Lu Y, Both M, Warren RS, Thoeni RF. Detection of hepatic metastases from cancers of the gastrointestinal tract by using noninvasive imaging methods (US, CT, MR imaging, PET): a meta-analysis. Radiology 2002;224:748–756.
18. Deville WL, Bezemer PD, Bouter LM. Publications on diagnostic test evaluation in family medicine journals: an optimal search strategy. J Clin Epidemiol 2000;53:65–69.
19. Berlin JA. Does blinding of readers affect the results of meta-analyses? University of Pennsylvania Meta-analysis Blinding Study Group. Lancet 1997;350:185-186.
20. Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Meth-odol 2003;3:25.
21. Van Houwelingen HC, Zwinderman KH, Stijnen T. A bivariate approach to meta-analysis. Stat Med 1993;12:2273–2284.

CT, MRI and PeT for diagnosis colorectal liver metastases: meta-analysis
���
22. Van Houwelingen HC, Arends LR, Stijnen T. Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med 2002;21:589–624.
23. Liang KY, Zeger SL. Regression analysis for correlated data. Annu Rev Public Health 1993;14:43–68.
24. Acunas B, Rozanes I, Acunas G, et al. Preoperative CT staging of colon carcinoma (excluding the recto-sigmoid region). Eur J Radiol 1990;11:150–153.
25. Lundstedt C, Ekberg H, Hederstrom E, Tranberg KG. The accuracy of computed tomography of the liver in colo-rectal carcinoma. Clin Radiol 1990;42:335–339.
26. Machi J, Isomoto H, Kurohiji T, et al. Accuracy of intraoperative ultrasonography in diagnosing liver metas-tasis from colorectal cancer: evaluation with postoperative follow-up results. World J Surg 1991;15:551–556.
27. Wernecke K, Rummeny E, Bongartz G, et al. Detection of hepatic masses in patients with carcinoma: comparative sensitivities of sonography, CT, and MR imaging. AJR Am J Roentgenol 1991;157:731–739.
28. Yamaguchi A, Ishida T, Nishimura G, et al. Detection by CT during arterial portography of colorectal cancer metastases to liver. Dis Colon Rectum 1991;34:37–40.
29. Oudkerk M, van Ooijen B, Mali SP, et al. Liver metastases from colorectal carcinoma: detection with continuous CT angiography. Radiology 1992;185:157–161.
30. Soyer P, Levesque M, Elias D, Zeitoun G, Roche A. Preoperative assessment of resectability of hepatic metastases from colonic carcinoma: CT portography vs sonography and dynamic CT. AJR Am J Roentgenol 1992;159:741–744.
31. Soyer P, Levesque M, Elias D, Zeitoun G, Roche A. Detection of liver metastases from colorectal cancer: comparison of intraoperative US and CT during arterial portography. Radiology 1992;183:541–544.
32. Kerner BA, Oliver GC, Eisenstat TE, Rubin RJ, Salvati EP. Is preoperative computerized tomography useful in assessing patients with colorectal carcinoma? Dis Colon Rectum 1993;36:1050–1053.
33. Knol JA, Marn CS, Francis IR, et al. Comparisons of dynamic infusion and delayed computed tomography, intraoperative ultrasound, and palpation in the diagnosis of liver metastases. Am J Surg 1993;165:81–87.
34. Ohlsson B, Tranberg KG, Lundstedt C, Ekberg H, Hederstrom E. Detection of hepatic metastases in colorec-tal cancer: a prospective study of laboratory and imaging methods. Eur J Surg 1993;159:275–281.
35. Soyer P, Elias D, Zeitoun G, Roche A, Levesque M. Surgical treatment of hepatic metastases: impact of intraoperative sonography. AJR Am J Roentgenol 1993;160:511–514.
36. Stewart PJ, Chu JM, Kos SC, Chapuis PH, Bokey EL. Intra-operative ultrasound for the detection of hepatic metastases from colorectal cancer. Aust N Z J Surg 1993;63:530–534.
37. Paul MA, Mulder LS, Cuesta MA, et al. Impact of intraoperative ultrasonography on treatment strategy for colorectal cancer. Br J Surg 1994;81:1660–1663.
38. Leen E, Angerson WJ, Wotherspoon H, et al. Detection of colorectal liver metastases: comparison of lapa-rotomy, CT, US, and Doppler perfusion index and evaluation of postoperative follow-up results. Radiology 1995;195:113–116.
39. Carter R, Hemingway D, Cooke TG, et al. A prospective study of six methods for detection of hepatic colorectal metastases. Ann R Coll Surg Engl 1996;78:27–30.
40. van Ooijen B, Oudkerk M, Schmitz PI, Wiggers T. Detection of liver metastases from colorectal carcinoma: is there a place for routine computed tomography arteriography? Surgery 1996;119:511–516.
41. Lai DT, Fulham M, Stephen MS, et al. The role of whole-body positron emission tomography with [18F]fluorodeoxyglucose in identifying operable colorectal cancer metastases to the liver. Arch Surg 1996;131:703–707.
42. Delbeke D, Vitola JV, Sandler MP, et al. Staging recurrent metastatic colorectal carcinoma with PET. J Nucl Med 1997;38:1196–1201.
43. Ogunbiyi OA, Flanagan FL, Dehdashti F, et al. Detection of recurrent and metastatic colorectal cancer: comparison of positron emission tomography and computed tomography. Ann Surg Oncol 1997;4:613–620.

��6
Chapter 7
44. Abdel-Nabi H, Doerr RJ, Lamonica DM, et al. Staging of primary colorectal carcinomas with fluorine-18 fluorodeoxyglucose whole-body PET: correlation with histopathologic and CT findings. Radiology 1998;206:755–760.
45. Yasuda S, Makuuchi Y, Sadahiro S, et al. Colorectal cancer recurrence in the liver: detection by PET. Tokai J Exp Clin Med 1998;23:167–171.
46. Valk PE, Abella-Columna E, Haseman MK, et al. Whole-body PET imaging with [18F]fluorodeoxyglucose in management of recurrent colorectal cancer. Arch Surg 1999;134:503–511.
47. Zhuang H, Sinha P, Pourdehnad M, et al. The role of positron emission tomography with fluorine-18-de-oxyglucose in identifying colorectal cancer metastases to liver. Nucl Med Commun 2000;21:793–798.
48. Whiteford MH, Whiteford HM, Yee LF, et al. Usefulness of FDG-PET scan in the assessment of suspected metastatic or recurrent adenocarcinoma of the colon and rectum. Dis Colon Rectum 2000;43:759–767.
49. Hung GU, Shiau YC, Tsai SC, et al. Value of 18F-fluoro-2-deoxyglucose positron emission tomography in the evaluation of recurrent colorectal cancer. Anticancer Res 2001;21:1375–1378.
50. Johnson K, Bakhsh A, Young D, Martin TE Jr, Arnold M. Correlating computed tomography and positron emission tomography scan with operative findings in metastatic colorectal cancer. Dis Colon Rectum 2001;44:354–357.
51. Hagspiel KD, Neidl KF, Eichenberger AC, Weder W, Marincek B. Detection of liver metastases: comparison of superparamagnetic iron oxide–enhanced and unenhanced MR imaging at 1.5 T with dynamic CT, intraoperative US, and percutaneous US. Radiology 1995;196:471–478.
52. Vitola JV, Delbeke D, Sandler MP, et al. Positron emission tomography to stage suspected metastatic colorectal carcinoma to the liver. Am J Surg 1996;171:21–26.
53. Strotzer M, Gmeinwieser J, Schmidt J, et al. Diagnosis of liver metastases from colorectal adenocarcinoma: comparison of spiral-CTAP combined with intravenous contrast-enhanced spiral-CT and SPIO-enhanced MR combined with plain MR imaging. Acta Radiol 1997;38:986–992.
54. Lencioni R, Donati F, Cioni D, et al. Detection of colorectal liver metastases: prospective comparison of unenhanced and ferumoxides-enhanced magnetic resonance imaging at 1.5 T, dual-phase spiral CT, and spiral CT during arterial portography. MAGMA 1998;7:76–87.
55. Valls C, Lopez E, Guma A, et al. Helical CT versus CT arterial portography in the detection of hepatic metastasis of colorectal carcinoma. AJR Am J Roentgenol 1998;170:1341–1347.
56. Rahusen FD, Cuesta MA, Borgstein PJ, et al. Selection of patients for resection of colorectal metastases to the liver using diagnostic laparoscopy and laparoscopic ultrasonography. Ann Surg 1999;230:31–37.
57. Ward J, Naik KS, Guthrie JA, Wilson D, Robinson PJ. Hepatic lesion detection: comparison of MR imaging after the administration of superparamagnetic iron oxide with dual-phase CT by using alternative–free response receiver operating characteristic analysis. Radiology 1999;210:459–466.
58. Schmidt J, Strotzer M, Fraunhofer S, Boedeker H, Zirngibl H. Intraoperative ultrasonography versus helical computed tomography and computed tomography with arterioportography in diagnosing colorectal liver metastases: lesion-by-lesion analysis. World J Surg 2000;24:43–47.
59. Arulampalam T, Costa D, Visvikis D, et al. The impact of FDG-PET on the management algorithm for recur-rent colorectal cancer. Eur J Nucl Med 2001;28:1758–1765.
60. Baulieu F, Bourlier P, Scotto B, et al. The value of immunoscintigraphy in the detection of recurrent colorec-tal cancer. Nucl Med Commun 2001;22:1295–1304.
61. Scott DJ, Guthrie JA, Arnold P, et al. Dual phase helical CT versus portal venous phase CT for the detection of colorectal liver metastases: correlation with intra-operative sonography, surgical and pathological find-ings. Clin Radiol 2001;56:235–242.
62. Valls C, Andia E, Sanchez A, et al. Hepatic metastases from colorectal cancer: preoperative detection and assessment of resectability with helical CT. Radiology 2001;218:55–60.
63. Haider MA, Amitai MM, Rappaport DC, et al. Multi–detector row helical CT in preoperative assessment of
small (≤ 1.5 cm) liver metastases: is thinner collimation better? Radiology 2002;225:137–142.

CT, MRI and PeT for diagnosis colorectal liver metastases: meta-analysis
��7
64. Ruers TJ, Langenhoff BS, Neeleman N, et al. Value of positron emission tomography with [F-18]fluorodeox-yglucose in patients with colorectal liver metastases: a prospective study. J Clin Oncol 2002;20:388–395.
65. Pijl ME, Wasser MN, Joekes EC, van De Velde CJ, Bloem JL. Metastases of colorectal carcinoma: compari-son of soft and hard copy helical CT interpretation. Radiology 2003;227:747–751.
66. Soyer P, Laissy JP, Sibert A, et al. Hepatic metastases: detection with multisection FLASH MR imaging during gadolinium chelate–enhanced arterial portography. Radiology 1993;189:401–405.
67. Soyer P, Laissy JP, Sibert A, et al. Focal hepatic masses: comparison of detection during arterial portogra-phy with MR imaging and CT. Radiology 1994;190:737–740.
68. Ward J, Chen F, Guthrie JA, et al. Hepatic lesion detection after superparamagnetic iron oxide enhance-ment: comparison of five T2-weighted sequences at 1.0 T by using alternative–free response receiver operating characteristic analysis. Radiology 2000;214:159–166.
69. del Frate C, Bazzocchi M, Mortele KJ, et al. Detection of liver metastases: comparison of gadobenate dimeglumine–enhanced and ferumoxides-enhanced MR imaging examinations. Radiology 2002;225:766–772.
70. Soyer P, Levesque M, Caudron C, et al. MRI of liver metastases from colorectal cancer vs. CT during arterial portography. J Comput Assist Tomogr 1993;17:67–74.
71. Peterson MS, Baron RL, Murakami T. Hepatic malignancies: usefulness of acquisition of multiple arterial and portal venous phase images at dynamic gadolinium-enhanced MR imaging. Radiology 1996;201:337–345.
72. Oudkerk M, van den Heuvel AG, Wielopolski PA, et al. Hepatic lesions: detection with ferumoxide-en-hanced T1-weighted MR imaging. Radiology 1997;203:449–456.
73. Pijl MEJ, Wasser MNJM, van Persijn van Meerten EL, et al. Comparison of inversion-recovery gradient- and spin-echo and fast spin-echo techniques in the detection and characterization of liver lesions. Radiology 1998;209:427–434.
74. Semelka RC, Cance WG, Marcos HB, Mauro MA. Liver metastases: comparison of current MR tech-niques and spiral CT during arterial portography for detection in 20 surgically staged cases. Radiology 1999;213:86–91.
75. Matsuo M, Kanematsu M, Itoh K, et al. Detection of malignant hepatic tumors: comparison of gadolinium- and ferumoxide-enhanced MR imaging. AJR Am J Roentgenol 2001;177:637–643.
76. Ward J, Guthrie JA, Wilson D, et al. Colorectal hepatic metastases: detection with SPIO-enhanced breath-hold MR imaging—comparison of optimized sequences. Radiology 2003;228(3):709–718.
77. Yang M, Martin DR, Karabulut N, Frick MP. Comparison of MR and PET imaging for the evaluation of liver metastases. J Magn Reson Imaging 2003;17:343–349.
78. Schiepers C, Penninckx F, De Vadder N, et al. Contribution of PET in the diagnosis of recurrent colorectal cancer: comparison with conventional imaging. Eur J Surg Oncol 1995;21:517–522.
79. Flanagan FL, Dehdashti F, Ogunbiyi OA, Kodner IJ, Siegel BA. Utility of FDG-PET for investigating unex-plained plasma CEA elevation in patients with colorectal cancer. Ann Surg 1998;227:319–323.
80. Staib L, Schirrmeister H, Reske SN, Beger HG. Is (18)F-fluorodeoxyglucose positron emission tomography in recurrent colorectal cancer a contribution to surgical decision making? Am J Surg 2000;180:1–5.
81. Willkomm P, Bender H, Bangard M, et al. FDG PET and immunoscintigraphy with 99mTc-labeled antibody fragments for detection of the recurrence of colorectal carcinoma. J Nucl Med 2000;41:1657–1663.
82. Rohren EM, Paulson EK, Hagge R, et al. The role of F-18 FDG positron emission tomography in preopera-tive assessment of the liver in patients being considered for curative resection of hepatic metastases from colorectal cancer. Clin Nucl Med 2002;27:550–555.
83. Rydzewski B, Dehdashti F, Gordon BA, et al. Usefulness of intraoperative sonography for revealing hepatic metastases from colorectal cancer in patients selected for surgery after undergoing FDG PET. AJR Am J Roentgenol 2002;178:353–358.
84. Littenberg B, Moses LE. Estimating diagnostic accuracy from multiple conflicting reports: a new meta-analytic method. Med Decis Making 1993;13:313–321.

Chapter 7
��� ���
85. Moses LE, Shapiro D, Littenberg B. Combining independent studies of a diagnostic test into a summary ROC curve: data-analytic approaches and some additional considerations. Stat Med 1993;12:1293–1316.
86. Rutter CM, Gatsonis CA. Regression methods for meta-analysis of diagnostic test data. Acad Radiol 1995;2(suppl 1):S48–S56.
87. Rutter CM, Gatsonis CA. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat Med 2001;20:2865–2884.
88. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999;282:1061–1066.
89. Pham B, Platt R, McAuley L, Klassen TP, Moher D. Is there a “best” way to detect and minimize publication bias? an empirical evaluation. Eval Health Prof 2001;24:109–125.
90. Bossuyt PM, Reitsma JB, Bruns DE, et al. Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. Radiology 2003;226:24–28.
91. de Vries SO, Hunink MG, Polak JF. Summary receiver operating characteristic curves as a technique for meta-analysis of the diagnostic performance of duplex ultrasonography in peripheral arterial disease. Acad Radiol 1996;3:361–369.
92. Nelemans PJ, Leiner T, de Vet HC, van Engelshoven JM. Peripheral arterial disease: meta-analysis of the diagnostic performance of MR angiography. Radiology 2000;217:105–114.
���

��� ���

8C h a p t e r

Evidence-based guideline on management of colorectal liver metastases in the Netherlands
Shandra BipatMaarten S. van LeeuwenJan N.M. IJzermansEmile F.I. ComansAndre S.Th. PlantingPatrick M.M. BossuytJan-Willem GreveJaap Stoker
The Netherlands Journal of Medicine 2007;65:5-14

���
Chapter 8
absTRaCT
A Dutch national evidence-based guideline on the diagnosis and treatment of patients with
colorectal liver metastases has been developed. The most important recommendations are as
follows.
For synchronous liver metastases, spiral computed tomography (CT) or magnetic resonance
imaging (MRI) should be used as imaging. For evaluation of lung metastases, imaging can be
limited to chest radiography.
For detection of metachronous liver metastases, ultrasonography could be performed as
initial modality, if the entire liver is adequately visualized. In doubtful cases or potential candi-
dates for surgery, CT or MRI should be performed as additional imaging. For evaluation of ex-
trahepatic disease, abdominal and chest CT could be performed. Fluorodeoxyglucose Positron
Emission Tomography (FDG-PET) could be valuable in patients selected for surgery based on
CT (liver/abdomen/chest), for identifying additional extrahepatic disease.
Surgical resection is the treatment of choice with a 5-years survival of 30 to 40%. Variation
in selection criteria for surgery is caused by inconclusive data in the literature concerning surgi-
cal margins <10 mm, presence of extrahepatic disease and the role of (neo)-adjuvant therapy.
To minimize variation in selection criteria, selection should be performed according to this
guideline and preferable in qualified centers.
If resection is not possible, due to extensive disease, palliative chemotherapy is recommend-
ed. Systemic chemotherapy with fluoropyrimidine first-line chemotherapy (5-FU/Leucovorin)
combined with irinotecan or oxaliplatin should be considered as standard regimens.
Radiofrequency ablation, isolated hepatic perfusion, portal vein embolization, and intra-
arterial chemotherapy are considered experimental and should only be performed as part of
a clinical research protocol.

evidence-based guideline ‘Management of colorectal liver metastases’
���
InTRoDUCTIon
Colorectal cancer is the second leading cause of cancer-related deaths in the Netherlands with an
incidence of 9900 and 4400 deaths in 2003 according to the Association of Comprehensive Can-
cer Centers [1]. Approximately 50 to 60% of patients with colorectal cancer eventually develop
liver metastases.
As there are variations in the therapeutic strategies for these patients, the optimal therapy
should be determined on an individual basis. A Dutch survey on the diagnostic and therapeutic
work-up of patients with colorectal liver metastases performed in 2004 showed substantial varia-
tion between different centers in both diagnostic work up and treatment. The most important
points of concern according to the responders of this survey were the absence of a national
guideline for diagnosis and treatment of patients with colorectal liver metastases and the absence
of a registration system [2].
MeTHoDs
To develop a national evidence-based guideline, a working group was established representing
the disciplines involved in this field, including surgeons, medical oncologists, radiologists, gastro-
enterologists and nuclear medicine specialists. All specialists were mandated by their respective
health professional organizations. A list of the members of the working group is presented in
appendix 1.
We performed literature searches in the Cochrane, MEDLINE, CANCERLIT, EMBASE, CINAHL
and Web of Science databases from 1992 to 2005 for different questions. The search strategies
are described in table1. Literature searches were performed for:
1) The diagnostic accuracy of computed tomography (CT), magnetic resonance imaging (MRI),
and 18-fluorodeoxyglucose positron emission tomography (FDG-PET) in the detection of
liver metastases and for detection of extrahepatic lesions; no search was performed for the
diagnostic accuracy of ultrasonography (US), as this modality has a low accuracy;
2) The diagnostic accuracy of diagnostic laparoscopy in the detection of liver metastases and
for detection of extrahepatic lesions;
3) The selection criteria on which surgery is based;
4) The effectiveness of neoadjuvant or adjuvant chemotherapy;
5) The role and effectiveness of the experimental therapeutic options such as portal vein
embolization, ablation techniques and isolated hepatic perfusion;
6) The effectiveness of different chemotherapeutic regimens used;
7) The role of follow-up after treatment of colorectal liver metastases.
All evidence was collected, discussed and categorized by the working group according to general
systems used in evidence-based medicine (table 2). Based on the relevant evidence and taking
into account factors such as experience and availability, recommendations were formulated for

���
Chapter 8
daily practice. These recommendations with corresponding evidence were sent to all the disci-
plines involved for comments, remarks and approval; all disciplines responded with minor com-
ments, remarks and suggestions and approved the final draft of the guideline. All comments and
remarks were incorporated in the final version of the guideline.
In this paper, on behalf of the working group, we report the recommendations with the cor-
responding evidence (including the level of evidence) for the diagnosis, treatment and follow-up
of patients with colorectal liver metastases in the Netherlands.
Table 1. Search strategies
DIAGNOSISMEDLINE
(Colorectal Neoplasms [MESH]) AND (Liver neoplasms [MESH]) AND ((Laparoscopy [MESH]) OR (Tomography, Emission-Computed [MESH]) OR (magnetic resonance imaging [MESH]) OR (Tomography, X-Ray Computed [MESH]) OR (ULTRASONOGRAPHY [MESH])) AND ((sensitivity and specificity [MESH]) OR (specificity [WORD]) OR (false negative [WORD]) OR (diagnosis [SH]) OR (diagnostic use [SH]) OR (detection [WORD]) OR (accuracy [WORD]))
EMBASE
(Colorectal Cancer [MESH]) AND (Liver metastasis [MESH])
CINAHL/SUMSEARCH
(Colorectal Neoplasm [MESH]) AND ((Liver Neoplasms [MESH]) OR (Neoplasm Metastasis [MESH]))
Web of Science/CANCERLIT/ COCHRANE
(Colorectal cancer) AND ((liver metastases) OR (hepatic metastasis))
TREATMENTMEDLINE
(Colorectal Neoplasms [MESH]) AND (Liver Neoplasms [MESH]) AND ((surgery [MESH]) OR (Hepatectomy [MESH]) OR (PERIOPERATIVE CARE [MESH]) OR (Catheter Ablation [MESH]) OR (Cryosurgery [MESH]) OR (Hyperthermia, Induced [MESH]) OR (Palliative Care [MESH]) OR (Drug therapy [MESH]) OR (Antineoplastic Agents [MESH]) OR (Infusions, Intra-Arterial [MESH]) OR (Perfusion, Regional [MESH]) OR (Radiotherapy [MESH])) AND ((Treatment outcome [MESH]) OR (Survival analysis [MESH] OR (Survival [MESH]) OR (Mortality [MESH]) OR (Morbidity [MESH]))
EMBASE
(Colorectal Cancer [MESH]) AND (Liver metastasis [MESH])
CINAHL/SUMSEARCH
(Colorectal Neoplasm [MESH]) AND ((Liver Neoplasms [MESH]) OR (Neoplasm Metastasis [MESH]))
Web of Science/CANCERLIT/ COCHRANE
(Colorectal cancer) AND ((liver metastases) OR (hepatic metastasis))

evidence-based guideline ‘Management of colorectal liver metastases’
���
DIaGnosIs
Beside medical history, physical examination and laboratory test (e.g. CEA measurements), imag-
ing modalities such as transabdominal ultrasonography (US), CT, MRI, and FDG-PET imaging play
a major role in the selection of patients with liver metastases [3-11]. During the past ten years,
improvements in the imaging modalities and changes in applications have been made [6, 7,
10]. Extensive research has been carried out on the diagnostic performance of US, CT, MRI, and
FDG-PET for the detection of liver metastases. Another diagnostic technique playing a role in the
evaluation of liver metastases is diagnostic laparoscopy. However, the optimal imaging staging
strategy has not yet been defined.
Imaging plays a major role at: (1) the time of the diagnosis and treatment of the primary
tumor (for detection of synchronous liver and lung metastases); (2) during the follow-up after
the treatment of the primary tumor (for detection of metachronous liver metastases); and (3) for
Table 2. Levels of Evidence Based on the Categories of Literature*
Level of evidence
1 systematic review (A1) or at least two independent performed studies of category A2
2 systematic review (B1) or at least two independent performed studies of category B2
3 1 study of category A2, B2 or C
4 Expert opinion (category D)
Categories of literature
A1 Systematic reviews of category A2 studies with consistent findings
A2 D: accuracy study (index test compared with reference test) with high quality (prospective performed with blinded interpretation of index test and reference test and large number of consecutive patients undergoing complete verification) T: Randomized controlled trails of high quality (randomized, blinded, complete follow-up, simi-lar baseline characteristics, intension to treat analysis)
B1 Systematic reviews of category B2 studies with consistent findings
B2 D: accuracy study (index test compared with reference test) with poor quality (missing the above mentioned characteristics).T: Randomized controlled trail of low quality or other comparative studies such as non-random-ized, cohort and case-control studies.
C D: Non-comparative study (index test not compared with reference test)T: Non-randomized, cohort and case-control studies with poor quality or descriptive studies (non-comparative studies)
D Opinion form expert committee or clinical experience
D: diagnosis; T: treatment* Sackett DL, Strauss SE, Richardson WS, Rosenberg W, Haynes RB. Evidence-based medicine: How to practice and teach EBM. 2nd ed. Edinburgh: Churchill Livingstone 2000.

��6
Chapter 8
determining the resectability (detection of liver metastases and extrahepatic disease). The recom-
mendations are described in the following paragraphs.
At the time of initial diagnosis and treatment 1) To study baseline characteristics, a spiral CT or MRI of the liver should be performed in stead of
US, due to the low accuracy of US. Baseline CT or MRI are important not only for the detection or
characterization of liver lesions, but also for determining whether patients need adjuvant therapy.
In case of doubt about the presence and characterization of lesions, the CT or MRI examination
should be repeated after three months. Level of evidence: 4
2) For the evaluation of the lungs, imaging can be limited to plain chest radiography, due to the
low prevalence of lung metastases. CT provides a high sensitivity, but it should be noted that
chest CT also gives more false positives. In addition, in patients with negative chest radiography,
the additional value of CT is limited [12, 13]. Level of evidence: 3
During the follow-up and to determine resectability1) For the detection of metachronous liver metastases, we recommend using CEA as marker, if an
elevated CEA level was measured at the time of detection of the primary colorectal tumor. For the
evaluation of the liver, imaging may be limited to US, if the entire liver is assessable. For follow-up
no additional value of spiral CT or MRI to US has been demonstrated [14]. Level of evidence: 2
Because of its non-invasive character, low cost, and widespread availability, US is a valuable
screening tool for the imaging of liver metastases. Moreover US is highly efficient in helping to
distinguish between two groups of patients with liver metastases: patients with diffuse metasta-
ses who are no longer eligible for curative treatment and patients with no or a limited number
of metastases. In daily practice, therefore US is often used as initial imaging modality for the
detection of metachronous liver metastases [2].
2) If the liver cannot be evaluated properly by US, or the CEA elevation cannot be explained or
the irresectability cannot be determined based on US, an additional spiral CT or MRI should be
performed. MRI with Gadolinium (Gd) or superparamagnetic iron oxide (SPIO) contrast medium
and spiral CT with > 45 gram Iodine have a comparable sensitivity for the detection of liver me-
tastases [15]. Level of evidence: 1
The choice between spiral CT with > 45 gr Iodine or MRI with contrast agent (Gd or SPIO),
should therefore be mainly based on local infrastructure (costs, availability and expertise).
3) The role of FDG-PET for the detection of liver metastases and determining the resectability is
limited and should therefore not be performed routinely. In case of doubt concerning lesion char-
acterization on CT and MRI examination, an additional FDG-PET could be helpful, as in patients
with a long interval between CT and FDG-PET or patients selected for additional FDG-PET; this
modality seems to be sensitive for the detection of liver metastases [2] and is therefore also used
as additional modality in daily practice. Level of evidence: 1
4) The prevalence of extrahepatic disease (lung metastases and lymph nodes metastases) in
patient selected for surgery based on extensive imaging is low. From a practical point of view,
during the CT of the liver, additional CT of the abdomen could be performed for evaluation of

evidence-based guideline ‘Management of colorectal liver metastases’
��7
the abdomen. There are no studies evaluating the additional role of abdominal CT for detection
of extrahepatic disease.
For the evaluation of the lungs, a chest CT could also be performed, however chest CT provides
a high number of false positives and the additional value in patients with negative chest radiog-
raphy seems to be low [12, 13]. Level of evidence: 3
Taken into account the low prevalence of lung metastases and the limited additional value of
chest CT for evaluation of the lungs, imaging can be limited to plain chest radiography.
5) In patients selected for surgery after chest, liver and abdominal CT, an additional FDG-PET can
be considered. FDG-PET seems to be sensitive for the detection of extrahepatic disease [16]. Level
of evidence: 1
Moreover the preliminary results of the POLEM study (randomized study: half of the patients
selected for surgery based on abdominal, chest and liver CT, underwent FDG-PET), showed that
unnecessary laparotomy can be prevented in significantly more patients in the FDG-PET group.
In the non-FDG-PET group 29% (14/49) underwent unnecessary laparotomy, while in FDG-PET
group only 11% (5/48) underwent unnecessary laparotomy (P = 0.02); in the FDG-PET group,
surgery was cancelled in 4 patients after FDG-PET. However these data are based on preliminary
nine-month follow–up of 97 patients, while 150 patients are included in this study. (Report
POLEM study, the Netherlands Organization for Health Research and Development (ZonMw)
grant 945-11-017).
PET-CT Hybrid PET-CT can be used for detection of liver metastases and extrahepatic disease when equip-
ment and sufficient expertise is available. Studies have shown that accuracy rates of up to 98%
can be achieved for the detection of liver metastases, extrahepatic disease and local recurrence in
patients who have been treated for colorectal tumor [17-19]. Level of evidence: 3
Diagnostic laparoscopy There is no role for diagnostic laparoscopy in routine daily practice, due to the invasiveness of
diagnostic laparoscopy, low prevalence of small subcapsular lesions and extrahepatic disease and
absence of clinical consequences of small liver metastases, as these generally can be resected.
The additional value of diagnostic laparoscopy in patients after extensive imaging also seems to
be limited [20, 21]. Level of evidence: 3
Additional examination 1) If liver metastases seem to be resectable based on imaging examination, additional examina-
tion of the cardiopulmonary system should be performed to study the clinical condition of the
patient. In general no cytological/ histological biopsies are performed.
2) If liver metastases based on imaging examination and the clinical condition of the patient seem
to be irresectable, no cytological/ histological biopsies should be performed to verify the diagnosis
because of the increased risk for developing needle tract metastases [22]. Biopsies should only be
performed, if histopathology will have clinical consequences.

���
Chapter 8
sURGeRY
Approximately 20% of the patients with liver metastases are considered candidates for surgery,
with a five-year survival of 30 to 40% [23-26].
Selection criteria for surgery are: a residual liver volume of ≥ 30% after resection, the feasibility
of an R0 resection (clear resection margin), limited or no presence of extrahepatic disease and
adequate clinical condition of the patient. However, there is some variation in the prognostic fac-
tors such as the presence of extrahepatic disease, surgical margins of < 10 mm and the timing of
the resection of synchronous liver metastases [2]. Neoadjuvant and adjuvant chemotherapy are
usually administrated to increase the effectiveness of surgery [27, 28], however the effectiveness
is also unknown.
Recommendations based on the evidence found in the literature:
1) In patient with normal functioning liver, at least 30% of the liver parenchyma should remain
after surgery. Up to 70% of the liver volume can be removed in these patients with a normal
functioning liver without risks of postoperative failure [29-31].
Level of evidence: 3
2) As there are no uniform results in the literature concerning a margin of < 10 mm [32-
36] (Level of evidence: 3) and due to the fact that the surgical margin cannot be accurately
determined pre-operatively, a surgical margin of ≥ 10 mm is recommended. Depending on the
anatomic location, a margin of < 10 mm is acceptable as long as a radical resection can be ob-
tained.
3) Attention should be paid to the preoperative evaluation of extrahepatic disease, as patients
with extrahepatic disease have a significantly worse prognosis compared to patients without
extrahepatic disease [37, 38]. Level of evidence: 3
However, there is controversial data on the consequences of the involvement of lymph nodes
located near the liver hilum. Several papers report that this should not be considered an absolute
contraindication for resection and an extended lymphadenectomy should be performed [39, 40],
while in a systematic review only few five-year survivors after liver resection with involvement of
hilum lymph nodes were reported [41]. In summary, there is no uniform evidence concerning the
resection of lymph nodes in the hilum of the liver.
4) The presence of a limited number of lung metastases, without mediastinal lymph node
involvement, is not considered an absolute contraindication for resection of liver metastases, as
resection of a limited number of lung metastases can prolong long-term survival [42-46]. Level
of evidence: 3
Therefore after radical surgery of the liver, subsequent lung surgery could be considered when
only a limited number of lung metastases are found.
5) High age in a patient with good cardiopulmonary condition should not be a contraindica-
tion for liver resection for colorectal cancer metastases. In patients > 70 years a median survival
of up to 33 months and a five-year survival of up to 22% can be achieved [47, 48]. Level of
evidence: 3

evidence-based guideline ‘Management of colorectal liver metastases’
���
6) Although patients with solitary metachronous liver metastases have a better survival com-
pared to patients with synchronous metastases, the presence of synchronous liver metastases
should not be a contraindication for surgery, as five-year survival of up to 31% can be obtained
by resection of synchronous metastases [49-51]. Level of evidence: 3
7) Even though survival after simultaneous resection of colorectal cancer and liver metastases
and resection of liver metastases after an interval of two to three months are comparable [51,
52], simultaneous resection should be avoided, due to the high complication rate. In addition, in
two-thirds of patients major hepatic surgery is avoided, because of the detection of an increased
number of hepatic or distant metastases after an interval of two to three months [52]. Level of
evidence: 3
8) Repeat hepatectomy is advised in patients with new liver metastases after previous liver
surgery for colorectal metastases, if the patient fulfils all criteria for resectability. Repeat liver re-
section for colorectal liver metastases is safe and in well-selected patients can provide prolonged
survival after recurrence of colorectal liver metastases with limited mortality and morbidity rate
[53-59]. Level of evidence: 3
9) Data on the effectiveness of neoadjuvant chemotherapy are controversial and we therefore
recommend the use of neoadjuvant chemotherapy only in clinical research protocols. In a selected
patient population, neoadjuvant chemotherapy with the more effective regimens (combination
of 5-FU/LV with irinotecan or oxaliplatin) can induce response, making curative resection of previ-
ously irresectable liver metastases possible [27, 60-65]. Level of evidence: 3
10) The role of adjuvant chemotherapy after curative surgery is unclear and not advised rou-
tinely [66-71]. Level of evidence: 2
As there is a substantial variation in prognostic factors (see above), the working group recom-
mends that:
1) Liver resection should be performed in centers with high experience level, where appropri-
ate equipment is available and with enough experience in intensive care, anesthesiology and
interventional radiology. Administration of neoadjuvant or adjuvant chemotherapy should be
limited to trials.
2) Registration of patients should be performed, also outside trials. Registration systems are
important tools in evaluating indications for resection and results of resections.
eXPeRIMenTal THeRaPY
As most of the patients with liver metastases are not considered suitable for surgery, other treat-
ment modalities such as ablative therapy, portal vein embolization and isolated hepatic perfusion
have been developed during the last decades [72-82]. However, there is no information available
on the effectiveness of these modalities and the criteria for their application in the Netherlands
[2]. The recommendations of the working group are given for each experimental therapy.

��0
Chapter 8
Portal vein embolization Some patients not considered candidates for surgery due to insufficient remnant liver volume
with increased risk of postoperative liver failure can undergo portal vein embolization (PVE) of
the liver parts to be resected. Portal vein embolization results in atrophy of the embolized parts
and hypertrophy of the remnant liver, reducing the risk of hepatic failure after extended hepa-
tectomy.
So far, only retrospective studies with long-term results [83, 84] or prospective studies with
short-term results in terms of success rate and complications [74, 85-88] have been reported, with
in general, favorable results/findings. Level of evidence: 3 Moreover, small numbers of patients
have been included in these studies. Due to the lack of data on long-term results, PVE should
only be performed in trials, in centers with high experience and where clear-cut indications are
defined.
Ablative therapy Another treatment modality developed during the last decades for patients with liver malignan-
cies is local ablation therapy. The principle of ablation is based on tumor destruction by applying
heat (RFA or interstitial laser therapy) or cold (cryotherapy) or by chemical tumor destruction
(ethanol injection).
1) No recommendations could be made on the role of laser ablation, due to the small number of
studies evaluating long-term results of laser therapy [89, 90]. Level of evidence: 3
2) The number of studies with long-term results on cryotherapy is limited. In comparison with
RFA, cryotherapy has a higher complication rate (bleeding and infection) and more recurrence
[73, 89, 91]. Level of evidence: 3
3) The use of ethanol injection for colorectal liver metastases is not advised, due to the small
number of studies and the low response rate obtained [92-94]. Level of evidence: 3
4) RFA is the most promising technique for ablation purposes [95-98]. Level of evidence: 3
This technique is highly effective for tumor destruction. However, it is not known whether RFA
will prolong the survival of patients with extensive disease. In an ongoing randomized phase III
study (CLOCC trial), the role of local treatment by RFA in patients with irresectable colorectal liver
metastases is being studied. In this study one arm receives RFA combined with chemotherapy
while the second arm receives only chemotherapy. Current evidence on the safety and efficacy
of RFA for colorectal cancer liver metastases does not appear adequate and this experimental
therapy should therefore only be performed as part of a clinical research protocol.
Isolated hepatic perfusion In patients with extensive non-resectable liver metastases, isolated hepatic perfusion (IHP) can be
considered. IHP involves intraoperative perfusion of the isolated liver with extremely high-dose
chemotherapy. The results of recent studies show that high response rates and considerable
survival benefit can be achieved by IHP with different treatment strategies, including IHP with
melphalan alone and melphalan combined with TNF-α or followed by monthly hepatic intra-arte-
rial infusion of fluorodeoxyuridine (FUDR) and leucovorin. In these studies, IHP for colorectal liver

evidence-based guideline ‘Management of colorectal liver metastases’
���
metastases showed response rates of up to 74%, a median time to progression of up to 14.5
months and a median survival of up to 27 months [75, 99]. Level of evidence: 3
IHP was first clinically applied over 40 years ago, but its technical complexity, the potential
morbidity, toxicity rate and the lack of documented efficacy probably have prevented widespread
use. Patient selection is important to ensure good results with minimal morbidity and mortality.
Work to define the appropriate clinical groups is ongoing in the Leiden University Medical Center
and the Erasmus Medical Center Rotterdam and therefore it is necessary to wait for the results of
these studies.
CHeMoTHeRaPY
Most patients with extensive and non-resectable metastases are only eligible for systemic chemo-
therapy. The following recommendations for systematic chemotherapy can be made:
1) For systemic chemotherapy fluoropyrimidine first-line chemotherapy (either oral or systemic
5-FU/Leucovorin) combined with irinotecan or oxaliplatin should be considered as standard regi-
mens; however the optimal regimens with either irinotecan or oxaliplatin are unknown. The effect
of oral 5-FU prodrug monotherapy is comparable with intravenous bolus 5-FU regimens. [100-
103]. Level of evidence: 1
Irinotecan or oxaliplatin combined with 5-FU/leucovorin increases the response and disease-
free-survival compared with 5-FU/leucovorin alone [104-106]. Level of evidence: 2
2) In the absence of contraindications, bevacizumab could be added to the first-line chemother-
apy. This has additional therapeutic value if bevacizumab is added to a fluoropyrimidine first-line
chemotherapy regimen (higher response rate, disease-free and total survival) [107, 108]. Level
of evidence: 2
3) An improvement in the field of chemotherapy is the development of regional (intra-arterial)
chemotherapy [109-111]. With regional chemotherapy higher doses can be administrated and
therefore higher tumor response rates could be achieved; however the effectiveness in terms of
disease-free survival and overall survival are yet unknown [112]. Level of evidence: 1
Therefore, regional chemotherapy at this stage has no role in the routine management.
folloW-UP
When possible, surgical resection is the treatment of choice for hepatic colorectal metastases,
with five-year survival rates of up to 30 to 40%. However, in most of the reported series, disease
recurs in up to 80% of patients after hepatectomy. The recurrence usually involves the liver and is
confined to the liver in approximately half of these cases.
As with initial hepatectomy, the feasibility of repeat resection depends not only on the disease
being confined to the liver but also on the distribution of hepatic disease permitting curative resec-
tion. Overall, only 23% to 33% of hepatic recurrences are resectable [59]. Repeat hepatectomy

���
Chapter 8
is associated with five-year survival rates equivalent to those reported for first hepatectomy [53]
and therefore detecting hepatic recurrence at a resectable stage would significantly improve
prognosis for this selected group of patients.
The aim of follow-up, therefore, is to select patients who are candidates for repeat resection.
This has also been shown in a recently published review [56]. However, there is no evidence avail-
able on the timing, frequency and the program of follow up.
Based on the results of the studies included in the review, a follow-up visit every three months
is recommended for two years, thereafter every six months until five years. Each visit is accompa-
nied with clinical examination, CEA measurements, and CT of the chest and abdomen.
ReGIsTRaTIon sYsTeM
Based on the survey/recommendations from the field, the working group also advocates the
development of a national registration system for the diagnosis and treatment of patients with
colorectal liver metastases. Registration systems are important tools in evaluating patient man-
agement. The collaboration between medical specialists and consulting specialists of the Associa-
tion of Comprehensive Cancer Centers provides the possibility of a national registration.
IMPleMenTaTIon of THe GUIDelIne
For all practitioners involved in the management of patients with colorectal liver metastases in the
Netherlands, the guideline is available on www.oncoline.nl or www.vikc.nl.
Although we are aware that passive dissemination of a guideline may be unlikely to lead to
change, whereas the combination of several active meetings is more likely to lead to success, we
firstly choose to disseminate the guideline by internet. This is because in general, guidelines for
oncologic diseases reported by these sites are easily implemented in daily practice. In addition,
a compact and transparent summary of the guideline has been written which will be sent to all
chairmen of oncology committees in each hospital, in which referral is made to the complete
guideline. Also, the working group has presented this guideline during meetings of the several
disciplines involved in the management of patients with colorectal liver metastases.
There is ongoing research both on diagnosis (POLEM study) and treatment (CLOCC trial and
experimental IHP, PVE). The results of these studies will most likely change the management of
this patient group. Therefore this guideline should be updated, when the results of these and
other relevant studies will be available.

evidence-based guideline ‘Management of colorectal liver metastases’
���
Flowchart Diagnostic and therapeutic strategy in the follow-up after primary colorectal tumor management2 and 3 are considered experimental therapeutic strategies and the working group therefore recommends per-forming these strategies in trials or in centers with extensive experience, with proper equipments and where registration is optimal.

���
Chapter 8
References
1. http://www.ikcnet.nl
2. Bipat S, van Leeuwen MS, Ijzermans JN, Bossuyt PM, Greve JW, Stoker J. Imaging and treatment of patients with colorectal liver metastases in the Netherlands: a survey. Neth J Med 2006;64:147-151.
3. Hagspiel KD, Neidl KF, Eichenberger AC, Weder W, Marincek B. Detection of liver metastases: comparison of superparamagnetic iron oxide-enhanced and unenhanced MR imaging at 1.5 T with dynamic CT, intra-operative US, and percutaneous US. Radiology 1995;196:471-478.
4. Hung GU, Shiau YC, Tsai SC, Chao TH, Ho YJ, Kao CH. Value of 18F-fluoro-2-deoxyglucose positron emis-sion tomography in the evaluation of recurrent colorectal cancer. Anticancer Res 2001;21:1375-1378.
5. Ruers TJ, Langenhoff BS, Neeleman N, et al. Value of positron emission tomography with [F-18]fluoro-deoxyglucose in patients with colorectal liver metastases: a prospective study. J Clin Oncol 2002;20:388-395.
6. Schmidt J, Strotzer M, Fraunhofer S, Boedeker H, Zirngibl H. Intraoperative ultrasonography versus helical computed tomography and computed tomography with arterioportography in diagnosing colorectal liver metastases: lesion-by-lesion analysis. World J Surg 2000;24:43-47.
7. Scott DJ, Guthrie JA, Arnold P, et al. Dual phase helical CT versus portal venous phase CT for the detec-tion of colorectal liver metastases: correlation with intra-operative sonography, surgical and pathological findings. Clin Radiol 2001;56:235-242.
8. Valls C, Andia E, Sanchez A, et al. Hepatic metastases from colorectal cancer: preoperative detection and assessment of resectability with helical CT. Radiology 2001;218:55-60.
9. Vitola JV, Delbeke D, Sandler MP, et al. Positron emission tomography to stage suspected metastatic colorectal carcinoma to the liver. Am J Surg 1996;171:21-26.
10. Ward J, Naik KS, Guthrie JA, Wilson D, Robinson PJ. Hepatic lesion detection: comparison of MR imaging after the administration of superparamagnetic iron oxide with dual-phase CT by using alternative-free response receiver operating characteristic analysis. Radiology 1999;210:459-466.
11. Whiteford MH, Whiteford HM, Yee LF, et al. Usefulness of FDG-PET scan in the assessment of suspected metastatic or recurrent adenocarcinoma of the colon and rectum. Dis Colon Rectum 2000;43:759-767.
12. Kronawitter U, Kemeny NE, Heelan R, Fata F, Fong Y. Evaluation of chest computed tomography in the staging of patients with potentially resectable liver metastases from colorectal carcinoma. Cancer 1999;86:229-235.
13. Povoski SP, Fong Y, Sgouros SC, Kemeny NE, Downey RJ, Blumgart LH. Role of chest CT in patients with negative chest x-rays referred for hepatic colorectal metastases. Ann Surg Oncol 1998;5:9-15.
14. Berman JM, Cheung RJ, Weinberg DS. Surveillance after colorectal cancer resection. Lancet 2000;355:395-399
15. Bipat S, van Leeuwen MS, Comans EF et al. Colorectal liver metastases: CT, MR imaging, and PET for diagnosis—meta-analysis. Radiology 2005;237:123-131.
16. Wiering B, Krabbe PF, Jager GJ, Oyen WJ, Ruers TJ. The impact of fluor-18-deoxyglucose-positron emission tomography in the management of colorectal liver metastases. Cancer 2005;104:2658-2670.
17. Kamel IR, Cohade C, Neyman E, Fishman EK, Wahl RL. Incremental value of CT in PET/CT of patients with colorectal carcinoma. Abdom Imaging 2004;29:663-668.
18. Kim JH, Czernin J, len-Auerbach MS, et al. Comparison between 18F-FDG PET, in-line PET/CT, and software fusion for restaging of recurrent colorectal cancer. J Nucl Med 2005;46:587-595.
19. Selzner M, Hany TF, Wildbrett P, McCormack L, Kadry Z, Clavien PA. Does the novel PET/CT imaging mo-dality impact on the treatment of patients with metastatic colorectal cancer of the liver? Ann Surg 2004 ;240 :1027-1034.
20. D’Angelica M, Fong Y, Weber S, et al. The role of staging laparoscopy in hepatobiliary malignancy: pro-spective analysis of 401 cases. Ann Surg Oncol 2003;10:183-189.

evidence-based guideline ‘Management of colorectal liver metastases’
���
21. Jarnagin WR, Conlon K, Bodniewicz J, et al. A clinical scoring system predicts the yield of diagnostic laparoscopy in patients with potentially resectable hepatic colorectal metastases. Cancer 2001;91:1121-1128.
22. Metcalfe MS, Bridgewater FH, Mullin EJ, Maddern GJ. Useless and dangerous—fine needle aspiration of hepatic colorectal metastases. BMJ 2004;328:507-508.
23. Fong Y, Cohen AM, Fortner JG, et al. Liver resection for colorectal metastases. J Clin Oncol 1997;15:938-946.
24. Jatzko GR, Lisborg PH, Stettner HM, Klimpfinger MH. Hepatic resection for metastases from colorectal carcinoma—a survival analysis. Eur J Cancer 1995;31A:41-46.
25. Mutsaerts EL, van Ruth S, Zoetmulder FA, Rutgers EJ, Hart AA, van Coevorden F. Prognostic factors and evaluation of surgical management of hepatic metastases from colorectal origin: a 10-year single-institute experience. J Gastrointest Surg 2005;9:178-186.
26. Sasaki A, Iwashita Y, Shibata K, Matsumoto T, Ohta M, Kitano S. Analysis of preoperative prognostic fac-tors for long-term survival after hepatic resection of liver metastasis of colorectal carcinoma. J Gastrointest Surg 2005 ;9 :374-380.
27. Adam R, Avisar E, Ariche A, et al. Five-year survival following hepatic resection after neoadjuvant therapy for nonresectable colorectal. Ann Surg Oncol 2001;8:347-353.
28. Kemeny MM. Chemotherapy after hepatic resection of colorectal metastases. Cancer Treat Res 1994;69:121-128.
29. de Baere T, Roche A, Elias D, Lasser P, Lagrange C, Bousson V. Preoperative portal vein embolization for extension of hepatectomy indications. Hepatology 1996;24:1386-91.
30. Kubota K, Makuuchi M, Kusaka K, et al. Measurement of liver volume and hepatic functional reserve as a guide to decision-making in resectional surgery for hepatic tumors. Hepatology 1997;26:1176-81.
31. Schneider PD. Preoperative assessment of liver function. Surg Clin North Am 2004;84:355-373.
32. Cady B, Jenkins RL, Steele GD Jr, et al. Surgical margin in hepatic resection for colorectal metastasis: a critical and improvable determinant of outcome. Ann Surg 1998;227:566-571.
33. Elias D, Cavalcanti A, Sabourin JC, Pignon JP, Ducreux M, Lasser P. Results of 136 curative hepatectomies with a safety margin of less than 10 mm for colorectal metastases. J Surg Oncol 1998;69:88-93.
34. Elias D, Cavalcanti A, Sabourin JC, et al. Resection of liver metastases from colorectal cancer: the real impact of the surgical margin. Eur J Surg Oncol 1998;24:174-179.
35. Kokudo N, Miki Y, Sugai S, et al. Genetic and histological assessment of surgical margins in resected liver metastases from colorectal carcinoma: minimum surgical margins for successful resection. Arch Surg 2002;137:833-840.
36. Pawlik TM, Scoggins CR, Zorzi D, et al. Effect of surgical margin status on survival and site of recurrence after hepatic resection for colorectal metastases. Ann Surg 2005;241:715-737.
37. Beckurts KT, Holscher AH, Thorban S, Bollschweiler E, Siewert JR. Significance of lymph node involvement at the hepatic hilum in the resection of colorectal liver metastases. Br J Surg 1997;84:1081-1084.
38. Jamison RL, Donohue JH, Nagorney DM, Rosen CB, Harmsen WS, Ilstrup DM. Hepatic resection for meta-static colorectal cancer results in cure for some patients. Arch Surg 1997;132:505-510.
39. Elias D, Ouellet JF, Bellon N, Pignon JP, Pocard M, Lasser P. Extrahepatic disease does not contraindicate hepatectomy for colorectal liver metastases. Br J Surg 2003;90:567-574.
40. Jaeck D. The significance of hepatic pedicle lymph nodes metastases in surgical management of colorectal liver metastases and of other liver malignancies. Ann Surg Oncol 2003;10:1007-1011.
41. Rodgers MS, McCall JL. Surgery for colorectal liver metastases with hepatic lymph node involvement: a systematic review. Br J Surg 2000;87:1142-1155.
42. Ike H, Shimada H, Togo S, Yamaguchi S, Ichikawa Y, Tanaka K. Sequential resection of lung metastasis following partial hepatectomy for colorectal cancer. Br J Surg 2002;89:1164-1168.
43. Kobayashi K, Kawamura M, Ishihara T. Surgical treatment for both pulmonary and hepatic metastases from colorectal cancer. J Thorac Cardiovasc Surg 1999;118:1090-1096.

��6
Chapter 8
44. Lehnert T, Knaebel HP, Duck M, Bulzebruck H, Herfarth C. Sequential hepatic and pulmonary resections for metastatic colorectal cancer. Br J Surg 1999;86:241-243.
45. Mineo TC, Ambrogi V, Tonini G, et al. Longterm results after resection of simultaneous and sequential lung and liver metastases from colorectal carcinoma. J Am Coll Surg 2003;197:386-391.
46. Regnard JF, Grunenwald D, Spaggiari L, et al. Surgical treatment of hepatic and pulmonary metastases from colorectal cancers. Ann Thorac Surg 1998; 66:214-218.
47. Brand MI, Saclarides TJ, Dobson HD, Millikan KW. Liver resection for colorectal cancer: liver metastases in the aged. Am Surg 2000;66:412-415.
48. Termuhlen PM, Kemeny MM. Surgery in the older patient. Oncology (Williston Park) 2002;16:183-189.
49. Fujita S, Akasu T, Moriya Y. Resection of synchronous liver metastases from colorectal cancer. Jpn J Clin Oncol 2000;30:7-11.
50. Lyass S, Zamir G, Matot I, Goitein D, Eid A, Jurim O. Combined colon and hepatic resection for synchronous colorectal liver metastases. J Surg Oncol 2001;78:17-21.
51. Vogt P, Raab R, Ringe B, Pichlmayr R. Resection of synchronous liver metastases from colorectal cancer. World J Surg 1991;15:62-67.
52. Lambert LA, Colacchio TA, Barth RJ, Jr. Interval hepatic resection of colorectal metastases improves patient selection. Arch Surg 2000;135:473-479.
53. Adam R, Bismuth H, Castaing D, et al. Repeat hepatectomy for colorectal liver metastases. Ann Surg 1997;225:51-60.
54. Fong Y, Blumgart LH, Cohen A, Fortner J, Brennan MF. Repeat hepatic resections for metastatic colorectal cancer. Ann Surg 1994;220:657-662.
55. Imamura H, Kawasaki S, Miyagawa S, Ikegami T, Kitamura H, Shimada R. Aggressive surgical approach to recurrent tumors after hepatectomy for metastatic spread of colorectal cancer to the liver. Surgery 2000;127:528-535.
56. Metcalfe MS, Mullin EJ, Maddern GJ. Choice of surveillance after hepatectomy for colorectal metastases. Arch Surg 2004;139:749-754.
57. Muratore A, Polastri R, Bouzari H, Vergara V, Ferrero A, Capussotti L. Repeat hepatectomy for colorectal liver metastases: A worthwhile operation? J Surg Oncol 2001;76:127-132.
58. Nagakura S, Shirai Y, Suda T, Hatakeyama K. Multiple repeat resections of intra- and extrahepatic recur-rences in patients undergoing initial hepatectomy for colorectal carcinoma metastases. World J Surg 2002 ;26 :141-147.
59. Nordlinger B, Vaillant JC, Guiguet M, et al. Survival benefit of repeat liver resections for recurrent colorectal metastases: 143 cases. Association Francaise de Chirurgie. J Clin Oncol 1994 ;12 :1491-1496.
60. Adam R, Delvart V, Pascal G, et al. Rescue surgery for unresectable colorectal liver metastases downstaged by chemotherapy: a model to predict long-term survival. Ann Surg 2004;240:644-657.
61. Giacchetti S, Itzhaki M, Gruia G, et al. Long-term survival of patients with unresectable colorectal cancer liver metastases following infusional chemotherapy with 5-fluorouracil, leucovorin, oxaliplatin and surgery. Ann Oncol 1999;10:663-669.
62. Meric F, Patt YZ, Curley SA, et al. Surgery after downstaging of unresectable hepatic tumors with intra-arterial chemotherapy. Ann Surg Oncol 2000;7:490-495.
63. Punt CJ. New options and old dilemmas in the treatment of patients with advanced colorectal cancer. Ann Oncol 2004;15:1453-1459.
64. Rivoire M, De CF, Meeus P, Negrier S, Sebban H, Kaemmerlen P. Combination of neoadjuvant chemo-therapy with cryotherapy and surgical resection for the treatment of unresectable liver metastases from colorectal carcinoma. Cancer 2002;95:2283-2292.
65. Wein A, Riedel C, Kockerling F, et al. Impact of surgery on survival in palliative patients with metastatic colorectal cancer after first line treatment with weekly 24-hour infusion of high-dose 5-fluorouracil and folinic acid. Ann Oncol 2001;12:1721-1727.

evidence-based guideline ‘Management of colorectal liver metastases’
��7
66. Figueras J, Valls C, Rafecas A, Fabregat J, Ramos E, Jaurrieta E. Resection rate and effect of postoperative chemotherapy on survival after surgery for colorectal liver metastases. Br J Surg 2001 ;88 :980-985.
67. Kemeny N, Huang Y, Cohen AM, et al. Hepatic arterial infusion of chemotherapy after resection of hepatic metastases from colorectal cancer. N Engl J Med 1999;341:2039-2048.
68. Kemeny N, Gonen M, Sullivan D, et al. Phase I study of hepatic arterial infusion of floxuridine and dexa-methasone with systemic irinotecan for unresectable hepatic metastases from colorectal cancer. J Clin Oncol 2001;19:2687-2695.
69. Lorenz M, Muller HH, Staib-Sebler E, et al. Relevance of neoadjuvant and adjuvant treatment for patients with resectable liver metastases of colorectal carcinoma. Langenbecks Arch Surg 1999;384:328-338.
70. Ruers T, Bleichrodt RP. Treatment of liver metastases, an update on the possibilities and results. Eur J Cancer 2002;38:1023-1033.
71. Tono T, Hasuike Y, Ohzato H, Takatsuka Y, Kikkawa N. Limited but definite efficacy of prophylactic hepatic arterial infusion chemotherapy after curative resection of colorectal liver metastases: A randomized study. Cancer 2000;88:1549-1556.
72. Abdalla EK, Hicks ME, Vauthey JN. Portal vein embolization: rationale, technique and future prospects. Br J Surg 2001;88:165-175.
73. Adam R, Hagopian EJ, Linhares M, et al. A comparison of percutaneous cryosurgery and percutaneous radiofrequency for unresectable hepatic malignancies. Arch Surg 2002;137:1332-1339.
74. Azoulay D, Castaing D, Smail A, et al. Resection of nonresectable liver metastases from colorectal cancer after percutaneous portal vein embolization. Ann Surg 2000;231:480-486.
75. Bartlett DL, Libutti SK, Figg WD, Fraker DL, Alexander HR. Isolated hepatic perfusion for unresectable hepatic metastases from colorectal cancer. Surgery 2001;129:176-187.
76. Imamura H, Shimada R, Kubota M, et al. Preoperative portal vein embolization: an audit of 84 patients. Hepatology 1999;29:1099-1105.
77. Livraghi T, Solbiati L, Meloni F, Ierace T, Goldberg SN, Gazelle GS. Percutaneous radiofrequency ablation of liver metastases in potential candidates for resection: the “test-of-time approach”. Cancer 2003;97:3027-3035.
78. Makuuchi M, Thai BL, Takayasu K, et al. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery 1990;107:521-527.
79. Marinelli A, de Brauw LM, Beerman H, et al. Isolated liver perfusion with mitomycin C in the treatment of colorectal cancer metastases confined to the liver. Jpn J Clin Oncol 1996;26:341-350.
80. Pearson AS, Izzo F, Fleming RY, et al. Intraoperative radiofrequency ablation or cryoablation for hepatic malignancies. Am J Surg 1999;178:592-599.
81. Rothbarth J, Pijl ME, Vahrmeijer AL, et al. Isolated hepatic perfusion with high-dose melphalan for the treatment of colorectal metastasis confined to the liver. Br J Surg 2003;90:1391-1397.
82. Vahrmeijer AL, van Dierendonck JH, Keizer HJ, et al. Increased local cytostatic drug exposure by isolated hepatic perfusion: a phase I clinical and pharmacologic evaluation of treatment with high dose melphalan in patients with colorectal cancer confined to the liver. Br J Cancer 2000;82:1539-1546.
83. Elias D, De Baere T, Roche A, Bonvallot S, Lasser P. Preoperative selective portal vein embolizations are an effective means of extending the indications of major hepatectomy in the normal and injured liver. Hepatogastroenterology 1998;45:170-177.
84. Elias D, Ouellet JF, de BT, Lasser P, Roche A. Preoperative selective portal vein embolization before hepa-tectomy for liver metastases: long-term results and impact on survival. Surgery 2002;131:294-299.
85. Imamura H, Shimada R, Kubota M, et al. Preoperative portal vein embolization: an audit of 84 patients. Hepatology 1999;29:1099-1105.
86. Fujii Y, Shimada H, Endo I, et al. Changes in clinicopathological findings after portal vein embolization. Hepatogastroenterology 2000;47:1560-1563.
87. Kodama Y, Shimizu T, Endo H, Miyamoto N, Miyasaka K. Complications of percutaneous transhepatic portal vein embolization. J Vasc Interv Radiol 2002;13:1233-1237.

���
Chapter 8
88. Fujii Y, Shimada H, Endo I, et al. Effects of portal vein embolization before major hepatectomy. Hepato-gastroenterology 2003;50:438-442.
89. Christophi C, Nikfarjam M, Malcontenti-Wilson C, Muralidharan V. Long-term survival of patients with unresectable colorectal liver metastases treated by percutaneous interstitial laser thermotherapy. World J Surg 2004;28:987-994.
90. Mack MG, Straub R, Eichler K, et al. Percutaneous MR imaging-guided laser-induced thermotherapy of hepatic metastases. Abdom Imaging 2001;26:369-374.
91. Seifert JK, Morris DL. Prognostic factors after cryotherapy for hepatic metastases from colorectal cancer. Ann Surg 1998;228:201-208.
92. Giorgio A, Tarantino L, Mariniello N, et al. [Ultrasonography-guided percutaneous ethanol injection in large an/or multiple liver metastasis]. Radiol Med (Torino) 1998;96:238-242.
93. Giovannini M, Seitz JF. Ultrasound-guided percutaneous alcohol injection of small liver metastases. Results in 40 patients. Cancer 1994;73:294-297.
94. Livraghi T, Vettori C, Lazzaroni S. Liver metastases: results of percutaneous ethanol injection in 14 patients. Radiology 1991;179:709-712.
95. Gillams AR, Lees WR. Radio-frequency ablation of colorectal liver metastases in 167 patients. Eur Radiol 2004;14:2261-2267.
96. Solbiati L, Ierace T, Goldberg SN, et al. Percutaneous US-guided radio-frequency tissue ablation of liver metastases: treatment and follow-up in 16 patients. Radiology 1997;202:195-203.
97. Solbiati L, Livraghi T, Goldberg SN, et al. Percutaneous radio-frequency ablation of hepatic metastases from colorectal cancer: long-term results in 117 patients. Radiology 2001;221:159-166.
98. Solbiati L, Ierace T, Tonolini M. Long-term survival of patients treated with radiofrequency ablation for liver colorectal metastases: improved outcome with increasing experience. Radiolog 2003S;229:411.
99. Alexander HR, Jr., Bartlett DL, Libutti SK, Fraker DL, Moser T, Rosenberg SA. Isolated hepatic perfusion with tumor necrosis factor and melphalan for unresectable cancers confined to the liver. J Clin Oncol 1998 ;16 :1479-1489.
100. Carmichael J, Popiela T, Radstone D, et al. Randomized comparative study of tegafur/uracil and oral leucovorin versus parenteral fluorouracil and leucovorin in patients with previously untreated metastatic colorectal cancer. J Clin Oncol 2002;20:3617-3627.
101. Douillard JY, Hoff PM, Skillings JR, et al. Multicenter phase III study of uracil/tegafur and oral leucovorin versus fluorouracil and leucovorin in patients with previously untreated metastatic colorectal cancer. J Clin Oncol 2002;20:3605-3616.
102. Hoff PM, Ansari R, Batist G, et al. Comparison of oral capecitabine versus intravenous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: results of a randomized phase III study. J Clin Oncol 2001;19:2282-2292.
103. van Cutsem E, Twelves C, Cassidy J, et al. Oral capecitabine compared with intravenous fluorouracil plus leucovorin in patients with metastatic colorectal cancer: results of a large phase III study. J Clin Oncol 2001 ;19 :4097-4106.
104. de Gramont A, Figer A, Seymour M, et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol 2000;18:2938-2947.
105. Douillard JY, Cunningham D, Roth AD, et al. Irinotecan combined with fluorouracil compared with fluoro-uracil alone as first-line treatment for metastatic colorectal cancer: a multicentre randomized trial. Lancet 2000;355:1041-1047.
106. Giacchetti S, Perpoint B, Zidani R, et al. Phase III multicenter randomized trial of oxaliplatin added to chro-nomodulated fluorouracil-leucovorin as first-line treatment of metastatic colorectal cancer. J Clin Oncol 2000;18:136-147.
107. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004;350:2335-2342.

evidence-based guideline ‘Management of colorectal liver metastases’
���
108. Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus fluorouracil and leucovorin in first-line metastatic colorectal cancer: results of a randomized phase II trial. J Clin Oncol 2005;23:3697-3705.
109. Harmantas A, Rotstein LE, Langer B. Regional versus systemic chemotherapy in the treatment of colorectal carcinoma metastatic to the liver. Is there a survival difference? Meta-analysis of the published literature. Cancer 1996;78:1639-1645.
110. Kerr DJ, McArdle CS, Ledermann J, et al. Intrahepatic arterial versus intravenous fluorouracil and folinic acid for colorectal cancer liver metastases: a multicentre randomized trial. Lancet 2003;361:368-373.
111. Lorenz M, Muller HH. Randomized, multicenter trial of fluorouracil plus leucovorin administered either via hepatic arterial or intravenous infusion versus fluorodeoxyuridine administered via hepatic arterial infusion in patients with nonresectable liver metastases from colorectal carcinoma. J Clin Oncol 2000;18:243-254.
112. Reappraisal of hepatic arterial infusion in the treatment of nonresectable liver metastases from colorectal cancer. Meta-Analysis Group in Cancer. J Natl Cancer Inst 1996;88:252-258.

Chapter 8
��0 ���
aPPenDIX 1
The working group Chairman: J. Stoker, MD, PhD, radiologist, Academic Medical Center, Amsterdam
Vice-chairman: J.W. Greve MD, PhD, surgeon, Maastricht University Hospital, Maastricht
Other members in alphabetic order:
S. Bipat MSc, researcher, Academic Medical Center, Amsterdam
P.M.M. Bossuyt PhD, clinical epidemiologist, Academic Medical Center, Amsterdam
A. Cats MD, PhD, gastro-enterologist, Netherlands Cancer Institute, Amsterdam
E.F.I. Comans MD, PhD, nuclear medicine specialist, VU University Medical Center, Amsterdam
T.M. van Gulik MD, PhD, surgeon, Academic Medical Center, Amsterdam
R.L.H.Jansen MD, PhD, medical oncologist, Maastricht University Hospital, Maastricht
M.S. van Leeuwen MD, PhD, radiologist, University Medical Center Utrecht, Utrecht
M.E.J. Pijl MD, PhD, radiologist, Martini hospital, Groningen
A.S.Th. Planting MD, PhD, medical oncologist, Erasmus Medical Center Rotterdam, Rotterdam
R.A. Tollenaar MD, PhD, surgeon, Leiden University Medical Center, Leiden
J.N.M. IJzermans MD, PhD, surgeon, Erasmus Medical Center Rotterdam, Rotterdam
��0

��0 ���

9C h a p t e r

Multivariate random-effects approach: for meta-analysis of cancer staging studies
Shandra BipatAeilko H. ZwindermanPatrick M.M. BossuytJaap Stoker
Submitted

���
Chapter 9
absTRaCT
Background: Meta-analyses of diagnostic accuracy studies produce summary estimates of sen-
sitivity and specificity. Cancer staging however relies on staging systems and meta-analysis is
often performed after dichotomization. For each dichotomization, summary estimates of sensi-
tivity and specificity can be calculated by repeated bivariate random-effects analyses. However
staging information is lost and under- and overstaging can not be adequately expressed.
Methods: We propose a new multivariate random-effects approach, which is an extension of
the bivariate random-effects approach. In this approach, staging data were used to calculate
correct staging and under- and overstaging. We also calculated sensitivity and specificity for
each dichotomization, using the results obtained by the multivariate approach and compared
these estimates with the results from the repeated bivariate analyses. We used data from a
meta-analysis comparing Endoluminal Ultrasonograpy (EUS) and Magnetic Resonance Imaging
(MRI) in staging of rectal cancer.
Results: In both approaches EUS was more accurate than MRI in staging. The sensitivity and
specificity values of EUS or MRI for the dichotomizations, calculated from the results of the
multivariate approach, were comparable with the sensitivity and specificity estimates of EUS or
MRI obtained by the bivariate analysis. The multivariate analysis demonstrated more overstag-
ing with MRI than EUS.
Conclusion: The multivariate random-effects approach can be a useful meta-analytic method for
summarizing cancer staging data presented in diagnostic accuracy studies.

Multivariate random-effects approach
���
InTRoDUCTIon
Systematic reviews of diagnostic test accuracy studies are undertaken to collect the available
evidence, to evaluate the quality of published studies, and to account for variation in findings
between studies [1-6].
The diagnostic accuracy of a test is often quantified in terms of its sensitivity and specificity.
When results from several studies of a diagnostic test are available, pooling of the results in a
meta-analysis can be done in several ways. For summarizing sensitivity and specificity, several au-
thors [7-9] have shown the potential of a bivariate random-effects approach, and others (10) have
proposed a hierarchical summary receiver operating characteristic (HSROC) model for obtaining
summary estimates sensitivity and specificity. These two models are very closely related [11].
Sensitivity and specificity are important for the differentiation between disease and non-disease.
In the work up of patients with cancer the correct differentiation between disease and non-
disease is not the only important issue. Correctly determining the extent of tumor invasion (T-stag-
ing) is of primary interest as well [12-16]. So far, summary estimates of the results of T-staging
as compared to the reference standard are usually obtained by first dichotomizing the staging
results in each study, and then performing meta-analysis of the resulting sensitivity and specificity
pairs. In rectal cancer, for example, four stages of the primary tumor are reported: T1, T2, T3
and T4. To analyze the data in terms of sensitivity and specificity one can compare: T1 versus
T2+T3+T4, T1+T2 versus T3+T4 and T1+T2+T3 versus T4. Such repeated analyses necessitate a
number of decisions by the analyst which are hard to objectify.
In this paper we propose a new multivariate random-effects approach in which staging data
(k x k tables) are used to calculate correct staging, understaging and overstaging. We suggest
performing meta-analysis directly on these tables as obtained from the included primary studies.
In this way only one data-analysis is required, while every comparison can be calculated from the
results of this single analysis.
We will compare this multivariate approach with the result of the repeated bivariate approach
after dichotomization, using data from a previously published meta-analysis [17] on staging rectal
cancer: 11 data sets on Magnetic Resonance Imaging (MRI) and 26 data sets on endoluminal
ultrasonography (EUS).
The first section contains a short description of the bivariate approach and is applied to the MRI
and EUS data. The second section described the multivariate random- effects approach and its
application to the same data. Finally, we will compare both methods, and discuss our findings.
bIVaRIaTe RanDoM-effeCTs aPPRoaCH
The vast majority of diagnostic accuracy studies report their findings as pairs of sensitivity and
specificity. Sensitivity and specificity have become the most familiar measures to clinicians. Con-
sequently, these statistics are also considered as the main outcome measures in meta-analysis of
diagnostic accuracy studies.

��6
Chapter 9
1. PrincipleDichotomizing data for bivariate analysis
T-staging of a rectal cancer is defined as follows; T1-stage: invasion of the submucosa; T2-
stage: invasion of muscularis propria; T3-stage: invasion of perirectal tissue and T4-stage: invasion
of adjacent organs. If the results of EUS or MRI of n patients are compared to the reference
standard, the results in a particular study can be summarized in a 4-by-4 table (table 1), where n11
is the number of on these tables as obtained from the included primary studies. In this way only
patients with T1 stage by either EUS or MRI and verified by the reference standard. Similarly, n12 is
the number of patients with T1 stage by EUS/MRI and T2 stage according to reference standard;
and so on.
If the table is dichotomized as T1 vs. T2+T3+T4, the specificity in this study is computed
as p1=n11/n1 and sensitivity as p2= (n22+n23+n24+n32+n33+n34+n42+n43+n44)/ (n2+n3+n4). If
the table is dichotomized as T1+T2 vs. T3+T4 the specificity in this study is computed as p1=
(n11+n12+n21+n22)/ (n1+n2) and the sensitivity as p2=n33+n34+n43+n44)/ (n3+n4). Finally, if the table
is dichotomized as T1+T2+T3 vs. T4 the specificity in this study is computed as p1= (n11+n12+n13+
n21+n22+n23+n31+n32+n33/ (n1+n2+n3), and the sensitivity as p2=n44/n4.
Table 1. EUS or MRI data compared with reference standard
Reference standard
T1 T2 T3 T4
EUS or MRI
T1 n11 n12 n13 n14
T2 n21 n22 n23 n24
T3 n31 n32 n33 n34
T4 n41 n42 n43 n44
Sum n1 n2 n3 n4
The bivariate analysis
The bivariate model uses pairs of sensitivity and specificity estimates from a series of studies (9).
In this model, the assumption is made that the true values of sensitivity and specificity of the dif-
ferent studies follow a bivariate distribution. As sensitivity and specificity only vary between 0 and
1, the logit-transformed sensitivity and logit-transformed specificity values are modeled.
Logit-transformed sensitivity and specificity are calculated as follows:
ln and ln respectively.

Multivariate random-effects approach
��7
The logit-transformed specificities and logit-transformed sensitivities are assumed to follow a
bivariate normally distribution across studies
with means (µ1, µ2) and covariance matrix , where represents the variance
of the logit-specificity, the variance of the logit-sensitivity and , the covariance between
logit-sensitivity and logit-specificity.
In this approach, unexplained variability between studies can be incorporated. This variation
in (underlying) sensitivities and specificities between studies can thus be related to remaining
differences in study population, differences in implicit thresholds, or unnoticed variations in index
test protocol. The potential presence of a (negative) correlation between sensitivity and specificity
within studies is addressed by explicitly incorporating this correlation into the analysis, through
modeling the covariance parameter .
In addition to the variability between studies in sensitivity and specificity, there is also varia-
tion due to sampling. As studies differ in size, variability due to chance is more likely to occur in
smaller studies. For this reason, the bivariate model is extended by incorporating the precision
by which sensitivity and specificity have been measured in each study. When comparing T1 vs.
T2+T3+T4, the model evaluates the binomial likelihood of observing n11 correct T1-stages by EUS
or MRI given n1 true T1-stages according to reference standard, and the binomial likelihood of
correctly observing n22+n23+n24+n32+n33+n34+n42+n43+n44 T2, T3 or T4 stages by EUS or MRI
given n2+n3+n4, T2, T3, or T4 stages observed by the reference standard. This means that studies
with a more precise estimate of sensitivity and specificity are given a higher weight in the analysis
of sensitivities and specificities.
This bivariate model can be analyzed using linear and nonlinear mixed model techniques,
which are now widely available in statistical packages (SAS proc Nlmixed).
2. Outcomes of bivariate random-effects approachThe bivariate model produces the following relevant results:
1. Summary estimates of the mean logit sensitivity (µ2) and logit specificity (µ1) with corre-
sponding standard errors. Summary estimates of sensitivity and specificity and their 95% confi-
dence interval can be calculated after anti-logit transformation. These intervals take into account
the heterogeneity beyond chance between studies (random-effects model).
2. The parameters of the bivariate distribution can also be used to obtain a summary Receiver
Operating Characteristics (sROC) curve. The relation between logit-transformed sensitivity and
logit-transformed specificity is given by: logit-sensitivity= α+β*logit-specificity. The slope (β) of this
line equals / , and the intercept (α) equals α = µ2- β*µ1. After anti-logit transformation of
the regression line, a sROC curve is obtained.

���
Chapter 9
3. Other measures derived from sensitivity and specificity can be calculated, such as the diag-
nostic odds ratios (exp[µ1+µ2]), and likelihood ratios:
positive likelihood ratio = (exp[µ2]+exp[µ1+µ2])/(exp[µ2]+1), and
negative likelihood ratio = (exp[µ1]+1)/ (exp[µ1]+exp[µ1+µ2]).
4. Covariates can be added to this bivariate model. These can lead to separate effects on sen-
sitivity and specificity. Net effects on the diagnostic odds ratio are also available. This means that
we can explicitly test whether sensitivity or specificity, or both, differ between two diagnostic tech-
nologies. A detailed technical description of this bivariate model can be found in Reitsma et al [9].
3. Example bivariate random-effects approach We have applied this method to data from a previously published meta-analysis on staging of
rectal cancer: only data sets from 1993-2002 were included: 11 data sets on MRI and 26 data
sets on EUS (17). The EUS and MRI data sets of the studies included in this study are given in ap-
pendix 1. We performed bivariate meta-analyses of three dichotomizations: T1 versus T2+T3+T4,
of T1+T2 versus T3+T4, and T1+T2+T3 versus T4.
Figures 1A-C show the sensitivity and specificity obtained in each study per imaging technique
for the three dichotomizations, with corresponding estimates of sensitivity and specificity ob-
tained by the bivariate approach. In all data sets EUS was found to be more accurate than MRI
(see table 2); by MRI significant numbers of patients were incorrectly categorized as T4, while
they were either T1, T2 or T3 (p < 0.001) compared to EUS.
Table 2. Bivariate pooled sensitivity and specificity estimates for the three dichotomizations
EUS MRI
specificity sensitivity specificity sensitivity
T1 vs. T2+T3+T4 0.86 (0.74-0.93)
0.99 (0.97- 0.995)
0.69 (0.34-0.90)
0.99 (0.96-0.998)
T1+T2 vs. T3+T4 0.84 (0.76-0.89)
0.94 (0.91-0.96)
0.75 (0.57-0.87)
0.91 (0.80-0.96)
T1+T2+T3 vs. T4 0.99 (0.98-0.996)*
0.81(0.68-0.89)
0.97 (0.971-0.976)*
0.79 (0.31-0.97)
Values in parentheses are 95% confidence intervals. * P < 0.001.
For EUS, the Diagnostic Odds Ratios were 488 (95% CI: 145-1646), 75 (95% CI:37-153) and 523
(95% CI:183-1492) for T1 vs. T2+T3+T4, T1+T2 vs. T3+T4, and T1 vs. T2+T3+T4, respectively.
For MRI, the Diagnostic Odds Ratios were 244 (95% CI: 29-2033), 29 (95% CI: 8-105) and 132
(95% CI: 16-1122) respectively.
Both for EUS and MRI, and for all three dichotomizations of the T-system, the random-effects
model fitted the data better than the corresponding fixed-effects model; the Akaike Information
Criterion (AIC) values of the random-effects model were lower. A lower AIC value indicates a
better fit (18).

Multivariate random-effects approach
���
Even in the random-effects model, some parameters of the covariance matrix were difficult to
estimate, as computationally it tooks many iterations. For example, as one can see in Figure 1
(A and B) there was much more between study variations in specificity than in sensitivity when
comparing T1 vs. T1+T2+T3 and T1+T2 vs. T3+T4. As a result, the variance of the logit-sensitivity
( ) was difficult to estimate when comparing T1 vs. T2+T3+T4 and T1+T2 vs. T3+T4. Figure 1C
shows that there was much more variation between studies in sensitivity than in specificity when
comparing T1+T2+T3 vs. T4. Therefore, the variance of the logit-specificity ( ) was difficult to
estimate when comparing T1+T2+T3 vs. T4.
Moreover, the covariance between logit-sensitivity and logit-specificity ( ) was difficult to
estimate in all cases: in none of the analyses we found that the covariance was significantly dif-
ferent from zero.
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Speci�city
Sens
itiv
ity
EUSMRIEstimate EUSEstimate MRI
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Speci�city
Sens
itiv
ity
EUSMRIEstimate EUSEstimate MRI
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Speci�city
Sens
itiv
ity
EUSMRIEstimate EUSEstimate MRI
T1 vs T2+T3+T4 T1+T2 vs T3+T4 T1+T2+T3 vs T4
Figure 1A. The distribution of sensitivity and specificity for T1 vs. T2+T3+T4 Summary sensitivity and specificity for EUS were 0.99 (95% CI:0.97-0.995) and 0.86 (95% CI:0.74-0.93)
Summary sensitivity and specificity for MRI were 0.99 (95% CI: 0.96-0.998) and 0.69 (95% CI: 0.34-0.90)

��0
Chapter 9
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Speci�city
Sens
itiv
ity
EUSMRIEstimate EUSEstimate MRI
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Speci�city
Sens
itiv
ity
EUSMRIEstimate EUSEstimate MRI
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Speci�city
Sens
itiv
ity
EUSMRIEstimate EUSEstimate MRI
T1 vs T2+T3+T4 T1+T2 vs T3+T4 T1+T2+T3 vs T4
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Speci�city
Sens
itiv
ity
EUSMRIEstimate EUSEstimate MRI
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Speci�city
Sens
itiv
ity
EUSMRIEstimate EUSEstimate MRI
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
Speci�city
Sens
itiv
ity
EUSMRIEstimate EUSEstimate MRI
T1 vs T2+T3+T4 T1+T2 vs T3+T4 T1+T2+T3 vs T4
Figure 1B. The distribution of sensitivity and specificity for T1+T2 vs. T3+T4Summary sensitivity and specificity for EUS were 0.94 (95% CI:0.91-0.96) and 0.84 (95% CI:0.76-0.89)
Summary sensitivity and specificity for MRI were 0.91 (95% CI: 0.80-0.96) and 0.75 (95% CI: 0.57-0.87)
Figure 1C. The distribution of sensitivity and specificity for T1+T2+T3 vs. T4Summary sensitivity and specificity for EUS were 0.81 (95% CI:0.68-0.89) and 0.99 (95% CI:0.98-0.996)
Summary sensitivity and specificity for MRI were 0.79 (95% CI: 0.31-0.97) and 0.974 (95% CI: 0.971-0.976)

Multivariate random-effects approach
���
MUlTIVaRIaTe RanDoM-effeCTs aPPRoaCH
In the bivariate random-effects approach three different analyses were required. We extended the
bivariate approach to a multivariate model with which we can discriminate between all T-stages,
and hence report on correct staging, but also on understaging and overstaging of tumor.
1. PrincipleIn this example of rectal cancer staging four T- stages are reported. So in rectal cancer staging, the
entire 4 x 4 table is relevant. Instead of only two proportions, as in the bivariate case (i.e. sensitiv-
ity, and specificity), we now consider all 16 proportions. For any particular study, the 4-by-4 table
will contain 16 proportions (see table 3), where p11 is defined as p11=n11/n1, and p21=n21/n1,
and p12=n12/n2, and so on. Notice that we require that p11+p21+p31+p41=1, and similarly for the
other true T-stages according to reference standard. Hence, there are only 12 “independent”
proportions, because ρ11 + ρ21 + ρ31 + ρ41 =1, similar ρ12 + ρ22 + ρ32 + ρ42 = ρ13 + ρ23 + ρ33 + ρ43 =
ρ14 + ρ24 + ρ34 + ρ44= 1.
Table 3. Example of a 4 by 4 table containing the 16 proportions
Reference standard
T1 T2 T3 T4
EUS or MRI T1 p11 p12 p13 p14
T2 p21 p22 p23 p24
T3 p31 p32 p33 p34
T4 p41 p42 p43 p44
Sum 1 1 1 1
Similar to the bivariate meta-analysis, we assume that these 12 “independent” proportions vary
between studies according to a 12-variate distribution. Here also it is awkward to model pro-
portions, because these may vary only between zero and 1, and therefore we modeled the
“logit”-transformed proportions. The “logit”-transform is slightly more complex when there are
four categories. For the ith true T-stage (according to the reference standard) the proportion
pji of patients scored in T-stage j by EUS or MRI is modeled as , where a4i= 0. In
this notation, we chose the T4 category by EUS or MRI as the reference category (details see
appendix 2).
The 12 transformed parameters aji were assumed to follow a normal distribution with means
(µ11 ,..., µji, ..., µ34), and 12-variate covariance matrix Σ. This covariance matrix is symmetric and

���
Chapter 9
has 12 variances on the diagonal and (12*11/2=) 66 different covariances on the 132 off-diago-
nal cells (see also appendix 2).
Unless many different studies are available it may be difficult to estimate all of these covarianc-
es, and some constraints may be required, for instance all covariances can be set to zero or might
be assumed to be equal. Variation due to chance is incorporated by evaluating the multinomial
likelihood that out of n1 true T1-stages according to the reference standard n11 correct T1-assess-
ments were observed by EUS/MRI, and n21, n31, and n41 incorrect T2-, T3-, and T4-stages. Similar
multinomial likelihoods for the n2, n3, and n4 true T2-, T3-, and T4-stages observed by reference
standard review can be defined. The parameters are estimated by maximizing the product of
these four multinomial likelihoods integrated over the 12-variate normal distribution. This is done
in SAS proc NLmixed. An example of the SAS syntax is provided in the appendix 3.
2. Outcomes multivariate random-effects approachThis multivariate random-effects approach can produce the following relevant results:
1. Summary estimates of the means (µ11 ,..., µji, ..., µ34) will be obtained, and from these all
average proportions (ρji) of the 4-by-4 table can be calculated by anti-“logit” transform.
2. Other measures can be derived from the calculated proportions ρji. Specificity of T1 vs.
T2+T3+T4 can be calculated as ρ11, and sensitivity as (ρ22+ρ23+ρ24+ρ32+ρ33+ρ34+ρ42+ρ43+ρ44)/3,
and sensitivity and specificity of T1+T2 vs. T3+T4, and of T1+T2+T3 vs. T4 can be calculated in a
similar fashion.
3. Accuracy of EUS/MRI staging is defined as (ρ11+ρ22+ρ33+ρ44)/4, and the multivariate diag-
nostic odds ratio may be defined as ρ11*ρ22*ρ33*ρ44/[(1-ρ11)(1-ρ22)(1-ρ33)(1-ρ44)].
3. Example multivariate random-effects approach:We reanalyzed the dataset (EUS and MRI in rectal cancer staging) as previously reported, using
the multivariate random-effects approach. The results obtained by the multivariate approach on
EUS and MRI are listed in tables 4 and 5 respectively.
With the multivariate random-effects approach EUS was found to be more accurate than MRI
in staging (80% [95% CI: 77%-83%] vs. 72% [95% CI: 64%-80%), but the differences were not
statistically significant. MRI seemed more often to overstage than EUS: T1 cancers were more
often seen by MRI as T2 or even T3 (12% vs. 2%), and T2 cancers were more often seen as T3
(42% vs. 28%). With respect to staging T3- and T4-cancers EUS- and MRI-results were more
comparable. The multivariate Odds Ratios were 426 (95% CI: 99-737) and 59 (95% CI: 14-244)
for EUS and MRI respectively.
Both for US and for MRI the AIC values of the random-effects models were significantly lower
than the AIC values of the corresponding fixed-effects models; this points to significant differ-
ences between the studies with respect to T-staging. These differences are illustrated in Figure 2.
The fractions of correctly identified T1-stage cancers by EUS in the different studies are plotted;
there is a considerable difference between studies since the fractions varied between 0.17 and
1.00. The fractions correctly identified T2-, T3-, and T4-stage cancers by EUS, and MRI also varied
considerably between studies. Also the fractions of T1-stage cancers that were classified as T2 by

Multivariate random-effects approach
���
EUS in the different studies are plotted, and here too there were noticeable differences between
studies (the fractions varied between 0.00 and 0.50), and the same applied for almost all other
incorrect classifications.
Table 4. Staging results of EUS obtained by the multivariate approach
T stage on reference standard
T1 T2 T3 T4
T stage on EUS
uT1 0.88 (0.82-0.91)
0.08(0.04-0.10)
0.02 (0-0.03)
0.00(0-0)
uT2 0.10 (0.07-0.15)
0.63 (0.59-0.71)
0.08 (0.05-0.11)
0.01(0-0.04)
uT3 0.02 (0.01-0.04)
0.28 (0.22-0.34)
0.90 (0.89-0.93)
0.20 (0.12-0.28)
uT4 0 (0-0.01)0.01
(0-.015)0.01
(0-0.02)0.78
(0.69-0.87)
Proportions per stage are presented with 95% confidence intervals in parentheses
Table 5. Staging results of MRI obtained by the multivariate approach
T stage on reference standard
T1 T2 T3 T4
T stage on MRI
mT1 0.71 (0.55-0.81)
0.03 (0.01-0.08)
0 (0-0.01)
0 (0-0.005)
mT2 0.17 (0.10-0.29)
0.54 (0.44-0.67)
0.11 (0.07-0.17)
0.02 (0-0.11)
mT3 0.12 (0.05-0.22)
0.42 (0.29-0.52)
0.85 (0.79-0.90)
0.20 (0.07-0.40)
mT4 0 (0-0)
0 (0-0.03)
0.04 (0.02-0.07)
0.78(0.57-0.91)
Proportions per stage are presented with 95% confidence intervals in parentheses
As with the bivariate approach some of the parameters of the multivariate random-effects models
were difficult to estimate, especially the parameters associated with cells with low numbers.
There was, for instance, not a single patient with a T4-cancer who was diagnosed as T1 by EUS/
MRI. The associated parameter was (correctly) estimated to be minus infinity, and the variance
representing differences between studies with respect to this specific cell of the four-by-four
table was estimated as zero. Some other cells contained only 2 patients from two studies, and
the variances of the associated parameters were also estimated as zero. Just as with the previ-
ous bivariate analyses the correlations between the 12 random-effects were small (they varied
between –0.15 and +0.02 for EUS, and –0.16 and +0.13 for MRI).

���
Chapter 9
-1.00 0.50 0.00 0.50 1.00
Proportion
Incorrectly
staged as
T2
Correcly
staged as
T1
-1.00 0.50 0.00 0.50 1.00
Proportion
Incorrectly
staged as
T2
Correcly
staged as
T1
Left: proportions of T1-stage cancers incorrectly classified as T2-stage by EUS; there were notice-able differences between studies, with proportions varied between 0.00 and 0.50.
Right: proportions of correctly identified T1-stage cancers by EUS in the different studies; there is also considerable difference between studies, since the fractions varied between 0.17 and 1.00.
Figure 2 shows the proportions of T1-stage cancers incorrectly classified as T2-stage by EUS and the proportions of correctly identified T1-stage cancers by EUS in the different studies.

Multivariate random-effects approach
���
CoMPaRIson of boTH aPPRoaCHes
The results from the multivariate approach were used to calculate the sensitivity and specificity for
the three dichotomizations. The results are summarized in table 6, which also includes the results
from the repeated bivariate approach.
Table 6. Comparison of the results of the bivariate and multivariate approaches
EUS MRI
multivariate bivariate multivariate bivariate
spec/sens spec/sens spec/sens spec/sens
T1 vs. T2+T3+T4 0.89/0.98 0.86/0.99 0.71/0.97 0.69/0.99
T1+T2 vs. T3+T4 0.87/0.91 0.84/0.94 0.73/0.94 0.75/0.91
T1+T2+T3 vs. T4 0.99/0.81 0.99/0.81 0.98/0.78 0.97/0.79
spec: specificity; sens: sensitivity
DIsCUssIon
The proportions of patients correctly staged, understaged and overstaged for each stage were
obtained by the multivariate approach. EUS was more accurate in correct staging compared
to MRI. When the results of the multivariate model were used to calculate the sensitivity and
specificity for the three dichotomizations (T1 vs. T2+T3+T4, T1+T2 vs. T3+T4, and T1+T2+T3
vs. T4), the findings were comparable with the results of the bivariate analyses for the three
dichotomizations.
For meta-analysis of diagnostic accuracy studies several approaches exist: a bivariate random-
effects approach [7-9] and a hierarchical summary receiver operating characteristic (HSROC)
model [10]. These models are very close related [11].
We extended the bivariate approach to a multivariate approach for analyzing staging data.
This multivariate approach has four additional advantages. Firstly, the multivariate approach en-
tails only a single statistical analysis, and does not require decisions on dichotomizations of data.
This will reduce chance findings by reducing the impact of subjective decisions in the statistical
analysis. Secondly, the multivariate analysis does provide all cell probabilities and the confidence
intervals of all cells of the 4-by-4 table, and with that information it is much easier to pinpoint
the amount of under- and overstaging, and how much studies vary in that aspect. The third
advantage of the multivariate approach is that studies that only report the results of particular
dichotomizations, say T1+T2 vs. T3+T4, can still be used in the meta-analysis, and this applies in
general for all dichotomizations. In contrast, with the repeated bivariate model the study who
only reported the results of T1+T2 vs. T3+T4 cannot be used when analyzing other dichotomiza-
tions. The fourth advantage is that the multivariate analysis requires one single statistical analysis

��6
Chapter 9
and afterwards all these parameters could be used to calculate sensitivity and specificity of any
dichotomizations.
As argued, the multivariate model can be extended with covariates, and these can be incor-
porated in several ways: (i) the regression parameters may be fixed or vary between the studies,
and (ii) the regression parameters may be different but they may also be similar for the three
possible dichotomizations, T1 vs. T2+T3+T4, T1+T2 vs. T3+T4, and T1+T2+T3 vs. T4), since the
staging-system is likely measured on an ordinal scale.
The calculations were performed in the SAS system with the NLmixed procedure. We found
the program to be robust, but a severe limitation was that the calculations took a very long time
for the multivariate analyses. The calculations took 48 hours on a PC, or more. We therefore
implemented the multivariate model in the Winbugs program which uses a Bayesian algorithm.
This took much less computing time, typically about two hours. Another advantage of the Bayes-
ian approach is that it is much easier to calculate the confidence intervals of the probabilities as
reported in tables 4 and 5. The Winbugs-implementation can be obtained from the first author.
From the clinical point of view, understaging and overstaging are important issues, as the
choice of the treatment is mostly influenced by the invasiveness of the tumor. For example,
patients with T1-stage rectal cancer will mostly undergo transanal endoscopic microsurgery
(TEM), a minimally invasive procedure [19, 20], whereas patients with more advanced (T2, T3
and T4-stages), in general, undergo total mesorectal excision (TME), with or without (extended)
radiotherapy [21-23]. Another example, in cervical cancer staging, overstaging of a T2A tumor
and understaging of a T2B tumor would lead to inappropriate treatment of patients. Patients
with early stage tumor in general undergo surgery, while patients with advanced stage tumor will
undergo more complex treatment [24-27].
There are numerous types of cancer in which T-stages (e.g. esophageal cancer, prostate can-
cer) are important for selecting the appropriate therapeutic procedures and accurate staging is
required [28-33]. In the literature, imaging data are presented per stage and we feel these should
be summarized properly, without dichotomizing data or selecting data in order to calculate sen-
sitivity and specificity [34, 35]. The multivariate random-effects approach described above could
also be used to summarize data on lymph node status (N-status), as these results are also reported
per stage, for example N0, N1, N2 and N3 stages in lung cancer [36].
In conclusion, for summarizing ordinal or nominal data in diagnostic accuracy studies, this
multivariate random-effects approach is a very helpful meta-analytic method. Because of the
increased interest in meta-analysis for evidence-based guideline development, an adequate statis-
tical analysis should be used to summarize the staging findings.

Multivariate random-effects approach
��7
References
1. Cook DJ, Greengold NL, Ellrodt AG, Weingarten SR. The relation between systematic reviews and practice guidelines. Ann Intern Med 1997;127:210-216.
2. Cook DJ, Mulrow CD, Haynes RB. Systematic reviews: synthesis of best evidence for clinical decisions. Ann Intern Med 1997;126:376-380.
3. Gallagher EJ. Systematic reviews: a logical methodological extension of evidence-based medicine. Acad Emerg Med 1999;6:1255-1260.
4. Deville WL, Buntinx F, van der Windt DA, et al. Didactic guidelines for conducting systematic reviews of studies evaluating the accuracy of diagnostic tests. 2001. Knottnerus JA, editor. The evidence Base of diagnosis. London: BMJ Publishing Group.
5. Deeks JJ. Systematic reviews in health care: Systematic reviews of evaluations of diagnostic and screening tests. BMJ 2001;323:157-162.
6. Khan KS. Systematic reviews of diagnostic tests: a guide to methods and application. Best Pract Res Clin Obstet Gynaecol 2005;19(1):37-46
7. van Houwelingen HC, Arends LR, Stijnen T. Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med 2002;21:589-624.
8. Arends LR, Voko Z, Stijnen T. Combining multiple outcome measures in a meta-analysis: an application. Stat Med 2003;22:1335-1353.
9. Reitsma JB, Glas AS, Rutjes AW, Scholten RJ, Bossuyt PM, Zwinderman AH. Bivariate analysis of sen-sitivity and specificity produces informative summary measures in diagnostic reviews. J Clin Epidemiol 2005;58:982-990.
10. Rutter CM, Gatsonis CA. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat Med 2001;20:2865-2884.
11. Harbord RM, Deeks JJ, Egger M, Whiting P, Sterne JA. A unification of models for meta-analysis of diag-nostic accuracy studies. Biostatistics 2006
12. Steele SR, Martin MJ, Place RJ. Flexible endorectal ultrasound for predicting pathologic stage of rectal cancers. Am J Surg 2002;184:126-130.
13. Garcia-Aguilar J, Pollack J, Lee SH, et al. Accuracy of endorectal ultrasonography in preoperative staging of rectal tumors. Dis Colon Rectum 2002;45:10-15.
14. Herzog U, von Flue M, Tondelli P, Schuppisser JP. How accurate is endorectal ultrasound in the preopera-tive staging of rectal cancer? Dis Colon Rectum 1993;36:127-134.
15. Hadfield MB, Nicholson AA, MacDonald AW, Farouk R, Lee PW, Duthie GS et al. Preoperative staging of rectal carcinoma by magnetic resonance imaging with a pelvic phased-array coil. Br J Surg 1997;84:529-531.
16. Drew PJ, Farouk R, Turnbull LW, Ward SC, Hartley JE, Monson JR. Preoperative magnetic resonance stag-ing of rectal cancer with an endorectal coil and dynamic gadolinium enhancement. Br J Surg 1999;86:250-254.
17. Bipat S, Glas AS, Slors FJ, Zwinderman AH, Bossuyt PM, Stoker J. Rectal cancer: local staging and assess-ment of lymph node involvement with endoluminal US, CT, and MR imaging--a meta-analysis. Radiology 2004;232:773-783.
18. Akaike, H. A new look at the Statistical Model Identification. IEEE Trans Automat Control 1974; 19:716-23
19. Langer C, Liersch T, Markus P, et al. Transanal endoscopic microsurgery (TEM) for minimally invasive resec-tion of rectal adenomas and “Low-risk” carcinomas (uT1, G1 - 2). Z Gastroenterol 2002;40:67-72.
20. Burghardt J, Buess G. Transanal endoscopic microsurgery (TEM): a new technique and development dur-ing a time period of 20 years. Surg Technol Int 2005;14:131-137
21. Marijnen CA, Nagtegaal ID, Kapiteijn E, et al. Radiotherapy does not compensate for positive resection margins in rectal cancer patients: report of a multicenter randomized trial. Int J Radiat Oncol Biol Phys 2003;55:1311-1320.

���
Chapter 9
22. Goldberg S, Klas JV. Total mesorectal excision in the treatment of rectal cancer: a view from the USA. Semin Surg Oncol 1998;15:87-90.
23. Wiig JN, Carlsen E, Soreide O. Mesorectal excision for rectal cancer: a view from Europe. Semin Surg Oncol 1998;15:78-86.
24. Loizzi V, Cormio G, Loverro G, Selvaggi L, Disaia PJ, Cappuccini F. Chemoradiation: A new approach for the treatment of cervical cancer. Int J Gynecol Cancer 2003;13:580-586.
25. Panici PB, Cutillo G, Angioli R. Modulation of surgery in early invasive cervical cancer. Crit Rev Oncol Hematol 2003;48:263-270.
26. duPont NC, Monk BJ. Chemotherapy in the management of cervical carcinoma. Clin Adv Hematol Oncol 2006;4:279-286.
27. Duenas-Gonzalez A, Cetina L, Mariscal I, de la GJ. Modern management of locally advanced cervical carcinoma. Cancer Treat Rev 2003;29:389-399.
28. Kelsen DP, Ginsberg R, Pajak TF, et al. Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med 1998;339:1979-1984.
29. Hulscher JB, van Sandick JW, de Boer AG, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med 2002;347:1662-1669.
30. Hulscher JB, Tijssen JG, Obertop H, van Lanschot JJ. Transthoracic versus transhiatal resection for carci-noma of the esophagus: a meta-analysis. Ann Thorac Surg 2001;72:306-313.
31. Mazhar D, Ngan S, Waxman J. Improving outcomes in early prostate cancer: Part II--neoadjuvant treat-ment. BJU Int 2006;98:731-734.
32. Mazhar D, Ngan S, Waxman J. Improving outcomes in early prostate cancer: Part I--adjuvant treatment. BJU Int 2006;98:725-730.
33. Pisansky TM. External-beam radiotherapy for localized prostate cancer. N Engl J Med 2006;355:1583-1591.
34. Engelbrecht MR, Jager GJ, Laheij RJ, Verbeek AL, van Lier HJ, Barentsz JO. Local staging of prostate cancer using magnetic resonance imaging: a meta-analysis. Eur Radiol 2002;12:2294-2302.
35. van Westreenen HL, Westerterp M, Bossuyt PM, et al. Systematic review of the staging performance of 18F-fluorodeoxyglucose positron emission tomography in esophageal cancer. J Clin Oncol 2004;22:3805-3812.
36. Cerfolio RJ, Ojha B, Bryant AS, Raghuveer V, Mountz JM, Bartolucci AA. The accuracy of integrated PET-CT compared with dedicated PET alone for the staging of patients with nonsmall cell lung cancer. Ann Thorac Surg 2004;78:1017-1023.

Multivariate random-effects approach
���
aPPenDIX 1
Numbers of patients with EUS T-stages and T-stages obtained by reference standard
Study T1 by reference standard
T2 by reference standard
T3 by reference standard
T4 by reference standard
EUS T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4
Herzog 1993 19 3 0 0 1 17 8 0 0 0 67 0 0 0 0 2
Nielsen 1993 0 0 0 0 0 2 3 0 0 0 14 0 0 0 2 7
Houvenaeghel 1993 2 3 1 1 2 5 1 0 2 2 12 0 0 0 0 1
Hulsmans 1994 1 0 2 0 1 4 16 1 0 1 25 0 0 0 1 3
Kim 1994 1 0 0 0 0 3 1 0 0 1 25 1 0 0 1 1
Adams 1995 59 0 0 0 1 2 0 0 0 0 0 0 0 0 0 0
Starck 1995 1 1 0 0 0 8 1 0 0 2 21 0 0 0 0 0
Fedyaev 1995 0 0 0 0 0 30 3 0 0 2 41 2 0 0 3 28
Kaneko 1996 3 1 0 0 0 9 1 0 0 3 21 0 0 0 0 0
Pegios 1996 6 1 0 0 0 13 3 0 0 3 51 1 0 0 7 15
Osti 1997 3 0 0 0 0 11 7 0 0 4 32 0 0 0 0 6
Sailer 1997 43 10 0 0 1 12 16 0 0 1 61 5 0 1 2 8
Hunerbein 1997 17 1 0 0 0 19 4 0 1 3 18 0 0 1 0 6
Maier 1997 4 2 0 0 0 15 6 0 0 2 45 0 0 0 4 2
Akasu 1997 32 1 1 0 4 19 11 0 0 4 78 2 0 0 3 9
Massari 1998 13 0 1 0 0 16 2 0 2 2 32 0 0 0 0 7
Scialpi 1999 0 0 0 0 0 0 0 0 0 0 16 1 0 0 1 3
Barbaro 1999 0 0 0 0 0 9 1 0 0 1 15 0 0 0 0 2
Carmody 2000 11 4 0 0 1 7 2 0 0 0 11 0 0 0 0 0
Gualdi 2000 2 0 0 0 0 5 5 0 0 1 13 0 0 0 0 0
Blomqvist 2000 1 1 3 1 4 3 4 0 0 4 25 0 0 0 0 3
Akahoshi 2000 9 1 0 0 0 2 1 0 0 5 20 0 0 0 0 1
Akasu 2000 74 4 2 0 8 40 26 0 0 6 149 0 0 0 0 0
Hunerbein 2000 16 0 0 0 0 10 1 0 0 1 1 0 0 0 0 1
Steele 2002 5 5 2 0 0 7 5 1 0 3 12 1 0 0 3 1
Garcia-Aquilar 2002 226 24 0 0 24 104 37 2 3 25 92 2 0 0 2 4

�60
Chapter 9
Numbers of patients with MRI T-stages and T-stages obtained by reference standard
Study T1 by reference standard
T2 by reference standard
T3 by reference standard
T4 by reference standard
MRI T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4
Okizuka 1993 11 1 1 0 2 3 1 0 0 5 7 0 0 0 0 2
Schnall 1994 8 3 0 0 0 6 4 0 0 0 15 0 0 0 0 0
Murano 1995 2 1 2 0 0 3 2 0 0 2 9 0 0 0 0 1
Pegios 1996 16 1 0 0 0 5 1 0 0 0 4 0 0 0 0 2
Hadfield 1997 2 3 2 0 0 2 2 0 0 6 17 3 0 0 1 0
Vogl 1997 5 1 0 0 0 4 1 0 0 0 5 0 0 0 0 4
Drew 1999 0 2 2 0 1 2 10 1 0 2 7 1 0 0 1 0
Gualdi 2000 2 0 0 0 0 6 4 0 0 0 14 0 0 0 0 0
Blomqvist 2000 0 2 4 0 0 4 7 0 1 2 25 2 0 0 3 0
Kim 2000 3 1 0 0 0 20 17 0 0 15 141 6 0 1 1 12
Hunerbein 2000 14 0 0 0 1 9 1 0 0 0 2 0 0 0 0 1

Multivariate random-effects approach
�6�
aPPenDIX 2
The proportions, ρ11, ρ21, ρ31, ρ41, are transformed into:
ρ11 = , ρ21 = ,
ρ31 = , ρ41 = ,
depending on the parameters: a11, a21, a31. The proportions (ρ12, ρ22, ρ32, ρ42), (ρ13, ρ23, ρ33, ρ43)
and (ρ14, ρ24, ρ34, ρ44), are transformed similarly depending on parameters (a12, a22, a32), (a13, a23,
a33) and (a14, a24, a34) respectively. We will assume that in our model, these 12 parameters (a11,
a21, a31, a12, a22, a32, a13, a23, a33, a14, a24, a34) follow a 12–variate normal distribution with means
(µ11, µ21, µ31, µ12, µ22, µ32, µ13, µ23, µ33, µ14, µ24, µ34) and covariance matrix ∑.
This covariance matrix is symmetric and has therefore 12 variances on the diagonal and (12*11/2)
66 different covariances on the 132 off-diagonal cells; the variances representing differences
between studies; σ5,8 representing covariance between parameters 5 and 8, similarly σ10, 12 rep-
resenting the covariance between parameters 10 and 12.

�6�
Chapter 9
aPPenDIX 3
Technical description of the model in which covariances are assumed to be zero. A copy of the
full SAS program is available on request from the first author.
proc NLmixed data=data df=1000;
p11=exp(a11)/(1+exp(a11)+exp(a21)+ exp(a31));
p21=exp(a21)/(1+exp(a11)+exp(a21)+ exp(a31));
p31=exp(a31)/(1+exp(a11)+exp(a21)+ exp(a31));
p41=1 /(1+exp(a11)+exp(a21)+ exp(a31));
p12=exp(a12)/(1+exp(a12)+exp(a22)+ exp(a32));
p22=exp(a22)/(1+exp(a12)+exp(a22)+ exp(a32));
p32=exp(a32)/(1+exp(a12)+exp(a22)+ exp(a32));
p42=1 /(1+exp(a12)+exp(a22)+ exp(a32));
p13=exp(a13)/(1+exp(a13)+exp(a23)+ exp(a33));
p23=exp(a23)/(1+exp(a13)+exp(a23)+ exp(a33));
p33=exp(a33)/(1+exp(a13)+exp(a23)+ exp(a33));
p43=1 /(1+exp(a13)+exp(a23)+ exp(a33));
p14=exp(a14)/(1+exp(a14)+exp(a24)+ exp(a34));
p24=exp(a24)/(1+exp(a14)+exp(a24)+ exp(a34));
p34=exp(a34)/(1+exp(a14)+exp(a24)+ exp(a34));
p44=1 /(1+exp(a14)+exp(a24)+ exp(a34));
ll = n11*log(p11)+n12*log(p12)+n13*log(p13)+n14*log(p14)+
n21*log(p21)+n22*log(p22)+n23*log(p23)+n24*log(p24)+
n31*log(p31)+n32*log(p32)+n33*log(p33)+n34*log(p34)+
n41*log(p41)+n42*log(p42)+n43*log(p43)+n44*log(p44);
model n11 ~ general(ll);
random a11 a21 a31 a12 a22 a32 a13 a23 a33 a14 a24 a34 ~
normal ([µ11, µ21, µ31, µ12, µ22, µ32, µ13, µ23, µ33, µ14, µ24, µ34],
[s1,0,s2,0,0,s3,0,0,0,s4,0,0,0,0,s5,0,0,0,0,0,s6,0,0,0,0,0,0,s7,0,0,0,0,0,0,0,s8,0,0,0,0,0,0,0,0,s
9,0,0,0,0,0,0,0,0,0,s10,0,0,0,0,0,0,0,0,0,0,s11,0,0,0,0,0,0,0,0,0,0,0,s12]) subject=nr;
run;
Data are entered into the SAS system as they are given in appendix 1: n11, n21, n31, and 41
denote the numbers of patients with T1-stage cancer identified by EUS/MRI (separately) as T1,
T2, T3, or T4, respectively, and n12, n22, n32, n42 are the numbers of patients with T2-stage
cancer but identified as T1, T2, T3, or T4 by EUS/MRI.

Multivariate random-effects approach
�6�
The variable ll denotes the sum of the four multinomial log likelihoods associated with the true
T1-, T2-, T3-, and T4-stages, and the variables p11 .... p44 are the associated cell probabilities of
the 4-by-4 table. The parameters a11 ... a34 are the “logit”-transformed parameters of the cell
probabilities, which are assumed to be normally distributed with means µ11 ... µ34, and variances
s1 ... s12. In the example above all covariances are fixed to be zero, but this is not a necessary
requirement. We used different reference categories than in the main text of the paper; here we
used the most prevalent categories as references.

�6�
Chapter 9
Reference appendix 1
1. Herzog U, von Flue M, Tondelli P, Schuppisser JP. How accurate is endorectal ultrasound in the preopera-tive staging of rectal cancer? Dis Colon Rectum 1993;36:127-134.
2. Nielsen MB, Pedersen JF, Christiansen J. Rectal endosonography in the evaluation of stenotic rectal tumors. Dis Colon Rectum 1993;36:275-279.
3. Houvenaeghel G, Delpero JR, Giovannini M, et al. Staging of rectal cancer: a prospective study of digital ex-amination and endosonography before and after preoperative radiotherapy. Acta Chir Belg 1993;93:164-168.
4. Hulsmans FJ, Tio TL, Fockens P, Bosma A, Tytgat GN. Assessment of tumor infiltration depth in rectal cancer with transrectal sonography: caution is necessary. Radiology 1994;190:715-720.
5. Kim NK, Choi JS, Sohn SK, Min JS. Transrectal ultrasonography in preoperative staging of rectal cancer. Yonsei Med J 1994;35:396-403.
6. Adams WJ, Wong WD. Endorectal ultrasonic detection of malignancy within rectal villous lesions. Dis Colon Rectum 1995;38:1093-1096.
7. Starck M, Bohe M, Fork FT, Lindstrom C, Sjoberg S. Endoluminal ultrasound and low-field magnetic reso-nance imaging are superior to clinical examination in the preoperative staging of rectal cancer. Eur J Surg 1995;161:841-845.
8. Fedyaev EB, Volkova EA, Kuznetsova EE. Transrectal and transvaginal ultrasonography in the preoperative staging of rectal carcinoma. Eur J Radiol 1995;20:35-38.
9. Kaneko K, Boku N, Hosokawa K, et al. Diagnostic utility of endoscopic ultrasonography for preoperative rectal cancer staging estimation. Jpn J Clin Oncol 1996;26:30-35.
10. Pegios W, Vogl J, Mack MG, et al. MRI diagnosis and staging of rectal carcinoma. Abdom Imaging 1996;21:211-218.
11 Osti MF, Padovan FS, Pirolli C, et al. Comparison between transrectal ultrasonography and computed to-mography with rectal inflation of gas in preoperative staging of lower rectal cancer. Eur Radiol 1997;7:26-30.
12. Sailer M, Leppert R, Kraemer M, Fuchs KH, Thiede A. The value of endorectal ultrasound in the assessment of adenomas, T1- and T2-carcinomas. Int J Colorectal Dis 1997;12:214-219.
13. Hunerbein M, Schlag PM. Three-dimensional endosonography for staging of rectal cancer. Ann Surg 1997;225:432-438.
14. Maier AG, Barton PP, Neuhold NR, Herbst F, Teleky BK, Lechner GL. Peritumoral tissue reaction at tran-srectal US as a possible cause of overstaging in rectal cancer: histopathologic correlation. Radiology 1997;203:785-789.
15. Akasu T, Sugihara K, Moriya Y, Fujita S. Limitations and pitfalls of transrectal ultrasonography for staging of rectal cancer. Dis Colon Rectum 1997;40(10 Suppl):S10-S15.
16. Massari M, De Simone M, Cioffi U, Rosso L, Chiarelli M, Gabrielli F. Value and limits of endorectal ultraso-nography for preoperative staging of rectal carcinoma. Surg Laparosc Endosc 1998;8:438-444.
17. Scialpi M, Rotondo A, Angelelli G. Water enema transvaginal ultrasound for local staging of stenotic rectal carcinoma. Abdom Imaging 1999;24:132-136.
18. Barbaro B, Schulsinger A, Valentini V, Marano P, Rotman M. The accuracy of transrectal ultrasound in predicting the pathological stage of low-lying rectal cancer after preoperative chemoradiation therapy. Int J Radiat Oncol Biol Phys 1999;43:1043-1047.
19. Carmody BJ, Otchy DP. Learning curve of transrectal ultrasound. Dis Colon Rectum 2000;43:193-197.
20. Gualdi GF, Casciani E, Guadalaxara A, d’Orta C, Polettini E, Pappalardo G. Local staging of rectal cancer with transrectal ultrasound and endorectal magnetic resonance imaging: comparison with histologic find-ings. Dis Colon Rectum 2000;43:338-345.
21. Blomqvist L, Machado M, Rubio C, et al. Rectal tumour staging: MR imaging using pelvic phased-array and endorectal coils vs endoscopic ultrasonography. Eur Radiol 2000;10:653-660.

Multivariate random-effects approach
�6�
22. Akahoshi K, Kondoh A, Nagaie T, et al. Preoperative staging of rectal cancer using a 7.5 MHz front-loading US probe. Gastrointest Endosc 2000;52:529-534.
23. Akasu T, Kondo H, Moriya Y, et al. Endorectal ultrasonography and treatment of early stage rectal cancer. World J Surg 2000;24:1061-1068.
24. Hunerbein M, Pegios W, Rau B, Vogl TJ, Felix R, Schlag PM. Prospective comparison of endorectal ultra-sound, three-dimensional endorectal ultrasound, and endorectal MRI in the preoperative evaluation of rectal tumors. Preliminary results. Surg Endosc 2000;14:1005-1009.
25. Steele SR, Martin MJ, Place RJ. Flexible endorectal ultrasound for predicting pathologic stage of rectal cancers. Am J Surg 2002;184:126-130.
26. Garcia-Aguilar J, Pollack J, Lee SH, et al. Accuracy of endorectal ultrasonography in preoperative staging of rectal tumors. Dis Colon Rectum 2002;45:10-15.
27. Okizuka H, Sugimura K, Ishida T. Preoperative local staging of rectal carcinoma with MR imaging and a rectal balloon. J Magn Reson Imaging 1993;3:329-335.
28. Schnall MD, Furth EE, Rosato EF, Kressel HY. Rectal tumor stage: correlation of endorectal MR imaging and pathologic findings. Radiology 1994;190:709-714.
29. Murano A, Sasaki F, Kido C, et al. Endoscopic MRI using 3D-spoiled GRASS (SPGR) sequence for local staging of rectal carcinoma. J Comput Assist Tomogr 1995;19:586-591.
30. Hadfield MB, Nicholson AA, MacDonald AW, et al. Preoperative staging of rectal carcinoma by magnetic resonance imaging with a pelvic phased-array coil. Br J Surg 1997 April;84(4):529-31.
31. Vogl TJ, Pegios W, Mack MG, et al. Accuracy of staging rectal tumors with contrast-enhanced transrectal MR imaging. AJR Am J Roentgenol 1997;168:1427-1434.
32. Drew PJ, Farouk R, Turnbull LW, Ward SC, Hartley JE, Monson JR. Preoperative magnetic resonance stag-ing of rectal cancer with an endorectal coil and dynamic gadolinium enhancement. Br J Surg 1999;86:250-254.
33. Kim NK, Kim MJ, Park JK, Park SI, Min JS. Preoperative staging of rectal cancer with MRI: accuracy and clinical usefulness. Ann Surg Oncol 2000;7:732-737.

2C h a p t e r

Summary and Conclusions

�6�
summary and Conclusions
sUMMaRY
The aim of the work summarized in this thesis was to collect primary findings and to summarize
evidence for diagnosing and staging of several gynecological and gastrointestinal malignancies by
means of either ultrasonography (US), computed tomography (CT), magnetic resonance imaging
(MRI) or positron emission tomography with 18-fluorodeoxyglucose (FDG-PET). The results of our
analyses can be used for making evidence-based recommendations for clinical practice.
In chapter 2 lymph nodes detection by MRI in patients with vulva tumor was evaluated. As
lymphatic spread remains an important prognostic factor in these patients and no uniform results
are described in the literature, two observers retrospectively analyzed the accuracy of MRI for
lymph node detection in 60 patients with vulva carcinoma. The MRI findings were compared
to pathological results of sentinel node procedures or lymphadenectomy specimen. Sensitivity,
specificity, positive and negative predictive values were 52%, 85%, 46%, and 87% for observer
1 and 52% 89%, 52%, and 89% for observer 2.
We concluded that at this stage no role exists for standard MRI in evaluating lymph node
involvement in patients with vulva carcinoma.
In chapter 3 we performed a systematic review on the diagnostic performance of CT and
MRI in staging of cervical carcinoma. The diagnostic performance of both modalities in the evalu-
ation of parametrial invasion, bladder and rectum invasion, and lymph node involvement were
reported.
Sensitivity estimates for parametrial invasion were 74% (95% CI: 68%-79%) for MRI and 55%
(95% CI: 44%-66%) for CT, and for lymph node involvement, 60% (95% CI: 52%-68%) and 43%
(95% CI: 37%-57%), respectively. MRI and CT had comparable specificities for parametrial inva-
sion and lymph node involvement.
For bladder invasion and rectum invasion the sensitivities for MRI were 75% (95% CI: 66%-
83%) and 71% (95% CI: 53%-83%), respectively, both higher (not significant) compared than for
CT. The specificity in evaluating bladder invasion for MRI was significantly higher compared with
CT: 91% (95% CI: 83%-95%) for MRI and 73% (95% CI: 52%-87%) for CT. The specificities for
rectum invasion were comparable.
On the basis of our systematic review, the following clinical practice guidelines could be for-
mulated for staging cervical carcinoma. In clinically early-stage cancer, the prevalence of disease
spreading outside the cervix is low and therefore the additional value of MRI is limited. In more
advanced disease, MRI can play an important role, as clinical staging has significant limitations in
advanced disease.
In chapter 4 we compared the diagnostic value of endoluminal US (EUS), CT and MRI for local
staging and assessment of lymph node involvement in patients with rectal cancer by means of a
meta-analysis.
For muscularis propria invasion, EUS and MRI had similar sensitivities. Specificities were 86%
(95% CI: 80%-90%) and 69% (95% CI: 52%-82%) respectively. For perirectal tissue invasion,
sensitivity of EUS was 90% (95% CI: 88%-92%); significantly higher than that of CT (79% [95%
CI: 74%-84%]) and that of MRI (82% [95% CI: 74%-87%]). Specificities were comparable. For

summary and Conclusions
�6�
adjacent organ invasion and lymph node involvement, estimates for EUS, CT, and MRI were
comparable.
The summary ROC curve for EUS in detecting perirectal tissue invasion showed better diagnos-
tic accuracy than for CT and MRI. Summary ROC curves for lymph node involvement showed no
differences in accuracy.
On the basis of the results of this meta-analysis, EUS seems to be a better diagnostic imaging
test for local staging than CT and MRI. However, EUS cannot identify the mesorectal fascia and
possible tumor involvement, while this is possible with MRI. Mesorectal fascia identification is im-
portant in determining the spread of tumors in patients considered for total mesorectal excision.
EUS could be helpful in selecting patients for available therapeutic strategies, such as transanal
endoscopic microsurgery. The identification of lymph nodes with EUS, CT, and MRI remains a
major point of concern.
In chapter 5 we systematically reviewed the evidence on the diagnostic value of US, CT and
MRI for diagnosis and determining resectability of pancreatic adenocarcinoma. The aim of this
study was to obtain summary estimates of US, conventional CT, helical CT, and MRI for the diag-
nosis and determination of resectability of pancreatic adenocarcinoma.
For diagnosis, sensitivities of US, conventional CT, helical CT, and MRI were 76%, 86%, 91%,
and 84% and specificities were 75%, 79%, 85%, and 82%, respectively. Sensitivities for MRI and
US were significantly lower than with helical CT (P = 0.04 and P = 0.0001).
For determining resectability, sensitivities of US, conventional CT, helical CT, and MRI were
83%, 82%, 81%, and 82% and specificities were 63%, 76%, 82%, and 78% respectively. Specific-
ity of US was significantly lower than with helical CT (P = 0.011).
Based on the high sensitivity for diagnosis of helical CT compared with MRI and US and the
high specificity for resectability compared with US, we feel that helical CT is preferable as imaging
modality for the diagnosis and assessment of resectability of pancreatic adenocarcinoma.
In chapter 6 we summarized the findings of a survey performed on the management of
patients with colorectal liver metastases in the Netherlands. In this survey we documented the
extent of variation in diagnosis and treatment strategies. This survey showed substantial variation
in the diagnostic and therapeutic work-up of patients with colorectal liver metastases. This varia-
tion reflects either under- or over-utilization of diagnosis and treatment options. Evidence-based
guidelines taking into account the available evidence, experience and availability could solve this
variation (presented in chapter 8).
In chapter 7 the results of a meta-analysis on the diagnostic accuracy of CT, MRI and FDG-PET
for detection of colorectal liver metastases were presented. The aim of this study was to obtain
estimates of sensitivity of CT, MRI and FDG-PET for detection of colorectal liver metastases on
per-patient and per-lesion basis.
Sensitivity estimates on a per-patient basis for non-helical CT, helical CT, 1.5 T MRI, and FDG-PET
were 60.2%, 64.7%, 75.8%, and 94.6%, respectively; FDG-PET was the most accurate modality.
On a per-lesion basis, sensitivity estimates for non-helical CT, helical CT, 1.0 T MRI, 1.5 T MRI,
and FDG-PET were 52.3%, 63.8%, 66.1%, 64.4%, and 75.9%, respectively; non-helical CT had
the lowest sensitivity. Estimates of gadolinium-enhanced MRI and superparamagnetic iron oxide

�70
summary and Conclusions
(SPIO)-enhanced MRI were significantly better, compared with non-enhanced MRI (P = 0.019 and
P < 0.001, respectively) and with helical CT with ≤ 45 g of iodine (P = 0.02 and P < 0.001, respec-
tively). For lesions ≥ 1 cm, SPIO-enhanced MRI was the most accurate modality (P < 0.001).
The choice between helical CT performed with > 45 g of iodine and MRI with a gadolinium-
based contrast agent or SPIO should also depend on availability and expertise and not on diag-
nostic accuracy only. The role of FDG-PET for the detection of colorectal liver metastases at this
moment is limited. FDG-PET will therefore mainly be used as an additional imaging modality for
detection of extrahepatic disease.
In chapter 8 we summarized an evidence-based guideline developed for diagnosis and treat-
ment of patients with colorectal liver metastases. The most important recommendations for
diagnosis and treatment are:
For synchronous liver metastases, imaging should comprise spiral CT or MRI. For evaluation of
lung metastases, imaging can be limited to chest radiography.
For detection of metachronous liver metastases, ultrasonography could be performed as initial
modality, if the entire liver is adequate visualized. In doubtful cases or potential candidates for
surgery, CT or MRI should be performed as additional imaging.
For evaluation of extrahepatic disease, abdominal and chest CT could be performed. FDG-PET
could be valuable in patients selected for surgery based on CT (liver/abdomen/chest), for identify-
ing extrahepatic disease.
Surgical resection is the treatment of choice with a 5-years survival of 30%-40%. Variation in
selection criteria for surgery is caused by equivocal literature data concerning surgical margins
<10 mm, presence of extrahepatic disease and the role of (neo)-adjuvant therapy. A substantial
variation also exists in surgical techniques (e.g. anatomic vs. non-anatomic). To minimize variation
in selection criteria, selection should be performed according to the guideline and preferable in
qualified centers.
If resection is not possible, due to extensive disease, palliative chemotherapy is recommended.
Systemic chemotherapy with fluoropyrimidine first-line chemotherapy (5-FU/Leucovorin) com-
bined with irinotecan or oxaliplatin should be considered as standard regimens.
Radiofrequency ablation, isolated hepatic perfusion, portal vein embolization, and intra-arterial
chemotherapy are considered experimental and should only be performed as part of a clinical
research protocol.
In chapter 9 we described a new multivariate random-effects approach for meta-analysis of
staging data, one that allows calculating estimates of correct staging, under and overstaging.
In cancer, the differentiation between disease and non-disease is not the only issue. Correct
staging, understaging and overstaging of the tumor are equally important. When using existing
meta-analytic approaches, such as the bivariate random-effects approach, data should be di-
chotomized for calculation of sensitivity and specificity. In a four category T-stage staging system,
three dichotomies can be made: T1 vs. T2+T3+T4, T1+T2 vs. T3+T4 and T1+T2+T3 vs. T4). These
dichotomies lose information on understaging and overstaging.
By using above mentioned multivariate random-effects approach, estimates of correct staging,
understaging and overstaging were calculated. We also calculated summary estimates of sensitiv-

summary and Conclusions
�7�
ity and specificity for the three dichotomizations. For all these aims a subset of data sets previously
analyzed by the bivariate approach for comparing Endoluminal US (EUS) and MRI in staging rectal
cancer was used (chapter 4).
EUS was more accurate than MRI in staging (80% vs. 72%), but the differences were not
statistically significant. MRI especially seemed to more often overstage than EUS: T1 cancers were
more often seen by MRI as T2 or even T3 (12% vs. 2%), and T2 cancers were more often seen as
T3 (42% vs. 28%).
The sensitivity and specificity estimates of EUS or MRI for the three dichotomizations, calcu-
lated from the results of the multivariate approach, were comparable with the sensitivity and
specificity estimates of EUS or MRI obtained by the bivariate random-effects analyses.
We believe that the multivariate random-effects approach can be a very helpful, informative
and precise meta-analytic method for summarizing ordinal or nominal data in diagnostic accuracy
studies.
ConClUsIons anD fUTURe ReseaRCH
The work in this thesis illustrates that performing diagnostic studies of sufficient methodological
quality and systematically reviewing the literature are both valuable and essential tools in making
evidence-based recommendations for clinical practice.
MethodologyIn general, systematic reviews of diagnostic accuracy studies go through a number of key stages:
defining a clinical question, performing comprehensive literature search, defining explicit selec-
tion criteria to identify relevant studies, assessing the methodological quality of included studies,
assessing data on the diagnostic accuracy, explore differences among study results, and synthe-
size study results, if possible in a quantitative way through meta-analysis. At each level various
problems may arise, e.g. several studies may never appear in print (publication bias), studies may
be selectively included in reference lists, their methodological quality may be suboptimal or the
papers suffer from incomplete data reporting. Although advanced statistical approaches exist to
overcome some of these problems, a number of issues in analyzing the evidence need careful
consideration:
Like any other systematic review, systematic reviews of diagnostic accuracy studies are threat-
ened by publication-bias. In general, funnel plots are used to investigate publication bias in ran-
domized controlled trials; the log odds ratio is plotted against the sample size or precision (recip-
rocal of the standard error). Various statistical tests such as Begg’s rank correlation [1], Egger’s
regression test [2] and Macaskill’s regression [3] have been proposed to objectively study plot
asymmetry. Song et al [4] supposed that the funnel plots and Begg’s and Egger’s tests could also
be used for reviews of diagnostic tests. Deeks et al [5] recently however reported that the Begg’s,
Egger’s and Macaskill’s tests are misleading if used in reviews of diagnostics accuracy studies and
proposed a new approach: effective sample size funnel plots and associated regression tests for

�7�
summary and Conclusions
asymmetry. Future research should focus on a more uniform approach on both studying publica-
tion bias and on handling publication bias in meta-analysis of diagnostic accuracy studies.
Many studies on diagnostic accuracy have major shortcomings in design or conduct. Several
authors showed the influence of shortcomings in methodological criteria on the diagnostic value
of a test [6-8]. Important criteria that may affect the diagnostic value of the test are: retrospective
study design, non-blinded reading of imaging and reference standard results, use of different ref-
erence standards (differential verification), the absence of details about the diagnostic criteria for
the diagnostic test and insufficient information about the study population. In our meta-analyses,
we assessed these criteria by the QUADAS tool [9] and studied the effect of these criteria on
the diagnostic accuracy and adjusted where needed. However it is important to remember that
studies may be assessed as having poor methodological quality either because they were poorly
conducted or poorly reported.
In many studies on diagnostic accuracy, the study design is not or incompletely reported.
The research methods, characteristics of study population and test procedures are often poorly
reported in primary research. A set of minimal reporting standards for diagnostic research has
recently been developed and introduced (Standards for Reporting of Diagnostic Accuracy initia-
tive [10] to improve the quality of the reporting of diagnostic studies. Without complete and ac-
curate reporting we cannot correctly identify potential sources of heterogeneity between studies.
Moreover adequate reporting of the study design will facilitate reviewing the evidence and the
implementation of the findings from the literature. In all, there is strong need: 1) to improve the
methodological quality of diagnostic accuracy studies and 2) to better reporting of studies.
The statistical methodology for meta-analysis of diagnostic accuracy studies is a long way
behind compared to the methodology for meta-analysis of the results of randomized controlled
trials [11-13]. In recent years, the importance of meta-analyses of diagnostic accuracy studies for
evidence-based guidelines is increasingly recognized. All existing methods use dichotomous data
(in terms of sensitivity and specificity). However, in cancer, the differentiation between disease
and non-disease is not the only issue. Correct staging, understaging and overstaging are equally
important. In chapter 9, we describe an approach how to analyze this type of data. Future meta-
analysis of staging data should therefore use a proper approach to summarize these findings in
stead of dichotomizing these data.
Clinical/radiological aspectsImprovements in imaging of several abdominal and pelvic malignancies areas are required to
improve the management of these patients.
In many cancers, such as in gynecological cancer and rectal cancer, evaluation of lymph nodes
is important. The presence or absence of malignant lymph nodes will alter management. So far,
the detection of malignant lymph nodes by any imaging modalities seems to be disappointing
(Chapters 2-4). Recent advantages in lymph node specific MRI contrast agents have shown im-
provements in the differentiation between benign and malignant lymph nodes. In several initial
studies the use of Ultrasmall SuperParamagnetic Iron Oxide particles (USPIO) led to improved
sensitivity of MRI in the detection of malignant lymph nodes [14-18]. Macrophage transport of

summary and Conclusions
�7�
particles will result in accumulation of USPIO in the normal or hyperplastic lymph nodes. In malig-
nant lymph nodes however, macrophages are being replaced by metastatic cells that will prevent
accumulation of the iron particles in (area’s of) the lymph nodes. This technique can be used to
discriminate benign and malignant lymph nodes. At this moment the use of these iron particles
for the detection of malignant lymph nodes is in phase III clinical trials [19, 20].
Another major improvement in radiological imaging is the introduction of combined PET-com-
puted tomography (PET-CT) scanners. In the past few years, PET-CT imaging has increasingly been
used for the diagnosis, staging, monitoring of response and restaging of malignant diseases.
The success of this emerging modality has primarily been attributed to its ability to combine the
advantages of both PET and CT imaging while minimizing their weaknesses. PET is a functional
imaging modality, which is mainly used in clinical oncology to detect primary and metastatic
disease by assessing the metabolic activity of cells [21-25]. Images from dedicated PET scanners
are characterized by long scan durations, which increase patient motion. Moreover there is a lack
of an anatomic framework to correlate the functional information depicted in the PET image.
On the other hand, CT is an anatomic imaging modality that is characterized by high acquisition
speed, high resolution, relatively low noise, and excellent tissue differentiation. In isolation, CT
offers little functional information and depends largely on size and morphology in differentiating
tumor from normal structures [26, 27]. By combining a PET and a CT scanner in a single imaging
device, the disadvantages of one imaging modality could be offset by the other, leading to a
hybrid imaging device with great potential impact on diagnostic clinical oncology [28-32]. Numer-
ous reports have shows the usefulness of PET-CT in tumor diagnosis and staging, (pre-treatment),
monitoring response (post-treatment) and in the follow-up for detection of recurrence [33-36].
However clear-cut indications for the use of PET-CT are not defined for all oncological areas.
Future research should focus on these indications, and the role of PET-CT with respect to other
imaging techniques.
Diagnostic imaging is playing a major role in the management of patients with cancer in the
abdomen. To improve the management of these patients, several new techniques (MRI with liver
specific contrast agents, introduction of PET-CT, lymph node specific contrast agents) are being
developed and evaluated in the literature. The diagnostic value of these techniques should be
evaluated to determine the role and place in the management of these patients in order to de-
veloped evidence-based guidelines. This is mainly done by systematically reviewing the literature
and/or by meta-analysis. If so, it is important to use proper statistical approaches to summarize
the findings of the literature.

�7�
summary and Conclusions
References
1. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50:1088-1101.
2. Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629-634.
3. Macaskill P, Walter SD, Irwig L. A comparison of methods to detect publication bias in meta-analysis. Stat Med 2001;20:641-654.
4. Song F, Khan KS, Dinnes J, Sutton AJ. Asymmetric funnel plots and publication bias in meta-analyses of diagnostic accuracy. Int J Epidemiol 2002;31:88-95.
5. Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J Clin Epidemiol 2005;58:882-893.
6. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999;282:1061-1006.
7. Whiting P, Rutjes AW, Reitsma JB, Glas AS, Bossuyt PM, Kleijnen J. Sources of variation and bias in studies of diagnostic accuracy: a systematic review. Ann Intern Med 2004;140:189-202.
8. Rutjes AW, Reitsma JB, Di Nisio M, Smidt N, van Rijn JC, Bossuyt PM. Evidence of bias and variation in diagnostic accuracy studies. CMAJ 2006 February 14;174(4):469-76.
9. Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Meth-odol 2003;3:25.
10. Bossuyt PM, Reitsma JB, Bruns DE, et al. Towards complete and accurate reporting of studies of diagnostic accuracy: The STARD Initiative. Radiology 2003;226:24-28.
11. Rutter CM, Gatsonis CA. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat Med 2001 October 15;20(19):2865-84.
12. Littenberg B, Moses LE. Estimating diagnostic accuracy from multiple conflicting reports: a new meta-analytic method. Med Decis Making 1993;13:313-321
13. Reitsma JB, Glas AS, Rutjes AW, Scholten RJ, Bossuyt PM, Zwinderman AH. Bivariate analysis of sen-sitivity and specificity produces informative summary measures in diagnostic reviews. J Clin Epidemiol 2005;58:982-990.
14. Bellin MF, Lebleu L, Meric JB. Evaluation of retroperitoneal and pelvic lymph node metastases with MRI and MR lymphangiography. Abdom Imaging 2003;28:155-163
15. Harisinghani MG, Saini S, Weissleder R, et al. MR lymphangiography using ultrasmall superparamagnetic iron oxide in patients with primary abdominal and pelvic malignancies: radiographic-pathologic correla-tion. AJR Am J Roentgenol 1999;172:1347-1351.
16. Keller TM, Michel SC, Frohlich J, et al. USPIO-enhanced MRI for preoperative staging of gynecological pelvic tumors: preliminary results. Eur Radiol 2004;14:937-944.
17. Kim JH, Beets GL, Kim MJ, Kessels AG, Beets-Tan RG. High-resolution MR imaging for nodal staging in rectal cancer: are there any criteria in addition to the size? Eur J Radiol 2004;52:78-83.
18. Rockall AG, Sohaib SA, Harisinghani MG, et al. Diagnostic performance of nanoparticle-enhanced mag-netic resonance imaging in the diagnosis of lymph node metastases in patients with endometrial and cervical cancer. J Clin Oncol 2005;23:2813-2821.
19. Anzai Y, Piccoli CW, Outwater EK, et al. Evaluation of neck and body metastases to nodes with ferumox-tran 10-enhanced MR imaging: phase III safety and efficacy study. Radiology 2003;228:777-788.
20. Harisinghani MG, Saksena MA, Hahn PF, et al. Ferumoxtran-10-enhanced MR lymphangiography: does contrast-enhanced imaging alone suffice for accurate lymph node characterization? AJR Am J Roentgenol 2006;186:144-148.
21. Bomanji JB, Costa DC, Ell PJ. Clinical role of positron emission tomography in oncology. Lancet Oncol 2001;2:157-164.

summary and Conclusions
�7�
22. Delbeke D. Oncological applications of FDG PET imaging: brain tumors, colorectal cancer, lymphoma and melanoma. J Nucl Med 1999;40591-40603.
23. Gambhir SS, Czernin J, Schwimmer J, Silverman DH, Coleman RE, Phelps ME. A tabulated summary of the FDG PET literature. J Nucl Med 2001;42(5 Suppl):1S-93S.
24. Hustinx R, Benard F, Alavi A. Whole-body FDG-PET imaging in the management of patients with cancer. Semin Nucl Med 2002;32:35-46.
25. Smith TA. FDG uptake, tumour characteristics and response to therapy: a review. Nucl Med Commun 1998;19:97-105.
26. Beigelman-Aubry C, Hill C, Guibal A, Savatovsky J, Grenier PA. Multi-detector row CT and postprocessing techniques in the assessment of diffuse lung disease. Radiographics 2005;25:1639-1652.
27. Rydberg J, Liang Y, Teague SD. Fundamentals of multichannel CT. Radiol Clin North Am 2003 May;41(3):465-74.
28. Antoch G, Stattaus J, Nemat AT, et al. Non-small cell lung cancer: dual-modality PET/CT in preoperative staging. Radiology 2003;229:526-533.
29. Lardinois D, Weder W, Hany TF, et al. Staging of non-small-cell lung cancer with integrated positron-emis-sion tomography and computed tomography. N Engl J Med 2003;348:2500-7.
30. Gould MK, Kuschner WG, Rydzak CE, et al. Test performance of positron emission tomography and computed tomography for mediastinal staging in patients with non-small-cell lung cancer: a meta-analysis. Ann Intern Med 2003;139:879-892.
31. Goerres GW, von Schulthess GK, Steinert HC. Why most PET of lung and head-and-neck cancer will be PET/CT. J Nucl Med 2004;45 Suppl 1:66S-71S.
32. Mawlawi O, Pan T, Macapinlac HA. PET/CT imaging techniques, considerations, and artifacts. J Thorac Imaging 2006;21:99-110.
33. Amit A, Beck D, Lowenstein L et al. The role of hybrid PET/CT in the evaluation of patients with cervical cancer. Gynecol Oncol 2006;100:65-69.
34. Antoch G, Saoudi N, Kuehl H, et al. Accuracy of whole-body dual-modality fluorine-18-2-fluoro-2-deoxy-D-glucose positron emission tomography and computed tomography (FDG-PET/CT) for tumor staging in solid tumors: comparison with CT and PET. J Clin Oncol 2004;22:4357-4368.
35. Gearhart SL, Frassica D, Rosen R, Choti M, Schulick R, Wahl R. Improved staging with pretreatment positron emission tomography/computed tomography in low rectal cancer. Ann Surg Oncol 2006;13:397-404.
36. Israel O, Mor M, Guralnik L, et al. Is 18F-FDG PET/CT useful for imaging and management of patients with suspected occult recurrence of cancer? J Nucl Med 2004;45:2045-2051.

2C h a p t e r

Samenvatting en Conclusies

�7�
saMenVaTTInG
Het onderzoek in dit proefschrift had als doel het verzamelen van primaire resultaten en het sa-
menvatten van het wetenschappelijke bewijs ten aanzien van diagnose en stadiering van verschil-
lende gynaecologische en gastrointestinale maligniteiten door middel van echografie, computer
tomografie (CT), Magnetische Resonantie Imaging (MRI) en Positron Emissie Tomografie met
18-fluorodeoxyglucose (FDG-PET). De resultaten van onze analyses kunnen een bijdrage leveren
aan het ontwikkelen van evidence-based richtlijnen voor de klinische praktijk.
In hoofdstuk 2 is de diagnostische waarde van MRI voor de detectie van lymfeklieren in
patiënten met vulvatumor bepaald. Omdat de aanwezigheid van maligne lymfeklieren een be-
langrijke prognostische factor is in deze patiënten en er geen uniforme resultaten in de literatuur
beschreven zijn ten aanzien van preoperatieve detectie van de klieren, hebben twee beoorde-
laars, retrospectief en onafhankelijk van elkaar, MRI onderzoeken van 60 patiënten met vulva
tumor geëvalueerd op de aanwezigheid van maligne lymfeklieren. De MRI bevindingen werden
vergeleken met histopathologische bevindingen, verkregen middels sentinel node procedure
of lymfadenectomie. Sensitiviteit, specificiteit, positief voorspellende en negatief voorspellende
waarde waren respectievelijk 52%, 85%, 46%, en 87% voor beoordelaar 1 and 52% 89%, 52%,
en 89% voor beoordelaar 2.
De conclusie van dit onderzoek is dat er op dit moment geen rol is voor MRI bij de evaluatie
van lymfeklieren in patiënten met vulva tumor.
In hoofdstuk 3 zijn de resultaten van een systematische review naar de diagnostische waarde
van CT en MRI bij het stadieren van cervix carcinoom gerapporteerd. De diagnostische waarden
(sensitiviteit en specificiteit) van beide modaliteiten voor het identificeren van invasie in parame-
tria, blaas en rectum en voor de detectie van maligne lymfeklieren werden bepaald.
Sensitiviteiten van MRI en CT voor het beoordelen van invasie in parametria waren 74% (95%
CI: 68%-79%) en 55% (95% CI: 44%-66%) respectievelijk. Voor de detectie van maligne lymfe-
klieren, 60% (95% CI: 52%-68%) en 43% (95% CI: 37%-57%), respectievelijk. De specificiteiten
van beide modaliteiten voor het beoordelen van parametria invasie en lymfeklieren waren verge-
lijkbaar.
Voor het evalueren van invasie van de blaas en het rectum, waren de sensitiviteiten van MRI,
75% (95% CI: 66%-83%) en 71% (95% CI: 53%-83%), respectievelijk; beide (niet significant)
hoger vergeleken met de waarden van CT. De specificiteit van MRI voor het evalueren van blaas
invasie was significant hoger vergeleken met die van CT: 91% (95% CI: 83%-95%) en 73% (95%
CI: 52%-87%). De specificiteiten van beide modaliteiten voor de beoordeling van rectum invasie
waren vergelijkbaar.
Op basis van de bevindingen van onze systematische review, werden de volgende aanbeve-
lingen voor het stadieren van cervix carcinoom gedaan. In patiënten met klinische laagstadia
tumoren, is de prevalentie van invasie buiten de cervix laag en daarom de additionele waarde
van MRI ook beperkt. Echter in patiënten met hoogstadia tumoren kan MRI een belangrijke rol
spelen; klinisch onderzoek heeft namelijk beperkingen ten aanzien van het bepalen van invasie
buiten de cervix.
samenvatting en Conclusies

�7�
In hoofdstuk 4 hebben we de diagnostische waarden van endoluminale echografie (EUS), CT en
MRI voor het beoordelen van lokale en regionale (lymfeklieren) stadiering van rectum tumoren
vergeleken middels een meta-analyse.
Voor het beoordelen van muscularis propria invasie, hadden EUS en MRI vergelijkbare sensitivi-
teiten. Specificiteiten waren 86% (95% CI: 80%-90%) en 69% (95% CI: 52%-82%) respectievelijk.
Voor het beoordelen van de invasie van het perirectale weefsel, was de sensitiviteit van EUS 90%
(95% CI: 88%-92%); significant hoger dan die van CT en van MRI (79% [95% CI: 74%-84%] en
82% [95% CI: 74%-87%]). Specificiteiten waren vergelijkbaar. Voor de beoordeling van invasie
van aangrenzende organen/structuren en voor de detectie van maligne lymfeklieren hadden alle
modaliteiten vergelijkbaren sensitiviteiten en specificiteiten.
Ook de summary ROC curve van EUS bij het bepalen van invasie van het perirectale weefsel
liet een betere diagnostische accuratesse zien vergeleken met CT en MRI. Summary ROC curven
voor de detectie van lymfeklieren lieten geen verschillen zien in accuratesse tussen de drie moda-
liteiten.
Op basis van de resultaten van deze meta-analyse, lijkt EUS een betere diagnostische modali-
teit te zijn voor het bepalen van lokale stadiering dan CT en MRI. Echter EUS is niet in staat om
de mesorectale fascie te identificeren, terwijl dit wel mogelijk is met MRI. De identificatie van de
mesorectale fascie is belangrijk voor het bepalen van de afstand van de tumor tot deze fascie,
in patiënten die potentieel in aanmerking komen voor totale mesorectale excisie (TME). EUS
kan echter wel gebruikt worden voor de selectie van patiënten voor beschikbare therapeutische
strategieën, zoals transanale endoscopische microchirurgie (TEM) en de TME. De identificatie van
lymfeklieren met EUS, CT, en MRI blijft een belangrijk probleem.
In hoofdstuk 5 hebben wij het beschikbare wetenschappelijke onderzoek naar de diagnosti-
sche waarde van echografie (US), CT en MRI bij de diagnose en het bepalen van resectabiliteit van
pancreas carcinoom systematisch samengevat. Het doel van dit onderzoek was om diagnostische
uitkomstmaten te verkrijgen van echografie, conventionele CT, spiraal CT en MRI voor de diag-
nose en het bepalen van resectabiliteit van pancreas adenocarcinoom.
Voor de diagnose waren de sensitiviteiten van US, conventionele CT, spiraal CT, en MRI respec-
tievelijk 76%, 86%, 91%, en 84% en de specificiteiten respectievelijk 75%, 79%, 85%, en 82%.
De sensitiviteiten van MRI en US waren significant lager dan die van spiraal CT (P = 0.04 en P =
0.0001).
Voor het bepalen van resectabiliteit waren de sensitiviteiten van US, conventionele CT, spiraal
CT, en MRI respectievelijk 83%, 82%, 81%, en 82% en specificiteiten respectievelijk 63%, 76%,
82%, en 78%. Specificiteit van US was significant lager dan die van spiraal CT (P = 0.011).
Vanwege de hoge sensitiviteit van spiraal CT voor de diagnose van pancreascarcinoom verge-
leken met MRI en US en de hoge specificiteit van spiraal CT voor het bepalen van resectabiliteit
vergeleken met US, kan spiraal CT als modaliteit van keuze beschouwd worden voor zowel de
diagnose en het bepalen van de resectabiliteit van pancreas adenocarcinoom.
In hoofdstuk 6 hebben wij de resultaten van een enquête gepresenteerd. In de enquête werd
gevraagd naar de diagnostiek en behandeling van patiënten met colorectale levermetastasen. Uit
de resultaten van de enquête bleek dat er in Nederland veel variatie bestond in zowel de diagnose
samenvatting en Conclusies

��0
als behandeling van deze patiënten. Deze enquête diende ook om factoren die de implementatie
van de te ontwikkelen richtlijn in de weg zouden kunnen staan, op te sporen. Een evidence-based
richtlijn waarin rekening wordt gehouden met beschikbare evidence, de expertise en beschikbaar-
heid kan de variatie verhelpen (gepresenteerd in hoofdstuk 8).
In hoofdstuk 7 worden de resultaten van een meta-analyse gepresenteerd. In deze meta-
analyses werden de diagnostische uitkomstmaten van CT, MRI en FDG-PET voor de detectie van
colorectale levermetastasen vergeleken. Het doel van dit onderzoek was om schattingen van
sensitiviteit van CT, MRI en FDG-PET op per-patient en per-laesie basis te verkrijgen.
Op per-patient basis waren de sensitiviteiten van conventionele CT, spiraal CT, 1.5 T MRI,
en FDG-PET 60.2%, 64.7%, 75.8%, en 94.6%, respectievelijk; FDG-PET was de meest accurate
modaliteit.
Op per-laesie basis, waren de sensitiviteiten van conventionele CT, spiraal CT, 1.0 T MRI, 1.5 T
MRI, en FDG-PET, respectievelijk 52.3%, 63.8%, 66.1%, 64.4%, en 75.9%; conventionele CT had
de laagste sensitiviteit. Sensitiviteiten van MRI met gadolinium en MRI met superparamagnetische
ijzer oxide (SPIO) waren significant beter, vergeleken met MRI zonder contrast (P = 0.019 en P <
0.001, respectievelijk) en vergeleken met spiraal CT met ≤ 45 g Jodium (P = 0.02 en P < 0.001, res-
pectievelijk). Voor laesies ≥ 1 cm, was MRI met SPIO de meest accurate modaliteit (P < 0.001).
De keuze tussen spiraal CT met > 45 gr Jodium of MRI met gadolinium of MRI met SPIO, moet
ook afhankelijk zijn van de beschikbaarheid en expertise en niet alleen van de diagnostische ac-
curatesse. De rol van FDG-PET voor de detectie van colorectale levermetastasen op dit moment
is beperkt. FDG-PET zal daarom vooral als additionele imaging modaliteit voor de detectie van
extrahepatische afwijkingen worden toegepast.
In hoofdstuk 8 vatten we een evidence-based richtlijn samen, die ontwikkeld is voor de diag-
nose en behandeling van patiënten met colorectale levermetastasen. De belangrijkste aanbeve-
lingen zijn als volgt:
Voor de detectie van synchrone levermetastasen wordt geadviseerd om een spiraal CT of MRI
van de lever te verrichten. Voor de beoordeling van de longen wordt geadviseerd om beeldvor-
mende diagnostiek te beperken tot een X-thorax.
Voor het aantonen van metachrone levermetastasen kan beeldvorming beperkt blijven tot
echografie, als de lever als geheel echografisch goed te beoordelen is. Als dit niet het geval is, of
als irresectabiliteit niet kan worden vastgesteld, dient er aanvullend onderzoek middels Spiraal CT
of MRI verricht te worden.
Voor evaluatie van de extrahepatische afwijkingen, kan een abdominale en thoracale CT ver-
richt worden. FDG-PET kan een bijdrage leveren in patiënten die geselecteerd zijn voor resectie
op basis van CT (lever/abdomen/thorax), voor de identificatie van aanvullende extrahepatische
afwijkingen.
Resectie is de behandeling van keuze met een 5-jaars overleving van 30%-40%. Er blijkt echter
een enorme variatie in prognostische factoren te bestaan. Over marges < 10 mm bestaat er
geen duidelijkheid. Over het beleid bij aanwezigheid van extrahepatische metastasen bestaan
er twijfels. Er is een enorme variatie waarneembaar in de technische uitvoering van resecties
(anatomische vs. niet-anatomische). Duidelijke resultaten over de effectiviteit van combinatiebe-
samenvatting en Conclusies

���
handelingen met (neo)-adjuvante chemotherapie ontbreken. Om de variatie in selectie criteria
te minimaliseren, dienen patiënten geselecteerd te worden zoals beschreven in de richtlijn en bij
voorkeur in centra met veel ervaring.
Als resectie niet mogelijk is, gezien de uitgebreidheid en/of niet-resectabele metastasen, wordt
palliatieve chemotherapie geadviseerd. Voor systemische therapie wordt een fluoropyrimidine be-
vattende eerstelijns chemotherapie (zowel orale 5-FU prodrugs als intraveneus 5-FU/Leucovorin)
gecombineerd met oxaliplatin of irinotecan als standaardbehandeling beschouwd.
Radiofrequente ablatie, geisoleerde lever perfusie, vena-porta embolisatie en intra-arteriele
chemotherapie worden als experimentele behandelingstechnieken beschouwd en dienen bij
voorkeur in onderzoeksverband uitgevoerd te worden.
In hoofdstuk 9 hebben wij een nieuw methode voor het analyseren van stadiering data be-
schreven. Met dit multivariaat random-effects model kunnen schattingen van correcte stadiering
en de mate van onder- en overstadiering berekend worden.
Bij kanker is de differentiatie tussen ziekte en niet-ziekte niet het enige punt van belang, maar
ook de correcte stadiering en de mate van onder- en overstadiering zijn belangrijk. Bij bestaande
meta-analytische methoden, zoals het bivariaat random-effects model, dient data gedichotomi-
seerd te worden, alvorens sensitiviteit en specificiteit berekend kan worden. Bijvoorbeeld in 4-ca-
tegorie stadiering data, kunnen drie dichotomieën worden verkregen: T1 vs. T2+T3+T4, T1+T2 vs.
T3+T4 en T1+T2+T3 vs. T4). Hierbij gaat informatie met betrekking tot onder- en overstadiering
verloren.
Bovengenoemd multivariaat random-effects model werd gebruikt om schattingen van cor-
recte stadiering en van onder- en overstadiering te berekenen. Ook werden schattingen van
sensitiviteit en specificiteit voor de drie dichotomieën berekend. Voor deze doelen werd een
subset van data (data vanaf 1993) die eerder voor de vergelijking van Endoluminale US (EUS) en
MRI voor de stadiering van rectum tumoren (chapter 4) was geanalyseerd volgens het bivariaat
random-effects model opnieuw geanalyseerd.
EUS was accurater dan MRI in correcte stadiering (80% vs. 72%), maar de verschillen waren
niet statistisch significant. Overstadiering met MRI was groter vergeleken met EUS: middels MRI
werden T1 tumoren vaker als T2/T3 gestadieerd (12% vs. 2%), en T2 tumoren werden ook vaker
als T3 gestadieerd (42% vs. 28%).
De sensitiviteit en specificiteit van EUS en MRI voor de drie dichotomieën, berekend met de
resultaten van het multivariaat random-effects model, waren vergelijkbaar met de sensitiviteit en
specificiteit verkregen met bivariaat random-effects analyses.
Het multivariaat random-effects model kan een behulpzame, informatieve en precieze metho-
de zijn voor het analyseren van ordinale of nominale data voor meta-analyses van diagnostische
accuratesse studies.
samenvatting en Conclusies

���
ConClUsIes en ToeKoMsTIG onDeRZoeK
Het onderzoek beschreven in dit proefschrift laat zien dat zowel het uitvoeren van primaire diag-
nostische studies van voldoende methodologische kwaliteit en het systematisch samenvatten van
de literatuur, beiden waardevolle en essentiële middelen zijn voor het formuleren van evidence-
based aanbevelingen voor de klinische praktijk.
MethodologieOver het algemeen, zijn er een aantal essentiële stappen in het uitvoeren van systematische
reviews van diagnostische accuratesse studies: het definiëren van een klinische vraag, het uitvoe-
ren van een uitgebreide literatuur zoekstrategie, het definiëren van criteria voor het selecteren
van relevante artikelen, het scoren van methodologische kwaliteitskenmerken, het verzamelen
van data over de diagnostische accuratesse, het verklaren van heterogeniteit in studie resulta-
ten, het analyseren van studie resultaten en als het mogelijk is het analyseren van data in een
kwantitatieve methode “meta-analyses”. Op elk niveau kunnen er problemen zijn: bijvoorbeeld,
studies die nooit gepubliceerd zijn (publicatie bias), studies waarvan de methodologische kwaliteit
suboptimaal is of studies die niet alle relevante data (incompleet data) rapporteren. Ondanks dat
er geavanceerde statistische methoden zijn om bovengenoemde problemen te verhelpen, zijn er
een aantal issues, waar aandacht aan besteed dient te worden:
Zoals in elke systematische review, kan ook in systematische reviews van diagnostische accu-
ratesse studies sprake zijn van publicatie bias. Over het algemeen worden in gerandomiseerde
gecontroleerde trials, funnel plots gecreëerd voor het bestuderen van publicatie bias; de log odds
ratio wordt afgezet tegen het aantal patiënten of tegen de precisie (inverse van de standaard
error). Verschillende statistische testen zoals Begg’s rank correlatie [1], Egger’s regressie test [2]
en Macaskill’s regressie test [3] zijn in de literatuur beschreven om de plot asymmetrie objectief
te beoordelen. Song et al [4] suggereren dat funnel plots en Begg’s en Egger’s testen ook kun-
nen worden gebruikt voor het bestuderen van publicatie bias in reviews van diagnostische testen.
Deeks et al [5] echter rapporteren dat de Begg’s, Egger’s en Macaskill’s testen misleidend zijn als
ze worden toegepast in reviews van diagnostische accuratesse studies en komen met een nieuw
voorstel, de zogeheten effective sample size funnel plots en hieraan geassocieerde regressie
testen voor asymmetrie. Door de enorme diversiteit aan methoden, dient in de toekomst meer
aandacht besteed te worden aan het ontwikkelen van een uniform model voor het bestuderen
van publicatie bias en hoe om te gaan met publicatie bias in reviews van diagnostische accura-
tesse studies.
Veel diagnostische accuratesse studies hebben tekortkomingen in de methodologische ka-
rakteristieken. Verschillende auteurs hebben aangetoond dat deze tekortkomingen vaak effect
hebben op de diagnostische waarde van een bepaalde test [6-8]. Belangrijke karakteristieken die
een effect kunnen hebben op de diagnostische waarde van een test zijn: retrospective studie
design, niet geblindeerde beoordeling van imaging en referentie standaard bevindingen, toepas-
sen van verschillende referentie standaarden (differentiele verificatie), het ontbreken van details
over de diagnostische criteria van een diagnostische test en onvoldoende beschrijving van de
samenvatting en Conclusies

���
studie populatie. In onze meta-analyses, hebben we al deze karakteristieken gescoord volgens
de QUADAS methode [9] en hebben we bestudeerd wat de effecten van tekortkomingen op de
diagnostische waarde waren en waar nodig gecorrigeerd. Het is echter belangrijk om te weten
dat studies welke gescoord worden als methodologisch slechte studies, niet per se suboptimaal
uitgevoerd zijn, maar dat dit ook veroorzaakt kan worden door suboptimale rapportage van de
studies.
In veel studies over diagnostische accuratesse, wordt de uitvoering van de studie incompleet
gerapporteerd. Recent is er een lijst ontwikkeld waarin wordt aangegeven wat er minimaal ge-
rapporteerd dient te worden in een diagnostische accuratesse studie (Standards for Reporting
of Diagnostic Accuracy initiative [10]); dit voor het verbeteren van rapportage van diagnostische
studies. Zonder complete en accurate reportage, is het heel lastig om de oorzaken van de hete-
rogeniteit tussen studieresultaten te bestuderen. Ook kan adequate reportage van studie design
karakteristieken een positieve bijdrage leveren aan het verzamelen van wetenschappelijk bewijs
en de implementatie van deze bevindingen uit de literatuur in de praktijk. Concluderend, het is
belangrijk om 1) de methodologische kwaliteit van diagnostische accuratesse studies te verbete-
ren en 2) de rapportage van studies te verbeteren.
De statistische methodologie van meta-analyses van diagnostische accuratesse studies loopt
achter op de ontwikkeling van de methodologie van meta-analyses van gerandomiseerde gecon-
troleerde trials [11-13]. In de afgelopen jaren is het belang van meta-analyses van diagnostische
accuratesse studies voor het ontwikkelen van evidence-based richtlijnen enorm toegenomen.
Echter, alle bestaande methoden maken gebruik van dichotome data (voor de berekening van
sensitiviteit en specificiteit). Echter, bij patiënten met een tumor is het onderscheid tussen zieken
en niet-zieken niet alleen belangrijk, maar ook correcte stadiering, alsook de mate van onder- en
overstadiering. In hoofdstuk 9, beschrijven we een methode waarmee stadiering data geanaly-
seerd kan worden. Toekomstige meta-analyses van stadiering data dient middels een geschikte
methode geanalyseerd te worden in plaats van deze data dichotomiseren.
Klinische/radiologische aspectenOntwikkelingen op het gebied van imaging van abdominale en pelvine aandoeningen hebben
vooral als doel het verbeteren van de zorg van patiënten met deze aandoeningen.
Bij patiënten met bijvoorbeeld gynaecologische en rectum tumoren, is de evaluatie van lymfe-
klieren belangrijk. De aan- of afwezigheid van maligne lymfeklieren kan leiden tot het veranderen
van het beleid. Tot nu toe is de detectie of maligne lymfeklieren middels een beeldvormende
modaliteit teleurstellend (Hoofdstukken 2-4). Recente ontwikkelingen op het gebied van lym-
feklierspecifiek MRI contrast middelen (Ultrasmall SuperParamagnetic Iron Oxide=USPIO) laten
verbeteringen zien in het onderscheid tussen benigne en maligne lymfeklieren bij MRI. Verschil-
lende pilot studies rapporteren een hoge sensitiviteit voor de detectie van maligne lymfeklieren
als USPIO wordt toegediend [14-18]. Macrofagen in lymfeklieren zorgen voor transport van US-
PIO partikels, wat resulteert in accumulatie van deze partikels in normale of in hyperplastische
lymfeklieren. In maligne lymfeklieren echter wordt normaal lymfklierweefsel met macrofagen
vervangen door metastasen en vindt er geen of nauwelijks accumulatie van de partikels plaats.
samenvatting en Conclusies

���
Hierdoor kan er onderscheid gemaakt worden tussen benigne en maligne klieren. Op dit moment
worden de diagnostische waarde van toediening van USPIO partikels onderzocht in fase III studies
[19, 20].
Een andere belangrijke ontwikkeling op het gebied van radiologische imaging is de introductie
van de gecombineerde PET-CT scanners. In de afgelopen jaren is de toepassing van PET-CT voor
de diagnose, stadiering, monitoren van respons en restadiering van maligniteiten toegenomen.
Het succes van deze gecombineerde techniek komt primair tot stand door de combinatie van de
voordelen van afzonderlijke PET en CT technieken in combinatie met het minimaliseren van de
beperkingen van de technieken. PET is een functionele imaging modaliteit, welke vooral wordt
toegepast in de klinische oncologie voor de detectie van primaire tumor en metastasen, waarbij
de toegenomen metabolische activiteit van tumorweefsel wordt vastgesteld [21-25]. Echter, de
scan tijd van PET is lang, welke gepaard gaat met beweging van patiënten. Ook ontbreekt er een
anatomisch frame om de functionele informatie verkregen met het PET plaatje te correleren. CT
is juist een anatomische imaging modaliteit, gekarakteriseerd door hoge acquisitie snelheid, hoge
resolutie, relatief lage ruis en goede weefseldifferentiatie. CT verschaft echter weinig informatie
over functie en is erg afhankelijk van vorm en grootte voor het maken van onderscheid tussen
tumor en normale structuren [26, 27]. Door het combineren van PET en CT scanner in een enkele
modaliteit, konden de tekortkomingen van de ene modaliteit worden gecompenseerd door de
voordelen van de andere modaliteit [28-32]. Veel onderzoeken hebben het belang van de toe-
passing van PET-CT bij de diagnose en stadiering van tumor, het monitoren van respons en in de
follow-up voor de detectie van recidief [33-36] aangetoond. Echter duidelijke indicaties voor de
toepassing van PET-CT ontbreken nog voor veel toepassingen. Toekomstig onderzoek dient meer
aandacht te besteden aan deze indicaties, en aan de plaats van PET-CT in relatie tot de plaats van
andere imaging modaliteiten.
Diagnostiek middels radiologische technieken speelt een belangrijke rol bij de behandeling van
patiënten met tumoren in het abdomen en het bekken. Om het beleid voor deze patiënten te ver-
beteren, zijn verschillende nieuwe technieken (MRI met lever specifiek contrastmiddel, introductie
van PET-CT scanners, lymfeklier specifiek contrast middelen) ontwikkeld en ook geëvalueerd in
de literatuur. De diagnostische waarde van deze technieken dient geëvalueerd te worden om te
bepalen wat de rol en plaats van deze technieken in het beleid van deze patiënten is; dit alles
met als doel het ontwikkelen van evidence-based richtlijnen. De rol en plaats van deze technieken
wordt vooral bepaald door het systematisch reviewen van de literatuur en/of door het uitvoeren
van meta-analyses. Daarom is het dus belangrijk om geschikte statistische methoden te gebruiken
voor het analyseren van de bevindingen uit de literatuur.
samenvatting en Conclusies

���
Referenties
1. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50:1088-1101.
2. Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629-634.
3. Macaskill P, Walter SD, Irwig L. A comparison of methods to detect publication bias in meta-analysis. Stat Med 2001;20:641-654.
4. Song F, Khan KS, Dinnes J, Sutton AJ. Asymmetric funnel plots and publication bias in meta-analyses of diagnostic accuracy. Int J Epidemiol 2002;31:88-95.
5. Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J Clin Epidemiol 2005;58:882-893.
6. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999;282:1061-1006.
7. Whiting P, Rutjes AW, Reitsma JB, Glas AS, Bossuyt PM, Kleijnen J. Sources of variation and bias in studies of diagnostic accuracy: a systematic review. Ann Intern Med 2004;140:189-202.
8. Rutjes AW, Reitsma JB, Di Nisio M, Smidt N, van Rijn JC, Bossuyt PM. Evidence of bias and variation in diagnostic accuracy studies. CMAJ 2006 February 14;174(4):469-76.
9. Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Meth-odol 2003;3:25.
10. Bossuyt PM, Reitsma JB, Bruns DE, et al. Towards complete and accurate reporting of studies of diagnostic accuracy: The STARD Initiative. Radiology 2003;226:24-28.
11. Rutter CM, Gatsonis CA. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat Med 2001 October 15;20(19):2865-84.
12. Littenberg B, Moses LE. Estimating diagnostic accuracy from multiple conflicting reports: a new meta-analytic method. Med Decis Making 1993;13:313-321
13. Reitsma JB, Glas AS, Rutjes AW, Scholten RJ, Bossuyt PM, Zwinderman AH. Bivariate analysis of sen-sitivity and specificity produces informative summary measures in diagnostic reviews. J Clin Epidemiol 2005;58:982-990.
14. Bellin MF, Lebleu L, Meric JB. Evaluation of retroperitoneal and pelvic lymph node metastases with MRI and MR lymphangiography. Abdom Imaging 2003;28:155-163
15. Harisinghani MG, Saini S, Weissleder R, et al. MR lymphangiography using ultrasmall superparamagnetic iron oxide in patients with primary abdominal and pelvic malignancies: radiographic-pathologic correla-tion. AJR Am J Roentgenol 1999;172:1347-1351.
16. Keller TM, Michel SC, Frohlich J, et al. USPIO-enhanced MRI for preoperative staging of gynecological pelvic tumors: preliminary results. Eur Radiol 2004;14:937-944.
17. Kim JH, Beets GL, Kim MJ, Kessels AG, Beets-Tan RG. High-resolution MR imaging for nodal staging in rectal cancer: are there any criteria in addition to the size? Eur J Radiol 2004;52:78-83.
18. Rockall AG, Sohaib SA, Harisinghani MG, et al. Diagnostic performance of nanoparticle-enhanced mag-netic resonance imaging in the diagnosis of lymph node metastases in patients with endometrial and cervical cancer. J Clin Oncol 2005;23:2813-2821.
19. Anzai Y, Piccoli CW, Outwater EK, et al. Evaluation of neck and body metastases to nodes with ferumox-tran 10-enhanced MR imaging: phase III safety and efficacy study. Radiology 2003;228:777-788.
20. Harisinghani MG, Saksena MA, Hahn PF, et al. Ferumoxtran-10-enhanced MR lymphangiography: does contrast-enhanced imaging alone suffice for accurate lymph node characterization? AJR Am J Roentgenol 2006;186:144-148.
21. Bomanji JB, Costa DC, Ell PJ. Clinical role of positron emission tomography in oncology. Lancet Oncol 2001;2:157-164.
samenvatting en Conclusies

��6 ��7
22. Delbeke D. Oncological applications of FDG PET imaging: brain tumors, colorectal cancer, lymphoma and melanoma. J Nucl Med 1999;40591-40603.
23. Gambhir SS, Czernin J, Schwimmer J, Silverman DH, Coleman RE, Phelps ME. A tabulated summary of the FDG PET literature. J Nucl Med 2001;42(5 Suppl):1S-93S.
24. Hustinx R, Benard F, Alavi A. Whole-body FDG-PET imaging in the management of patients with cancer. Semin Nucl Med 2002;32:35-46.
25. Smith TA. FDG uptake, tumour characteristics and response to therapy: a review. Nucl Med Commun 1998;19:97-105.
26. Beigelman-Aubry C, Hill C, Guibal A, Savatovsky J, Grenier PA. Multi-detector row CT and postprocessing techniques in the assessment of diffuse lung disease. Radiographics 2005;25:1639-1652.
27. Rydberg J, Liang Y, Teague SD. Fundamentals of multichannel CT. Radiol Clin North Am 2003 May;41(3):465-74.
28. Antoch G, Stattaus J, Nemat AT, et al. Non-small cell lung cancer: dual-modality PET/CT in preoperative staging. Radiology 2003;229:526-533.
29. Lardinois D, Weder W, Hany TF, et al. Staging of non-small-cell lung cancer with integrated positron-emis-sion tomography and computed tomography. N Engl J Med 2003;348:2500-7.
30. Gould MK, Kuschner WG, Rydzak CE, et al. Test performance of positron emission tomography and computed tomography for mediastinal staging in patients with non-small-cell lung cancer: a meta-analysis. Ann Intern Med 2003;139:879-892.
31. Goerres GW, von Schulthess GK, Steinert HC. Why most PET of lung and head-and-neck cancer will be PET/CT. J Nucl Med 2004;45 Suppl 1:66S-71S.
2. Mawlawi O, Pan T, Macapinlac HA. PET/CT imaging techniques, considerations, and artifacts. J Thorac Imaging 2006;21:99-110.
33. Amit A, Beck D, Lowenstein L et al. The role of hybrid PET/CT in the evaluation of patients with cervical cancer. Gynecol Oncol 2006;100:65-69.
34. Antoch G, Saoudi N, Kuehl H, et al. Accuracy of whole-body dual-modality fluorine-18-2-fluoro-2-deoxy-D-glucose positron emission tomography and computed tomography (FDG-PET/CT) for tumor staging in solid tumors: comparison with CT and PET. J Clin Oncol 2004;22:4357-4368.
35. Gearhart SL, Frassica D, Rosen R, Choti M, Schulick R, Wahl R. Improved staging with pretreatment positron emission tomography/computed tomography in low rectal cancer. Ann Surg Oncol 2006;13:397-404.
36. Israel O, Mor M, Guralnik L, et al. Is 18F-FDG PET/CT useful for imaging and management of patients with suspected occult recurrence of cancer? J Nucl Med 2004;45:2045-2051.
samenvatting en Conclusies
��6

��6 ��7

2C h a p t e r

List of Publications

��0
Bipat S, Glas AS, van der Velden J, Zwinderman AH, Bossuyt PM, Stoker J. Computed tomog-
raphy and magnetic resonance imaging in staging of uterine cervical carcinoma: a systematic
review. Gynecologic Oncology 2003;91(1):56-66
Bipat S, Glas AS, Slors FJM, Zwinderman AH, Bossuyt PM, Stoker J. Rectal cancer: local staging
and assessment of lymph node involvement with endoluminal US, CT, and MR imaging--a meta-
analysis. Radiology 2004:232(2):773-783
Bipat S, Phoa SS, van Delden OM, Bossuyt PM, Gouma DJ, Laméris JS, Stoker J. Ultrasonography,
computed tomography and magnetic resonance imaging for diagnosis and determining resect-
ability of pancreatic adenocarcinoma: a meta-analysis. Journal of Computer Assisted Tomography
2005;29(4):438-445
Bipat S, van Leeuwen MS, Comans EF, Pijl ME, Bossuyt PM, Zwinderman AH, Stoker J. Colorectal
liver metastases: CT, MR imaging, and PET for diagnosis--meta-analysis. Radiology 2005;237(1):123-
131
Bipat S, van Leeuwen MS, IJzermans JN, Bossuyt PM, Greve JW, Stoker J. Imaging and treatment
of patients with colorectal liver metastases in the Netherlands: a survey. The Netherlands Journal
of Medicine 2006;64(5):147-151
Bipat S, Fransen GA, Spijkerboer AM, van der Velden J, Bossuyt PM, Zwinderman AH, Stoker J. Is
there a role for magnetic resonance imaging in the evaluation of inguinal lymph node metastases
in patients with vulva carcinoma? Gynecologic Oncology 2006;103(3):1001-1006
Bipat S, van Leeuwen MS, IJzermans JN, Comans EF, Planting AS, Bossuyt PM, Greve JW, Stoker
J. Evidence-based guideline on management of colorectal liver metastases in the Netherlands. The
Netherlands Journal of Medicine 2007;65(1):5-14
Bipat S, Zwinderman AH, Bossuyt PM, Stoker J. Multivariate random-effects approach: for meta-
analysis of cancer staging studies. Submitted
Jensch S, van Gelder RE, Florie J, Thomassen-de Graaf MA, Lobe JV, Bossuyt PM, Bipat S, Nio YC,
Stoker J. Performance of Radiographers in the Evaluation of CT Colonographic Images. American
Journal of Roentgenology (in press)
Jensch S, de Vries AH, Peringa J, Bipat S, Dekker E, Baak LC, Bartelsmans JF, Heutinck A, Mon-
tauban van Swijndregt Alexander, Stoker J. Performance characteristics of CT colonography with
a minimal bowel preparation in an increased risk population. Submitted
list of Publications

���
van Randen A, Bipat S, Zwinderman AH, Ubbink DT, Stoker J, Boermeester MA. Acute appendi-
citis: a meta-analysis of test accuracy of computed tomography and ultrasonography related to
prevalence of disease. Submitted
Horsthuis K, Bipat S, Bennink RJ, Stoker J. Ultrasonography, Magnetic Resonance Imaging, Scin-
tigraphy, and Computed Tomography in the detection of active inflammatory bowel disease: a
meta-analysis. Submitted
Florie J, van Gelder RE, Schutter M, van Randen A, Venema H, de Jager S, Prent A, Bipat S, Baak
L, Stoker J. Computed tomography colonography using limited bowel preparation at low mAs
levels; Feasibility study. Submitted
Coenegrachts K, Delanote J, ter Beek L, Haspeslagh M, Bipat S, Stoker J, van Kerkhove F, Steyaert
L, Rigauts H, Casselman JW. Improved focal liver lesion detection: Comparison of single shot dif-
fusion-weighted echo planar and single shot T2W turbo spin echo techniques. The British Journal
of Radiology (in press)
Coenegrachts K, Delanote J, ter Beek L, Haspeslagh M, Bipat S, Stoker J, Steyaert L, Rigauts
H, Casselman JW. Comparison of Respiratory-Triggered T2-weighted Turbo Spin-Echo imaging
versus Breath-Hold T2-weighted Turbo Spin-Echo imaging in focal liver lesion detection and char-
acterization. Submitted
Coenegrachts K, Delanote J, ter Beek L, Haspeslagh M, Bipat S, Stoker J, Steyaert L, Rigauts H,
Casselman JW. Evaluation of true diffusion, perfusion factor, and apparent diffusion coefficient
in non-necrotic liver metastases and uncomplicated liver hemangiomas using black-blood echo
planar imaging. Submitted
Coenegrachts K, Orlent H, ter Beek L, Haspeslagh M, Bipat S, Stoker J, Steyaert L, Rigauts H.
Improved focal liver lesion detection: comparison of black-blood single-shot spin echo planar and
SPIO-enhanced MR imaging. Submitted
list of Publications

2C h a p t e r

Dankwoord Curriculum Vitae

��� ���

��� ������
Mijn familie, vrienden en collega’s hebben op verschillende manieren bijgedragen aan het tot
stand komen van dit proefschrift. Ik zou dan ook iedereen, die op welke manier dan ook een
bijdrage heeft geleverd, hartelijk willen bedanken, een aantal personen in het bijzonder:
Allereerst Prof. dr. J. Stoker, beste Jaap, dank voor je initiatief om mij meta-analyses uit te laten
voeren en mij het vertouwen te geven dat dit zou lukken. Je openheid voor nieuwe uitdagingen
en ontwikkelingen maken jou een geweldige radioloog, maar vooral een fantastische begeleider.
Jij bent ook een heel bijzonder mens (niet alleen op radiologisch en wetenschappelijk gebied) en
ik vind het dan ook heel fijn om onder jouw begeleiding te mogen werken.
Prof. dr. P.M.M. Bossuyt, beste Patrick, heel veel dank voor jouw methodologische en vooral
psychische steun de afgelopen tijd. Voor elk probleem kwam/kom jij met een gepaste oplossing.
Jouw inzicht in de methodologie van diagnostische studies, heeft bijgedragen tot de opzet van
een aantal essentiële studies in dit proefschrift. Mede door jouw geweldige steun en enthousi-
asme, heb ik de epidemiologie opleiding gedaan. Bedankt voor alles.
Prof. dr. A.H. Zwinderman, beste Koos, ik had een geweldige radioloog en een geweldige me-
thodoloog, maar een statisticus maakte het geheel compleet. Ik wil jou dan ook bedanken voor
alle hulp. Jouw statistische hulp heeft heel veel toegevoegd aan dit proefschrift. Je hebt mij niet
alleen geholpen met het bivariate random-effects model, maar je staat ook altijd klaar voor alle
andere statistische moeilijkheden. Zo ook onze multivariate analyse. De prettige manier waarop
je mij statistiek (inclusief winbugs) probeert uit te leggen, waardeer ik zeer.
Beste Ko, Frederik, Saffire, Afina, Maarten (van L), Emile, Milan en Otto, heel veel dank voor het
selecteren en beoordelen van al die artikelen voor de meta-analyses. Milan, het was een gedoe,
maar het resultaat telt! Ook heel veel dank voor het lezen en becommentariëren van de manus-
cripten. Beste Ko en Maarten, ik hoop dat we in de toekomst meer kunnen doen op het gebied
van gynaecologische oncologie en lever imaging. Ook Anje en Gerwin, bedankt dat jullie bereid
waren om de MRI plaatjes te beoordelen.
Een van de reviews heeft bijgedragen tot het ontwikkelen van een landelijke richtlijn voor Di-
agnostiek en behandeling van patiënten met colorectale levermetastasen. Ik bedank alle werk-
groepleden voor hun hulp en inzet. Tijdens deze richtlijnontwikkeling heb ik heel veel van jullie
geleerd; de rol van diagnostiek bij het selecteren van patiënten voor een breed scala aan be-
handelingsstrategieën is niet zwart-wit. Het was eigenlijk een eer om als niet-medisch specialist
bij te dragen aan een enorm specialistisch en complex geheel. Dank aan de voorzitters van alle
oncologiecommissies en medisch specialisten die bereid waren om vragenlijsten in te vullen en
te retourneren. Ook dank aan alle wetenschappelijke verenigingen, die bereid waren om de
definitieve richtlijn te beoordelen en commentaar dan wel aanvullingen te geven. Ook dank ik de
medewerkers van de Orde van Medisch Specialisten, Van Zuiden Communications en de Vereni-
Dankwoord

ging van Integrale Kankercentra, die zorg dragen voor de verspreiding van deze richtlijn, in het
bijzonder dr. J. Benraadt van het IKA.
Mijn (ex-) G1-collega’s, Adrienne, Annette, Maartje, Maaike, Nicole, Wouter, Rogier (van G),
Jasper, Karin, Marjolein, Ayso, Sebastiaan, Anneke, Rosemarie, Jochem en Wytze (niet echt G1,
maar toch een beetje), en natuurlijk Mirjam, Sabine, Sandra en Annemarie, dank jullie wel voor de
gezelligheid, lunches, hulp, steun, en samenwerking. Mirjam, ik heb heel veel bewondering voor
je. Anneke, ik ben blij dat een vrouw met zoveel lef en karakter naast me wilt staan. Ook mijn
oude kamergenote Corinne, en natuurlijk Frans, dank jullie beiden voor alles, vooral voor het eten,
dat ik mocht opeten, als Corinne weer eens nachtdienst had. Brigitte, dank voor het bellen van
alle voorzitters van de oncologiecommissies, heel veel succes in Breda. Ook alle andere collega’s
van de afdeling Radiologie, die voor de prettige en leuke sfeer zorgen, wil ik bedanken, in het
bijzonder Onno. Wat een hoop ellende heb ik je aangedaan met het “SAS” programma (Sorry).
Ook oud-collega’s en studenten, dank voor de leuke tijd, in het bijzonder Marjon en Rogier (D).
Cristina, bedankt voor de tip over de titel.
Petra en Gre van de klinische epidemiologie, Jolanda Dijkstra, Eveline Goldberg, wil ik bedanken
voor feit dat ze altijd bereid waren/zijn om een afspraak te regelen. Ook dank aan alle andere
(ex-)collega’s van de klinische epidemiologie, in het bijzonder, Afina, Jeroen, en Anne “de kern
van de diagnostiek”.
Prof. dr. G.J. den Heeten, beste Ard, als er ooit een muizen-MRI komt, dan zal ik daar aan werken.
Dank je wel dat je mij bij Jaap hebt ondergebracht.
Prof. dr. J.S. Laméris, dank voor de mogelijkheden die u mij heeft geboden om me in de afgelopen
jaren als onderzoeker te ontwikkelen. Veel dank voor het nemen van het risico op het gebied van
evidence-based radiologie en dat u bereid bent om zitting te nemen in de beoordelingscommissie
en promotiecommissie. Ook de overige leden Prof. dr. M.P.M. Burger, Prof. dr. D.J. Gouma, Prof.
dr. M.G.M. Hunink, Prof. dr. W.P.Th. M. Mali, Prof. dr. H.C.W. de Vet wil ik bedanken voor het
feit dat ze zitting hebben willen nemen in de beoordelingscommissie en promotiecommissie.
Mijn dierbare vrienden Michèle, Stephan, Ronald, Marianna, Brenda, Justin, Eddy, Sery, Ange-
lique, Werner, Franca, Ronald (van Franca), Laura en Thom, Dominique, en natuurlijk ook Heleen,
wil ik bedanken voor alle mooie en bijzondere momenten en voor de steun en gezelligheid. Do,
zelfs als ik je opsluit in mijn huis wil je nog terugkomen. En natuurlijk Adrie en Fania, dank jul-
lie wel voor alle etentjes, logeerpartijtjes en voor de mooie momenten, bijv. het gesprek in de
McDonald’s was een mooi moment (7 jaar geleden?).
Mijn nichtjes en neefjes, in het bijzonder Sharmila, wil ik bedanken voor de leuke tijd.
Dankwoord
��6��6

Dankwoord
��7
Mijn familie wil ik bedanken voor de warme, liefdevolle en zorgeloze jeugd. Tja, ik ging op mijn
18de verhuizen en daarna emigreren. Het gaat inderdaad om wie je bent en niet om wat je bent.
Het is iedere keer weer triest om na een bezoek afscheid van jullie te moeten nemen. Ik mis jullie
dan ook heel erg.
Mijn pleegouders, dank jullie wel dat jullie er altijd voor me zijn. Mijn ouders hebben inderdaad
gelijk, echte liefde heeft niks met papieren te maken. Lieve Mischa, ik hoop dat het in Engeland
allemaal voorspoedig gaat en dat je snel terugkomt. Ik ben dan ook heel blij dat je nu ook, net als
toen, naast me wilt staan. Hoon, Peter, Sun, Wendy, Cecilia, Barry en uiteraard mijn ooms Rein
en Hans, bedankt dat jullie zo lief, attent en zorgzaam zijn.
Mijn schoonouders, John en Hannie, mijn schoonzusjes, Mar en Roos, en natuurlijk Ark en Robert,
bedankt voor jullie gezelligheid, interesse, steun en vooral voor de zorgzaamheid. Mar, ik denk
dat ik een goede oppas ben. Ik ben echt heel blij met jullie als schoonfamilie.
Tot slot, mijn Danny. Het is geweldig om zo’n lief, schattig, behulpzaam, eerlijk en oprecht maatje
te hebben. Zelfs in de meest stressvolle periode heb jij aandacht en tijd voor mij. Zoals je zelf zei:
“Jij hebt… and me”. Jou schattebout ;-)

��� ���

��� ���
Curriculum Vitae
Shandra Bipat is op 19 september 1973 geboren in Nickerie, Suriname. Na het VWO en pro-
pedeuse geneeskunde is zij geëmigreerd naar Nederland, waar zij in 1994 is begonnen aan de
studie “Medische Biologie” aan de Vrije Universiteit in Amsterdam, met als specialisatie “Medi-
sche Oncologie”. De doctoraalfase werd afgerond in augustus 1998. Na een tussenstop voor
oriëntatiecursussen/stages is zij sinds augustus 1999 werkzaam bij de afdeling Radiologie van het
Academisch Medisch Centrum, eerst bij de administratie – tot mei 2000 – en daarna als onderzoe-
ker. In de periode tussen januari 2003 en juni 2005 heeft ze een postacademische Epidemiologie
opleiding gevolgd aan het EMGO instituut van de Vrije Universiteit.
Tijdens de periode 2000 - heden heeft zij onder leiding van Prof. dr. J. Stoker (Radioloog) en Prof.
dr. P.M.M. Bossuyt (Klinisch Epidemioloog en Methodoloog) met name onderzoek gedaan naar
de waarde van verschillende diagnostische modaliteiten bij verschillende maligniteiten, aan de
hand van het beschikbare wetenschappelijke bewijs, met als doel evidence-based aanbevelingen
te doen voor de praktijk.
Na haar promotie zal zij als onderzoeker werkzaam blijven op de afdeling Radiologie van het
AMC.
���

�00 PB