Embed Size (px)
Citation preview

USING THE PROXIMAL PERFORATOR-BASED ANTEROLATERALTHIGH FLAP FROM THE SAME DONOR SITE TO SALVAGE THERECONSTRUCTION AFTER FAILURE OF THE DISTALPERFORATOR-BASED ANTEROLATERAL THIGH FLAP
KUN-HAN CHEN M.D., HAW-YEN CHIU M.D., Ph.D., JING-WEI LEE M.D., SHYH-JOU SHIEH M.D., Ph.D., and
YAO-CHOU LEE M.D.*
We presented a patient who experienced the anterolateral thigh (ALT) flap failure but the reconstruction was successfully salvaged by har-vesting a second ALT flap from the same donor site 2 days after the first reconstruction. A 47-year-old man received cancer ablation forright mouth floor squamous cell carcinoma. The resultant defect was planned to be reconstructed with the ALT flap. During the flap dis-section, we identified three proximal cutaneous perforators originating from the transverse branch of the lateral circumflex femoral artery(t-LCFA) and two distal cutaneous perforators originating from the descending branch (d-LCFA). We harvested a skin flap based on thedistal two perforators and divided the d-LCFA just distal to the bifurcation of the d-LCFA and the t-LCFA. Unfortunately, the ALT flapshowed venous congestion on postoperative day 2 and eventually failed. We harvested a second ALT flap from the same donor sitebased on the previously preserved perforators. The recovery course was smooth thereafter. We believe that the harvest of a secondALT flap from the same donor site may be an option, to avoid other donor site violation, in some patients who experienced the first flaploss. VC 2014 Wiley Periodicals, Inc. Microsurgery 34:409–412, 2014.
The anterolateral thigh (ALT) flap has been renowned
for a variety of advantages such as long pedicle length,
large caliber, versatility in volume and contents, and
minimal donor site morbidity since its first introduction
by Song et al. in 1984.1 The perforators of the ALT flap
were reported from the descending branch of the lateral
circumflex femoral artery (d-LCFA) in 67.6% and from
the transverse branch (t-LCFA) in 32.4%.2 Yu further
categorized the perforators of the ALT flap into perfora-
tor “A,” perforator “B,” and perforator “C” by defining
the “B” perforators located around the midpoint between
anterior superior iliac spine and superolateral patella, “A”
perforators about 5 cm proximal to the midpoint, and
“C” perforators about 5 cm distal to the midpoint.3 Clini-
cally, we usually can identify more than one perforators
originating from the same or different source vessels and
theoretically capable to harvest an ALT flap with multi-
ple skin paddles. Reconstruction of separate defects with
two or three skin paddles from one ALT donor site has
been reported to be a useful technique.4–9 Of those cases,
multiple skin flaps from one ALT donor site were always
harvested in a simultaneous fashion.
Herein, we presented a patient who experienced the
ALT flap failure but the reconstruction was successfully
salvaged by harvesting a second ALT flap from the same
donor site 2 days after the first reconstruction.
CASE REPORT
A 47-year-old man with diagnosis of right mouth
floor squamous cell carcinoma was presented. The result-
ant intraoral defect was 14 3 6 cm2 after cancer ablative
surgery. During the left ALT flap dissection, we identi-
fied five cutaneous perforators which included two “A”
perforators, one “B” perforator, and two “C” perforators.
We performed retrograde dissection to clarify the source
vessel of each perforator and found that the “A” and “B”
perforators were originated from the t-LCFA whereas the
“C” perforators were from the d-LCFA. We designed a
fasciocutaneous flap (14 cm 3 6 cm) based on these two
“C” perforators to reconstruct the intraoral defect (Fig.
1). The flap edges showed fresh bleeding before the pedi-
cle division. We divided the pedicle vessels just distal to
the bifurcation of the d-LCFA and the t-LCFA and a 19-
cm pedicle length was obtained. The “A” and “B” perfo-
rators and the t-LCFA were well preserved. The pedicle
artery and vein were anastomosed in an end-to-end fash-
ion with right superior thyroid artery and right external
jugular vein, respectively. The donor site was closed pri-
marily. Unfortunately, the flap showed venous congestion
on postoperative day 2. In the salvage operation, the flap
still showed poor capillary refill and diminished venous
backflow after thrombectomy and flap milking. There-
fore, we decided to harvest a second ALT flap from the
same donor site by using the previously preserved “A”
Division of Plastic and Reconstructive Surgery, Department of Surgery,National Cheng Kung University Hospital, College of Medicine, NationalCheng Kung University, Tainan, Taiwan.
*Correspondence to: Yao-Chou Lee, MD, Attending Plastic Surgeon, Divisionof Plastic and Reconstructive Surgery, Department of Surgery, NationalCheng Kung University Hospital, 138 Sheng-Li Rd., Tainan 70403, Taiwan.E-mail: [email protected]
Received 15 July 2013; Revision accepted 2 January 2014; Accepted 6January 2014
Published online 18 January 2014 in Wiley Online Library(wileyonlinelibrary.com). DOI: 10.1002/micr.22227
� 2014 Wiley Periodicals, Inc.
and “B” perforators which were originated from the t-
LCFA (Fig. 2). A bulky skin flap in the size of 18 cm 3
7 cm with a pedicle length of 7 cm was obtained. The
bulkiness of this proximal perforator-based ALT flap was
reduced by immediate thinning procedure. The shortage
of the pedicle length was overcome by proximal de-
epithelialization of the skin paddle. The pedicle artery
was anastomosed to right superior thyroid artery in an
end-to-end fashion and the pedicle vein was anastomosed
with right internal jugular vein in an end-to-side fashion.
The donor site was closed primarily again. The patient
was discharged uneventfully after 21 days of hospitaliza-
tion. The follow-up 3 months later showed satisfactory
results (Fig. 3).
DISCUSSION
Simultaneous reconstruction of separate defects by
using multiple skin paddles from one ALT donor site has
been proved to be a feasible and effective method. Com-
plex pharyngoesophageal defects could be reconstructed
with a single ALT flap that was divided into two skin
islands based on separate cutaneous perforators: one for
esophageal reconstruction and the other for external neck
defect or as a monitor flap.4,5 Two independent flaps
from one single ALT flap donor site were also able to be
harvested to reconstruct two separate defects either on
the lower extremity or in the oral cavity.6,7 Peng et al.
successfully applied this technique to reconstruct two
separate defects in the upper extremity at the same time.8
Tripaddled ALT flap for simultaneous reconstruction of
bilateral buccal defects after buccal cancer ablation and
severe oral submucous fibrosis release was also success-
fully performed in a patient with three widely separated
perforators on the ALT donor site.9 All the aforemen-
tioned reports described that multiple skin flaps from one
ALT donor site could be simultaneously harvested if two
or more cutaneous perforators were available. In our
report, we showed that a second ALT flap may be har-
vested from the same donor site in a delayed fashion.
In our case, the ALT flap vascular anatomy showed
the presence of two proximal “A” perforators, one mid-
dle “B” perforator, and two distal “C” perforators. The
“A” and “B” perforators were originated from the t-
LCFA and the “C” perforators were originated from the
d-LCFA. It was feasible to harvest an ALT flap based on
the “A” and “B” perforators with the t-LCFA or the “C”
perforators with the d-LCFA. We decided to design an
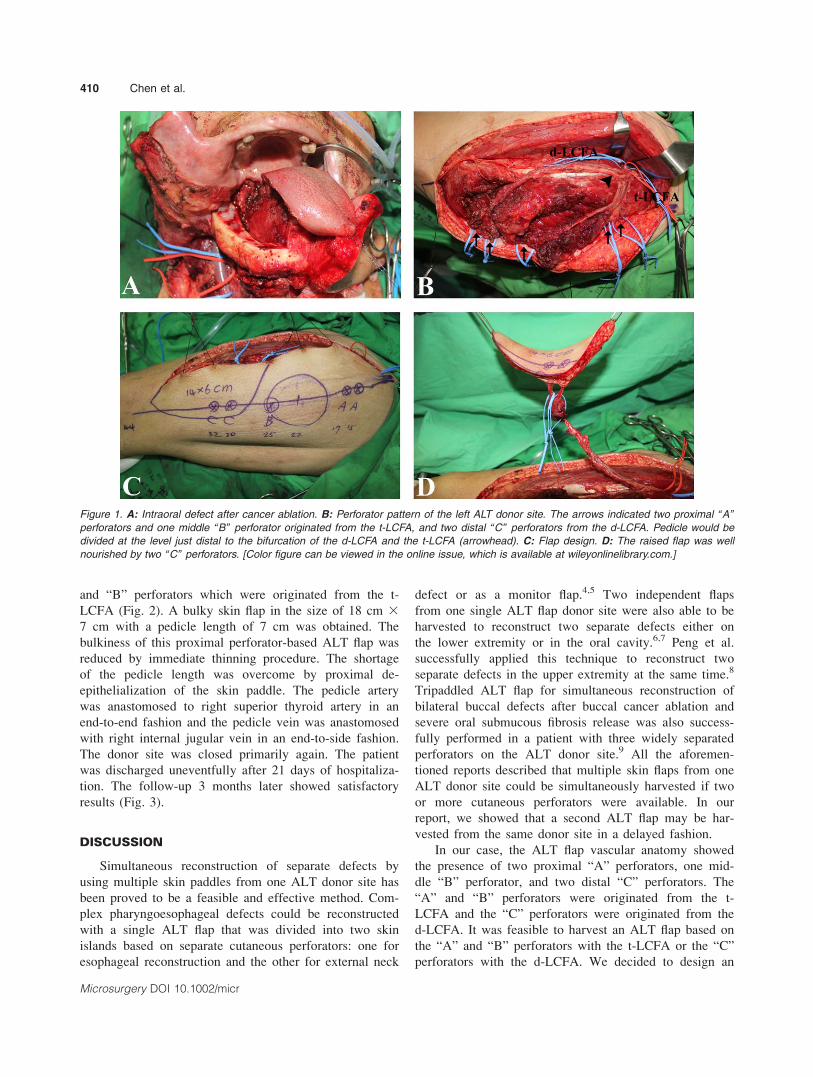
Figure 1. A: Intraoral defect after cancer ablation. B: Perforator pattern of the left ALT donor site. The arrows indicated two proximal “A”
perforators and one middle “B” perforator originated from the t-LCFA, and two distal “C” perforators from the d-LCFA. Pedicle would be
divided at the level just distal to the bifurcation of the d-LCFA and the t-LCFA (arrowhead). C: Flap design. D: The raised flap was well
nourished by two “C” perforators. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
410 Chen et al.
Microsurgery DOI 10.1002/micr
ALT flap based on the distal “C” perforators at the first
reconstructive surgery because the distal ALT flap was
thin and pliable to avoid disturbing tongue mobility.
Traditionally, we divide the pedicle vessels just distal
to the branch to the rectus femoris muscle to avoid the
complication of rectus femoris muscle necrosis and to
obtain a sufficient pedicle length and caliber.10,11 How-
ever, in this case, we intentionally divided the pedicle
more distally to preserve another three perforators origi-
nating from the t-LCFA. Although additional 2–3 cm
pedicle length can be obtained if we sacrificed the “A”
and “B” perforators originating from the t-LCFA, the
selection of “C” perforators originating from the d-LCFA
already allowed us to obtain a lengthy pedicle which was
19 cm in our case. Because the pedicle reached to the
recipient vessels without difficulty, we believed that the
shorter than usual pedicle by preservation of the “A” and
“B” perforators did not responsible for the flap loss in
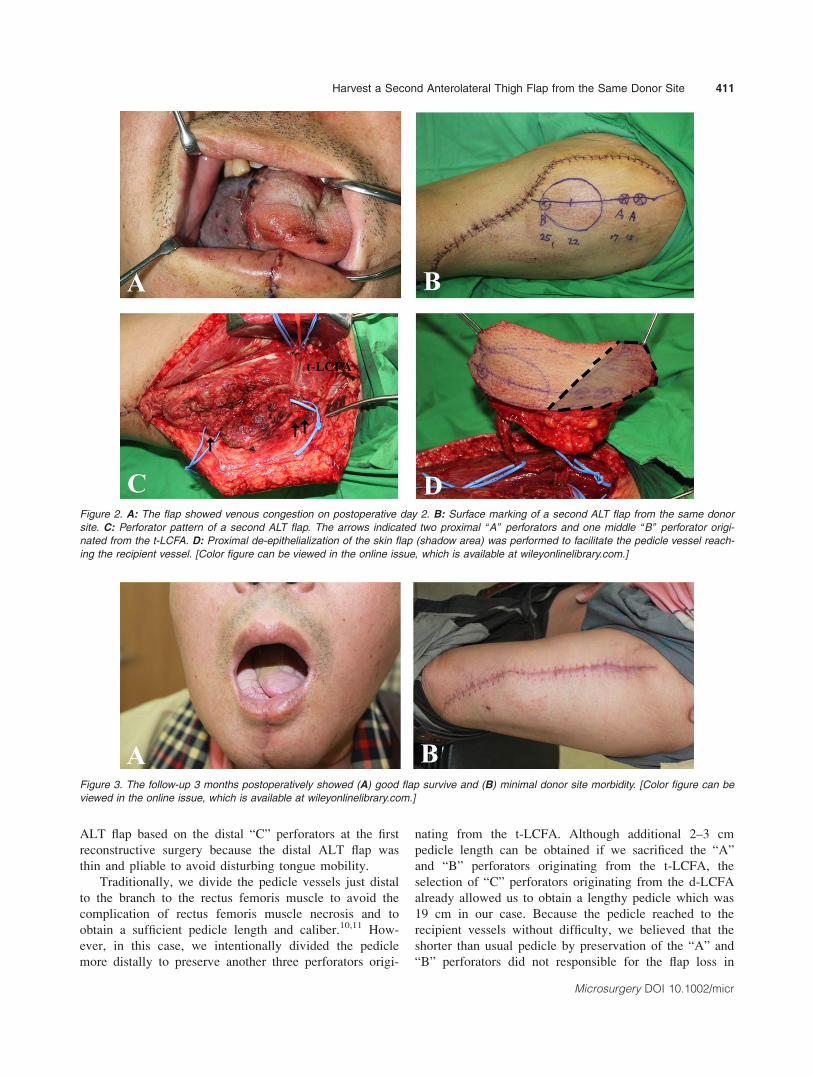
Figure 2. A: The flap showed venous congestion on postoperative day 2. B: Surface marking of a second ALT flap from the same donor
site. C: Perforator pattern of a second ALT flap. The arrows indicated two proximal “A” perforators and one middle “B” perforator origi-
nated from the t-LCFA. D: Proximal de-epithelialization of the skin flap (shadow area) was performed to facilitate the pedicle vessel reach-
ing the recipient vessel. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Figure 3. The follow-up 3 months postoperatively showed (A) good flap survive and (B) minimal donor site morbidity. [Color figure can be
viewed in the online issue, which is available at wileyonlinelibrary.com.]
Harvest a Second Anterolateral Thigh Flap from the Same Donor Site 411
Microsurgery DOI 10.1002/micr

our case. Surprisingly, this decision allowed us to have a
second chance to harvest another ALT flap from the
same donor site after flap failure in this patient.
However, the proximal perforator-based ALT flap had
the disadvantages of bulkiness and short pedicle length.
In order not to violate other donor site, we still decided
to harvest the second ALT flap from the same donor site.
The flap bulkiness was reduced by immediate thinning
procedures. The drawback of short pedicle length was
overcome by harvesting a longer flap with proximal de-
epithelialization of the skin paddle to facilitate the pedi-
cle vessel reaching the recipient vessel.
We believe that this is the first case showing the har-
vest of a second ALT flap from the same donor site in a
delayed fashion in the scenario of first flap failure. By
doing this, additional donor site violation could be mini-
mized. However, it seems premature to recommend this
technique after just one case. In addition, the harvest of
a second ALT flap from the same donor site has some
limitations. First, if only single perforator could be iden-
tified in the ALT donor site, harvest of a second ALT
flap would be impossible. Second, if the defects required
a large ALT flap, harvest of another large flap from the
same donor site would be infeasible. Third, harvest of a
second flap based on another set of intentionally pre-
served vascular system in a delayed fashion may be diffi-
cult due to severe scarring. The harvest of a second ALT
flap from the same donor site in a delayed fashion should
take these into considerations in the circumstance of sal-
vage of reconstruction after failure of the first ALT flap.
REFERENCES
1. Song YG, Chen GZ, Song YL. The free thigh flap: A new free flapconcept based on the septocutaneous artery. Br J Plast Surg 1984;37:149–159.
2. Shieh SJ, Chiu HY, Yu JC, Pan SC, Tsai ST, Shen CL. Free antero-lateral thigh flap for reconstruction of head and neck defects follow-ing cancer ablation. Plast Reconstr Surg 2000;105:2349–2357.
3. Yu P. Characteristics of the anterolateral thigh flap in a Westernpopulation and its application in head and neck reconstruction. HeadNeck 2004;26:759–769.
4. Yu P. One-stage reconstruction of complex pharyngoesophageal, tra-chea, and anterior neck defects. Plast Reconstr Surg 2005;116:949–956.
5. Tan NC, Yeh MC, Shih HS, Nebres RP, Yang JC, Kuo YR. Singlefree anterolateral thigh flap for simultaneous reconstruction of com-posite hypopharyngeal and external neck skin defect after head andneck cancer ablation. Microsurgery 2011;31:524–528.
6. Chou EK, Ulusal B, Ulusal A, Wei FC, Lin CH, Tsao CK. Using thedescending branch of the lateral femoral circumflex vessel as a sourceof two independent flaps. Plast Reconstr Surg 2006;117:2059–2063.
7. Huang JJ, Wallace C, Lin JY, Tsao CK, Kao HK, Huang WC,Cheng MH, Wei FC. Two small flaps from one anterolateral thighdonor site for bilateral buccal mucosa reconstruction after release ofsubmucous fibrosis and/or contracture. J Plast Reconstr Aesthet Surg2010;63:440–445.
8. Peng F, Chen L, Han D, Xiao C, Bao Q, Wang T. Reconstruction oftwo separate defects in the upper extremity using anterolateral thighchimeric flap. Microsurgery 2013;33:631–637.
9. Jiang C, Guo F, Li N, Huang P, Jian X, Munnee K. Tripaddledanterolateral thigh flap for simultaneous reconstruction of bilateralbuccal defects after buccal cancer ablation and severe oral submu-cous fibrosis release: A case report. Microsurgery 2013;33:667–671.
10. Agostini T, Lazzeri D, Spinelli G. Anterolateral thigh flap: system-atic literature review of specific donor-site complications and theirmanagement. J Craniomaxillofac Surg 2013;41:15–21.
11. Kimata Y, Uchiyama K, Ebihara S, Sakuraba M, lida H, NakatsukaT, Harii K. Anterolateral thigh flap donor-site complications andmorbidity. Plast Reconstr Surg 2000;106:584–589.
412 Chen et al.
Microsurgery DOI 10.1002/micr





























