Embed Size (px)
Citation preview

UR
Appti7t
FGMDYDTTUA
Ra
RDCSa
0©d
Reviews www.AJOG.org
5
se of metformin in polycystic ovary syndrome
uchi Mathur, MD; Carolyn J. Alexander, MD; Jacqueline Yano, MA; Bradley Trivax, MD; Ricardo Azziz, MD, MPH, MBAifiectotaclaatpP5Imt
buftdtn
topimmoclvtP
IIh6ofspphcrmurptlt
IogdidllhcptgsPw
lthough it was in 1935 when Stein andLeventhal1 first published their re-
ort describing what is now called theolycystic ovary syndrome (PCOS), it ishe last 2 decades that has seen a flurry ofnterest in the disorder. PCOS affects-10% of reproductive-aged women,2,3 ishe most common cause of oligoovulatory
rom the Department of Obstetrics/ynecology, Department of Medicine (Drathur), and Center for Androgen-Relatedisorders (Drs Mathur and Azziz, and Msano), Cedars-Sinai Medical Center; andepartments of Obstetrics/Gynecology (Drsrivax and Azziz) and Medicine (Dr Azziz),he David Geffen School of Medicine atniversity of California Los Angeles, Losngeles, CA
eceived April 22, 2008; revised July 29, 2008;ccepted Sept. 3, 2008.
eprints: Ricardo Azziz, MD, MPH, MBA,epartment of Obstetrics/Gynecology,edars-Sinai Medical Center, 8635 W. Thirdt., Suite 160W, Los Angeles, CA [email protected].
002-9378/free2008 Published by Mosby, Inc.
oi: 10.1016/j.ajog.2008.09.010
For Editors’ Commentary,
Women with polycystic ovary syndrome (PCfeatures that may guide therapeutic optiinduction. The use of metformin may provwomen with PCOS. Hyperinsulinemia, as2-hour 75-g load glucose tolerance test, isor not to initiate metformin therapy to womdelaying the onset of type 2 diabetes mellitumarkers of subclinical inflammation, andformin therapy. For ovulation induction, mcitrate as first-line therapy for women withmetformin reduces pregnancy loss or impcurrently recommended that metformin betest result, unless there are other medicaaddresses practical management guidelinePCOS.
Key words: infertility, insulin resistance, mpregnancy
osee Table of Contents
96 American Journal of Obstetrics & Gynecology
nfertility, and accounts for a significantraction of health care costs.4 The disorders generally considered to exhibit androgenxcess, ovulatory dysfunction, and poly-ystic ovaries, and is diagnosable afterhe exclusion of related ovulatory orther androgen excess disorders (eg,
hyroid dysfunction, hyperprolactinemia,ndrogen-secreting neoplasms, or non-lassic adrenal hyperplasia). Hyperinsu-inemia is a cornerstone of both the met-bolic syndrome and of PCOS, and isssociated with a high risk of developingype 2 diabetes mellitus (DM). In com-arison with women who do not haveCOS, the prevalence of type 2 DM is-10 times higher in women with PCOS.n addition to lifestyle modification,
etformin has been proposed to reducehe risk of DM in women with PCOS.
Infertility is also a common issue facedy women with PCOS, most often attrib-ted to anovulation. In addition, other
actors may be operant in PCOS to lowerhese women’s fertility, including re-uced oocyte quality, defects in endome-rial development, and implantation ab-ormalities.5 However, the primary goal
) have a myriad of phenotypic and clinicalfor metabolic protection and ovulation
eneficial in a subset of the population ofonstrated by elevated insulin levels on aimportant parameter in deciding whether
with PCOS with the hope of preventing orDM). Cardiovascular risk factors includinglipidemia may also be improved by met-formin is not as effective as clomipheneS. There are no clear data to suggest thats pregnancy outcome in PCOS, and it isontinued with the first positive pregnancy
ndications (eg, type 2 DM). This reviewor the uses of metformin in women with
ormin, polycystic ovary syndrome,
f treatment for PCOS-associated infer- s
DECEMBER 2008
ility continues to be the restoration ofvulation. Several approaches have beenroposed for the restoration of ovulation
n women with PCOS, including lifestyleodifications, clomiphene citrate (CC),etformin, ovarian drilling, and gonad-
tropins. In this review, we will providelinically relevant management guide-ines for the role of metformin in the pre-ention of metabolic morbidities and thereatment of infertility in women withCOS.
nsulin resistance in PCOSnsulin resistance (IR) and secondaryyperinsulinemia affect approximately5-70% of women with PCOS.6,7 Manyf these women are also obese, whichurther exacerbates their IR. Insulintimulates ovarian theca cell androgenroduction and secretion, and sup-resses the hepatic production of sexormone-binding globulin. The in-reased intraovarian androgens then dis-upt folliculogenesis.8 Hyperinsulinemiaay also directly cause premature follic-
lar atresia and antral follicle arrest.9 Theesulting anovulation also leads to unop-osed estrogen production and endome-rial proliferation in women with PCOS,eading to an increased risk of endome-rial hyperplasia.
Consistent with the high prevalence ofR and obesity, patients with PCOS dem-nstrate a greater prevalence of impairedlucose tolerance (IGT),10 type 2 DM,11
yslipidemia, and chronic subclinicalnflammation.12,13 Recognition of aysmetabolic pattern of elevated trig-
ycerides, modestly altered low-densityipoprotein (LDL), and decreasedigh-density lipoprotein (HDL)14,15 islinically important when counselingatients regarding lifestyle modifica-ions and in following up patients lon-itudinally as a baseline for compari-on. In addition, many patients withCOS demonstrate features consistentith the metabolic (or dysmetabolic)
OSonse bdem
anens (
dyset
PCOrovediscl is f
etf
yndrome.16

C
TDWitaUbprPuthsf5dsIalbt
TTpvuwtiabodmwzt
prwwidr
MMufpcrobwsiibemfmim
C
MMdu
DDhtcsfcwg
mtvcccowntfggvthn
a1PdpaYmlrlbseGt2coteld
sm
www.AJOG.org Reviews
linical considerations
1. The practical management of met-abolic syndrome in women withPCOS must include tight bloodpressure control, weight loss, dietmodification, and possibly the useof agents for lipid modification.
2. As with other cases of oligomenor-rhea, women with IR and subse-quent oligomenorrhea should beconsidered for endometrial biopsy,particularly if a thickened endome-trial stripe (� 10 mm) is seen onultrasound.
reatment of IR in PCOSietary restrictioneight reduction is a critical component
n the treatment of PCOS, particularly inhe 60-70% of women with PCOS whore overweight or obese, at least in thenited States. Weight reduction haseen shown to normalize ovulation, im-rove hyperandrogenism, and increaseates of conception in women withCOS.17 Although IR is a major contrib-ting factor in the resultant abnormali-
ies seen in PCOS, restriction of carbo-ydrates in particular has not beenhown to have a distinctive benefit overat restriction.11 Women who lose even-10% of their total body weight can re-uce central fat up to 30%, improve in-ulin sensitivity, and restore ovulation.18
ncreased physical activity and exercise islso an important component of healthyifestyle, and evidence exists to supportenefit for the metabolic disturbancesypically seen in PCOS.19
hiazolidinedioneshiazolidinediones (TZDs) (includingioglitazone, rosiglitazone, and the pre-iously used troglitazone) have beensed in PCOS to reduce IR. Obeseomen with PCOS who were adminis-
ered troglitazone demonstrated benefitn insulin sensitivity, glucose tolerance,nd hyperandrogenemia.20,21 A double-lind placebo-controlled trial, in whichvulation increased, testosterone levelsecreased, and glycemic parameters nor-alized in a dose-dependent manner inomen with PCOS treated with troglita-
one, confirmed previous findings.22 Al-
hough TZDs have been considered to aaradoxically induce weight gain, moreecent data suggest that TZDs in womenith PCOS may not cause as mucheight gain as first anticipated.23 In clin-
cal practice, the use of TZDs in repro-uctive-aged women with PCOS is notoutinely advocated.
etforminetformin is currently the most widely
sed drug worldwide for the treatmentor type 2 DM. Its primary action ap-ears to be an inhibition of hepatic glu-ose production and an increase in pe-ipheral insulin sensitivity. The benefitsf metformin on insulin sensitivity haveeen demonstrated in non-DM womenith PCOS. The use of metformin is as-
ociated with increased menstrual cyclic-ty, improved ovulation, and a reductionn circulating androgen levels.24 Meta-olic benefits are enhanced in the pres-nce of weight loss, and weight loss itselfay be enhanced in the presence of met-
ormin.25 Below, we discuss further theechanisms of action of metformin and
ts clinically relevant role in the treat-ent of PCOS.
linical considerations
1. Women who lose even 5-10% oftheir total body weight can reducecentral fat up to 30%, improve in-sulin sensitivity, and restore ovula-tion. Lifestyle intervention shouldbe the cornerstone of therapy.
2. In clinical practice, the use of TZDsin reproductive-aged women withPCOS is not recommended rou-tinely.
3. The initiation of metformin may beconsidered in women with PCOSwho exhibit abnormal results onthe 75-g load oral glucose tolerancetest (OGTT), but do not meet thecriteria for DM.
4. In a subset of patients with oligo-menorrheic PCOS, the initiation ofmetformin will instigate regularmenstrual cycles.
etformin: mechanisms of actionetformin (1,1-dimethylbuguanide hy-
rochloride) is a biguanide currentlysed as an oral antihyperglycemic agent,
nd is approved by the US Food and sDECEMBER 2008 Am
rug Administration to manage type 2M. Its primary clinical action is to in-ibit hepatic glucose production, al-hough it also decreases intestinal glu-ose uptake and increases insulinensitivity in peripheral tissues. Met-ormin has antilipolytic effects, loweringirculating free fatty acid concentrations,hich ultimately aids in reducingluconeogenesis.26,27
Metformin activates the adenosineonophosphate (AMP)-activated pro-
ein kinase pathway (AMPK), both initro and in vivo,28,29 resulting in de-reased glucose production and in-reased fatty acid oxidation in hepato-ytes, skeletal muscle cells,30 and mousevarian tissue.31 The mechanism byhich metformin activates the AMPK isot clear; however, phosphorylation of
hreonine in AMPK is necessary for met-ormin’s action.30 A recent study sug-ests that metformin inhibits hepaticluconeogenesis through an AMP-acti-ated protein kinase-dependent regula-ion of the orphan nuclear receptor smalleterodimer partner (SHP),32 althoughot all investigators agree.33
Metformin is available as 500-, 850-,nd 1000-mg tablets with a target dose of500-2550 mg per day. Many studies inCOS have used a dose of 850 mg twice aay for 6 months. A sustained releasereparation is also available (Glucoph-ge-XR; Bristol-Myers Squibb, Nework, NY). Side effects of metformin areainly gastrointestinal (GI) and are
isted in Table 1, although the sustainedelease preparation may have an overallower rate of side effects. Metformin isest taken on an empty stomach. Theustained release is usually taken with thevening meal. To reduce the incidence ofI side effects, it is recommended that
he dose of metformin is started low (eg,50-500 mg/day) and then gradually in-reased during a period of 4-6 weeks. It isur experience that patients who do notolerate metformin because of its GI sideffects may benefit from the extended re-ease formulation, albeit given in dividedoses.Because metformin may cause malab-
orption of vitamin B12, patients takingetformin should be monitored for
igns and symptoms of vitamin B12 de-
erican Journal of Obstetrics & Gynecology 597

fisiAjMwtmfMtty
MaMDoag(Awtoshmhwp
wbwmaapscPw
C
MoMpwitdtphrtpwoepm
hewtocPaIiaod
bobw
aoltsmaPLsr7sg3gtgqd
MfMttbaPmsa2nnahsImp(ccosfc
n
Reviews www.AJOG.org
5
ciency including numbness, paresthe-ia, macroglossia, memory loss, behav-oral changes, and pernicious anemia.24
lthough lactic acidosis is cited as a ma-or concern, it is a rare complication.
etformin should not be prescribed toomen with renal insufficiency, conges-
ive heart failure, or sepsis,34 or be ad-inistered to patients with hepatic dys-
unction or a history of alcohol abuse.24
etformin is indicated in patients olderhan 10 years, and the sustained prepara-ion is indicated in those older than 17ears.
etformin as treatment for PCOS-ssociated subfertilityetformin, body weight, and fertilityuring preconception counseling ofbese patients with PCOS, weight loss isn important recommendation with theoal of decreasing gestational DMGDM) and perinatal complications.necdotally, Glueck et al35 reported thatomen with PCOS who conceived while
aking metformin had a lower likelihoodf developing GDM. An informativetudy designed to evaluate the effects of aypocaloric diet combined with 6onths of metformin (1700 mg/day) vs
ypocaloric diet and placebo in 20 obeseomen with PCOS and the abdominal
TABLE 1Side effects of metforminGastrointestinalside effects
DiarrheaNauseaVomitingBloatingAbdominal discomfortFlatulenceIndigestionConstipationHeartburnUnpleasant metallic tastein mouth
...........................................................................................................
Other sideeffects
SneezingCoughRunny noseFlushing of skinNail changes
...........................................................................................................
Rare sideeffects
Lactic acidosisChest painRash
...........................................................................................................
Mathur. Use of metformin in polycystic ovarysyndrome. Am J Obstet Gynecol 2008.
henotype and 20 obese women who c
98 American Journal of Obstetrics & Gynecology
ere comparable for age and pattern ofody fat distribution but without PCOSas conducted.36 The combination ofetformin and hypocaloric diet inducedgreater reduction in body weight and
bdominal fat, particularly visceral de-osits, and a more consistent decrease inerum insulin, testosterone, and leptinoncentrations in the obese women withCOS and abdominal obesity comparedith control subjects.
linical considerations
1. In clinical practice, close follow-upof patients with monitoring of theirweight at each visit and food diarieshas motivated patients to maintainweight loss and the addition ofmetformin has improved their hy-perinsulinemia and appears to de-crease their appetite.
etformin alone for the treatmentf subfertilityetformin likely plays its role in im-
roving ovulation induction in womenith PCOS through a variety of actions,
ncluding reducing insulin levels and al-ering the effect of insulin on ovarian an-rogen biosynthesis, theca cell prolifera-ion, and endometrial growth. Also,otentially through a direct effect, it in-ibits ovarian gluconeogenesis and thuseduces ovarian androgen produc-ion.37-39 In determining which clinicalarameters may predict which patientsill benefit most from metformin forvulation induction, fasting insulin lev-ls and glucose to insulin ratios do notredict the ovulatory response toetformin.40
In a meta-analysis, metformin aloneas been shown to have a significant ben-fit on inducing ovulation in womenith PCOS, but there is limited evidence
hat it improves pregnancy rates.41 An-ther meta-analysis of 17 randomizedontrol trials (n � 1639 patients withCOS) compared metformin vs placebo,nd CC alone vs metformin plus CC.42
n a pooled statistical estimate compar-ng metformin with placebo, metforminlone statistically improved the odds ofvulation (odds ratio [OR], 2.94), butid not statistically improve the rate of
linical pregnancy (OR, 1.56) or live wDECEMBER 2008
irth rate (OR, 0.44). With regard tovulation metformin alone appeared toe more effective in non-CC-resistantomen.42
Alternatively, metformin alone is nots effective as CC alone for the treatmentf infertility in women with PCOS. In the
argest study to date of more than 600herapeutically naïve women with PCOSeeking fertility randomized to treat-
ent with metformin alone, CC alone,nd metformin and CC combined (theregnancy in PCOS [PPCOS] trial),egro et al41 reported that CC alone re-ulted in significantly greater live birthates than metformin alone, 22.5% vs.2%. Of note, multiple births were onlyeen with CC therapy (6.0% in the CCroup, 0% in the metformin group, and.1% in the combination therapyroup). Assuming that the goal of infer-ility treatment is to achieve a singletonestation, it may be argued that CC is notuite as successful as suggested by theata of the PPCOS trial.37
etformin in combination with CCor the treatment of subfertility
etformin has been suggested for thereatment of PCOS oligoovulatory infer-ility, either alone (see above), or in com-ination with dietary restriction (seebove), CC, or gonadotropins. In thePCOS trial, Legro et al41 reported thatetformin alone was significantly less
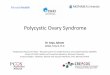
uccessful than the combination of CCnd metformin (live birth rates 7.2% vs6.8%) (Figure 1). However, the combi-ation of metformin and CC was not sig-ificantly different from the rate of CClone (see above). Other investigatorsave confirmed these data in somewhatmaller, albeit randomized studies.43,44
n a meta-analysis, the combination ofetformin and CC significantly im-
roved ovulation and pregnancy ratesOR, 4.39 and 2.67, respectively) whenompared with CC alone. However,ombined therapy did not improve thedds of live birth (OR, 2.01). The resultsuggested combination therapy (met-ormin plus CC) as the treatment ofhoice in CC-resistant women.42
In contrast to its use in therapeuticallyaive patients, it is possible that women
ho have failed to ovulate with CC (ie,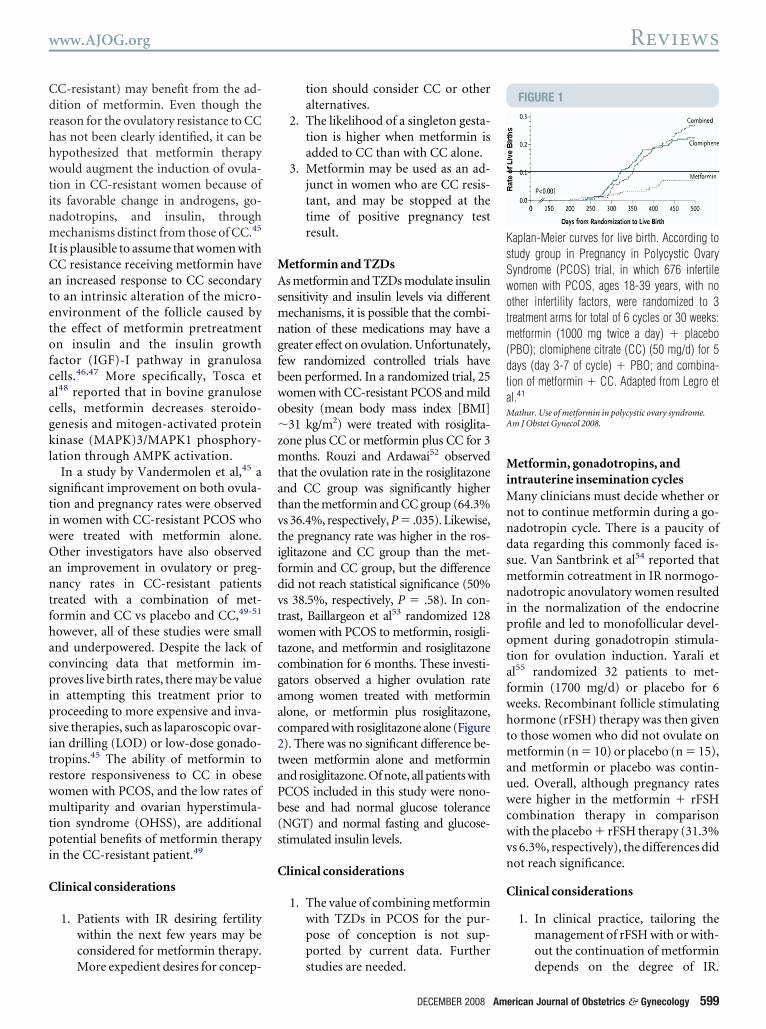
CdrhhwtinmICatetofcacgkl
stiwOantfhacpipsitrwmtpi
C
MAsmngfbwo�zmtatvtifdvtwtcgaac2taPb(s
C
MiMnndsmnipotafwhtmauwcwvn
C
KsSwotm(dtaMA
www.AJOG.org Reviews
C-resistant) may benefit from the ad-ition of metformin. Even though theeason for the ovulatory resistance to CCas not been clearly identified, it can beypothesized that metformin therapyould augment the induction of ovula-
ion in CC-resistant women because ofts favorable change in androgens, go-adotropins, and insulin, throughechanisms distinct from those of CC.45
t is plausible to assume that women withC resistance receiving metformin haven increased response to CC secondaryo an intrinsic alteration of the micro-nvironment of the follicle caused byhe effect of metformin pretreatmentn insulin and the insulin growthactor (IGF)-I pathway in granulosaells.46,47 More specifically, Tosca etl48 reported that in bovine granuloseells, metformin decreases steroido-enesis and mitogen-activated proteininase (MAPK)3/MAPK1 phosphory-
ation through AMPK activation.In a study by Vandermolen et al,45 a
ignificant improvement on both ovula-ion and pregnancy rates were observedn women with CC-resistant PCOS whoere treated with metformin alone.ther investigators have also observed
n improvement in ovulatory or preg-ancy rates in CC-resistant patients
reated with a combination of met-ormin and CC vs placebo and CC,49-51
owever, all of these studies were smallnd underpowered. Despite the lack ofonvincing data that metformin im-roves live birth rates, there may be value
n attempting this treatment prior toroceeding to more expensive and inva-ive therapies, such as laparoscopic ovar-an drilling (LOD) or low-dose gonado-ropins.45 The ability of metformin toestore responsiveness to CC in obeseomen with PCOS, and the low rates ofultiparity and ovarian hyperstimula-
ion syndrome (OHSS), are additionalotential benefits of metformin therapy
n the CC-resistant patient.49
linical considerations
1. Patients with IR desiring fertilitywithin the next few years may beconsidered for metformin therapy.
More expedient desires for concep-tion should consider CC or otheralternatives.
2. The likelihood of a singleton gesta-tion is higher when metformin isadded to CC than with CC alone.
3. Metformin may be used as an ad-junct in women who are CC resis-tant, and may be stopped at thetime of positive pregnancy testresult.
etformin and TZDss metformin and TZDs modulate insulin
ensitivity and insulin levels via differentechanisms, it is possible that the combi-
ation of these medications may have areater effect on ovulation. Unfortunately,ew randomized controlled trials haveeen performed. In a randomized trial, 25omen with CC-resistant PCOS and mildbesity (mean body mass index [BMI]31 kg/m2) were treated with rosiglita-
one plus CC or metformin plus CC for 3onths. Rouzi and Ardawai52 observed
hat the ovulation rate in the rosiglitazonend CC group was significantly higherhan the metformin and CC group (64.3%s 36.4%, respectively, P � .035). Likewise,he pregnancy rate was higher in the ros-glitazone and CC group than the met-ormin and CC group, but the differenceid not reach statistical significance (50%s 38.5%, respectively, P � .58). In con-rast, Baillargeon et al53 randomized 128omen with PCOS to metformin, rosigli-
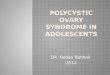
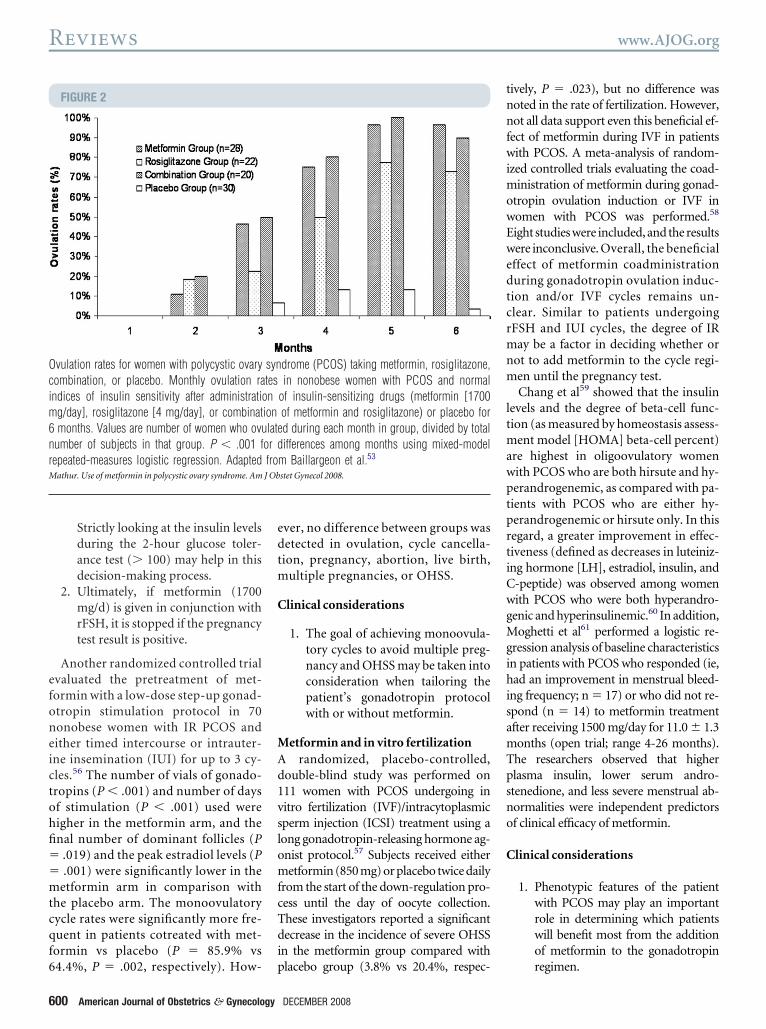
azone, and metformin and rosiglitazoneombination for 6 months. These investi-ators observed a higher ovulation ratemong women treated with metforminlone, or metformin plus rosiglitazone,ompared with rosiglitazone alone (Figure). There was no significant difference be-ween metformin alone and metforminnd rosiglitazone. Of note, all patients withCOS included in this study were nono-ese and had normal glucose toleranceNGT) and normal fasting and glucose-timulated insulin levels.
linical considerations
1. The value of combining metforminwith TZDs in PCOS for the pur-pose of conception is not sup-ported by current data. Further
studies are needed.DECEMBER 2008 Am
etformin, gonadotropins, andntrauterine insemination cycles
any clinicians must decide whether orot to continue metformin during a go-adotropin cycle. There is a paucity ofata regarding this commonly faced is-ue. Van Santbrink et al54 reported that
etformin cotreatment in IR normogo-adotropic anovulatory women resulted
n the normalization of the endocrinerofile and led to monofollicular devel-pment during gonadotropin stimula-ion for ovulation induction. Yarali etl55 randomized 32 patients to met-ormin (1700 mg/d) or placebo for 6eeks. Recombinant follicle stimulatingormone (rFSH) therapy was then giveno those women who did not ovulate on
etformin (n � 10) or placebo (n � 15),nd metformin or placebo was contin-ed. Overall, although pregnancy ratesere higher in the metformin � rFSH
ombination therapy in comparisonith the placebo � rFSH therapy (31.3%s 6.3%, respectively), the differences didot reach significance.
linical considerations
1. In clinical practice, tailoring themanagement of rFSH with or with-out the continuation of metformin
FIGURE 1
aplan-Meier curves for live birth. According totudy group in Pregnancy in Polycystic Ovaryyndrome (PCOS) trial, in which 676 infertileomen with PCOS, ages 18-39 years, with nother infertility factors, were randomized to 3reatment arms for total of 6 cycles or 30 weeks:
etformin (1000 mg twice a day) � placeboPBO); clomiphene citrate (CC) (50 mg/d) for 5ays (day 3-7 of cycle) � PBO; and combina-ion of metformin � CC. Adapted from Legro etl.41
athur. Use of metformin in polycystic ovary syndrome.m J Obstet Gynecol 2008.
depends on the degree of IR.
erican Journal of Obstetrics & Gynecology 599
efoneictohfi��mtcqf6
edtm
C
MAd1vslomfcTdi
tnnfwimowEwedtcrmnm
ltmawptprtiCwgMgihisamTpsno
C
Ocim6nrM
Reviews www.AJOG.org
6
Strictly looking at the insulin levelsduring the 2-hour glucose toler-ance test (� 100) may help in thisdecision-making process.
2. Ultimately, if metformin (1700mg/d) is given in conjunction withrFSH, it is stopped if the pregnancytest result is positive.
Another randomized controlled trialvaluated the pretreatment of met-ormin with a low-dose step-up gonad-tropin stimulation protocol in 70onobese women with IR PCOS andither timed intercourse or intrauter-ne insemination (IUI) for up to 3 cy-les.56 The number of vials of gonado-ropins (P � .001) and number of daysf stimulation (P � .001) used wereigher in the metformin arm, and thenal number of dominant follicles (P
.019) and the peak estradiol levels (P
.001) were significantly lower in theetformin arm in comparison with
he placebo arm. The monoovulatoryycle rates were significantly more fre-uent in patients cotreated with met-ormin vs placebo (P � 85.9% vs
FIGURE 2
vulation rates for women with polycystic ovaryombination, or placebo. Monthly ovulation randices of insulin sensitivity after administratio
g/day], rosiglitazone [4 mg/day], or combinatmonths. Values are number of women who ovu
umber of subjects in that group. P � .001 fepeated-measures logistic regression. Adapted
athur. Use of metformin in polycystic ovary syndrome. Am
4.4%, P � .002, respectively). How- p
00 American Journal of Obstetrics & Gynecology
ver, no difference between groups wasetected in ovulation, cycle cancella-ion, pregnancy, abortion, live birth,
ultiple pregnancies, or OHSS.
linical considerations
1. The goal of achieving monoovula-tory cycles to avoid multiple preg-nancy and OHSS may be taken intoconsideration when tailoring thepatient’s gonadotropin protocolwith or without metformin.
etformin and in vitro fertilizationrandomized, placebo-controlled,
ouble-blind study was performed on11 women with PCOS undergoing initro fertilization (IVF)/intracytoplasmicperm injection (ICSI) treatment using aong gonadotropin-releasing hormone ag-nist protocol.57 Subjects received eitheretformin (850 mg) or placebo twice daily
rom the start of the down-regulation pro-ess until the day of oocyte collection.hese investigators reported a significantecrease in the incidence of severe OHSS
n the metformin group compared with
drome (PCOS) taking metformin, rosiglitazone,in nonobese women with PCOS and normal
of insulin-sensitizing drugs (metformin [1700of metformin and rosiglitazone) or placebo ford during each month in group, divided by totalifferences among months using mixed-model
m Baillargeon et al.53
stet Gynecol 2008.
lacebo group (3.8% vs 20.4%, respec-
DECEMBER 2008
ively, P � .023), but no difference wasoted in the rate of fertilization. However,ot all data support even this beneficial ef-
ect of metformin during IVF in patientsith PCOS. A meta-analysis of random-
zed controlled trials evaluating the coad-inistration of metformin during gonad-
tropin ovulation induction or IVF inomen with PCOS was performed.58
ight studies were included, and the resultsere inconclusive. Overall, the beneficialffect of metformin coadministrationuring gonadotropin ovulation induc-ion and/or IVF cycles remains un-lear. Similar to patients undergoingFSH and IUI cycles, the degree of IRay be a factor in deciding whether or
ot to add metformin to the cycle regi-en until the pregnancy test.Chang et al59 showed that the insulin
evels and the degree of beta-cell func-ion (as measured by homeostasis assess-
ent model [HOMA] beta-cell percent)re highest in oligoovulatory womenith PCOS who are both hirsute and hy-erandrogenemic, as compared with pa-ients with PCOS who are either hy-erandrogenemic or hirsute only. In thisegard, a greater improvement in effec-iveness (defined as decreases in luteiniz-ng hormone [LH], estradiol, insulin, and-peptide) was observed among womenith PCOS who were both hyperandro-enic and hyperinsulinemic.60 In addition,oghetti et al61 performed a logistic re-
ression analysis of baseline characteristicsn patients with PCOS who responded (ie,ad an improvement in menstrual bleed-
ng frequency; n � 17) or who did not re-pond (n � 14) to metformin treatmentfter receiving 1500 mg/day for 11.0 � 1.3onths (open trial; range 4-26 months).he researchers observed that higherlasma insulin, lower serum andro-tenedione, and less severe menstrual ab-ormalities were independent predictorsf clinical efficacy of metformin.
linical considerations
1. Phenotypic features of the patientwith PCOS may play an importantrole in determining which patientswill benefit most from the additionof metformin to the gonadotropin
syntesn
ionlate
or dfroJ Ob
regimen.
MoiIntgldtapmlfpbtwtmdmOli
Cpgmwot
iPfudmotmaewoittT
ttmf
C
MaRlapicsdea
m J
www.AJOG.org Reviews
etformin in the treatmentf PCOS-associated oligoovulatory
nfertility: summaryn summary, metformin alone doesot appear to be a highly effective ini-
ial therapy for the treatment of oli-oovulatory infertility in PCOS, ateast compared with CC ovulation in-uction; nonetheless, it is more effec-ive than placebo alone and is associ-ted with a significantly lower multipleregnancy and OHSS rate. In general,etformin should not be used as first-
ine monotherapy. However, met-ormin alone may play a role in the rareatient who desires improvement inoth metabolic and reproductive func-ion, but who is not on a fast track to-ard obtaining a pregnancy, or in
hose who absolutely wish to avoidultiple gestations, or in patients who
o not tolerate CC (eg, secondary toood changes, visual disturbances).f interest, genetic factors may modu-
ate the effectiveness of metformin in
TABLE 2Histology of serial endometrial biop
SubjectRandomizedmedication
Ovra
1 Rosiglitazone 0...................................................................................................................
2 Metformin 50...................................................................................................................
3 Rosiglitazone 0...................................................................................................................
4 Metformin 66...................................................................................................................
5 Rosiglitazone 17...................................................................................................................
6 Rosiglitazone 66...................................................................................................................
7 Metformin —...................................................................................................................
8 Rosiglitazone 83...................................................................................................................
9 Rosiglitazone 83...................................................................................................................
10 Metformin 0...................................................................................................................
11 Rosiglitazone 0...................................................................................................................
12 Rosiglitazone 83...................................................................................................................
13 Metformin 0...................................................................................................................
14 Metformin 33...................................................................................................................
15 Rosiglitazone 17...................................................................................................................
16 Metformin —...................................................................................................................
Adapted from Legro et al.68
a Six treatment cycles of either metformin (2000 mg/day) or...................................................................................................................
Mathur. Use of metformin in polycystic ovary syndrome. A
nducing ovulation. Data from the PP- o
OS trial indicated that a polymor-hism of a serine-threonine kinaseene expressed in the liver, STK11 (for-erly known as LKB1), was associatedith a significantly decreased chance ofvulation in women with PCOSreated with metformin.62
Metformin may be effective in induc-ng ovulation in some women withCOS and CC resistance. Whether met-
ormin is of value in patients with PCOSndergoing gonadotropin ovulation in-uction or IVF remains to be deter-ined; perhaps the severity of IR noted
n a 2-hour 75-g load glucose toleranceest may help in this decision. In agree-
ent, Moll et al63 performed a meta-nalysis including 27 trials evaluating theffectiveness of metformin in subfertileomen with PCOS with the primaryutcome being live birth rate. Prior to
nitiating gonadotropins, the combina-ion of CC and metformin in CC-resis-ant women is the preferred treatment.his combination usually requires a dose
and corresponding ovulation rate ontion
a Baseline biopsy Se
—c Pro.........................................................................................................................
Simple hyperplasia Se.........................................................................................................................
Proliferative We.........................................................................................................................
Mid proliferative Ea.........................................................................................................................
Early proliferative La.........................................................................................................................
Proliferative Pro.........................................................................................................................
Simple hyperplasia Pro.........................................................................................................................
Early proliferative Mi.........................................................................................................................
Proliferative Se.........................................................................................................................
Proliferative Pro.........................................................................................................................
Mid proliferative Mi.........................................................................................................................
Early proliferative Pro.........................................................................................................................
Weakly proliferative Sim.........................................................................................................................
Mid proliferative Pro.........................................................................................................................
Secretory Pro.........................................................................................................................
Adenocarcinoma —.........................................................................................................................
litazone (8 mg/day). b After 3 months of combined therapy. c N.........................................................................................................................
Obstet Gynecol 2008.
f at least 1500 mg/day of metformin. Al- m
DECEMBER 2008 Am
ernatively, this analysis concluded thathere was no evidence for an improve-
ent in live birth rate when adding met-ormin to LOD or gonadotropins.
linical considerations
1. Overall, it should be rememberedthat metformin is a modestly actingagent, operating indirectly to im-prove ovulation, and the expecta-tion that it is a powerful ovulatorydrug for PCOS is unfounded.
etformin, the endometrium,nd menstrual bleedingesearchers have found that excess insu-
in levels stimulate endometrial growth,nd may serve to stimulate endometrialroliferation.64 Metformin may have an
mpact on the endometrium, hypotheti-ally both improving the potential for auccessful pregnancy implantation and re-ucing the long-term risks of unopposedndometrial proliferation. Jakubowicz etl65,66 observed that metformin treat-
sulin sensitizer treatment
d biopsyb Third biopsyb
rative Weakly proliferative..................................................................................................................
ory Mid proliferative..................................................................................................................
y proliferative Weakly proliferative..................................................................................................................
roliferative Weakly proliferative..................................................................................................................
roliferative Proliferative..................................................................................................................
rative Secretory..................................................................................................................
rative —c
..................................................................................................................
oliferative —c
..................................................................................................................
ory Mid proliferative..................................................................................................................
rative Proliferative..................................................................................................................
oliferative Weakly proliferative..................................................................................................................
rative Secretory..................................................................................................................
hyperplasia Weakly proliferative..................................................................................................................
rative Proliferative..................................................................................................................
rative Secretory..................................................................................................................
—c
..................................................................................................................
luable data for these outcomes...................................................................................................................
sy inulate, % con
life......... .........
cret......... .........
akl......... .........
rly p......... .........
te p......... .........
life......... .........c life......... .........
d pr......... .........
cret......... .........
life......... .........
d pr......... .........
life......... .........
ple......... .........
life......... .........
life......... .........c c
......... .........
rosig o eva......... .........
ent enhanced uterine vascularity and
erican Journal of Obstetrics & Gynecology 601

botmafmwidi
mwbt(3IhcTdona(hWctbqcttb
peht
cumteoitda
qtqbaatm(ngalaittsoHtfiilestp
ag
vmdt
C
MAsritstr(2tnttCtZetmCb
m J
Reviews www.AJOG.org
6
lood flow in women with PCOS. Pal-mba et al67 studied uterine vasculariza-ion, endometrial thickness, and endo-
etrial pattern in 37 patients withnovulatory PCOS treated with met-ormin for 6 months, and in 30 age-
atched control subjects. In the patientsith PCOS, metformin was observed to
mprove a majority of parameters of en-ometrial receptivity, although it did not
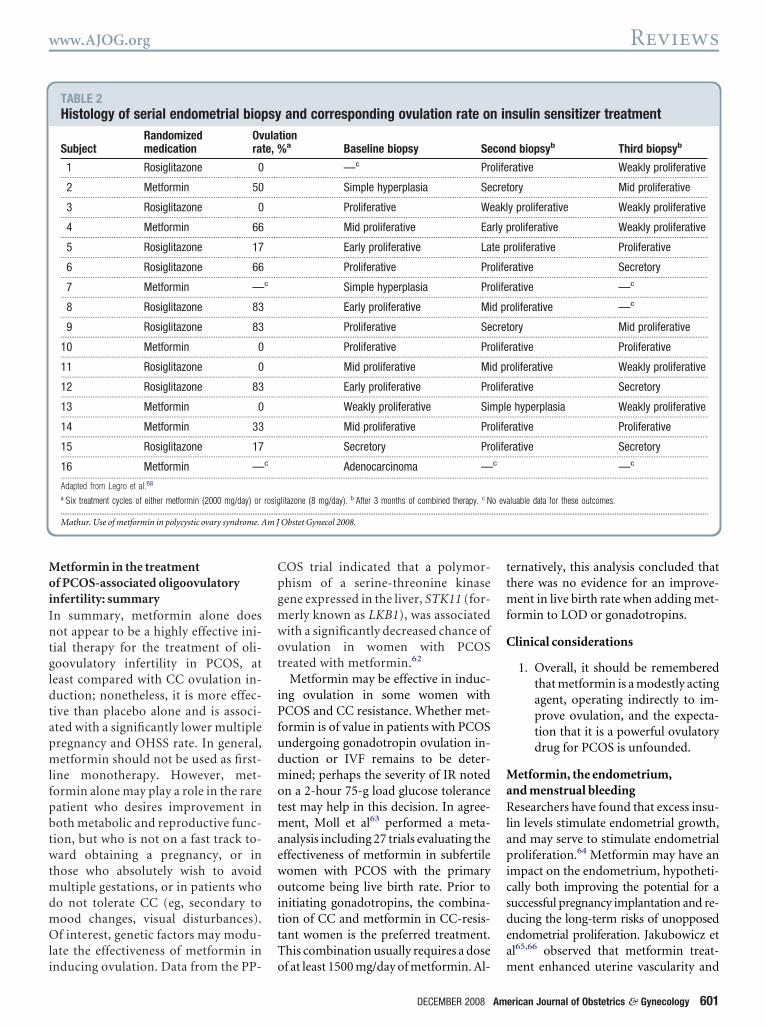
mprove endometrial thickness.A randomized open-label study ofetformin and rosiglitazone in 16omen with PCOS consisted of a 6-weekaseline observation period, a 3-monthreatment period of single-agent therapyrosiglitazone or metformin), and then a-month period of combined therapy.nvestigators observed that endometrialistology tended to normalize during theourse of the study as shown in Table 2.68
hree subjects displayed abnormal en-ometrial histology at the baseline bi-psy (simple hyperplasia or adenocarci-oma), 1 subject had abnormal histologyfter 3 months of single-agent therapysimple hyperplasia), and no subjectsad abnormal histology at 6 months.hen examining the prevalence of se-
retory endometrial hyperplasia indica-ive of ovulation based on the randomiopsies, a steady increase in the fre-uency of this histology during theourse of the study was observed, al-hough no significant differences orrends in the 32 graded histologic itemsy treatment arm were noted (Table 3).Overall, metformin appears to im-
rove ultrasound-detected markers ofndometrial receptivity and endometrialistology through: (1) improved ovula-
TABLE 3Metformin alone for treatment of hStudy N (hirsute/contr
Kolodziejczyk et al,83 34/0...................................................................................................................
Moghetti et al,61 32/0...................................................................................................................
Pasquali et al,36 9/4...................................................................................................................
Kelly and Gordon,84 5/5...................................................................................................................
FG, Ferriman-Gallwey hirsutism.a Not documented....................................................................................................................
Mathur. Use of metformin in polycystic ovary syndrome. A
ory function; (2) possibly reduced cir- m
02 American Journal of Obstetrics & Gynecology
ulating levels of insulin; and (3) otherndetermined factors. Consequently,etformin administration has the po-
ential to reduce the risk of unopposedndometrial proliferation, hyperplasia,r carcinoma by improving the regular-
ty of ovulatory function and by reducinghe effect of hyperinsulinemia on the en-ometrium. However, definitive studiesre lacking.
We should note that it is not infre-uent for there to be a disconnect be-ween ovulatory response and the fre-uency or regulation of withdrawalleeding. Periodic vaginal bleeding mayrise as a result of the decline in estrogennd progesterone at the end of an ovula-ory cycle in a nonpregnant patient (ie, a
enstrual bleed). Alternatively, periodicalthough not necessarily regular) vagi-al bleeding may also occur when therowth properties of the endometriumre altered, through alterations in circu-ating hormones and uterine vascularity,s described above. Many studies exam-ning the effect of metformin on ovula-ory function have reported primarily onhe frequency of vaginal bleeding (as-umed to be a menstrual flow) and notn the degree of ovulatory function.owever, in many oligoamenorrheic pa-
ients with PCOS treated with met-ormin there is discordance between themprovement in periodic vaginal bleed-ng and the development of regular ovu-atory function. For example, Moghettit al61 assessed ovulatory function by aerum progesterone measured in the lu-eal phase of 39 cycles in 10 women ex-eriencing regular menses after treat-
utismDuration (mos) Placebo controll
3 No.........................................................................................................................
11.3 No.........................................................................................................................
6 Yes.........................................................................................................................
14 Yes.........................................................................................................................
.........................................................................................................................
Obstet Gynecol 2008.
ent with metformin. In only 32 of these p
DECEMBER 2008
ssessments (79%), did the serum pro-esterone levels confirm ovulation.Thus, the periodicity and frequency of
aginal bleeding in a patient receivingetformin should not be used as evi-
ence of ovulatory function or endome-rial protection.
linical considerations
1. The presence of ovulation in pa-tients treated with metforminalone should be confirmed throughthe measurement of luteal phase(cycle day 20-24) progesterone lev-els (with levels generally above 3-4ng/mL indicating prior ovulation).
etformin and pregnancy lossnumber of observational studies have
uggested that metformin reduces theisk of pregnancy loss.35,69,70 However,n the prospective randomized PPCOSrial, spontaneous abortion rates wereimilar in all 3 treatments and there was arend toward a greater rate of miscar-iages in the metformin only group40.0% in the metformin only group vs5.8% in the CC only group vs 30.0% inhe CC plus metformin group).41 Alter-atively, Moll et al43 randomized 228
herapeutically naïve women with PCOSo metformin plus CC or placebo plusC, and did not observe a difference in
he pregnancy loss rate (11% vs 12%).ain et al44 did not observe any differ-nce in pregnancy losses among 115 pa-ients with PCOS randomized to receive
etformin (1500 mg/day) (38 patients),C at incremental doses (39 patients), oroth medications in combination (38
Improved Change in FG score
Yes -2.3%..................................................................................................................
No —..................................................................................................................
Yes -15%..................................................................................................................
Yes N/Da
..................................................................................................................
..................................................................................................................
irsol) ed
......... .........
......... .........
......... .........
......... .........
......... .........
atients).

C
MFitfiwltnombscwnmi
fdotcspGidato6obpfibeeecc(o
avgt
gdtmnGcupmdtwl
C
EoAeg
(dwcmmtnnotwff
7Ttirw
prfpco(ogLmztPsasa
tdrdvheihrapalmafpar
tahdocur
www.AJOG.org Reviews
linical considerations
1. At the present time there are noconclusive data to support a bene-ficial effect of metformin on preg-nancy loss, although the trend to-ward a higher miscarriage rate inthe PPCOS trial, which used ex-tended release metformin, isconcerning.
etformin use during pregnancyor women who become pregnant it is
mportant to note that the TZDs piogli-azone and rosiglitazone are both classi-ed as pregnancy category C, associatedith fetal growth retardation in mid to
ate gestation in animal studies. In con-rast, metformin is classified as preg-ancy category B.71 Despite the absencef contradictory data, the safety ofetformin in pregnancy has not yet
een established. A meta-analysis of 8tudies focusing on pregnancy out-ome after metformin use in womenith PCOS concluded that there waso evidence of an increased risk forajor malformations (95% confidence
nterval, 0.15-1.60).72
It is possible that the use of met-ormin during pregnancy might re-uce the risk of developing GDM andther pregnancy complications poten-ially associated with IR (eg, pregnan-y-induced hypertension). In a pro-pective observational study of 42regnancies in 39 women with PCOS,lueck et al73 suggested that metformin
n combination with dietary control re-uced the likelihood of developing GDMnd prevented androgen excess in the fe-us. Kovo et al74 evaluated the neonatalutcomes of 33 women with PCOS and6 healthy women. These investigatorsbserved a significantly lower meanirth weight percentile of neonates ex-osed to metformin in utero during therst trimester compared with the meanirth weight percentile of neonates notxposed to metformin. A recent studyvaluated 126 infants born to 109 moth-rs with PCOS who conceived on andontinued metformin through pregnan-y.75 These investigators concluded that:1) metformin reduced the risk of devel-
ping GDM; (2) metformin was not ter- ptogenic; and (3) metformin did not ad-ersely affect birth length, birth weight,rowth, or motor-social development inhe first 18 months of life.75
In summary, there are few data to sug-est that metformin might be harmfuluring pregnancy. Although observa-ional and anecdotal data suggest that
etformin may be beneficial in preg-ancy by potentially reducing the risk ofDM or other IR-associated pregnancy
omplications, at present, the routinese of metformin during pregnancy inatients with PCOS to prevent theseorbidities is not recommended. In fact,
efinitive data regarding the continua-ion of metformin during pregnancy foromen with documented IR are also
acking.
linical considerations
1. Although observational and anec-dotal data suggest that metforminmay be beneficial in pregnancy bypotentially reducing the risk ofGDM or other IR-associated preg-nancy complications, at present,the routine use of metformin dur-ing pregnancy for patients withPCOS to prevent these morbiditiesis not recommended.
2. At present, cessation of metforminon a positive pregnancy test resultis a reasonable course of action.
ffects of metforminn androgens and hirsutismmple evidence supports the beneficialffect of metformin on the hyperandro-enism of patients with PCOS.25,41,76-78
In a study comparing metformin2250 mg/day) with flutamide (250 mg/ay) as a treatment for nonobese youngomen with PCOS, free testosterone de-
reased significantly with both treat-ents.79 In addition, a comparison ofetformin alone (2250 mg/day), rosigli-
azone alone (4 mg/day), and the combi-ation of both drugs, to placebo inonobese, non-IR women with PCOSbserved that the mean serum-free tes-osterone levels in subjects on therapyere significantly lower than the levels
ound in subjects on placebo (met-ormin: 2.34 pg/mL, rosiglitazone: 3.06
g/mL, and combination: 2.39 pg/mL vs fDECEMBER 2008 Am
.26 pg/mL for placebo, P � .05).53
hese findings suggest that 6 months ofreatment with either metformin or ros-glitazone in the doses studied amelio-ated hyperandrogenemia in nonobeseomen with PCOS.Conversely, when Yilmaz et al80 com-
ared metformin (1700 mg/day) withosiglitazone (4 mg/day) administeredor 12 weeks to groups of lean and obeseatients with PCOS, they observed de-reases in testosterone, androstenedi-ne, or dehydroepiandrosterone statusDHEAS) levels in all 4 groups, althoughnly the decreases in the rosiglitazoneroups were statistically significant.astly, when comparing the effects ofetformin (2250 mg/day) and pioglita-
one (30 mg/day) randomly adminis-ered for 6 months in 52 women withCOS, a �30% decrease in the hirsutismcore was observed in both groups. Inddition, both treatments demonstratedignificant decreases in free testosterone,ndrostenedione, and LH.81
Metformin may reduce hirsutismhrough amelioration of their hyperan-rogenemia (see above) and possibly byeducing circulating insulin levels. An-rogens stimulate the terminalization ofellus hairs and the growth of terminalairs in skin areas that are sensitive to theffects of these steroids (ie, those exhib-ting sufficient androgen receptor, 17-�-ydroxysteroid dehydrogenase, and 5�-eductase, and areas with reducedromatase activities). In addition to theubic and axillary regions, an exagger-ted androgen effect in these areas canead to excess terminal hair growth in a
ale-like pattern (ie, hirsutism). Finally,s insulin also acts as an anabolic growthactor in hair,82 it is possible that the sup-ression of circulating insulin levelslone may be sufficient to ameliorate theate of terminal hair growth.
A number of small studies, some con-rolled, others not (Table 2), have gener-lly indicated modest improvements inair growth.36,61,83,84 Two small, ran-omized trials have compared the effectf metformin alone with an oral contra-eptive pill (OCP) alone. Morin-Pap-nen et al85 randomized 18 patients toeceive either metformin (1000 mg/day
or 3 months, then 2000 mg/day for 3erican Journal of Obstetrics & Gynecology 603

aeedOitmnaatlgssOmfHt
fThO
fwedo1t(olpatsf
C
MoiMBwtrtwtugiBssLcprfsraPttowdim(brcw1mcw
CtamtmdFM J Ob
Reviews www.AJOG.org
6
dditional months) or an OCP (35 �g ofthinyl estradiol and 2 mg of cyprot-rone acetate), and observed a greaterecrease in the hirsutism score with theCP. Luque-Ramirez et al86 random-
zed 34 consecutive patients with PCOSo oral treatment with metformin (1700
g/day) or with an OCP (35 �g of ethi-yl estradiol plus 2 mg of cyproteronecetate) for 24 weeks. They observed thatlthough the hirsutism score, serum-freeestosterone levels, and androstenedioneevels decreased with treatment in theroup as a whole, the improvements re-ulted mostly from the decrease ob-erved in the patients treated with theCP, which was marked down muchore than those observed with met-
ormin. Alternatively, in a similar design,arborne et al87 randomized 37 patients
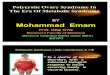
FIGURE 3
hanges in Ferriman-Gallwey hirsutism score iaking placebo (PLAC), metformin (MET), flutamt 6 (white bars) and 12 (black bars) months ing/day), FLUT (500 mg/day), and MET�FLUT. D
o differences in changes of hirsutism score froonths, between groups treated with MET, FLU
ifferences in changes of hirsutism score fromLUT, or MET�FLUT and PLAC. Adapted fromathur. Use of metformin in polycystic ovary syndrome. Am
o receive either the same OCP or met- (
04 American Journal of Obstetrics & Gynecology
ormin (1500 mg/day) for 12 months.hey reported a greater decrease in theirsutism score with metformin than theCP arm (-25% vs -5%, P � .01).Metformin alone is much less effective
or the treatment of hirsutism comparedith antiandrogen therapy. Gambineri
t al88 carried out a prospective, ran-omized, placebo-controlled trial of 76bese women with PCOS.88 After a-month diet, the patients were allocatedo treatment with placebo, metformin1700 mg/day), flutamide (500 mg/day),r metformin plus flutamide for the fol-
owing 6 months, while continuing hy-ocaloric dieting. Flutamide treatmentlone was significantly more effectivehan metformin alone for treating hir-utism; combination therapy with met-ormin did not add any further benefit
omen with polycystic ovary syndrome (PCOS)(FLUT), or combination. Changes (�) in scoreents with PCOS treated with PLAC, MET (1700are shown as mean � SEM. a, P � .001 refersaseline to 6 months, and from baseline to 12r MET�FLUT and PLAC. b, P � .05 refers to12 months between groups treated with MET,
mbineri et al.88
stet Gynecol 2008.
Figure 3). m
DECEMBER 2008
linical considerations
1. Although metformin, like OCPs,may have a beneficial effect on ex-cess hair growth, both agents have arelatively modest effect during anextended period. Antiandrogentherapy, alone or preferably incombination with androgen sup-pression, is the preferred first-linetreatment for PCOS-associatedhirsutism.
etformin and the preventionf metabolic morbidity
n women with PCOSetformin, hyperinsulinemia, and IR
y the age of 30 years, 30-50% of obeseomen with PCOS develop IGT or overt
ype 2 DM. This is a 3- to 7-fold greaterisk than an age-comparable popula-ion.89-91 In addition, many patientsith PCOS demonstrate features consis-
ent with the metabolic syndrome.16 These of metformin in women with PCOSenerally increases insulin sensitiv-ty,25,53,78-81,92 and decreases weight andMI.25,77,79,93 In a meta-analysis of 13
tudies, metformin improved fasting in-ulin levels, blood pressure, and levels ofDL cholesterol,69 perhaps as a result ofhanges in body weight. Salpeter et al94
erformed a meta-analysis of the pooledesults of 31 trials with 4570 participantsollowed up for 8267 patient-years to as-ess the effect of metformin on metabolicisk. These investigators did not observesignificant difference in results betweenCOS and non-PCOS individuals, al-
hough unfortunately no trial examinedhe effect of metformin on the incidencef type 2 DM. In this meta-analysis,omen with PCOS experienced a 5.3%ecrease in BMI, a 2.6% mean decrease
n fasting glucose, and a 19.7% improve-ent in IR as assessed by the HOMA
HOMA-IR). Fasting insulin decreasedy 5.7%, although the difference did noteach significance. In addition, HDLholesterol increased by a mean of 9.4%hereas triglycerides decreased by1.9%. These results were of similaragnitude to those of non-PCOS, ex-
ept the measurement of fasting insulin,hich in non-PCOS was improved by a
n widepatiata
m bT, o6 to
Ga
ean of 16.1%.

wdoPtcaioodlcnsiApmEtPmcH
C
MCmeswdicw(cfwcpeeif
mazscmbg
siit3flmttcWpcscO
C
MMtttPcPwa(votaiays
ftgl
wafdTcfw
C
MMiepwmaBIonidssamweifcsy
wftP
www.AJOG.org Reviews
Metformin appears to benefit peopleith PCOS irrespective of their weight oregree of IR.25,80 A study including lean,verweight, and obese patients withCOS observed that all 3 groups of pa-
ients demonstrated a significant de-rease in fasting insulin and HOMA-IRfter 6 months of metformin treatment,rrespective of their pretreatment degreef IR.25 In addition, the overweight andbese groups demonstrated a significantecrease in area under the curve of insu-
in (AUCinsulin) response to an oral glu-ose challenge. Investigators studyingormal-weight women with PCOS ob-erved that metformin significantlymproved insulin sensitivity and theUCglucose to AUCinsulin ratio in com-arison with both the baseline assess-ent and against a placebo group.92
ven in studies performed to examinehe effects of metformin in women withCOS with normal weight and with nor-al insulin sensitivity, significant de-
reases in fasting insulin, AUCinsulin, andOMA-IR were observed.78
linical considerations
1. In women with PCOS and hyperin-sulinemia, metformin improvesfasting insulin levels, blood pres-sure, and levels of LDL cholesterol.Studies are needed to determinewhether this translates into im-proved morbidity and mortality.
etformin vs TZDs or OCPsomparisons have been made betweenetformin and other medications to
valuate degrees of efficacy on insulinensitivity. Metformin (2550 mg/day)as compared with pioglitazone (30 mg/ay).81 Both medications improved fast-
ng insulin levels and insulin sensitivityomparably. Pioglitazone was associatedith an increase in the waist-to-hip ratio
WHR), body weight, and BMI. Whenomparing rosiglitazone with met-ormin in both lean and obese patientsith PCOS, both treatments signifi-
antly decreased fasting insulin levels, C-eptide levels, and HOMA-IR.80 How-ver, in this study rosiglitazone moreffectively decreased androgen levels andncreased menstrual regularity than met-
ormin. Other investigators compared setformin alone with rosiglitazonelone with a metformin plus rosiglita-one combination, and observed that in-ulin sensitivity was significantly in-reased in the metformin alone and theetformin plus rosiglitazone groups,
ut not in the rosiglitazone aloneroup.53
Although OCPs help hyperandrogenicymptoms and regulate menstrual cyclesn women with PCOS, they may worsennsulin sensitivity.95 This remains con-roversial. In a meta-analysis comparing
trials of metformin vs OCPs,85,87,96
asting insulin levels were significantlyower in patients who were treated with
etformin whereas the insulin levels inhose treated with OCP did not change;here were no differences in fasting glu-ose levels between the 2 interventions.97
hen a comparison of 2 trials32,98 waserformed analyzing a metformin-OCPombination vs OCPs alone, fasting in-ulin levels demonstrated a nonsignifi-ant trend in favor of the metformin-CP combination.97
linical considerations
1. Overall, current data suggest thatmetformin appears to be equally aseffective, if not more, than TZDsfor the treatment of hyperinsulin-ism in PCOS, and may be of addi-tional value in patients takingOCPs.
etformin and the risk of Type 2 DMetformin may slow the progression to
ype 2 DM.24 Most of the data to supporthis assertion arise from study popula-ions that may include women withCOS, but these studies do not specifi-ally identify this subset. The Diabetesrevention Trial enrolled 3234 subjectsith IGT who were at risk for type 2 DM,
nd randomized them to metformin1700 mg/day), intensive lifestyle inter-ention, or standard of care/control (theriginal design had a fourth arm, trogli-azone therapy, which was discontinuedfter 18 months secondary to the emerg-ng risk of hepatic dysfunction).99 Theverage follow-up for this study was 2.8ears. Compared with the control group,ubjects treated with metformin demon-
trated a 31% decrease in the relative risk mDECEMBER 2008 Am
or progression to overt type 2 DM, al-hough the decrease was greatest in theroup of patients treated with intensiveifestyle intervention (-58%).
One retrospective study of womenith PCOS treated with metformin for
n average of 43 months found that met-ormin appeared to delay or prevent theevelopment of IGT and type 2 DM.100
hese investigators found an 11-fold de-rease in the annual conversion raterom NGT to IGT, with 55% of patientsith IGT reverting to NGT.
linical consideration
1. Although it is likely that metforminwill reduce the risk of type 2 DMspecifically in PCOS, prospectiveand controlled studies have notbeen conducted in this particularpopulation to evaluate the long-term metabolic benefits of met-formin and the effects of subse-quent drug discontinuation.
etformin and weight lossetformin has been suggested to assist
n weight loss in patients with PCOS. Tant al25 analyzed data from 3 groups ofatients with PCOS: (1) lean, (2) over-eight, and (3) obese, and found thatetformin use was significantly associ-
ted with decreased body weight andMI in the overweight and obese groups.
n one study, the use of metformin wasbserved to decrease body weight even inonobese women with PCOS.79 Other
nvestigators observed a significant re-uction in waist circumference but noignificant change in weight in obeseubjects treated with metformin.101 Innother study, researchers observed thatetformin reduced BMI in patients bothith and without IR, but it had no influ-
nce on the WHR.77 Conversely, othernvestigators have concluded that met-ormin has no effect on BMI or waist cir-umference.69 These differences in re-ultant weight loss among studies haveet to be explained.It is possible that the differences ineight loss after treatment with met-
ormin are dose dependent. A prospec-ive cohort study of 4 groups of obeseCOS subjects on 2 different doses of
etformin were analyzed: (1) obeseerican Journal of Obstetrics & Gynecology 605

PoPotmsarplodmwg
wh3m�motn�dfbaioOvg
C
MBieImwtdrmt
tiOHstiemttpw
pbdtfgr(gbT6(hsecCtbar(wdetaa
hprpgcIontt
CipbmPwbopttvcarsc
C
CfMartsiwstlasdattpn
acrwbPel
Reviews www.AJOG.org
6
COS on 1500 mg/day; (2) morbidlybese PCOS on 1500 mg/day; (3) obeseCOS on 2550 mg/day; and (4) morbidlybese PCOS on 2550 mg/day.93 Al-hough all of the patients who received 8
onths of metformin treatment demon-trated significant reductions in weightnd BMI, only obese women with PCOSesponded to metformin in a dose-de-endant manner, with the greater weight
oss evident at the higher dose. Morbidlybese women demonstrated a similaregree of weight loss at both doses ofetformin, and a similar amount ofeight loss was observed in the obeseroup at the higher metformin dose.The use of metformin in combinationith dietary restriction for weight lossas also been studied. A meta-analysis ofsuch trials85,87,96 reviewing the effect ofetformin vs OCPs (ethinyl estradiol 35g combined with cyproterone acetate 2g) did not observe a difference in BMI
r WHR between the 2 treatments.97 Arial comparing 6 months of OCPs (ethi-yl estradiol 35 �g combined with 250g norgestimate in a cyclic regimen of 21ays of active pills followed by 7-day pill-
ree interval) alone vs the OCP com-ined with metformin (1500 mg/day)lso reported no significant differencesn body weight.32 Finally, meta-analysisf 2 studies investigating OCP alone vsCP combined with metformin32,98 re-
ealed no difference in BMI between theroups.97
linical consideration
1. These data suggest that the effect ofmetformin on weight is minimal,and patients should be advised thatthis agent should not be used solelyfor the purpose of weight reduction.
etformin and cardiovascular riskecause the metabolic syndrome and IR
ncrease the risk of cardiovascular dis-ase (CVD), it is important to considerR and long-term health when selecting a
edical treatment in overweight womenith PCOS.102 At baseline, many pa-
ients with PCOS have some degree ofyslipidemia. Typically, this can includeeduced levels of HDL cholesterols andodestly increased levels of LDL choles-
erol, triglycerides, and total choles i
06 American Journal of Obstetrics & Gynecology
erol.103 In a meta-analyses of 2 stud-es87,104 comparing metformin with
CP therapy, no difference in total,DL, or LDL cholesterols was ob-
erved. However, in comparison withhe OCP therapy, metformin did resultn significantly lower triglyceride lev-ls.97 Other investigators studying nor-al-weight women with PCOS found
hat metformin significantly improvedheir LDL cholesterol levels when com-ared with their baseline levels andith the placebo group.92
Metformin has been shown to im-rove endothelial function, as measuredy brachial arterial flow-mediated vaso-ilation.105 Metformin is also reportedo improve coronary microvascularunction and coronary flow rate.106 Oneroup of investigators evaluated the se-um levels of cellular adhesion moleculeCAM), which reflect the degree of low-rade chronic inflammation and haveeen associated with several IR states.107
hey found that women with PCOS (n �2) in comparison with control subjectsn � 45) had significantly higher levels ofigh-sensitivity C-reactive protein (CRP),oluble intracellular CAM-1, and solublendothelial leukocyte adhesion mole-ule-1 (sE-selectin). Soluble vascularAM (sVCAM)-1 did not differ between
he 2 groups. In women with PCOS,aseline levels of high-sensitivity CRPnd sVCAM-1 levels were significantlyeduced by taking a dose of metformin1700 mg/day) for 6 months. In obeseomen with PCOS, metformin alone re-uces circulating levels of CRP.108 How-ver, in combination with an OCP con-aining ethinylestradiol and cyproteronecetate, the reductions seen in CRP wasttenuated.
In summary, some, but not all studiesave indicated that metformin decreasesarameters implicated as cardiovascularisk factors in women with PCOS. Inarticular, benefit may be seen in athero-enic profiles, including markers of sub-linical inflammation, dyslipidemia, andR. Enhanced endothelial function, cor-nary microvascular function, and coro-ary flow rate may also be seen in addi-
ion to the overall benefit of a decrease inotal body weight. Notwithstanding the
mprovements observed in secondary cDECEMBER 2008
VD markers with metformin therapyn women with PCOS, conclusive androspective long-term studies have yet toe carried out. A recent position state-ent from the Androgen Excess and
COS Society recommended thatomen with PCOS, regardless of weight,e screened for IGT or type 2 DM by anral glucose tolerance test at their initialresentation and every 2 years thereaf-er.109 However, this statement notedhat the use of metformin to treat or pre-ent the progression of IGT could beonsidered but should not be mandatedt this point in time, as well-designedandomized controlled trials demon-trating efficacy have yet to beonducted.
linical considerations
1. Subclinical chronic inflammationin women with PCOS may be im-proved by metformin therapy, yetcontroversy exists as to whetherthese effects are long lasting.
onclusions: clinical considerationsor metformin therapy
etformin is an agent that acts indirectlynd modestly to improve ovulation andeduce long-term metabolic complica-ions. The management of metabolicyndrome in women with PCOS mustnclude tight blood pressure control,eight loss, diet modification, and pos-
ibly the use of agents for lipid modifica-ion. Metformin reduces the circulatingevels of many markers of atherosclerosisnd subclinical chronic inflammation,uggesting that it may be beneficial in re-ucing the long-term risk of type 2 DMnd CVD in women with PCOS, al-hough long-term studies are lacking. Athe present time, the use of TZDs in re-roductive-aged women with PCOS isot routinely recommended.Pregnancies achieved on metformin
re more likely to be singleton and toarry less risk of OHSS. There may be aole for metformin in women with PCOSho are CC resistant. Periodic vaginalleeding improves in many patients withCOS, but this does not ensure that allpisodes of bleeding result from an ovu-atory cycle. In addition, there are no
lear data to suggest that metformin re-
dnrdnmcoito
R1wG2aon3ps14Sop25wO6lic7lss8ppf19IE31gio11N1MDtmd6
1dicat21AoosM1Pdd41md1Ts21fL1o92gsbs22WgaJ2gtdd2tsE2t22iiE212Atms2
ad2Ra23AbJ3Dmie43easdt3oos13p23SwH3EafipM3fdM3kle3oaiN4pa4Ct24Won4
www.AJOG.org Reviews
uces pregnancy loss or improves preg-ancy outcome in PCOS, and it is cur-ently recommended that metformin beiscontinued with the first positive preg-ancy test result, unless there are otheredical indications (eg, type 2 DM) for
ontinued therapy. Phenotypic featuresf the patient with PCOS may play an
mportant role in determining which pa-ients will benefit most from the additionf metformin (Table 3). f
EFERENCES. Stein I, Leventhal M. Amenorrhea associatedith bilateral polycystic ovaries. Am J Obstetynecol 1935;29:181-91.. Azziz R, Sanchez LA, Knochenhauer ES, etl. Androgen excess in women: experience withver 1000 consecutive patients. J Clin Endocri-ol Metab 2004;89:453-62.. Yildiz BO, Knochenhauer ES, Azziz R. Im-act of obesity on the risk for polycystic ovaryyndrome. J Clin Endocrinol Metab 2008;93:62-8.. Azziz R, Marin C, Hoq L, Badamgarav E,ong P. Health care-related economic burdenf the polycystic ovary syndrome during the re-roductive life span. J Clin Endocrinol Metab005;90:4650-8.. Legro RS. Pregnancy considerations inomen with polycystic ovary syndrome. Clinbstet Gynecol 2007;50:295-304.. Burghen GA, Givens JR, Kitabchi AE. Corre-
ation of hyperandrogenism with hyperinsulin-sm in polycystic ovarian disease. J Clin Endo-rinol Metab 1980;50:113-6.. DeUgarte CM, Barolucci AA, Azziz R. Preva-
ence of insulin resistance in the polycystic ovaryyndrome using the homeostasis model as-essment. Fertil Steril 2005;83:1454-60.. Jonard S, Dewailly D. The follicular excess inolycystic ovaries, due to intra-ovarian hy-erandrogenism, may be the main culprit for the
ollicular arrest. Hum Reprod Update 2004;10:07-17.. Franks S, Gilling-Smith C, Watson H, Willis D.
nsulin action in the normal and polycystic ovary.ndocrinol Metab Clin North Am 1999;28:61-78.0. Legro RS, Finegood D, Dunaif A. A fastinglucose to insulin ratio is a useful measure of
nsulin sensitivity in women with polycysticvary syndrome. J Clin Endocrinol Metab998;83:2694-8.1. Ehrmann DA. Polycystic ovary syndrome.Engl J Med 2005;352:1223-36.
2. Talbott EO, Zborowski JV, Boudreaux MY,cHugh-Pemu KP, Sutton-Tyrrell K, GuzickS. The relationship between C-reactive pro-
ein and carotid intima-media wall thickness iniddle-aged women with polycystic ovary syn-rome. J Clin Endocrinol Metab 2004;89:
061-7. f3. Talbott EO, Zborowski JV, Rager JR, Bou-reaux MY, Edmundowicz DA, Guzick DS. Ev-
dence for an association between metabolicardiovascular syndrome and coronary andortic calcification among women with polycys-ic ovary syndrome. J Clin Endocrinol Metab004;89:5454-61.4. Legro RS, Azziz R, Ehrmann D, FereshetianG, O’Keefe M, Ghazzi MN. Minimal responsef circulating lipids in women with polycysticvary syndrome to improvement in insulin sen-itivity with troglitazone. J Clin Endocrinoletab 2003;88:5137-44.5. Ehrmann DA, Liljenquist DR, Kasza K, et al.revalence and predictors of the metabolic syn-rome in women with polycystic ovary syn-rome. J Clin Endocrinol Metab 2006;91:8-53.6. Essah PA, Wickham EP, Nestler JE. Theetabolic syndrome in polycystic ovary syn-rome. Clin Obstet Gynecol 2007;50:205-25.7. Norman RJ, Davies MJ, Lord J, Moran LJ.he lifestyle modification in polycystic ovaryyndrome. Trends Endocrinol Metab 2002;13:51-7.8. Balen AH. PCOS, obesity, and reproductive
unction: RCOG special study group on obesity.ondon: RCOG Press; 2007.9. Hoeger KM. Exercise therapy in polycysticvary syndrome. Semin Reprod Med 2008;26:3-100.0. Ehrmann D, Schneider DJ, Sobel BE. Tro-litazone improves defects in insulin action, in-ulin secretion, ovarian steroidogenesis and fi-rinolysis in women with polycystic ovaryyndrome. J Clin Endocrinol Metab 1997;82:108-16.1. Dunaif A, Scott D, Finegood D, Quintana B,hitcomb R. The insulin sensitizing agent tro-
litazone improves metabolic and reproductivebnormalities in the polycystic ovary syndrome.Clin Endocrinol Metab 1996;81:3299-306.2. Azziz R, Ehrmann DA, Legro RS, et al. Tro-litazone improves ovulation and hirsutism inhe polycystic ovary syndrome: a multicenter,ouble blind, placebo-controlled trial. J Clin En-ocrinol Metab 2001;86:1626-32.3. Sepilian V, Nagamani M. Effects of rosigli-azone in obese women with polycystic ovaryyndrome and severe insulin resistance. J Clinndocrinol Metab 2005;90:60-5.4. Nestler JE. Metformin for the treatment ofhe polycystic ovary syndrome. N Engl J Med008;358:47-54.5. Tan S, Hahn S, Benson S, et al. Metformin
mproves polycystic ovary syndrome symptomsrrespective of pre-treatment insulin resistance.ur J Endocrinol 2007;157:669-76.6. Bailey C, Turner R. Metformin. N Engl J Med996;334:574-9.7. Morin-Papunen LC, Koivunen RM, Ruokonen, Martikainen HK. Metformin therapy improves
he menstrual pattern with minimal endocrine andetabolic effects in women with polycystic ovary
yndrome. Fertil Steril 1998;69:691-6.8. Musi N, Hirshmen MF, Nygren J, et al. Met-
ormin increases AMP activated protein kinase b
DECEMBER 2008 Am
ctivity in skeletal muscle of subjects with type 2iabetes. Diabetes 2002;51:2074-81.9. Zhou G, Myers R, Li Y, Chen Y, Shen X.ole of AMP activated protein kinase in mech-nism of metformin action. J Clin Invest001;108:1167-74.0. Zou MH, Kirkpatrick SS, Davis BJ, et al.ctivation of the AMP activated protein kinasey the anti-diabetic drug metformin in vivo.Biol Chem 2004;279:43940-51.1. Elia E, Sander V, Luchetti CG, Solano ME,i Girolamo G, Gonzalez C, Motta AB. Theechanisms involved in the action of metformin
n regulating ovarian function in hyperandrog-nized mice. Mol Hum Reprod 2006;12:75-81.2. Cibula D, Fanta M, Vrbikova J, et al. Theffect of combination therapy with metforminnd combined oral contraceptives (COC) ver-us COC alone on insulin sensitivity, hyperan-rogenemia, SHBG and lipids in PCOS pa-ients. Hum Reprod 2005;20:180-4.3. Arlt W, Auchus RJ, Miller WL. Thiazolidinedi-nes but not metformin directly inhibit the steroid-genic enzymes P450c17 and 3 beta- hydroxy-teroid dehydrogenase. J Biol Chem 2001;276:6767-71.4. Barbieri RL. Metformin for treatment of theolycystic ovary syndrome. Obstet Gynecol003;101:785-93.5. Glueck CJ, Wang P, Goldenberg N, Sieve-mith L. Pregnancy outcomes among womenith polycystic ovary syndrome with metformin.um Reprod 2002;17:2858-64.6. Pasquali R, Gambineri A, Biscotti D, et al.ffect of long-term treatment with metformindded to hypocaloric diet on body composition,at distribution, and androgen and insulin levelsn abdominally obese women with and withoutolycystic ovary syndrome. J Clin Endocrinoletab 2000;85:2767-74.7. Barbieri RL. Clomiphene versus metformin
or ovulation induction in polycystic ovary syn-rome: the winner is. . .. J Clin Endocrinoletab 2007;92:3399-401.8. Shaw RJ, Lamia KA, Vasquez D, et al. Theinase LKB1 mediates glucose homeostasis in
iver and therapeutic effects of metformin. Sci-nce 2005;310:1642-6.9. Nestler JE, Jakubowicz DJ. Decreases invarian cytochrome P-450c17 alpha activitynd serum free testosterone after reduction of
nsulin secretion in polycystic ovary syndrome.Engl J Med 1996;335:617-23.
0. Lord JM, Flight IH, Norman RJ. Metformin inolycystic ovary syndrome: systematic reviewnd meta-analysis. BMJ 2003;327:951-3.1. Legro RS, Barnhart HX, Schlaff WD, et al.lomiphene, metformin, or both for infertility in
he polycystic ovary syndrome. N Engl J Med007;356:551-66.2. Creanga AA, Bradley HM, McCormick C,itkop CT. Uses of metformin in polycystic
vary syndrome: a meta analysis. Obstet Gy-ecol 2008;111:959-68.3. Moll E, Bossuyt PMM, Korevaar JC, Lam-
alk CB, van der Veen F. Effect of clomifeneerican Journal of Obstetrics & Gynecology 607

cpwst4RfoaoF4Sifcm34AsF4vacR4Jcat34Mcpo5fawM5Rmd5tcprS5JandF5mfemcd
5amtr25dpotoi25AP25sdmds5Aoag6Baosl6fapblJ6OopM6os16pB26elgaflE6Re
6etH6eats6sztR7Sttfis7t37of67Lpivlct57Rctt7On7Fostm67foG7Bwsn7fawd
Reviews www.AJOG.org
6
itrate plus metformin and clomifene citrate pluslacebo on induction of ovulation in womenith newly diagnosed polycystic ovaryyndrome: randomized double blind clinicalrial. BMJ 2006;332:1461-2.4. Zain MM, Jamaluddin R, Ibrahim A, NormanJ. Comparison of clomiphene citrate, met-
ormin, or the combination of both for first-linevulation induction, achievement of pregnancy,nd live birth in Asian women with polycysticvary syndrome: a randomized controlled trial.ertil Steril 2008. Mar 3 [Epub ahead of print].5. Vandermolen DT, Ratts VS, Evans WS,toval DW, Kauma SW, Nestler JE. Metformin
ncreases the ovulatory rate and pregnancy raterom clomiphene citrate in patients with poly-ystic ovary syndrome who are resistant to clo-iphene citrate alone. Fertil Steril 2001;75:10-5.6. Sonntag B, Gotte M, Wiilfing P, SchuringN, Kiesel L, Greb RR. Metformin alters insulinignaling and viability of human granulosa cells.ertil Steril 2005;84:1173-9.7. Seibel SA, Chou KH, Capp E, Spritzer PM,on Eye Corleta H. Effect of metformin on IGF-1nd IGFBP-1 levels in obese patients with poly-ystic ovary syndrome. Eur J Obstet Gynecoleprod Biol 2008;138:122-4.8. Tosca L, Chabrolle C, Svetlana U, Dupont. Effects of metformin on bovine granulosaells steroidogenesis: possible involvement ofdenosine 5’ monophosphate-activated pro-ein kinase (AMPK). Biol Reprod 2007;76:68-78.9. Kocak M, Caliskan E, Simsir C, Haberal A.etformin therapy improves ovulatory rates,
ervical scores, and pregnancy rates in clomi-hene citrate resistant women with polycysticvary syndrome. Fertil Steril 2002;77:101-6.0. Malkawi HY, Qublan HS. The effect of met-
ormin plus clomiphene citrate on ovulationnd pregnancy rates in clomiphene-resistantomen with polycystic ovary syndrome. Saudied J 2002;23:663-6.1. Hwu YM, Lin SY, Huang WY, Lin MH, LeeK. Ultra-short metformin pretreatment for clo-iphene citrate-resistant polycystic ovary syn-rome. Int J Gynaecol Obstet 2005;90:39-43.2. Rouzi AA, Ardawi MS. A randomized con-rolled trial of the efficacy of rosiglitazone andlomiphene citrate versus metformin and clomi-hene citrate in women with clomiphene cit-ate-resistant polycystic ovary syndrome. Fertilteril 2006;85:428-35.3. Baillargeon JP, Jakubowicz DJ, Iuorno MJ,akubowicz S, Nestler JE. Effects of metforminnd rosiglitazone, alone and in combination, inonobese women with polycystic ovary syn-rome and normal indices of insulin sensitivity.ertil Steril 2004;82:893-902.4. Van Santbrink EJP, Hohmann FP, Eijke-ans MJC, Laven JSE, Fauser BCJ. Does met-
ormin modify ovarian responsiveness duringxogenous FSH ovulation induction in nor-ogonadotrophic anovulation? A placebo-
ontrolled double-blind assessment. Eur J En-
ocrinol 2005;152:611-7. d08 American Journal of Obstetrics & Gynecology
5. Yarali H, Yildiz BO, Demirol A, et al. Co-dministration of metformin during rFSH treat-ent in patients with clomiphene citrate-resis-
ant polycystic ovarian syndrome: a prospectiveandomized trial. Hum Reprod 2002;17:89-94.6. Palomba S, Falbo A, Orio F Jr, et al. A ran-omized controlled trial evaluating metforminre-treatment and co-administration in non-bese insulin-resistant women with polycys-ic ovary syndrome treated with controlledvarian stimulation plus timed intercourse or
ntrauterine insemination. Hum Reprod 2005;0:2879-86.7. Tang T, Glanville J, Orsi N, Barth JH, BalenH. The use of metformin for women withCOS undergoing IVF treatment. Hum Reprod006;21:1416-25.8. Costello MF, Chapman M, Conway U. Aystematic review and meta-analysis of ran-omized controlled trials on metformin co-ad-inistration during gonadotropin ovulation in-uction or IVF in women with polycystic ovaryyndrome. Hum Reprod 2006;21:1387-99.9. Chang WY, Knochenhauer ES, BartolucciA, Azziz R. Phenotypic spectrum of polycysticvary syndrome: clinical and biochemical char-cterization of the three major clinical sub-roups. Fertil Steril 2005;83:1717-23.0. Genazzani AD, Lanzoni C, Ricchieri F,araldi E, Casarosa E, Jasonni VM. Metformindministration is more effective when non-bese patients with polycystic ovary syndromehow both hyperandrogenism and hyperinsu-
inemia. Gynecol Endocrinol 2007;23:146-52.1. Moghetti P, Castello R, Negri C, et al. Met-
ormin effects on clinical features, endocrinend metabolic profiles, and insulin sensitivity inolycystic ovary syndrome: a randomized, dou-le-blind, placebo-controlled 6-month trial, fol-
owed by open, long-term clinical evaluation.Clin Endocrinol Metab 2000;85:139-46.2. Legro RS, Barnhart HX, Schlaff WD, et al.vulatory response to treatment of polycysticvary syndrome is associated with a polymor-hism in the STK11 gene. J Clin Endocrinoletab 2008;93:792-800.3. Moll E, van der Veen F, van Wely M. The rolef metformin in polycystic ovary syndrome: aystematic review. Hum Reprod Update 2007;3:527-37.4. Giudice LC. Endometrium in PCOS: im-lantation and predisposition to endocrine CA.est Pract Res Clin Endocrinol Metab 2006;0:235-44.5. Jakubowicz DJ, Seppala M, Jakubowicz S,t al. Insulin reduction with metformin increases
uteal phase serum glycodelin and insulin-likerowth factor-binding protein 1 concentrationsnd enhances uterine vascularity and bloodow in the polycystic ovary syndrome. J Clinndocrinol Metab 2001;86:1126-33.6. Jakubowicz DJ, Iuorno MJ, Jakubowicz S,oberts KA, Nestler JE. Effects of metformin onarly pregnancy loss in the polycystic ovary syn-
rome. J Clin Endocrinol Metab 2002;87:524-9. 2DECEMBER 2008
7. Palomba S, Russo T, Orio F Jr, et al. Uterineffects of metformin administration in anovula-ory women with polycystic ovary syndrome.um Reprod 2006;21:457-65.8. Legro RS, Zaino RJ, Demers LM, et al. Theffects of metformin and rosiglitazone, alonend in combination, on the ovary and endome-rium in polycystic ovary syndrome. Am J Ob-tet Gynecol 2007;196:402.e1-10.9. Lord JM, Flight IH, Norman RJ. Insulin-sen-itizing drugs (metformin, troglitazone, rosiglita-one, pioglitazone, D-chiro-inositol) for polycys-ic ovary syndrome. Cochrane Database Systev 2003;3:CD003053. Review.0. Glueck CJ, Phillips H, Cameron D, Sieve-mith L, Wang P. Continuing metformin
hroughout pregnancy in women with polycys-ic ovary syndrome appears to safely reducerst-trimester spontaneous abortion: a pilottudy. Fertil Steril 2001;75:46-52.1. Petitti DB. Combination estrogen-proges-in oral contraceptives. N Engl J Med 2003;49:1443-50.2. Gilbert C, Valois M, Koren G. Pregnancyutcome after first-trimester exposure to met-
ormin: a meta-analysis. Fertil Steril 2006;86:58-63.3. Glueck CJ, Goldenberg P, Wang P,oftspring M, Sherman A. Metformin duringregnancy reduces insulin, insulin resistance,
nsulin secretion, weight, testosterone and de-elopment of gestational diabetes: prospectiveongitudinal assessment of women with poly-ystic ovary syndrome from preconceptionhroughout pregnancy. Hum Reprod 2004;19:10-21.4. Kovo M, Weissman A, Gur D, Levran D,otmensch S, Glezerman M. Neonatal out-ome in polycystic ovarian syndrome patientsreated with metformin during pregnancy. J Ma-ern Fetal Neonatal Med 2006;19:415-9.5. Hellmuth E, Damm P, Molsted-Pedersen L.ral hypoglycemic agents in 118 diabetic preg-ancies. Diabet Med 2000;17:507-11.6. Velazquez EM, Mendoza S, Hamer T, Sosa, Glueck CJ. Metformin therapy in polycysticvary syndrome reduces hyperinsulinemia, in-ulin resistance, hyperandrogenemia, and sys-olic blood pressure, while facilitating normalenses and pregnancy. Metabolism 1994;43:47-54.7. Nawrocka J, Starczewski A. Effects of met-
ormin treatment in women with polycysticvary syndrome depends on insulin resistance.ynecol Endocrinol 2007;23:231-7.8. Marcondes JA, Yamashita SA, Maciel GA,aracat EC, Halpern A. Metformin in normal-eight hirsute women with polycystic ovaryyndrome with normal insulin sensitivity. Gy-ecol Endocrinol 2007;23:273-8.9. Sahin I, Serter R, Karakurt F, et al. Met-
ormin versus flutamide in the treatment of met-bolic consequences of non-obese youngomen with polycystic ovary syndrome: a ran-omized prospective study. Gynecol Endocrinol
004;19:115-24.
8frad8eroo28md8RhwS8oE8RJfesn8Bsstmwd8Ntd48Tcosc28Cpwt
9Dttsw19nic29smd39Rwd49pp29BtJ9RJewd89Jcaeo29daisR9eb
1Ctr31BcpcH1ocd1odr21Melp21TzawE1fld(1ait21AfiJ1ses
www.AJOG.org Reviews
0. Yilmaz M, Biri A, Karakoc A, et al. The ef-ects of rosiglitazone and metformin on insulinesistance and serum androgen levels in obesend lean patients with polycystic ovary syn-rome. J Endocrinol Invest 2005;28:1003-8.1. Ortega-Gonzalez C, Luna S, Hernandez L,t al. Responses of serum androgen and insulinesistance to metformin and pioglitazone inbese, insulin-resistant women with polycysticvary syndrome. J Clin Endocrinol Metab005;90:1360-5.2. Deplewski D, Rosenfield RL. Role of hor-ones in pilosebaceous unit development. En-ocr Rev 2000;21:363-92.3. Kolodziejczyk B, Duleba AJ, SpaczynskiZ, Pawelczyk L. Metformin therapy decreasesyperandrogenism and hyperinsulinemia inomen with polycystic ovary syndrome. Fertilteril 2000;73:1149-54.4. Kelly CJ, Gordon D. The effect of metforminn hirsutism in polycystic ovary syndrome. Eur Jndocrinol 2002;147:217-21.5. Morin-Papunen LC, Vauhkonen I, KoivunenM, Ruokonen A, Martikainen HK, TapanainenS. Endocrine and metabolic effects of met-ormin versus ethinyl-estradiol-cyproterone ac-tate in obese women with polycystic ovaryyndrome: a randomized study. J Clin Endocri-ol Metab 2000;85:3161-8.6. Luque-Ramirez M, Alvarez-Blasco F,otella-Carretero JI, Martinez-Bermejo E, La-uncion MA, Escobar-Morreale HF. Compari-on of ethinyl-estradiol plus cyproterone ace-ate versus metformin effects on classicetabolic cardiovascular risk factors in womenith the polycystic ovary syndrome. J Clin En-ocrinol Metab 2007;92:2453-61.7. Harborne L, Fleming R, Lyall H, Sattar N,orman J. Metformin or antiandrogen in the
reatment of hirsutism in polycystic ovary syn-rome. J Clin Endocrinol Metab 2003;88:116-23.8. Gambineri A, Patton L, Vaccina A, et al.reatment with flutamide, metformin, and theirombination added to a hypocaloric diet inverweight-obese women with polycystic ovaryyndrome: a randomized, 12-month, placebo-ontrolled study. J Clin Endocrinol Metab006;91:3970-80.9. Ehrmann DA, Barnes RB, Rosenfield RL,avaghan MK, Imperial J. Prevalence of im-aired glucose tolerance and diabetes inomen with polycystic ovary syndrome. Diabe-
es Care 1999;22:141-6. N
0. Legro RS, Kunselman AR, Dodson WC,unaif A. Prevalence and predictors of risk for
ype 2 diabetes mellitus and impaired glucoseolerance in polycystic ovary syndrome: a pro-pective, controlled study in 254 affectedomen J Clin Endocrinol Metab 1999;84:65-9.1. Legro RS, Gnatuk CL, Kunselman AR, Du-aif A. Changes in glucose tolerance over time
n women with polycystic ovary syndrome: aontrolled study. J Clin Endocrinol Metab005;90:3236-42.2. Palomba S, Falbo A, Russo T, et al. Insulinensitivity after metformin suspension in nor-al-weight women with polycystic ovary syn-rome. J Clin Endocrinol Metab 2007;92:128-35.3. Harborne LR, Sattar N, Norman JE, Fleming. Metformin and weight loss in obese womenith polycystic ovary syndrome: comparison ofoses. J Clin Endocrinol Metab 2005;90:593-8.4. Salpeter SR, Buckley NS, Kahn JA, Sal-eter EE. Meta-analysis: metformin treatment inersons at risk for diabetes mellitus. Am J Med008;121:149-57.5. Korytkowski MT, Mokan M, Horwitz MJ,erga SL. Metabolic effects of oral contracep-
ives in women with polycystic ovary syndrome.Clin Endocrinol Metab 1995;80:3327-34.6. Morin-Papunen LC, Vauhkonen I, KoivunenM, Ruokonen A, Martikainen HK, TapanainenS. Metformin versus ethinyl-estradiol-cyprot-rone acetate in the treatment of nonobeseomen with polycystic ovary syndrome: a ran-omized trial. J Clin Endocrinol Metab 2003;8:148-56.7. Costello M, Shrestha B, Eden J, Sjoblom P,ohnson N. Insulin-sensitizing drugs versus theombined oral contraceptive pill for hirsutism,cne and risk of diabetes, cardiovascular dis-ase, and endometrial cancer in polycysticvary syndrome. Cochrane Database Syst Rev007;1:CD005552.8. Elter K, Imir G, Durmusoglu F. Clinical, en-ocrine and metabolic effects of metformindded to ethinyl-estradiol-cyproterone acetate
n non-obese women with polycystic ovarianyndrome: a randomized controlled study. Humeprod 2002;17:1729-37.9. Knowler WC, Barrett-Connor E, Fowler SE,t al. Reduction in the incidence of type 2 dia-etes with lifestyle intervention or metformin.
Engl J Med 2002;346:393-403. JDECEMBER 2008 Am
00. Sharma ST, Wickham EP III, Nestler JE.hanges in glucose tolerance with metformin
reatment in polycystic ovary syndrome: a ret-ospective analysis. Endocr Pract 2007;13:73-9.01. Tang T, Glanville J, Hayden CJ, White D,arth JH, Balen AH. Combined lifestyle modifi-ation and metformin in obese patients witholycystic ovary syndrome: a randomized, pla-ebo-controlled, double-blind multicenter study.um Reprod 2006;21:80-9.02. Meyer C, McGrath BP, Teede HJ. Effectsf medical therapy on insulin resistance and theardiovascular system in polycystic ovary syn-rome. Diabetes Care 2007;30:471-8.03. Lakhani K, Prelevic GM, Seifalian AM, Ati-mo WU, Hardiman P. Polycystic ovary syn-rome, diabetes and cardiovascular disease:isk and risk factors. J Obstet Gynaecol004;24:613-21.04. Rautio K, Tapanainen JS, Ruokonen A,orin-Papunen LC. Effects of metformin and
thinyl estradiol-cyproterone acetate on lipidevels in obese and non-obese women witholycystic ovary syndrome. Eur J Endocrinol005;152:269-75.05. Tarkun I, Cetinarslan B, Turemen E, Sahin, Canturk Z, Komsuoglu B. Effects of rosiglita-one on insulin resistance, C-reactive proteinnd endothelial function in non-obese youngomen with polycystic ovary syndrome. Eur Jndocrinol 2005;153:115-9.06. Topcu S, Tok D, Caliskan M, et al. Met-
ormin therapy improves coronary microvascu-ar function in patients with polycystic ovary syn-rome and insulin resistance. Clin Endocrinol
Oxf) 2006;65:75-80.07. Diamanti-Kandarakis E, Paterakis T, Alex-ndraki K, et al. Indices of low-grade chronic
nflammation in polycystic ovary syndrome andhe beneficial effect of metformin. Hum Reprod006;21:1426-31.08. Morin-Papunen LC, Rautio K, Ruokonen, Hedberg P, Puukka M, Tapanainen JS. Met-
ormin reduces serum C-reactive protein levelsn women with polycystic ovary syndrome.
Clin Endocrinol Metab 2003;88:4649-54.09. Salley KES, Wickham EP, Cheang KI, Es-ah PA, Karjane NW, Nestler JE. Glucose intol-rance in polycystic ovary syndrome–a positiontatement of the Androgen Excess Society.
Clin Endocrinol Metab 2007;92:4546-56.erican Journal of Obstetrics & Gynecology 609