Embed Size (px)
Citation preview

Stephen R Hammes, M.D., Ph.D.
Division of Endocrinology and Metabolism
University of Rochester Medical Center
Polycystic Ovary Syndrome: Are Androgens
all Bad in Women?

Stein-Leventhal Description of PCOS

Stein-Leventhal Description of PCOS
Stein I.F. and Leventhal M.L. (1935) American Journal of Obstetrics and Gynecology 29, 181-191.

Outline
1. Definition of PCOS
2. Pathophysiology of PCOS
3. Treatment of PCOS
4. Are androgens all bad??

Some Basic Facts and Statistics about PCOS
1. The incidence of PCOS is 5 - 10% of reproductive age women.
2. PCOS is one of the leading cause of infertility in women.
3. PCOS is often associated with obesity and metabolic syndrome;
thus, as the obesity epidemic rages on, so does PCOS.
4. About 50% of women with PCOS also have insulin resistance.
This number increases as the population becomes more obese.

1. Hyperandrogenemia - either with laboratory values or with
Symptoms (e.g., hirsutism, acne, balding, voice deepening)
2. Oligomenorrhea - periods less frequent than every 35 days
or 10 per year
3. Exclusion of related disorders
Definition of PCOS
1990 NIH Consensus Conference

1. Oligo- or anovulation
2. Clinical or biochemical signs of hyperandrogenemia
3. Polycystic ovaries
Definition of PCOS
Rotterdam Criteria (2003)
In addition to excluding other causes, two of the following are needed:

>12 follicles of 2-9 mm diameter
and/or an ovarian volume >10cm3
PCOS Ultrasounds

Ways to Measure Testosterone
Total Testosterone
2% Free 98% Protein Bound
80% SHBG (tight)20% Albumin (loose)
Bioavailable
Testosterone

Ways to Measure Testosterone
Total Testosterone
2% Free 98% Protein Bound
80% SHBG (tight)20% Albumin (loose)
Bioavailable
Testosterone
What we use:
1. Free and total testosterone by LC-MS/MS
2. SHBG
3. Calculate BAT: www.issam.ch/freetesto.htm

The definition of PCOS is a moving target, but most
agree that one needs to have:
1. Biochemical or clinical Hyperandrogenemia
2. Oligo/Anovulation

What is the Pathophysiology of PCOS?

Hormone Levels During the Menstrual Cycle
Follicular Phase Luteal Phase
Ovulation
Estrogen
LH
FSH
Progesterone
14 280Day:

Oocyte
Pituitary
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
Hypothalamic/Pituitary/Gonadal Axis

Oocyte
Pituitary
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
GnRH is Secreted from the Hypothalamus in
a pulsatile Fashion

Oocyte
Pituitary
FSH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
GnRH First Stimulates FSH Secretion

Pituitary
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
FSH Promotes Follicle Growth
FSH

Pituitary
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
FSH Increases Aromatase Activity; thus
Increasing Estradiol Secretion
EstradiolFSH

Pituitary
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
EstradiolFSH
Estradiol Acutely Increases GnRH Secretion

Pituitary
FSH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH (+)
Inhibin (-)
LH
Increased Pulsatile GnRH Secretion Favors
LH over FSH Release

Pituitary
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
OVULATION
(Oocyte and
Corpus Luteum)
The LH Surge Triggers Ovulation
GnRH
LH

Pituitary
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
Progesterone is Secreted from the Ovary
and the Corpus Luteum
Progesterone
OVULATION
(oocyte and
Corpus luteum)
GnRH

Pituitary
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
OVULATION
(oocyte and
Corpus luteum)
Progesterone Slows Pulsatile GnRH Secretion
Progesterone

Pituitary
Hypothalamus
GnRH
Corpus Luteum
Loss
Progesterone
As Progesterone Drops, Pulsatile GnRH Increases
And the cycle Starts Again
OocyteCumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells

Summary of Normal Cycling
1. GnRH is secreted in a pulsatile fashion.
2. FSH stimulates follicle growth and estradiol secretion.
3. High levels of estradiol acutely increase GnRH pulsatility,
resulting in an LH surge and ovulation.
4. Progesterone suppresses GnRH pulsatility to reset the axis.
5. Progesterone withdrawal starts the GnRH pulses again.

Summary of Normal Cycling
1. GnRH is secreted in a pulsatile fashion.
2. FSH stimulates follicle growth and estradiol secretion.
3. High levels of estradiol acutely increase GnRH pulsatility,
resulting in an LH surge and ovulation.
4. Progesterone suppresses GnRH pulsatility to reset the axis.
5. Progesterone withdrawal starts the GnRH pulses again.
6. What does the elevated testosterone in PCOS do to all of this?

Testosterone stimulates GnRH secretion
in the hypothalamus

Testosterone Blocks the Suppressive Effects of
Progesterone on GnRH Pulsatility
Pastor, C. L. et al. J Clin Endocrinol Metab 1998;83:582-590

Pituitary
Hypothalamus
GnRH
Pulsatile GnRH Secretion is Increased in PCOS
OocyteCumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells

Pituitary
LH/FSH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
Excess GnRH Stimulates FSH and LH Secretion

Pituitary
LH
FSH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
Inhibin Blocks FSH Secretion
Inhibin (-)

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
Without Aromatase, LH Stimulates
Ovarian Testosterone Secretion
Testosterone
LH
FSH
Inhibin (-)

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
Testosterone Further Stimulates GnRH Pulsatility
Testosterone
LH
FSH
Inhibin (-)

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
The Vicious Positive Feedback Loop of PCOS
Testosterone
LH
FSH
Inhibin (-)

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
Without Ovulation, No Progesterone is Made
To Inhibit GnRH Secretion
Testosterone
LH
FSH
Inhibin (-)
No Ovulation -
No Progesterone

Excess Androgens from any Source can
Result in PCOS

NORMAL6 YEARS
AFFECTED4 YEARS
AFFECTED2 YEARS

Cholesterol
Pregnenolone
DHEA
17OH-Pregnenolone 17OH-Progesterone
Androstenedione
Progesterone
StAR
CYP11A1 CYP21
CYP17
CYP17
CYP17
CYP17
3bHSD
3bHSD
Adrenal Source of Androgens:
Congenital Adrenal Hyperplasia
Aldosterone
Cortisol
CYP21
3bHSD
CAH

Cholesterol
Pregnenolone
DHEA
17OH-Pregnenolone 17OH-Progesterone
Androstenedione
Progesterone
StAR
CYP11A1 CYP21
CYP17
CYP17
CYP17
CYP17
3bHSD
3bHSD
Adrenal Source of Androgens:
Congenital Adrenal Hyperplasia
Aldosterone
Cortisol
CYP21
3bHSD
CAH

Adrenal Source of Androgens:
Congenital Adrenal Hyperplasia
Increased: Not Increased:
1. Polycystic ovaries 1. Insulin Resistance
2. Ovarian androgen production
3. Infertility
Suggests:
1. Androgens themselves are capable of promoting PCOS.
2. Androgen exposure in-utero may initiate a “program”that results in PCOS.


Exogenous Source of Androgens
1. Anabolic Steroid Abuse
a. More polycystic ovaries and problems with fertility
b. Less insulin resistance
Franke and Berendonk (1997), Hormonal doping and androgenization of athletes:
a secret program of the German Democratic Republic government,
Clinical Chemistry 43, 1262-1279.
2. Female to male transgender patients
a. Increased ovarian size and number of cystic follicles
b. Increased androgen receptor expression in ovary and
uterus
Pache et. al. (1991) Histopathology 19, 445-452
Chadha et. al. (1994) Human Pathology 25, 1198-1204

What about Insulin Resistance?

What about Insulin Resistance?
Relative to mock-treated rats, rats treated with IV insulin for four
weeks had:
1. Abnormal estrus cycles
2. Increased testosterone
3. Decreased progesterone
4. Abnormal Follicular Growth
Chakrabarty et. al (2006) J. Soc. Gynecol. Investig 13, 122-129.

Nestler et. al. (1998) JCEM 83, 2001-2005
The Ovaries in PCOS Patients May be More
Sensitive to Insulin-Stimulated Testosterone
Production

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
Insulin and PCOS
Testosterone
LH
FSH
Inhibin (-)
Insulin

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
Treatment of PCOS
Testosterone
LH
FSH
Inhibin (-)

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
Testosterone
LH
FSH
Inhibin (-)
Treatment of PCOS

Wedge Resection or Ovarian Mining
1. Used since the time of Stein and Leventhal
2. Remove part of ovary to decrease ovarian androgen production
3. Decreased androgen levels will improve symptoms and
hyperandrogenemia and will break the positive feedback to permit
cycling to resume.
Farquhar (2004) Best Practice & Research Clinical Obst. and Gyn. 18, 789-802.

Wedge Resection or Ovarian Mining
4. Can sometimes improve pregnancy rates
5. Many small studies demonstrate success, but never a good,
randomized, controlled study.
6. Long term concerns with surgery include adhesions and an
increased incidence of premature ovarian failure.
Farquhar (2004) Best Practice & Research Clinical Obst. and Gyn. 18, 789-802.

Insulin Sensitizers
1. Metformin and thiazolidinediones
2. Improve insulin sensitivity, which then lowers insulin levels
3. Decreased insulin signaling in the ovary may lower insulin-
mediated steroidogenesis.
4. These drugs may also directly inhibit ovarian steroidogenesis

Insulin Sensitizers
5. Improve cycling and ovulation rates in many patients
6. Improve fertility in some studies.

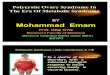
Insulin Sensitizers Improve Ovulation
Ibanez et. al. (2001) JCEM 86, 3595-3598

Insulin Sensitizers
Ibanez et. al. (2001) JCEM 86, 3595-3598
Insulin: 16.1 to 11.1
BMI=21.4 - no change

Androgen Receptor Blockade
Spironolactone
1. Improves signs of hyperandrogenemia – hirsutism, acne, etc.
2. Cycling can improve over 6-12 months
3. Testosterone and insulin levels can be lower (similar to metformin)
4. Improvements correlate with BMI - better results with lower BMI.
5. Necessary doses range from 50 – 200 mg per day.
6. Not to be used to improve fertility

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
The Ovarian Axis in PCOS
Testosterone
LH
FSH
Inhibin (-)

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
The Ovarian Axis in PCOS
Testosterone
LH
FSH
Inhibin (-)

Oral Contraceptives
1. High estrogen and progesterone levels suppress GnRH
pulsations, thus lowering LH and testosterone levels.
2. Can use progesterone alone, at it will still suppress GnRH
pulsations.
3. Symptoms of hyperandrogenemia will improve.
4. Will establish regular periods.
5. Not useful if goal is pregnancy.

GnRH Agonists and OCPs Lower Testosterone
Equally Well in Patients with PCOS
Carr et. al. (1995) JCEM 80, 169-1178

Pituitary
LH
Cumulus
Granulosa Cells
Mural
Granulosa Cells
Theca Cells
Hypothalamus
GnRH
Stop the Positive Feedback Loop!
Testosterone
LH
FSH
Inhibin (-)

To Best Improve Fertility, Ovulation Induction
is Still the Most Effective
Clomiphene Citrate
1. Estrogen agonist/antagonist (SERM)
2. Start at 50 mg per day for 5 days on 5th day of
cycle
3. Increases FSH production and estradiol
production
4. After stopping, surge in estrogen signaling
enhances GnRH pulsatility and LH secretion.
5. Enhanced ovulation
6. Improves fertility better than metformin

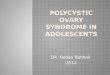
Clomiphene Induces Ovulation Better than
Metformin
Legro et. al. (2007) NEJM 356, 551-566

BMI dropped a little in both metformin groups (35 to 34kg/m2)
Insulin levels did not change in any group
Testosterone dropped in both metformin groups (62 to 53 ng/dL)
The higher the BMI, the less effective for all treatments combined
Clomiphene Induces Ovulation Better than
Metformin

To Best Improve Fertility, Ovulation Induction
is Still the Most Effective
Aromatase Inhibitor
1. Take 5 days starting the 3rd day of cycle
(2.5 -5 mg letrozole)
2. Blocks estrogen production
3. Increased FSH production
4. Estrogen surge when drug is stopped
5. Triggers LH release from pituitary
6. Improves fertility

Letrozole Works as Well as Clomiphene in
Inducing Ovulation
Legro et al, N Engl J Med 2014; 371:119-129

If Too Many Androgens Cause Unregulated
Follicle Overgrowth, then What Happens with
Too Little Androgen?

Androgen Receptor Knockout Mice have
Decreased Fertility
Hu et. al. (2004), PNAS 101, 11209-14
Kato (2006), PNAS 103, 224-9
Reduced litter numbers
Reduced Litter sizes
Smaller ovarian follicles
Premature Ovarian Failure

Hypothalamus
Pituitary
Uterus
Ovary
Theca cells
Granulosa cells
Oocytes
The Follicle
Androgen Receptor is Expressed
Throughout the HPG Axis

Hypothalamus
Pituitary
Uterus
Ovary
Theca cells
Oocytes
The Follicle
Granulosa cells
Androgen Receptor is Expressed
Throughout the HPG Axis

Loss of AR in Granulosa Cells Results in:
Reduced litter numbers
Reduced Litter sizes
Smaller ovarian follicles
Premature Ovarian Failure
Sen and Hammes (2010) Molecular Endocrinology 24, 1393-403

Androgens Promote Follicle Growth
and Prevent Follicle Atresia
Primary Pre-Antral Antral Ovulation
Corpus Luteum
Primordial
Atresia
AR
AR
Sen and Hammes (2010) Molecular Endocrinology 24, 1393-403
Sen and Hammes (2014) PNAS 111, 3008-13
Ma, Hammes, and Sen (2017) Endocrinology 158, 2944-2954

Sunkara and Coomarasamy (2011), Fertility and Sterility 95, 73-74
DHEA Treatment in Patient with
Diminished Ovarian Reserve Might
Improve Pregnancy Rate

“Balance is Key”Mr. Miyagi
Too many androgens: PCOS
Too few androgens: Diminished Ovarian Reserve

Summary
1. Androgens are important for normal ovarian function.
2. Too many androgens leads to PCOS, a common disease that is
becoming even more prevalent.
3. Too few androgens may lead to diminished ovarian reserve.
4. PCOS is accompanied by significant co-morbidities, including the
metabolic syndrome and insulin resistance.
5. Etiologies of PCOS are diverse; however, the result is a powerful
positive feedback loop involving neuronal and ovarian signaling.
6. Treatment strategies for PCOS should focus on goals and
expectations of the patient.