Embed Size (px)
Citation preview

UPMC Pathology Resident Didactic Series
March 31 & April 7, 2009
CNS NEOPLASMS
Scott M. Kulich, MD, PhDVA Pittsburgh Healthcare SystemAssistant ProfessorDivision of NeuropathologyDepartment of Pathology
University of Pittsburgh
Acknowledgements:Marta Couce, MD, PhDRonald Hamilton, MD
Geoff Murdoch, MD, PhD

Outline• Neuroradiology for pathologists• Familial tumor syndromes • CNS neoplasms
– Astrocytic neoplasms• Diffuse astrocytomas -> GBM
– Variants
• Pilocytic astrocytomas• Pleomorphic xanthoastrocytoma• Subependymal giant cell astrocytoma
– Oligodendrogliomas• Oligoastrocytomas
– Other neuroepithelial • Angiocentric glioma, chordoid glioma, astroblastoma
– Ependymomas

Outline (CNS neoplasms cont.)• Choroid plexus
• Neuronal - Neuroglial Tumors– Ganglioglioma
– Central neurocytoma
– Paraganglioma
• Embryonal tumors
• Meningeal tumors

Outline• Neuroradiology for pathologists• Familial tumor syndromes • CNS neoplasms
– Astrocytic neoplasms• Diffuse astrocytomas -> GBM
– Variants
• Pilocytic astrocytomas• Pleomorphic xanthoastrocytoma• Subependymal giant cell astrocytoma
– Oligodendrogliomas• Oligoastrocytomas
– Other neuroepithelial • Angiocentric glioma, chordoid glioma, astroblastoma
– Ependymomas

NEURORADIOLOGY FOR PATHOLOGISTSQuestion: Who cares?

NEURORADIOLOGY FOR PATHOLOGISTSQuestion: Who cares?
Answer: You will when your favorite neurosurgeon hands you a piece of tissue the size of a grain of salt and tells you he needs you to tell him if he can go ahead and stick Gliadel chemotherapeutic wafers in the patient’s brain

NEURORADIOLOGY FOR PATHOLOGISTSQuestion: Who cares?
Neuroradiology = Gross pathology
Answer: You will when your favorite neurosurgeon hands you a piece of tissue the size of a grain of salt and tells you he needs you to tell him if he can go ahead and stick Gliadel chemotherapeutic wafers in the patient’s brain

NEURORADIOLOGY FOR PATHOLOGISTS
• Two main imaging techniques– Computerized tomography (CT)
• 3D X-rays • White areas = areas that absorb or “attenuate”
the passage of x-ray beam (acute hematoma, bone, calcium = hyperdense/ attenuating)
• Black areas = areas that do not absorb or “attenuate” the passage of x-ray beam (fat, air, CSF, edema = hypodense/ attenuating)
Neuroradiology for

Neuroradiology for

NEURORADIOLOGY FOR PATHOLOGISTS
• Magnetic resonance imaging (MRI)• Not ionizing radiation but magnetic field to
excite protons which emit “signal” upon relaxation
• Image appearance dependent upon time interval between each excitation and time interval between each collection
• Two basic “weights” of images based upon TE and TR
– T1: Short TE and TR » T1 is the one…that looks like a brain
– T2 :Long TE and TR

NEURORADIOLOGY FOR PATHOLOGISTS
• Magnetic resonance imaging (MRI)• Not ionizing radiation but magnetic field to
excite protons which emit “signal” upon relaxation
• Image appearance dependent upon time interval between each excitation and time interval between each collection
• Two basic “weights” of images based upon TE and TR
– T1: Short TE and TR » T1 is the one…that looks like a brain
– T2 :Long TE and TR

NEURORADIOLOGY FOR PATHOLOGISTS
• Magnetic resonance imaging (MRI)• Not ionizing radiation but magnetic field to
excite protons which emit “signal” upon relaxation
• Image appearance dependent upon time interval between each excitation and time interval between each collection
• Two basic “weights” of images based upon TE and TR
– T1: Short TE and TR » T1 is the one…that looks like a brain
– T2 :Long TE and TR

NEURORADIOLOGY FOR PATHOLOGISTS
• T1

NEURORADIOLOGY FOR PATHOLOGISTS
• T2

NEURORADIOLOGY FOR PATHOLOGISTS
• Important info to glean from neuroimaging– Age– Location, location, location– Multicentricity– Bilateral hemisphere involvement– Architecture– Contrast enhancement– Interaction with surrounding tissue

Location, location, location…

Location, location, location…
CHILDREN

Location, location, location…ADULTS


NEURORADIOLOGY FOR PATHOLOGISTS
• Multicentricity– Neoplasms
• Metastatic disease• Others (lymphoma, high-grade glioma,…)
– Non-neoplastic• Demyelinating disease• Infectious
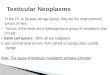
• Bilateral hemisphere involvement– “butterfly” lesion
• Glioblastoma multiforme (GBM), lymphoma

NEURORADIOLOGY FOR PATHOLOGISTS
• Multicentricity– Neoplasms
• Metastatic disease• Others (lymphoma, high-grade glioma,…)
– Non-neoplastic• Demyelinating disease• Infectious
• Bilateral hemisphere involvement– “butterfly” lesion
• Glioblastoma multiforme (GBM), lymphoma

NEURORADIOLOGY FOR PATHOLOGISTS:Butterfly lesion (GBM)

NEURORADIOLOGY FOR PATHOLOGISTS
• Architecture– CYSTIC = LOW-GRADE
• JPA (juvenile pilocytic astrocytoma), PXA (pleomorphic xanthoastrocytoma), ganglion cell tumors,
• Others (hemangioblastoma, craniopharygioma, supratentorial ependymomas, extraventricular neurocytoma)
• Frequently associated with a mural nodule (JPA, PXA, hemangioblastoma, ganglion cell tumors,PGNT, extraventricular neurocytoma)
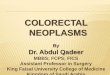
– Dural tail• Meningioma

NEURORADIOLOGY FOR PATHOLOGISTS:JPA

NEURORADIOLOGY FOR PATHOLOGISTS
• Architecture– CYSTIC = LOW-GRADE
• JPA (juvenile pilocytic astrocytoma), PXA (pleomorphic xanthoastrocytoma), ganglion cell tumors,
• Others (hemangioblastoma, craniopharygioma, supratentorial ependymomas, extraventricular neurocytoma)
• Frequently associated with a mural nodule (JPA, PXA, hemangioblastoma, ganglion cell tumors,PGNT, extraventricular neurocytoma)
– Dural tail• Meningioma

NEURORADIOLOGY FOR PATHOLOGISTS:Meningioma

NEURORADIOLOGY FOR PATHOLOGISTS
• Contrast enhancement– Breached blood-brain barrier– Seen with neoplasms but can be seen with other
conditions (e.g. infectious, demyelinating, …)– Pattern of enhancement often helpful
• Homogeneous versus non-homogeneous– Lymphoma, hemangiopericytoma, meningioma– GBM, mets, abscesses
• Patchy versus circumferential ( i.e. ring enhancement)

NEURORADIOLOGY FOR PATHOLOGISTS
• Contrast enhancement– Breached blood-brain barrier– Seen with neoplasms but can be seen with other
conditions (e.g. infectious, demyelinating, …)– Pattern of enhancement often helpful
• Homogeneous versus non-homogeneous– Lymphoma, hemangiopericytoma, meningioma– GBM, mets, abscesses
• Patchy versus circumferential ( i.e. ring enhancement)

NEURORADIOLOGY FOR PATHOLOGISTSHeterogeneous enhancement (GBM)

NEURORADIOLOGY FOR PATHOLOGISTSHomogeneous enhancement (Meningioma)

NEURORADIOLOGY FOR PATHOLOGISTS
• Interaction with surrounding tissue– Edema
• “Activity” of lesion– Malignant neoplasms– Inflammatory lesions
– Skull• Erosion: Long-standing low-grade lesions
– Dysembryoplastic neuroepithelial tumor (DNET), PXA, ganglion cell tumors,oligodendrogliomas,epidermoid cysts
• Hyperostosis– Meningiomas

NEURORADIOLOGY FOR PATHOLOGISTS
• Interaction with surrounding tissue– Edema
• “Activity” of lesion– Malignant neoplasms– Inflammatory lesions
– Skull• Erosion: Long-standing low-grade lesions
– Dysembryoplastic neuroepithelial tumor (DNET), PXA, ganglion cell tumors,oligodendrogliomas,epidermoid cysts
• Hyperostosis– Meningiomas

NEURORADIOLOGY FOR PATHOLOGISTS
• Interaction with surrounding tissue– Edema
• “Activity” of lesion– Malignant neoplasms– Inflammatory lesions
– Skull• Erosion: Long-standing low-grade lesions
– Dysembryoplastic neuroepithelial tumor (DNET), PXA, ganglion cell tumors,oligodendrogliomas,epidermoid cysts
• Hyperostosis– Meningiomas

Approach to intraoperative consults

Approach to intraoperative consults
• Review of imaging and history
• Questions for surgeon– What do you NEED to know?– Can you get more tissue if necessary?
• Specimen preparation– Intraoperative cytology vs frozen sections
• touch and smear preparations

Approach to intraoperative consults
• Review of imaging and history
• Questions for surgeon– What do you NEED to know?– Can you get more tissue if necessary?
• Specimen preparation– Intraoperative cytology vs frozen sections
• touch and smear preparations

Approach to intraoperative consults
• Review of imaging and history
• Questions for surgeon– What do you NEED to know?– Can you get more tissue if necessary?
• Specimen preparation– Intraoperative cytology vs frozen sections
• touch and smear preparations

Approach to intraoperative consults
• Specimen preparation– Intraoperative cytology
• Smear preparations

Approach to intraoperative consults
• Specimen preparation– Intraoperative cytology
• Smear preparations

A “Wiley” approach to intraoperative consults

A “Wiley” approach to intraoperative consults

A “wiley” approach to intraoperative consults
• Abnormal versus normal
• Reactive versus neoplastic
• Primary versus metastatic
• Grade of lesion
• Does diagnosis correlate with clinical and imaging data?

A “wiley” approach to intraoperative consults
• Abnormal versus normal
• Reactive versus neoplastic
• Primary versus metastatic
• Grade of lesion
• Does diagnosis correlate with clinical and imaging data?

A “wiley” approach to intraoperative consults
• Abnormal versus normal
• Reactive versus neoplastic
• Primary versus metastatic
• Grade of lesion
• Does diagnosis correlate with clinical and imaging data?

A “wiley” approach to intraoperative consults
• Abnormal versus normal
• Reactive versus neoplastic
• Primary versus metastatic
• Grade of lesion
• Does diagnosis correlate with clinical and imaging data?

A “wiley” approach to intraoperative consults
• Abnormal versus normal
• Reactive versus neoplastic
• Primary versus metastatic
• Grade of lesion
• Does diagnosis correlate with clinical and imaging data?

Kulich
Any questions?