Embed Size (px)
Citation preview

Updates in the Treatment of Sepsis
Mitchell J Daley, PharmD, FCCM, BCPSClinical Pharmacy Specialist, Critical Care
Dell Seton Medical Center at the University of Texas and Seton Healthcare Family
Clinical Adjunct Faculty
University of Texas College of Pharmacy

Conflicts of Interest
Nothing to disclose

Objectives
1. Discuss emerging controversies related to fluid resuscitation in sepsis
2. Devise a treatment strategy for the management of vasopressor therapy for cardiovascular support of septic shock
3. Evaluate recent evidence related to metabolic and endocrine resuscitation in the treatment of sepsis

Outline
✓Definitions
✓ Bundled resuscitation
✓ Fluid Resuscitation✓ Balanced salt vs. “normal” saline
✓ Colloids
✓ Predicting fluid responsiveness
✓ Vasopressor therapy ✓ Catecholamines
✓ Vasopressin
✓ Weaning
✓ Angiotensin II
✓ Metabolic resuscitation✓ Steroids
✓ Vitamin C + thiamine
✓ Early Antibiotics

Sepsis and Septic Shock• Greek for decompensation of organic material by bacteria• Used for 2700 years with little change in meaning
– Hippocrates: “flesh rots and wounds fester”– Historically thought localized infection → bloodstream– Advent of antibiotics really highlighted the “host theory”
• Pro-inflammatory AND anti-inflammatory reactions • Tremendous healthcare burden in the US
– Mortality 20-55% with persistent ↓ physical and cognitive function– Cost: more than $20 billion annually
• Difficult to define clinically with attempts starting in 1992 (SIRS)
Angus DC, et al. NEJM 2013;369:840.

Sepsis Definitions: Version 3.0
Singer M, et al. JAMA 2016; 315: 801.
Septic Shock 2001
Severe sepsis Hypoperfusion
Severe Sepsis 2001
Sepsis≥ 1 sign of organ
dysfunction
Sepsis 2001
Systemic inflammatory response syndrome (SIRS)
Documented or suspected infection
Septic Shock 2016
Metabolic/cellular abnormalities ↑ mortality
Vasopressors for MAP >65
Lactate ≥ 2 despite fluid
Sepsis 2016
Life-threatening organ dysfunction caused by
dysregulated host response to infection
Non-ICU: 2/3 quick SOFA
ICU: SOFA ≥ 2 change

Applying SOFA and qSOFA
Ferreira FL, et al. JAMA 2001;286:1754.
qSOFA
SBP ≤ 100 mm Hg
RR ≥ 22 bpm
Altered mental status (GCS < 15)
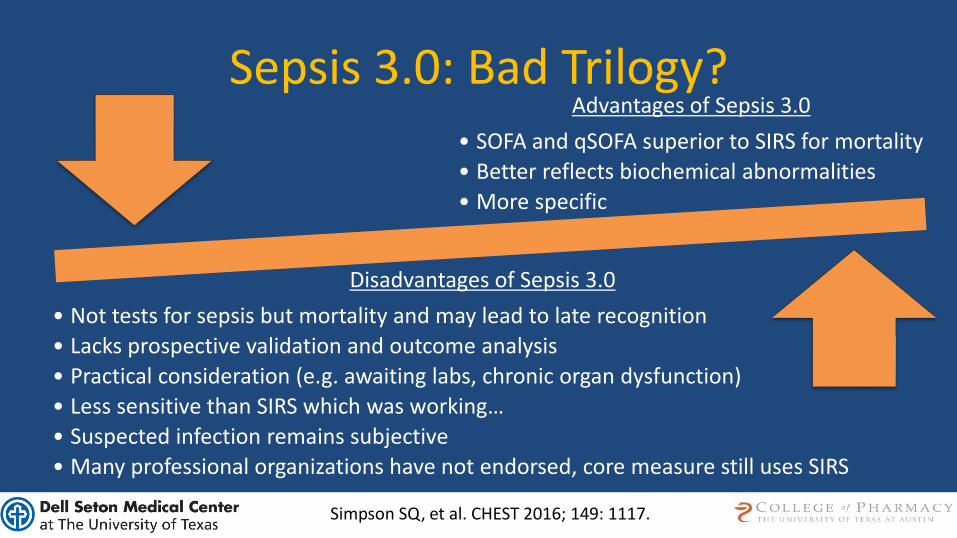
Sepsis 3.0: Bad Trilogy? Advantages of Sepsis 3.0
• SOFA and qSOFA superior to SIRS for mortality
• Better reflects biochemical abnormalities
• More specific
Disadvantages of Sepsis 3.0
• Not tests for sepsis but mortality and may lead to late recognition
• Lacks prospective validation and outcome analysis
• Practical consideration (e.g. awaiting labs, chronic organ dysfunction)
• Less sensitive than SIRS which was working…
• Suspected infection remains subjective
• Many professional organizations have not endorsed, core measure still uses SIRS
Simpson SQ, et al. CHEST 2016; 149: 1117.

Case: RM
• RM is a 56 y/o, 66 kg, male admitted to ED w/ CAP• BP 83/47 mm Hg, lactate 6.2 mmol/L; UOP 30 mL/hour• In addition to antibiotics, which would be the best
therapy for RM right now?A. NS - targeting a CVP of 8 mm HgB. Albumin 5% - 500 mLC. LR - 30 mL/kgD. LR - if stroke volume variability >12%

Early Goal Directed Therapy
Angus DC, et al. Intensive Care Med 2015;41:1549.
ProMISe 184/623 181/620 32.23 1.02 (0.80, 1.30)
Jones 34/150 25/150 4.87 1.47 (0.82, 2.60)
Test for overall effect: p=0.90
ARISE 147/792 150/796 30.71 0.98 (0.76, 1.26)
ProCESS 92/439 167/902 21.78 1.17 (0.88, 1.55)
Rivers 38/130 59/133 10.40 0.52 (0.31, 0.86)
Overall 495/2134 582/2601 100.00 1.01 (0.88, 1.16)Test for heterogeneity: I2 =56.7%, p=0.055
0.3 1 3 Favors EGDT
StudyEvents, EGDT
Events, Control Weight %
OR (fixed)(95% CI)
Favors control
Primary Mortality Outcome

Surviving Sepsis Bundle
2016
• Within 3 hours of recognition– Measure lactate, repeat if ↑
– Obtain blood cultures
– Administer antibiotics
– Give 30 ml/kg fluid
• Within 6 hours of recognition– Apply pressor if hypotension
– Focused exam
2018
• Within 1 hour of triage– Measure lactate, repeat if ↑
– Obtain blood cultures prior to antibiotics
– Begin 30 ml/kg fluid for hypotension of lactate >4
– Apply pressors if hypotensive during or after fluid to maintain MAP > 65 mm Hg
Crit Care Clin 2016;32:539-546

Fluid Resuscitation• Primary focus for years has early fluid resuscitation
– Intravenous fluids are given to ↑ preload, ↑ stroke volume, ↑ cardiac output
– Maximize oxygen delivery
• Surviving sepsis recommends 30 mL/kg within 3 hr– Life after “Early Goal Directed Therapy”– Average volume from PROCESS, ARISE and PROMISE (2 L)– Fixed volume facilitate early aggressive resuscitation– Controversial…
Crit Care Clin 2016;32:539-546

Total Body Water (TBW) - 1896Intracellular fluid (ICF)
2/3 total body water
Extracellular fluid (ECF)
1/3 total body water
Intracellular fluid
66% of TBW
Intra-vascular
¼ ECF
8.25% TBW
↑ osmoticpressure
Interstitial
¾ ECF
24.75% TBW
↓ osmotic pressure
Pumps
Sem
iper
mea
ble
m
emb
ran
e
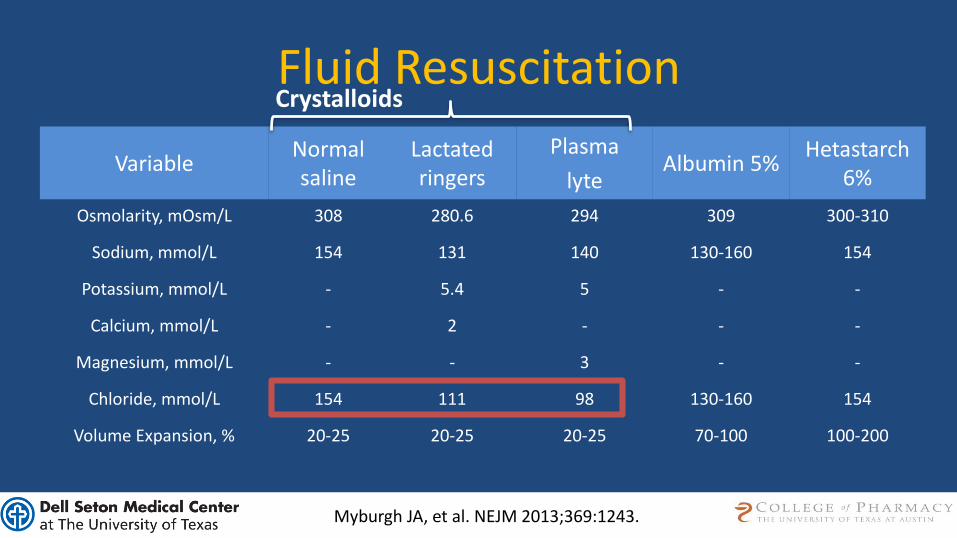
Fluid Resuscitation
VariableNormal saline
Lactated ringers
Plasma
lyteAlbumin 5%
Hetastarch 6%
Osmolarity, mOsm/L 308 280.6 294 309 300-310
Sodium, mmol/L 154 131 140 130-160 154
Potassium, mmol/L - 5.4 5 - -
Calcium, mmol/L - 2 - - -
Magnesium, mmol/L - - 3 - -
Chloride, mmol/L 154 111 98 130-160 154
Volume Expansion, % 20-25 20-25 20-25 70-100 100-200
Myburgh JA, et al. NEJM 2013;369:1243.
Crystalloids
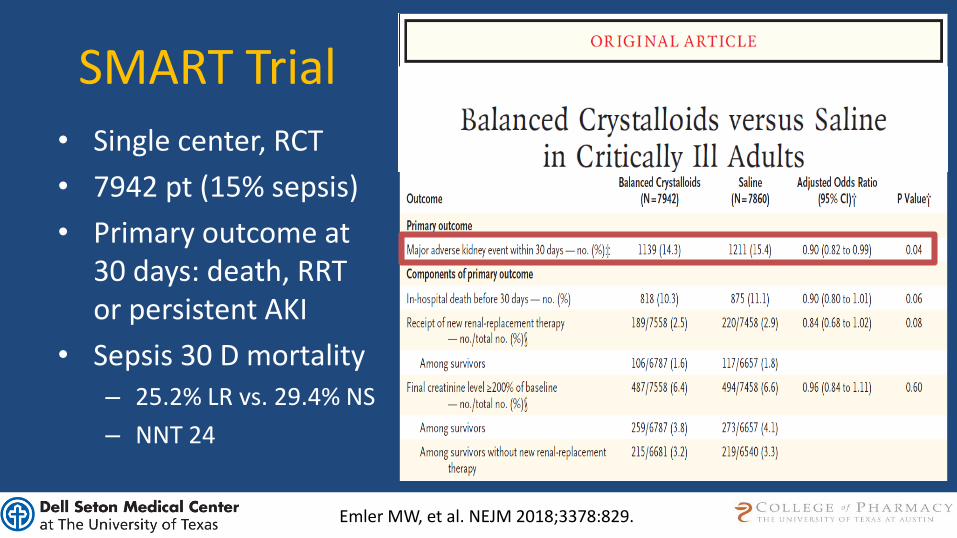
SMART Trial
• Single center, RCT
• 7942 pt (15% sepsis)
• Primary outcome at 30 days: death, RRT or persistent AKI
• Sepsis 30 D mortality– 25.2% LR vs. 29.4% NS
– NNT 24
Emler MW, et al. NEJM 2018;3378:829.

Crystalloid Resuscitation Pearls• Hyperkalemia is likely NOT a contraindication to balanced
salt solutions– Excluded from the SMART trial– Safer than NS in renal transplant studies
• LR should NOT be avoided for fear of lactic acidosis– Sodium lactate ≠ lactate acid – May misinterpret the rise in lactate levels
• Cost comparable • NS may still have a primary role in neurologic injury
Reddy S, Crit Care 2016;20:59.
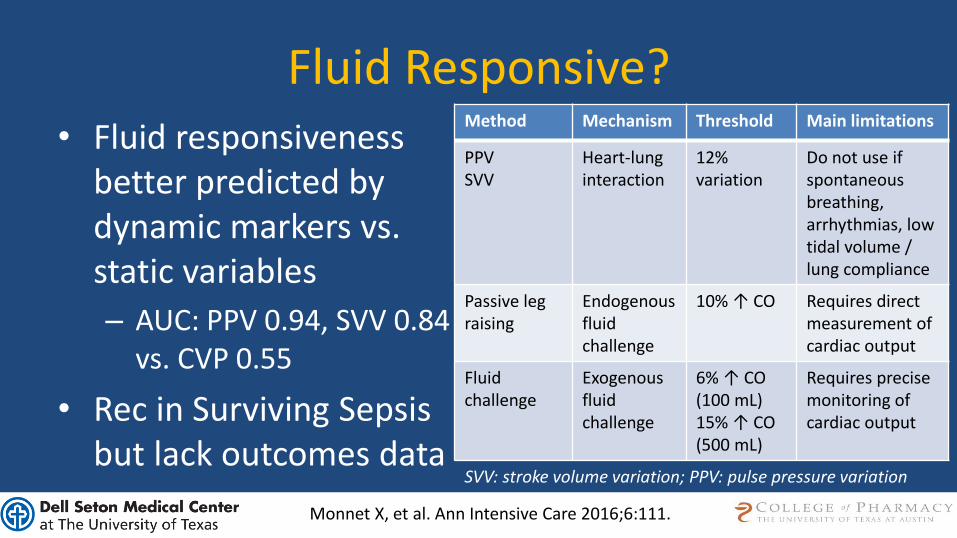
SVV: stroke volume variation; PPV: pulse pressure variation
Fluid Responsive?• Fluid responsiveness
better predicted by dynamic markers vs. static variables
– AUC: PPV 0.94, SVV 0.84 vs. CVP 0.55
• Rec in Surviving Sepsis but lack outcomes data
Method Mechanism Threshold Main limitations
PPVSVV
Heart-lunginteraction
12% variation
Do not use if spontaneous breathing, arrhythmias, low tidal volume / lung compliance
Passive leg raising
Endogenousfluid challenge
10% ↑ CO Requires direct measurement of cardiac output
Fluid challenge
Exogenousfluid challenge
6% ↑ CO(100 mL)15% ↑ CO(500 mL)
Requires precise monitoring of cardiac output
Monnet X, et al. Ann Intensive Care 2016;6:111.

Fluid Resuscitation
VariableNormal saline
Lactated ringers
Plasma
lyteAlbumin 5%
Hetastarch 6%
Osmolarity, mOsm/L 308 280.6 294 309 300-310
Sodium, mmol/L 154 131 140 130-160 154
Potassium, mmol/L - 5.4 5 - -
Calcium, mmol/L - 2 - - -
Magnesium, mmol/L - - 3 - -
Chloride, mmol/L 154 111 98 130-160 154
Volume Expansion, % 20-25 20-25 20-25 70-100 100-200
ColloidsCrystalloids
Myburgh JA, et al. NEJM 2013;369:1243.

Colloids Post SAFE Trial• Albumin / ALBIOS trial
– Severe sepsis or shock randomized to albumin 20% 300 mL daily vs. placebo to keep level >3g/dL for 28 days
– Quicker time to pressor discontinued
– 90 day mortality benefit in septic shock?
• Similar to SAFE…
Caironi P, et al. NEJM 2014;370:1412.

Colloids Post SAFE Trial• Albumin / ALBIOS trial
– Severe sepsis or shock randomized to albumin 20% 300 mL daily vs. placebo to keep level >3g/dL for 28 days
– Quicker time to pressor discontinued
– 90 day mortality benefit in septic shock?
Caironi P, et al. NEJM 2014;370:1412.
Hetastarch Blackbox warning for AKI and mortality in sepsis Recommended against
Surviving sepsis guidelines: Consider addition of albumin if “substantial amount of fluids…”
Weak recommendation, Low quality of evidence
Case: RM
• RM is a 56 y/o, 66 kg, male admitted to ED w/ CAP• BP 83/47 mm Hg, lactate 6.2 mmol/L; UOP 30 mL/hour• In addition to antibiotics, which would be the best
therapy for RM right now?A. NS - targeting a CVP of 8 mm HgB. Albumin 5% - 500 mLC. LR - 30 mL/kgD. LR - if stroke volume variability >12%
Case: RM
• RM is started on 30 ml/kg LR and norepinephrine up to 0.4 mcg/kg/min but his lactate remains > 4 mmol/L
• His MAP remains <60 mm Hg and he is in Afib w/RVR• He is not predicted to be fluid responsive, which is the best
therapy?A. Vasopressin infusion 0.03 units/min, wean lastB. Dopamine 5-20 mcg/kg/min, wean firstC. Phenylephrine 0.5-3 mcg/kg/min, wean lastD. Epinephrine 0.03-0.3 mcg/kg/min, wean first
Vasopressors
Crit Care Clin 2016;32:539-546
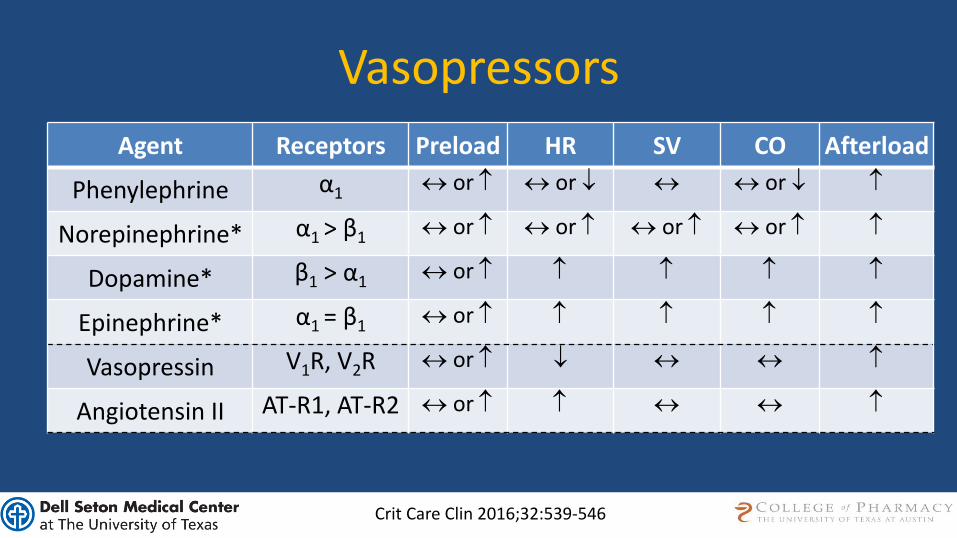
Agent Receptors Preload HR SV CO Afterload
Phenylephrine α1 or or or
Norepinephrine* α1 > β1 or or or or
Dopamine* β1 > α1 or
Epinephrine* α1 = β1 or
Vasopressin V1R, V2R or
Angiotensin II AT-R1, AT-R2 or

Surviving Sepsis: Vasopressors
Rhodes A, et al. Crit Care Med 2017;45:486.
• Norepinephrine (NE) first choice
• Dopamine (DA) alternative to NE in select patients
• Epinephrine (EPI) second line (↑ adverse effects, ↑ lactate)
• Phenylephrine dropped for lack of evidence
• Vasopressin (VP) for relative vasopressin deficiency is a Second line vasopressor or for NE sparing effect (VASST)
• Target a MAP 65 mm Hg (↓ Afib and pressors, = mortality)

DA vs. NE in Septic Shock
De Backer D, et al. Crit Care Med 2012;40:725.
Overall 396/732 330/676 1.12 (1.01-1.20)
Study DA n/N NE n/N28-Day Mortality
RR (95% CI)Martin 10/16 7/16 1.43 (0.73-2.80)
Marik 6/10 5/10 1.20 (0.54-2.67)
Ruokonen 3/5 4/5 0.75 (0.32-1.74)
Mathur 19/25 14/25 1.36 (0.90-2.05)
De Backer 291/542 249/502 1.08 (0.98-1.19)
Patel 67/134 51/118 1.16 (0.89-1.51)
0 1 2 3Test for heterogeneity: I2 = 0%, p = 0.77Test for overall effect: p = 0.035
Favors DA Favors NE
Surviving Sepsis: Vasopressors
Rhodes A, et al. Crit Care Med 2017;45:486.
• Norepinephrine (NE) first choice
• Dopamine (DA) alternative to NE in select patients
• Epinephrine (EPI) second line (↑ adverse effects, ↑ lactate)
• Phenylephrine dropped for lack of evidence
• Vasopressin (VP) for relative vasopressin deficiency is a Second line vasopressor or for NE sparing effect (VASST)
• Target a MAP 65 mm Hg (↓ Afib and pressors, = mortality)

VANISH
• Baseline characteristics well matched– APACHE II 24, 58% intubated, time to receive study drug 3.5 hours
– 76% received NE prior to enrollment at high doses (0.16 mcg/kg/min)
Gordon AC, et al. JAMA 2016;316:509.
Study Population Intervention Endpoints
Gordon
Multicenter Double blind
RCT
Include:Adult patientsSeptic shock
Within 6 hours
Exclude:Previous VP
Ongoing need for steroidESRD
Vasospastic disease
VP + HCT (n=101)
VP + Placebo (n=104)
NE + HCT (n=101)
NE + Placebo (n=103)
VP up to 0.06 units/minNE up to 12 mcg/min
HCT 50 mg q6h, tapered 11 days
10 endpoint: - Kidney failure free days within 28 days
2o endpoint:- Rates and duration of renal replacement therapy- Length of kidney failure- 28 day, ICU and hospital mortality rates- Organ failure free days (SOFA)
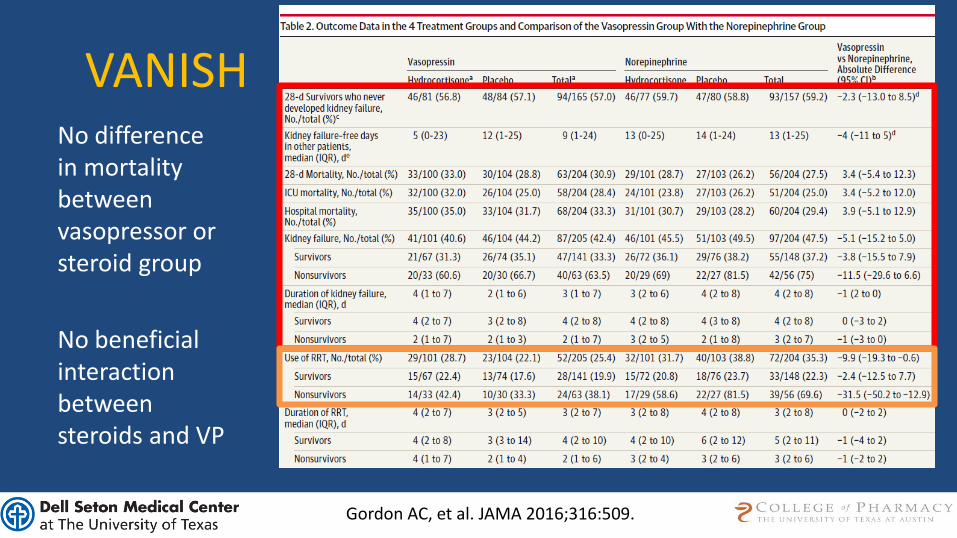
VANISHNo difference in mortality between vasopressor or steroid group
No beneficial interaction between steroids and VP
Gordon AC, et al. JAMA 2016;316:509.

Vasopressin on Mortality
Rhodes A, et al. Crit Care Med 2017;45:486.

Breaking the BANK!• Vasopressin branded VP through a NDA (4/14)• Price went from $8.67/day → $400/day (50 fold ↑)• Strategies:
– Reduce standard concentration (e.g. 20 units/100 mL)– Remove from emergency carts and kits– Restriction criteria (e.g. sepsis requiring a certain rate NE)– Mandatory approval by pharmacist or attending– Education– Altered clinical care (e.g. dose, weaning strategy, alternative pressors)
Curtis N, et al. AJHP 2017:74:105.
Price escalation appears to have little influence on use in septic shock…

Weaning VasopressorsStudy /Design Patient Population Interventions Results
Hammond DA
J Intensive Care Med
2017
epub ahead of print
Retrospective
154 adult patients
with septic shock on
both NE and VP
Categorized into groups based on
which was discontinued first
NE vs. VP
• More clinically significant hypotension after
VP dc’d first (10.9% vs. 67.8%; p<0.01)
• In adjusted analysis, discontinuing VP first
associated with ↑ clinically significant
hypotension (OR 13.83; 95%CI 3.4-56)
• No difference in mortality of LOS
Sacha GL
Pharmacotherapy
2018
Epub ahead of print
Retrospective
585 adults in the recovery phase of septic shock who received VP + NE for at least 6 hours
Categorized into groups based on
which was discontinued first
NE vs. VP
• No difference noted between groups for
clinically significant hypotension (54.8% vs.
49.8%; p=0.28) but quicker hypotension
• Adjusted analysis showed independent risk
for hypotension with VP dc’d first
• No difference in mortality or LOS
Hypotension: restart pressor, increase alternative pressor or fluid

Weaning VasopressorsStudy /Design Patient Population Interventions Results
Hammond DA
J Intensive Care Med
2017
epub ahead of print
Retrospective
154 adult patients
with septic shock on
both NE and VP
Categorized into groups based on
which was discontinued first
NE vs. VP
• More clinically significant hypotension after
VP dc’d first (10.9% vs. 67.8%; p<0.01)
• In adjusted analysis, discontinuing VP first
associated with ↑ clinically significant
hypotension (OR 13.83; 95%CI 3.4-56)
• No difference in mortality of LOS
Sacha GL
Pharmacotherapy
2018
Epub ahead of print
Retrospective
585 adults in the recovery phase of septic shock who received VP + NE for at least 6 hours
Categorized into groups based on
which was discontinued first
NE vs. VP
• No difference noted between groups for
clinically significant hypotension (54.8% vs.
49.8%; p=0.28) but quicker hypotension
• Adjusted analysis showed independent risk
for hypotension with VP dc’d first
• No difference in mortality or LOS
Hypotension: restart pressor, increase alternative pressor or fluid
My practice:Individualize based on patients physiology
DC NE first if arrythmiaDC VP first due to cost
Case: RM
• RM is started on 30 ml/kg LR and norepinephrine up to 0.4 mcg/kg/min but his lactate remains > 4 mmol/L
• His MAP remains <60 mm Hg and he is in Afib w/RVR• He is not predicted to be fluid responsive, which is the best
therapy?A. Vasopressin infusion 0.03 units/min, wean lastB. Dopamine 5-20 mcg/kg/min, wean firstC. Phenylephrine 0.5-3 mcg/kg/min, wean lastD. Epinephrine 0.03-0.3 mcg/kg/min, wean first
Case: RM
• RM is now refractory to fluids, NE 0.5 mcg/kg/min and increasing, and VP at 0.03 units/min but he remains borderline hypotensive with a persistently elevated lactate. Which rescue therapy has the highest quality of evidence to support a reduction in mortality?A. Angiotensin II 20 ng/kg/min, titratedB. Vit C 1.5 g IVPB q6h + Thiamine 200 mcg IVPG q12hC. Hydrocortisone 50 mg IVP q6h + Fludro 50 mcg q24hD. Epinephrine 0.03-0.3 mcg/kg/min
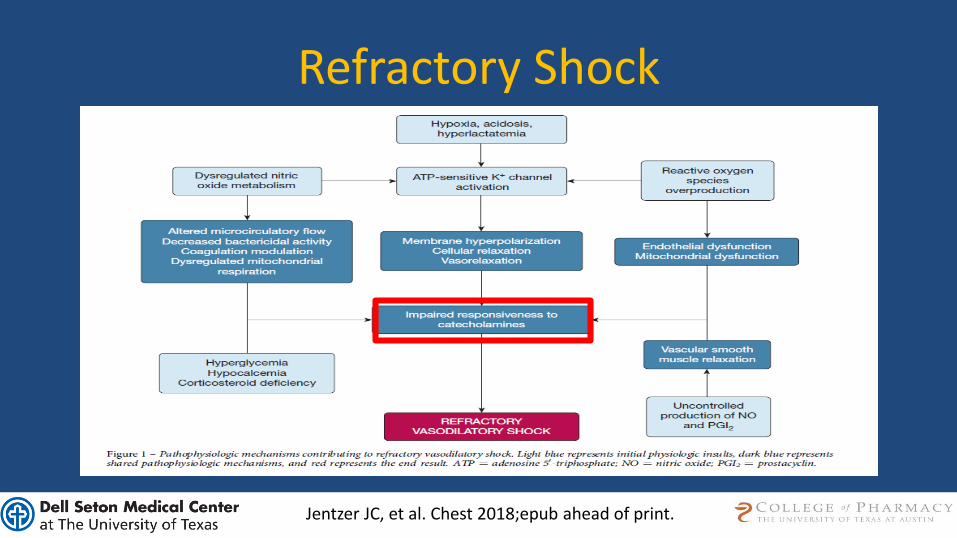
Refractory Shock
Jentzer JC, et al. Chest 2018;epub ahead of print.

Refractory Shock Treatment:New, Old, Re-Purposed

Angiotensin II
Correa TD, et al. Crit Care 2015;19:98.

ATHOS-3 Trial
• Baseline characteristics well matched– 80% sepsis, APACHE II 28, 28% ARDS, 70% received vasopressin
– Average NE dose was 0.34 mcg/kg/min
Khanna A, et al. NEJM 2017;377:419.
Study Population Intervention Endpoints
Venkatesh
MulticenterInternationalDouble-blind
Controlled
Include:Adult patients
Mechanical ventilationVasodilatory, high output shock
Treated with vasopressors for >4 hrsNE >0.25 mcg/kg/min for 6 hours
Exclude:Systemic steroids indicated
Received etomidate during stayDelayed enrollment > 24 hours
Angiotensin II20-200 ng/kg/min for 3
hrs, then max 40 ng/kg/min for 2-7 days
n=163
vs.
Placebon=158
Only study drug titrated for 3 hours
10 endpoint: - MAP response at 3 hours (>75 mm hg or ↑ by 10 mm Hg)
2o endpoint:- Changes in CV and total SOFA score at 48 hour- All-cause mortality at 7 and 28 days- Safety

ATHOS-3 Trial
Annane D B, et al. NEJM 2018;378:809.

ATHOS-3 Trial
Annane D B, et al. NEJM 2018;378:809.

Angiotensin II in Practice
Tumlin JA, et al. Crit Care Med 2018;46:949.
• Angiotensin II FDA approved in Jan 2018 to ↑ BP in sepsis or distributive shock state… – Dose: 20 ng/kg/min, titrate by 15 ng/kg/min every 5 min up to 80
ng/kg/min for 3 hours, then 40 ng/kg/min
– Warning for thrombosis (13% vs. 5% in ATHOS 3)
– Selection of high output states (e.g. ScVO2 >70% w/CVP <8 mm Hg or CI >2.3)
• Cost: 2.5 mg/mL ~$1,800 = ~1 day cost at starting dose
• Subgroup of ATHOS-3 in 105 pts with AKI requiring RRT– Angiotensin II possible 28-day mortality benefit (30% vs. 53%; p<0.01)
– At day 7, 38% off RRT vs. 15%
Outcomes data desperately needed before wide-spread use

ADRENAL Trial
• Baseline characteristics well matched– Age 62, 60% male, APACHEII 23-24, pulm and abd predominant infection
– Time from shock onset to randomization 21 hours
Venkatesh B, et al. NEJM 2018;378:797.
Study Population Intervention Endpoints
Khanna
MulticenterInternationalDouble-blind
Controlled
Include:Adult patients
Vasodilatory shock despite 25 ml/kg fluid + NE >0.2 mcg/kg/min for 6
hours
Exclude:Longer than 48 hours
Burns >20%, ACS, bronchospasm, liver failure, mesenteric ischemia, active bleeding, AAA, nutropenic,
ECMO, systemic steroids
Hydrocortisone200 mg infusion /day
for 7 D or transfer from ICUn=1832
vs.
Placebon=1826
10 endpoint: - Death from any cause at 90 days
2o endpoint:- Death from any cause at 28 days- Time to resolution of shock- Length of stay (ICU and hospital)- Frequency and duration of mechanical ventilation - Frequency and duration of renal replacement therapy- Secondary infection (bacteremia, fungemia)- Blood transfusion

ADRENAL Trial
Annane D B, et al. NEJM 2018;378:809.

APROCCHSS Trial
• Baseline characteristics well matched– Age 66, 66% male, SOFA score 11, pulm and abd predominant infection
– Mean dose of norepinephrine 1 mcg/kg/min
Venkatesh B, et al. NEJM 2018;378:797.
Study Population Intervention Endpoints
Annane
MulticenterInternationalDouble-blind
Controlled
* Initially included activatedprotein C
Include:Adult patients
Probable septic shockSOFA Score 3/4 for 2 organs for 6 hrs
Vasopressors for 6 hours
Exclude:Septic shock for > 24 hours
Pregnancy or lactationPrevious treatment with steroids
Hydrocortisone 50 mg IV q6h +
fludrocortisone 50 mcg daily for 7 days
n=627
vs.
Placebon=614
10 endpoint: - Death from any cause at 90 days
2o endpoint:- Death from any cause at ICU discharge, hospital
discharge and days 28 and 180- Time to weaning form pressors- Duration of mechanical ventilation - % of patients with organ failure free (SOFA < 6 28/90 D)- Length of stay (ICU and hospital)- Safety (superinfection, GI bleed, hyperglycemia,
neurologic sequelae)
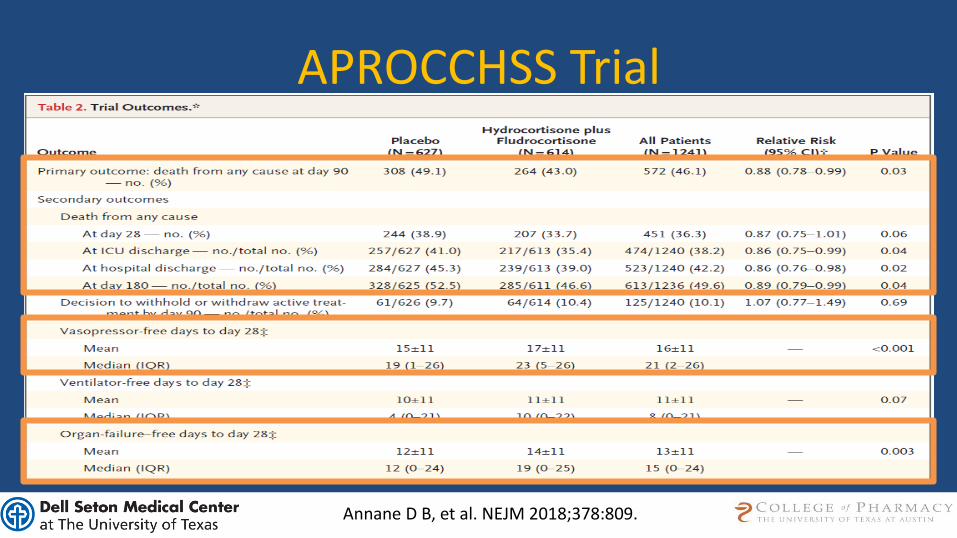
APROCCHSS Trial
Annane D B, et al. NEJM 2018;378:809.

Steroids in 2018Benefit
• Consistent result in quicker resolution of shock
• Decreased duration of mechanical ventilation
• Less mortality and organ failure in the sickest
Risks
• Hyperglycemia
Suffredini AF. NEJM 378;9:860.
Steroids in 2018Benefit
• Consistent result in quicker resolution of shock
• Decreased duration of mechanical ventilation
• Less mortality and organ failure in the sickest
Risks
• Hyperglycemia
J Burn Care Research 2008;29:257-266
Practical considerations:
Infusion vs. intermittent?HCT alone or HCT + Fludrocortisone?Duration if persistent shock remains?

Metabolic Resuscitation• Vitamins become depleted during sepsis
– Vitamin C ↓ correlates with ↑ multi-organ failure and death– Thiamine deficiency is associated with ↑ mortality
• Deficiencies relevant and cause clinical disease– Thiamine deficiency noted in 35% of shock patients with ↑ lactate
• Essential co-enzyme in Krebs cycle (production of ATP)• Wernicke’s encephalopathy and Beriberi
– Vitamin C • Maintains endothelial boundaries, required to synthesize
catecholamines, antioxidant prevents neutrophil induced lipid oxidation• Deficiency causes scurvy
Marik PE. Pharmacol Ther 2018;epub ahead of print.

Total Body Water (TBW) - 2018
NEJM 2013;369:1243-1251
GlycoproteinsProteoglycans

IV Vitamin C Sepsis Randomized Data Study /Design Patient Population Interventions Results
Fowler et al.
J Transl Med
2014;12:32
RCT
24 patients with
severe sepsis
randomized 1:1:1
Low dose Vit C 50 mg/kg/day
High dose Vit C:200 mg/kg/day
Placebo
Zabet et al.
J Res Pharm Pract
2016;5:94
RCT
28 surgical patients on pressors to maintain MAP > 65 mm Hg
Vit C 25 mg/kg every 6 hours for 3
days
Vs.
Placebo
• Total dose of norepinephrine for 72 hour:
Vit C 156 mcg vs. 302 mcg; p<0.01
• Duration of norepinephrine: Vit C 50 hr
vs. 72 hr; p<0.01
• 28 day mortality: Vit C 14% vs. 64%;
p<0.01

“The Marik Cocktail”
• Baseline characteristics well matched– Age 58-62, 49-57% male, 47-55% intubated, 46% required pressors
– SOFA score 8 with predicted mortality of about 40%
Marik PE, et al. Chest 2017;151:1229.
Study Population Intervention Endpoints
Marik
Retrospective Before-After
Study
Jan to July 2016
Include:Severe sepsis and septic
shockProcalcitonin > 2 ng/mL
Exclude:<18
Limitations on care
Vit C 1.5 g q6hHydrocortisone 50 mg q6h
Thiamine 200 mg q12hFor 4 days or transfer
n=47
vs.
Placebon=47
10 endpoint: - In hospital survival
2o endpoint:- Duration of vasopressor therapy- Requirement for renal replacement therapy- ICU length of stay- Change in serum procalcitonin over 72 hours- Change in SOFA score over 72 hours

“The Marik Cocktail”
Marik PE, et al. Chest 2017;151:1229.
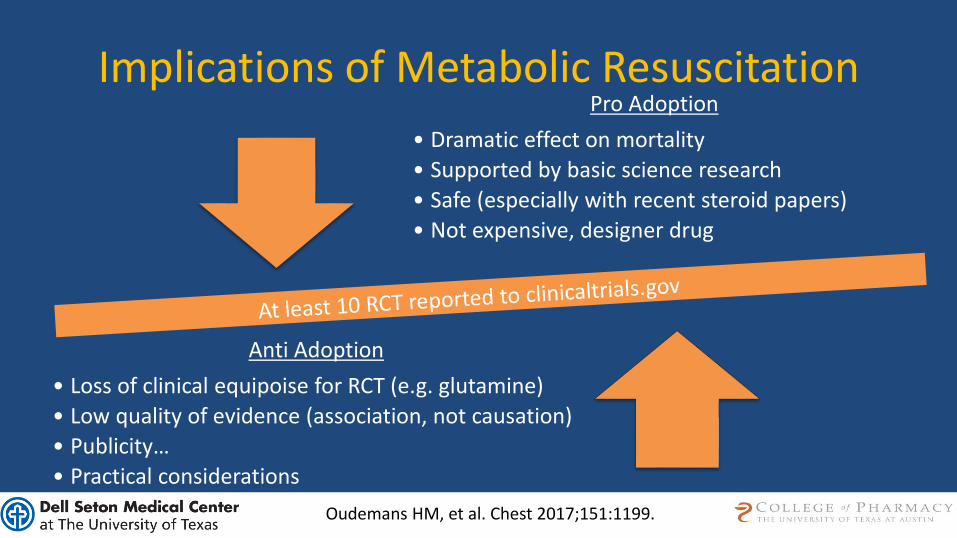
Implications of Metabolic ResuscitationPro Adoption
• Dramatic effect on mortality
• Supported by basic science research
• Safe (especially with recent steroid papers)
• Not expensive, designer drug
Anti Adoption
• Loss of clinical equipoise for RCT (e.g. glutamine)
• Low quality of evidence (association, not causation)
• Publicity…
• Practical considerations
Oudemans HM, et al. Chest 2017;151:1199.

Practical Considerations• Vitamin C 500 mg / mL x 50 mL ~$100 / vial
– Make 4 doses (1.5g/100 mL NS; 24 hr stability)
– Waste relative to number of active patients• One patient: course about $400 and waste 75%
• Four patients: course about $100 and waste little
– Monitor: osmotic diuresis, AKI, no POC glucose for 24 hrs (↑)
• Thiamine (~$50) and HCT (~120)
https://emcrit.org/isepsis/isepsis-vitamin-c-hydrocortisone-thiamine-metabolic-resuscitation-protocol/

Case: RM
• RM is now refractory to fluids, NE 0.5 mcg/kg/min and increasing, and VP at 0.03 units/min but he remains borderline hypotensive with a persistently elevated lactate. Which rescue therapy has the highest quality of evidence to support a reduction in mortality?A. Angiotensin II 20 ng/kg/min, titratedB. Vit C 1.5 g IVPB q6h + Thiamine 200 mcg IVPG q12hC. Hydrocortisone 50 mg IVP q6h + Fludroc 50 mcg q24hD. Epinephrine 0.03-0.3 mcg/kg/min

Don’t Forget - Early Antibiotics
Seymour CW, et al. NEJM 2017;376:2235.
• NY adoption of bundled care in 49,311 patients
• Longer time to administration of antibiotics associated with in-hospital mortality
– OR 1.04; 95% CI 1.03-1.06

Pushing the Envelope
Alam N, et al. Lancet Respir Med 2018;6:40
• Multicenter RCT (Netherlands)
• Patients with sepsis received ceftriaxone pre-hospital
• Time to antibiotics -26 min vs. 70 min
• Average qSOFA ≥ 2 ~20% of patients
Conclusions
• New definitions controversial, SIRS still used• Time requirement to bundle implementation is
decreasing• Fluid resuscitation
– Shift towards balanced crystalloids– Ongoing administration beyond 30 ml/kg should be
guided by dynamic markers of fluid responsiveness– Albumin considered for “large volumes” of fluid

Conclusions
• Vasopressors– Norepinephrine reigns supreme– No clear benefit to vasopressin and cost barrier– Wean based on physiologic condition
• Refractory septic shock– Angiotensin has an emerging but unproven role– Steroids reverse shock, appear safe and still may ↓ mortality– Vitamin C and thiamine promising but warrant validation
• Early antibiotics remain at the core for treatment of sepsis

Updates in the Treatment of Sepsis
Mitchell J Daley, PharmD, FCCM, BCPSClinical Pharmacy Specialist, Critical Care
Dell Seton Medical Center at the University of Texas and Seton Healthcare Family
Clinical Adjunct Faculty
University of Texas College of Pharmacy






![ResearchGlobal utilization of low-dose corticosteroids in ... · in patients with septic shock and relative adrenal insuffi-ciency refractory to vasopressor treatment [8], the use](https://img.dokumen.tips/doc/110x75/5ea9a11f7ca28a26e4170908/researchglobal-utilization-of-low-dose-corticosteroids-in-in-patients-with-septic.jpg)






















