Embed Size (px)
Citation preview

UpdateGuidelinesinSTEMIManagement:
FocusonLogisticandSystemApproachtoReperfusionTherapy
WacinBuddhari,MDCardiologyConsultant,BNHHospital
Director,CardiacCatheterizationLaboratoryKingChulalongkornMemorialHospital
Bangkok,Thailand
March 14th, 2018The First Asia Forum in Emergency Medicine
BNH Hospital, Bangkok, Thailand

Disclosure• AdvisoryBoardMember:
– AstraZeneca(dapagliflozin)– BoehringerIngelheim(empagliflozin)– MedtronicAsiaPacific(CoronaryandTranscatheterHeartValve)– MSD(DYSISII)
• LectureHonorarium– AstraZeneca– AbbotVascular– BoehringerIngelheim– DaiichiSankyo– Medtronic– MSD– Novartis– RocheDiagnostics– Sanofi– Sandoz– Takeda

PracticeGuidelines

Plaque rupture
Stableangina
Unstableangina
Non-Qwave MI
Q-waveMI
ST elevation ACS (MI)Non-ST elevation ACS
ECG
+
Degree of thrombosis
Management of ST Elevation MI
Reperfusion
Prevent re-occlusion
STOPInfarction
STOPMyocardial loss
FibrinolysisPrimary PCI
Antiplatelets, Anticoagulant, PCI

Ischemic myocardiumpotentially salvageableby intervention
Necroticmyocardium
100
80
60
40
20
21 43 5 126 2418 123 6 9 6
Hours Days WksIrreversibleinjury
Reversibleinjury
Ischemic myocardium potentially salvageable by reperfusion
“Time is muscle”Acute Myocardial Infarction

Mode of Reperfusion
1’ PCI
Fibrinolysis
REPERFUSION
Occluded LAD Open!!!

2 Reperfusion strategies
• Widely available• Can be given by GP, ER
doctors, gen med or gen cardiologist
• Rate of successful reperfusion varies from 40 – 85%
• Difficult to assess successful reperfusion
• Risk of re-occlusion is 10-20%
• Can be done only in some tertiary centers
• Need experienced interventional cardiologist
• Difficult to get done in a timely fashion (refer cases, after-hour)
• Can open the artery in 90-95% of cases
• Risk of re-occlusion is very low
Fibrinolysis Primary PCI

What’sNewin2017Guidelines?

What’sNewin2017Guidelines?
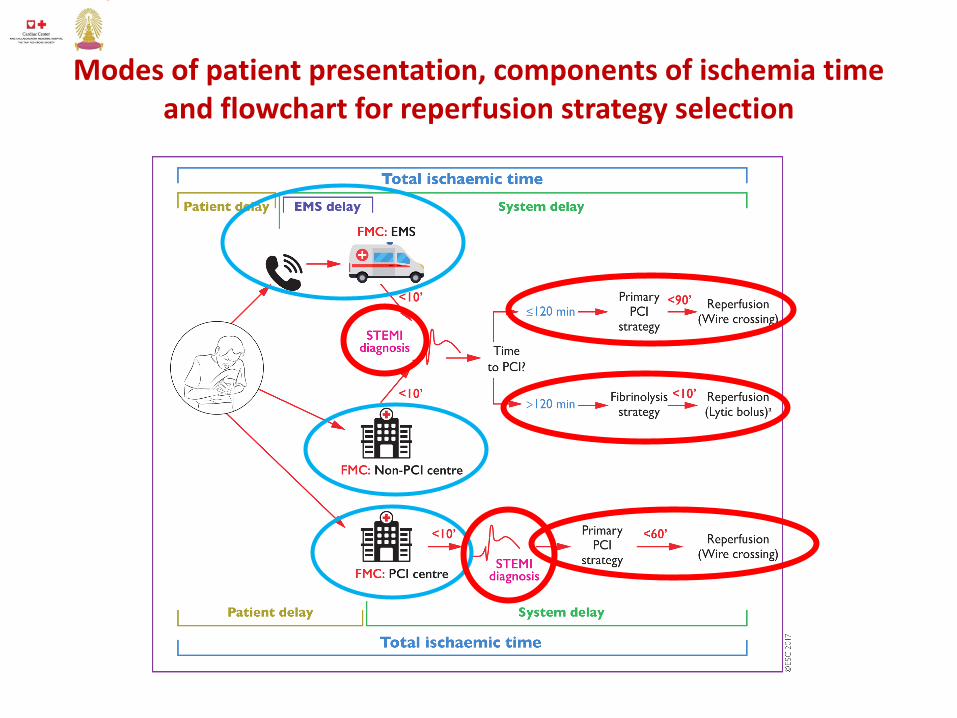
Modesofpatientpresentation,componentsofischemiatimeandflowchartforreperfusionstrategyselection

Delays
• TreatmentdelaysarethemosteasilyauditedindexofqualityofcareinSTEMI
• Shouldberecorded ineverysystemprovidingcaretoSTEMIpatientsandbereviewedregularly
• Ifprojectedtargettimesarenotmet,theninterventions areneededtoimproveperformance ofthesystem
• Allcomponents ofthesystemdelayrepresentthequalityofcare anditisrecommendedtomeasurethemasqualityindicators

Delays
• Inhospitals andEMS participatinginthecareofSTEMIpatients,thegoalistoreducethedelaybetweenFMCandSTEMIdiagnosis to< 10min
• STEMIdiagnosis referstothetimewhentheECGisinterpretedasST-segmentelevation orequivalentanditisthetimezero toguideappropriatetherapy
• Systemdelayismorereadilymodifiable byorganizationalmeasuresthanispatientdelay,anditisapredictorofoutcomes

Delays
• Forpatientspresentinginanon-PCIcenter,door-intodoor-outtime,definedasthedurationbetweenarrivalofthepatientatthehospitaltodischargeofthepatientinanambulanceen routetothePCIcenter,isanewclinicalperformancemeasure,and< 30minisrecommendedtoexpeditereperfusioncare

OrganizationofSTEMITreatmentinNetworks
• Cleardefinitionofgeographicareasofresponsibility
• Sharedwrittenprotocols,basedonriskstratificationandtransportationbyatrainedphysician,nurse,orparamedicstaffinappropriatelyequippedambulancesorhelicopters
• Pre-hospitaltriageofSTEMIpatientstotheappropriateinstitution,bypassingnon-PCIhospitalsorhospitalswithouta24haday,7daysaweek(24/7)primaryPCIprogram

OrganizationofSTEMITreatmentinNetworks
• Onarrivalattheappropriatehospital,thepatientshouldimmediatelybetakentothecatheterizationlaboratory,bypassingtheemergencydepartment
• Patientspresentingtoanon-PCI-capablehospitalandawaitingtransportationforprimaryorrescuePCImustbeattendedinanappropriatelymonitoredandstaffedarea
• IfthediagnosisofSTEMIhasnotbeenmadebytheambulancecrewandtheambulancearrivesatanon-PCI-capablehospital,theambulanceshouldawaitthediagnosisand,ifaSTEMIdiagnosisismade,shouldcontinuetoaPCI-capablehospital

Logisticsofpre-hospitalcare(1)

Logisticsofpre-hospitalcare(2)

Logisticsofpre-hospitalcare(3)

Recommendationsforreperfusiontherapy(1)
12 3

Recommendationsforreperfusiontherapy(2)

Recommendationsforreperfusiontherapy(3)

Fibrinolytictherapy

MaximumtargettimesaccordingtoreperfusionstrategyselectioninpatientspresentingviaEMSorinanon-PCIcenter
All STEMI should undergo CAG +/- PCI

ImportantTimeTargetsinAcuteSTEMI

QualityIndicators(1)

QualityIndicators(2)

Summary• CurrentguidelinesadvocatesbestpossibleSTEMIcareshould
bedonesystemically,involvingEMS,non-PCIcentersandPCI-capablecenters,workingaswell-planned“network”
• Timingforeachreperfusionstrategyhasbeenredefined
• PrimaryPCIcentershouldoperate24/7• TheultimategoalofthenetworkistoperformedprimaryPCI
inatimelymanortoasmanypatientsaspossible• IfprimaryPCIcannotbedoneinatimelymanor,then
fibrinolytictherapyhastobedeliveredASAP(10minafterDx)withoutanyhesitation
• Timedelayineverystephavetoberecordedandauditedasqualityindicators





























