Embed Size (px)
Citation preview
RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5
www.downstatesurgery.org

PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II
Liver disease followed at OSH x2 years (when moved from China), on tenofivir, lasix
Known umbilical hernia, acute onset of pain at hernia site x1d
Constipation, obstipation, nausea & vomiting x1d
www.downstatesurgery.org

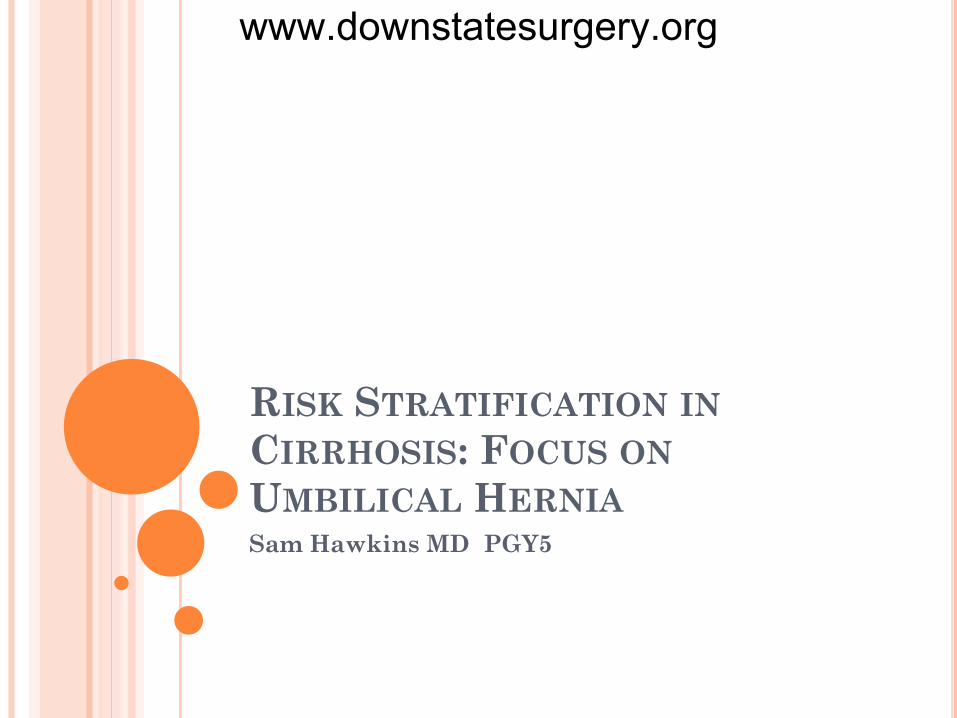
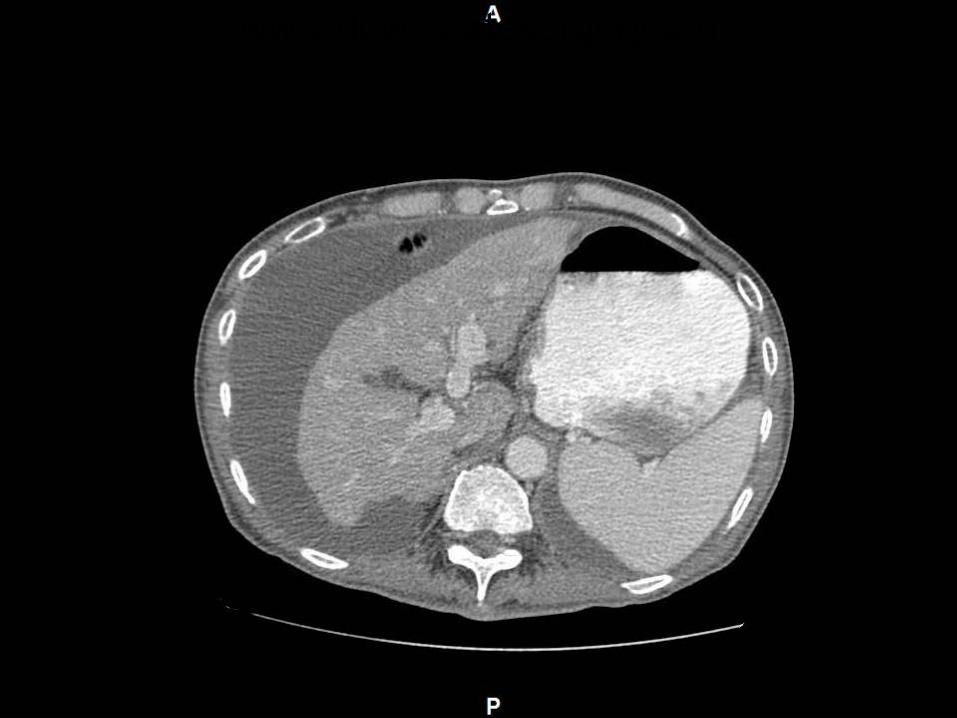
PATIENT PRESENTATION 98.5 95 143/78 16 100%RA NAD, AAOx3 Abdomen distended with fluid wave Umbilical hernia with erythematous appearing
skin and 2x3 scab at apex. Hernia fluid filled with palpable indurated mass within. Non-reducible. Non-tender.
Bilateral inguinal hernias, fluid filled
www.downstatesurgery.org

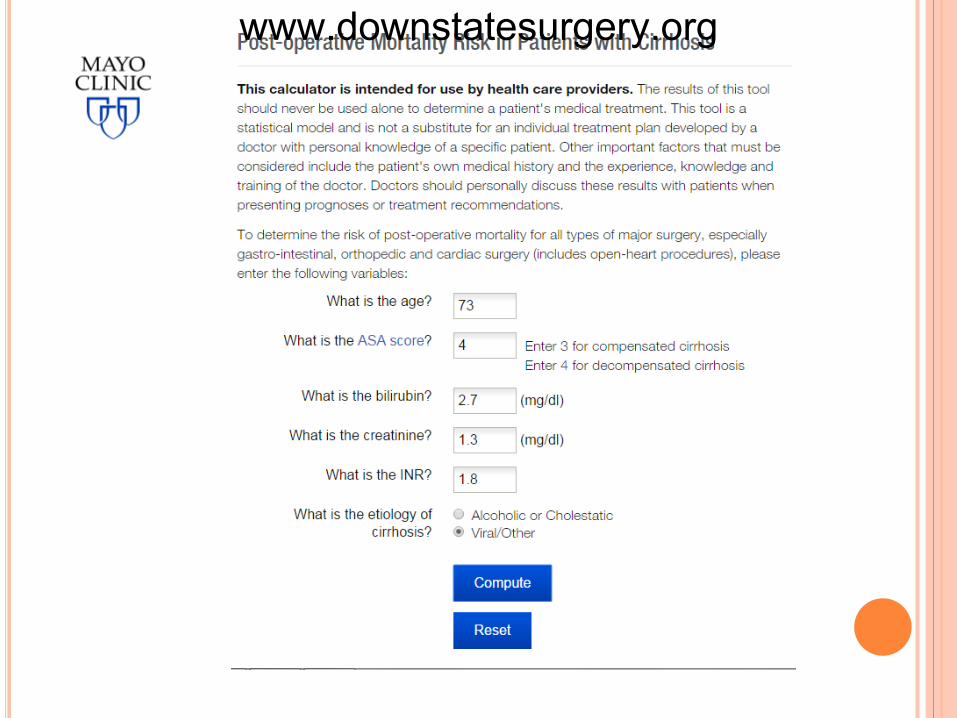
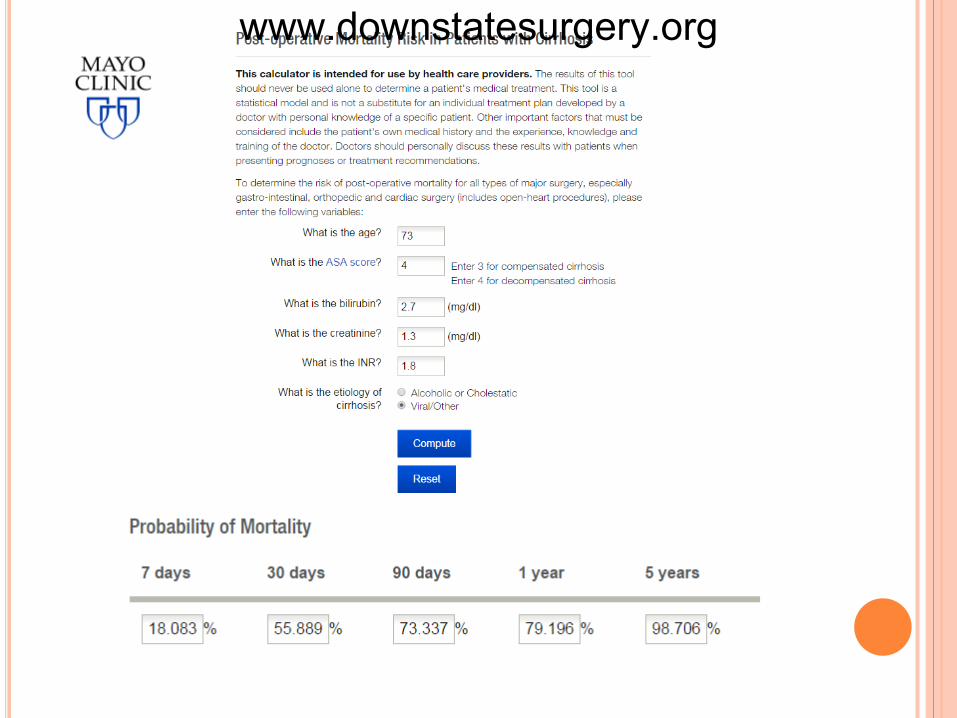
PATIENT PRESENTATION CBC: 5.1/12.2/37.1/53 BMP: 136/4.4/103/27/34/1.3/224 8.6/2.2/4.0 LFTs: 8.6/2.5/51/50/88/2.7 Coags: 16.3/27.8/1.8
www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org
www.downstatesurgery.org

www.downstatesurgery.org
www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org
PATIENT PRESENTATION Discussion with patient and son at bedside
including significant risks of surgery… DNR/DNI status Refusal of surgery
Admitted NGT/NPO Serial abdominal exams
www.downstatesurgery.org
PATIENT PRESENTATION HD 1-3 pt did not improve and hernia became
increasingly discolored, tense, and painful Patient expressed desire for surgery at night, added on
for following day 97.8 83 18 134/78 99% Creatinine 1.3 1.0 Bilirubin 2.7 4.1 INR 1.8 2.3 Pt became encephalopathic Ammonia 160 Son elected to consent to surgery the following
morning, taken to surgery emergently
www.downstatesurgery.org

OPERATIVE COURSE Opened hernia sac immediate release of large
ascites and obvious necrotic small bowel Hernia defect 1cm, opened to deliver dilated and
collapsed small bowel, viable in both directions from defect (opened to approx 6 cm)
Removed ascites (total 8L by end of case) Resected 25cm small bowel side-to-side stapled
anastomosis Closed defect w/ running #1 prolene Skin left open and packed Operative time: 2h Given 4u FFP, 1000 crystaloid EBL 100, UOP 300 Taken to SICU intubated
www.downstatesurgery.org

POSTOPERATIVE COURSE - OVERVIEW POD 0-2: critical POD 3-11: progression to multi-organ failure POD 12: family elected against escalation of care
and made DNR status, to maintain abx and ETT, institute comfort care
POD 15: expired in PM
www.downstatesurgery.org
POSTOPERATIVE COURSE - SYSTEMS N: non-responsive off sedation lactulose
POD 4 responsive with agitation POD 10 increasingly obtunded off sedation until expiration
C: initially NT/NTC POD 4 hypertensive with new onset afib w/ RVR amiodarone gtt + metoprolol POD 10 switched to metoprolol, rate maintained in afib
P/ID: initially kept intubated POD 3 failed SBT CXR after fever demonstrates bilateral infiltrates resp cx w/ MSSA and enterobacter abx initiated and maintained until expiration multiple self-extubations with successful re-intubations
www.downstatesurgery.org

POSTOPERATIVE COURSE - SYSTEMS Heme
Initially on HSQ for DVT ppx Vitamin K POD 8 pt had coffee-ground NGT aspirate and
dropped Hct 30 22. INR 3.1, platelets 38 (ranged throughout admission 20-50)
Transfused PRBC, platelets, FFP, HSQ d/c’d Intermittent coffee-ground emesis, no additional drop
in Hct or PRBC transfusions
www.downstatesurgery.org
POSTOPERATIVE COURSE - SYSTEMS Renal/Fluids
8L ascites drained intraop 1u albumin in PACU Normotensive over POD 0-3, became hypertensive
controlled with metoprolol until expiration BUN/Crt 40/1.2 BUN increased over 10 days to
120s, Crt stable 1.2-1.5 until POD 7, increased to 2, 3, 5
Na peaked at 154 on POD 4, NS initially to ½ NS @ maintenance rate
Lasix IV and spironolactone NG for ascites, albumin given daily with lasix, no return of ascitic distension
www.downstatesurgery.org

POSTOPERATIVE COURSE - SYSTEMS GI
Trickle feeds from POD1 advanced to goal feeds with hepatic formula
Bilirubin post-op stable at 4-5 until POD 8 increased to 10 then 20
www.downstatesurgery.org
www.downstatesurgery.org
OVERVIEW Pathophysiology of Cirrhosis Pre-operative and Post-operative considerations Risk stratification
Patient specific factors Contraindications to surgery
Scoring systems CTP, MELD, is there a right score to use?
Surgery specific factors Umbilical hernia as special case?
www.downstatesurgery.org
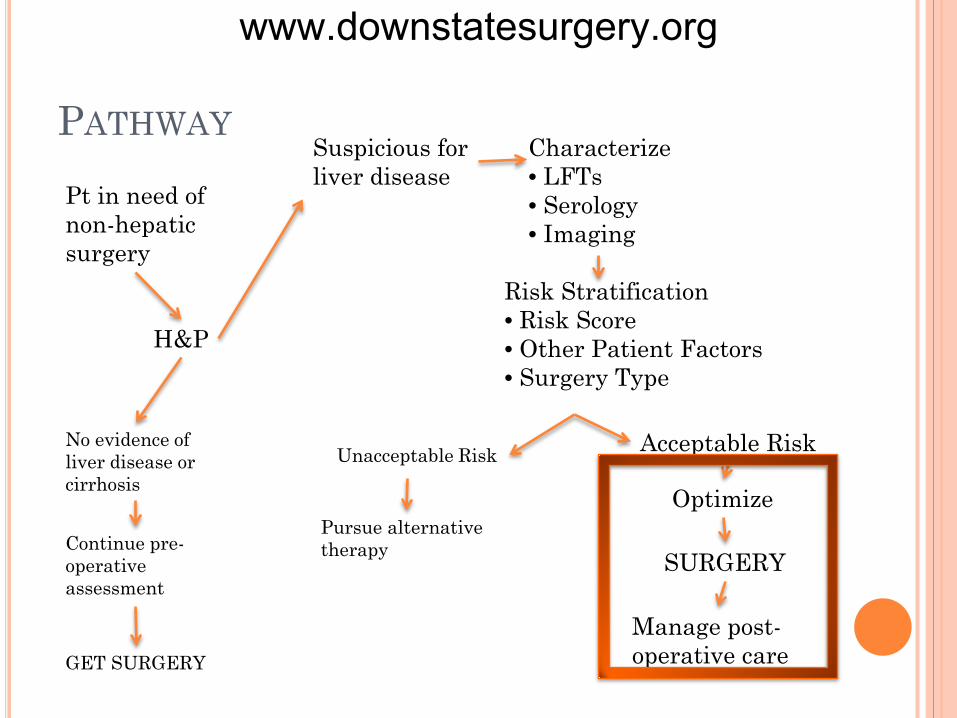
PATHWAY Pt in need of non-hepatic surgery
H&P
No evidence of liver disease or cirrhosis
Continue pre-operative assessment
GET SURGERY
Suspicious for liver disease
Characterize • LFTs • Serology • Imaging
Risk Stratification • Risk Score • Other Patient Factors • Surgery Type
Acceptable Risk
Optimize
SURGERY
Unacceptable Risk
Pursue alternative therapy
Manage post-operative care
www.downstatesurgery.org
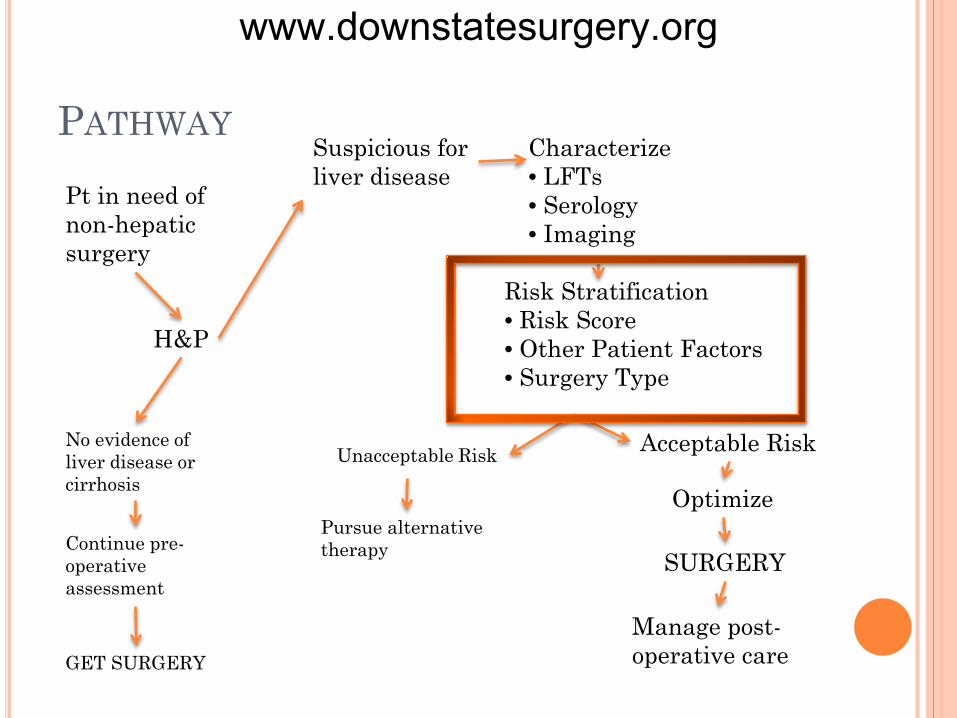
PATHWAY Pt in need of non-hepatic surgery
H&P
No evidence of liver disease or cirrhosis
Continue pre-operative assessment
GET SURGERY
Suspicious for liver disease
Characterize • LFTs • Serology • Imaging
Risk Stratification • Risk Score • Other Patient Factors • Surgery Type
Acceptable Risk
Optimize
SURGERY
Unacceptable Risk
Pursue alternative therapy
Manage post-operative care
www.downstatesurgery.org

PATHOPHYSIOLOGY OF CIRRHOSIS Portal Hypertension
Hemodynamics – circulating volume and pressure Cardiac function – hyperdynamism Renal function Ascites
Liver Function Synthetic
Coagulation Metabolic
Toxins, pharmacology Nutrition Infectious disease
www.downstatesurgery.org
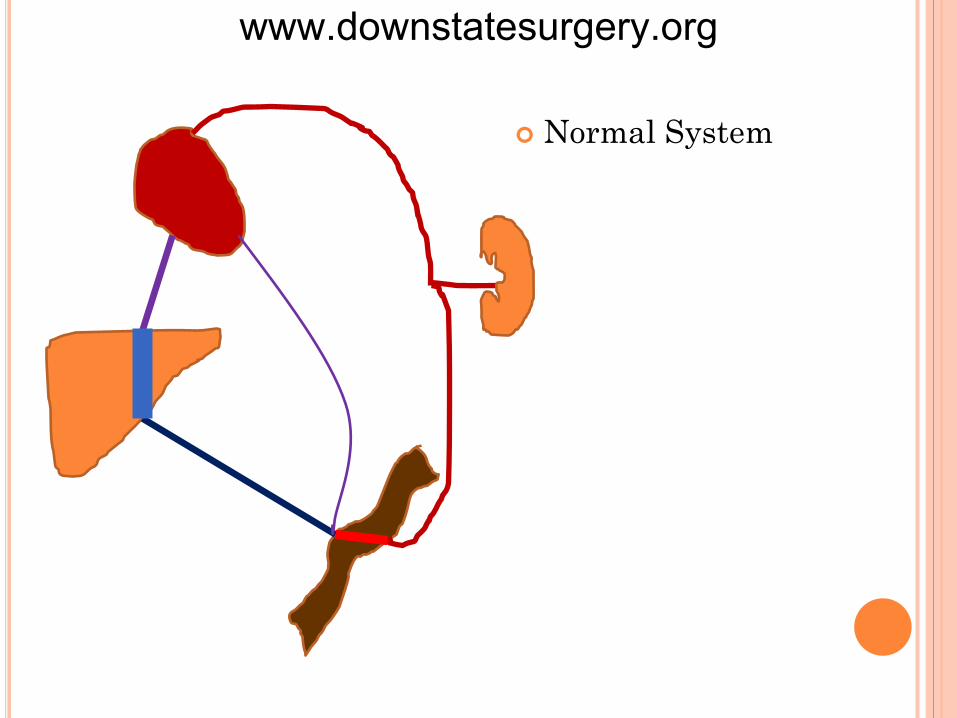
Normal System
www.downstatesurgery.org
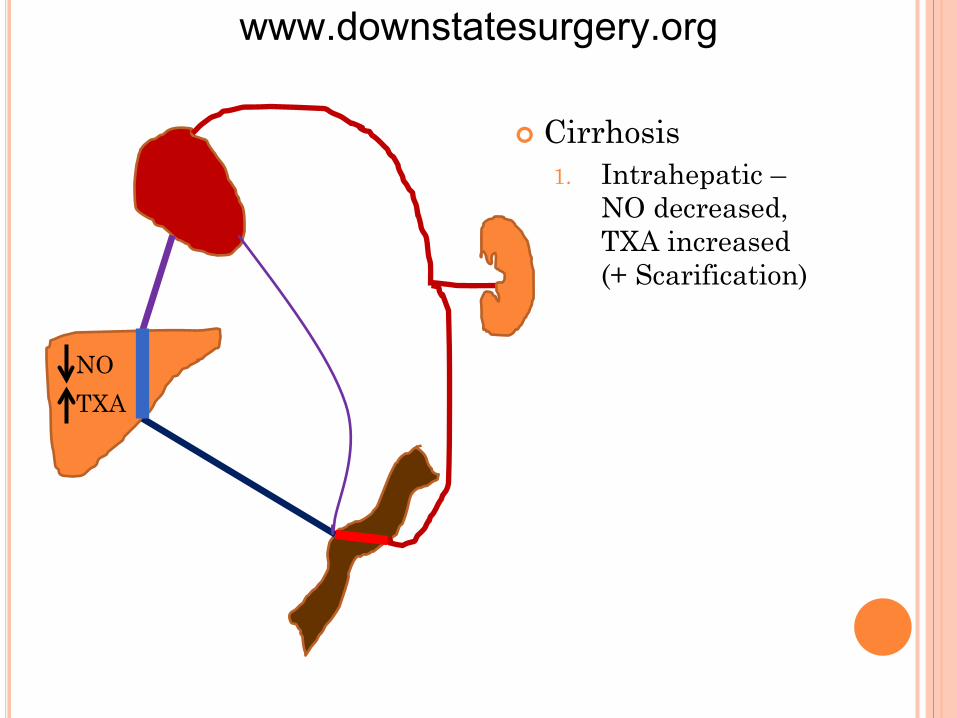
Cirrhosis 1. Intrahepatic –
NO decreased, TXA increased (+ Scarification)
NO TXA
www.downstatesurgery.org

Cirrhosis 1. Intrahepatic –
NO decreased, TXA increased (+ Scarification)
2. Collateral flow 3. Splanchnic
circulation becomes vasodilatory to compensate (with decrease in systemic)
NO TXA
NO TXA
www.downstatesurgery.org
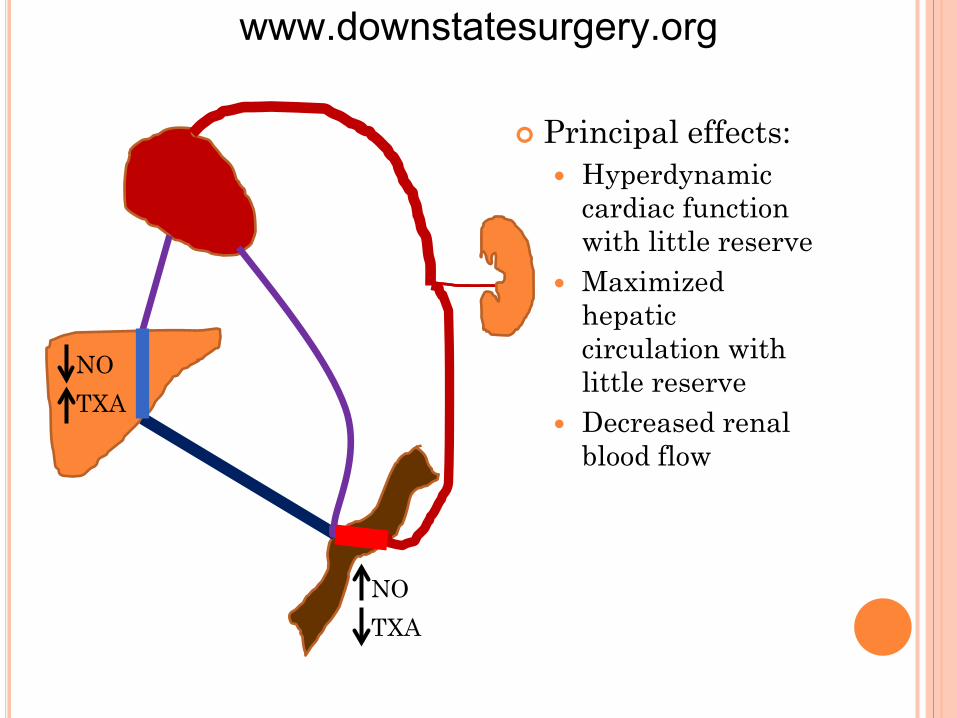
Principal effects: Hyperdynamic
cardiac function with little reserve
Maximized hepatic circulation with little reserve
Decreased renal blood flow
NO TXA
NO TXA
www.downstatesurgery.org
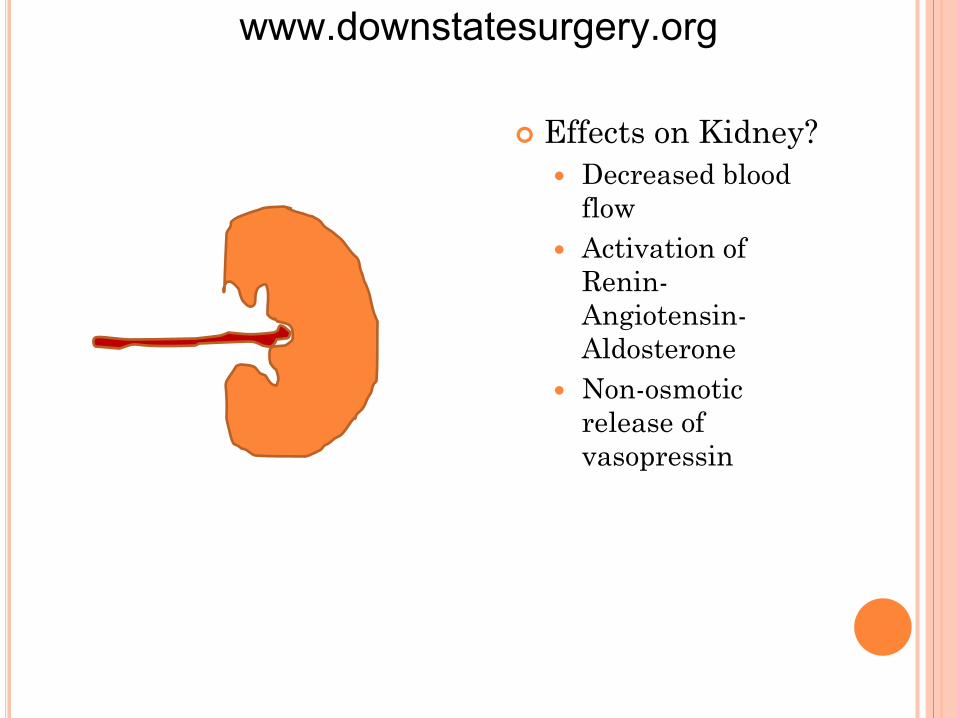
Effects on Kidney? Decreased blood
flow Activation of
Renin-Angiotensin-Aldosterone
Non-osmotic release of vasopressin
www.downstatesurgery.org

Effects on Kidney? Decreased blood flow Activation of Renin-
Angiotensin-Aldosterone Non-osmotic release of
vasopressin
renal hypoperfusion
sodium retention (fluid overload)
free-water retention in excess of sodium retention (hyponatremia)
www.downstatesurgery.org

NO TXA
NO TXA
Compensation vs Decompensation
www.downstatesurgery.org

PATHOPHYSIOLOGY OF CIRRHOSIS Ascites
10% in cirrhosis 60% 3 year survival after onset Hemodynamic consequences
Increased splanchnic flow + increased portal pressure
Capillary permeability increases Hypoalbuminemia
www.downstatesurgery.org
OPTIMIZATION BY SYSTEMS Cardiac – Hyper-dynamism
Pre-operative Cardiac assessment Awareness of lack of reserve
Post-operative Avoid inotropic agents
www.downstatesurgery.org
OPTIMIZATION BY SYSTEMS Renal
Pre-operative Renal function studies Assessment for hepatorenal syndrome Judicious use of diuretics for ascites and lactulose for
encephalopathy (volume) Albumin vs crystaloid
Post-operative Monitoring for HRS Albumin vs crystaloid
www.downstatesurgery.org

OPTIMIZATION BY SYSTEMS Hepatorenal Syndrome
Overwhelming activation of renin-angiotensin-aldosterone system
Difficult to reverse High mortality
www.downstatesurgery.org

OPTIMIZATION BY SYSTEMS Hepatorenal Syndrome
Treatment Terlipressin – splanchnic vasoconstriction Albumin+octreotide+midodrine RRT - failure
www.downstatesurgery.org
OPTIMIZATION BY SYSTEMS Ascites
Pre-operative Diuretic therapy- spironolactone and furosemide Large Volume Paracentesis (LVP) Albumin administration with LVP Screening for SBP
Post-operative Same
Paracentesis Induced Circulatory Dysfunction
Fluid shift vs vasodilation Hypovolemia and R-A-A activation Volume expansion >5L w/ albumin
www.downstatesurgery.org
OPTIMIZATION BY SYSTEMS Neurologic
Pre-operative Consider diagnosis of hepatic encephalopathy Lactulose, rifaximin, serial ammonia measurements
unhelpful Avoidance of sedation
Post-operative Same
www.downstatesurgery.org

OPTIMIZATION BY SYSTEMS Coagulation Synthetic (factors) + consumptive (platelets)
Pre-operative Vitamin K FFP and platelets No benefit of rfVII
Post-operative Same
www.downstatesurgery.org
OPTIMIZATION BY SYSTEMS Nutrition
Pre-operative, Post-operative Maximize nutrition, no good evidence for hepatic formulas
(including low-nitrogen)
Infectious Disease SBP Sepsis
No difference in GDT in cirrhotic - harder Inotropes less effective Lactate metabolism
www.downstatesurgery.org

OPTIMIZATION Cardiac – Avoidance of inotropes Neuro – Encephalopathy - lactulose Renal –
Hyponatremia – fluid restriction HRS – albumin, terlipressin, octreotide+midodrine
Ascites Diuretics, LVP w/ albumin
Coagulopathy Vitamin K, platelets and FFP
Awareness of the precariousness of cirrhotic physiology, readiness to act
www.downstatesurgery.org
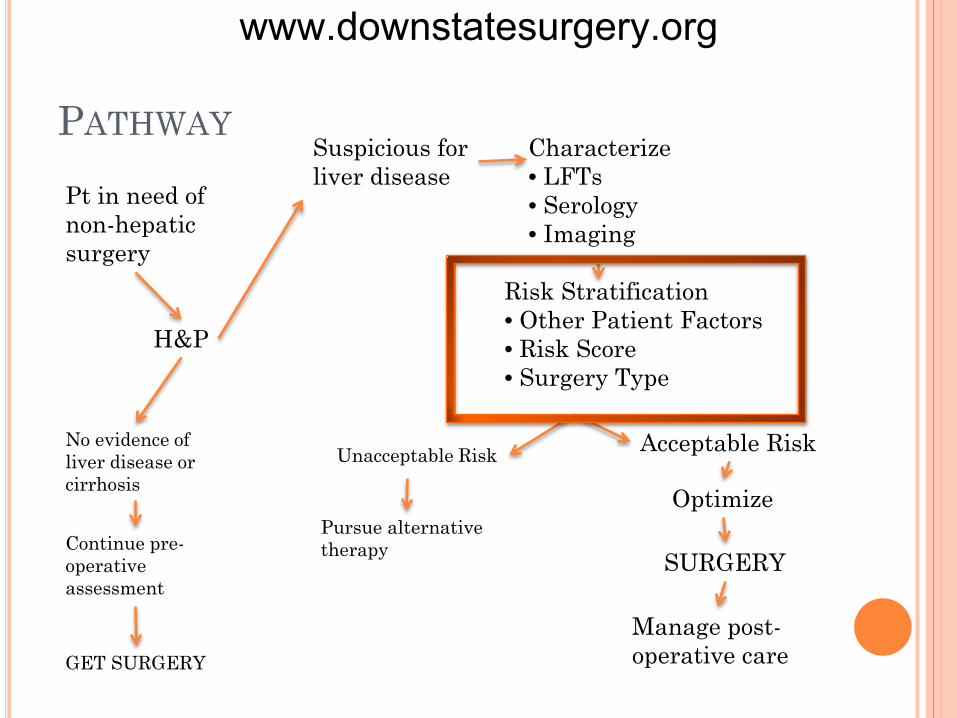
PATHWAY Pt in need of non-hepatic surgery
H&P
No evidence of liver disease or cirrhosis
Continue pre-operative assessment
GET SURGERY
Suspicious for liver disease
Characterize • LFTs • Serology • Imaging
Risk Stratification • Other Patient Factors • Risk Score • Surgery Type
Acceptable Risk
Optimize
SURGERY
Unacceptable Risk
Pursue alternative therapy
Manage post-operative care
www.downstatesurgery.org
WHY RISK STRATIFY? Patients with cirrhosis need surgery
Umbilical hernia Gallbladder Colon Cardiac Emergency surgical conditions Liver surgery and transplantation
Patients with cirrhosis do worse The effects of surgery (and other stressors) are
complicated and unpredictable
7
www.downstatesurgery.org

OTHER PATIENT FACTORS
www.downstatesurgery.org
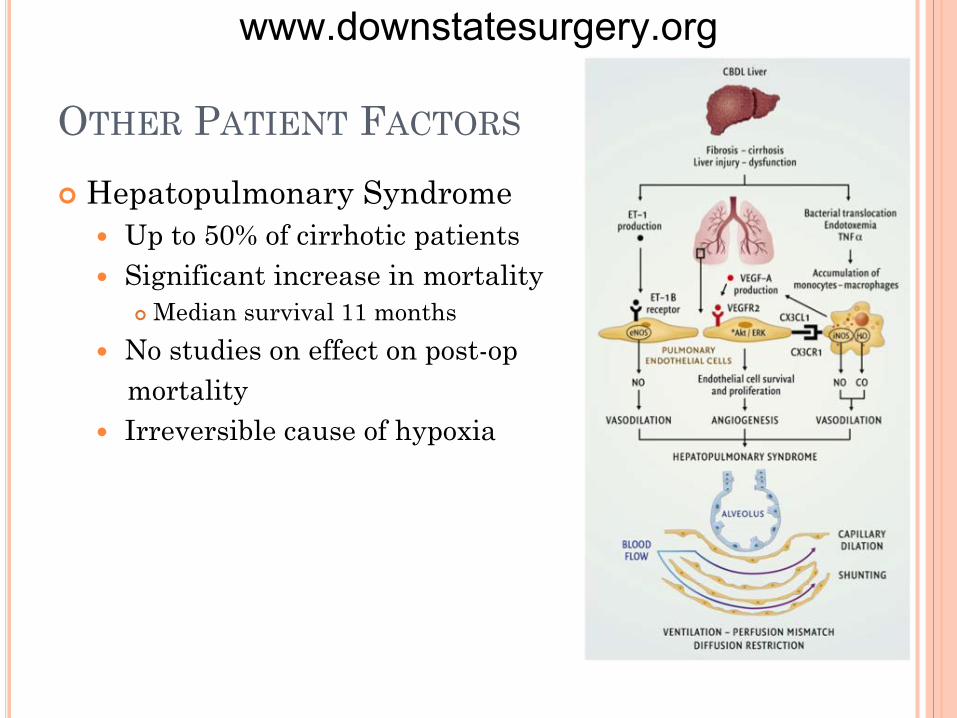
OTHER PATIENT FACTORS Hepatopulmonary Syndrome
Up to 50% of cirrhotic patients Significant increase in mortality
Median survival 11 months No studies on effect on post-op mortality Irreversible cause of hypoxia
www.downstatesurgery.org
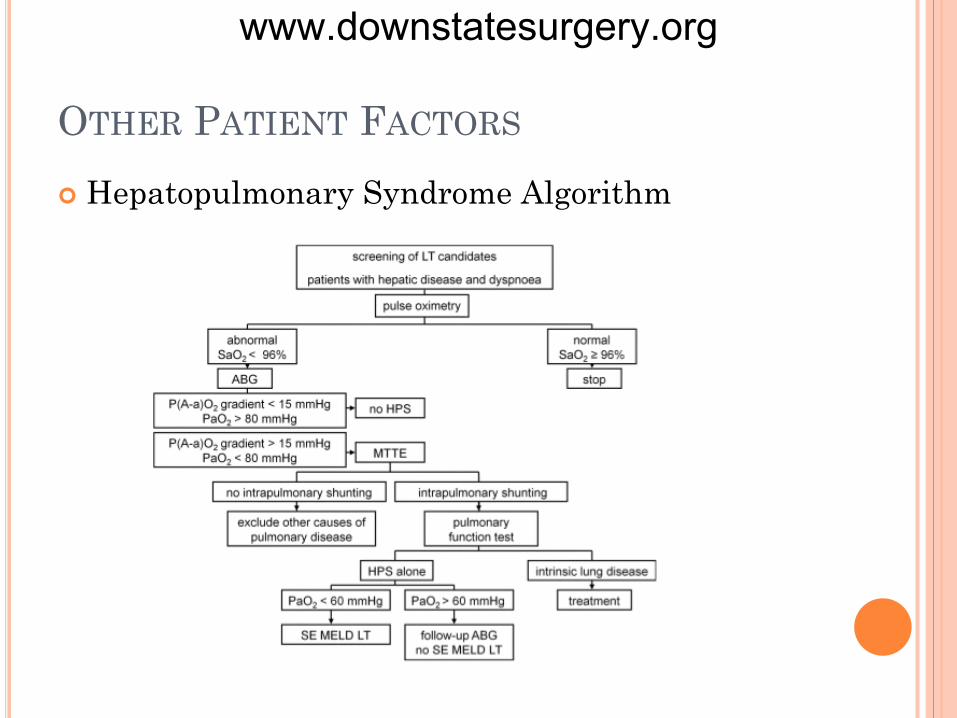
OTHER PATIENT FACTORS Hepatopulmonary Syndrome Algorithm
www.downstatesurgery.org
RISK SCORES: CHILD-TURCOTTE-PUGH 1964 - Child & Turcotte Mortality after shunting surgery for portal htn Variables, original:
Albumin Bilirubin Encephalopathy Ascites Nutritional status
www.downstatesurgery.org
RISK SCORES: CHILD-TURCOTTE-PUGH 1973 - Pugh et al “Transection of the oesophagus
for bleeding oesophageal varices” (BJS) Mortality after surgery for bleeding varices Variables, updated:
Albumin Bilirubin Encephalopathy Ascites Nutritional status Prothrombin time
www.downstatesurgery.org
RISK SCORES: CHILD-TURCOTTE-PUGH Ease of use, simplicity 40 years and 100s of papers
Ruptured esophageal varices Subclinical encephalopathy Hepatocellular carcinoma Alcoholic cirrhosis Decompensated HCV-related cirrhosis Primary sclerosing cholangitis Primary biliary cirrhosis Budd–Chiari syndrome Liver surgery and transplant Mortality after non-hepatic surgery
www.downstatesurgery.org
1997 92 patients with cirrhosis undergoing emergent
or elective surgery 54 variables evaluated retrospectively CTP score most predictive of mortality The study thought of as the “validation” study as
the mortality figures mirror those from original paper
www.downstatesurgery.org
RISK SCORES: CHILD-TURCOTTE-PUGH MDCalc
www.downstatesurgery.org
RISK SCORES: CHILD-TURCOTTE-PUGH Disadvantages:
Ascites and encephalopathy are SUBJECTIVE Validation has been mainly in RETROSPECTIVE
studies with SMALL study populations Variables NOT WEIGHTED CAUSE of cirrhosis not included SURGERY type not included
www.downstatesurgery.org

RISK SCORES: MELD MELD: Model for End-stage Liver Disease
2000 – retrospective 231 patients who underwent TIPS Cox-proportio……(statistics) 3 weighted variables: bilirubin, INR, creatinine
www.downstatesurgery.org

RISK SCORES: MELD
Validation with 4 larger data sets (n=282 to n=1179)
Mortality overall, unrelated to undergoing a procedure
Allogenic transplant allocation
www.downstatesurgery.org
RISK SCORES: MELD MDCalc
www.downstatesurgery.org
RISK SCORES: MELD
www.downstatesurgery.org

RISK SCORES: MELD
2004 - prospective 40 patients undergoing elective (n=24) or
emergent (n=16) surgical procedures CTP and MELD
www.downstatesurgery.org
RISK SCORES: MELD Advantages:
All variables are OBJECTIVE Validation for overall mortality risk has utilized
LARGE study populations Variables WEIGHTED
MELD = 3.78×ln[serum bilirubin (mg/dL)] + 11.2×ln[INR] + 9.57×ln[serum creatinine (mg/dL)] + 6.43
Disadvantages Assessment of mortality in cirrhotic patients after
surgery continued to rely on SMALL data sets CAUSE of cirrhosis not included SURGERY type not included
www.downstatesurgery.org

RISK SCORES - WHAT TO USE?
www.downstatesurgery.org
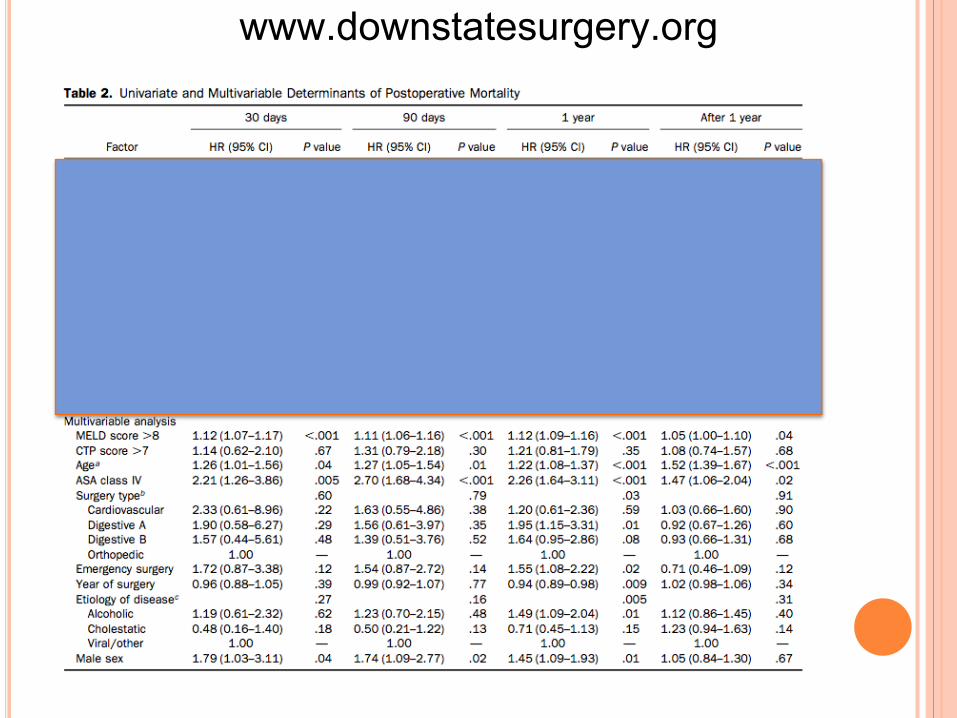
RISK SCORES - WHAT TO USE?
2007 - retrospective 772 cirrhotic patients undergoing
digestive(n=586), orthopedic (n=107) or cardiac surgery (n=79)
Multivariable analysis (w/ statistics)
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org

IS THAT IT? Pt in need of non-hepatic surgery
H&P
No evidence of liver disease or cirrhosis
Continue pre-operative assessment
GET SURGERY
Suspicious for liver disease
Characterize • LFTs • Serology • Imaging
Risk Stratification • Risk Score • Other Patient Factors • Surgery Type
Acceptable Risk
Optimize
SURGERY
Unacceptable Risk
Pursue alternative therapy
Manage post-operative care
www.downstatesurgery.org

SURGERY SPECIFIC FACTORS Type of surgery has significant impact
www.downstatesurgery.org

www.downstatesurgery.org
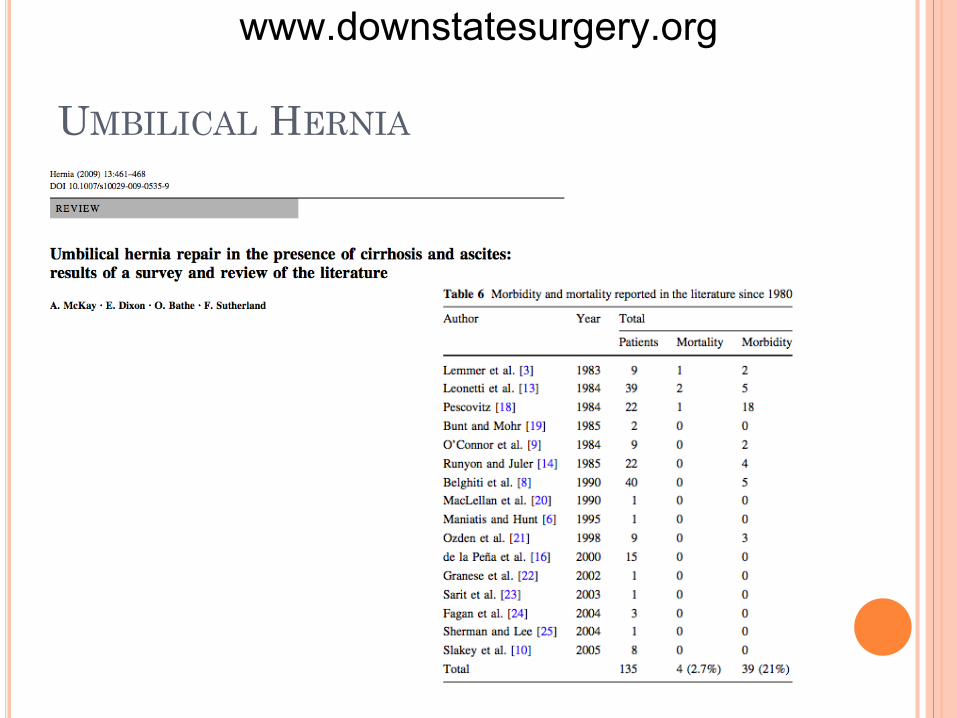
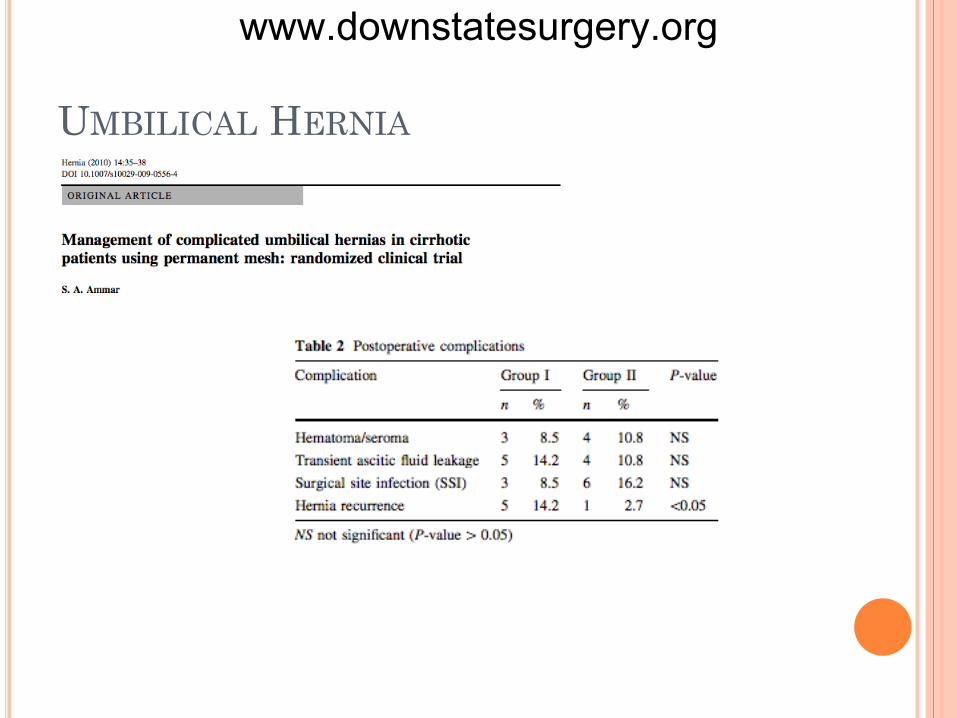
UMBILICAL HERNIA Significant problem in cirrhotics
20% prevalence, 40-50% in setting of ascites Enlarge over time Skin breakdown and necrosis SBP
What role do risk scores play? Surgery for UH an exception to these scores?
www.downstatesurgery.org
UMBILICAL HERNIA
www.downstatesurgery.org
UMBILICAL HERNIA
www.downstatesurgery.org

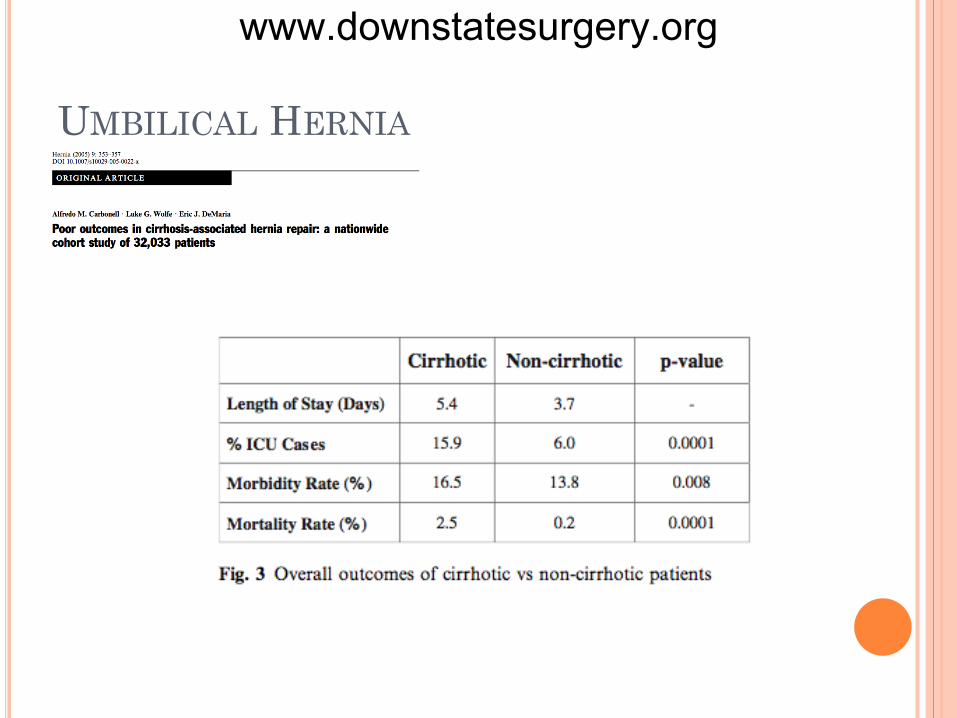
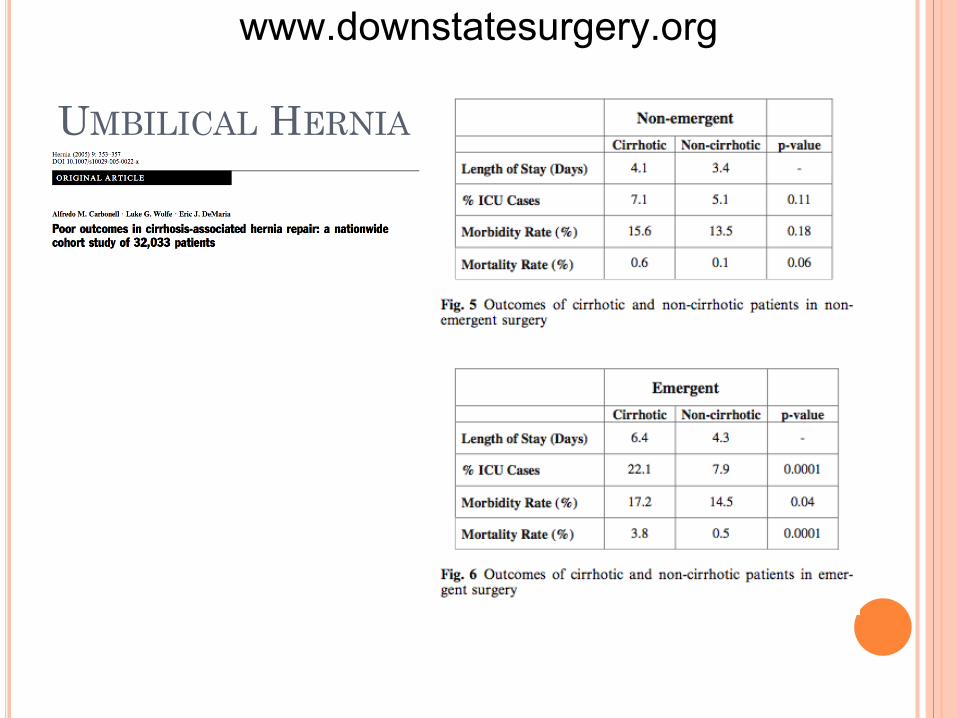
UMBILICAL HERNIA
32,033 patients who underwent abdominal wall hernias between 1999 and 2004 (excluding inguinal)
1197 cirrhotic patients Emergency surgery performed in 60% of
cirrhotics (vs 30% non-cirrhotics) Does not include table comparison between study
groups
www.downstatesurgery.org
UMBILICAL HERNIA
www.downstatesurgery.org
UMBILICAL HERNIA
www.downstatesurgery.org
UMBILICAL HERNIA
www.downstatesurgery.org
UMBILICAL HERNIA
www.downstatesurgery.org

SUMMARY 1 Pre- and Post-operative issues in cirrhotics
1. There are dysfunctions related to cirrhosis that deserve special attention
2. Awareness of the precariousness of cirrhotic physiology, readiness to act
www.downstatesurgery.org
SUMMARY 2 Risk stratification for cirrhotic patients
undergoing non-hepatic surgery includes 1. Review and consider contraindications to elective
surgery, including HPS 2. Calculation of a risk score, of which the Mayo Clinic
augmented MELD appears the most robust 3. Consideration of surgery specific data on morbidity
and mortality
www.downstatesurgery.org

SUMMARY 3 Umbilical hernia repair in cirrhotic patients
Is safe, with acceptable morbidity and mortality When performed under elective conditions, has
comparable morbidity and mortality to non-cirrhotics Should be performed when found to avoid the
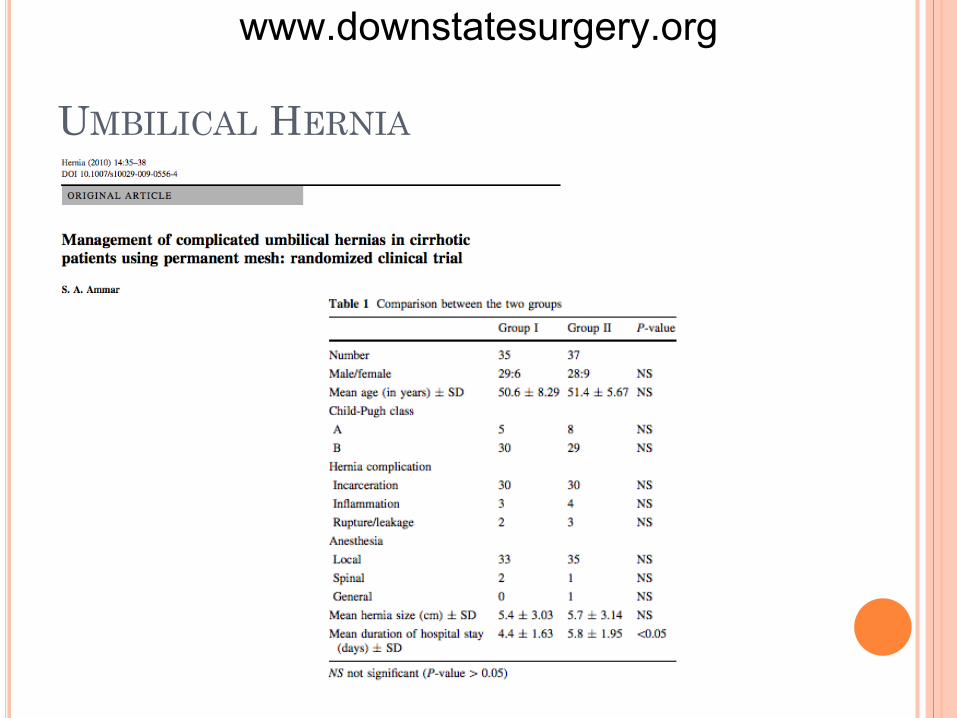
increase in mortality under emergent conditions Can probably be performed using synthetic mesh
www.downstatesurgery.org

www.downstatesurgery.org
www.downstatesurgery.org

www.downstatesurgery.org






![Same-day surgery for femoral, inguinal and umbilical hernia repair ... · PDF file[Type text] Same-day surgery for femoral, inguinal and umbilical hernia repair in adults Final Report](https://img.dokumen.tips/doc/110x75/5a741d7e7f8b9a63638b9c2b/same-day-surgery-for-femoral-inguinal-and-umbilical-hernia-repair-type.jpg)