Embed Size (px)
Citation preview

Type A Ao Dissection – Evolution in understanding of the Great Masquerader & assessing the
underlying Silent Killer
Dept. of Critical Care Medicine Grand RoundsUniversity of Calgary
March 21, 2018
Jehangir AppooDivision of Cardiac Surgery
On behalf of the Calgary Thoracic Aortic Program
aorta.ca
Audience for this talk:
Intensivists
Diverse backgrounds – Internal Medicine, Neurology, Pulmonary, Surgery, Anaesthesia….
Highly educatedInsightful, v. bright
Take care of the sickest patients in the hospital
What can I tell this group about Aortic Dissection that matters to them?
what we know what we don’t knowevolution
Doctors are men who prescribe medicines of which they know little, to cure diseases of which they know less, in human beings of whom they know nothing
- Voltaire (1694 – 1778)… (or was it T. Godinez? )

Case – June 2017
57yo male collapsed with Abdo Pain on soccer field around 8pm
EMS called and taken to RGH
PMHx : HealthyKnown for a 4.3cm ascending aorta
FHx: Mother had 2 sisters with aortic dissection

Case
8pm onwards - ongoing abdo pain in ER4:15 am CT abdo followed by CT chest
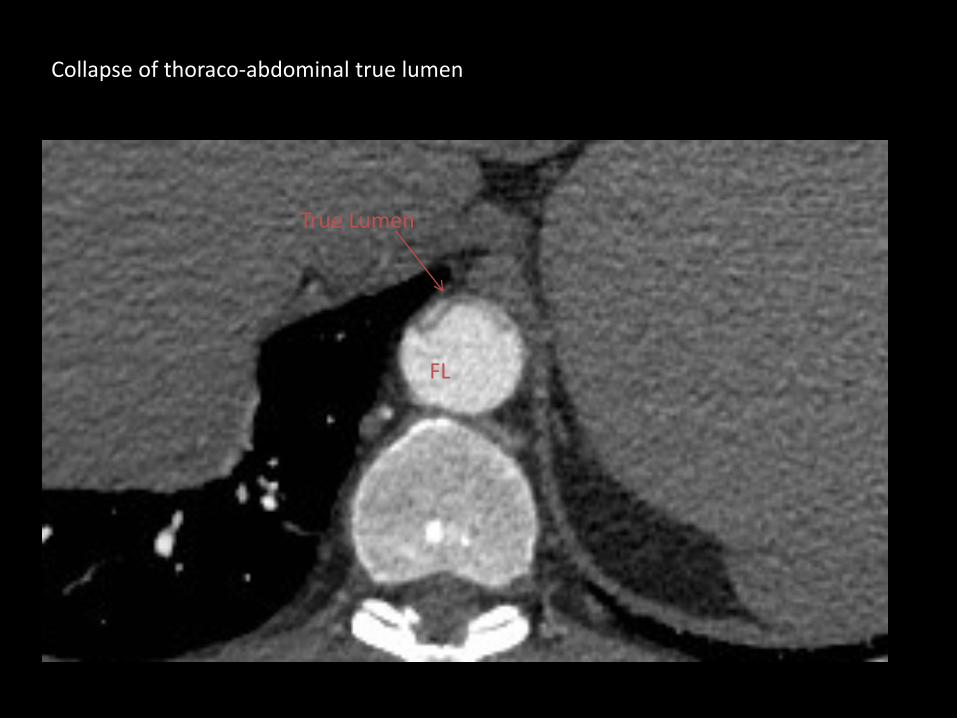
Collapse of thoraco-abdominal true lumen
True Lumen
FL

Collapse of thoraco-abdominal true lumen
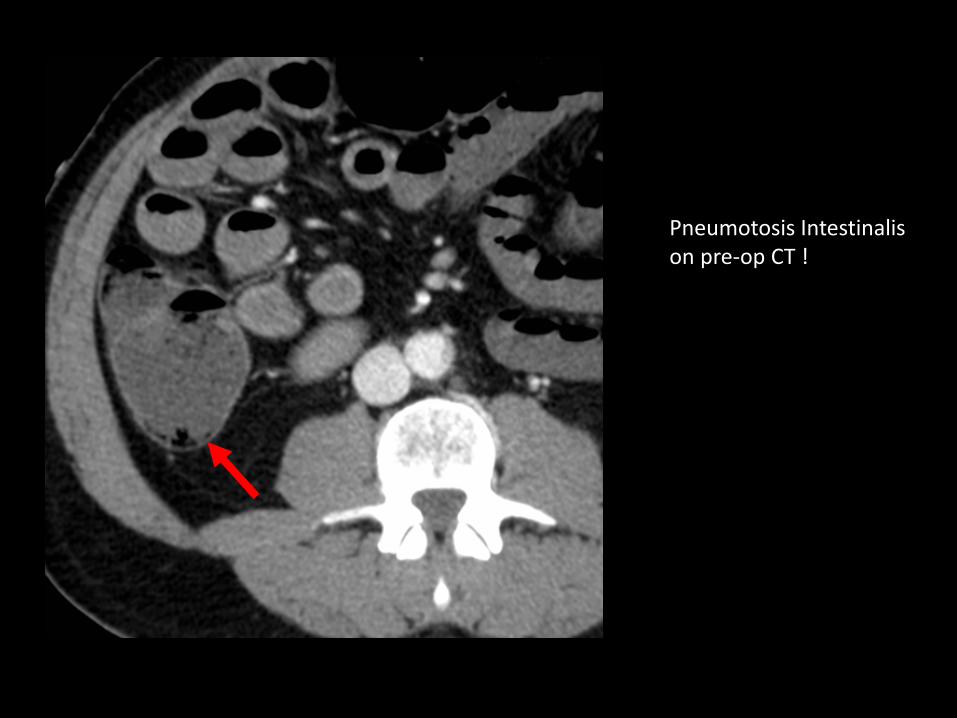
Pneumotosis Intestinalis on pre-op CT !
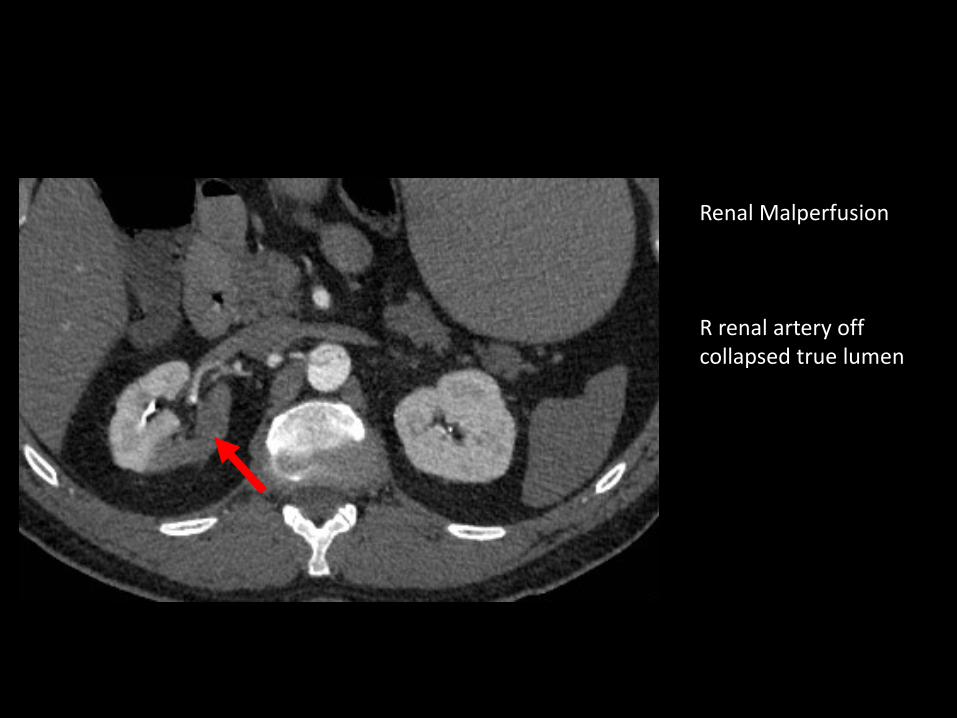
Renal Malperfusion
R renal artery off collapsed true lumen

Upon transfer to CVICU –10 -12 hours post collapse on soccer field
BP “stable”
Tender abdomenLactate 5pH 7.1K+ 6.9

Intraop TEESevere AINormal LV/RV FunctionNo significant pericardial effusion
Our patient’s acute problems secondary to Aortic Dissection:
Impending rupture of ascending aorta
Severe Aortic Insufficiency
Collapse of true lumen in thoraco-abdominal aorta
Visceral malperfusion with cell death/lysis Dead gut vs viable bowel ?
Renal malperfusion

11% 47% 11% 7% 4% 20%(n=157) (n=673) (n=161) (n=98) (n=58) (n=280)
• 1427 patients • 954 male• mean age 61.7 years
Contemporary Classification of Aortic Dissection
IRAD – Ann Thorac Surg 2016

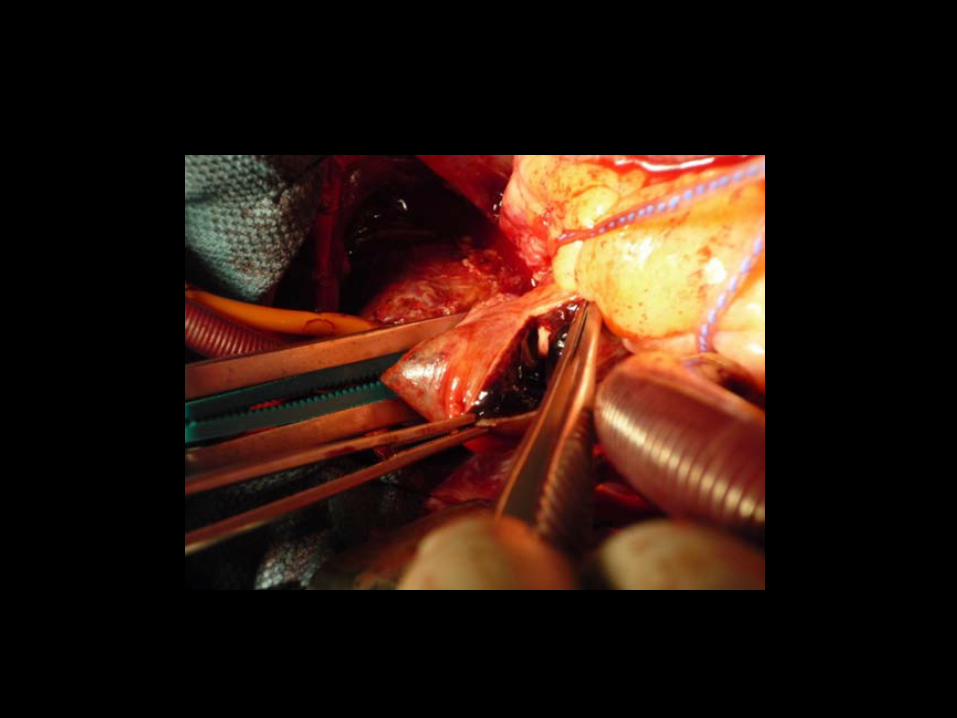
Intraop view of Type A Dissection
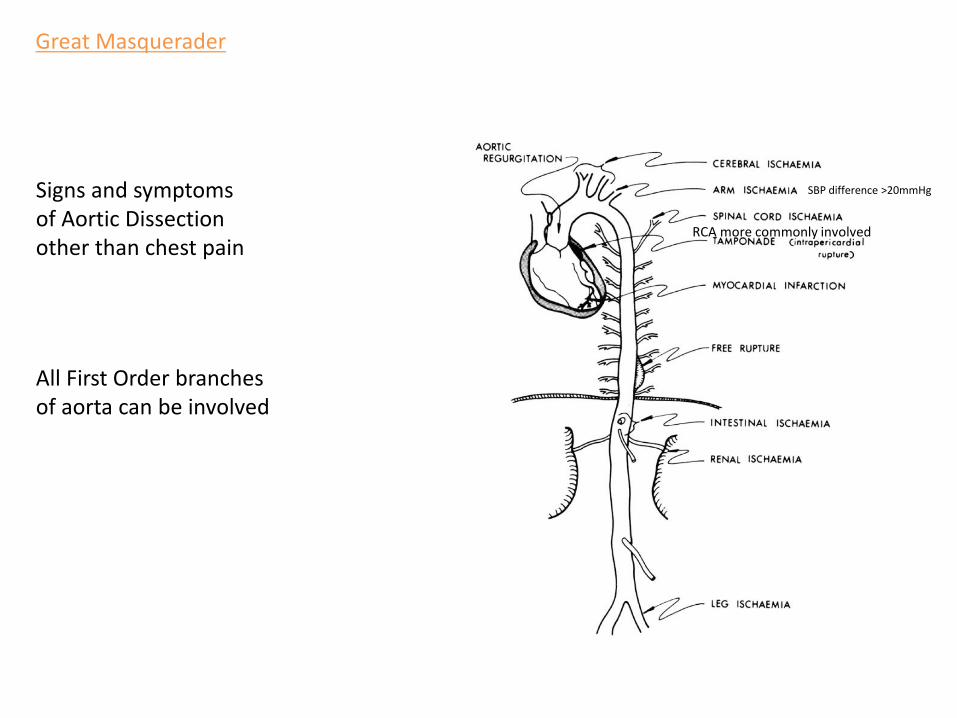
Great Masquerader
Signs and symptoms of Aortic Dissection other than chest pain
RCA more commonly involved
SBP difference >20mmHg
All First Order branches of aorta can be involved

You cannot deceive everybody all of the time
- Abraham Lincoln
Great Masquerader
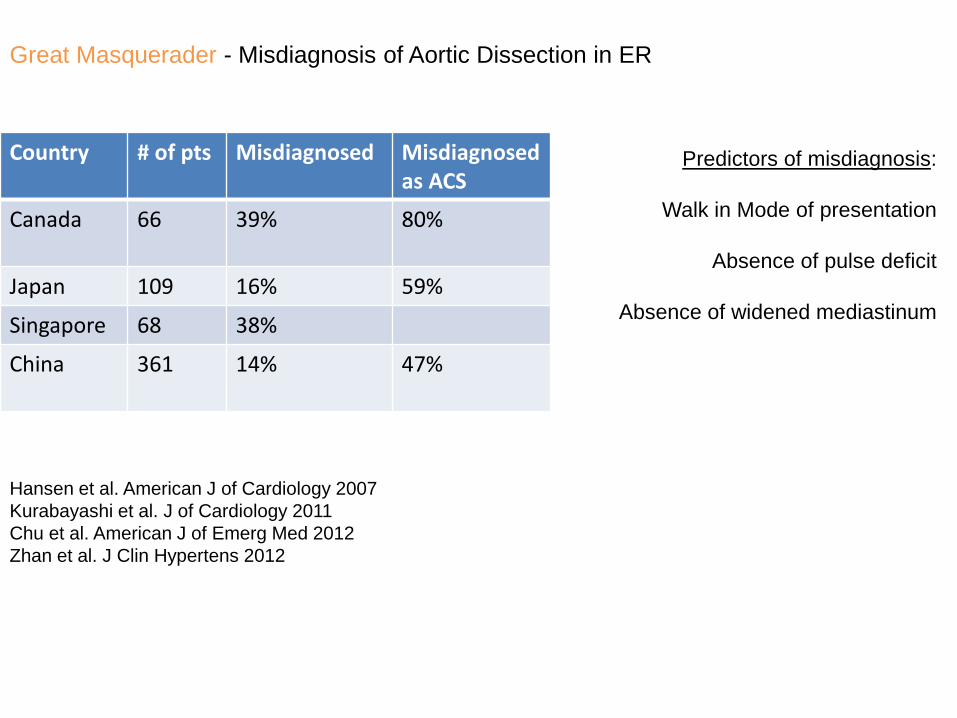
Country # of pts Misdiagnosed Misdiagnosedas ACS
Canada 66 39% 80%
Japan 109 16% 59%
Singapore 68 38%
China 361 14% 47%
Hansen et al. American J of Cardiology 2007Kurabayashi et al. J of Cardiology 2011Chu et al. American J of Emerg Med 2012Zhan et al. J Clin Hypertens 2012
Great Masquerader - Misdiagnosis of Aortic Dissection in ER
Predictors of misdiagnosis:
Walk in Mode of presentation
Absence of pulse deficit
Absence of widened mediastinum
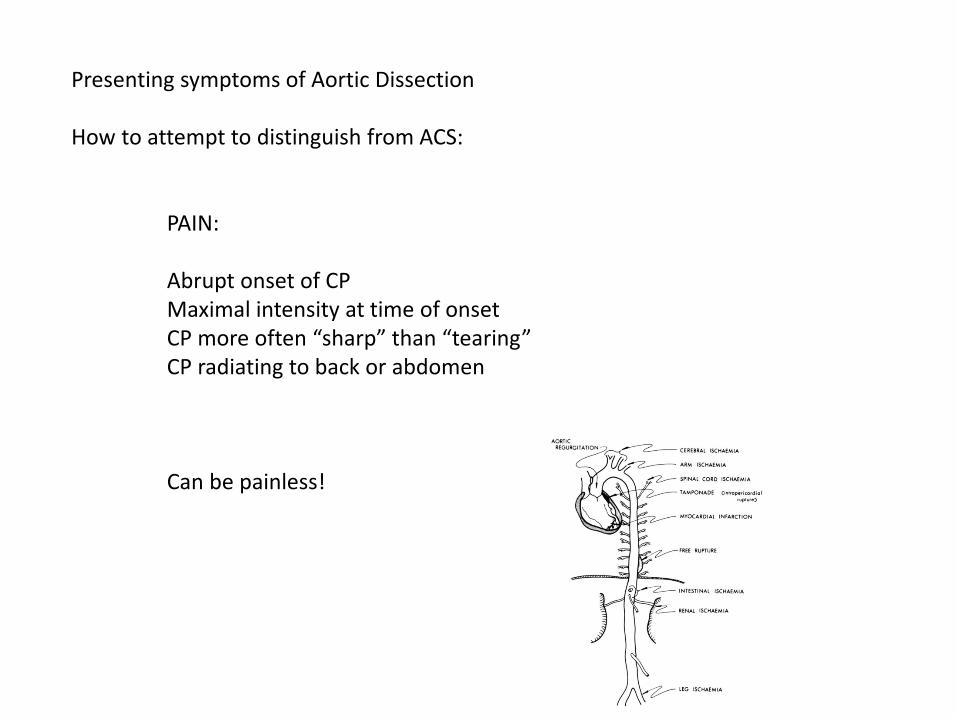
Presenting symptoms of Aortic Dissection
How to attempt to distinguish from ACS:
PAIN:
Abrupt onset of CPMaximal intensity at time of onsetCP more often “sharp” than “tearing”CP radiating to back or abdomen
Can be painless!
Consequences of Misdiagnosis:
Delayed diagnosis of lethal pathology of variable urgency
Inappropriate treatment antiplatelet agents anti-thrombin agentsfibrinolytics

Initial Medical Treatment of Aortic Dissection
Anti-impulse therapy 60/100 rule : HR 60bpmSBP 100mmHgIV B-blockers and Nipride
Pearl #1
Initial Medical Treatment of Aortic Dissection
Anti-impulse therapy 60/100 rule : HR 60bpmSBP 100mmHgIV B-blockers and Nipride
Pain control narcotics
Arterial line in arm with higher blood pressure

Initial Medical Treatment of Aortic Dissection
Anti-impulse therapy 60/100 rule : HR 60bpmSBP 100mmHgIV B-blockers and Nipride
Pain control narcotics
Arterial line in arm with higher blood pressure
Type B dissections: close observation in ICU for complications secondary to branch vessel involvement Remember the Great Masquerader

If Hypotensive:
Role of pericardiocentesis in ER ?
Fluid Resuscitation
Pearl #2
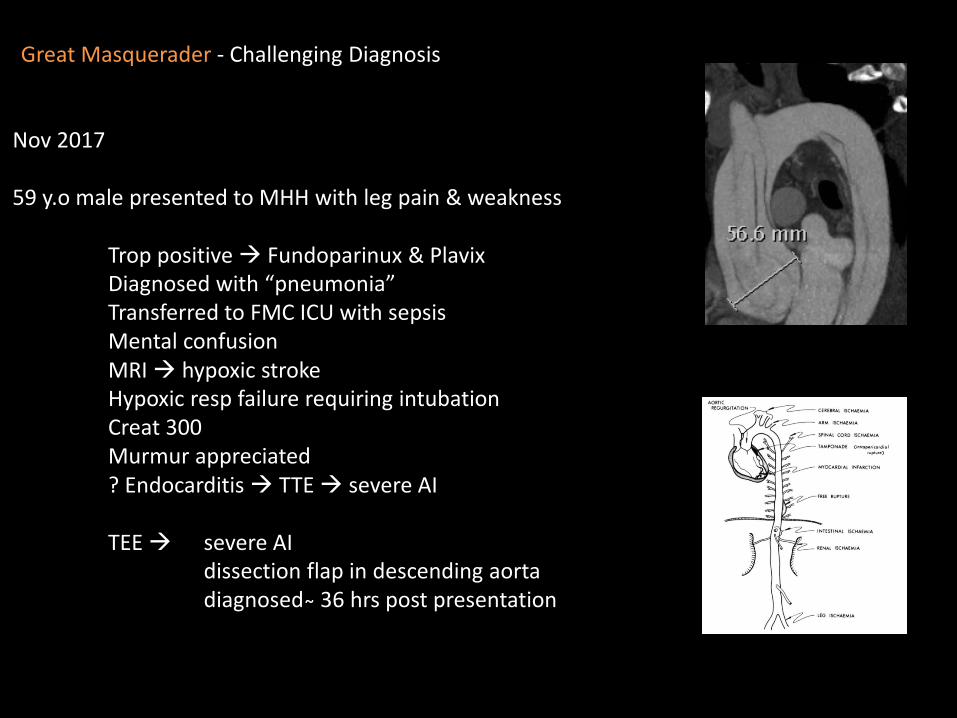
Nov 2017
59 y.o male presented to MHH with leg pain & weakness
Trop positive Fundoparinux & PlavixDiagnosed with “pneumonia” Transferred to FMC ICU with sepsisMental confusionMRI hypoxic strokeHypoxic resp failure requiring intubationCreat 300Murmur appreciated? Endocarditis TTE severe AI
TEE severe AIdissection flap in descending aortadiagnosed ̴ 36 hrs post presentation
Great Masquerader - Challenging Diagnosis

Even more true for the Great Masquerader

March 2016
20 y.o male abdo pain
Lap Appendectomy at Rural Hospital
Repeat CT POD4 for CP/unwell
Died prior to transfer
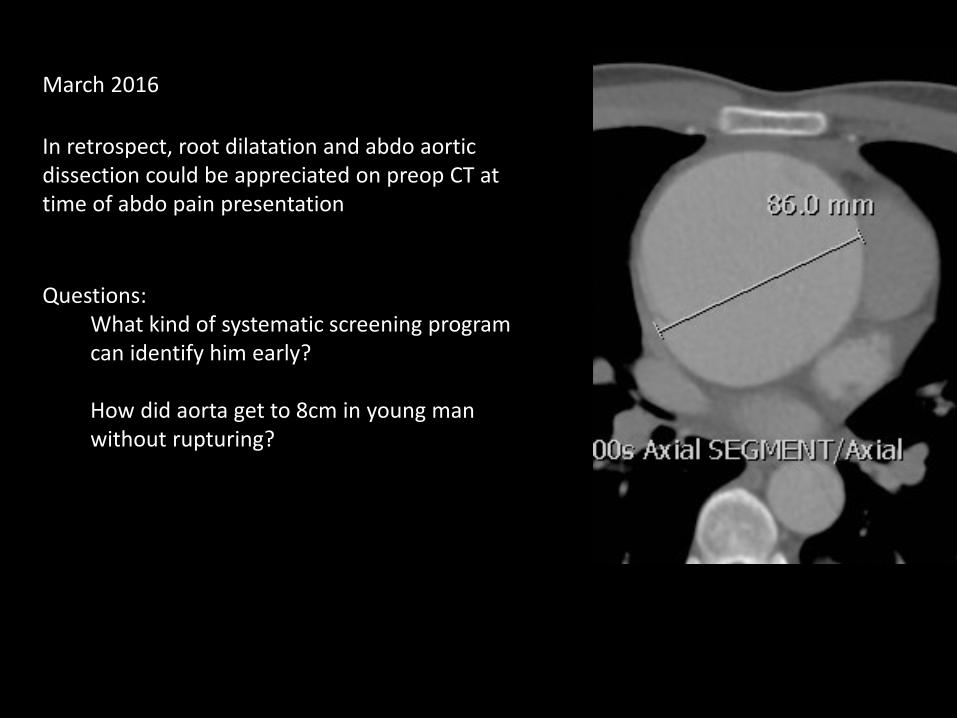
In retrospect, root dilatation and abdo aortic dissection could be appreciated on preop CT at time of abdo pain presentation
Questions:What kind of systematic screening program can identify him early?
How did aorta get to 8cm in young man without rupturing?
March 2016
Type A Aortic Dissection
Variable acuity 1%/hr
Variable presentation “Great Masquerader”
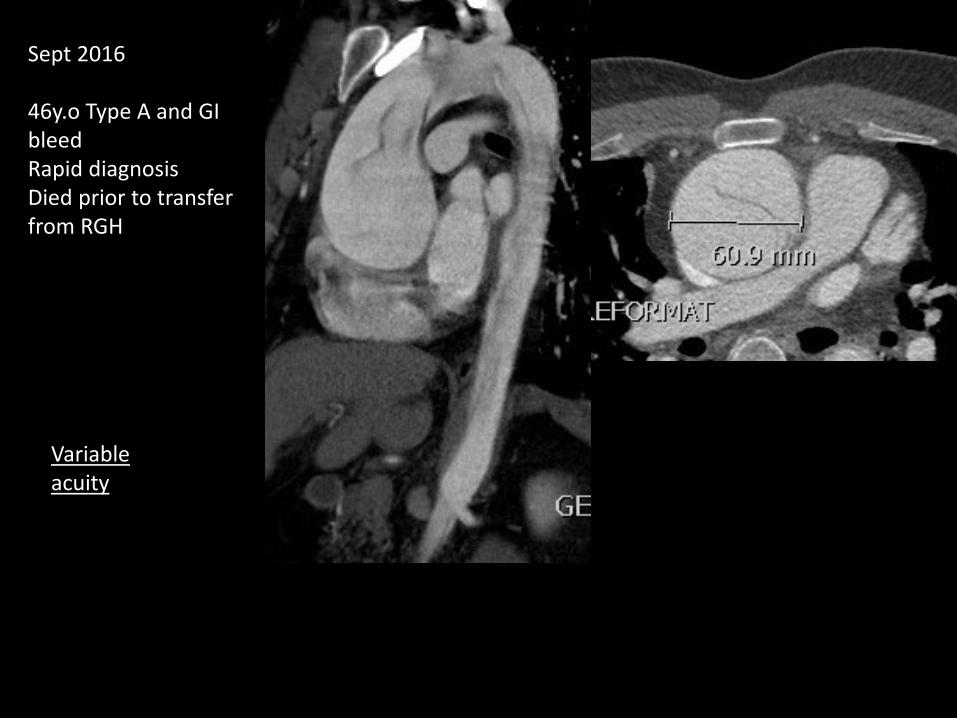
Sept 2016
46y.o Type A and GI bleedRapid diagnosisDied prior to transfer from RGH
Variable acuity
Why is Aorta Aneurysm challenging?
SILENT KILLER
LethalAneurysm disease top 20 causes of death of human beingsActual number likely underestimated
Asymptomatic95% are asymptomatic prior to catastrophic event
“Any aneurysm of the aorta is a hopeless condition” - William Osler, 1903
Etiology of the Silent Killer
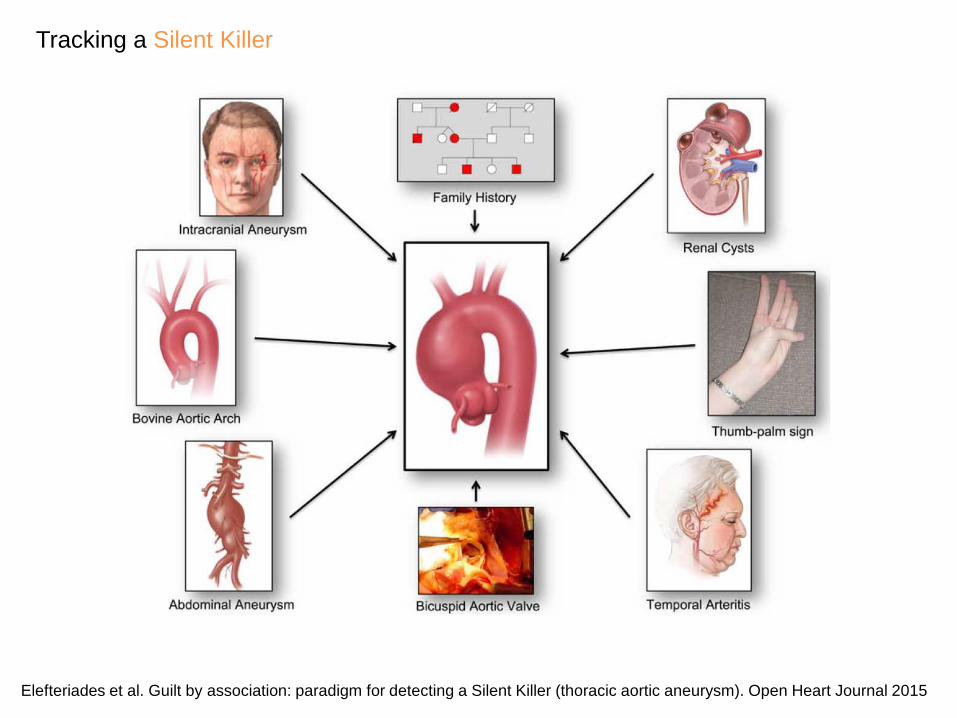
Tracking a Silent Killer
Elefteriades et al. Guilt by association: paradigm for detecting a Silent Killer (thoracic aortic aneurysm). Open Heart Journal 2015

SyndromicFamilial
Sporadic
High risk genetic variants
Low risk genetic variants
Genetic-------------------------------------------------------------Environmental
Slide courtesy of Dr. Ouzounian
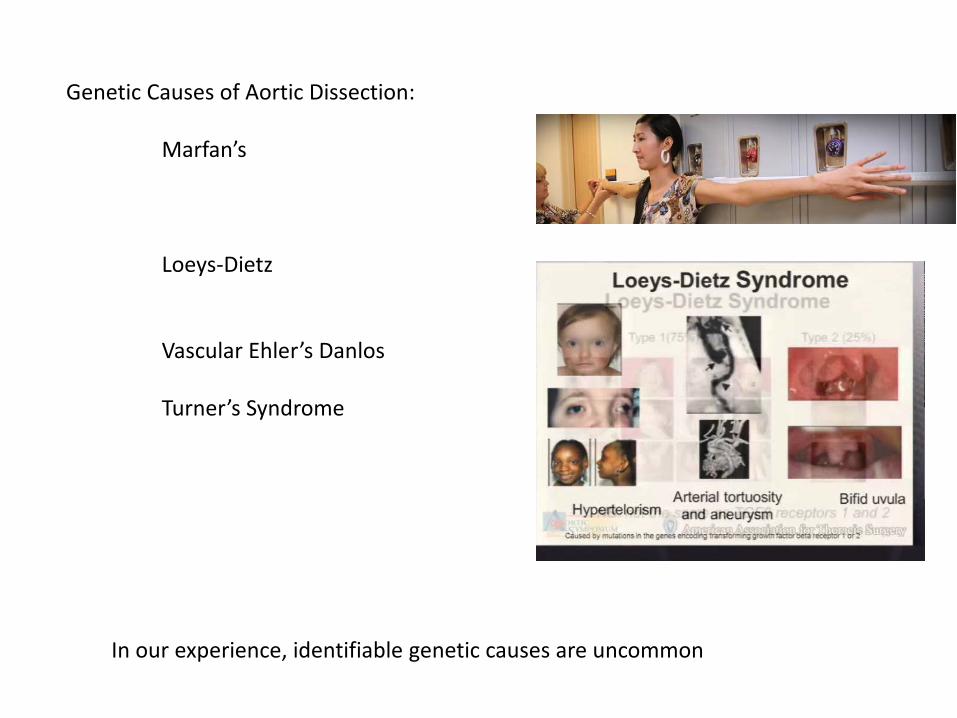
Genetic Causes of Aortic Dissection:
Marfan’s
Loeys-Dietz
Vascular Ehler’s Danlos
Turner’s Syndrome
In our experience, identifiable genetic causes are uncommon

Role of Hypertension in Etiology of Aortic Dissection
easy/intuitive blames patient
however, severe pre-op HTN not the norm
Need to look harder as to why aortas break
Conventional Operation
Tear specific operationResect Intimal Entry Site
“Standard of care” for acute Type A Dissection – when I started in 2005
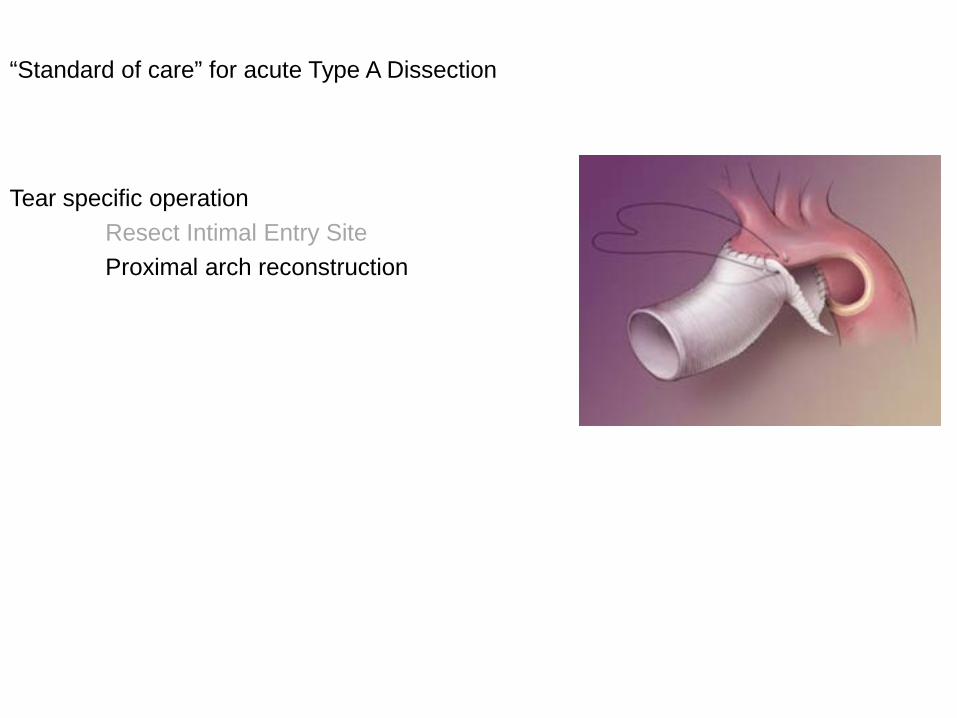
Conventional Operation
Tear specific operationResect Intimal Entry SiteProximal arch reconstruction
“Standard of care” for acute Type A Dissection
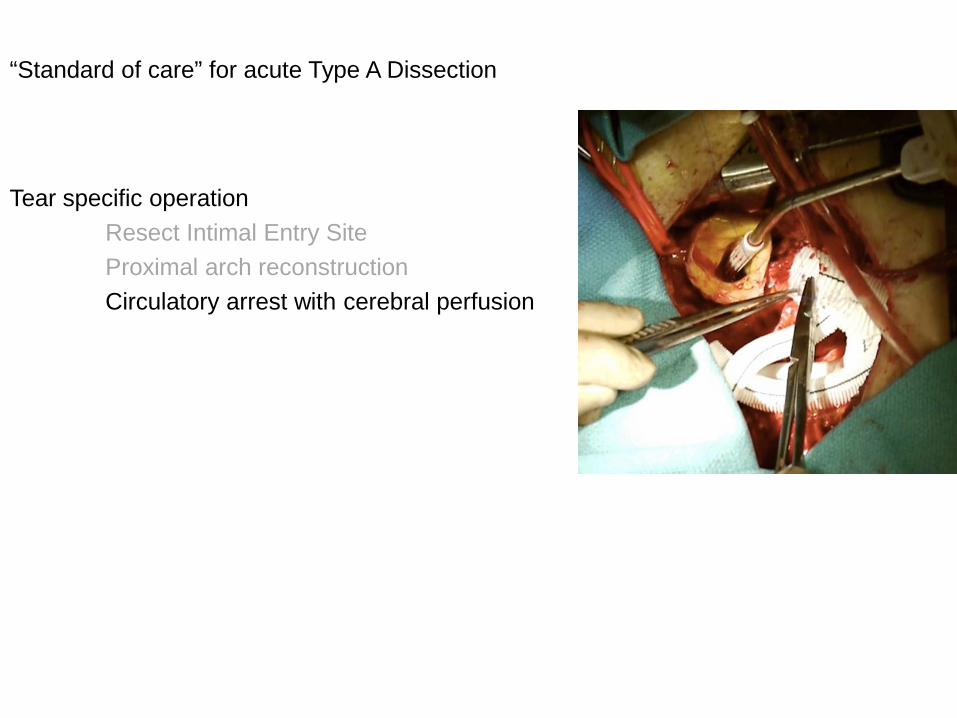
Conventional Operation
Tear specific operationResect Intimal Entry SiteProximal arch reconstructionCirculatory arrest with cerebral perfusion
“Standard of care” for acute Type A Dissection
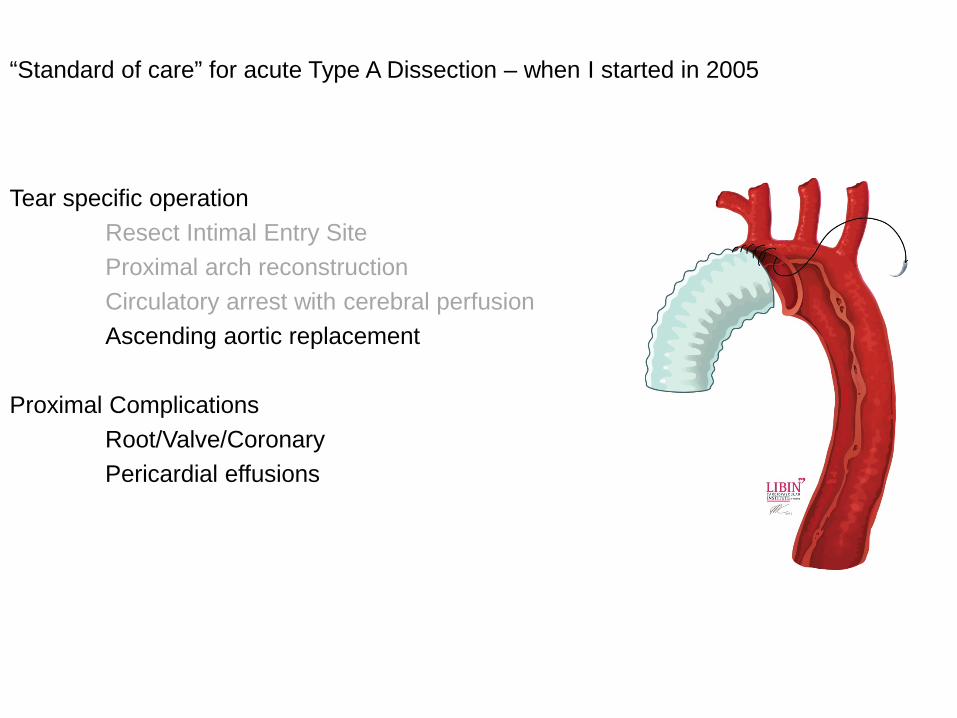
Conventional Operation
Tear specific operationResect Intimal Entry SiteProximal arch reconstructionCirculatory arrest with cerebral perfusionAscending aortic replacement
Proximal ComplicationsRoot/Valve/CoronaryPericardial effusions
“Standard of care” for acute Type A Dissection – when I started in 2005
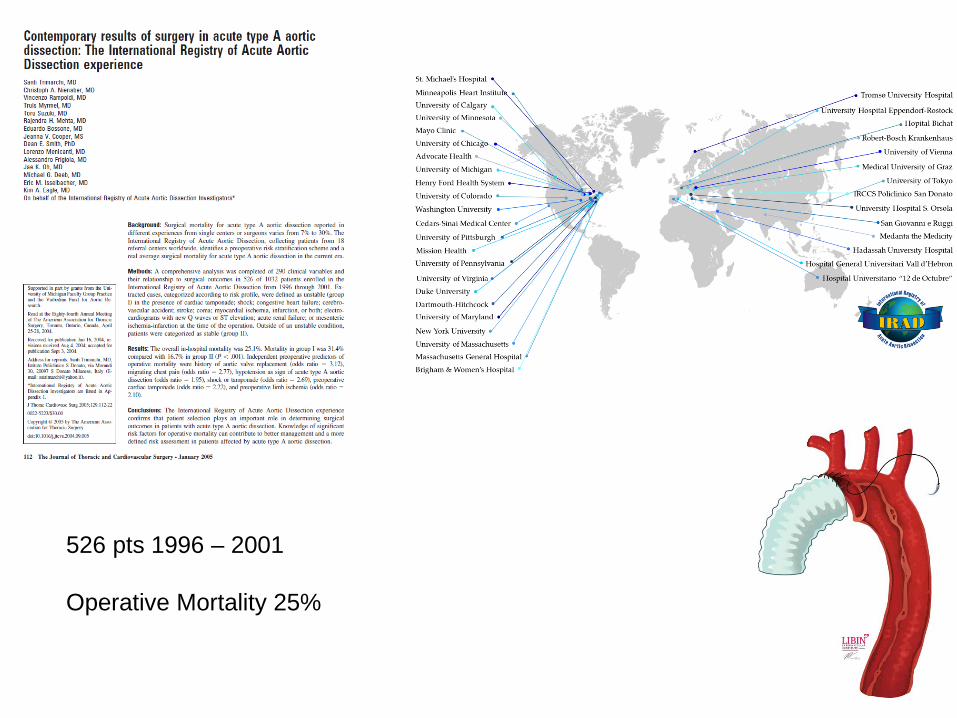
526 pts 1996 – 2001
Operative Mortality 25%
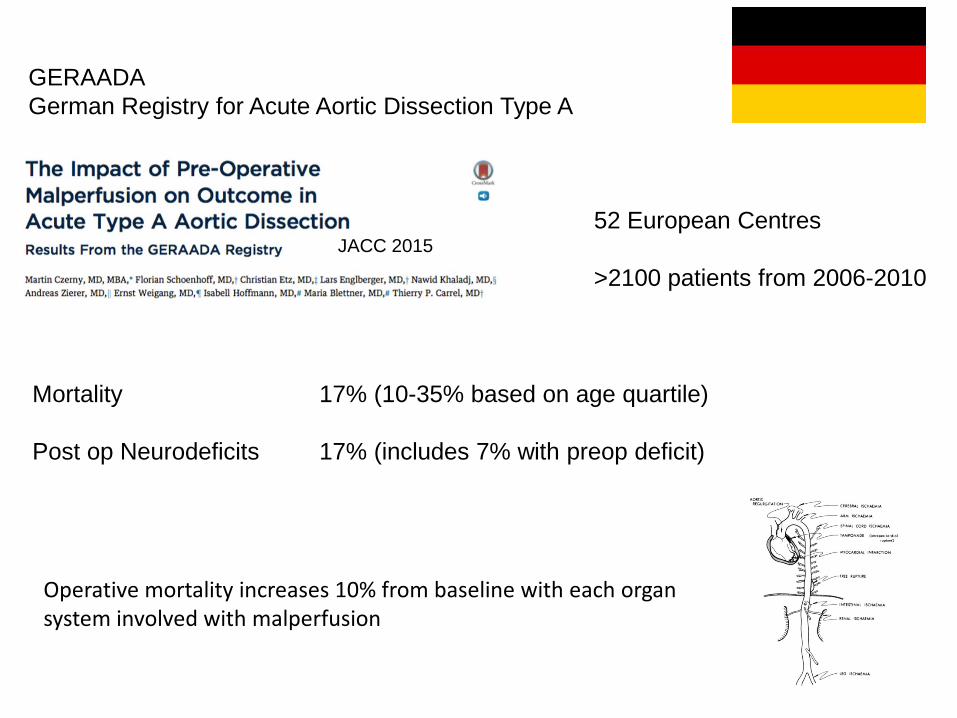
GERAADA German Registry for Acute Aortic Dissection Type A
52 European Centres
>2100 patients from 2006-2010JACC 2015
Mortality 17% (10-35% based on age quartile)
Post op Neurodeficits 17% (includes 7% with preop deficit)
Operative mortality increases 10% from baseline with each organ system involved with malperfusion
In addition to world wide high periop mortality (17-25%)....long term outcome for survivors is questionable
Double dagger of Type A Dissection Surgery
Example of possible outcome of conventional surgery
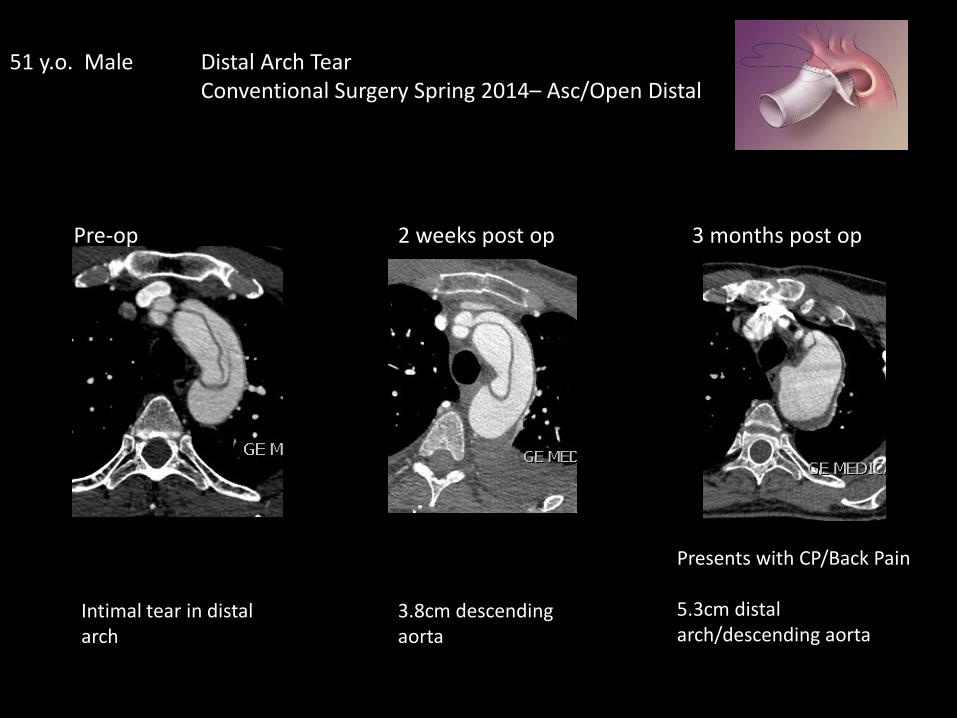
51 y.o. Male Distal Arch TearConventional Surgery Spring 2014– Asc/Open Distal
Pre-op 2 weeks post op 3 months post op
Intimal tear in distal arch
3.8cm descending aorta
Presents with CP/Back Pain
5.3cm distal arch/descending aorta

Given known CT disorder, rapid rate of growth, residual dissected arch, 4 branch arch with dominant left vertebral, redo sternotomy setting
Progressed to urgent thoracotomy & resection of distal arch and descending aorta
Profound HypothermiaL chest circ arrestCSF drain for Safi type C aneurysm
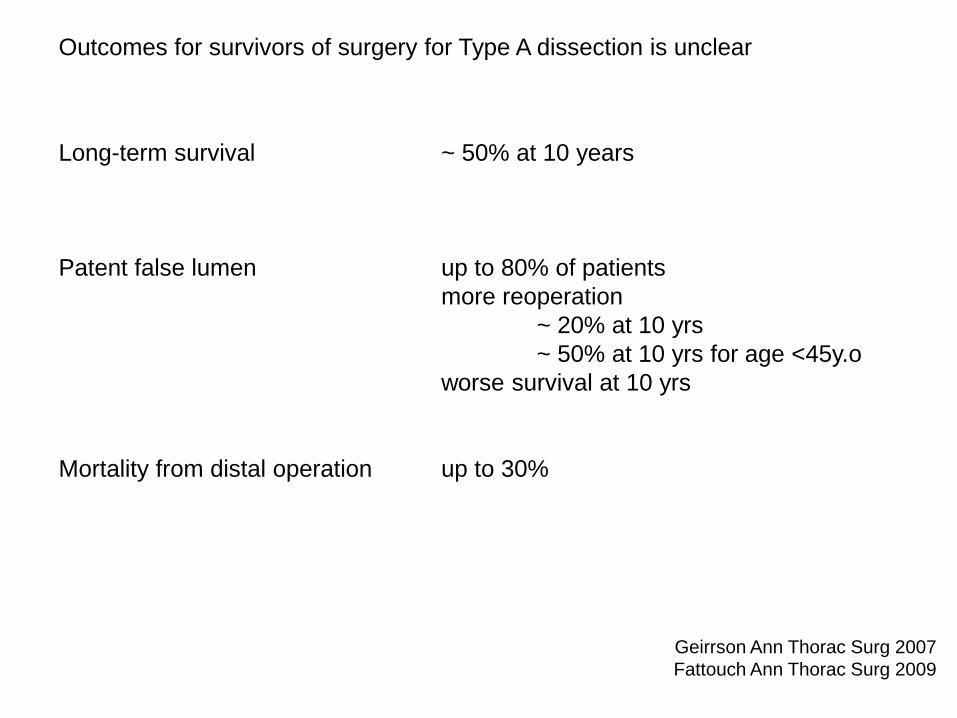
Outcomes for survivors of surgery for Type A dissection is unclear
Long-term survival ~ 50% at 10 years
Patent false lumen up to 80% of patientsmore reoperation
~ 20% at 10 yrs~ 50% at 10 yrs for age <45y.o
worse survival at 10 yrs
Mortality from distal operation up to 30%
Geirrson Ann Thorac Surg 2007Fattouch Ann Thorac Surg 2009
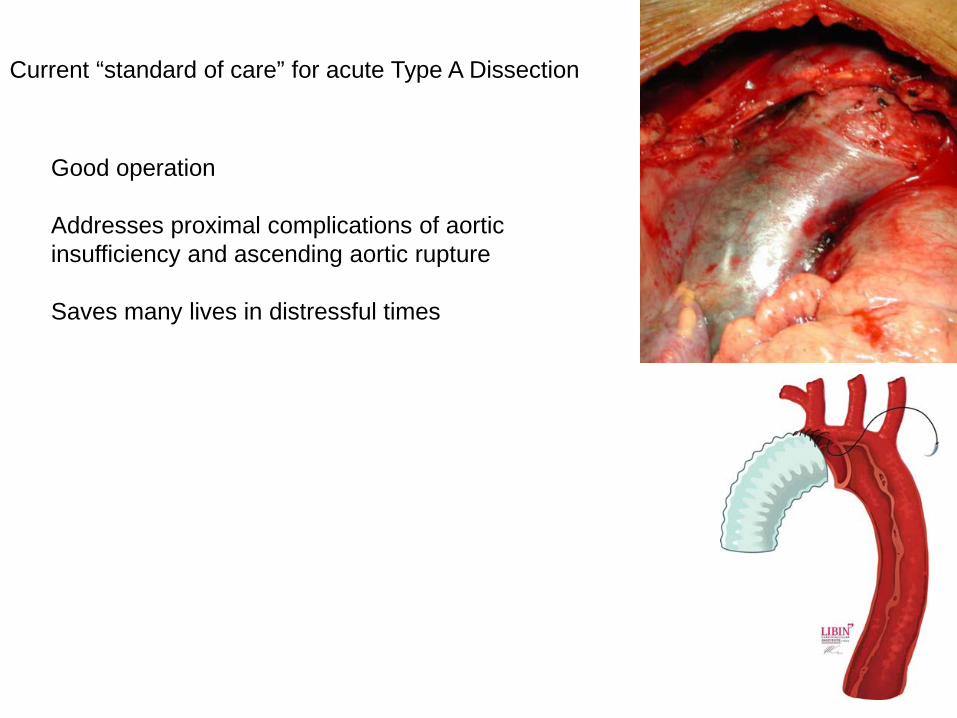
Conventional OperationCurrent “standard of care” for acute Type A Dissection
Good operation
Addresses proximal complications of aortic insufficiency and ascending aortic rupture
Saves many lives in distressful times
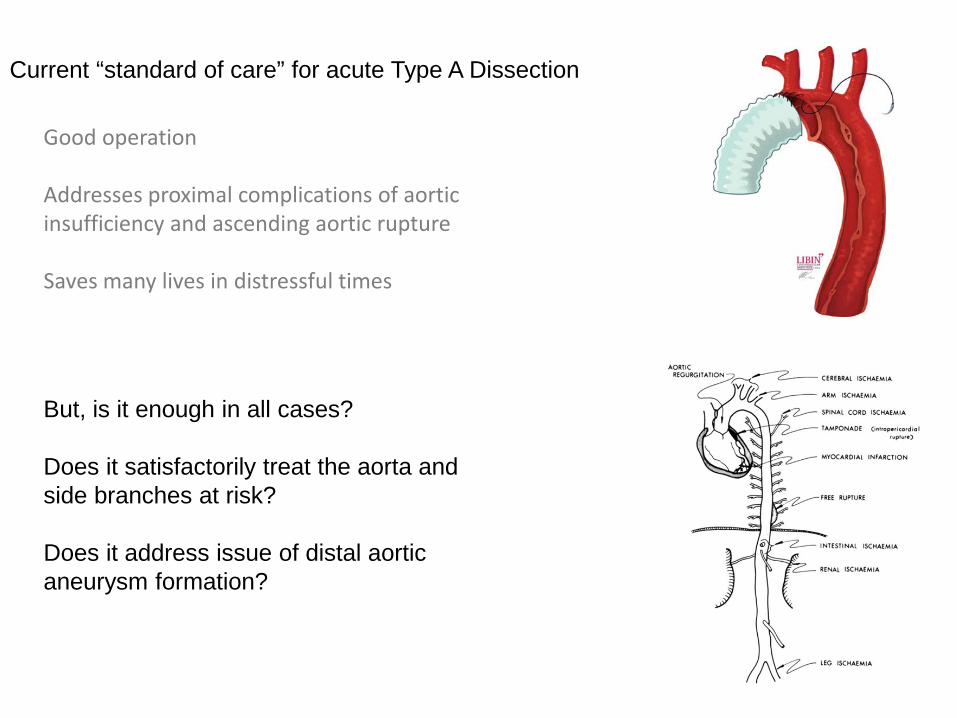
Conventional OperationCurrent “standard of care” for acute Type A Dissection
But, is it enough in all cases?
Does it satisfactorily treat the aorta and side branches at risk?
Does it address issue of distal aortic aneurysm formation?
Good operation
Addresses proximal complications of aortic insufficiency and ascending aortic rupture
Saves many lives in distressful times

Extended Arch operations for Acute Type A Aortic Dissectionincreases complexity of operation with high mortality ratefew centers world wide
Japan
China
Europe
USA
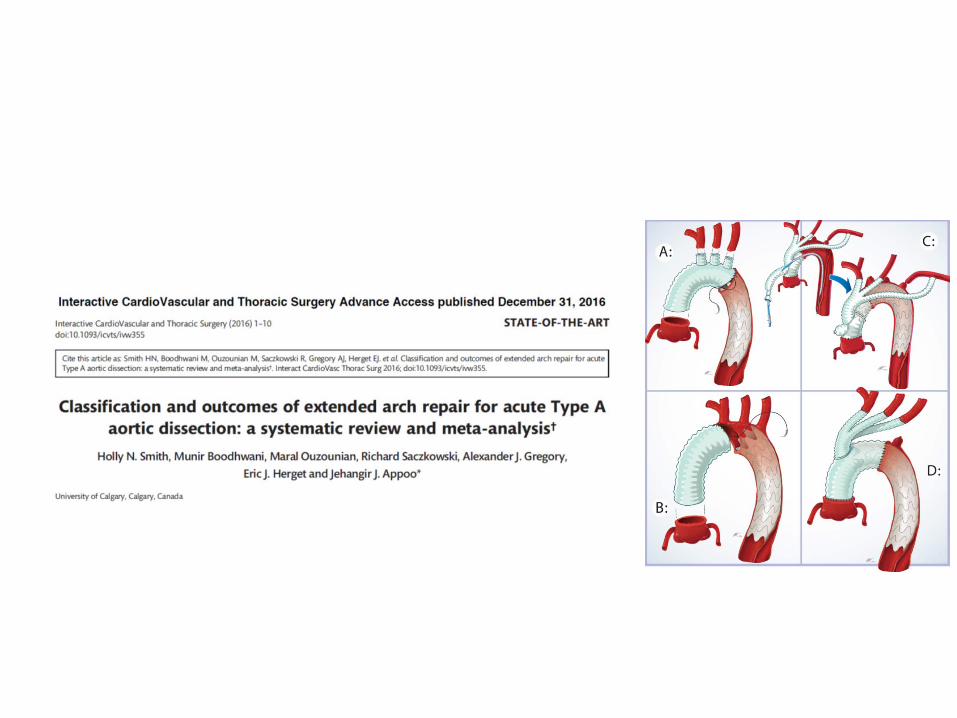
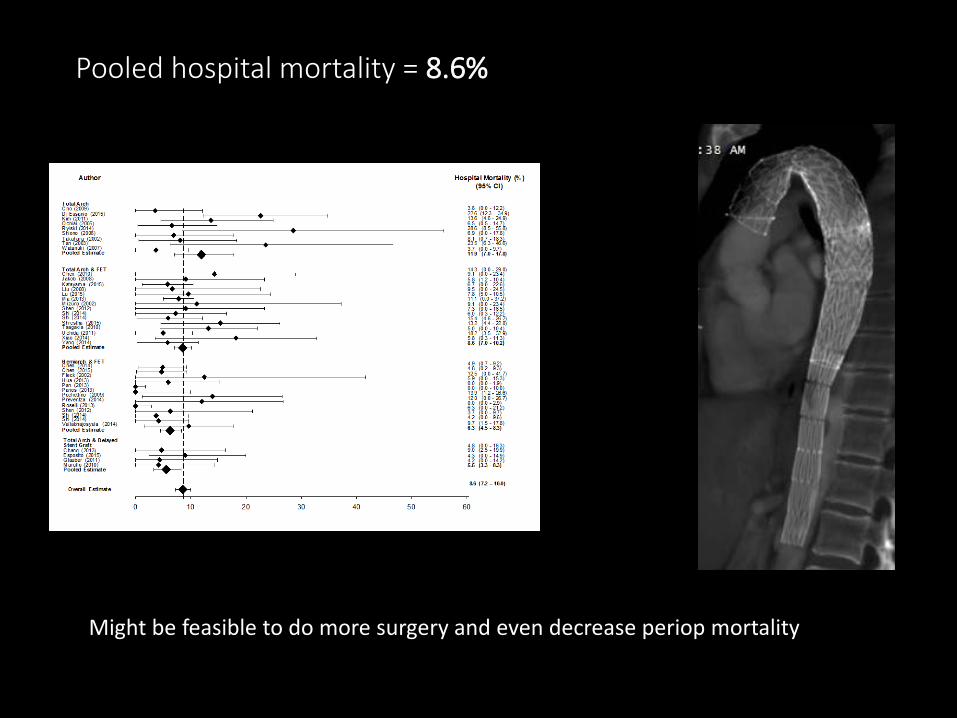
Pooled hospital mortality = 8.6%
Might be feasible to do more surgery and even decrease periop mortality



2018
Early Feasibility FDA Study: Acute Type A
5 sites in US enrolling
Technology is here….and future generations will improve on shortcomings...
Endovascular Treatment of Type A Aortic Dissections:
Evolution
Case reports and small case series published
For the right case, we are ready to try this in Calgary
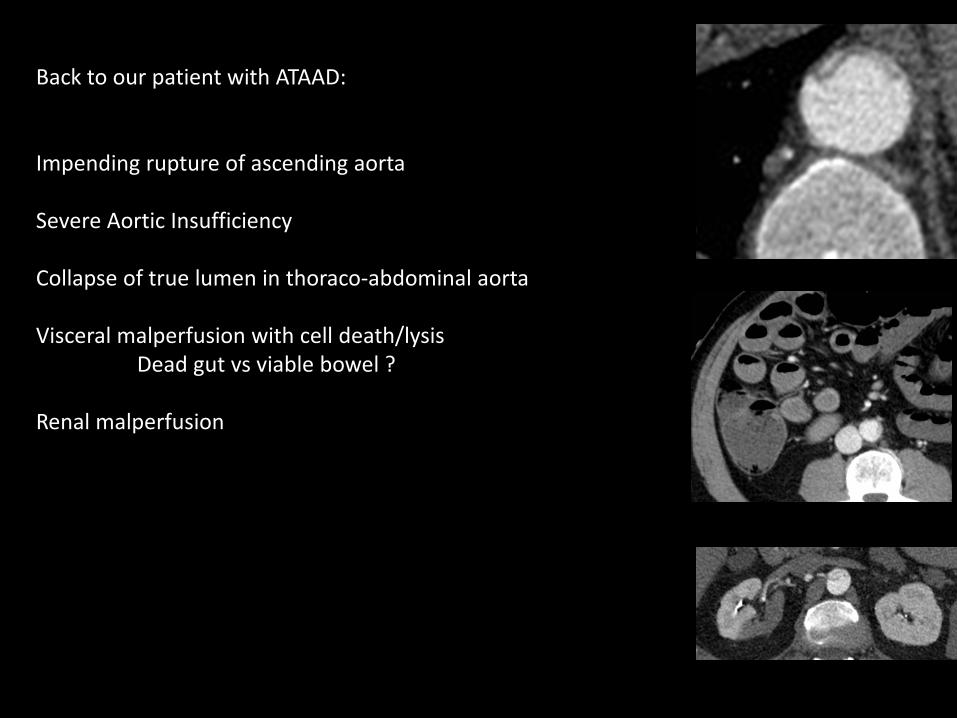
Back to our patient with ATAAD:
Impending rupture of ascending aorta
Severe Aortic Insufficiency
Collapse of true lumen in thoraco-abdominal aorta
Visceral malperfusion with cell death/lysis Dead gut vs viable bowel ?
Renal malperfusion
Surgical Strategy:
Pre op emergency Gen Surgery consultation re bowel viability and plan

Surgical Strategy:
Pre op emergency Gen Surgery consultation re bowel viability and plan
Rapid perfusion of bowel by accessing true lumen for cardiopulmonary bypass inflow prior to start of long operation
TL expansion but low flow due to small sizeBoth TL & FL cannulated and flows regulated based on TEE expansion of respective lumens
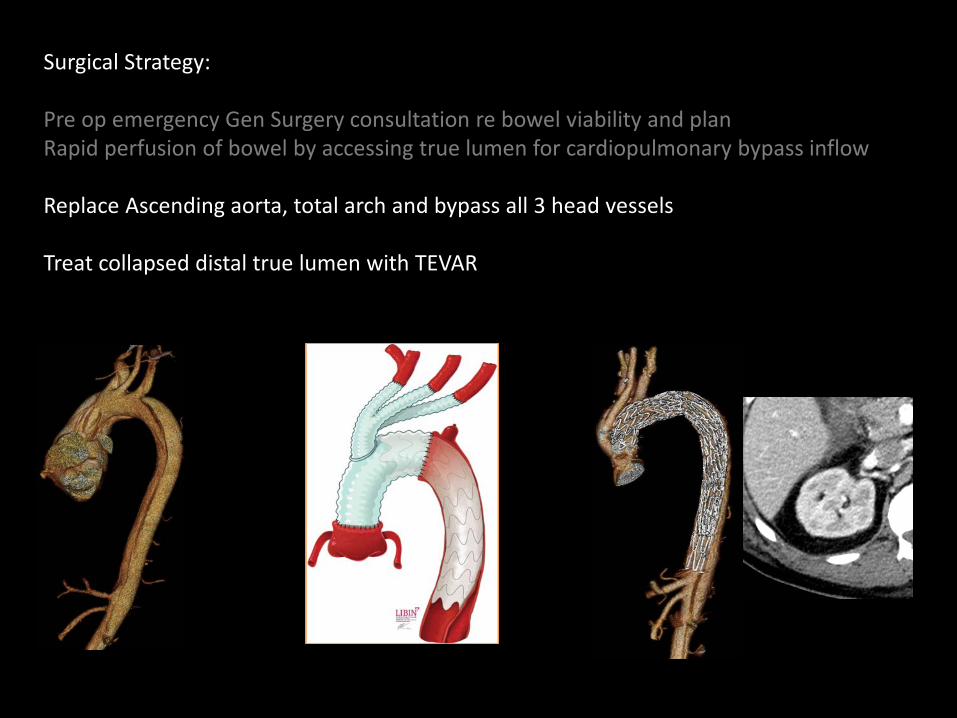
Surgical Strategy:
Pre op emergency Gen Surgery consultation re bowel viability and planRapid perfusion of bowel by accessing true lumen for cardiopulmonary bypass inflow
Replace Ascending aorta, total arch and bypass all 3 head vessels
Treat collapsed distal true lumen with TEVAR
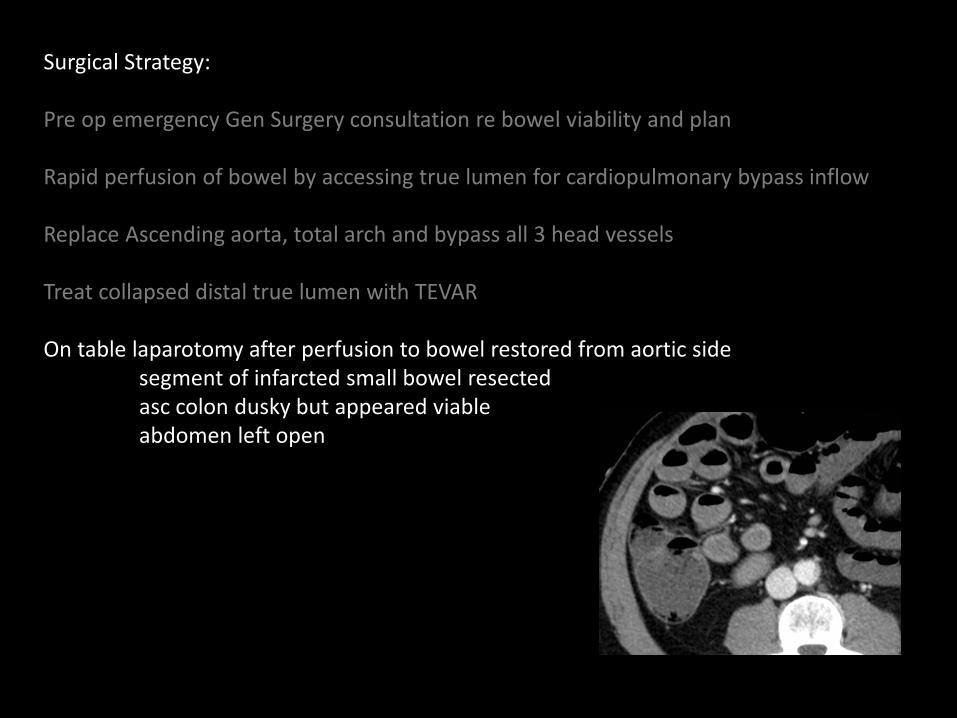
Surgical Strategy:
Pre op emergency Gen Surgery consultation re bowel viability and plan
Rapid perfusion of bowel by accessing true lumen for cardiopulmonary bypass inflow
Replace Ascending aorta, total arch and bypass all 3 head vessels
Treat collapsed distal true lumen with TEVAR
On table laparotomy after perfusion to bowel restored from aortic sidesegment of infarcted small bowel resectedasc colon dusky but appeared viableabdomen left open
Post op course:
Complications of ischemic gut GI bleedsStroke with hemiplegiaSepsisHITTIschemic strictures requiring laparotomy 3 months post op
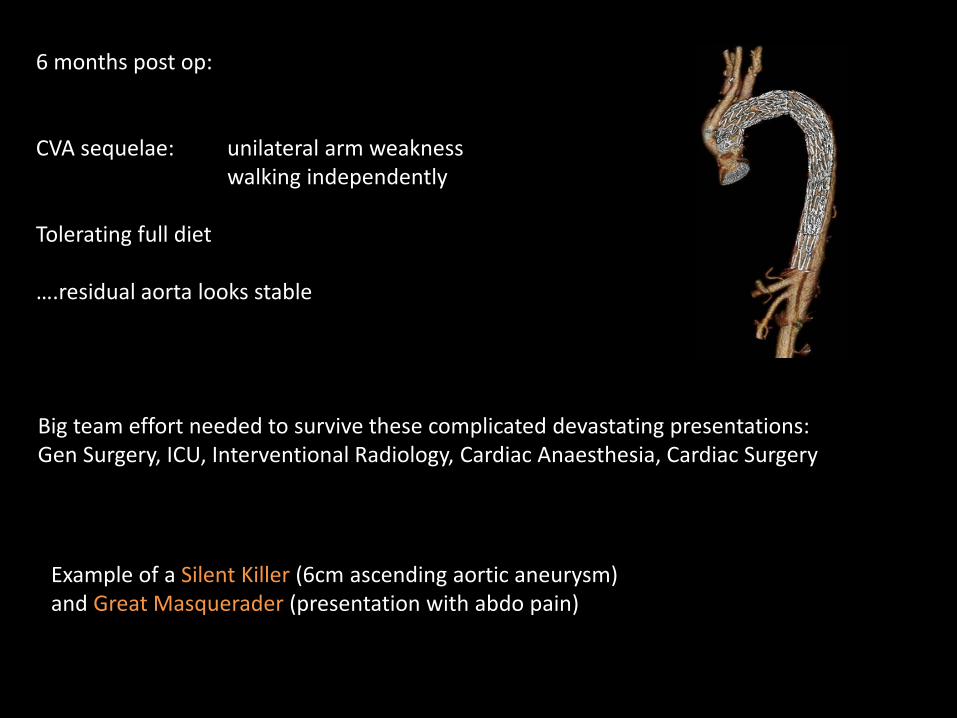
6 months post op:
CVA sequelae: unilateral arm weaknesswalking independently
Tolerating full diet
….residual aorta looks stable
Big team effort needed to survive these complicated devastating presentations: Gen Surgery, ICU, Interventional Radiology, Cardiac Anaesthesia, Cardiac Surgery
Example of a Silent Killer (6cm ascending aortic aneurysm) and Great Masquerader (presentation with abdo pain)
Share with you our research/evolution on:
I. Why/When do Aortas Dissect?II. Stroke Complication of Aortic DissectionIII. What type of operation should be performed ?
Why is Aorta challenging?
SILENT KILLER
LethalAneurysm disease top 20 causes of death of human beingsActual number likely underestimated
Asymptomatic95% are asymptomatic prior to catastrophic event
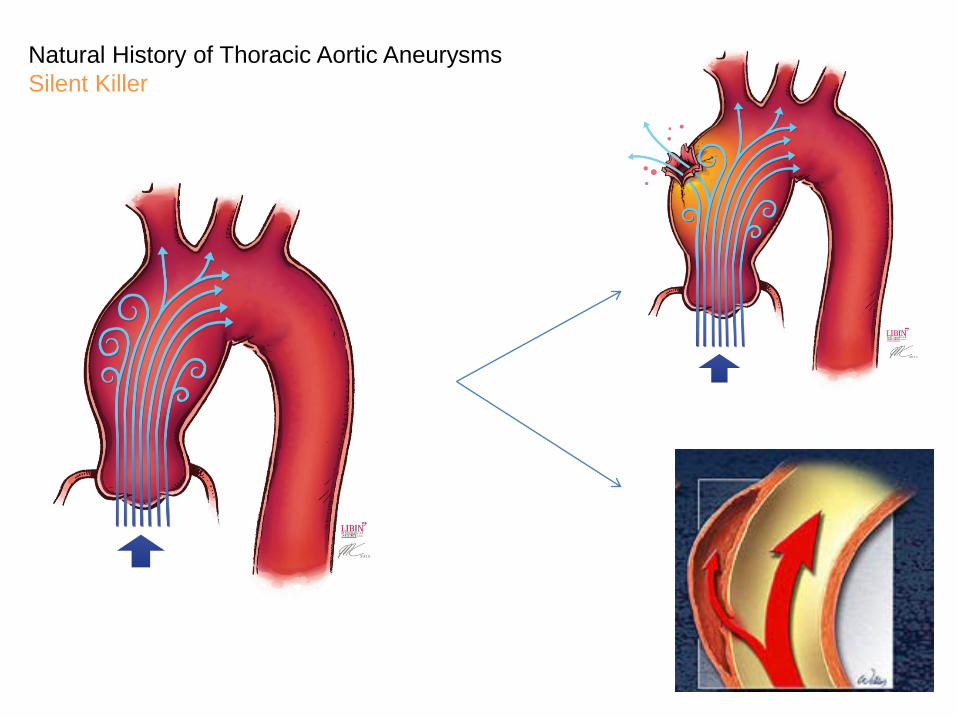
Natural History of Thoracic Aortic AneurysmsSilent Killer

Why understanding aortic behaviour is important?
Dilemma:
Young patients with small aneurysms can dissectvs.
Denominator is very large – many patients have large aortic aneurysms that are stable for prolonged periods of time
Intervention is invasive – has some risks
If we operated on every dilated aorta, we may do more harm than benefit

Summary of 2014-2016 ESC, AHA & CCC Guidelines for Prox Ao Intervention:
Asc Ao > 5.5cm
Asc Ao > 5.0cm with some risk factors (rate of growth, family history of dissection, hypertension, patient preference…)
Asc Ao 4.5 – 5.0cm for Connective Tissue Disease
Probably don’t need to be more aggressive if bicuspid valve

Summary of 2014-2016 Guidelines on Prox Aortic Intervention:
Level of scientific evidence is poor
no randomized data
no large non randomized studies
small, retrospective studies
consensus opinions
Lots of room for flexible interpretation including patient preference, aortic shape, rate of growth, patient size

How robust are the natural history data of Ascending Aortic Aneurysms?
Common Knowledge
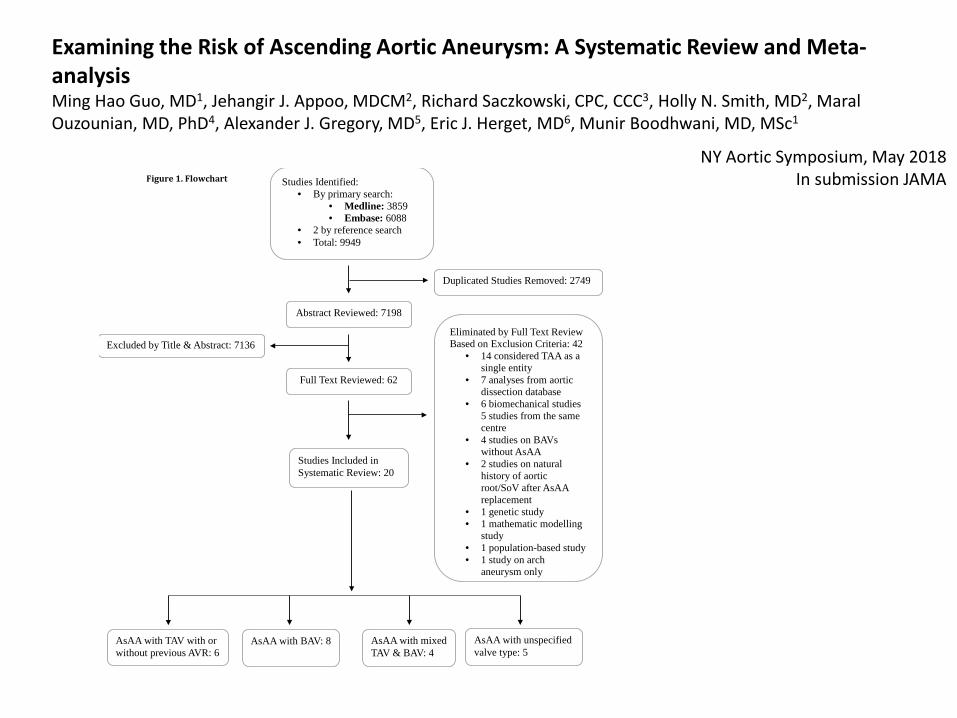
Figure 1. Flowchart
Studies Identified: • By primary search:
• Medline: 3859 • Embase: 6088
• 2 by reference search • Total: 9949
Abstract Reviewed: 7198
Duplicated Studies Removed: 2749
Excluded by Title & Abstract: 7136 Eliminated by Full Text Review Based on Exclusion Criteria: 42
• 14 considered TAA as a single entity
• 7 analyses from aortic dissection database
• 6 biomechanical studies 5 studies from the same centre
• 4 studies on BAVs without AsAA
• 2 studies on natural history of aortic root/SoV after AsAA replacement
• 1 genetic study • 1 mathematic modelling
study • 1 population-based study • 1 study on arch
aneurysm only
Studies Included in Systematic Review: 20
AsAA with TAV with or without previous AVR: 6
AsAA with BAV: 8 AsAA with unspecified valve type: 5
Full Text Reviewed: 62
AsAA with mixed TAV & BAV: 4
Examining the Risk of Ascending Aortic Aneurysm: A Systematic Review and Meta-analysisMing Hao Guo, MD1, Jehangir J. Appoo, MDCM2, Richard Saczkowski, CPC, CCC3, Holly N. Smith, MD2, Maral Ouzounian, MD, PhD4, Alexander J. Gregory, MD5, Eric J. Herget, MD6, Munir Boodhwani, MD, MSc1
NY Aortic Symposium, May 2018In submission JAMA

Linearized rate of dissection, rupture, or death:
Conclusions and Relevance: The growth rate of AsAA is slow and the risk of
dissection, rupture, and death may be lower than previously understood. A
randomized control trial may be required to understand the benefit of surgical
intervention compared to surveillance for patients with moderately dilated ascending
aorta.
Examining the Risk of Ascending Aortic Aneurysm: A Systematic Review and Meta-analysisMing Hao Guo, MD1, Jehangir J. Appoo, MDCM2, Richard Saczkowski, CPC, CCC3, Holly N. Smith, MD2, Maral Ouzounian, MD, PhD4, Alexander J. Gregory, MD5, Eric J. Herget, MD6, Munir Boodhwani, MD, MSc1
“Doctors are men who prescribe medicines of which they know little, to cure diseases of which they know less, in human beings of whom they know nothing” – Voltaire, 1694-1778
Is there a knowledge gap in understanding of ascending aortic aneurysm?
Do we as surgeons understand the NNT to save a life at one year?
What happens when endovascular repair of ascending aorta is feasible?
Anyone who isn’t confused doesn’t really understand the situation
Edward R. Morrow – TV News Anchor
On Research:
Sturgeon’s Law: “90% of everything is crap”
….so if you are going to critique/question, go after the good stuff or leave it alone
TITAN SvS: Treatment In Thoracic Aortic aNeurysm: Surgery vs. Surveillance
Multicentre Randomized Study of surgery vs surveillance for ascending aortic aneurysms 5.0-5.4cm
Munir Boodhwani, Ming Guo, Vamshi Kotha, Eric Herget, Alex Gregory, George Wells, Akash Fichadiya, & Jehangir Appoo
Libin Cardiovascular Insitiute, University of CalgaryEFW Radiology, University of Calgary
Ottawa Heart Institute, University of Ottawa

TITAN: SvSTreatment In Thoracic Aortic aNeurysm: Surgery vs. Surveillance
Primary Outcome:
Impact of Early Surgery vs. Surveillance strategy on all cause mortality and incidence of acute aortic syndrome at follow up

TITAN: SvSTreatment In Thoracic Aortic aNeurysm: Surgery vs. Surveillance
Secondary Outcomes:1. 30 day mortality of ascending aortic repair2. Incidence of elective ascending aortic surgery3. Incidence of CVA4. Annual ascending aortic growth rate 5. Quality of Life Assessment at 1 year and 3 years6. Non diameter related assessment of risk of acute aortic syndrome
1. Biobank of blood sample2. Biomedical Engineering Analysis
First trial to randomize ascending aortic aneurysms to surgery vs. medical therapy…evolution

TITAN: SvSTreatment In Thoracic Aortic aNeurysm: Surgery vs. Surveillance
Steps Accomplished 2016-2018
Raised Seed Funding $200,000Libin, Cumming School of Medicine, EFW, Ottawa Heart Institute
Ethics submitted in Ottawa & Calgary
Letter of Intent 12 Canadian sites
CIHR grant application $1M submitted March 2018

TITAN: SvSTreatment In Thoracic Aortic aNeurysm: Surgery vs. Surveillance
Next Steps:
Set up online database
Enroll first patients June 2018
Await result of CIHR grant application
Gradual roll out to all participating sites Fall 2018

Share with you our research/evolution on:
I. Why/When do Aortas Dissect? – TITAN SvSII. Stroke Complication of Aortic DissectionIII. What type of operation should be performed ?
Stroke and Aortic Dissection
Underappreciated problem
Cause ? Dissection extends to head vessels?Hypoperfusion during surgery?Emboli from surgical manipulation? Clot on dissection flap? Other?
Stroke and Aortic Dissection
Complicated problem
Needed expertise from other specialties
Formed a group including DI, Neuro Rads, Stroke Neurology, Anaesthesia & Surgery
Meta-analysis of the literature
Retrospective review of FMC cases
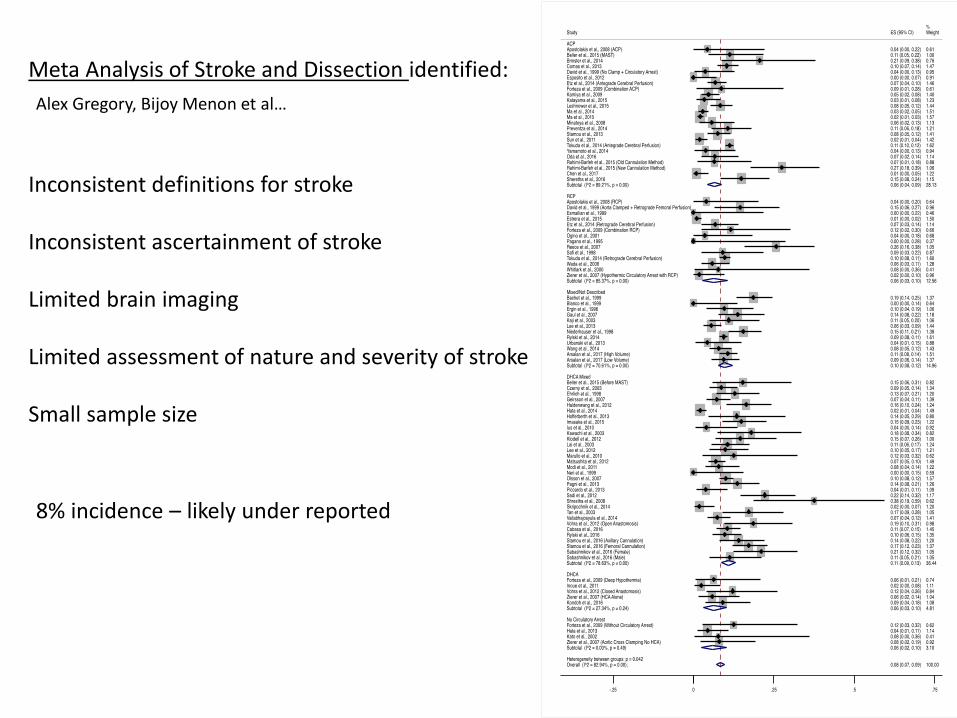
Meta Analysis of Stroke and Dissection identified:
Inconsistent definitions for stroke
Inconsistent ascertainment of stroke
Limited brain imaging
Limited assessment of nature and severity of stroke
Small sample size
8% incidence – likely under reported
Alex Gregory, Bijoy Menon et al…
Retrospective review of FMC Stroke and Ao Dissection :
38/189 (20%) incidence of stroke with Ao Dissection
87% had moderate stroke severity vs. only 5% with mild stroke92% had some neurological deficits at discharge10.5% died in hospital, 60% needed rehabilitationMortality at 30 days: 23.7%
=> Worked with DI & NeuroRads to change local protocol so that CTA H&N done at time of diagnosis of Aortic Dissection while patient still on CT table
Ericka Teleg, Bijoy Menon, Alex Gregory et al…
ASSIST : Aortic diSSection & stroke Imaging Study – Ericka Teleg et al.
Prospective study to identify mechanism of stroke in Aortic Dissection
Pre-operative neurovascular imaging in patients with ATAAD
Early post-operative imaging assessment of neuro-vasculature and physiology
Early detailed clinical neurological assessment of all patients with Aortic Dissection
Plan a prospective study nationally to address pending questions using a larger sample size
Share with you our research/evolution on:
I. Why/When do Aortas Dissect? => TITAN SvSII. Stroke Complication of Aortic Dissection =>ASSISTIII. What type of operation should be performed ?
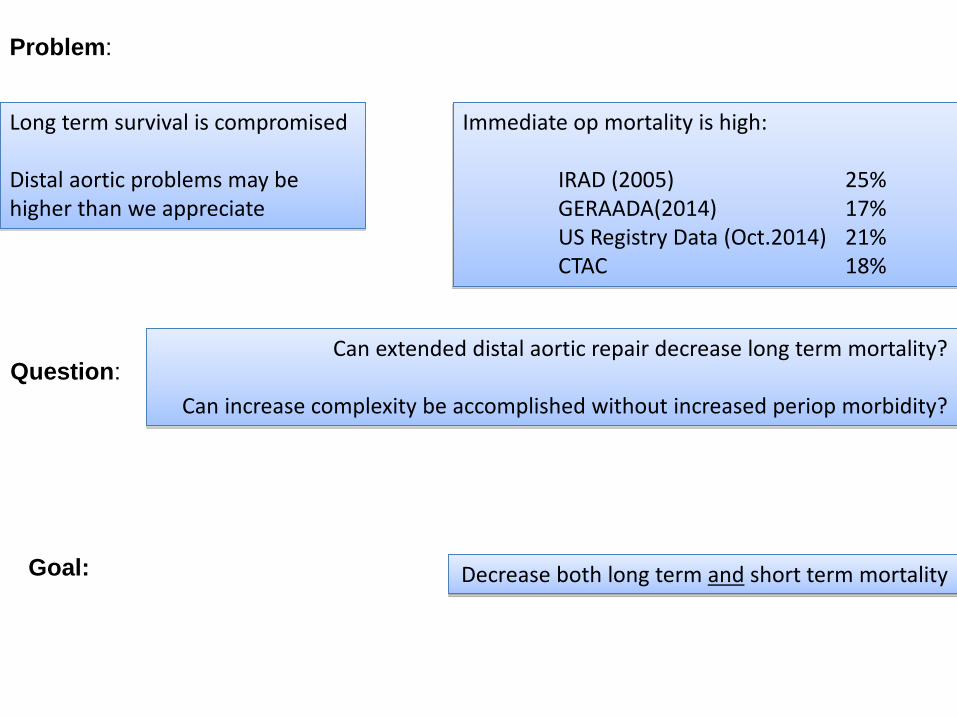
Problem:
Long term survival is compromised
Distal aortic problems may be higher than we appreciate
Immediate op mortality is high:
IRAD (2005) 25%GERAADA(2014) 17%US Registry Data (Oct.2014) 21%CTAC 18%
Question:Can extended distal aortic repair decrease long term mortality?
Can increase complexity be accomplished without increased periop morbidity?
Goal: Decrease both long term and short term mortality

HEMIARCH EXTENDED ARCH
P value
n 67 28
In-hospitalmortality
12% 7% 0.73
New post-op stroke 15% 21% 0.52
Permanent neurologic deficit
12% 7% 0.73
Calgary Experience 2011- 2015In submission

HEMIARCH EXTENDED ARCH
P value
Early prox FL obliteration 9% 58% <0.01
Mean prox aortic growth rate (mm/yr)
2.66 0.66 0.095
Redo thoracotomy 18% 0%
Calgary Experience 2011- 2015In submission
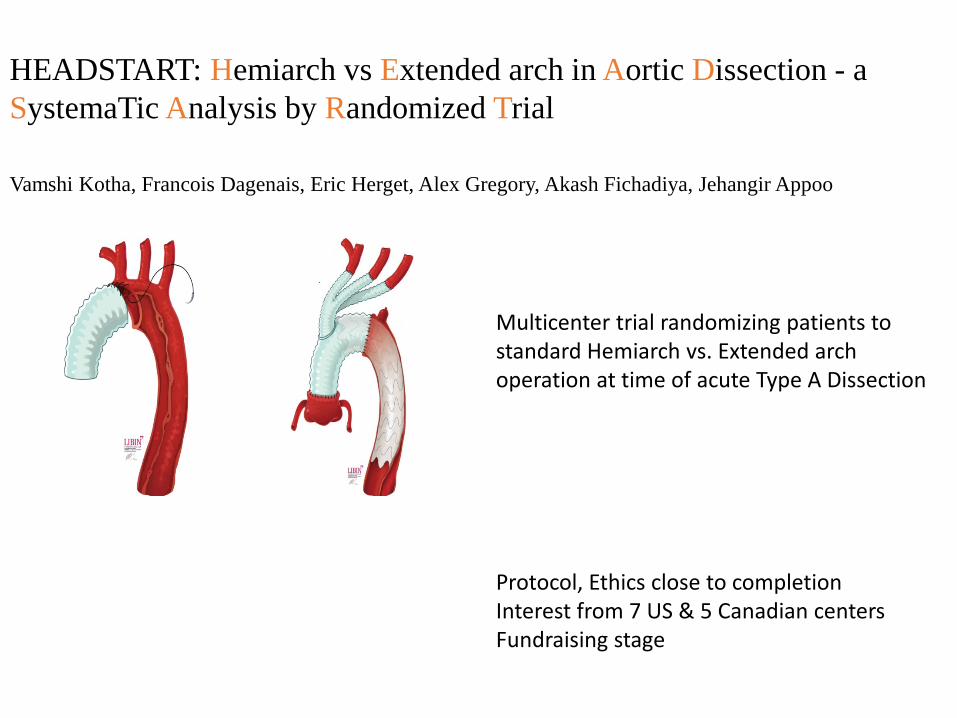
HEADSTART: Hemiarch vs Extended arch in Aortic Dissection - a SystemaTic Analysis by Randomized Trial
Vamshi Kotha, Francois Dagenais, Eric Herget, Alex Gregory, Akash Fichadiya, Jehangir Appoo
Multicenter trial randomizing patients to standard Hemiarch vs. Extended arch operation at time of acute Type A Dissection
Protocol, Ethics close to completionInterest from 7 US & 5 Canadian centersFundraising stage

For Trainees:
Lots of new Programs Developed
My definition of a “Program” in Medicine:
1. Clinical work – new therapies to take care of patients2. Education
i. Colleaguesii. Traineesiii. Referring physiciansiv. Patients
3. Innovation4. Research/Evolve
i. Start locallyii. Collaborate nationally/internationally
Summary
Aortic Aneurysms are Silent Killershigh index of suspicion required to track & identifyrisk of rupture/dissection process in evolution
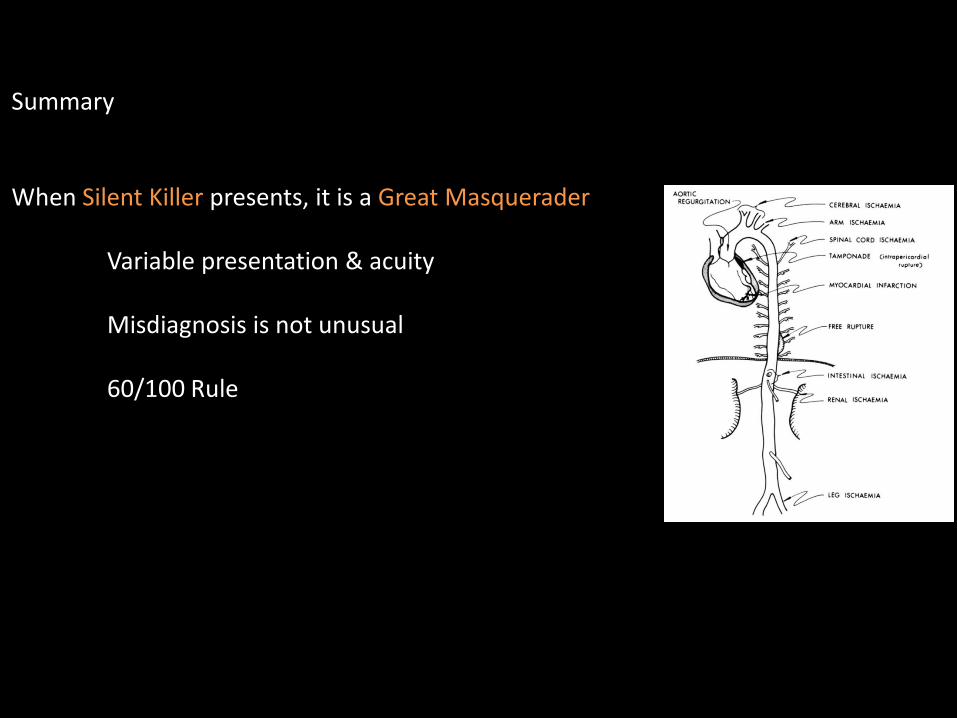
Summary
When Silent Killer presents, it is a Great Masquerader
Variable presentation & acuity
Misdiagnosis is not unusual
60/100 Rule
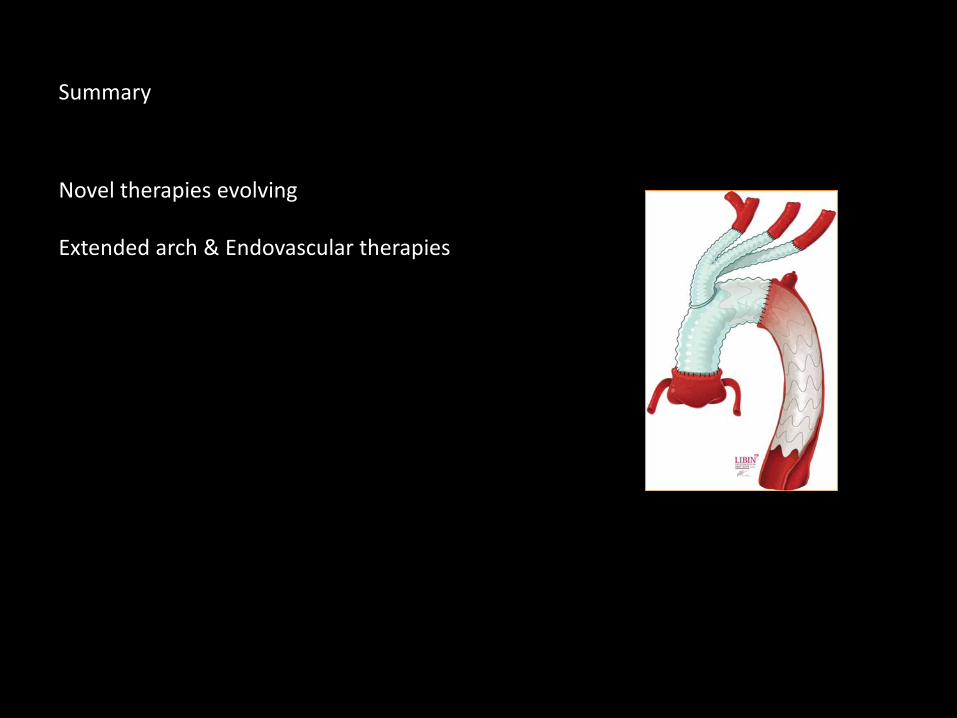
Summary
Novel therapies evolving
Extended arch & Endovascular therapies

Summary
Type B Aortic Dissection
topic for another time

It’s now clear to me that my purpose, your purpose and the purpose of everything else is to evolve and to contribute to evolution in some small way
Ray Dalio, Principles 2017
“Experience is what you got when you didn’t get what you wanted.”— Howard Marks
Evolution of Understanding and Therapy

Acknowledgements
“Life if too short to do business with people you don’t like”- Charlie Munger
www.aorta.ca
Aortic Program clinicalteachingresearchinnovation





























