Embed Size (px)
Citation preview

Two Little Water Cravers

Baby Mo (5mths/M)
• Chief complaint
• Repeated vomiting since 2 months old with poor weight gain
• PMH
• Gestation 40+6wks, BW 3.375kg
• Hx of fracture Rt clavicle at birth
• HbH disease – on folic supplement
• Vaccine up to date
• NKDA
• No developmental concern

HPI
• Repeated vomiting since birth ~2-3x/day • Moderate amount of undigested milk soon after feeding
• Non projectile, no bile stained
• On AF 5oz/feed, 5x/day
• Irritable, crying for milk
• Large amount of urine output ~ 7-8x/day
• BO 1x/day, YSS
• Failure to thrive • BW 50% at 1mth
• BW 25% at 2mths
• BW 0.6kg below 3% at 5mths

HPI
• No recurrent febrile episodes
• No coryzal symptoms
• No urinary symptoms
• TOCC: lives in Mainland China
• Attended Hospital in China
• USG brain unremarkable
• Abnormal thyroid function test

Physical Exam
• Afebrile
• P 158/min; SpO2 100% in RA
• AFNT
• No dysmorphism
• CR<2s, warm peripheries but dry oral mucosa
• Chest no distress, clear, AE adequate
• HS normal, no murmur
• Abd not distended, no hepatosplenomegaly, BS +ve
• Generalized hypotonia with head lag
• Spont movement of 4 limbs, reflexes normal and symmetrical

Investigations on Admission
• Hb 8.7g/dL (hypochromic microcytic)
• WBC, Plt normal
• Glucose normal
• VBG no aciodsis
• LFT normal
• RFT
• Na 167 mmol/L
• K 4.4 mmol/L
• Urea 7.8mmol/L
• Cr 32 umol/L

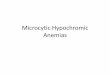
Hypernatremia in Children
• Na >145mmol/L
Dehydration
FENa <1%
Uosm > Posm
Extrarenal losses
Diarrhea
Skin loss
Excessive sweat
Fasting / thirst
FENa >1%
Uosm>= Posm
Osmotic Diuresis
Diuretics
Glycosuria
Post-obstructive diuresis
Non-oliguric ATN
FENa <1%
Uosm < Posm
Urine Concentrating Defect
Central DI
Nephrogenic DI

Hypernatremia in Children
Not dehydrated
FENa>1%
Uosm > Posm
Excess sodium
Increase renal solute load
Salt poisoning
FENa variable
Uosm < Posm
Central hypodipsia

Management of Baby Mo • Treat as hypernatremic dehydration
• NS bolus 10ml/kg
• ½ NS D5 solution (as maintenance + deficit replacement)
• However
• Na 171 mmol/L 174 mmol/L 177mmol/L
• K normal
• Urea 7.3mmol/L 6.4mmol/L 4.7mmol/L
• Cr 31umol/L 25umol/L 19 umol/L
• Urine ~10ml/kg/hr
• Switched IVF
• Maintenance: D5 :1/4 NS
• Urine ml to ml replacement with D5
• Gradual normalization of Na level to 155mmol/L

Polyuria

Back to Baby Mo

Further Investigations
• FENa 0.33% (hypovolemia)
• Plasma osmolality – 336mOsm/kg (H)
• Urine osmolality – 171mOsm/kg (L)
• Plasma ADH level: 30.7pg/mL (N: 1.0-13.3pg/mL)
• Water deprivation test given DDAVP (0.4mcg then 0.6mcg)
• Persistent high volume PU
• Urine osmol ~120mOsm/kg

Further Investigations
• Morning cortisol 307 (N)
• ACTH 4.4 (N)
• Low dose synacthen test: adequate cortisol response
• Growth hormone 1.9 (N)
• subclinical primary hypothyroidism:
• TSH 13.7 (H) fT4 18.1 (normal)
• Anti –TG <20 (N); anti TPO 98 (mildly raised)
• Thyroid scan: bilateral thyroid lobes uptakes present
• Urgent CT brain: NAD

Nephrogenic Diabetes Insipidus

Genetic Study
• Heterozygous AQP2 NM_000486. 5:c. 3G>T p. (Met1?)
• Heterozygous AQP2 NM_000486. 5:c 140C>T p. (Arg47Val)
• Both pathogenic
• AVPR 2 normal
• Conclusion: AQP2 related nephrogenic diabetes insipidus

Management
• Allow adequate fluid intake both day and night
• Nocturnal milk drip
• Fluid offered at 2 hourly intervals
• Management of GERD
• Nexium
• Gastrostomy feeding
• Low threshold for admission and intravenous hydration
• IV fluid hypotonic to urine
• 5% dextrose or 1/5 NS solution
• Close monitoring of body weight / fluid balance / biochemistries

Management of Hypernatremic Dehydration • Maintenance + Replacement of Loss
• Water + Sodium
• Replace over 48hrs
• Rate of correction of hypernatremia not to exceed 0.5mmol/L per hour
• Free water deficit
• (Measured Na x total body water) / (Desired Na) – (Total body water)
•

Example of Calculation
Maintenance Replacement of Loss Total Requirement
Water 100ml x 5.5 x 2 = 1100ml
Water 5.5 x 10% x 1000= 550ml (free water deficit = 455ml) (95ml loss as isotonic solution)
Water = 1100ml + 550ml = 1650ml
Sodium 3mmol/L x 5.5 x 2 = 33mmol/L
Sodium loss 154 /1000x ( 550-455) = 14mmol/L
Sodium = 33+ 14mmol/L = 47mmol/L
Body weight: 5 kg Estimated Dehydration: 10% Premorbid body weight: 5.5kg Plasma Na: 165mmol/L To correct over 48hrs
47mmol of Na in 1650ml to be given over 48hrs ie. 1/5 NS solution at 34ml/hr

Management
• Osmotic load reduction
• Consult dietician x renal solute load ~15mOsm/kg per day
• Diuretics
• Hydrochlorothiazide + amiloride (potassium sparing)
• Prostaglandin synthesis inhibitors
• Indomethacin
• Developmental Training

Renal Solute Load
• Osmotically active substances in diet
• Protein (1 gram protein yields 4 mmol Urea)
• Sodium
• Potassium
• Anions accompanying Na and K
• Renal solute load of diet = 2x (Na + K) + Protein(g) x 4
• Optimal: <15mOsm/kg/day
• Fluid (ml) required to excrete the load: 15mOsm x kg / urine osmol x 1000
• (i.e. a child with urine osmolality of 100mOsm need fluid intake of 150ml/kg/day to excrete that load)
• Carbohydrate and lipid will NOT increase osmotic load
• Metabolized without byproducts requiring renal excretion

Diuretics • Thiazides
• Inhibit reabsorption of sodium and chloride in distal convoluted tubule
• Induce mild volume depletion and thus up regulation of proximal tubular reabsorption of salt and water
• Less volume delivered to colkecting duct and lost in urine
• Hydrochlorothiazide 1mg/kg/dose BD dose
• Amiloride
• Potassium sparing effect (K supplement increase osmotic load)
• 0.1-0.3mg/kg/day

Prostaglandin Synthesis Inhibitor
• Indomethacin
• Partial chemical nephrectomy to reduce GFR
• 1-3mg/kg/day in 3-4 divided doses
• S/E: deterioration of renal function / hematological / GI upset

Progress • Catch up growth and development