Slide 1
Received: 25 October 2013/Accepted: 27 December 2013/Published
online: 5 January 2014 Springer Science+Business Media New York
2014AbstractTriple-negative breast cancer (TNBC) is
anKeywordsTriple negative Breast Future Diagnosis aggressive
subtype comprising about 1020 % of breastcancer patients with an
overall poor prognosis. Recently, itwas found to be a heterogeneous
disease that has beenclassied into six subtypes based on molecular
signature.In preclinical trials, these subtypes have different
activesignaling pathways with variable response to chemother-apy.
To improve treatment outcome of TNBC, therapyshould be tailored
according to the active driving signalingaberration. Molecular
testing represents the optimal way tostratify patients, but it has
some difculties to be imple-mented in routine clinical practice.
This article provides anassumption for stepped diagnostic algorithm
of TNBCbased on immunohistochemistry markers in addition to
asuggested tailored therapeutic strategy for advanced TNBCbased on
the driving aberrations. Furthermore, most TNBCpatients develop
early relapse despite adjuvant chemo-therapy. We provide a design
for future adjuvant therapyfor the disease. This design is based on
targeting proposedactive pathways in breast cancer stem cells
responsible forregenerating the tumor and disease relapse. Finally,
weprovide a proposed design for future clinical trials inTNBC to
allow for investigation of different medications inthis
heterogeneous disease based on upfront patient strati-cation and
then allocation to the suitable treatment arms.
S. Elsamany (&) S. AbdullahMedical Oncology Department,
Oncology Centre, KingAbdullah Medical City, 2677 Al-Mashaeer
District,Makkah 57657, Saudi Arabiae-mail:
[email protected]
S. ElsamanyMedical Oncology, Mansoura University, Mansoura,
EgyptManagement
Introduction
Triple-negative breast cancer (TNBC) constitutes approxi-mately
1020 % of breast cancer patients and represents anaggressive
subtype with poor overall prognosis [1]. TNBCpatients have a higher
rate of early recurrence and
distantmetastasistobrainandlungscomparedtootherbreastcancersubtypes
[1]. Chemotherapy is the only systemic therapycurrently available
for TNBC; however, most patients withTNBC relapse within 12 years
and\30 % of patients sur-vive 5 years despite adjuvant chemotherapy
[2].Despite initial high response rate to chemotherapy in
themetastatic setting, TNBC patients develop rapid
diseaseprogression resulting in a shorter overall survival
comparedto ER? breast cancer [3].The treatment options for TNBC
after chemotherapyfailure are limited. Overall, treatment of
patients withTNBC has been challenging due to the heterogeneity of
thedisease and the absence of well-dened molecular targets[4].
Although several small molecule inhibitors andmonoclonal antibodies
have been tested in clinical trials inunselected TNBC patients,
none has entered clinicalpractice due to limited efcacy [4]. Given
so, improvingtherapeutic outcome of TNBC patients requires
betterunderstanding of its molecular basis to identify
moleculardrivers that can be therapeutically targeted [5].In this
article, we will review recent data about themolecular basis of
TNBC, with a particular emphasis onpotential targets of novel
therapies. In addition, we willprovide assumptions of future
diagnostic and therapeuticapproaches of this disease.
123Med Oncol (2014) 31:834DOI 10.1007/s12032-013-0834-y
REVIEW ARTICLE
Triple-negative breast cancer: future prospects in diagnosisand
management
Shereef Elsamany Sakher Abdullahchemotherapy [5]. However, data
from ER-positive breastcancer revealed that single-agent PI3K
inhibition leads tofeedback activation of ER pathway, while
combined inhi-bition of both PI3K and ER may be more effective
thaninhibition of either pathway alone [9]. This displays thevalue
of combining PI3K inhibitors with other agents tooptimize
therapeutic efcacy.
Promising synergism of PARP inhibitors and PI3Kinhibitors
Several PARP inhibitors are being tested in clinical trialssuch
as olaparib (AZD2281), which has been shown to besafe and effective
in BRCA-related cancers. Meanwhile, thebenet of iniparib in phase
II trial was not conrmed in thesubsequent phase III trial
[10].Emerging preclinical data demonstrates synergisticactivity
when PARP inhibitors are combined with PI3Kinhibitors in cell lines
with active PI3K pathway [11].PARP enzymatic activity is necessary
for the repair ofsingle-strand breaks (SSBs) through the base
excisionrepair (BER) pathway, while BRCA1 and BRCA2 proteinsare
essential components for repair of the double-strandbreaks (DSBs)
through homologous recombination (HR)[12]. When PARP is inhibited,
unrepaired SSBs can betransformed to DSBs that, in BRCA-decient
cells, can nolonger be repaired by HR, resulting in lethal DNA
damage[13].PI3K pathway is required to maintain and
stabilizeBRCA1/2 protein levels. In this way, PI3K
inhibitionimpairs BRCA1/2 protein levels, which sensitizes
BRCA-procient TNBC to PARP inhibition as demonstrated incell lines
and animal models [11]. In addition, in an animalmodel of
BRCA1-decient breast cancer, combined ther-apy of the PARP
inhibitor olaparib with the PI3K inhibitorNVP-BKM120 caused a
14-fold delay in tumor growthcompared with therapy with either
agent alone [14].
Recent view of androgen receptor-positive TNBC
The luminal androgen receptor (LAR) subtype was iden-tied in 11
% of TNBC by gene analysis as reported byLehmann et al [5];
however, androgen receptor (AR) wasfound to be expressed in
one-third of TNBC via immu-nohistochemistry [15]. This subtype
showed enhancedsteroid hormone signaling and androgen receptor
mRNAwas detected at an average of ninefold higher than otherTNBC
subtypes [16]. Interestingly, LAR subtype belongsto either luminal
A or luminal B intrinsic subtype despitebeing negative for ER
expression [16].This subtype showed high response rate to
anti-andro-gens in preclinical trials [5]. Furthermore, the
anti-Subtype
Basal-like 1
Basal-like 2
Immunomodulatory
Mesenchymal
Mesenchymal stemlike
Luminal androgenreceptorGene expression prole
High expression of genes involved in cell cycleprogression, cell
division and DNA damageresponse pathwaysHigh expression of genes
involved in cell cycleprogression, cell division and growth
factorsignalingHigh expression of genes involved in
immuneprocessesHigh expression of genes involved in motilityand
extracellular matrixHigh expression of genes involved in
motility,extracellular matrix and growth factorsignalingHigh
expression of genes involved inhormonally regulated pathways834
Page 2 of 7
Table 1 Subtypes of TNBC based on gene expression prolingMed
Oncol (2014) 31:834
have enhanced response to PI3K inhibitors compared toMolecular
classication of TNBC
TNBC has been recently classied into six subtypes on thebasis of
gene analysis (Table 1) [5]. These subtypes haveprognostic
signicance with the basal-like subtypes havingthe worst clinical
outcome [4].
Basal-like subtypes
Basal-like 1 (BL-1) and basal-like 2 (BL-2) are the mostfrequent
TNBC subtypes (47 %) [5]. They are character-ized by high
proliferation rate with an average Ki-67staining of 70 % in
addition to high expression of genesinvolved in cell cycle and cell
division [5]. They have highsensitivity to chemotherapy, especially
the antimitoticagents as demonstrated by high rate of pathological
com-plete response (pCR) with neoadjuvant taxan-based che-motherapy
(63 % in BL-1 and BL-2 subtypes compared to1431 % in other TNBC
subtypes) [6].Interestingly, the majority of studies evaluating
neoad-juvant chemotherapy have identied high Ki-67 level as
apredictive factor of pCR [7]. In the study of Fasching et al.[7]
involving TNBC patients, pCR was 57 % in patientswith Ki-67 [35 %
compared to 4 % in those with Ki-67\35 %. Interestingly, Adamo and
Anders [8] suggestedthat TNBC patients can be divided into two
subgroups withdifferential response and prognosis after
preoperativechemotherapy based on Ki-67 level.
Mesenchymal and mesenchymal stem-like subtypes
Mesenchymal (M) and mesenchymal stem-like (MSL)subtypes have low
level of proliferation, but they areenriched with
phosphatidylinositol-3-kinase (PI3K) andWnt pathways activity. In
preclinical trials, these subtypes
123
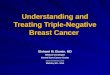
Fig. 1 Wnt/b-catenin signaling in TNBC. a In the absence of
Wntbinding to LRP5/6 and FZD, APC binds to axin and GSK3.
Thiscomplex promotes phosphorylation of b-catenin via CK1.
Phosphor-ylated b-catenin is then degraded by proteasome system. b
Wntproteins bind to LRP5/6 and FZD forming a complex that
prevents
androgen bicalutamide is currently being evaluated in aphase II
study in AR-positive ER-/PR-negative metastaticbreast cancer
patients [15].Meanwhile, PI3K pathway activation is involved in
theresistance to anti-androgens as demonstrated in animalmodels of
AR-positive TNBC treated with bicalutamide[17]. In addition,
synergistic activity between PI3K inhib-itors and anti-androgens
has been shown in cell lines andexperimental animals [17]. These
preclinical data providethe rationale for future clinical trials,
evaluating the com-bination of AR antagonists with PI3K inhibitors
in AR-positive TNBC patients.
Wnt/b-catenin pathway in TNBC
Wnt/b-catenin signaling pathway is preferentially activatedin
TNBC [18], especially in BL2 and mesenchymal sub-types [5]. Wnt
proteins bind to the lipoprotein receptor-related protein 5/6
(LRP5/6) and frizzled (FZD) trans-membrane receptor proteins, to
form a complex thatMed Oncol (2014) 31:834Page 3 of 7 834axin, CK1
and GSK3 from inducing b-catenin degradation. Free b-catenin is
translocated to the nucleus to bind with TCF transcriptionfactor.
The TCFb-catenin complex activates Wnt target genes. APCadenomatous
polyposis coli, GSK3 glycogen synthase kinase-3, CK1casein
kinase-1
prevents b-catenin degradation, which allows its translo-cation
to the nucleus to enhance cell proliferation [18](Fig.
1).Dysfunction of the Wnt ligands at the cell surface leadsto
aberrant activation of Wnt/b-catenin signaling thatdrives breast
carcinogenesis [19]. Among the 10 FZDproteins, FZD7, overexpressed
in 67 % of TNBC, is likelythe most important one involved in breast
cancer tumori-genesis [19]. Furthermore, downregulation of FZD7
orLRP5/6 suppressed cell growth and tumor transformationin TNBC
cell lines [20].Porcupine is an acyltransferase enzyme required for
thefunction and secretion of Wnt ligands. The porcupineinhibitor
LGK974 is a Wnt inhibitor under development forthe treatment of
cancers driven by the Wnt pathway in aWnt ligand-dependent manner
[21]. In preclinical evalua-tion, LGK974 attenuated tumor growth
and induced tumorregression as a single agent as well as in
combination withpaclitaxel in a human primary breast cancer model
[22].LGK974 is currently evaluated in a phase I trial in
patientswith advanced malignancies, including malignant
123
about possible combinations of Wnt, CAV1 and S6K positivities.
*3Chemotherapy may be considered given that no other options
forthose patients
these genes are either targets for dasatinib or substrates
forSrc kinases. Interestingly, expression of these genes
wasparticularlyobservedinTNBCcelllines [26].Finnetal[24]also
reported an association between CAV1 (Caveolin 1)mRNA expression
and sensitivity to dasatinib. Similarly,Tryfonopoulos et al [25]
detected an association betweendasatinib sensitivity and high
protein level of CAV1.Despite promising activity in TNBC cell
lines, the Srcinhibitor dasatinib had disappointing results in
clinicalstudies involving unselected TNBC patients. In a phase
IItrial including patients with advanced TNBC, dasatinibdisplayed
modest activity (5 % partial response, 10 %disease control) [4].
So, proper use of Src inhibitors inTNBC requires selecting patients
who are more likely tobenet from this therapy.
Tailored therapy for advanced TNBC
Evidence from preclinical trials illustrates that there
isdifferential response to therapeutic agents in TNBC834 Page 4 of
7Med Oncol (2014) 31:834Fig. 2 Proposed future tailored treatment
algorithm of advancedTNBC. PI3KI, PI3K inhibitor; PARPI, PARP
inhibitor. *1 No dataabout possible simultaneous Wnt?ve/CAV?ve
disease. *2 No data
melanoma, pancreatic cancer and TNBC
(www.clinicaltrials.gov).
New insights on Src pathway in TNBC
Src is a non-receptor tyrosine kinase involved in celladhesion
and motility [23]. Preclinical studies in breastcancer cell lines
displayed that compared to other subtypes,TNBC is uniquely
sensitive to growth inhibition by the Srcinhibitor, dasatinib, and
synergistic activity with chemo-therapy has been shown in TNBC cell
lines [24, 25]. Themesenchymal-like subtypes, being enriched in
cell motilitygenes, are the most common subtypes with high
Srcactivity and were found to be more sensitive to Srcinhibitors in
preclinical trials [4].Src expression is more frequent in TNBC;
however, thelevel of Src expression is not predictive of dasatinib
sensi-tivity [25]. Huang et al [26] identied a six-gene panel
thatcould predict sensitivity to dasatinib. These genes
includedEPHA2, CAV1, CAV2, ANXA1, PTRF and IGFBP2. All
123
subtypes depending on the active signaling pathway
[5].Currently, many trials in TNBC are ongoing (clinical
tri-als.gov), but unfortunately, most of these trials
involveunselected patients and are not directed by
predictivebiomarkers, which make their success, in a
heterogeneousdisease with different driving molecular pathways,
extre-mely doubtful.In view of this, TNBC can be considered an
excellentexample of the value of tailored therapy. A more
logicapproach should consider upfront stratication of TNBCpatients
based on genetic or surrogate immunohistochem-istry (IHC)
biomarkers that reect various subtypes anddriving pathways to allow
treatment to be personalizedaccording to the intrinsic tumor
signature. Ideally,stratifying patients based on genetic testing
represents theoptimal approach, but the cost, complexity and
requirementof facilities and trained personnel for genetic testing
maymake classifying patients based on IHC surrogate markersa more
attractive practical approach.The following is a suggested stepped
testing algorithmfor advanced TNBC patients that may allow for
propertreatment selection.1.Testing for Ki-67, CAV1 and Wnt
proteins expressionvia IHC:Fig. 4 Proposed design forfuture
clinical trials in TNBCMed Oncol (2014) 31:834
Fig. 3 Proposed futureadjuvant therapy of TNBC.PI3KI, PI3K
inhibitor; PARPI,PARP inhibitorPage 5 of 7 834Testing for Wnt
pathway proteins: FZD7 and LRP5/6 are selected being the most
commonly overex-pressed in TNBC.
123Testing for CAV1 protein level: as a marker ofdasatinib
sensitivity.2.In Ki-67\35 %: testing for AR and PI3K activity:AR
testing: via IHC.PI3K testing: through IHC testing for S6
kinase(S6K), the downstream signaling protein of PI3Kpathway, as a
surrogate marker [27].It is to be noted that Ki-67[35 % is selected
as surro-gate marker for BL1 and BL2 subtypes based on averageKi-67
of 70 % in these subtypes [5] and high response rateto chemotherapy
in patients with Ki-67[35 % [7]. Testingfor AR and PI3K activity is
suggested to be reserved forpatients with Ki-67\35 % given the low
proliferation ratein LAR and mesenchymal-like subtypes.Next, based
on the above panel of predictive markers,the following diagram
illustrates proposed future tailoredtreatment algorithm for
advanced TNBC (Fig. 2).
Proposed design for future adjuvant therapy
As stated above, most patients with TNBC relapse within12 years
despite adjuvant chemotherapy [2], whichhighlights the need for
additional therapy in early stageTNBC to prevent rapid relapse.
According to cancer stemcells (CSCs) theory, these cells are
intrinsically resistant tochemotherapy and could later regenerate
the tumorresulting in relapse [28]. Therefore, drugs that inhibit
keyactive pathways in CSCs, such as PI3K and Wnt pathways,may
suppress their tumor initiating property, which mayrepresent
promising therapeutic strategies in the adjuvantsetting of TNBC
[29].Constitutive activation of the Wnt/b-catenin signalingpathway
is essential for maintenance, clonogenicity ofCSCs and, most
importantly, Wnt/b-catenin signalingconfers resistance of CSCs to
radiation and chemotherapy[30]. Noteworthy, Wnt pathway inhibition
can controlCSCs. For example, salinomycin, through induction ofLRP6
degradation, was found to be a selective breast CSCsinhibitor [30].
This suggests that targeting Wnt/b-cateninpathway can control
breast CSCs which may optimize thetherapy of TNBC
[31].PI3K/Akt/mTOR signaling pathway is critical for CSCBased on
the above, the following therapeutic strategy issuggested for early
stage TNBC after nishing adjuvantchemotherapy (Fig. 3).Proposed
design of future clinical trials in TNBCOf course, these proposed
approaches of management ofearly and advanced TNBC should be
evaluated in well-planned clinical trials. To facilitate patients
recruitmentand conduction of trials in this disease with variable
sub-types where a plenty of drugs need to be investigated,upfront
testing of patients for predictive markers should beconsidered.
Multiple treatment arms should be availableand patients can be
allocated to the suitable therapy basedon their testing results
(Fig. 4).
Conclusion
Treatment outcome of TNBC is still unsatisfactory even inthe
early stage of the disease. TNBC should be viewed as agroup of
different diseases that have similar phenotype butdifferent
genotypes with variable response to chemother-apy. Recent data
revealed different molecular subtypes ofthe disease with different
driving molecular pathways andprovided insights about potential
therapeutic targets. Thisconcept raises the real need for
personalized therapies ofTNBC to improve the treatment outcome of
this disease.Several questions are still to be answered. The
propersequence of therapies, possible combinations, duration
oftherapy and validation of predictive markers are open eldsfor
future research. In addition, possible exclusion ofadjuvant
chemotherapy needs to be assessed in TNBCsubtypes with low
proliferation where chemotherapy haslittle effect and other
therapies may be more benecial.AcknowledgmentsThe authors would
like to thank Dr. Mian Us-man Farooq for his technical support in
the preparation of the guresof the manuscript.The authors declared
that they have no conictConict of interestof interest.
References1. Carey L, Winer E, Viale G, et al. Triple-negative
breast cancer:disease entity or title of convenience? Nat Rev Clin
Oncol.2010;7:68392.2. Dent R, Trudeau M, Pritchard K, et al.
Triple-negative breastcancer: clinical features and patterns of
recurrence. Clin CancerRes. 2007;13:442934.3. Foulkes WD, Smith IE,
Reis-Filho JS. Triple-negative breastcancer. N Engl J Med.
2010;363(20):193848.4. Peddi PF, Ellis MJ, Ma C. Molecular basis of
triple negativebreast cancer and implications for therapy. Int J
Breast Cancer.2012:217185, 17.834 Page 6 of 7Med Oncol (2014)
31:834survival, and CSCs were found to be more sensitive
toinhibition of this pathway than normal stem cells [32]. Thishas
been demonstrated in brain and prostate CSCs exposedto Akt
inhibitors where the drugs affected CSCs, but nothealthy stem cells
[33].Furthermore, adjuvant hormonal therapy improves theoutcome of
ER-positive breast cancer patients. This mayjustify evaluating the
efcacy of anti-androgens in adjuvanttherapy of AR-positive
TNBC.
123