Embed Size (px)
Citation preview

Update on Management of Triple Negative Breast Cancer
Banu Arun, M.D. Professor, Breast Medical Oncology Co-Director Clinical Cancer Genetics
The University of Texas MD Anderson Cancer Center
August, 2015
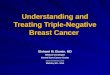
Basal-like 1: cell cycle, DNA repair and proliferation genes
Basal-like 2: Growth factor signaling (EGFR, MET, Wnt, IGF1R)
IM: immune cell processes (medullary breast cancer)
M: Cell motility and differentiation, EMT processes
MSL: similar to M but growth factor signaling, low levels of proliferation genes (metaplastic cancers)
LAR: Androgen receptor and downstream genes, luminal features
TNBC is Not One Disease
Lehmann et al. J Clin Invest 2011

Characteristics of TNBC
• At least 15% of breast cancers
• Higher incidence in AA and Hispanic women
• Germline BRCA mutation rate 11-37%
• Etiologic risk factors not known (except BRCA1 germline mutations carriers and ? AA women who did not breastfed)
• Sensitive to standard chemotherapy (pCR 35-40%)- but ↓DFS/OS
• Early relapse (2-3 yrs); after relapse time to death shorter • Significantly heterogeneous disease
• No targeted therapy currently available
Lehmann et al. J Clin Invest 2011, Kwon & Arun JCO 2010
Clinical Questions
• Specific type of chemotherapy? – Metastatic – Neoadjuvant, adjuvant
• BRCA-associated breast cancer, role of HRD assay in
sporadic TNBC (BRCAness)
• Role of antiangiogenic agents? • What are the targets in subsets of TNBC?

How does TNBC respond to available
chemotherapeutic agents?
-Anthracyclines
-Taxanes
-Capecitabine
-Ixabepilone
-Eribulin

Anthracyclines for TNBC
Trial Phase/no. TNBC pts
Setting Regimen Outcome in TNBC
Di Leo (2008) Meta-analysis
III (n=157) Adjuvant Anthracycline vs CMF
23% reduction in risk of relapse
Bidard (2008) II (n=120) Neoadjuvant CEF x 4-6 pCR: 17%
Gluz (2008) III (n=66) Neoadjuvant DD EC or CMF vs HD EC-ECThiotepa
5-yr EFS with HD 71% vs 26% with DD
Hudis C A , and Gianni L The Oncologist 2011;16:1-11
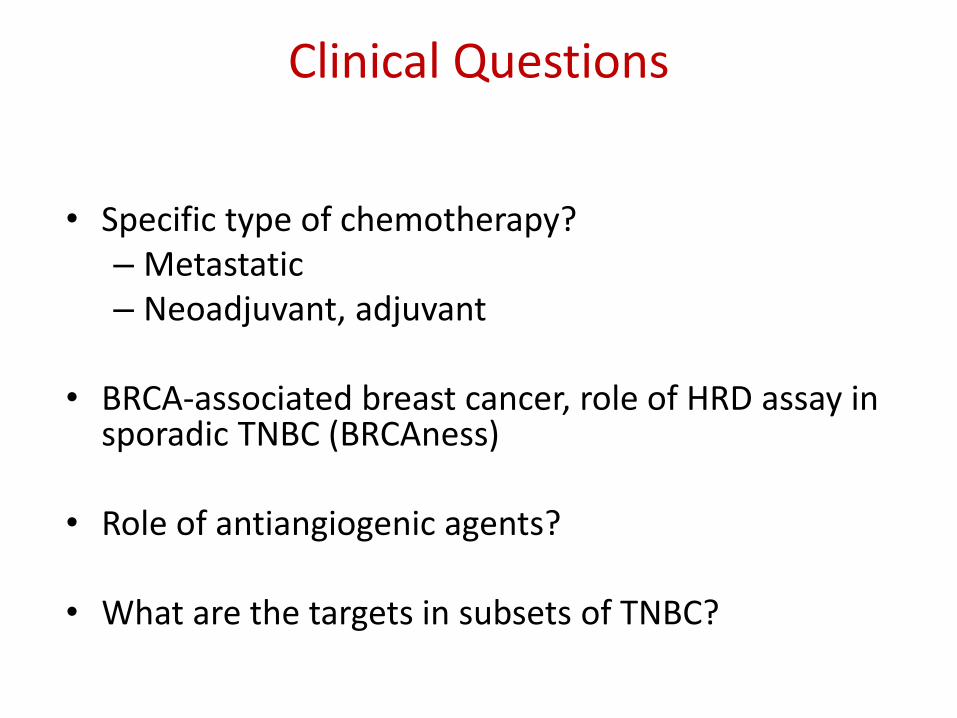
• Meta-analysis, stage IV, first-line trials
• Taxane-based vs anthracycline-based
• Results: Taxane better, ER-negative ~ ER-positive – HER2 not evaluated
TNBC and Taxanes
Piccart-Gebhart et al, JCO 2008

28-day cycle: Paclitaxel 90 mg/m2 D1, 8, and
15. Bevacizumab 10 mg/kg D1 and
15.
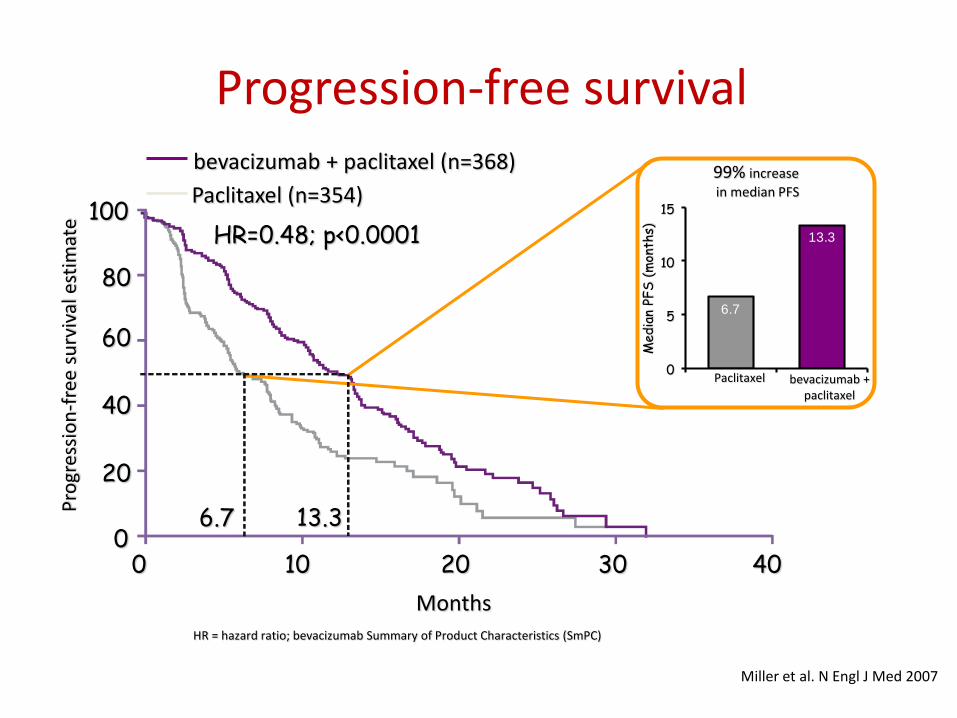
Paclitaxel +/- Bevacizumab as First-Line Therapy for Locally Recurrent or Metastatic Breast
Cancer (E2100)
R A N D OM I Z E
Paclitaxel+ Bevacizumab
Paclitaxel
Miller et al. N Engl J Med 2007
0
20
40
60
80
100
Months
Pro
gres
sio
n-f
ree
surv
ival
est
imat
e
0 10 20 30 40
6.7 13.3
HR=0.48; p<0.0001 13.3
6.7
99% increase
in median PFS
Med
ian
PFS
(m
onth
s)
15
10
5
0 bevacizumab +
paclitaxel
Paclitaxel
Paclitaxel (n=354)
bevacizumab + paclitaxel (n=368)
HR = hazard ratio; bevacizumab Summary of Product Characteristics (SmPC)
Progression-free survival
Miller et al. N Engl J Med 2007

Paclitaxel +/- Bevacizumab as First-Line Therapy for Locally Recurrent or Metastatic Breast Cancer (E2100)
Miller et al. N Engl J Med 2007

CALGB 40502/NCCTG N063H Randomized phase III Trial, first-Line therapy for locally recurrent
or metastatic breast cancer
Rugo H et al, ASCO 2012
Paclitaxel vs nab-paclitaxel vs Ixabepilone
- -
Control
1
Exp 2
N = 799 Untreated Stage IV Strata: Adj taxanes ER/PR status
nab-paclitaxel 150 mg/m2 weekly + bevacizumab 10 mg/kg q 2 wks2
ixabepilone 16 mg/m2 weekly +
bevacizumab 10 mg/kg q 2 wks3
Restage q 2 cycles until
disease progression
paclitaxel 90 mg/m2 weekly + bevacizumab 10 mg/kg q 2 wks1

CALGB 40502 Subset Analyses
Triple Negative Disease
Months From Study Entry
Pro
port
ion A
live
0 5 10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1
PacNabIxa
Triple Negative Disease
Comparison HR P-value 95% CI
nab vs. pac 0.93 0.7354 0.62 – 1.40
ixa vs. pac 1.46 0.0647 0.98 – 2.18
Pro
po
rtio
n P
rog
ressio
n F
ree
paclitaxel nab-paclitaxel ixabepilone
• 40502 overall findings: - Weekly paclitaxel > ixabepilone - Weekly paclitaxel less toxic
than either (in general)
• TNBC Subset: - No real difference from
parent trial - 98% received bevacizumab

• Women who underwent BRCA genetic testing and were treated with NST for breast cancer between 1997 and 2009
• 25% were positive for BRCA mutations
• Treatment with T+A or A, or T only
Arun et al JCO 2011
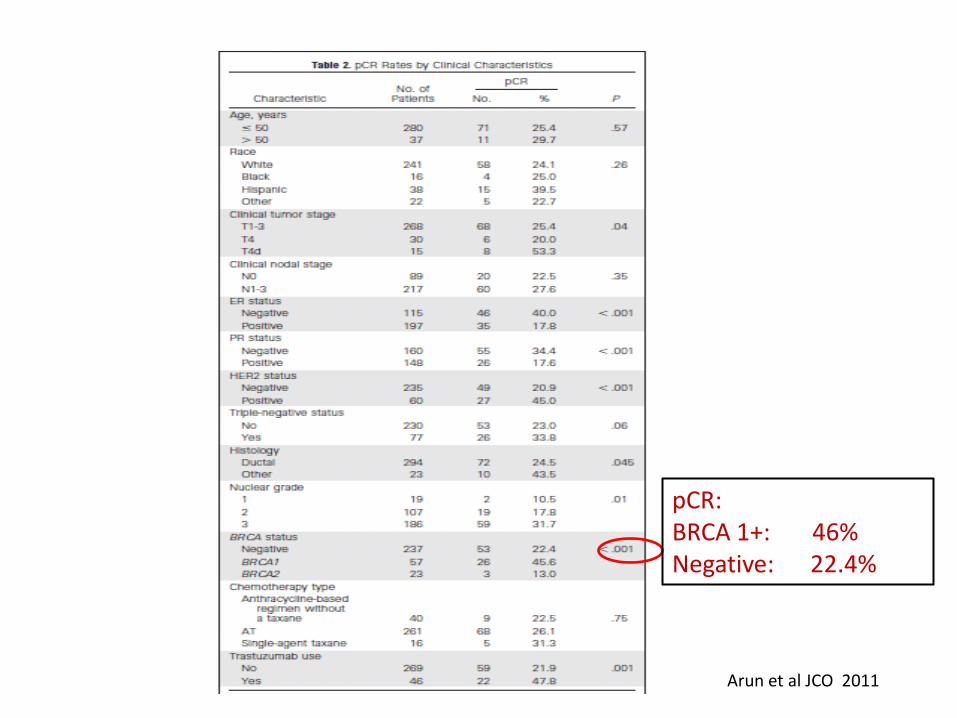
Arun et al JCO 2011
pCR: BRCA 1+: 46% Negative: 22.4%

Pathologic Complete Response
Arun et al JCO 2011
Further improvement with PARP inhibitors, Platinums?
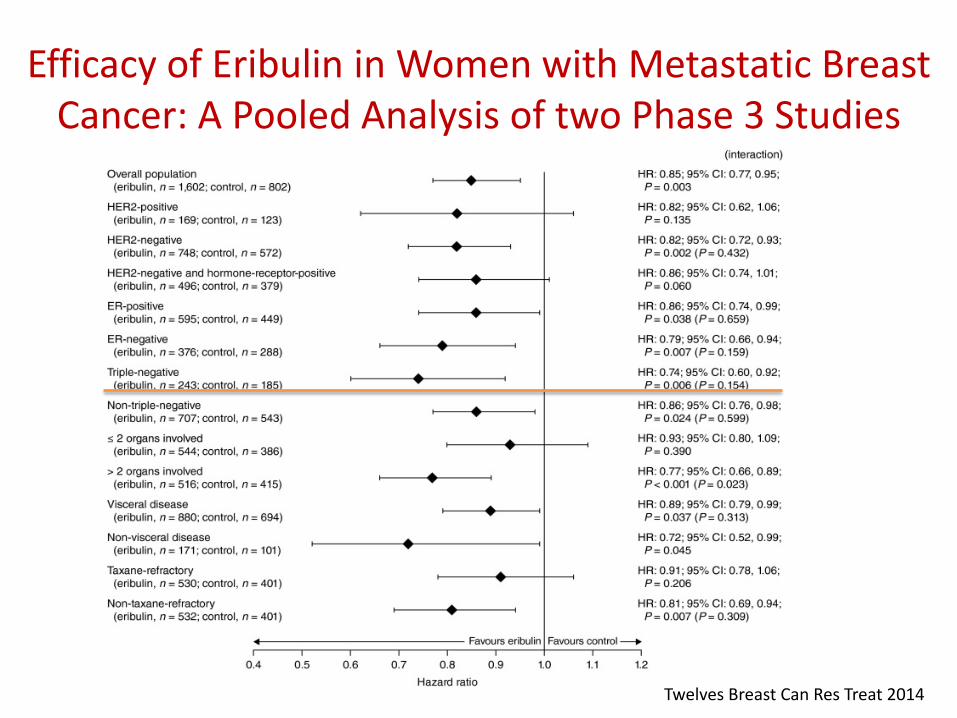
Efficacy of Eribulin in Women with Metastatic Breast Cancer: A Pooled Analysis of two Phase 3 Studies
Twelves Breast Can Res Treat 2014
TNBC: BRCA Germline associated vs BRCAness
• Sporadic TNBC (without germline BRCA mutations), shares clinical and molecular features with BRCA-associated cancers including defective DNA repair: – methylation-induced silencing of BRCA
– mutations in other genes that encode proteins involved in DNA repair
• Opportunity for DNA damaging agents: Platinums
• DNA repair inhibitors: PARPi
Foulkes NEJM 2010; Lips BrJ Ca 2013; Maxwell KN JCO a1510, 2014; Turner N Nat Rev Can 2004; Lehmann BD JCO 2011

TNBC and Platinums in Stage IV
Stage IV Trials Population Results
Control arm BALI-1 (CDDP) Sporadic TNBC 10% RR
Control arm Phase III iniparib (Gem/carbo) Sporadic TNBC 30% RR
TBCRC 001 (Cetuximab/Carbo) Sporadic TNBC 17% RR
TBCRC 009 (Carboplatin or Cisplatin) Sporadic TNBC 30% RR
Baselga, ESMO’10; O’Shaughnessy, ASCO’11; Carey et al, JCO’12; Isakoff, ASCO’11
Platinums:
Reasonable in sporadic TNBC – but what line?
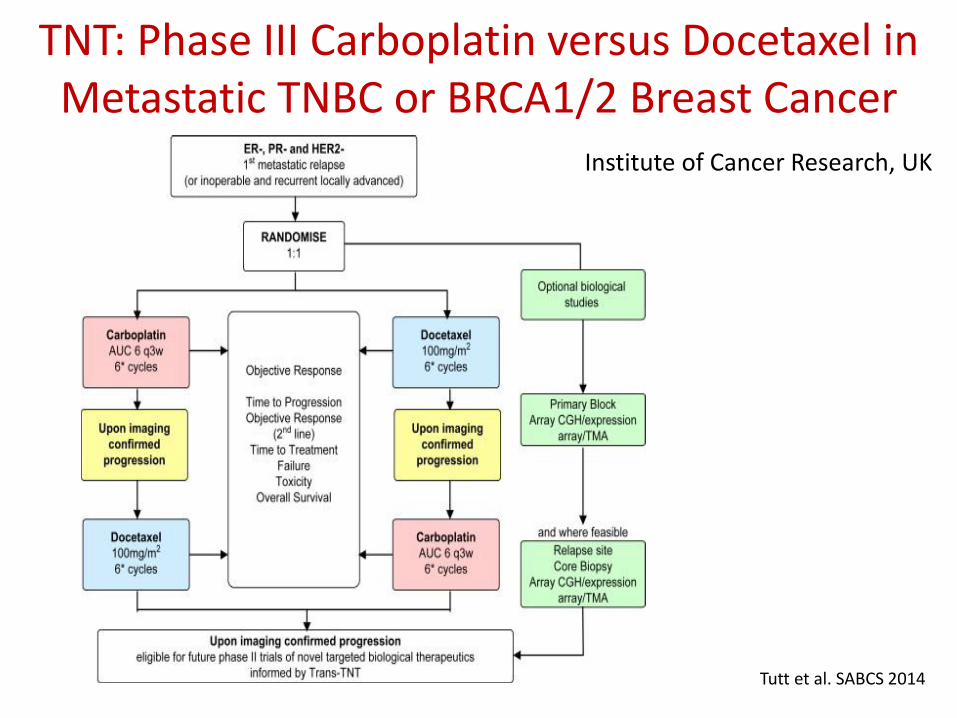
TNT: Phase III Carboplatin versus Docetaxel in Metastatic TNBC or BRCA1/2 Breast Cancer
Institute of Cancer Research, UK
Tutt et al. SABCS 2014

Tutt et al. SABCS 2014





Trial Type n Drugs Population pCR
DFCI1 Single arm Ph 2 21 CDDP x 4 TNBC 21%
DFCI2 Single arm Ph 2 51 CDDP+bev TNBC 15%
Polish Retrospective 13 CDDP x 4 BRCA+ 83%
GEICAM Randomized Ph 2 94 EC-D EC-D+carbo
Basal-like (IHC) 30% 35%
GeparSixto Randomized Ph 3 315 wP/LDox/bev +/- Carbo
TNBC (subset) 43% 57%
PreCOG0105 Single arm Ph 2 80 G/Carbo/iniparib TNBC 36%
CALGB 40603 Randomized Ph 2 455 T-AC(bev) T/carbo-AC(bev)
TNBC 41% 54%
Neodjuvant Platinum in TNBC
Silver et al, JCO’12; Ryan et al, ASCO’09; Byrski et al, JCO’10; Alba et al, BCRT’12; von Minckwitz et al, Lancet Oncol ‘14; Telli et al, ASCO a 1003’13; Sikov et al, SABCS’13

Schema of randomized phase II CALGB 40603 Trial
Sikov W M et al. JCO 2015;33:13-21
©2015 by American Society of Clinical Oncology

Pathologic complete response in breast
and breast/axilla
©2015 by American Society of Clinical Oncology
Sikov W M et al. JCO 2015;33:13-21

Sikov W M et al. JCO 2015;33:13-21

Do we add carboplatin to every TNBC?
• Addition of either carboplatin or bevacizumab to NACT increased pCR rates; ↑DFS/OS??
• Given results from recently reported adjuvant trials, further investigation of bevacizumab in this setting is unlikely
• Role of carboplatin could be evaluated in definitive studies in biologically defined patient subsets most likely to benefit from this agent (BRCA?)
• Decreased rate of completing all taxol and all AC cycles
Antiangiogenic Drugs Added to Chemotherapy?
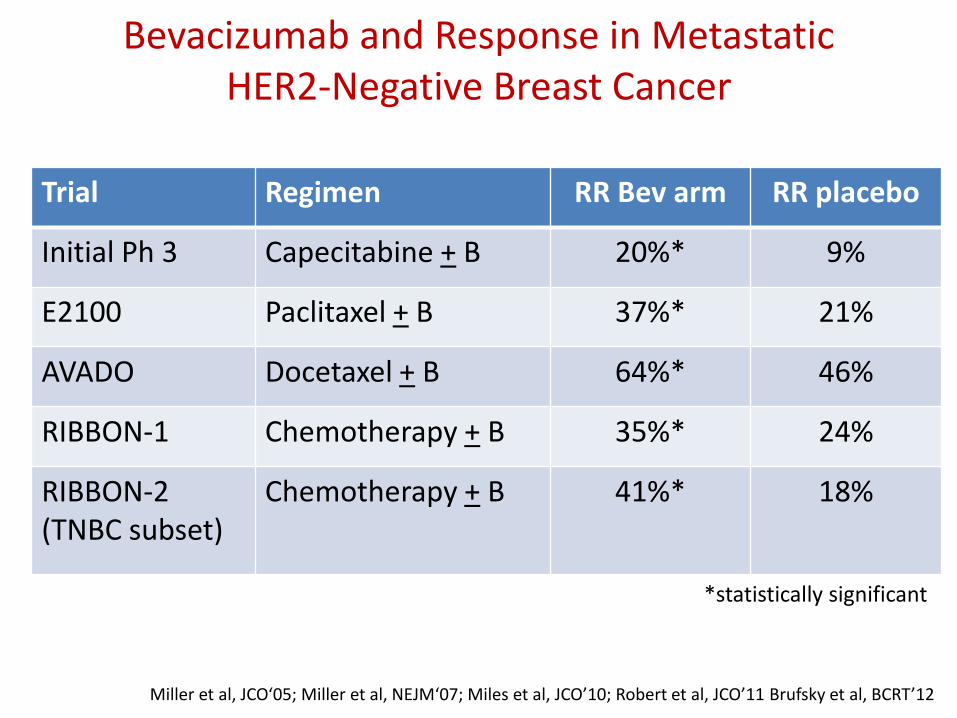
Bevacizumab and Response in Metastatic HER2-Negative Breast Cancer
Trial Regimen RR Bev arm RR placebo
Initial Ph 3 Capecitabine + B 20%* 9%
E2100 Paclitaxel + B 37%* 21%
AVADO Docetaxel + B 64%* 46%
RIBBON-1 Chemotherapy + B 35%* 24%
RIBBON-2 (TNBC subset)
Chemotherapy + B 41%* 18%
Miller et al, JCO‘05; Miller et al, NEJM‘07; Miles et al, JCO’10; Robert et al, JCO’11 Brufsky et al, BCRT’12
*statistically significant

Bevasuzumab: Neoadjuvant and Adjuvant in TNBC
Trial Setting Outcome P value
Gepar-Quinto Neoadjuvant pCR:33% → 43% 0.007
NSABP-B40 Neoadjuvant pCR:47% → 52% NS
BEATRICE Adjuvant No DFS benefit
E5103 Adjuvant No DFS benefit
Von Minckwithz NEJM 2012; Bear NEJM 2014, Cameron Lancet Oncol 2013; Miller JCO 2014)
• Metastatic setting: increases RR when added to chemotherapy, but has no impact on OS- therefore, when response is the endpoint, adding Bev is an option
• Neoadjuvant setting: Increase pCR; but DFS/OS impact is unknown
• Adjuvant setting: No impact on DFS and OS
Bevacizumab: Practical Conclusions

PARP Inhibitors
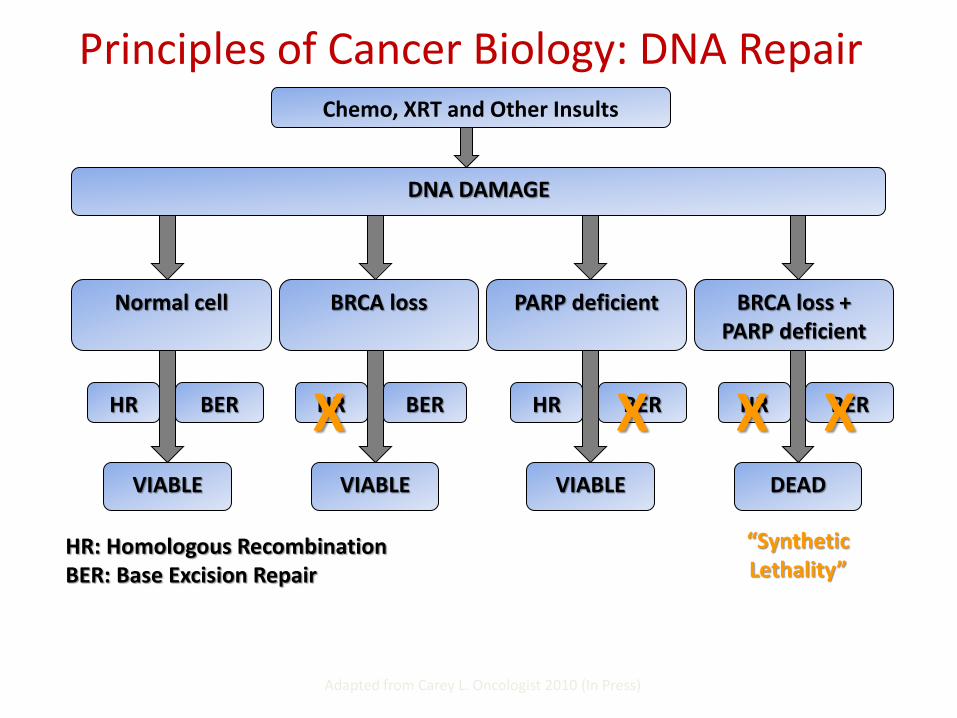
Principles of Cancer Biology: DNA Repair
Adapted from Carey L. Oncologist 2010 (In Press)
Chemo, XRT and Other Insults
DNA DAMAGE
Normal cell BRCA loss PARP deficient BRCA loss + PARP deficient
VIABLE VIABLE VIABLE DEAD
HR BER HR BER HR BER HR BER
HR: Homologous Recombination BER: Base Excision Repair
X X X X
“Synthetic Lethality”

PARP Inhibitor Trials – Activity Seen Only in BRCA1/2 Mutation Carriers
Agent Author BRCA1/BRCA2 TNBC Response Rate
Olaparib (phase I; mixture tumor
types)
Fong 60 patients 37% -BRCA1/2
mutations
N/A 63% clinical benefit rate
(only in BRCA associated cancers)
Olaparib 400 mg po BID
Tutt 27 patients BRCA1 67% BRCA2 33%
50% 41%
ABT888 +temozolomide
Isakoff 41 patients BRCA1: 7.3% BRCA2: 12%
56% BRCA 1 and 2: 37.5%
No response in normal BRCA status
Fong et al. N Engl J Med 2009 Tutt et al. Lancet 2010 Isakoff et al. ASCO 2010
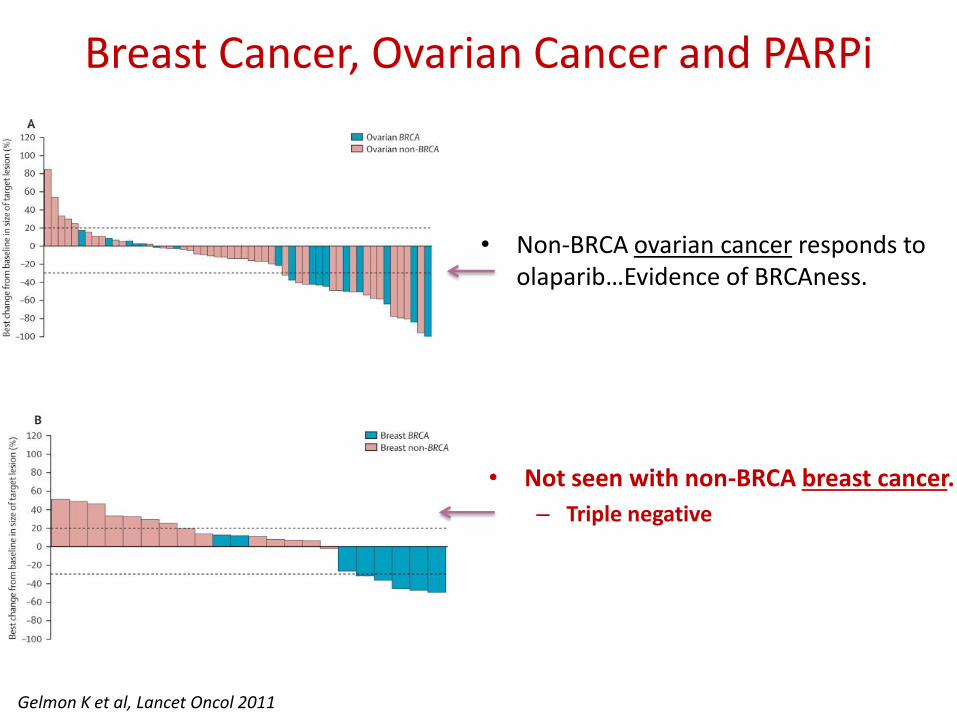
• Non-BRCA ovarian cancer responds to olaparib…Evidence of BRCAness.
Breast Cancer, Ovarian Cancer and PARPi
• Not seen with non-BRCA breast cancer.
– Triple negative
Gelmon K et al, Lancet Oncol 2011

Identifying BRCA Deficiency
• Major consequence is homologous recombination (HR) DNA repair defect
• Functional assays in development
Birkbak NJ et al. Cancer Discovery 2012
HRD score
Non-responders
BRCA1/2 intact responders
BRCA1/2 mutant responders
Telli M et al, SABCS 2012

What is next for TNBC? Targets Within Triple Negative Subsets?
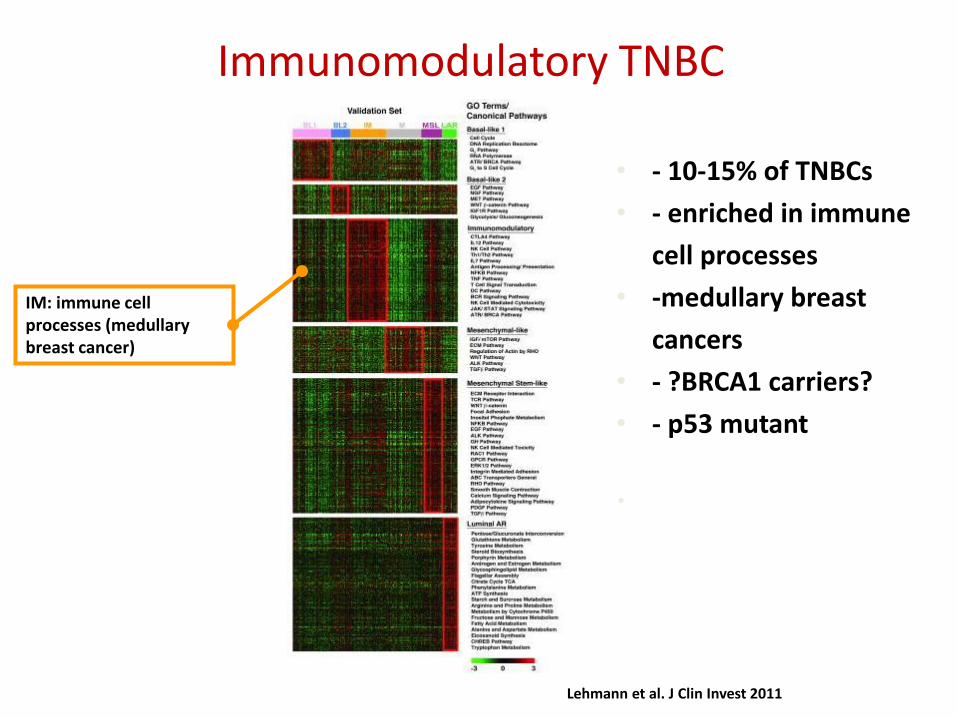
Immunomodulatory TNBC
Lehmann et al. J Clin Invest 2011
IM: immune cell processes (medullary breast cancer)
• - 10-15% of TNBCs
• - enriched in immune
cell processes
• -medullary breast
cancers
• - ?BRCA1 carriers?
• - p53 mutant
•
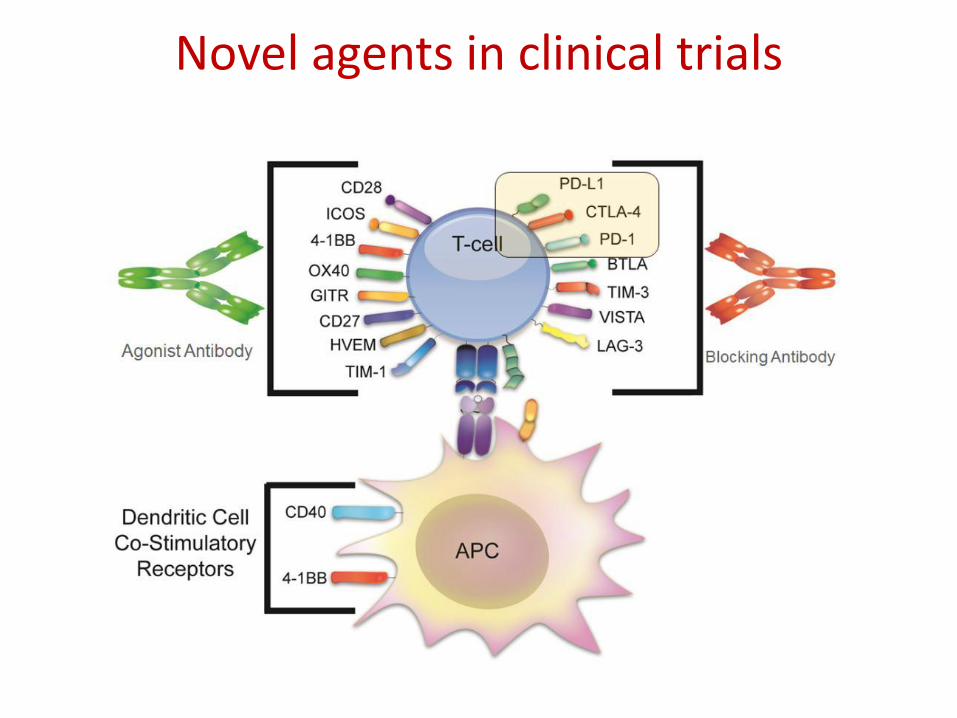
Novel agents in clinical trials

Other targets for triple-negative breast cancer
Hudis C A , and Gianni L The Oncologist 2011;16:1-11 ©2011 by AlphaMed Press

MDACC Moonshot Triaging
Platform
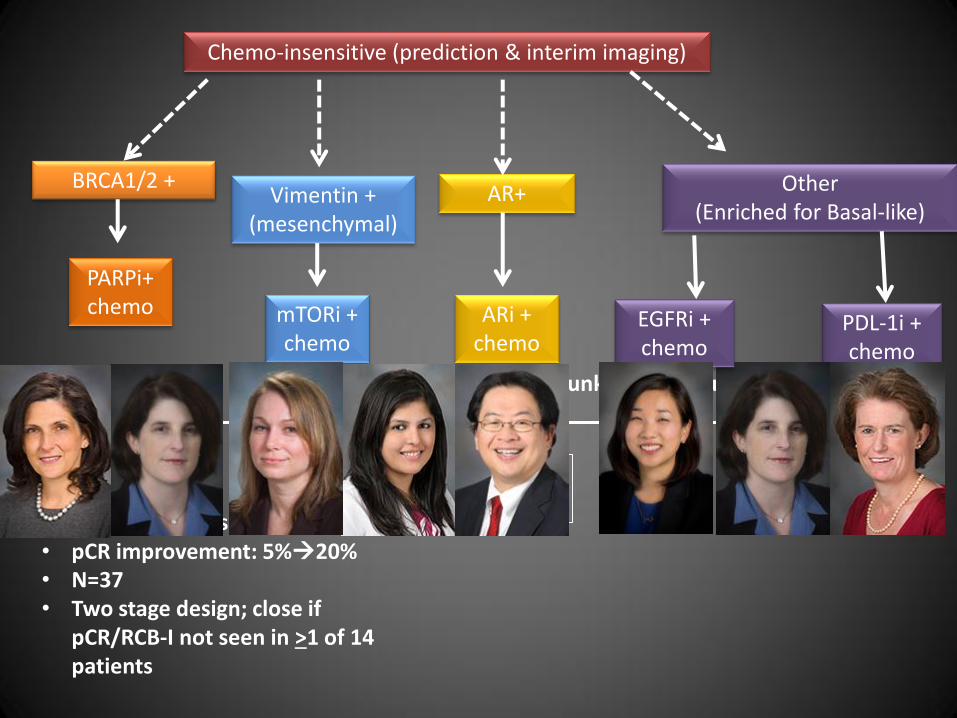
Chemo-insensitive (prediction & interim imaging)
Vimentin + (mesenchymal)
AR+ Other (Enriched for Basal-like)
mTORi + chemo
Improved rate of pCR/RCB-I?
ARi + chemo
PDL-1i + chemo
*comparison to control ‘predictor unknown’ group
BRCA1/2 +
PARPi+ chemo
• Single arm phase II trials • pCR improvement: 5%20% • N=37 • Two stage design; close if
pCR/RCB-I not seen in >1 of 14 patients
EGFRi + chemo

• TNBC is heterogeneous
• Stage 4: Chemotherapy is mainstay and (at the moment) is the same as for other subtypes.
– First-line taxanes or platinum appropriate
– Second+ lines: Eribulin to other options
• Neoadjuvant: Platinums ? Toxicity- clinical benefit ratio? No ↑EFS, BCS rate- additional markers needed: HRD score, TILs….more studies ongoing
• Residual disease ?: EA1131 phase III ECOG-ACRIN: Evaluate platinum after Tax based NAST. Endpoint: EFS
• BRCA1-associated TNBC may be different:
Platinums, PARP inhibition
• Subtype specific studies and novel study designs are ongoing
Conclusion
Thank you