-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
1/16
JOGNN R E V I E W
Trial of Labor and Vaginal Delivery
Rates in Women with a Prior CesareanKaren B. Eden, Mary Anna
Denman, Cathy L. Emeis, Marian S. McDonagh, Rongwei Fu, Rosalind K.
Janik,Alia R. Broman, and Jeanne-Marie Guise
Correspondence
Karen B. Eden, PhD,
Department of Medical
Informatics and Clinical
Epidemiology, Oregon
Health and Science
University, 3181 SW Sam
Jackson Park Rd, Portland,
OR 97229.
[email protected]
Keywords
VBAC
trial of labor
pregnancy
predictors
cesarean
evidence review
ABSTRACT
Objective: To evaluate evidence on trial of labor (TOL) and
vaginal delivery rates in women with a prior cesarean and
to understand the characteristics of women offered a trial of
labor.
Data Sources: MEDLINE, DARE, and Cochrane databases were
searched for articles evaluating mode of delivery for
women with a prior cesarean delivery published between 1980 and
September 2009.
Study Selection: Studies were included if they involved
human participants, were in English, conducted in the United
States or in developed countries, and if they were rated fair or
good base on U.S. Preventive Services Task Force
(USPSTF) criteria.
Data Extraction and Synthesis: The search yielded 3,134
abstracts: 69 full-text papers on TOL and vaginal birth
after cesarean (VBAC) rates and 10 on predictors of TOL. The TOL
rate in U.S. studies was 58% (95% CI [52, 65])
compared with 64% (95% CI [59, 70]) in non U.S. studies. The TOL
rate in the U.S. was 62% (95% CI [57, 66]) for
studies completed prior to 1996 and dropped to 44% (95% CI [34,
53]) in studies launched after 1996, p = .016. In
U.S.
studies, 74% (95% CI [72, 76]) of women who had a TOL delivered
vaginally. Women who had a prior vaginal birth or
delivered at a large teaching hospital were more likely to be
offered a TOL.
Conclusions: Although the TOL rate has dropped since 1996,
the rate of vaginal delivery after a TOL has remained
constant. Efforts to increase rates of TOL will depend on
patients understanding the risks and benefits of both options.
Maternity providers are well positioned to provide key education
and counseling when patients are not informed of their
options.
JOGNN, 41, 583-598; 2012. DOI:
10.1111/j.1552-6909.2012.01388.x
Accepted March 2012
Karen B. Eden, PhD, is an
associate professor in the
Oregon Evidence-based
Practice Center,
Department of Medical
Informatics and Clinical
Epidemiology, Oregon
Health and Science
University, Portland, OR.
Mary Anna Denman, MD,
MCR, is an assistant
professor in the Department
of Obstetrics and
Gynecology, Oregon Healthand Science University,
Portland, OR.
(Continued)
Prior to 1996, in the United States, the num-
ber of women having a vaginal birth after ce-
sarean (VBAC) reached an all-time high of 28%
(Menacker, Declercq, & Macdorman, 2006). How-
ever, with the release of information on uterine rup-
ture in 1996 (McMahon, Luther, Bowes, & Olshan,
1996), the number of women undergoing a trial of
labor (TOL) began to steadily decline. In 1999, the
American College of Obstetricians and Gynecolo-
gists (ACOG; 1999) recommended that hospitals
offering VBAC should have a surgical team imme-
diately available throughout labor. Some hospitalsunable to
provide an immediate surgical response
and concerned about liability during labor prohib-
ited the practice of VBAC, which left some women
with no option for a TOL (Scott, 2010; Shorten,
2010). In one study, the authors reported that
prior to the 1999 ACOG guideline, 24% of eligi-
ble women in California hospitals had a TOL, and
immediately following the release, 13.5% of eligi-
ble women made the attempt, p < .001
(Zweifler
et al., 2006). When questioned, a majority (85%) of
physicians cited the updated ACOG guideline as
one of many “most important” factors to consider
when recommending VBAC (Coleman, Erickson,
Schulkin, Zinberg, & Sachs, 2005). The culmina-
tion of these events led to a national VBAC rate of
8.3% in 2007 (Martin et al., 2010).
A reduction in the national VBAC rate could be
attributed to fewer women having TOLs (fewer
providers and hospitals offering TOLs or fewer
women at eligible sites being allowed TOLs), fewerwomen who have
TOLs and who deliver vaginally,
and/or a combination of factors. Because not all
settings allow TOL, this report provides a system-
atic review of the literature regarding TOL rates
and the subsequent vaginal delivery rates in set-
tings that allowed it. Because of variation in the
rate of TOL, we evaluated underlying health care
barriers (and enablers) found in the literature that
may have affected whether women were offered a
Disclosure: The authors re-port no conflict of interestor
relevant financial rela-tionships.
http://jognn.awhonn.org C 2012 AWHONN, the
Association of Women’s Health, Obstetric and Neonatal Nurses
583
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
2/16
R E V I E W TOL and VBAC rates
TOL. This systematic review was part of a larger
evidence report on VBAC conducted to inform the
U.S. 2010 National Institutes of Health (NIH) Con-
sensus Development Conference: Vaginal Birth
After Cesarean: New Insights (Guise, Denman,
et al., 2010; Guise, Eden, et al., 2010).
MethodsData Sources
Together with a medical librarian, we searched
MEDLINE, Database of Abstracts of Reviews of
Effectiveness (DARE), and the Cochrane Library
from 1980 to September 2009 using methods de-
scribed previously (Guise, Denman, et al., 2010;
Guise, Eden, et al., 2010). The search was limited
to publications after 1980 when the NIH held a
consensus conference that concluded that VBAC
was an acceptable option and resulted in changes
in practice. The searches included variations of
the terms VBAC, prior cesarean , and trial of
la-
bor . Additional articles were identified from refer-
encelists of reviews and editorials and through the
peer review process. The abstracts retrieved from
the searches were then entered into an electronic
database. This search was part of a larger search
that addressed several topics for the evidence re-
port related to TOL and VBAC rates, predictors of
TOL and VBAC, benefits and harms to mothers
and infants for TOL, and repeat cesarean (Guise,
Denman, et al.; Guise, Eden, et al.).
Study Selection
Cathy L. Emeis, PhD,
CNM, is an assistant
professor in the School of
Nursing, Oregon Health
and Science University,
Portland, OR.
Marian S. McDonagh,
PharmD, is an associate
professor in the Oregon
Evidence-based Practice
Center, Department of
Medical Informatics and
Clinical Epidemiology,
Oregon Health and Science
University, Portland, OR.
Rongwei Fu, PhD, is an
associate professor in the
Oregon Evidence-based
Practice Center,
Department of Public
Health and Preventive
Medicine and the
Department of EmergencyMedicine, Oregon Health
and Science University,
Portland, OR.
Rosalind K. Janik, BA, is a
project manager at Epic
Systems Corporation,
Verona, WI.
Alia R. Broman, BA, is a
student at the medical
school at the University of
Colorado, School of
Medicine, Aurora, CO.
Jeanne-Marie Guise, MD,
MPH, is an associatedirector for the Oregon
Evidence-based Practice
Center and an associate
professor in the Department
of Medical Informatics and
Clinical Epidemiology,
Department of Obstetrics
and Gynecology and
Department Public Health
and Preventive Medicine,
Oregon Health and Science
University, Portland, OR.
Full-text studies were included if they explicitly re-
ported on eligibility for TOL and if they provided
data for computing theTOL rate or vaginal delivery
rate after a TOL at the study sites. We were partic-
ularly interested in studies that provided informa-
tion on influencing factors and predictors of TOL.
Non-U.S. studies were included if the study was
conducted in a developed country because the
available technology and medical response were
thought to be similar to the United States and were
published in English (The World Factbook , 2008).
Two investigators reviewed each full-text article for
inclusion or exclusion. We excluded studies that
included women without a prior cesarean deliv-
ery, nulliparous patients, 10 participants or fewer,
breech delivery, exclusive focus on preterm de-
livery or low birth weight, multiple gestation, or
abortions.
Data Extraction and Quality Rating
Reviewers rated the quality of each study using
criteria developed by the U.S. Preventive Services
Task Force (USPSTF) and the National Health Ser-
vice Centre for Reviews and Dissemination (Harris
et al., 2001; Healthy Inclusion, 2001). Two review-
ers independently reviewed the studies. When
reviewers disagreed, a final rating was reached
through discussion and consensus of the whole
team. Studies that were rated as poor quality were
excluded from analyses. Parameters that were
particularly important for TOL and VBAC rates
were clear definition of eligibility for TOL, com-
parable groups, reliable and valid outcomes, un-
biased assessment of measures, follow-up long
enough for outcome to occur, acceptable level
of attrition (≤40%), and adjustment for potential
confounders (Guise, Denman, et al., 2010; Guise,
Eden, et al., 2010). For studies reporting on the
factors influencing or predicting TOL, clear defini-
tion of all factors was critical (Guise, Eden, et al.).
Data from included papers were extracted by one
researcher into evidence tables and verified by a
second.
Analysis
Meta-analyses were conducted using a random
effects model (DerSimonian & Laird,1986) to sum-
marize TOL and vaginal delivery rates. Statistical
heterogeneity was assessed by using the stan-
dard chi-squared test and the I 2 statistic (the
proportion of variation in study estimates due to
heterogeneity rather than sampling error) (Hig-
gins, Thompson, Deeks, & Altman, 2003; Hig-
gins, Thompson, Higgins, & Thompson, 2002).
To explore heterogeneity, we performed subgroup
analyses and meta-regression (Sutton, Abrams,
Jones, Sheldon, & Song, 2000; Thompson &
Sharp, 1999) to evaluate whether the summary
estimates differed by study-level characteristics,
including U.S. versus non-U.S. population, ges-
tational age of the population (term vs. any ges-
tational age), and year of data collection of the
study.
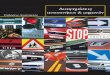
ResultsAs shown in Figure 1, of 3,134 citations identified
in searches, 963 full-text papers were reviewed
and 69 studies that contained adequate data tocompute the TOL
and/or vaginal delivery rate, and
10 studies on predictors of TOL met the inclusion
and quality standards. We included 19 studies of
good quality and 50 studies of fair quality that pro-
vided evidence on TOL and VBAC rates (Table 1).
The majority (7 of 10) of the studies providing
evidence on individual predictors were of good
quality (Cameron, Roberts, & Peat 2004; Chang,
Stamilio, & Macones, 2008; DeFranco et al., 2007;
584 JOGNN, 41, 583-598; 2012. DOI: 10.1111/j.1552-
6909.2012.01388.x http://jognn.awhonn.org
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
3/16
Eden, K.B. et al. R E V I E W
Figure 1. Search and Selection of Literature for TOL rate
and Vaginal Delivery Rate after TOL.
TOL = trial of labor; VBAC = vaginal birth after cesarean.
aSearched databases included MEDLINE, Cochrane and DARE.
bMany studies areincludedin more than
onetopicarea.Adaptedwithpermissionfrom Guise,J. M.,Eden,
K.,Emeis,C.,Denman,
M., Marshall, N., Fu, R., . . . McDonagh, M. (2010).
Vaginal birth after cesarean: New insights. Evidence
Report/Technology
AssessmentNo. 191 (AHRQpublication no.10-E001).Rockville, MD:
Agency forHealthcareResearch and Quality. Alsoadapted
with permission from Wolters Kluwer. from Eden, K.B., (2010).
New insights on vaginal birth after cesarean, can it be
predicted?
Obstetrics & Gynecology , 116 (4),
967–981.
Harper et al., 2009; Kabir, Pridjian, Steinmann,Herrera, &
Khan, 2005; McMahon et al., 1996;
Pang, Law, Leung, Lai, & La 2009), and the re-
mainder (3 of 10) were fair quality (Bujold, 2001;
Hueston & Rudy, 1994; Selo-Ojeme, Abulhassan,
Mandal, Tirlapur, & Selo-Ojeme 2008).
TOL Rate
Thirty-five studies consisting of 10 prospective
and 25 retrospective cohort studies provided data
on TOL rates (Table 1). These studies included
661,765 women and provided a combined TOL
rate of 61% (95% CI [57, 65]). However, the ratesof TOL
significantly variedacross thestudies rang-
ing from 28% to 82% (p < .0001) with an
I 2
for between-heterogeneity of greater than 99%
(Figure 2). Results from metaregression indicated
that TOL rates differed significantly by gestational
age and year of study (p
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
4/16
R E V I E W TOL and VBAC rates
Table 1: Evidence for TOL and Vaginal Delivery Rates
Study Quality U.S. or Cohort Evidence Evidence for
Non-U.S. Design for TOL Vaginal Delivery
after TOLa
Bais, 2001 Fair Non Prospective X X
Cameron, 2004 Good Non Retrospective X X
Caughey, 1999 Fair US Retrospective X
Costantine, 2009 Good US Retrospective X (Term)
De Franco, 2007 Good US Retrospective X X
Delaney, 2003 Fair Non Retrospective X
DiMaio, 2002 Fair US Retrospective X X (Term)
Dinsmoor, 2004 Fair US Retrospective X
Durnwald, 2004a Fair US Retrospective X
Durnwald, 2004b Fair US Retrospective X X
El-Sayed, 2007 Fair US Retrospective X (Term)
Elkousy, 2003 Fair US Retrospective X (Term)
Fisler, 2003 Fair US Retrospective X X (Term)
Flamm, 1987 Fair US Retrospective X
Flamm, 1994 Good US Prospective X X
Gonen, 2006 Fair Non Retrospective X X
Goodall, 2005 Fair US Retrospective X
Gregory, 1999 Good US Retrospective X X
Gregory, 2008 Fair US Retrospective X X (Term)
Gyamfi, 2004 Good US Retrospective X (Term)
Hammoud, 2004 Fair Non Retrospective X
Hashima, 2007 Fair US Retrospective X (Term)
Hendler, 2004 Good Non Prospective X
Hibbard, 2006 Good US Prospective X X (Term)
Hollard, 2006 Good US Retrospective X
Hook, 1997 Good US Prospective X X (Term)
Horenstein, 1984 Fair US Retrospective X
Horenstein, 1985 Fair US Retrospective X
Hoskins, 1997 Fair US Retrospective X
Huang, 2002 Fair US Retrospective X (Term)
Hueston, 1994 Fair US Retrospective X
Jakobi, 1993 Good Non Prospective X
Johnson, 1991 Fair US Retrospective X
Juhasz, 2005 Fair US Retrospective X
Kugler, 2008 Fair Non Retrospective X X
Landon, 2006 Fair US Prospective X X
Learman, 1996 Good US Retrospective X
586 JOGNN, 41, 583-598; 2012. DOI: 10.1111/j.1552-
6909.2012.01388.x http://jognn.awhonn.org
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
5/16
Eden, K.B. et al. R E V I E W
Table 1: Continued
Study Quality U.S. or Cohort Evidence Evidence for
Non-U.S. Design for TOL Vaginal Delivery
after TOLa
Lieberman, 2004 Fair US Prospective X
Locatelli, 2004 Good Non Retrospective X X
Loebel, 2004 Fair US Retrospective X X (Term)
Macones, 2005 Fair US Retrospective X X
McMahon, 1996 Good Non Retrospective X X
McNally, 1999 Fair Non Retrospective X
Nguyen, 1992 Fair US Retrospective X
Obara, 1998 Fair Non Retrospective X X
Ouzounian, 1996 Fair US Retrospective X
Pang, 2009 Good Non Retrospective X X (Term)
Pathadey, 2005 Fair Non Retrospective X
Phelan, 1987 Fair US Prospective X X
Pickhardt, 1992 Fair US Retrospective X X
Raynor, 1993 Fair US Retrospective X
Rozenberg, 1996 Good Non Prospective X X
Rozenberg, 1999 Fair Non Prospective X X
Sakala, 1990 Fair US Retrospective X
Selo-Ojeme, 2008 Fair Non Retrospective X X (Term)
Smith, 2002 Good Non Retrospective X X (Term)
Smith, 2005 Good Non Retrospective X X (Term)
Socol, 1999 Fair US Retrospective X X
Spaans, 2002 Fair Non Retrospective X X
Stovall, 1987 Fair US Prospective X X
Strong, 1996 Fair Non Prospective X X
Troyer, 1992 Fair US Retrospective X X (Term)
van Gelderen, 1986 Fair Non Prospective X
Vinueza, 2000 Fair US Retrospective X
Weinstein, 1996 Good Non Retrospective X
Wen, 2004 Fair Non Retrospective X X (Term)
Yetman, 1989 Fair US Retrospective X
Yogev, 2004 Fair Non Retrospective X
Zelop, 2001 Fair US Retrospective X
Note. TOL = trial of labor.aUnless noted by “Term,” the
studies accepted women of all gestational ages (term and
preterm).
Lieberman, 2003; Flamm, Goings, Liu, & Wolde-
Tsadik, 1994; Gregory, Korst, Cane, Platt, & Kahn,
1999; Hook, Kiwi, Amini, Fanaroff, & Hack, 1997;
Hueston & Rudy, 1994; Phelan, Clark, Diaz, &
Paul, 1987; Pickhardt et al., 1992; Stovall, Shayer,
Solomon, & Anderson, 1987; Troyer & Parisi,
1992), 63% (95% CI [58, 67]) for U.S. studies that
included 1996 (DeFranco et al., 2007; Durnwald &
JOGNN 2012; Vol. 41, Issue 5 587
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
6/16
R E V I E W TOL and VBAC rates
Figure 2. Trial of labor in studies conducted in the
United States and outside the United States. Adapted with
permission from Guise, J. M., Eden, K., Emeis,
C., Denman, M., Marshall, N., Fu, R., . . . McDonagh, M.
(2010). Vaginal birth after cesarean: New insights. Evidence
Report/Technology Assessment No. 191
(AHRQ publication no. 10-E001). Rockville, MD: Agency for
Healthcare Research and Quality.
Mercer, 2004b; Loebel, Zelop, Egan, & Wax, 2004;
Macones et al., 2005; Socol & Peaceman, 1999),
and 44% (95% CI [34, to 53] for U.S. studies initi-ated after
1996 (DiMaio, Edwards, Euliano, Treloar,
& Cruz, 2002; Gregory et al., 2008; Landon et al.,
2006). The TOL was significantly lower than the
rate prior to 1996 (p = .016) or that included 1996
(p = .019) (Figure 3). A similar trend was
present
for non-U.S. studies (Figure 3).
Almost all studies providing TOL rates were con-
ducted in tertiary care centers such as teach-
ing hospitals with residents and 24-hour anes-
thesia teams available; therefore, findings have
limited applicability to rural settings. We found
two retrospective studies completed before 1996(Hueston &
Rudy, 1994; McMahon, 1996) that re-
ported reduced attempts (TOL rates ranging from
36%–41%) for rural settings compared with ur-
ban and/or teaching settings (TOL rates ranged
from 60%–69%). In one retrospective study com-
pleted 1998 to 2001 (Cameron, 2004), the authors
reported that rural sites had a TOL rate of 47%
compared with 55% for a perinatal center set-
ting. Finally, a retrospective study launched and
completed in 2001 indicated that 70% of repeat
cesarean deliveries (RCD) in rural settings were
potentially unnecessary compared with 61% in ur-ban teaching
settings that is consistent with find-
ings above (Kabir, 2005). The authors in this study
coded a cesarean as “potentially unnecessary”
if it lacked an associated discharge diagnosis to
justify it. A diagnosis of a prior cesarean delivery
alone was not considered sufficient justification for
a repeat cesarean. Although we could not statisti-
cally analyze these results, they suggest that the
rates of TOL are lower in rural settings than non-
rural settings and that the TOL rates across sites
may have dropped since 1996.
Vaginal Delivery Rate with TOL
Sixty-seven studies including 14 prospective co-
hort studies and 53 retrospective cohort stud-
ies (Table 1) provided data on VBAC rate from
368,304 women. The range in VBAC rates across
studies inside and outside the United States was
49% for a high-birth-volume hospital in London
(Selo-Ojeme, 2008) to 87% for a national study of
U.S. birth centers (Lieberman, 2004) (Figures 5
588 JOGNN, 41, 583-598; 2012. DOI: 10.1111/j.1552-
6909.2012.01388.x http://jognn.awhonn.org
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
7/16
Eden, K.B. et al. R E V I E W
Figure 3. Global trial of labor rates have dropped over
time.
Adapted with permission from Guise, J. M., Eden, K., Emeis, C.,
Denman, M., Marshall, N., Fu, R., . . . McDonagh, M. (2010).
Vaginal birth after cesarean: New insights. Evidence
Report/Technology Assessment No. 191 (AHRQ publication no.
10-E001).
Rockville, MD: Agency for Healthcare Research and Quality.
and 6), and the overall summary estimate for
the vaginal delivery rate from the random ef-
fects model was 74% (95% CI [72, 75]). How-
ever, there was significant heterogeneity among
included studies (p < .001) with I 2 =
98.6%.
Metaregression was conducted to assess the as-
sociation between vaginal delivery rates with TOL
and country, gestation, true cohort (study included
TOL and elective repeatcesarean delivery [ERCD]
vs. studies of TOL only), and by years when the
data were collected. None of these factors could
explain the variation among studies. The summary
estimates were similar: for the 43 studies con-
ducted in the United States, 74% (95% CI [72, 76])
of women had a vaginal delivery compared to 73%
(95% CI[71, 74]) for the 24 studies conducted out-
side the United States (Table 1). In examining the
gestational age for enrolled patients, the summary
estimates were again similar: for the 18 studies of
term deliveries, 73% (95% CI [71, 75]) of women
delivered vaginally compared to 74% (95% CI [72,
76]) for the 49 studies that included preterm and
term deliveries (Table 1).
Figure 4. TOL and vaginal delivery rates with TOL over
time.
JOGNN 2012; Vol. 41, Issue 5 589
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
8/16
R E V I E W TOL and VBAC rates
Figure 5. Rate of vaginal delivery with TOL in studies
conducted in the United States.
Reprinted with permission from Guise, J. M., Eden, K., Emeis,
C., Denman, M., Marshall, N., Fu, R., . . . McDonagh, M.
(2010).
Vaginal birth after cesarean: New insights. Evidence
Report/Technology Assessment No. 191 (AHRQ publication no.
10-E001).
Rockville, MD: Agency for Healthcare Research and Quality.
Using only the subset of the U.S. studies that pro-
vided data to compute the TOL and vaginal de-
livery rates with TOL, the rates were ordered by
year the data collection was launched (ranged
between 1982–2002) and plotted together on the
same chart, Figure 4. With the exception of one
retrospective study that focused on costs of de-
livery for a cohort of 204 women with a prior
low transverse cesarean (DiMaio, 2002, shown in
Figure 4), the TOL rates in U.S. studies (shown
by the diamonds) have dropped dramatically over
the last 15 years. The first drop was seen after
1996when McMahon’s (1996) evidence on uterine
rupture and other complications was published.
590 JOGNN, 41, 583-598; 2012. DOI: 10.1111/j.1552-
6909.2012.01388.x http://jognn.awhonn.org
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
9/16
Eden, K.B. et al. R E V I E W
Figure 6. Rate of vaginal delivery with TOL in studies
conducted outside the United States.
Reprinted with permission from Guise, J. M., Eden, K., Emeis,
C., Denman, M., Marshall, N., Fu, R., . . . McDonagh, M.
(2010).
Vaginal birth after cesarean: New insights. Evidence
Report/Technology Assessment No. 191 (AHRQ publication no.
10-E001).Rockville, MD: Agency for Healthcare Research and
Quality.
A second dramatic decrease was seen in two
multisite cohort studies that enrolled patients after
the 1999 ACOG guideline on VBAC was released
(Gregory et al., 2008; Landon et al., 2006). How-
ever, during the same time period of 1982 to 2002,
the vaginal delivery rates with TOL (shown by the
squares) have remained relatively constant, fluc-
tuating around 70%.
Although the evidence is lean, these findings sug-
gest that practice changed with the emersion ofnew evidence
(McMahon, 1996) and a new VBAC
guideline (ACOG, 1999). We then examined the
studies for ways that practice may have changed,
for example, not allowing women with more than
oneprior cesareanor a certain type of scar to have
a TOL, reduction in either induction, or epidural
use. Many studies did not report the proportion
of women with more than one prior cesarean or
who had a certain type of scar or the proportion
who were induced or had epidurals (DiMaio, 2002;
Gregory, 1999; Gregory et al., 2008; Loebel, 2004;
Pickhardt et al., 1992; Troyer & Parisi, 1992). De-
scriptively, it appeared that studies enrolled fewer
and fewer women with more than one prior ce-
sarean over time. Studies completed before 1996
reported that 19% (Stovall, 1987) to 23% (Phe-
lan, 1987) of women with a TOL had more than
one prior cesarean. For studies launched in 1996,
between 9% (Macones et al., 2005) and 19% (De-
Franco et al., 2007) of women with a TOL hadmore than one
cesarean. However, the large Na-
tional Institute of Child Health and Human Devel-
opment Maternal - Fetal Medicine Units Network
(MFMU) study launched in 1999 reported only 5%
of women had more than a single prior cesarean
(Landon et al., 2006). We did not observe a con-
sistent change over time in TOL eligibility based
on type of scar (DiMaio, 2002; Durnwald & Mer-
cer, 2004b; Flamm, 1994; Landon et al., 2006;
JOGNN 2012; Vol. 41, Issue 5 591
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
10/16
R E V I E W TOL and VBAC rates
Women delivering in hospitals with higher delivery volumes,
tertiary care centers, and teaching hospitals were more likely
to
have a trial of labor.
Loebel, 2004; Macones et al., 2005; Phelan, 1987;Stovall, 1987;
Troyer & Parisi, 1992), use of induc-
tion, (DeFranco et al., 2007; Durnwald & Mercer,
2004b; Hook, 1997; Landon et al., 2006; Phelan,
1987; Stovall, 1987) or epidural (Durnwald & Mer-
cer, 2004b; Fisler, 2003; Landon et al., 2006; Sto-
vall, 1987).
Most evidence of TOL and vaginal delivery rates
after TOL are from studies based in large tertiary
care centers and are highly variable. Because
the vaginal delivery rate has not improved with
a smaller pool of women, we sought evidence
on whether characteristics of the delivery systemor the patient
contributed to the decision about
whether a TOL was offered.
What Factors Contributed to an Option
of a TOL?
Six good cohort studies (Cameron, 2004; Chang,
2008; DeFranco et al., 2007; Harper et al., 2009;
McMahon, 1996; Pang, 2009), three fair quality
cohort studies (Bujold, 2001; Hueston & Rudy,
1994; Selo-Ojeme, 2008), and one good quality
cross-sectional study (Kabir, 2005) reported fac-
tors that may have contributed to whether women
were offered a TOL. Two themes emerged fromthese studies related
to site of delivery and the
woman’s history of a prior vaginal delivery.
Women delivering in hospitals with higher deliv-
ery volumes, tertiary care centers, and teaching
hospitals were more likely to have a TOL (Table 2)
(Cameron, 2004; DeFranco et al., 2007; Hueston
& Rudy, 1994; McMahon, 1996). Delivery volume
in teaching hospitals predicted TOL in one ret-
rospective cohort study conducted in 1990 and
1991, even when adjusted by race, employment,
marital status, and obstetric risk (Hueston & Rudy,
1994).
Level of care also appeared to influence the deci-
sion for a TOL (Table 2). In one study women had
an increased likelihood of TOL if they delivered
at a Level 5 or 6 hospital (metro district hospital
for high-risk mothers/babies or perinatal center)
and a decreased likelihood at a Level 4 or below
(metro district for moderate-risk mothers/babies,
rural, and private hospitals) (Cameron, 2004). In
this study of Australian deliveries during 1998 to
2001 (Cameron, 2004), predictors of TOL were
evaluated for 14,350 charts of women eligible for
TOL by the ACOG standards (1999). In a sepa-
rate study conducted in Nova Scotia, Canada, be-
tween 1986 and 1992, researchers similarly found
that women in community and regional hospitals
wereonehalf aslikely tohave a TOL aswomende-
livering in tertiary care centers (McMahon, 1996).
The presence of a residency program consistently
improved the likelihood that women were offered
TOLs (DeFranco et al., 2007; Kabir, 2005) when
compared to settings without residency programs.
In a secondary analysis of a retrospective study
(conducted in 1996–2000) (DeFranco et al., 2007)
of 17 hospitals, women delivering in hospitals that
did not have an obstetric/gynecology residency
program were less likely to have a TOL (odds ratio
[OR] = .88, CI [0.82, 0.95]) even when adjusting
for age, obstetric history, birth weight, gestational
age, and maternal risks. In another secondary
analysis of the Agency for Healthcare Research
and Quality’s (AHRQ) 2001 Healthcare Cost and
Utilization Project (HCUP) National Inpatient Sam-
ple database, investigators reported that women
had a reduced likelihood of TOL if they were deliv-
ered in rural or nonteaching urban hospitals(Kabir,
2005). These investigators identified all women
who had unnecessary RCDs (had no discharge
indication, ICD-9 code, for a cesarean) as a way
to quantify the number of women who may not
have been offered a TOL; the database includes
data from 33 states. In this study, a prior cesareanalone was
not considered as sufficient justification
for a RCD. With this definition, 65% of RCDs were
considered unnecessary and overall bed size of
the hospital was not related to unnecessary RCDs.
When providers consider whether to offer the op-
tion of a TOL after a prior cesarean, careful at-
tention is given to prior obstetric history in es-
timating likelihood of VBAC. Three retrospective
cohort studies, (Cameron, 2004; McMahon, 1996;
Pang, 2009) and a secondary analysis (Harper
et al., 2009) of a large retrospective study (Ma-
cones et al., 2005) examined whether obstetricfactors such as
number of prior vaginal deliv-
eries or gestational age at the prior cesarean
predicted whether women had a TOL (Table 3).
The likelihood of TOL increased (OR ranged from
1.51 to 6.67) for women with prior vaginal de-
liveries (Cameron, 2004; McMahon, 1996; Pang,
2009) whereas it decreased for women who had
a prior cesarean before 34 weeks gestational age
(Harper et al., 2009).
592 JOGNN, 41, 583-598; 2012. DOI: 10.1111/j.1552-
6909.2012.01388.x http://jognn.awhonn.org
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
11/16
Eden, K.B. et al. R E V I E W
DiscussionVaginal delivery rates for women who had a TOL
have remained constant over the same time pe-
riod. Since 1996, the number of women who had
a TOL at sites still offering TOLs fell to less than
one half of those eligible. Among women who had
a TOL, 74% delivered vaginally. The vaginal deliv-ery rate with
TOL in this updated evidence report is
consistent with the previously reported rate (76%)
in the 2003 evidence report on VBAC (Guise et al.,
2003). The newer evidence suggests that many
women who would have delivered vaginally had
elective cesarean deliveries either by own choice
or because of barriers in the health system. It is
important to note that the TOL and vaginal deliv-
ery rates with TOL summarized in this report were
obtained from sites that still provided TOLs. Our
reported vaginal delivery rates with TOL will ex-
ceed reported national VBAC rates that include
sites that limit (or prohibit) TOLs.
With newly issued concluding consensus state-
ments, rates of TOL may again increase for stud-
Since 1996, the number of women who had a trial of labor atsites
still offering this option fell to less than one half of those
eligible.
ies launched after 2010. The 2010 Consensus De-
velopment Panel on VBAC urged that barriers to
TOL be removed to again give a woman an op-
portunity to make an informed choice with her
provider: “We recommend that hospitals, mater-
nity care providers, healthcare and professional
liability insurers, consumers, and policymakers
collaborate on the development of integrated ser-
vices that could mitigate or even eliminate current
barriers to TOL” (U.S. Department of Health and
Human Services, 2010, p. 3).
Although some barriers are obvious to the patient,
for example, the hospital will not allow TOLs, ef-
forts are needed to address less obvious barriers
(to the patient), such as liability to the provider.
In a survey of ACOG fellows, 41% of the 639
Table 2: Characteristics of Delivery Sites and Likelihood of
TOL
Author, Year Characteristic Adjusted Odds 95% CI
Ratio for TOL
Volume of Deliveries
Hueston & Rudy, 1994 252 women with prior CD/2y 1.00
Referent
135 women with prior CD/2y 0.46 0.29, 0.74
179 women with prior CD/2y 0.57 0.38, 0.85
193 women with prior CD/2y 0.38 0.25, 0.56
Hospital Level
Cameron, 2004 Level 6 (Perinatal center) 1.00 Referent
Level 5 (High-risk care) 1.22 1.09, 1.37
Level 4 (moderate-risk care) 0.90 0.81, 0.99
Level 1–3 (Rural)a 0.66 0.58, 0.74
Private 0.45 0.41, 0.50
McMahon, 1996 Tertiary care 1.00 Referent
Regional hospital 0.50 0.50, 0.60
Community hospital 0.40 0.30, 0.50
Teaching St atus
DeFranco, 2007 Obstetrics/Gynecology Residency program 1.00
Referent
No program 0.88 0.82, 0.95
Note. CD = cesarean delivery; CI = confidence interval; TOL
= trial of labor; y = year(s).Adapted with permission from Guise,
J. M., Eden, K., Emeis, C., Denman, M., Marshall, N., Fu, R., . . .
McDonagh, M. (2010). Vaginal
birth after cesarean: New insights. Evidence report/technology
assessment no. 191 (AHRQ publication no. 10-E001).
Rockville, MD:Agency for Healthcare Research and Quality.a96% rural
hospitals.
JOGNN 2012; Vol. 41, Issue 5 593
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
12/16
R E V I E W TOL and VBAC rates
Many patients may not be aware of risks and benefits or
prepared to advocate for their desired mode of delivery.
respondents cited “fear of liability” as one of many
“most important” factors to consider in advisingpatients about
whether to have a TOL (Coleman
et al., 2005). Similarly, investigators of a retro-
spective cohort study (Yang, Mello, Subramanian,
& Studdert, 2009) estimated that a decrease of
$10,000 (in 2003 dollars) in the malpractice pre-
mium (equivalent to a 20%–25% average premium
decrease for OB/GYNs) would have translated to
1,600 more VBACs and 6,000 fewer cesarean de-
liveries (including 3,600 fewer primary cesarean
deliveries), nationally in 2003.
The dawn of the economic recession in 2007 may
have augmented provider and insurer rationale forlow TOL rates
over the past 3 years. In a time
where most businesses are looking to cut costs
and fear of litigation remains high, changing pol-
icy to allow VBAC may be viewed as too risky
financially to implement. In addition to decreasing
TOL rates, it is important to note a striking de-
cline in the U.S. birth rate since 2007. The April
2010 Pew Research Center birth trends report
(compiled using data from the 25 states with fi-
nal 2008 birth numbers) shows that the national
U.S. birth rate grew steadily from 2003 to 2007,
then sharply declined by 2% from 2007 to 2008,
and has steadily decreased since (Livingston &Cohn, 2010).
Popular media outlets, such as The
New York Times and National Public Radio have
explored this topic, noting that many women are
focusing more on contraceptive use than family
growth because they are concerned about the
cost of raising children in a down economy (As-
sociated Press, 2010; Siegal, 2010). As individ-
ual hospitals lose revenue due to declining birth
rates, it will be interesting to analyze the effect of
the 2010 Clinical Management Guidelines (ACOG,
2010) on TOL.
Nursing Implications
National guidelines on VBAC from the Royal Col-
lege of Obstetricians and Gynaecologists in the
United Kingdom and Women’s Hospital Australa-
sia (Australia) emphasize the importance of of-
fering women information so that they can dis-
cuss the childbirth options(Foureur, Ryan, Nicholl,
& Homer, 2010). Although U.S. providers report
knowing the risks and benefits of VBAC and RCD
(Coleman et al., 2005), it is not clear that manypatients are
aware of such risks and benefits or
are prepared to advocate for their desired mode of
delivery. Perinatal nurses, nurse practitioners, and
certified nurse midwives are well positioned to as-
sess women’s knowledge about delivery options
and their associated risks and benefits. When
knowledge is lacking, they can provide education
and counseling to address this need.
The importance of informing patients also
emerged in the vision statement from Childbirth
Connection’s Transforming Maternity Care, a col-
laboration of 100 national leaders representing ob-stetrics,
nurse-midwifery, maternity nursing, family
medicine, health policy, health economics, quality,
Table 3: Past Obstetric Factors as Predictors of Trial of
Labor
Author, Year Study Design Characteristic Adjusted odds 95%
CI
Ratio or Relative
Risk for VBAC
Number of Previous Vaginal Deliveries
Cameron, 2004, Retrospective Cohort 1 Prior VD 1.51 1.35,
1.68
2 Prior VDs 2.35 1.92, 2.86
≥3 Prior VDs 2.94 2.23, 3.88
McMahon, 1996, Retrospective Cohort 1 Prior VD 3.20 Not
reported
2 Prior VDs 4.00 Not reported
Pang, 2009, Retrospective Cohort History of VD 6.67 2.70,
16.67
Note. CI = confidence interval; VD = vaginal delivery; VBAC
= vaginal birth after cesarean.Reprinted with permission from
Guise, J. M., Eden, K., Emeis, C., Denman, M., Marshall, N., Fu,
R., . . . McDonagh, M. (2010). Vaginal birth after
cesarean: New insights. Evidence Report/Technology Assessment No.
191 (AHRQ publication no. 10-E001). Rockville, MD:Agency for
Healthcare Research and Quality.
594 JOGNN, 41, 583-598; 2012. DOI: 10.1111/j.1552-
6909.2012.01388.x http://jognn.awhonn.org
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
13/16
Eden, K.B. et al. R E V I E W
patient safety, childbirth education, maternal fetal
medicine, and health consumer advocacy (Carter
et al., 2010). One of the guiding principles for their
2020 vision presented in April 2009 was to pro-
vide women with the opportunity to make informed
choices (Carter et al.). To make this vision a re-
ality, future work is needed in creating evidence-
based patient education products (brochures, de-
cision aids) designed using plain language so that
women feel informed and prepared to enter into a
dialog about birth choice. Additionally, future work
is needed to integrate these tools into current clini-
cal practice and may require health care providers
to adopt a shared style of decision making that
uses this new technology (Shorten, 2010). Less
than a year after the Childbirth’s Connections’ vi-
sion statement waspresented, the NIHVBAC Con-
sensus Development panel echoed the same sen-
timent but with an emphasis on shared decision
making among informed patients and providers:
“Information, including risk assessment, should be
shared withthe woman at a level and pace that she
can understand. When both TOL and ERCD are
medically equivalent options, a shared decision
making process should be adopted and, when-
ever possible, the woman’s preference should be
honored” (U.S. Department of Health and Human
Services, 2010, p. 33).
AcknowledgmentBased on a systematic evidence review con-
ducted for and presented to the National Institutes
of Health Consensus Development Conferenceon Vaginal Birth After
Cesarean: New Insights.
Funded by the Agency for Healthcare Research
and Quality (AHRQ), Contract No. HHSA 290-
2007-10057-I, Task Order No. 4 for the Office of
Medical Applications of Research at the National
Institutes of Health. The findings and conclusions
in this document are those of the authors, who are
responsible for its content, and do not necessarily
represent the views of AHRQ. No statement in this
report should be construed as an official position
of AHRQ or of the U.S. Department of Health and
Human Services.
REFERENCESAmerican College of Obstetricians and Gynecologists.
(1999). ACOG
practice bulletin. Vaginal birth after previous cesarean
delivery.
Number 5, July 1999 (replaces practice bulletin number 2,
Oc-
tober 1998). Clinical management guidelines for
obstetrician-
gynecologists. American College of Obstetricians and
Gynecol-
ogists. (1999). International Journal of Gynaecology
& Obstet-
rics , 66 (2), 197–204.
American College of Obstetricians and Gynecologists. (2010).
ACOG
practice bulletin no. 115: Vaginal birth after previous ce-
sarean delivery. Obstetrics &
Gynecology , 116 (2, Part 1), 450–
463.
Associated Press. (August 28, 2010). Birthrate is lowest in a
century.
The New York Times, A11.
Bais, J. M., van der Borden, D. M., Pel, M., Bonsel, G. J.,
Eskes, M.,
van der Slikke, H. J., & Bleker, O. P. (2001). Vaginal birth
after
caesarean section in a population with a low overall
caesarean
section rate. European Journal of Obstetrics, Gynecology,
& Re-
productive Biology , 96 (2), 158–162.
Bujold, E., & Gauthier, R. J. (2001). Should we allow a
trial of labor after
a previous cesarean for dystocia the second stage of labor?
Obstetrics & Gynecology , 98 (4),
652–655.
Cameron, C. A., Roberts, C. L., & Peat, B. (2004).
Predictors of labor
and vaginal birth after cesarean section. International
Journal of
Gynaecology & Obstetrics , 85 (3),
267–269.
Carter, M., Corry, M., Delbanco, S., Foster, T., Friedland, R.,
Gabel,
R., . . . Simpson, K. R. (2010). 2020 vision for a
high-quality,
high-value maternity care system. Women’s Health
Issues , 20 (1
Suppl), S7–17.
Caughey, A. B., Shipp, T. D., Repke, J. T., Zelop, C. M., Cohen,
A.,
& Lieberman, E. (1999). Rate of uterine rupture during a
trial
of labor in women with one or two prior cesarean deliveries.
American Journal of Obstetrics & Gynecology ,
181(4), 872–
876.
Chang, J. J., Stamilio, D. M., & Macones, G. A. (2008).
Effect of hospi-
tal volume on maternal outcomes in women with prior cesarean
delivery undergoing trial of labor. American Journal of
Epidemi-
ology , 167 (6), 711–718.
Coleman, V. H., Erickson, K., Schulkin, J., Zinberg, S., &
Sachs, B. P.
(2005). Vaginal birthafter cesarean delivery: Practice patterns
of
obstetrician-gynecologists. Journal of Reproductive
Medicine ,
50 (4), 261–266.
Costantine, M. M., Fox, K., Byers, B. D., Materus, J.,
Ghulmiyyah, L.
M., Blackwell, S., . . . Saade, G. (2009). Validation of the
predic-
tion model for success of vaginal birth after cesarean
delivery.
Obstetrics & Gynecology , 114 (5),
1029–1033.
DeFranco, E. A., Rampersad, R., Atkins, K. L., Odibo, A. O.,
Stevens,
E. J., Peipert, J. F., . . . Macones, G. A. (2007). Do vaginal
birth
after cesarean outcomes differ based on hospital
setting? Amer-
ican Journal of Obstetrics & Gynecology ,
197 (4), 400.e401–
406.
Delaney, T., & Young, D. C. (2003). Spontaneous versus
induced labor
after a previous cesarean delivery. Obstetrics &
Gynecology ,
102 (1), 39–44.
DerSimonian, R., & Laird, N. (1986). Meta-analysis in
clinical trials.
Controlled Clinical Trials , 7 (3), 177–188.
DiMaio, H., Edwards, R. K., Euliano, T. Y., Treloar, R. W.,
& Cruz, A. C.
(2002). Vaginal birth after cesarean delivery: An historic
cohort
cost analysis. American Journal of Obstetrics &
Gynecology ,
186 (5), 890–892.
Dinsmoor, M. J.,& Brock, E.L. (2004).Predictingfailedtrial
oflabor after
primary cesarean delivery. Obstetrics &
Gynecology , 103 (2),
282–286.
Durnwald, C. P., Ehrenberg, H. M., & Mercer, B. M. (2004a).
The im-
pact of maternal obesity and weight gain on vaginal birth
after
cesarean section success. American Journal of Obstetrics
&
Gynecology , 191(3), 954–957.
Durnwald, C. P., & Mercer, B. (2004b). Vaginal birth after
Cesarean
delivery: Predictingsuccess,risks of failure. Journal of
Maternal-
Fetal & Neonatal Medicine , 15 (6),
388–393.
Eden, K. B., McDonagh, M., Denman, M. A., Marshall, N., Emeis,
C.,
Fu, R., . . . Guise, J. M. (2010). New insights on vaginal
birth
after cesarean, can it be predicted? Obstetrics &
Genecology ,
116 (4), 967–981.
JOGNN 2012; Vol. 41, Issue 5 595
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
14/16
R E V I E W TOL and VBAC rates
El-Sayed, Y. Y., Watkins, M. M., Fix, M., Druzin, M. L., Pullen,
K. M., &
Caughey, A. B. (2007). Perinatal outcomes after successful
and
failed trials of labor after cesarean delivery. American
Journal
of Obstetrics & Gynecology , 196 (6),
583.e581–585; discussion
583.e585.
Elkousy, M. A., Sammel, M., Stevens, E., Peipert, J. F., &
Macones,
G. (2003). The effect of birth weight on vaginal birth after
cesareandelivery success rates.AmericanJournal of
Obstetrics
& Gynecology , 188 (3), 824–830.
Fisler, R. E., Cohen, A., Ringer, S. A., & Lieberman, E.
(2003). Neona-
tal outcome after trial of labor compared with elective
repeat
cesarean section. Birth , 30 (2), 83–88.
Flamm, B. L., Goings, J. R., Fuelberth, N. J., Fischermann, E.,
Jones,
C., & Hersh, E. (1987). Oxytocin during labor after previous
ce-
sarean section: Results of a multicenter study. Obstetrics
& Gy-
necology , 70 (5), 709–712.
Flamm, B. L., Goings, J. R., Liu, Y., & Wolde-Tsadik, G.
(1994). Elec-
tive repeat cesarean delivery versus trial of labor: A
prospec-
tive multicenter study. Obstetrics & Gynecology ,
83 (6), 927–
932.
Foureur, M., Ryan, C. L., Nicholl, M., & Homer, C. (2010).
Inconsistent
evidence: Analysis of six national guidelines for vaginal
birth
after cesarean section. Birth , 37 (1),
3–10.
Gonen, R., Nisenblat, V., Barak, S., Tamir, A., & Ohel, G.
(2006). Results
of a well-defined protocol for a trial of labor after prior
cesarean
delivery. Obstetrics &
Gynecology , 107 (2 Pt 1), 240–245.
Goodall, P. T., Ahn, J. T., Chapa, J. B., & Hibbard, J. U.
(2005). Obesity
as a risk factorforfailed trial oflaborin patients with previous
ce-
sarean delivery. American Journal of Obstetrics &
Gynecology ,
192 (5), 1423–1426.
Gregory, K. D., Korst, L. M., Cane, P., Platt, L. D., &
Kahn, K. (1999).
Vaginal birth after cesarean and uterine rupture rates in
Califor-
nia. Obstetrics & Gynecology , 94 (6),
985–989.
Gregory, K.D., Korst, L. M.,Fridman,M., Shihady,I.,
Broussard,P., Fink,
A., . . . Burnes Bolton, L. (2008). Vaginal birth after
cesarean:
Clinical risk factors associated with adverse
outcome. Ameri-
can Journal of Obstetrics &
Gynecology , 198 (4), 452.e451–410;
discussion 452.e410–452.
Guise,J. M.,Denman,M.,Emeis, C.,Marshall,N.,Walker,M.,Fu, R., .
. .
McDonagh,M. (2010). Vaginalbirth after cesarean:New insights
on maternal and neonatal outcomes. Obstetrics &
Gynecology ,
115 (6), 1267–1278.
Guise, J. M., Eden, K., Emeis, C., Denman, M., Marshall, N., Fu,
R.,
. . . McDonagh, M. (2010). Vaginal birth after cesarean:
New in-
sights. Evidence report/technology assessment No. 191
(AHRQ
Publication No. 10-E001) . Rockville, MD: Agency for
Healthcare
Research and Quality.
Guise, J. M., McDonagh, M. S., Hashima, J., Kraemer, D. F.,
Eden,
K. B., Berlin, M., . . . Helfand, M. (2003). Vaginal birth
after ce-
sarean (VBAC). Evidence report: Technology assessment No.
71 (AHRQ Publication No. 03-E018) . Rockville, MD: Agency
for
Healthcare Research and Quality.
Gyamfi,C., Juhasz, G.,Gyamfi, P.,& Stone,J.
L.(2004).Increased suc-
cess of trial of labor after previous vaginal birth after
cesarean.
Obstetrics & Gynecology , 104 (4),
715–719.
Hammoud, A., Hendler, I., Gauthier, R. J., Berman, S.,
Sansregret, A.,
& Bujold, E. (2004). The effect of gestational age on trial
of la-
bor after cesarean section. Journal of Maternal-Fetal &
Neonatal
Medicine , 15 (3), 202–206.
Harper, L. M., Cahill, A. G., Stamilio, D. M., Odibo, A. O.,
Peipert, J. F.,
& Macones, G. A. (2009). Effect of gestational age at the
prior
cesarean delivery on maternal morbidity in subsequent VBAC
attempt. American Journal of Obstetrics &
Gynecology , 200 (3),
276.e271–276.
Harris, R. P., Helfand, M., Woolf, S. H., Lohr, K. N., Mulrow,
C. D.,
Teutsch, S. M., & Atkins, D. (2001). Current methods of the
U.S.
Preventive Services Task Force: A review of the process.
Ameri-
can Journal of Preventive Medicine , 20 (3, Suppl
1), 21–35.
Hashima, J. N., & Guise, J. M. (2007). Vaginal birth after
cesarean: A
prenatal scoring tool. American Journal of Obstetrics
& Gyne-
cology , 196 (5), e22–23.
Healthy Inclusion. (2001). Undertaking systematic reviews
of re-
search on effectiveness: CRD’s guidance for those
carry-
ing out or commissioning reviews . Retrieved from
http://www.
healthy-inclusion.org.uk/
Hendler, I., & Bujold, E. (2004). Effect of prior vaginal
delivery or
prior vaginal birth after cesarean delivery on obstetric
outcomes
in women undergoing trial of labor. Obstetrics &
Gynecology ,
104 (2), 273–277.
Hibbard, J. U., Gilbert, S., Landon, M. B., Hauth, J. C.,
Leveno, K.
J., Spong, C. Y., . . . Gabbe, S. G. (2006). Trial of labor or
re-
peat cesarean delivery in women with morbid obesity and pre-
vious cesarean delivery. Obstetrics &
Gynecology , 108 (1), 125–
133.
Higgins, J. P., Thompson, S. G., Deeks, J. J., & Altman, D.
G. (2003).
Measuring inconsistency in meta-analyses. British Medical
Jour-
nal , 327 (7414), 557–560.
Higgins, J. P., Thompson, S. G., Higgins, J. P. T., &
Thompson, S. G.
(2002). Quantifying heterogeneity in a meta-analysis.
Statistics
in Medicine , 21(11), 1539–1558.
Hollard, A. L., Wing, D. A., Chung, J. H., Rumney, P. J., Saul,
L., Na-
geotte, M.P.,& LagrewD. (2006). Ethnicdisparity in
thesuccess
of vaginal birth after cesarean delivery. Journal of
Maternal-Fetal
& Neonatal Medicine , 19 (8), 483–487.
Hook,B.,Kiwi,R.,Amini, S.B.,Fanaroff,A.,& Hack,M. (1997).
Neonatal
morbidityafter electiverepeatcesareansectionand trialof
labor.
Pediatrics , 100 (3 Pt 1), 348–353.
Horenstein, J. M., Eglinton, G. S., Tahilramaney, M. P.,
Boucher, M.,
& Phelan, J. P. (1984). Oxytocin use during a trial of labor
in
patientswith previous cesareansection. Journal of
Reproductive
Medicine , 29 (1), 26–30.
Horenstein, J. M.,& Phelan, J. P. (1985). Previous cesarean
section:The
risks and benefits of oxytocin usage in a trial of labor.
American
Journal of Obstetrics & Gynecology , 151(5),
564–569.
Hoskins, I. A., & Gomez, J. L. (1997). Correlation between
maximum
cervical dilatation at cesarean delivery and subsequent
vaginal
birth after cesarean delivery. Obstetrics &
Gynecology , 89 (4),
591–593.
Huang, W. H., Nakashima, D. K., Rumney, P. J., Keegan, K. A.
Jr., &
Chan,K. (2002). Interdelivery interval and thesuccess of
vaginal
birth after cesarean delivery. Obstetrics &
Gynecology , 99 (1),
41–44.
Hueston, W. J., & Rudy, M. (1994). Factors predicting
elective repeat
cesarean delivery. Obstetrics & Gynecology ,
83 (5 Pt 1), 741–
744.
Jakobi, P., Weissman, A., Peretz, B. A., & Hocherman, I.
(1993). Eval-
uation of prognostic factors for vaginal delivery after
cesarean
section. Journal of Reproductive
Medicine , 38 (9), 729–733.
Johnson, C., Oriol, N., & Flood, K. (1991). Trial of labor:
A study of 110
patients. Journal of Clinical Anesthesia ,
3 (3), 216–218; discus-
sion 214–215.
Juhasz, G., Gyamfi, C., Gyamfi, P., Tocce, K., & Stone, J.
L. (2005). Ef-
fect of body mass index and excessive weight gain on success
of vaginal birth after cesarean delivery. Obstetrics
& Gynecol-
ogy , 106 (4), 741–746.
Kabir, A. A., Pridjian, G., Steinmann, W. C., Herrera, E. A.,
& Khan,
M. M. (2005). Racial differences in cesareans: An analysis
of
U.S. 2001 National Inpatient Sample Data [Erratum appears in
596 JOGNN, 41, 583-598; 2012. DOI: 10.1111/j.1552-
6909.2012.01388.x http://jognn.awhonn.org
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
15/16
Eden, K.B. et al. R E V I E W
Obstet Gynecol. 2005 Jun;105(6):1495]. Obstetrics &
Gynecol-
ogy , 105 (4), 710–718.
Kugler, E., Shoham-Vardi, I., Burstien, E., Mazor, M., &
Hershkovitz,
R. (2008). The safety of a trial of labor after cesarean
section
in a grandmultiparous population. Archives of Gynecology
&
Obstetrics , 277 (4), 339–344.
Landon, M.B., Spong,C. Y.,Thom,E.,Hauth,J. C.,Bloom,S.
L.,Varner,
M. W., . . . Gabbe, S. G. (2006). Risk of uterine rupture with
a
trial of labor in women with multiple and single prior
cesarean
delivery. Obstetrics &
Gynecology , 108 (1), 12–20.
Learman, L. A., Evertson, L. R., & Shiboski, S. (1996).
Predictors of
repeatcesarean delivery aftertrialof labor:do anyexist?
Journal
of the American College of Surgeons , 182 (3),
257–262.
Lieberman, E., Ernst, E. K., Rooks, J. P., Stapleton, S., &
Flamm, B.
(2004). Results of the national study of vaginal birth after
ce-
sarean in birth centers. Obstetrics & Gynecology ,
104 (5 Pt 1),
933–942.
Livingston, G., & Cohn, D. V. (2010). U.S. birth rate
decline linked
to recession . Washington, DC: Pew Research Center. Re-
trieved January 19, 2012, from
http://pewsocialtrends.org/files/
2010/10/753-birth-rates-recession.pdf
Locatelli, A., Regalia, A. L., Ghidini, A., Ciriello, E., Biffi,
A., & Pezzullo,
J. C. (2004). Risks of induction of labour in women with a
uterine
scar from previous low transverse caesarean section.
BJOG:
An International Journal of Obstetrics &
Gynaecology , 111(12),
1394–1399.
Loebel, G., Zelop, C. M., Egan, J. F. X., & Wax, J. (2004).
Maternal
and neonatal morbidity after elective repeat cesarean
delivery
versus a trial of labor after previous cesarean delivery in a
com-
munity teaching hospital. Journal of Maternal-Fetal &
Neonatal
Medicine , 15 (4), 243–246.
Macones, G. A., Peipert, J., Nelson, D. B., Odibo, A., Stevens,
E. J.,
Stamilio,D. M., . . . Ratcliffe,S. J.
(2005).Maternalcomplications
with vaginal birth after cesarean delivery: a multicenter
study.
American Journal of Obstetrics & Gynecology ,
193 (5), 1656–
1662.
Martin, J. A., Hamilton, B. E., Sutton, P. D., Ventura, S. J.,
Mathews, T.
J., Kirmeyer, S., & Osterman, M. J. (2010). Births: Final
data for
2007. National Vital Statistics
Reports , 58 (24), 1–85.
McMahon, M. J., Luther, E. R., Bowes, W. A. Jr., & Olshan,
A. F. (1996).
Comparison of a trial of labor with an elective second
cesarean
section. New England Journal of
Medicine , 335 (10), 689–695.
McNally, O. M., & Turner, M. J. (1999). Induction of labour
after 1
previous caesarean section. Australian & New Zealand
Journal
of Obstetrics & Gynaecology , 39 (4),
425–429.
Menacker, F., Declercq, E., & Macdorman, M. F. (2006).
Cesarean de-
livery: Background, trends, and epidemiology. Seminars in
Peri-
natology , 30 (5), 235–241.
Nguyen, T. V., Dinh, T. V., Suresh, M. S., Kinch, R. A., &
Anderson, G.
D. (1992). Vaginal birth after cesarean section at the
University
of Texas. Journal of Reproductive
Medicine , 37 (10), 880–882.
Obara, H., Minakami, H., Koike, T., Takamizawa, S., Matsubara,
S.,
& Sato, I. (1998). Vaginal birth after cesarean delivery:
Results
in 310 pregnancies. Journal of Obstetrics &
Gynaecology Re-
search , 24 (2), 129–134.
Ouzounian, J. G., Miller, D. A., & Paul, R. H. (1996).
Amnioinfusion
in women with previous cesarean births: A preliminary
report.
American Journal of Obstetrics &
Gynecology , 174 (2), 783–786.
Pang, M. W., Law, L. W., Leung, T. Y., Lai, P. Y., & La, T.
K. (2009).
Sociodemographic factors and pregnancy events associated
with women who declined vaginal birth after cesarean
section.
European Journal of Obstetrics, Gynecology, &
Reproductive
Biology , 143 (1), 24–28.
Pathadey, S. D., Van Woerden, H. C., & Jenkinson, S. D.
(2005). Induc-
tionof labour after a previous caesareansection:A
retrospective
study in a district general hospital. Journal of
Obstetrics & Gy-
naecology , 25 (7), 662–665.
Phelan, J. P., Clark, S. L., Diaz, F., & Paul, R. H. (1987).
Vaginal birth
after cesarean. American Journal of Obstetrics &
Gynecology ,
157 (6), 1510–1515.
Pickhardt, M. G., Martin, J. N. Jr., Meydrech, E. F., Blake, P.
G., Martin,
R. W., Perry, K. G. Jr., & Morrison, J. C. (1992). Vaginal
birth after
cesarean delivery: Are there useful and valid predictors of
suc-
cess or failure? American Journal of Obstetrics &
Gynecology ,
166 (6 Pt 1), 1811–1815; discussion 1815–1819.
Raynor, B. D. (1993). The experience with vaginal birth after
cesarean
delivery in a small rural community practice. American
Journal
of Obstetrics & Gynecology , 168 (1 Pt 1),
60–62.
Rozenberg, P., Goffinet, F., Phillippe, H. J., & Nisand, I.
(1996). Ultra-
sonographic measurement of lower uterine segment to assess
risk of defects of scarred uterus.
Lancet , 347 (8997), 281–284.
Rozenberg,P.,Goffinet,F.,Philippe,H. J.,& Nisand,
I.(1999).Thickness
of the lower uterine segment: Its influence in the management
of
patients with previous cesarean sections. European
Journal of
Obstetrics, Gynecology, & Reproductive
Biology , 87 (1), 39–45.
Sakala, E. P., Kaye, S., Murray, R. D., & Munson, L. J.
(1990). Oxytocin
use after previous cesarean: Why a higher rate of failed
labor
trial? Obstetrics & Gynecology , 75 (3
Pt 1), 356–359.
Scott, J. R. (2010). Solving the vaginal birth after cesarean
dilemma.
Obstetrics & Gynecology , 115 (6),
1112–1113.
Selo-Ojeme,D., Abulhassan,N., Mandal, R.,Tirlapur,S., &
Selo-Ojeme,
U. (2008). Preferredand actual delivery modeafter a
cesareanin
London, UK. International Journal of Gynaecology &
Obstetrics ,
102 (2), 156–159.
Shorten, A. (2010). Bridging the gap between mothers and
medicine:
“New Insights” from the NIH Consensus Conference on VBAC.
Birth , 37 (3), 181–183.
Siegal, R. (Narrator). (2010, August 25). Birth rates drop amid
falter-
ing economy [Radio broadcast]. In M. Martinez (Producer),
All
things considered . Washington, DC: National Public
Radio.
Smith, G. C. S., Pell, J. P., Cameron, A. D., & Dobbie, R.
(2002).
Risk of perinatal death associated with labor after previous
ce-
sarean delivery in uncomplicated term pregnancies. Journal
of
the American Medical Association , 287 (20),
2684–2690.
Smith, G. C. S., White, I. R., Pell, J. P., & Dobbie, R.
(2005). Predicting
cesarean section and uterine rupture among women attempting
vaginal birth after prior cesarean section.[see comment].
PLoS
Medicine/Public Library of Science , 2 (9), e252,
871–878.
Socol, M. L., & Peaceman, A. M. (1999). Vaginal birth after
cesarean:
An appraisal of fetal risk. Obstetrics &
Gynecology , 93 (5 Pt 1),
674–679.
Spaans, W. A., Sluijs, M. B., van Roosmalen, J., & Bleker,
O. P. (2002).
Risk factors at caesarean section and failure of subsequent
trial
of labour. European Journal of Obstetrics, Gynecology,
& Re-
productive Biology , 100 (2), 163–166.
Stovall, T. G., Shaver, D. C., Solomon, S. K., & Anderson,
G. D. (1987).
Trial of labor in previous cesarean section patients,
excluding
classical cesarean sections. Obstetrics &
Gynecology , 70 (5),
713–717.
Strong, J. M.,& McQuillan,K. (1996). Factors affecting mode
of delivery
in labour following a single previous birth by cesarean.
Journal
of Obstetrics & Gynaecology , 16 (5),
353–357.
Sutton, A. J., Abrams, K. R., Jones, D. R., Sheldon, T. A.,
& Song,
F. (2000). Methods for meta-analysis in medical
research . New
York, NY: John Wiley & Sons.
Thompson, S. G., & Sharp, S. J. (1999). Explaining
heterogeneity in
meta-analysis: A comparison of methods. Statistics in
Medicine ,
18 (20), 2693–2708.
JOGNN 2012; Vol. 41, Issue 5 597
-
8/19/2019 Trial of Labor and Vaginal Delivery Rates in Women
with Prev CS
16/16
R E V I E W TOL and VBAC rates
Troyer, L. R., & Parisi, V. M. (1992). Obstetric parameters
affecting suc-
cess ina trialof labor:Designation ofa scoring
system.American
Journal of Obstetrics & Gynecology , 167 (4
Pt 1), 1099–1104.
U.S. Department of Health and Human Services. National
Insti-
tutes of Health. (2010). NIH consensus development
confer-
ence statement: Vaginal birth after cesarean: New insights.
March 8–10, 2010 . Retrieved from
http://consensus.nih.gov/
2010/images/vbac/vbac_statement.pdf
van Gelderen, C. J., England, M. J., Naylor, G. A., &
Katzeff, T. C.
(1986). Labour in patients with a caesarean section scar.
The
place of oxytocin augmentation. South African Medical
Journal
Suid-Afrikaanse Tydskrif Vir
Geneeskunde , 70 (9), 529–532.
Vinueza, C. A., Chauhan, S. P., Barker, L., Hendrix, N. W.,
& Scardo, J.
A. (2000). Predicting the success of a trial of labor with a
simple
scoring system. Journal of Reproductive
Medicine , 45 (4), 332–
336.
Weinstein, D.,Benshushan, A., Tanos, V., Zilberstein, R., &
Rojansky, N.
(1996). Predictive score for vaginal birth after cesarean
section.
American Journal of Obstetrics &
Gynecology , 174 (1 Pt 1), 192–
198.
Wen, S. W., Rusen, I. D., Walker, M., Liston, R., Kramer, M. S.,
Bas-
kett, T., . . . Maternal Health Study Group, Canadian
Perinatal
Surveillance System. (2004). Comparison of maternal
mortality
and morbidity between trial of labor and elective cesarean
sec-
tion among women with previous cesarean delivery.
American
Journal of Obstetrics & Gynecology , 191(4),
1263–1269.
The world factbook . (2008). Washington, DC: Central
Intelligence
Agency.
Yang, Y. T., Mello, M. M., Subramanian, S. V., & Studdert,
D. M. (2009).
Relationship between malpractice litigation pressure and
rates
of cesarean section and vaginal birth after cesarean
section.
Medical Care , 47 (2), 234–242.
Yetman,T.J., & Nolan, T. E. (1989). Vaginal birthafter
cesarean section:
A reappraisal of risk. American Journal of Obstetrics &
Gynecol-
ogy , 161(5), 1119–1123.
Yogev, Y., Ben-Haroush, A., Lahav, E., H orowitz, E., Hod, M.,
& Kaplan,
B. (2004). Induction of labor with prostaglandin E2 in women
with previous cesarean section and unfavorable cervix.
Euro-
pean Journal of Obstetrics, Gynecology, & Reproductive
Biol-
ogy , 116 (2), 173–176.
Zelop, C. M., Shipp, T. D., Cohen, A., Repke, J. T., &
Lieberman,
E. (2001). Trial of labor after 40 weeks’ gestation in women
with prior cesarean. Obstetrics & Gynecology ,
97 (3), 391–
393.
Zweifler,J., Garza,A., Hughes, S.,Stanich, M.A., Hierholzer,
A.,& Lau,
M. (2006). Vaginal birth after cesarean in California: Before
and
after a change in guidelines. Annals of Family
Medicine , 4 (3),
228–234.
598 JOGNN 41 583-598; 2012 DOI: 10 1111/j 1552- 6909 2012 01388
x http://jognn awhonn org