Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2009) 62, 1497e1502
Treatment of large ischial ulcers communicatingwith the hip joint with proximal femoral resectionand reconstruction with a combined vastus lateralis,vastus intermedius and rectus femorismusculocutaneous flap
Tahsin Oguz Acarturk*
Department of Plastic, Reconstructive and Aesthetic Surgery, Cukurova University School of Medicine, Adana 01330, Turkey
Received 31 January 2008; accepted 19 April 2008
KEYWORDSVastus lateralis;Vastus intermedius;Rectus femoris;Pressure sore;Flap;Vacuum-assistedclosure;Lateral circumflexfemoral artery;Girdlestone arthroplasty
* Department of Plastic, Reconstruc532 6096409.
E-mail address: toacarturk@yahoo
1748-6815/$-seefrontmatterª2008Britdoi:10.1016/j.bjps.2008.04.063
Summary Pressure ulcers which communicate with the hip joint are very difficult to treat.Often, thehip joint is infectedwith osteomyelitis of theproximal femur resulting in bouts of sepsisandflap failure.Thesepatients requireproximal femoral resectionandwidedebridement inordertoeradicate the infection,which in turn results in largeanddeepcavities. Reconstruction requireseither a muscle flap or even a total thigh flap if the defect is very large and the pelvis is involved.
In a series of six ischial or ischio-trochanteric pressure sores communicating with the hip joint,following multiple serial debridements, the vastus lateralis, vastus intermedius and rectusfemoris muscles were raised as a single musculocutaneous flap (‘three muscle flap’), based onthe descending branch of the lateral femoral circumflex artery, and transposed into the defect.All patients were paraplegics and had signs of sepsis during admission. Two patients had priorfailed reconstructions within 3 months of admission and the others had not been operated onbefore.Theexternal skindefectof theulcers ranged from7� 5 cmto30� 12 cm. After 12 monthsfollow up there was no recurrence of pressure sores or sepsis.
The ‘three muscle flap’ offers the advantage of providing large bulk to fill deep cavities, whilepreserving the rest of the thigh. The flap elevation is fast and safe and the vascular pedicle is reli-able. This technique is not for simple pressure sores, but should be reserved for large pressuresores complicated with large cavities created after resection of the proximal femur.ª 2008 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
tive and Aesthetic Surgery, Cukurova University School of Medicine, Adana 01330, Turkey. Tel.: þ90
.com
ishAssociationofPlastic,ReconstructiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.

1498 T.O. Acarturk
Multiple large pressure ulcers are often seen in long termparaplegic patients, especially in neglected cases. In longstanding cases, these ulcers may extend and involve deeperstructures. When ischial or trochanteric pressure sorescommunicate with the hip joint a refractory form of thedisease is encountered. Even though a small pressure soremay be present on the surface, the patient may still havedeep, extensive, non-healing large cavities in the hip joint.Sometimes the presence of the communication is missed,resulting in persistent infection and fevers, recurrentosteomyelitis, pyoarthrosis, reconstructive failure, flapbreakdown, recurrent ulceration and draining sinuses. Inorder to achieve complete control of the disease, thefemoral head resection (Girdlestone arthroplasty) shouldbe performed with wide debridement resulting in deep andwide cavities.1e5 The use of the vastus lateralis muscle flapis useful in such cases.2e5 However, in some neglected longstanding cases the degree and duration of infection andinflammatory process is so extensive that wider areas of thefemur and acetabulum are involved and exposed. In addi-tion, the hip communicates with the ischial pressure sorethrough a wide draining sinus wound and involvement of theischial bone. Thus, in order to control the infection and theinflammatory process, large tissues need to be resected,which in turn result in huge cavities. Ordinarily for suchvery large pressure sores and cavities, where the hip joint isexposed and there is intractable infection in the pelvis,a total thigh and leg amputation has been used to recon-struct such large cavity defects.6
In this paper, we describe a series of cases where deepand wide ischial and trochanteric ulcers with exposed hipjoints with intractable infection are covered by a combinedvastus lateralis, vastus intermedius and rectus femoris flap(‘three muscle flap’) based on the lateral circumflexfemoral artery following proximal femoral resection. Thismethod provides larger bulk than a single muscle flap aswell as obviating the need to use a whole thigh as a flapwhen large cavities need to be filled.
Material and methods
Five consecutive paraplegic patients (six ulcers) with ischialpressure ulcers (single or combined) that were communi-cating with the hip joint were included in the study and thedata were collected prospectively.
The ulcers were examined manually to determine theexistence of communication with the hip joint, the depth ofthe cavity and involvement of the femoral head (Figure 1A).Cultures were obtained from the cavities. An initial radicaldebridement of the pressure sore, the cavity, surroundingfibrotic tissue and heterotrophic bone formations was per-formed in addition to the resection of the exposed femur(femoral head, neck and proximal femur) and debridementand curettage of the cartilage of the surface of theacetabulum (Figure 2A). In patients where the hip joint wasnot well visualised, an incision from the ischial pressuresore to the area overlying the joint was made extendinglaterally in the direction of the greater throchanter. Thebone was sent for biopsy and cultures. This was followed byseveral minor debridements. After each debridementdressing changes were applied to the cavity with 0.5%
Dakins solution for 2 days followed by vacuum-assistedclosure (VAC) for 6 days (Figure 3A).
Once the wound was ready for final closure, the patientwas placed in a semilateral decubitis position (Figures 1e3).After the hip joint cavity, pressure sore and edges of theskin were debrided, the width and the length of the skindefect was measured with the hip in semiflexed position.The distal edge skin island of the flap was placed 5 cmproximal to the upper edge of the patella. The midsection ofthe skin island was positioned over the intermuscularseptum between the vastus lateralis and rectus femorismuscles determined by a line drawn between the anteriorsuperior iliac spine and the supero-lateral edge of thepatella. The width of the flap was equal to the width of theskin defect. The length of flap was determined to beapproximately 50% longer than the length of the defect (thisprevented the pedicle of the flap being squeezed once theflap is transposed into the defect, as no tunnelling wasused). Once the skin island was cut, the incision continuedto the defect from the upper edge of the skin flap in order toopen the tunnel where the flap would lie. Later vastuslateralis, vastus intermedius and rectus femoris muscleswere raised from distal to proximal in an en-block fashionwithout exposing the descending branch of the lateralfemoral circumflex artery. The periosteum of the femur wasleft behind so as not to skeletonise the bone. The mostproximal part of the vastus lateralis on the femur, whichcorresponded to the area where the femur was resected,was detached from the bone to allow easy transposition ofthe flap. During this dissection, the vascular pedicle (lateralcircumflex femoral artery and its descending branch) laywithin these three muscles and was protected from anyinjury. The flap was transposed into the defect. Severalsutures were taken, over suction drains, between themuscle layer of the flap and deepest part of the woundcavity. Then, the flap was inserted to cover the bonystructures and the defect of the ischial pressure sore.Finally, the skin was closed in two layers. The donor areaswere closed primarily. The patient was not allowed to lie onthe flap for 2 weeks and hyperflexion of the hip was pre-vented by adequate positioning.
Results
There were four male and one female patients with an agerange of 16 to 57 years. There were two ischial ulcers, twoischio-gluteal ulcers, one ischio-sacro-gluteal ulcer and oneischio-trochanteric ulcer. One patient had bilateral ulcer-ation. The external skin defect of the ulcers ranged in sizefrom 7� 5 cm to 30� 12 cm. All ulcers communicated withthe hip joint. The duration of the ulcers ranged between 6and 30 years. Two patients had prior failed local flapcoverage of their pressure sores. The remaining threepatients had never been operated on before.
During the initial examination gross purulence wascoming from the hip joint and all patients had signs ofsepsis with recurrent high fever and chills which requiredhospital admission. The fever was relapsing over a 3 monthperiod before the patients were referred to our clinic andhad used multiple antibiotics. All patients had leukocytosisand high C-reactive protein levels. Bone biopsy and cultures

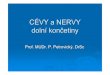
Figure 1 Patient with an ischial ulcer with a prior failed repair. (A) Ischial ulcer extending into the hip joint. (B) ‘Three muscleflap’ with skin island raised. (C) Wide resection of the proximal femur, acetabulum and ischial bone with the entire cavity opened.(D) Flap is transposed into the defect completely filling the cavity. The periosteum on the femur is preserved. (E) The defect isclosed. The donor area is closed primarily.
Treatment of large ischial ulcers communicating with the hip joint 1499
obtained at the initial debridement indicated osteomyelitisof the femur. The most common organism was Stahylo-coccus aureus followed by Enterococcus, Escherichia, Ser-ratia and Pseudomonas with all cultures beingpolymicrobial. Patients were placed on appropriate anti-biotics. All patients were chronically debilitated withanaemia and protein malnutrition. Before final recon-struction their general condition was improved with highprotein and calorie intake and correction of the anaemiawith blood transfusions when necessary.
The patients had an average of three (range 2e5)debridements before final closure, with the initialdebridement being the most radical one. In all patientsthere were heterotrophic bone formations which wereresected with the debridements. The patients received anaverage of 1.5 units (range 1e2 units) of transfused bloodbefore and an average of three units (range 2e4 units)during the final reconstructive procedure.
The width of the cutaneous portion of the flap rangedfrom 7 to 12 cm and the length ranged from 21 to 25 cm(Figures 1, 2). In one patient with an ischio-trochantericpressure sore, which communicated subcutaneously,a ‘three muscle flap’ with two separate skin islands of7� 5 cm was used (Figure 3). In five defects, the bulk of the
‘three muscle flap’ completely filled the cavity. In onepatient where the defect was extremely large, the vastusmedialis muscle was also included in the flap. There was noflap necrosis. All the donor defects were closed primarilywithout any wound breakdown. In one patient, there wasa 2 cm superficial dehiscence in the skin of the recipientarea which healed with local wound care. There were nohaematomas, seromas or flap failures.
The patients were followed up for an average of 12months (range 10 to 16 months). During this time there wasno recurrence of the disease at the operative site orrecurrence of sepsis. Two patients had small superficialpressure ulcers at the medial aspect of the ipsilateral kneewhich healed with local wound care. One patient with a 30-year history of pressure sores was diagnosed with epider-moid carcinoma at the initial debridement and later died ofmetastatic disease.
Discussion
Girdlestone arthroplasty is a technique to treat intractablehip infections.1 It is mostly used either after removal of aninfected hip prosthesis or in spinal cord injury patients with

Figure 2 Patient with an ischial pressure sore that was not previously operated on. (A) The cavity of the hip joint after severaldebridements before final closure. (B) Flap elevated and the skin bridge is opened. (C) Wide resection of the acetabulum, ischialbone and proximal femur creating a wide cavity. (D) Flap transposed and defect closed. Donor area is closed primarily.
1500 T.O. Acarturk
involvement of the femoral head. After resection, thecavity often needs to be filled with healthy tissue in orderto obliterate the dead space and prevent the pistoning ofthe femur against the acetabulum.
Meland et al. used a rectus femoris or a vastus lateralismuscle flap in the treatment of non-healing infected
Figure 3 Patient with an ischio-trochanteric pressure sore. (A)‘three muscle flap’ is raised with two separate island flaps. (C) Thtransposed. (E) Both defects are closed with skin islands of the fla
total-hip arthroplasties after the removal of the prosthesis(Gridlestone arthroplasty).7 In their series, simultaneousrectus femoris and vastus lateralis muscles were usedwhenever a single muscle flap was not enough to obliteratethe cavity. In several cases rectus abdominis was also addedto increase the bulk. All patients had re-implantation of the
The VAC treatment has created granulating surfaces. (B) Thee flap is elevated and the skin bridge is opened. (D) The flap isps and the muscle is placed into the cavity.

Treatment of large ischial ulcers communicating with the hip joint 1501
prosthesis 12 months after the muscle procedure withoutany complication. Jones et al. used pedicled vastus later-alis or free muscle flaps to fill cavity defects followingremoval of infected hip prosthesis with no recurrence ofinfection in any of the patients.8 Huang et al. have usedvastus lateralis musculocutaneous flaps when treatingdefects following removal of an infected prosthesis.9 Therecurrence of infection has been extremely rare in theseseries even after 50 years of chronic infection.7,8
Girdlestone arthroplasty and coverage with muscle flapsis also used in recalcitrant pressure sores which communi-cate with an infected hip joint. This is an even biggerproblem than patients with an infected prosthesis as thereis fibrosis, extensive scarring, inflammation, decreasedvascularity and heterotrophic bone formation around thewound, in a chronically debilitated patient who ismalnourished and partly immobilised.
The aim of the initial debridement is to create a singlewide open cavity by removal of the exposed femur. Thiswould facilitate dressing changes and prevents formation ofpockets which would later form abscess cavities. Theexposed femoral bone is usually avascular by the time ofthe operation, precluding any salvage procedure.8 In ourseries, resection was continued until clinically healthy bonetissue was encountered. In addition, due to extensivedestruction of the ligaments and soft tissue around the hipjoint there was frequently a dislocation. The wall of thecavity is typically fibrotic with decreased vascularity due torecurrent infections and multiple operations. The use ofvacuum-assisted closure enhanced the vascularity, createda granulating surface and removed the secretions, whichpromoted adherence of the muscle flap. Creating andmaintaining a single cavity throughout serial debridementsenabled complete filling and surfacing of the deep lesionwith the muscle flap in the final stage. The importance ofobliterating the dead space in chronic cavities to treat andprevent further infection cannot be overemphasised. Ifcomplete obliteration cannot be achieved, a simplesecondary closure or a small-sized flap for the cutaneousdefect is doomed to fail. In our series, there were twopatients with ischial pressure sores who had prior failedflaps. These were encountered within 3 months of theoperation and were possibly due to undiagnosed commu-nication with the hip joint and pyoarthroses. Manualexamination is the most important tool, but in difficultcases a sinography, CT scan or MRI can be obtained toconfirm hip joint involvement. Serial debridements areimportant in eradicating the infection and scarred tissuebefore final closure is attempted.
Mathes and Alpert were the first to report the use of thefemoral head resection followed by closure with a muscleflap in paraplegic patients.10 Klein et al. used the vastuslateralis muscle flap with a skin graft following proximalfemoral resection to treat ischial or trochanteric pressuresores communicating with the hip joint.2 They used anexternal fixator to prevent the pistoning of the flailingfemur against the acetabulum and movement in the flap,until complete healing was achieved. Rubayi et al., ina group of patients with trochanteric ulcers communicatingwith an infected hip joint, also used a similar technique ofresection followed by interposing a vastus lateralis muscleflap.3 They used a silastic cushion to keep the extremity
immobilised until healing occurred. In a group of septicparaplegic patients with pyoarthrosis and osteomyelitis ofthe femoral head, Evans et al. performed Girdlestonearthroplasty and coverage with various local muscle flaps(vastus lateralis, rectus femoris, biceps femoris, rectusabdominis).4 They did not use any stabilising devices, whichdid not adversely affect the outcome. In our series, we didnot use any stabilising devices other than simple positioningto prevent hyperflexion and frequent position changes.Schmidt et al. used a vastus lateralis musculocutaneous flapto cover simultaneous defects of the sacral and trochan-teric pressure sores following Girdlestone arthroplasty.5
The rate of recurrence of infection and pressure sores atthe original site was 0% and 4%, respectively, when histor-ical data from the literature are analysed.2e5 This isconcurrent with our findings. Thus, the method of proximalfemoral resection, wide excision and filling with a muscleflap is very effective.
Vastus lateralis as a muscle flap was first used by Ger andLevine in the treatment of pressure sores.11 Bovet et al.were the first to use the vastus lateralis as a myocutaneousflap in the treatment of trochanteric ulcers.12 Drimmer andKrasna expanded the use to cover ischial and posteriorthigh defects.13 Schmidt et al. further expanded the use tocover simultaneous trochanteric and sacral defects.5 Inorder to cover the sacral defect they harvested the skincomponent of the flap from the distal part of the thigh. Linet al. have used tensor fascia lata combined with tangen-tially split vastus lateralis musculocutaneous flap forsimultaneous reconstruction of trochanteric and ischialpressure sores.14 Since the descending branch of the lateralcircumflex femoral artery lies in between ‘the threemuscles’ and is never visualised during flap dissection,harvesting of this flap is safer than harvesting isolated thevastus lateralis muscle flap. The pedicle consistentlysupplies the three muscles in addition to providing muscu-locutaneous and septotocutaneous perforators to theoverlying skin paddle.15
Although the vastus lateralis muscle alone is able to fillcavities of Girdlestone arthroplasty in ambulatory patients,it may not be enough in paraplegic patients with longstanding chronic ulcers.7,16 In the latter group, the legmuscles are severely atrophic and, thus, a single muscle(vastus lateralis or the rectus femoris) alone may notprovide enough bulk to fill large cavities. Secondly, thebone and joint destruction combined with infection may bemore extensive, which requires a wider area of resection ofthe femoral head and neck resulting in a larger cavity.Thirdly, due to the communication with the ischial pressuresore, there is a wider surface area to be covered. A totalthigh flap with a leg amputation was described for pressuresores with large cavities, where the hip joint and pelvicbones were exposed with intractable infection.6 This hasmany disadvantages, including changing the pressure pointin the patient making the pelvic area prone to new pressuresores. In addition, because the whole leg is sacrificed, thechance to use the unused leg as a donor area for futurereconstructions is lost. In contrast, in our technique, whenonly the anterior compartment muscles and skin wereraised as a flap, the remaining thigh can still be used forfurther reconstruction. The descending branch of thelateral circumflex femoral artery reliably and safely

1502 T.O. Acarturk
supplies three muscles in the anterior compartment (vastusmedialis, vastus intermedius, rectus femoris). When a threemuscle flap based on the named artery is raised it canreliably reach as far as the anus and lateral border of thesacrum as well as filling large cavities in the pelvis. In ourseries, the bulk of all three muscles was just enough to fillthe cavities in five cases. In one patient with a very largecavity, the addition of the vastus medialis was necessary.Another advantage is that when all three muscles are har-vested from the anterior compartment, even a large donorskin defect up to 12 cm can be closed primarily due to the‘hollowing’ of the thigh.
In conclusion, the main advantages of the ‘three muscleflap’ are: (a) the flap has a consistent reliably identifiedvascular pedicle which permits a wide arc of rotation andsafe dissection; (b) sufficient muscle volume enabling fillingof large open wounds; (c) the structural integrity of themuscle is not violated by previous operations; (d) noimportant functional deficit is attributable to the proce-dure and (e) the rest of the leg is preserved for future use.This technique is not for simple pressure sores, but shouldbe reserved for large pressure sores complicated with largecavities created after resection of the proximal femur.
References
1. Girdlestone GR. Acute pyogenic arthritis of the hip: an oper-ation giving free access and effective drainage (Classicreprint). Clin Orthop 1982;170:3e7.
2. Klein NE, Luster S, Green S, et al. Closure of defects frompressure sores requiring proximal femoral resection. Ann PlastSurg 1988;21:246e50.
3. Rubayi S, Pompan D, Garland D. Proximal femoral resectionand myocutaneous flap for treatment of pressure ulcers inspinal injury patients. Ann Plast Surg 1991;27:132e8.
4. Evans GR, Lewis VL, Mason PN, et al. Hip joint communicationwith pressure sore: the refractory wound and the role of gir-dlestone arthroplasty. Plast Reconstr Surg 1993;91:288e94.
5. Schmidt AB, Fromberg G, Ruidisch MH. Applications of thepedicled vastus lateralis flap for patients with complicatedpressure sores. Spinal Cord 1997;35:437e42.
6. Berger SR, Rubayi S, Griffin AC. Closure of multiple pressuresores with split total thigh flap. Ann Plast Surg 1994;33:548e51.
7. Meland NB, Arnold PG, Weiss HC. Management of the recalci-trant total-hip arthroplasty wound. Plast Reconstr Surg 1991;88:681e5.
8. Jones NF, Eadie P, Johnson PC, et al. Treatment of chronicinfected hip arthroplasty wounds by radical debridement andobliteration with pedicled and free muscle flaps. PlastReconstr Surg 1991;88:95e101.
9. Huang KC, Peng KT, Li YY, et al. Modified vastus lateralis flap intreating a difficult hip infection. J Trauma 2005;59:665e71.
10. Mathes SJ, Alpert BS. Advances in muscle and musculocuta-neous flaps. Clin Plast Surg 1980;7:15e26.
11. Ger R, Levine SA. The management of decubitus ulcers bymuscle transposition. Plast Reconstr Surg 1976;58:419e28.
12. Bovet JL, Nassif TM, Guimberteau JC, et al. The vastus lateralismusculocutaneous flap in the repair of trochanteric pressuresores: technique and indication. Plast Reconstr Surg 1982;69:830e4.
13. Drimmer MA, Krasna MJ. The vastus lateralis myocutaneousflap. Plast Reconstr Surg 1987;79:560e6.
14. Lin MT, Chang KP, Lin SD, et al. Tensor fascia lata combinedwith tangentially split vastus lateralis musculocutaneous flapfor the reconstruction of pressure sores. Ann Plast Surg 2004;53:343e7.
15. Valdatta L, Tuinder S, Buoro M, et al. Lateral circumflexfemoral arterial system and perforators of the anterolateralthigh flap: an anatomic study. Ann Plast Surg 2002;49:145e50.
16. Shieh SJ, Jou IM. Management of intractable hip infection afterresectional arthroplasty using a vastus lateralis muscle flap andsecondary total hip arthroplasty. Plast Reconstr Surg 2007;120:202e7.