Embed Size (px)
Citation preview
10/19/2016
1
Treatment of chronic hepatitis C virus infection
Mark Sulkowski, MDJohns Hopkins University School of Medicine
Baltimore Maryland
Disclosures
PI for research grants related to HCV with funds paid to Johns Hopkins University
– AbbVie, BMS, Gilead, Janssen, Merck
DSMB related to HBV with funds paid to Johns Hopkins University
– Gilead
Scientific advisor related to HCV
– Terms of these arrangement are being managed by the JHU in accordance with its conflict of interest policies
– AbbVie, Achillion, BMS, Cocrystal, Gilead, Janssen, Merck

10/19/2016
2
HCV: A Global Health Problem
> 180 Million People Infected with HCV Worldwide
Retrieved from http://wwwnc.cdc.gov/travel/yellowbook/2016/infectious-diseases-related-to-travel/hepatitis-c. Accessed 5/6/16.Mohd Hanafiah K, et al. Hepatology. 2013:57(4):1333-42.
North Africa/Middle East
> 15 M
North America> 4.4 M
Eastern Europe> 6.2 M
East Asia> 50 M
South Asia> 50 M
Central America> 3.4 M
Western Europe> 10 M
South America> 4.2 M
Worldwide Distribution of HCV Genotype
Retrieved from http://wwwnc.cdc.gov/travel/yellowbook/2016/infectious-diseases-related-to-travel/hepatitis-c. Accessed 5/6/16;Mohd Hanafiah K, et al. Hepatology. 2013:57(4):1333-42; Messina JP, et al. Hepatology. 2015;61(1):77-87.
1 2 3 4 5 6HCV genotype:
10/19/2016
3
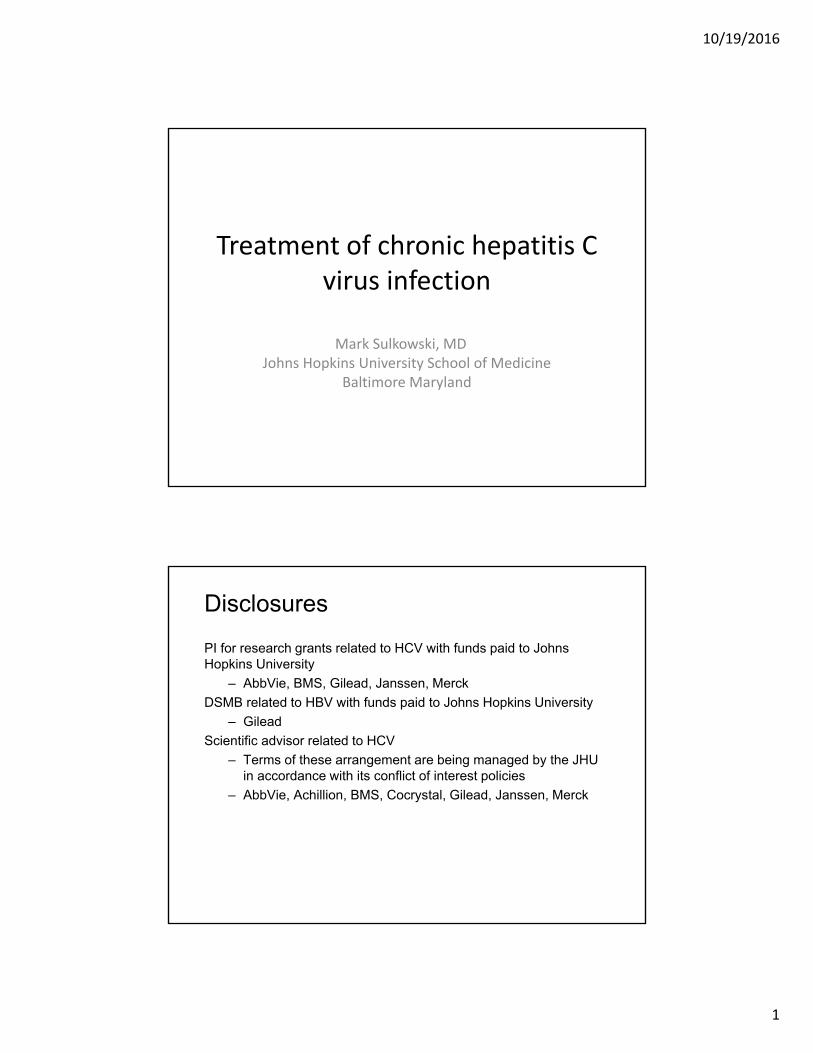
Distribution of HCV Genotypes in the United States
70%
15–20%
10–12%
1% < 1%
55% Genotype 1a 35% Genotype 1b
Genotype 1
Genotype 2
Genotype 3
Genotype 4 Genotype 5 or 6
Manos MM, et al. J Med Virol. 2012;84(11):1744-1750; Nainan OV, et al. Gastroenterology. 2006;131(2):478-484.
1. Lindenbach BD, Rice CM. Nature 2005;436(Suppl):933–8; 2. Liang J, Ghany MG. N Engl J Med 2014;370:2043–7; 3. Burki T. Lancet Infect Dis 2014;14:452–3
Current HCV direct acting antiviral regimens cure the majority of persons treated in phase 3 trials
Receptor bindingand endocytosis
Fusion and uncoating
Transportand release
(+) RNATranslation andpolyprotein processing
RNA replication
Virionassembly
ER lumen
LD
LDER lumen
LD
NS3 protease inhibitors Nucleos(t)ide and Non-nucleoside NS5B inhibitors
NS5A inhibitors
Membranousweb
96%
Sustained Virologic Response
[SVR]
Summary of New England Journal of Medicine studies on IFN‐free therapy in GT 1
published in 20142
3680/3826
Highly efficacious DAAs target different points in the HCV lifecycle1

10/19/2016
4
Key information needed to decide how to treat a person with chronic HCV infection• HCV genotype and, if genotype 1, subtype• HCV RNA level (viral load)• Testing for resistance associated variants (RAVs) in some patients
with genotype 1a*• Presence of cirrhosis
• If cirrhosis, Child‐Turcotte‐Pugh classification A, B or C• PT INR, total bilirubin, albumin
• Kidney function • Estimated GFR
• Hemoglobin • Ability to take ribavirin which causes hemolytic anemia (~ 2.5 g/dL decline in
hemoglobin)
• Prior HCV treatment experience
Payors may mandate one regimen over others
HCV genotype 1
10/19/2016
5
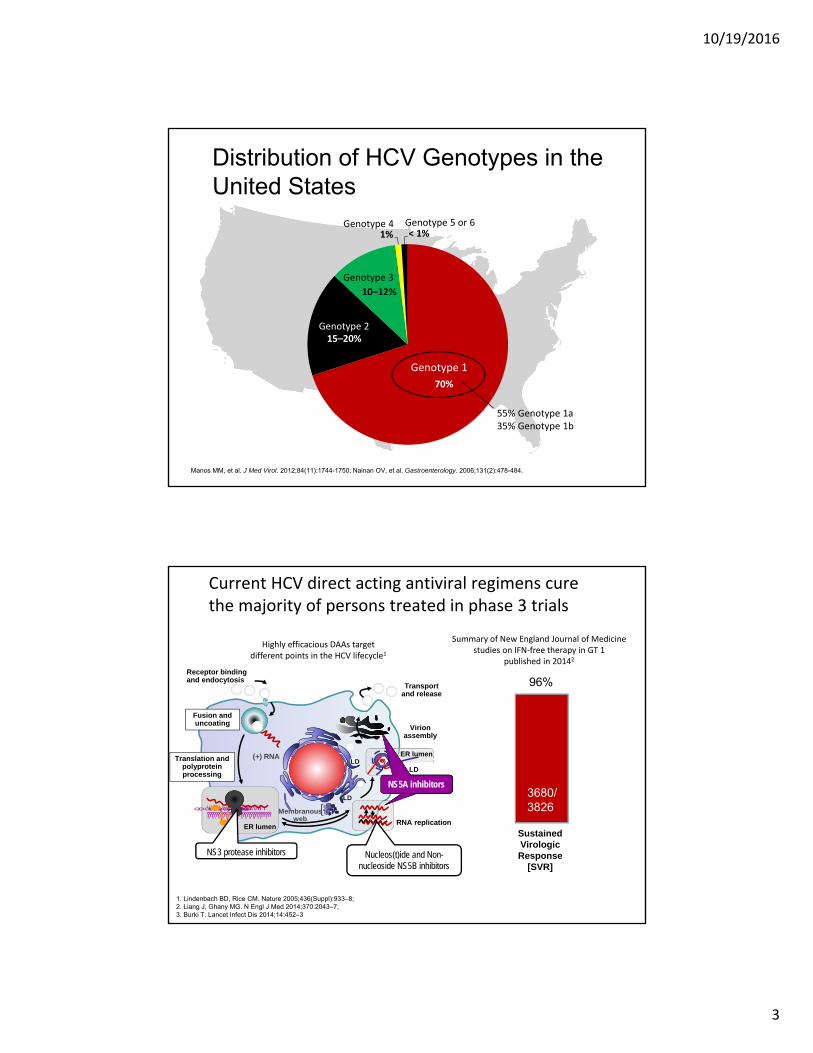
Multiple, highly effective, antiviral regimens are available to treat persons with HCV genotype 1 infection
Antiviral
NS3 NS5ANon‐NucNS5B
NucNS5B
RBV
Paritaprevir/ritonavir/Ombitasvir + Dasabuvir
Grazoprevir/Elbasvir FDC
Sofosbuvir/Ledipasvir FDC
Sofosbuvir/Velpatasvir FDC
Sofosbuvir + Daclatasvir
Sofosbuvir + Simeprevir
1a (all)
1a if RAVsat 28, 30, 31, or 93
Patients with CTP B and C and CTP A with prior Tx failure
All NS3 containing regimens: Do not use in patients with CTP B and C
All Nuc NS5B regimens: not recommended with eGFR < 30
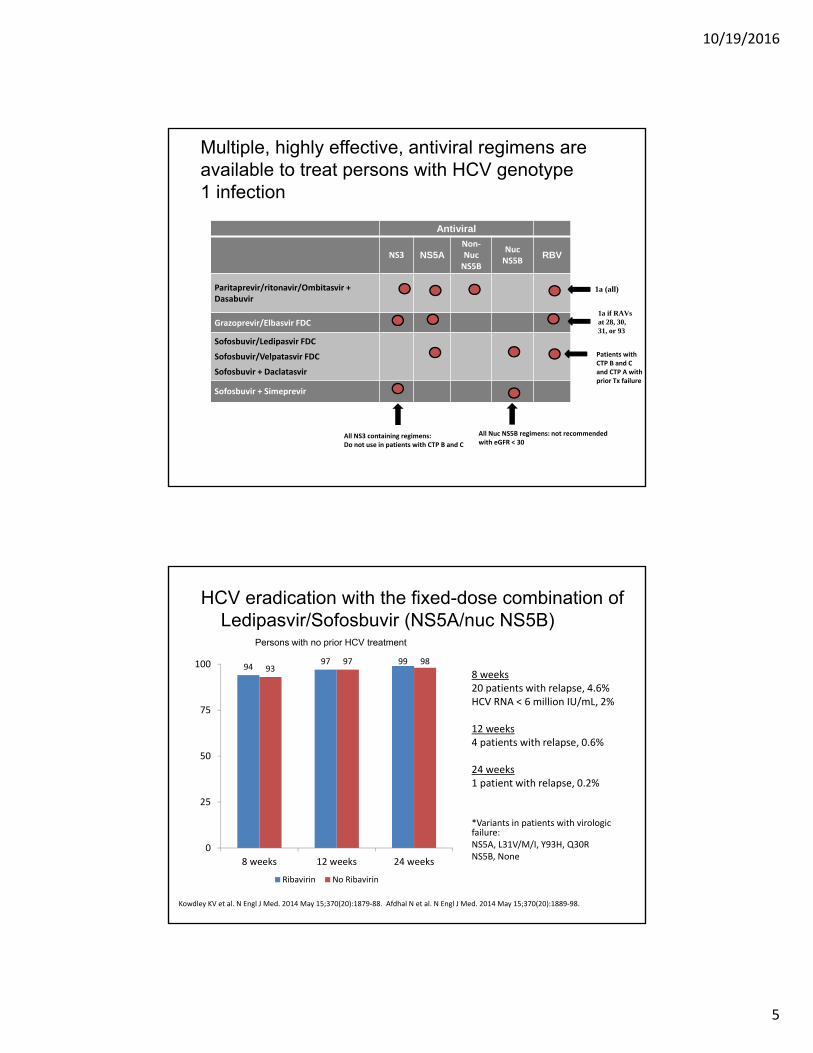
HCV eradication with the fixed-dose combination of Ledipasvir/Sofosbuvir (NS5A/nuc NS5B)
9497 99
9397 98
0
25
50
75
100
8 weeks 12 weeks 24 weeks
Ribavirin No Ribavirin
Kowdley KV et al. N Engl J Med. 2014 May 15;370(20):1879‐88. Afdhal N et al. N Engl J Med. 2014 May 15;370(20):1889‐98.
8 weeks20 patients with relapse, 4.6%HCV RNA < 6 million IU/mL, 2%
12 weeks 4 patients with relapse, 0.6%
24 weeks 1 patient with relapse, 0.2%
*Variants in patients with virologic failure: NS5A, L31V/M/I, Y93H, Q30R NS5B, None
Persons with no prior HCV treatment
10/19/2016
6
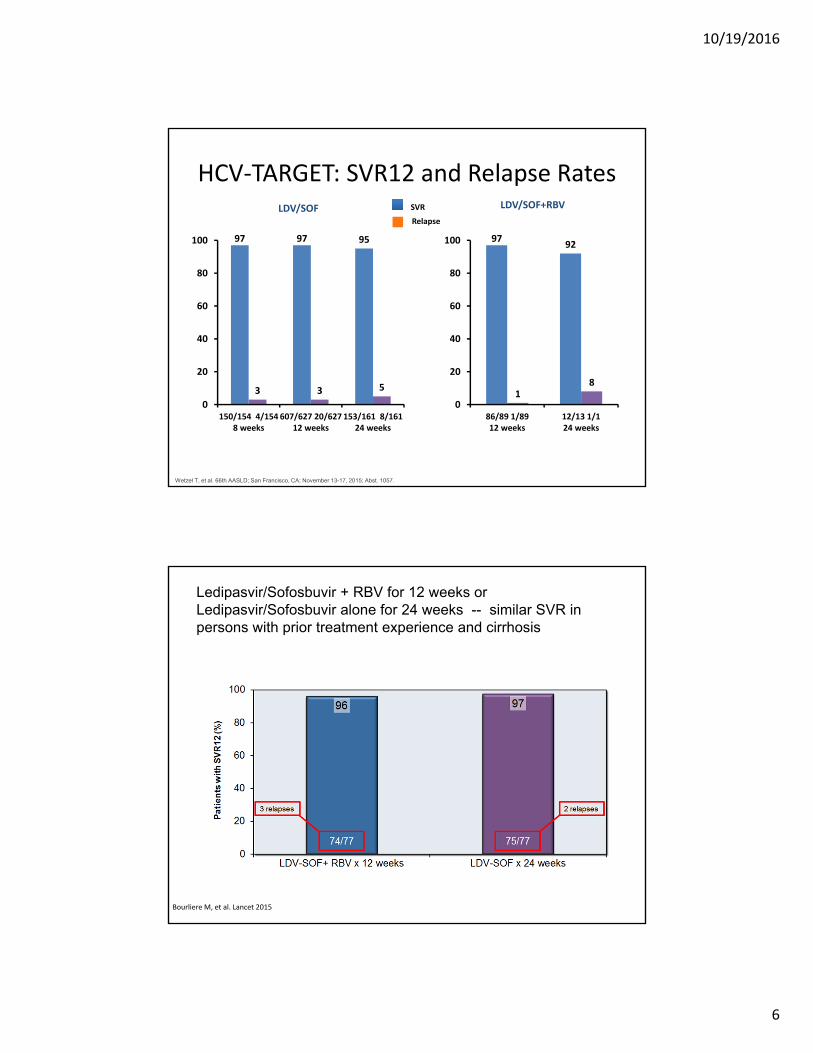
97 97 95
3 3 5
0
20
40
60
80
100
150/154 4/1548 weeks
607/627 20/62712 weeks
153/161 8/16124 weeks
SVR
Relapse
LDV/SOF LDV/SOF+RBV
9792
18
0
20
40
60
80
100
86/89 1/8912 weeks
12/13 1/124 weeks
HCV‐TARGET: SVR12 and Relapse Rates
Wetzel T, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. 1057.
Ledipasvir/Sofosbuvir + RBV for 12 weeks or Ledipasvir/Sofosbuvir alone for 24 weeks -- similar SVR in persons with prior treatment experience and cirrhosis
Bourliere M, et al. Lancet 2015
10/19/2016
7
Naive Exp’d 1a + Q80K
1a no Q80K
All pts
97
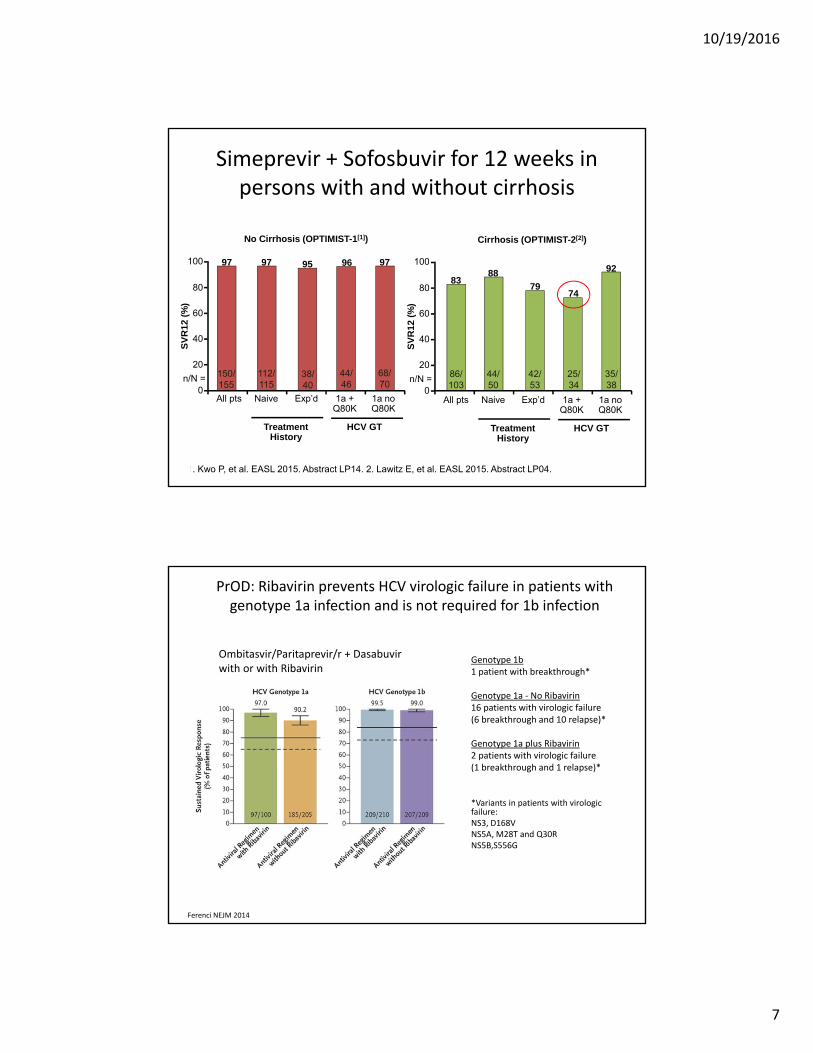
Simeprevir + Sofosbuvir for 12 weeks in persons with and without cirrhosis
1. Kwo P, et al. EASL 2015. Abstract LP14. 2. Lawitz E, et al. EASL 2015. Abstract LP04.
SV
R12
(%
)
100
80
60
40
20
0
97 95 96
112/115
38/40
44/46
68/70
n/N =
Naive Exp’d
Treatment History
HCV GT
1a + Q80K
1a no Q80K
97
150/155
All pts
88
7974
92
44/50
42/53
25/34
35/38
Treatment History
HCV GT
83
86/103
No Cirrhosis (OPTIMIST-1[1]) Cirrhosis (OPTIMIST-2[2])
SV
R12
(%
)
100
80
60
40
20
0n/N =
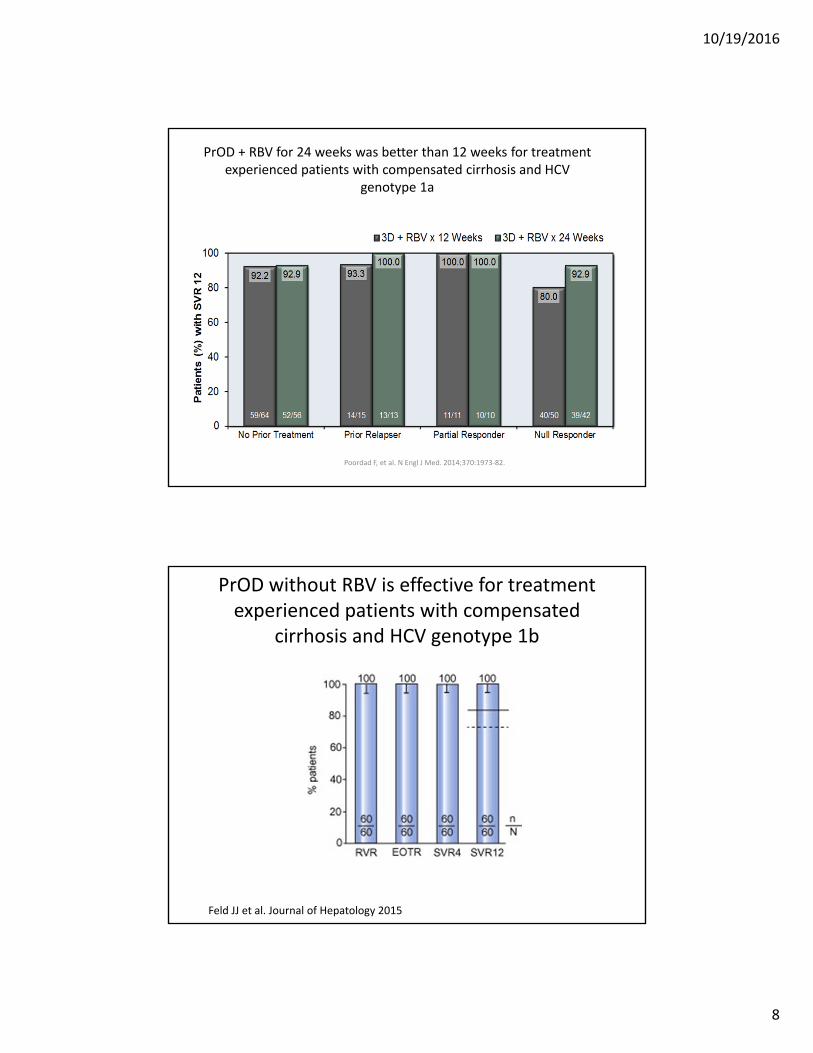
PrOD: Ribavirin prevents HCV virologic failure in patients with genotype 1a infection and is not required for 1b infection
Ombitasvir/Paritaprevir/r + Dasabuvir with or with Ribavirin
Genotype 1b1 patient with breakthrough*
Genotype 1a ‐ No Ribavirin16 patients with virologic failure (6 breakthrough and 10 relapse)*
Genotype 1a plus Ribavirin2 patients with virologic failure (1 breakthrough and 1 relapse)*
*Variants in patients with virologic failure: NS3, D168V NS5A, M28T and Q30R NS5B,S556G
Ferenci NEJM 2014
10/19/2016
8
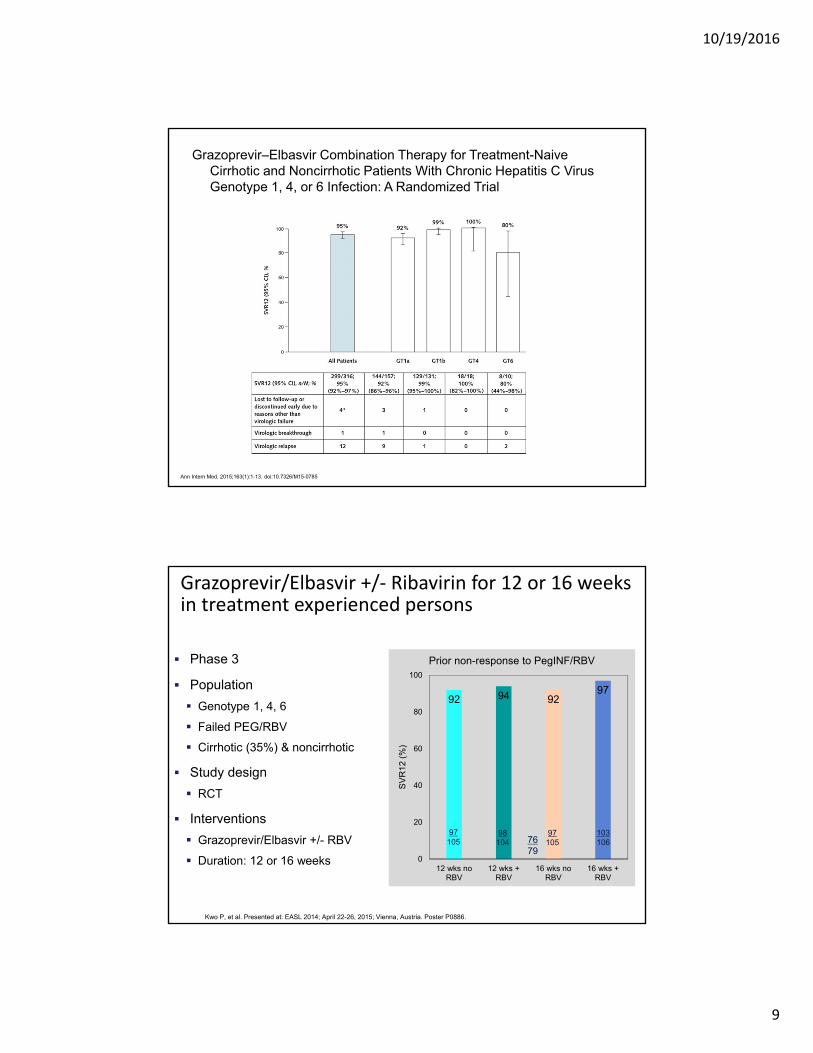
PrOD + RBV for 24 weeks was better than 12 weeks for treatment experienced patients with compensated cirrhosis and HCV
genotype 1a
Poordad F, et al. N Engl J Med. 2014;370:1973‐82.
PrOD without RBV is effective for treatment experienced patients with compensated
cirrhosis and HCV genotype 1b
Feld JJ et al. Journal of Hepatology 2015
10/19/2016
9
Grazoprevir–Elbasvir Combination Therapy for Treatment-Naive Cirrhotic and Noncirrhotic Patients With Chronic Hepatitis C Virus Genotype 1, 4, or 6 Infection: A Randomized Trial
Ann Intern Med. 2015;163(1):1-13. doi:10.7326/M15-0785
Grazoprevir/Elbasvir +/‐ Ribavirin for 12 or 16 weeks in treatment experienced persons
Phase 3
Population
Genotype 1, 4, 6
Failed PEG/RBV
Cirrhotic (35%) & noncirrhotic
Study design
RCT
Interventions
Grazoprevir/Elbasvir +/- RBV
Duration: 12 or 16 weeks
92 94 9297
0
20
40
60
80
100
12 wks noRBV
12 wks +RBV
16 wks noRBV
16 wks +RBV
SV
R12
(%
)
Prior non-response to PegINF/RBV
Kwo P, et al. Presented at: EASL 2014; April 22-26, 2015; Vienna, Austria. Poster P0886.
7679
97105
98104
97105
103106

10/19/2016
10
GZV/EBR: Baseline RAVs impact response in patients with genotype 1a but not 1b
Jacobson I, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. LB-22.
NGS 1% ST Supplemented by PopSeq when NGS was not available.NS5A Class RAV Listed = any variant from reference strain at NS5A position 24, 28, 30, 31, 32, 38, 58, 92, and 93. †At position 31, SVR was achieved in 14/16 (87.5%) with L31M and 3/3 (100%) with L31I.±At position 93, SVR was achieved in 20/21 (95.2%) with Y93H and 1/1 (100%) with Y93S.
GT1a-infected EBR/GZR 12 Weeks (No RBV): Lower SVR with key RAVSPopulation sequencing is adequate for clinical interpretation [no need for “deep” sequencing
GT1b-infected EBR/GZR 12 Weeks (No RBV): No impact of RAVS
RAV Position SVR12 Patients with RAVs (NGS 1% ST) SVR12 Patients with RAVs (PopSeq)
30 14/23 (60.9%) 4/10 (40.0%)
31 15/23 (65.2%) 5/13 (38.5%)
93 9/14 (64.3%) 5/8 (62.5%)
RAV Position SVR12 Patients with RAVs (PopSeq)
30 16/16 (100.0%)
31 17/19 (89.5%)†
93 21/22 (95.5%)‡
GZV/EBR: longer treatment (16 weeks) and addition of RBV overcome baseline RAVsEfficacy of EBR/GZR 16/18 Weeks (+ RBV) in GT1a PR Non-responders with Baseline NS5A RAVs†
15%
8%27%
2%
100 100 100 100100 100 100 100
020406080
100
EBR RAVs NS5A classRAVs
EBR RAVs NS5A classRAVs
SV
R12
(%
)
Patients without RAVs
Next-Generation Sequencing at 1% ST‡
EBR RAVs NS5A Class RAVsPopulation Sequencing
EBR RAVs NS5A Class RAVs
Pre
vale
nc
e
No RAVs: 51/52 (98%)
No RAVs: 44/52(85%)
No RAVs: 48/52(92%)
No RAVs: 38/52(73%)
51—51
1—1
44—44
8—8
48—48
4—4
38—38
14—14
Jacobson I, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. LB-22.
10/19/2016
11
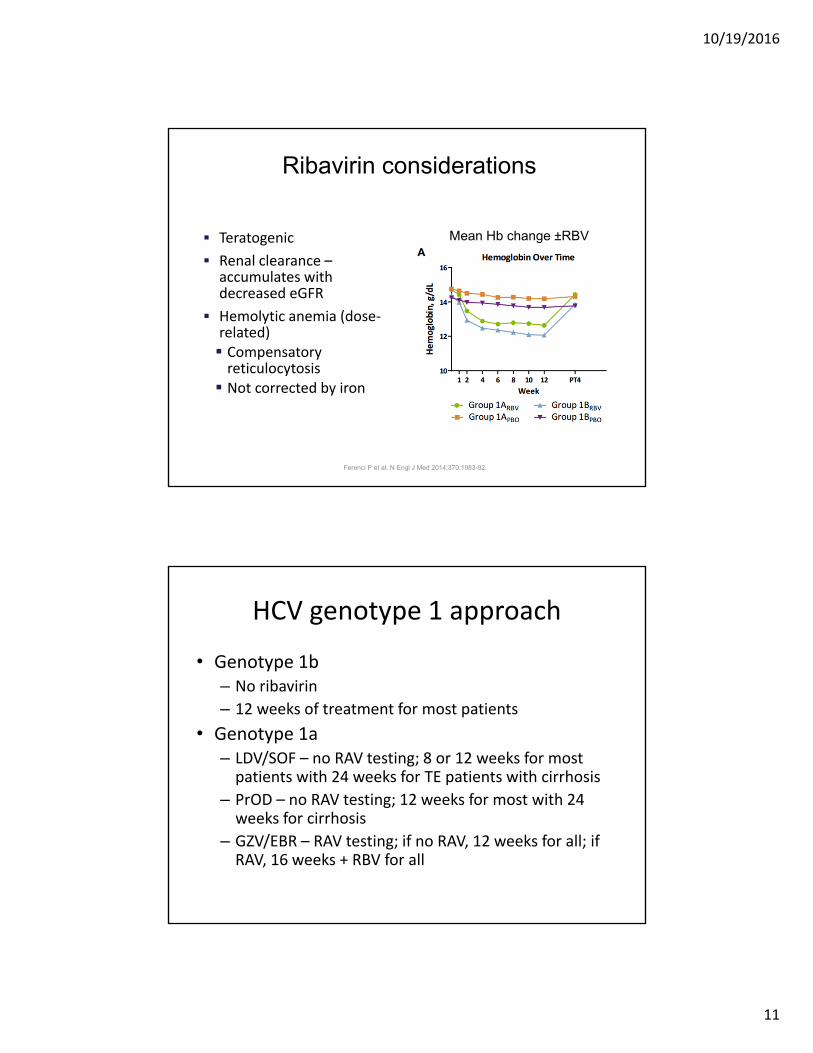
Ribavirin considerations
Teratogenic
Renal clearance –accumulates with decreased eGFR
Hemolytic anemia (dose‐related) Compensatory reticulocytosis Not corrected by iron
Ferenci P et al. N Engl J Med 2014;370:1983-92.
Mean Hb change ±RBV
HCV genotype 1 approach
• Genotype 1b – No ribavirin
– 12 weeks of treatment for most patients
• Genotype 1a– LDV/SOF – no RAV testing; 8 or 12 weeks for most patients with 24 weeks for TE patients with cirrhosis
– PrOD – no RAV testing; 12 weeks for most with 24 weeks for cirrhosis
– GZV/EBR – RAV testing; if no RAV, 12 weeks for all; if RAV, 16 weeks + RBV for all
10/19/2016
12
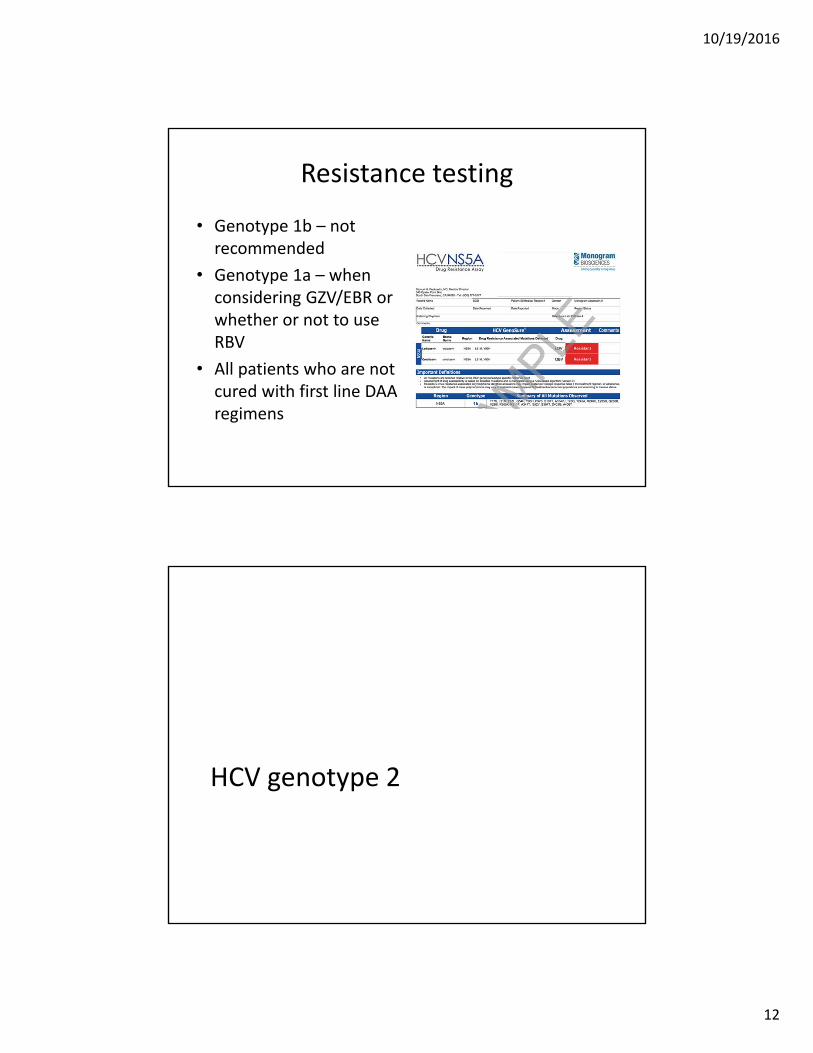
Resistance testing
• Genotype 1b – not recommended
• Genotype 1a – when considering GZV/EBR or whether or not to use RBV
• All patients who are not cured with first line DAA regimens
HCV genotype 2

10/19/2016
13
ASTRAL‐2: Sofosbuvir/Velpatasvir in patients with HCV Genotype 2 infection
Sofosbuvir/Velpatasvir(n=134)
Sofosbuvir + RBV(n=132)
Phase 3Open-labelHCV genotype 2Compensated cirrhosis allowedHCV treatment-naïve or
treatment-experiencedHCV RNA >104 IU/mLNo HBV or HIV
Week 0 12
Velpatasvir (formerly GS-5816). Primary endpoint: SVR12.Baseline demographics (sofosbuvir/velpatasvir):
Mean age: 57 years.Male: 64%.White: 93%.IL28B CC: 41%Mean BMI: 28 kg/m2.HCV RNA >800K IU/mL: 83%.Treatment-experienced: 14%.Compensated cirrhosis: 14%.
Foster GR, et al. N Engl J Med. 2015;373:2608-2617.
ASTRAL‐2: SVR Rates With Sofosbuvir/Velpatasvir in HCV Genotype 2 Patients
0
20
40
60
80
100
SV
R12
(%
)
99%* 100%
93%
81%
100% 100%100%
94% 96%99%
Sofosbuvir/velpatasvir Sofosbuvir + RBV
No Cirrhosis(n=100|96)
Cirrhosis(n=15|15)
No Cirrhosis(n=15|16)
Cirrhosis(n=4|4)
Treatment-Naïve
Overall(n=134|132)
Treatment Experienced
Relapse(n=6)
Relapse(n=2)
Relapse(n=6)
Relapse(n=3)
*Met non-inferiority and superiority criteria. All patients with baseline NS3 and NS5A RAVs achieved SVR12. No virologic relapse in the sofosbuvir/velpatasvir arm.
Foster GR, et al. N Engl J Med. 2015;373:2608-2617.

10/19/2016
14
HCV genotype 3
Daclatasvir + Sofosbuvir for Treatment of Persons with HCV Genotype 3 Infection
Nelson DR, et al. Hepatology. 2015;61(4):1127‐1135.Leroy V, et al. AASLD 2015. LB‐3.
ALLY‐3: 12 weeks
73/75
11/19
32/34
Treatment-naïve
97
58
9469100
80
60
40
20
0
SV
R12
(%
)
Cirrhosis absentCirrhosis present
n/N =
Treatment-experienced
9/13
21/24
25/26
8896100
80
60
40
20
0
SV
R4
(%)
n/N =
ALLY‐3+: 12 vs 16 weeks+ Ribavirin
12 Weeks
16 Weeks
10/19/2016
15
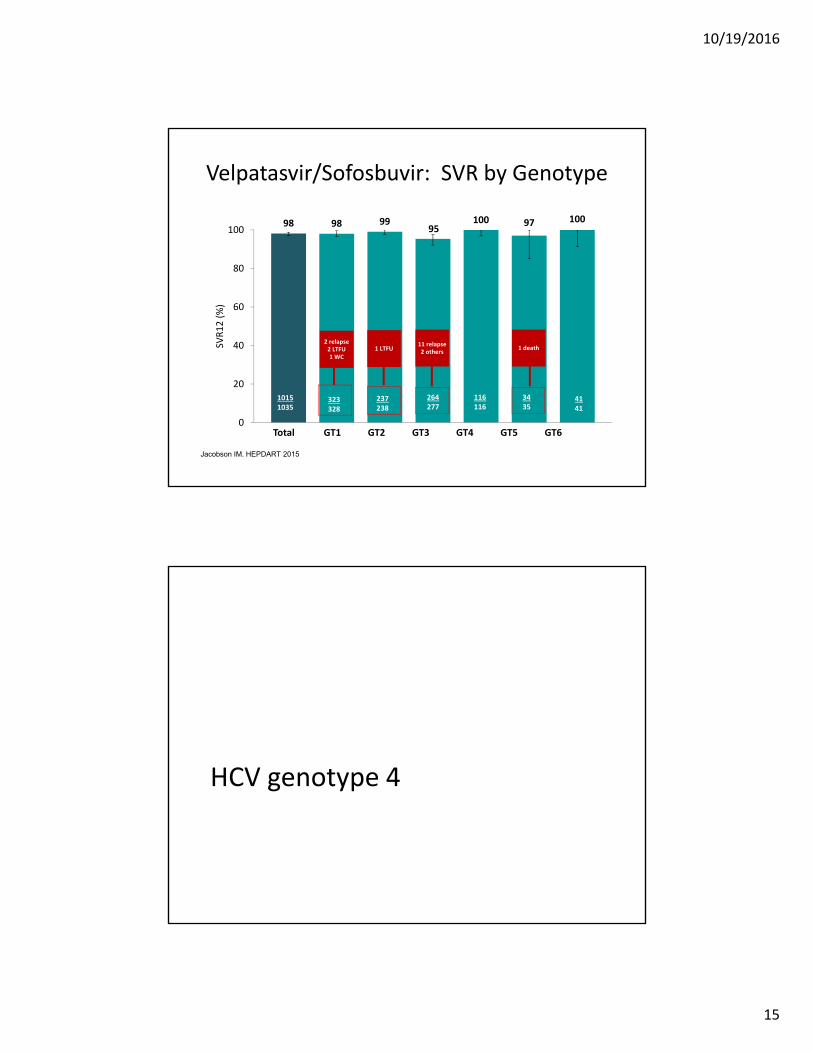
98 98 9995
100 97 100
0
20
40
60
80
100SV
R12 (%)
Velpatasvir/Sofosbuvir: SVR by Genotype
Jacobson IM. HEPDART 2015
Total GT1 GT2 GT3 GT4 GT5 GT6
323328
237238
264277
116116
3435
4141
10151035
1 death2 relapse2 LTFU1 WC
11 relapse2 others1 LTFU
HCV genotype 4
10/19/2016
16
Kapoor R, et al. AASLD 2014; Oral #240.
SYNERGY: All‐Oral Treatment for GT 4 with LDV/SOF
DemographicsAge 55 ± 10Male, n (%) 14 (67)Black, n (%) 9 (43)Country of origin
Egypt, n (%) 6 (29)USA, n (%) 5 (24)Ethiopia, n (%) 4 (19)Cameroon, n (%) 3 (14)
HCV RNA > 800,000 IU/mL, n (%) 13 (62)Treatment experienced, n (%) 8 (38)Cirrhotic, n (%) 7 (33)
Wk 0 Wk 12 Wk 24
LDV/SOF SVR12N=21
95
0
20
40
60
80
100
19/20*
95% SVR12 with LDV/SOF for GT 4 HCV – No patient discontinued due to an AE**S
VR
12
(%
)
*One patient has not reached SVR12 time point yet;**One discontinuation in a patient who reported taking one dose of medication
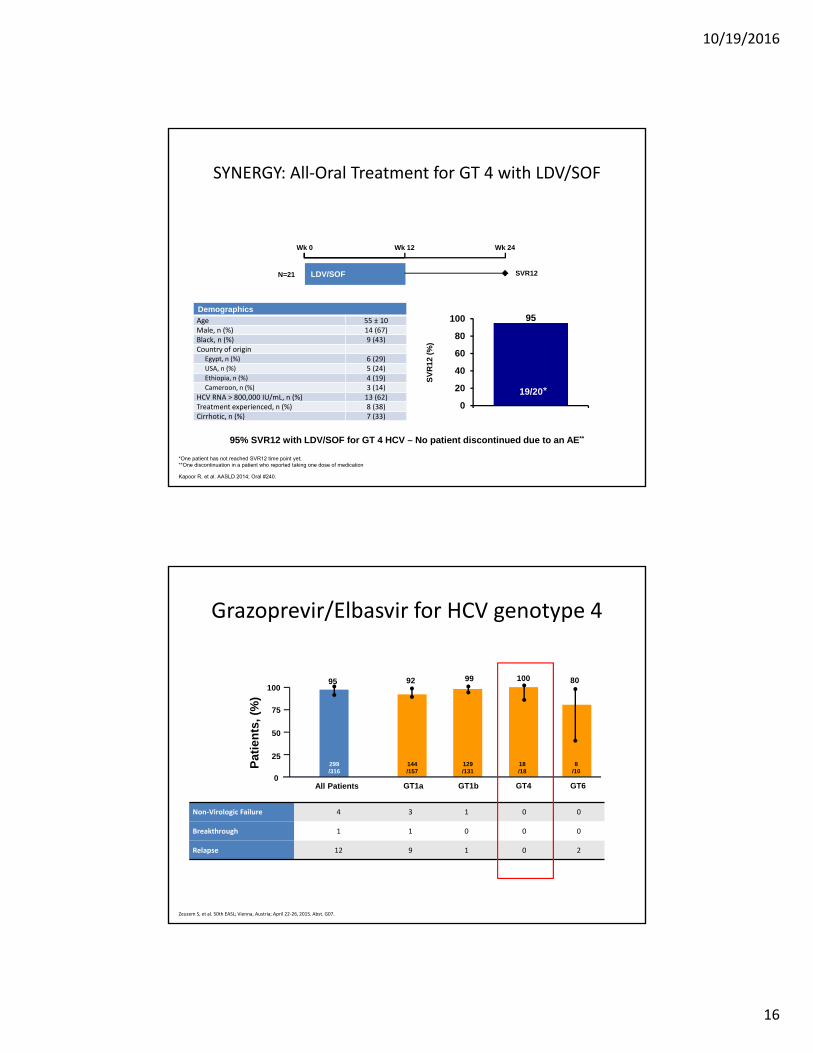
Grazoprevir/Elbasvir for HCV genotype 4
Non‐Virologic Failure 4 3 1 0 0
Breakthrough 1 1 0 0 0
Relapse 12 9 1 0 2
0
Pat
ien
ts,
(%)
All Patients
144/157
129/131
299/316
92 9995
GT1a GT1b GT4
100
18/18
25
50
75
100
8/10
80
GT6
Zeuzem S, et al. 50th EASL; Vienna, Austria; April 22‐26, 2015. Abst. G07.

10/19/2016
17
ASTRAL‐1: SVR12 by HCV Genotype
Feld J, et al. 66th AASLD; San Francisco, CA; November 13‐17, 2015; Abst. LB‐2.
99 98 99 100 100 97 100
0
20
40
60
80
100
Total 1a 1b 2 4 5 6
SV
R12
(%
)
Genotype
618624
206210
117118
104104
116116
3435
4141
1 relapse2 lost to follow-up1 withdrew consent
1 relapse 1 death
AGATE‐I: Ombitasvir/Paritaprevir/r + RBV inHCV Genotype 4 With Compensated Cirrhosis
• SVR12 rates did not differ by baseline RAVs
– RAVS versus no RAVs: 97% versus 100%
• Virologic breakthrough (n=1)
– Genotype 4a, FibroScan 15.6 kPa, no NS3 RAVs
– NS5A RAVs: baseline P58L; L28L/M and Y93Y/H at failure
• No relapses
• Safety
– No deaths, serious adverse events related to study drug, or discontinuations dues to adverse events
– Most common adverse events: asthenia (25%), fatigue (25%), headache (23%), anemia (18%)
– RBV dose modification: 30%
– Grade 3 total bilirubin elevation: 7%
Asselah T, et al. J Hepatol. 2016;64(suppl 2):S827. Abstract SAT-278.
0
20
40
60
80
100
SV
R12
(%
)
97%
SVR12 Rates (ITT)
98%
12-WeekRegimen
(n=59)
16-WeekRegimen
(n=61)

10/19/2016
18
Unique patient considerations
Considerations in patients withrenal dysfunction
How to dose ribavirin
Creatinine clearance RBV dose daily
> 50 mL/min <75 kg = 1000 mg≥75 kg = 1200 mg
30 – 50 mL/min Alternate 200 mg & 400 mg QD
< 30 mL/min 200 mg QD
Hemodialysis 200 mg QD
Copegus package insert.
• CrCl ≥ 30 mL/min: No dosage adjustments required withsofosbuvir or ledipasvir/sofosbuvir FDC or simeprevir or paritaprevir/ritonavir/ombitasvir FDC + dasabuvir BID
• CrCl < 30 mL/min: Consult an expert
10/19/2016
19
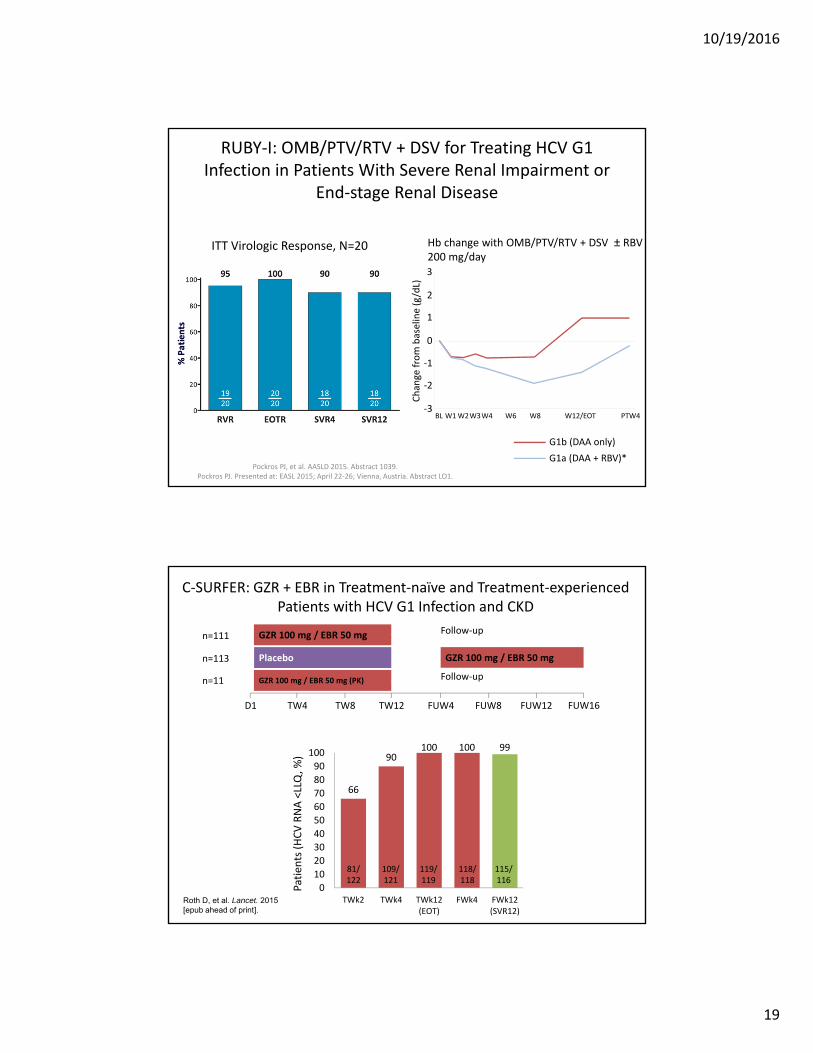
RUBY‐I: OMB/PTV/RTV + DSV for Treating HCV G1 Infection in Patients With Severe Renal Impairment or
End‐stage Renal Disease
Pockros PJ, et al. AASLD 2015. Abstract 1039.Pockros PJ. Presented at: EASL 2015; April 22‐26; Vienna, Austria. Abstract LO1.
ITT Virologic Response, N=20 Hb change with OMB/PTV/RTV + DSV ± RBV 200 mg/day 3
2
1
0
‐1
‐2
‐3Change from baseline (g/dL)
BL W1W2W3W4 W6 W8 W12/EOT PTW4
G1b (DAA only)
G1a (DAA + RBV)**8 of 14 patients held RBV
C‐SURFER: GZR + EBR in Treatment‐naïve and Treatment‐experienced Patients with HCV G1 Infection and CKD
1 G1b, non‐cirrhotic, patient relapsed at FWk12
Virologic response (ITG)
Patien
ts (HCV RNA <LLQ, %
)
66
90100 100 99
0
10
20
30
40
50
60
70
80
90
100
TWk2 TWk4 TWk12(EOT)
FWk4 FWk12(SVR12)
81/122
109/121
118/118
115/116
119/119
Roth D, et al. Lancet. 2015 [epub ahead of print].
GZR 100 mg / EBR 50 mg
Placebo
n=111
n=113
GZR 100 mg / EBR 50 mg (PK)n=11
Follow‐up
Follow‐up
GZR 100 mg / EBR 50 mg
D1 TW4 TW8 TW12 FUW4 FUW8 FUW12 FUW16
Randomized

10/19/2016
20
Consideration in patients with cirrhosis (CTP A, B or C)
• Use NS5A inhibitors + SOF (and Ribavirin)
– Ledipasvir/sofosbuvir ± RBV
– Daclatasvir + sofosbuvir ± RBV
• Do not use protease inhibitors –
Paritaprevir, Grazoprevir, Simeprevir
• FDA warning for PrOD Serious liver injury risk
Since approval, 26 cases reported worldwide to
the FDA with most cases 1‐4 weeks after
starting
• When treating patients with cirrhosis,
monitor for increasing direct bilirubin
and clinical signs of hepatic
decompensation
AASLD/IDSA/IAS–USA: Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed October 16, 2015.Viekira Pak (ombitasvir, paritaprevir and ritonavir + dasabuvir) tablets [package insert]. North Chicago, IL: AbbVie Inc.; October 2015.
Recommendation
HIV/HCV‐coinfected persons should be treated and retreated the same as persons without HIV infection, after recognizing and managing interactions with antiretroviral medications
Rating: Class I, Level B
• Treatment should be prioritized in patients at high risk for liver‐related complications which includes patients with HCV/HIV coinfection, regardless of fibrosis stage
• Treating patients at high risk for transmitting HCV to others may decrease transmission and HCV disease prevalence which includes MSM with high‐risk sexual practices and active injection drug users
Guidelines from EASL and AASLD/IDSA: Prioritize HCV Treatment for Persons with HIV Coinfection
40AASLD/IDSA/IAS–USA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org.

10/19/2016
21
Drug Interactions Between HIV Antiretrovirals and HCV Direct Acting Antivirals
41AASLD/IDSA/IAS–USA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org.
SMV + SOF SOF LDV/SOF DCV + SOFOMV/PTV/RTV + DSV EBV/GZV
Atazanavir + ritonavir
Darunavir + ritonavir
Lopinavir/ritonavir
Tipranavir + ritonavir
Efavirenz
Rilpivirine
Etravirine
Raltegravir
Elvitegravir + cobicistat
Dolutegravir
Maraviroc
Tenofovir DF
Tenofovir TAF
No clinically significant interaction expected
Potential interaction may require adjustment to dosage, altered timing of administration, or additional monitoring
Do not coadminister
Key information needed to decide how to treat a person with chronic HCV infection• HCV genotype and, if genotype 1, subtype• HCV RNA level (viral load)• Testing for resistance associated variants (RAVs) in some patients
with genotype 1a*• Presence of cirrhosis
• If cirrhosis, Child‐Turcotte‐Pugh classification A, B or C• PT INR, total bilirubin, albumin
• Kidney function • Estimated GFR
• Hemoglobin • Ability to take ribavirin which causes hemolytic anemia (~ 2.5 g/dL decline in
hemoglobin)
• Prior HCV treatment experience
Payors may mandate one regimen over others

10/19/2016
22