Embed Size (px)
Citation preview

Treatment failure and PI monotherapy
Bonaventura ClotetIrsicaixa Foundation
HIV Clinical UnitHospital Universitari “Germans Trias i Pujol”
Badalona, Catalonia

• Transparency declaration
• I have served during the past 2 years as a consultant on advisory boards or participated in speakers’ bureaus or conducted clinical trials with BMS, Abbott, Gilead, Janssen, Merck and ViiV

Principles of HIV treatment
Toxicity Tolerability
Maximal, lifelong, and continuous suppression of HIV replicationPrevent resistancePromote immune recoveryPrevent transmission
Regimen adherence considerations
Goal of therapy
Convenience
EfficacyMinimum requirement
Patient Cost1
SOURCE: Antiretroviral Treatment of Adult HIV Infection. 2012 Recommendations of the International Antiviral Society – USA Panel, July 25, 2012

Antiretroviral therapy, 27 years of continuous improvement,30 drugs, 6 classes…
1981 1990 2000 2010
2008
2007
2005
2003
2001
1999
1998
1997
1996
1987
1992
1991
1983
AIDS,
1st
cases Didanosine
Zalcitabine
Zidovudine
Stavudine, Lamivudine, saquinavir, ritonavir, indinavir
Delavirdine
Nevirapine, nelfinavir
Efavirenz, abacavir, amprenavir
Lopinavir/r
Emtricitabine
Tipranavir
Maraviroc, raltegravir, darunavir
Etravirine
Tenofovir
2002
2004
Enfuvirtide, fosamprenavir, atazanavir
Rilpivirine
2012
Trizivir* Atripla* Eviplera*
NRTIs
NNRTIs
PIs
Fusion inhibitor
CCR5 inhibitor
Integrase inhibitor
* STR (single tablet regimen)
1981
HIV
discovery
2013
2014
Elvitegravir
Dolutegravir
Stribild*
1920
s
Modified from F Raffi
TAF, 744-Cabotegravir
Triumeq*
2015
?

TAF (Tenofavir alafenamida) NRTI
Doravirine (MK-1439) NNRTI
DRV/COBI PI
GSK 744 Cabotegravir, Integrasa Inhibidor long acting (LA)
TMC 278 LA
BMS-663068 Entry Inhibidor
CENICRIVIROC (CVC)-CCR5/CCR2 antagonist
GENERICS
2015
2015 2020 2025 2030 2035 2040 2045
Antiretroviral therapy, the future……………..
2030
End of AIDS
Epidemic ?
0%
Modified from J.Montaner

Patent Expiry dates: 2014-2019
In 11 years (2015-2026) many drugs will be available as individual generics, but co-formulated versions will still maintain the patent
2014: ZDV, 3TC, NVP, EFV, RTV, Combivir – already generic
2016: ABC, LPV/r (soft-gel)
2017: TDF, ATV/r, DRV/r
2019: ETR, ABC/3TC (Kivexa)
2024: TDF/FTC (Truvada)
2025: raltegravir
2026: TDF/3TC/EFV (Atripla), TDF/FTC/RPV (Complera), dolutegravir
Ref: Medecins Sans Frontieres 2014: Untangling the web of ARV price reductions

The Highest the BL VL
The longest it takes to
reach VL<50 c/ml
To maintain viral suppression
how much potency and how many
drugs are required?
3 or 2 drugs?
BL VL matters?

78
77
76
STARTMRK RAL (n=281)
CASTLE ATV + RTV (n=440)
ABT 730 LPV/r qd (n=333)
CASTLE LPV/r (n=443)
84
82THRIVE EFV (n=538)
76ABT 730 LPV/r bid (n=331)
86
GS-102 STRIBILD (n=348)
90GS-103 STRIBILD (n=353)
87GS-103 ATV + RTV (n=355)
86
GS-102 ATRIPLA (n=352)
84ARTEMIS DRV + RTV (n=343)
83ECHO RPV (n=346)
76GS-903 EFV (n=299)
82STARTMRK EFV (n=282)
80GS 934 EFV (n=244)
78ARTEMIS LPV/r (n=346)
SPRING-2 DTG (n=242) 89
SINGLE DTG (n=414) 88
SPRING-2 RAL (n=169)
88
82STaR EFV (n=392)
86STaR RPV (n=394)
86THRIVE RPV (n=340)
83ECHO EFV (n=344)
65KLEAN LPV/r (n=444)
66KLEAN FPV/r (n=434)
Pivotal ART studies, VL <50 c/mL, 48 weeks ITT, by NRTIs
81SINGLE EFV (n=419)
QDMRK RAL BID (n=388) 89
EFV ZDV 3TC
006 Study
64%
Dec 1999
Modified from E Ribera
83.6%
In high BL
VL>100K
The 4 rules to have a
successful anti-HIV therapy
• No baseline resistance mutations
• Good adherence >95% (less number of
pills or STR better….but consider cost
and co-packaging alternatives)
• No PK interactions with other drugs
• No significant toxicities
If fulfilled…..100% should achieve and
maintain VL<40

How can we reduce drug burden?
• Reduced dosing of individual drugs
• PI monotherapy
• Class-sparing strategies
• Dual therapy including 3TC

How can we reduce drug burden?
• Reduced dosing of individual drugs
• PI monotherapy
• Class-sparing strategies
• Dual therapy including 3TC
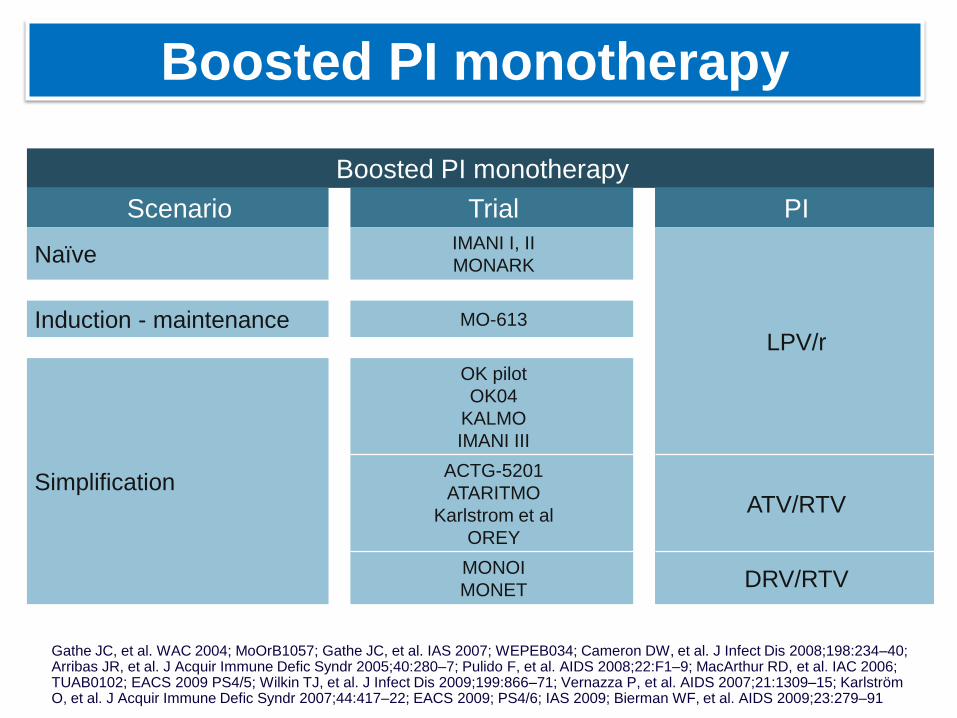
Boosted PI monotherapy
Gathe JC, et al. WAC 2004; MoOrB1057; Gathe JC, et al. IAS 2007; WEPEB034; Cameron DW, et al. J Infect Dis 2008;198:234–40; Arribas JR, et al. J Acquir Immune Defic Syndr 2005;40:280–7; Pulido F, et al. AIDS 2008;22:F1–9; MacArthur RD, et al. IAC 2006;TUAB0102; EACS 2009 PS4/5; Wilkin TJ, et al. J Infect Dis 2009;199:866–71; Vernazza P, et al. AIDS 2007;21:1309–15; Karlström O, et al. J Acquir Immune Defic Syndr 2007;44:417–22; EACS 2009; PS4/6; IAS 2009; Bierman WF, et al. AIDS 2009;23:279–91
Boosted PI monotherapy
Scenario Trial PI
NaïveIMANI I, II
MONARK
LPV/rInduction - maintenance MO-613
Simplification
OK pilot
OK04
KALMO
IMANI III
ACTG-5201
ATARITMO
Karlstrom et al
OREY
ATV/RTV
MONOI
MONETDRV/RTV

Monotherapy: later looks better...
1. Delfraissy JF, et al. AIDS 2008;22:385–93; 2. Cameron DW, et al. J Infect Dis 2008;198:234–40;
3. Arribas J, et al. J Acquir Immune Defic Syndr 2005;40:280–7
Discontinued
On study, HIV-1 RNA >400
On study, HIV-1 RNA 50–400
On study, HIV-1 RNA <50
.
MONARK1
Initial therapy
M03-6132
Induction/Maintenance
0
20
40
60
80
100
0 16 32
Wk
48 0 16 32 48 64 80 96
Wk Wk
36 4812
OK043
Simplification
0 24
Pa
tie
nts
(%
)

DRV/RTV Monotherapy:
Noninferior or not noninferior?
87.5 92.0ITT Analysis
94.199
MONOI 48 Wks[2]
92.1 90.7
Switch (Intensification With NRTIs) Allowed
DRV/RTV Mono
80.6
MONET 96 Wks[1]
DRV/RTV Mono
DRV/RTV + 2 NRTIs
Lower
limit of
90% CI:
-9.1
TLOVR, S = F
74.8 = -5.8% (-16.0% to +4.4%)
129127
DRV/RTV + 2 NRTIs
= +1.4%
(-5.5% to +8.3%)
129127
PP Analysis (Switches allowed)
Lower
limit of
90% CI:
-11.2
DRV/RTV Mono
DRV/RTV + 2 NRTIs
DRV/RTV Mono
DRV/RTV + 2 NRTIs
1. Rieger A, et al. AIDS 2010. Abstract THLBB209. 2. Katlama C, et al. AIDS. 2010;24:2365-2374.
Mono not noninferior
Mono noninferior
Mono noninferior
Mono not
noninferior
113112
102 102
100
80
60
40
20
0
100
80
60
40
20
0
100
80
60
40
20
0
100
80
60
40
20
0
Pa
tie
nts
Me
etin
g
Prim
ary
En
dp
oin
t /%
)P
atie
nts
Me
etin
g
Prim
ary
En
dp
oin
t /%
)
DRV/r BID and
with NRTIs
Introduction
Results show
non-inferiority
Non inferiority
Non demonstrated

PLoS One. 2012;7(5):e37442
92 patients followed for a median of 73wks.
Treatment failure at 48 wks:-Per protocol 9.8%

RESULTS
VF: 9 (9.8%) patients; 4 (44.4%) reported poor adherence. All were re-
suppressed
OT: 77 (83.7%) patients
Full dataset analysis: 77 (81.1%) patients
Blips: 17 (18.5%), no VF.
No factors associated with VF PLoS One. 2012;7(5):e37442

• DRV/r monotherapy appears to be safe and effective in
patients with sustained viral suppression in routine clinical
practice.
• Monotherapy with DRV/r is associated with a low rate of
VF. In addition, as in clinical trials, viral resuppression is
achieved in almost all patient experiencing VF, mainly by
reintroducing NRTIs or other antiretroviral regimens.
•In clinical practice, VF to DRV/r monotherapy is not
associated to DRV-resistance development
• With the possible exception of patients previously
receiving LPV/r, DRV/r monotherapy does not seem to
confer a clear benefit in the management of dyslipidemia.
CONCLUSIONS

PLoS One (2013); 8(7): e70201

STUDY MONOKAL
Methods:
•Single centre cross-sectional, exploratory, case-control study.
•pVL <50 copies/mL.
•Primary endpoint: The proportion of patients with complete virological
suppression (HIV RNA <1 copy/mL) in CSF.
•Secondary endpoints:
-The proportion of patients with neurocognitive impairment (NCI),
defined by performing at least 1 SD below the standardized mean in at
least 2 neurocognitive areas.
-Differences on neurocognitive status in terms of GDS, which is a
validated method to study compositely impairment on neurocognitive
functioning.
Objective: to compare the presence of HIV replication in CSF and the
neurocognitive performance in patients who had been receiving LPV/r-
based standard HAART (LPV/r-HAART) or LPV/r-MT for at least 96 weeks.
PLoS One (2013); 8(7): e70201

Of 162 potential candidates, 37 patients agreed to participate
RESULTS
PLoS One (2013); 8(7): e70201

Patients with complete CSF-virological suppression
(RNA HIV <1 copy/mL)
LPV/r-MT group LPV/r-HAART group0
20
40
60
80
100 p= 0.601
14 (82.4%)
16 (94.1%)
% o
f pat
ient
s
• The proportion of patients with HIV-1 RNA <1 copy/mL in CSF in the LPV/r-MT group was similar to
LPV/r-HAART group.
• 3 patients on LPV/r-MT had determinations of CSF HIV-1 RNA of 1, 75 and 120 copies/mL.
• 1 patient on LPV/r + ABC/3TC ( LPV/r-HAART group) had a CSF HIV RNA of 2 copies/mL.
PLoS One (2013); 8(7): e70201

THERAPEUTIC DRUG MONITORING
0 10 20 30 400.1
1
10
100
1000
10000
100000Plasma
CSF
TPD
LP
V c
on
cen
trati
on
(n
g/m
L)
Measured CSF concentrations exceeded the 50% IC50 for WT HIV-
1 (0.69 mg/ml) by a median 32.2-fold (IQR: 16.4-45.4)
PLoS One (2013); 8(7): e70201

PERCENTAGES OF SUBJECTS WITH NCI
•In the LPV/r-MT group: 7 (41%) patients with NCI while in LPV/r-HAART group: 10 (59%)
patients with NCI (p=0.48).
•When patients with possible confounding comorbidities were excluded, the results were
similar (p=0.43).
•Considering neurocognitive functioning, values were mildly better in MT group. In total
sample, GDS was 0.23 in MT group and 0.46 in HAART group (p=0.025), and in non-
comorbities sample 0.25 and 0.5 (p=0.04), respectively.
Whole sample Non-comorbidities sample0
20
40
60
80
100 LPV/r-MT
LPV/r-ART
7 (41%)
10 (59%)
6 (46%)
8 (61%)
p=0.48 p=0.43
Pat
ients
with N
CI,
%
PLoS One (2013); 8(7): e70201

CONCLUSIONS
• The proportion of patients with complete viral suppression
(HIV-1 RNA <1 copy/mL) was similar between LPV/r-MT
and LPV/r-HAART.
• Although the difference was not statistically significant,
there were fewer patients with NCI in the LPV/r-MT group.
• Neurocognitive functioning proved to be slightly better in
patients on LPV/r-MT compared to LPV/r-HAART.
• This study suggests that in patients receiving LPV/r-MT
for a long time, CSF HIV replication is completely
suppressed in most of them. Additionally, the use of
LPV/r-MT does not appear to be associated with worse
neurocognitive functioning. PLoS One (2013); 8(7): e70201

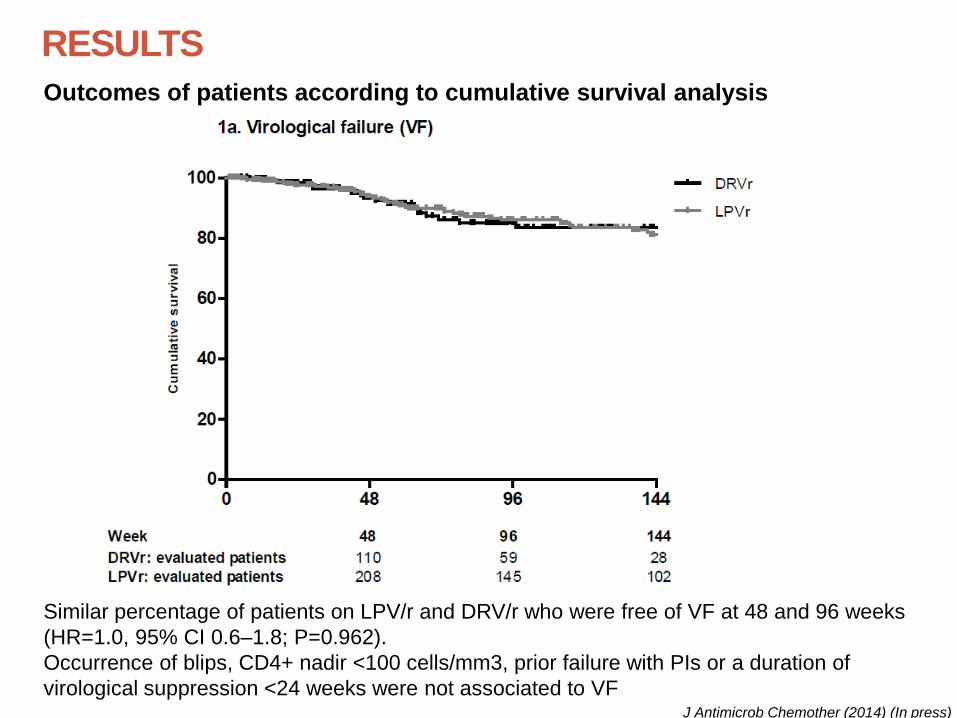
RESULTS
Outcomes of patients according to cumulative survival analysis
Similar percentage of patients on LPV/r and DRV/r who were free of VF at 48 and 96 weeks
(HR=1.0, 95% CI 0.6–1.8; P=0.962).
Occurrence of blips, CD4+ nadir <100 cells/mm3, prior failure with PIs or a duration of
virological suppression <24 weeks were not associated to VFJ Antimicrob Chemother (2014) (In press)

RESULTS
Outcomes of patients according to cumulative survival analysis
•LPV/r free of TF at 48 and 96 weeks: 76% (95% CI 71%–81%) and 59% (95% CI 53%–65%),
respectively.
•DRV/r free of TF at 48 and 96 weeks: 86% (95% CI 76%–88%) and 68% (95% CI 59%–75%),
respectively.
•Patients on LPV/r had a 1.5-fold greater risk (95% CI 1.1–2.1; P=0.012) of TF.
•TF was not associated with any of the other factors J Antimicrob Chemother (2014) (In press)

Safety
• AEs were registered as the main reason for the discontinuation (23.6% of patients on LPV/r and 7.5% of patients on DRV/r).
• The most frequent AE leading to treatment discontinuation were GI disturbances (43.8%) and dyslipidaemia (38.2%)
• The AEs were usually mild and none was Grade 3–4.
• Patients on LPV/r were at significantly greater risk than those on DRV/r of experiencing AE leading to a discontinuation of treatment (HR=2.3, 95% CI 1.3–3.9; P=0.003).
• No cases of HIV-related encephalopathy or other serious CNS AEs
RESULTS
J Antimicrob Chemother (2014) (In press)

CONCLUSIONS
• Monotherapy with LPV/r or DRV/r seems to be safe and
effective in HIV-1-infected patients with sustained viral
suppression in clinical practice.
• Better tolerability and convenience of administration
suggest that DRV/r might be the preferred option for PI
monotherapy.
• The proper selection of candidates for PI monotherapy is
mandatory in order to minimize the risk of failure
J Antimicrob Chemother (2014) (In press)

New Microbiol 2015 (ACCEPTED 2015)
OBJECTIVE
• To evaluate changes in BMD by dual-energy X-ray absorptiometry
(DXA) in HIV-infected patients after 1, 2, or 3 years since the switch
from triple ART to PI monotherapy (LPV/r or DRV/r).
New Microbiol 2015 (in revision)
METHODS
• A single-centre longitudinal study including 46 HIV-infected patients.
• Inclusion criteria:
– Treatment with PI monotherapy (LPV/r BID or DRV/r QD) for at
least 1 year
– Triple ART at the moment of the switch to the PI monotherapy
– DXA scan close to the date of the switch to the PI monotherapy
(from 4 months before to 2 months after starting the
monotherapy).
• Exclusion criteria:
– Concomitant treatment for osteoporosis/osteopenia
(bisphosphonates), or secondary causes of low bone
mineralization (testosterone deficit, thyroid disease) during the
monotherapy
– Any change or interruption of the treatmentNew Microbiol 2015 (in revision)

RESULTS
Median percentage of change from baseline in Bone mineral density in total
femur and lumbar spine.
•In the one-year group, the median percentage of change was 0.20 (IQR, -2.29 to 2.08,
p=0.910) in total femur BMD and -0.08 (IQR, -5.55 to 4.32, p=0.955) in lumbar spine BMD
•There were no significant changes in two- or three-year groups
New Microbiol 2015 (in revision)

CONCLUSIONS
• Treatment with PI monotherapy (both LPV/r and DRV/r)
during 1, 2, or 3 years leads to the stabilization of BMD
in patients with long-term virological suppression.
• Prospective comparative studies are necessary
New Microbiol 2015 (in revision)

Rules for a succesful switch to
PI Monotherpay
• Nadir CD4 > 200/mm3 (ideally > 300/mm3)
• Low proviral DNA at the time of switching
• No baseline resistances to PIs (no primary
resistances)
• No treatment failures to any PI based
approach


How can we reduce drug burden?
• Reduced dosing of individual drugs
• PI monotherapy
• Class-sparing strategies
• Dual therapy including 3TC

Study PI/r + 3TC armPI component
Comparator arm
First line GARDEL LPV/r LPV/r + 3TC + NRTI
Switch OLE LPV/r LPV/r + 3TC/FTC + NRTI
SALT ATV/RTV ATV/RTV + 2 NRTI
ATLAS DRV/RTV or LPV/r
DRV/RTV or LPV/r
MOBIDIP DRV/RTV or LPV/r
DRV/RTV or LPV/r
PI/r + LAMIVUDINE (3TC)

GARDEL: Study design
Phase III, randomized, international , controlled, open-label study
• Study included adult patients from Argentina, Chile, Mexico, Peru, Spain, US.
DT:LPV/r 400/100mg BID+ 3TC 150 mg BID(n=217)
TT:LPV/r 400/100mg BID+ 3TC or FTC and a third investigator-selected NRTI in fixed-dose combination(n=209)
ARV- naive patients,
18 years
HIV-1 RNA >1000 copies/ml
No IAS-USA defined NRTI or PI resistance at screening*
HB(s)Ag negative
(N = 426)
Stratified by screening HIV-1 RNA (≤ or > 100,000 copies/mL)
Wk 48 primary endpoint
*Defined as > 1 major or > 2 minor LPV/r mutations) LPV major mutations include the following mutations: V32I; I47V/A; L76V; V82A/F/T/S
Wk 24 interim analysis
Cahn, Lancet Inf. Dis, 2014

Viral load <50 copies/mL at week 48 (ITTe)
(p= 0.171, difference +4.6% [CI95%:-2.2% to +11.8%])
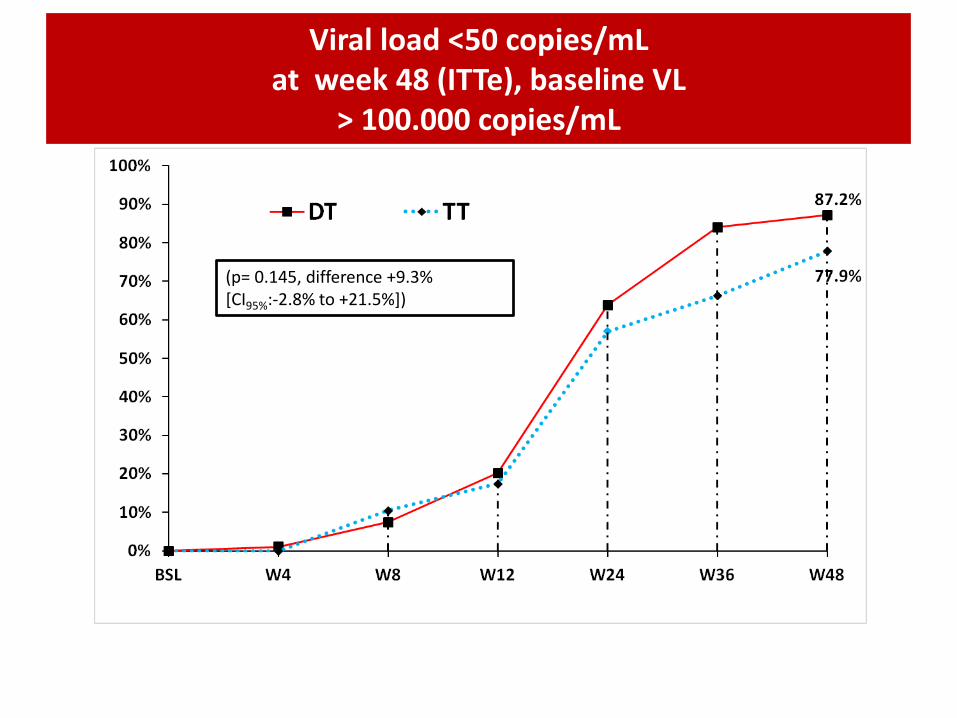
Viral load <50 copies/mL at week 48 (ITTe), baseline VL
> 100.000 copies/mL
(p= 0.145, difference +9.3% [CI95%:-2.8% to +21.5%])

CD4 increase from BL to W48
310330350370390410430450470490510530550570
BSL W4 W12 W24 W36 W48
DT TT
+ 227 cells/mm3
+ 217 cells/mm3
p=0.625

DT(n=214)
TT(n=202)
P[IC95%]
HIV – RNA < 50 copies/mL (n; %)
189 (88.3%) 169 (83.7%) 0.171[-2.2% ; +11.8%]
HIV – RNA >50 copies/mL (n; %)
10 (4.7%) 12 (5.9%)0.720
[-6.1%; +3.5%]
No Virologic data at week 48 windowReasons:Discontinued studydue to adverse eventor death
2 (0.9 %)* 10 (4.9 %)**0.03
[-7.8%; -3.0%]
Discontinued studyfor other reasons***
13 (6.1%) 11 (5.4%)0.948
[-4.3; +5.6]
Virologic Outcome at W48
*** (Non compliance with study procedures, consent withdrawal, adherence, opportunistic infection, lost to follow-up, pregnancy)
* 1 death: Sepsis, 1 nephrotic syndrome ** 2 Rash, 3 anemia, 5 GI intolerance

Protocol-Defined Virologic Failure and Emergent Resistance Mutations
Number of patients, n (%)DT
(N=214)TT
(N=202)
Confirmed virological failures 10 (4.6 %) 12 (5.9 %)*
HIV-1 RNA at failure (copies/ml)(median-IQR)
236(183-17,687)
1027(123-4,880)
Never suppressed 2 8
Rebounders 8 4
Primary PI RAMs 0 0
NRTI RAMs (M184V) 2 0
*p=0.72
PDVF: 2 measurements of HIV-1 RNA at least 1 week apart>400 copies/mL at week 24 > 50 copies/mL at week 48
Emergent resistance mutations, in samples successfully amplified:DT: 2 out of 5 both M184V TT: 0 out of 8

Rolon et al: IAC 2014; Abstr WePe 080

• Our results demonstrate that DT with LPV/r+3TC was non-inferior to triple therapy after 48 weeks of treatment, regardless of baseline viral load.
• The DT regimen showed fewer discontinuations due to safety and tolerability .
• Virologic failure, occurring at similarly low levels in both treatment arms, did not result in PI resistance development, preserving a wide range of drugs for 2nd line ARV therapy.
• These results suggest that a dual LPV/r+3TC regimen warrants further clinical research and consideration as a potential therapeutic option for ARV naïve subjects.
GARDEL: conclusions

OLE:Study design
Randomization 1:1
LPV/r BID + 3TC/FTC QD + NRTI (TT)
LPV/r BID + 3TC/FTC QD (DT)
48 weeks
• 48-week multicenter, prospective, randomized, open-label, non-inferiority trial (n:250)
• Eligibility criteria
HIV-infected patients with plasma HIV-1 RNA < 50 copies/ml
for ≥ 6 months on TT with LPV/r + 3TC/FTC + NRTI and
no resistance to LPV/r or 3TC/FTC
• Primary endpoint:
- Proportion of patients free of therapeutic failure at 48 weeks, in the m-ITT
population defined as two consecutive viral load measurements >= 50
copies/ml, death, progression to new AIDS defining disease, loss to follow-
up or change or

Difference (95% CI)-0.6% (-6.9% to + 8.1%)
Primary endpoint
0.8%3.3%3.4% 2.5% 2.5%2.5%
91.5% 90.9%
1.7% 0.8%

Resistance mutationsDT
(n=118)TT
(n=121)
Patients with protocol-defined virologicfailure*
3 3
Patients with virological failure and VL> 500 copies/mL
2 0
Patients with blip 12 12
Patients with any detectable viral load (>50 copies /mL)
15 15
*Protocol defined VF: 2 consecutive VL >50 copies/mL
DT(n=118)
TT(n=121)
Patients analyzed for resistance 1/3 0/3
Patients with data available 1/3 -
Patients with resistance to ARV regimen
1 (103N and 184V) -

How can we reduce drug burden?
• Reduced dosing of individual drugs
• PI monotherapy
• Class-sparing strategies
• Dual therapy including 3TC

Dual therapy under investigation
PI/r + integrase inhibitor
PI/r + CCR5 inhibitor
PI/r + 3TC/FTC
PI/r + NNRTI
Integrase inhibitor + NNRTI
Integrase Inhibitor + 3TC/FTC





























