Embed Size (px)
Citation preview
Transfusion Medicine and Bleeding Disorders
Ashley InmanNovember 6, 2014
Bleeding Disorders Result From:
• Increased fragility of vessels• Platelet deficiency or dysfunction• Derangement of coagulation
Vascular wall ( Endothelium)
• Antithrombotic properties– Antiplatelet effects– Anticoagulant properties– Fibrinolytic properties
• Prothrombotic properties– Von Willebrand factor– Tissue factor– Fibrinolysis inhibitors
Bleeding Disorders Due to Vessel Wall Abnormalities
• Infections• Drug Reactions• Scurvy• Ehlers-Danlos Syndrome• Henoch-Schonlein Purpura• Hereditary Hemorrhagic Telangiectasia
(Weber-Osler-Rendu Syndrome)
75-y.o. female with pinpoint superficial hemorrhage. PT, PTT, PFA-100 and Platelet count normal. Hct. 36%. WBC 6,000/mm3. D-Dimer not increased. Diagnosis?
A. CirrhosisB. Chronic renal failureC. MeningococcemiaD. ScurvyE. Metastatic melanoma

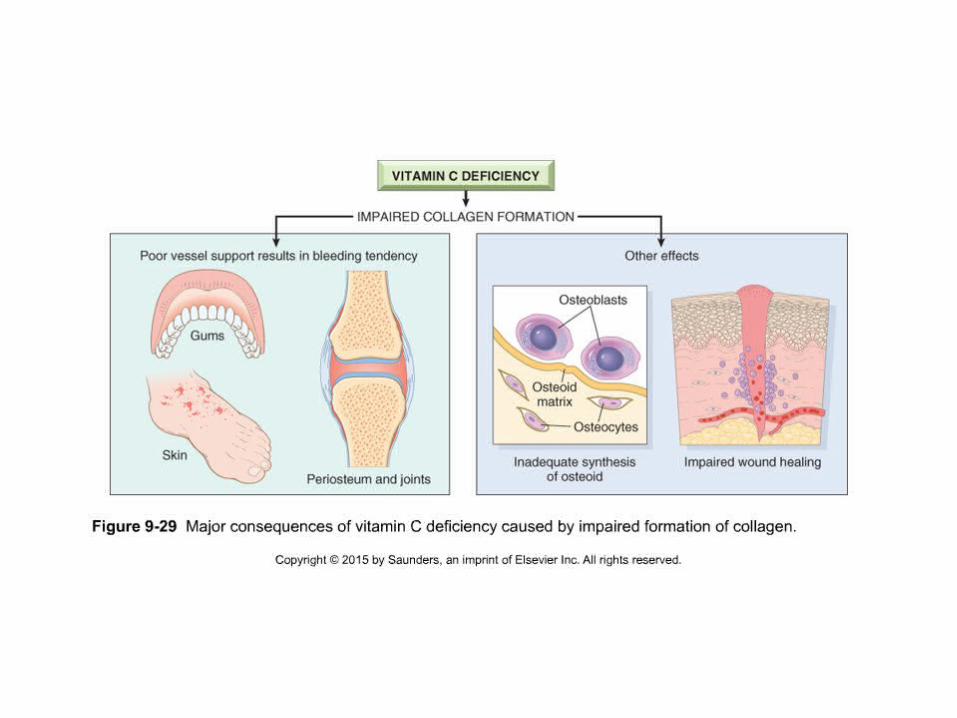
Answer D (scurvy)
• Vitamin C deficiency with vascular fragility• Gingival hemorrhages• Hemorrhagic perifollicular hyperkeratotic
papules (corkscrew hairs)• Meningococcemia would give high WBC
Bleeding Disorders Result From:
• Increased fragility of vessels• Platelet deficiency or dysfunction• Derangement of coagulation
Platelets
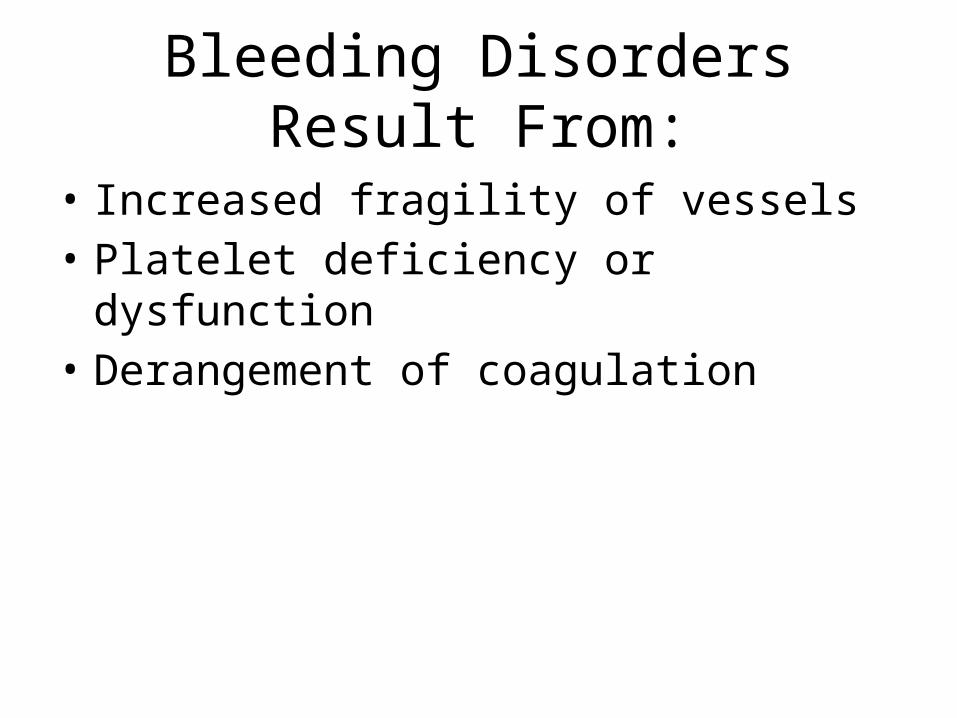
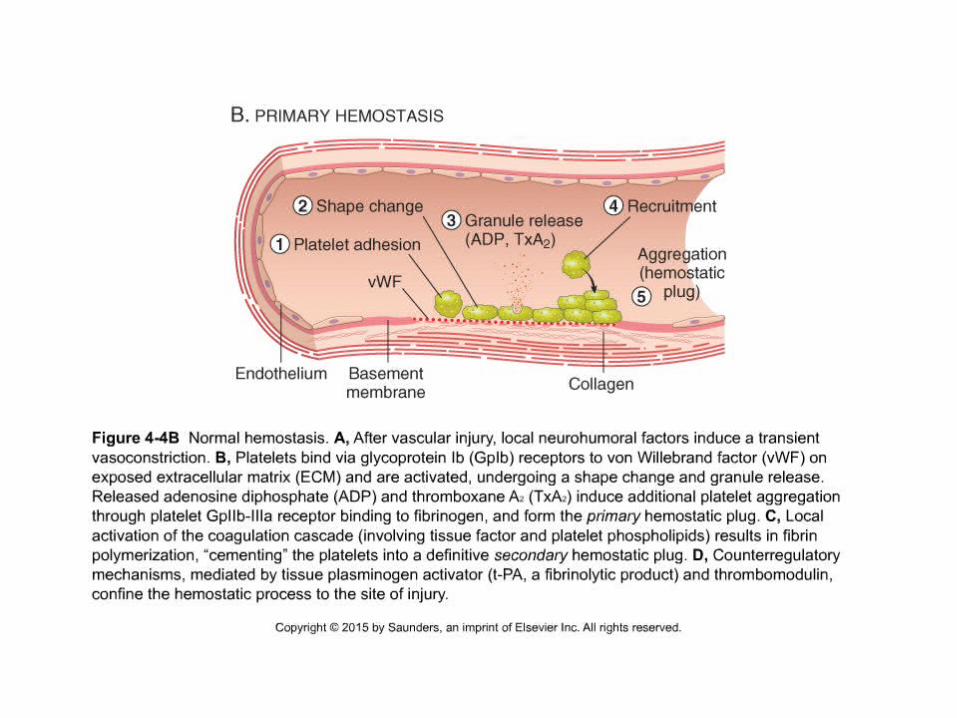
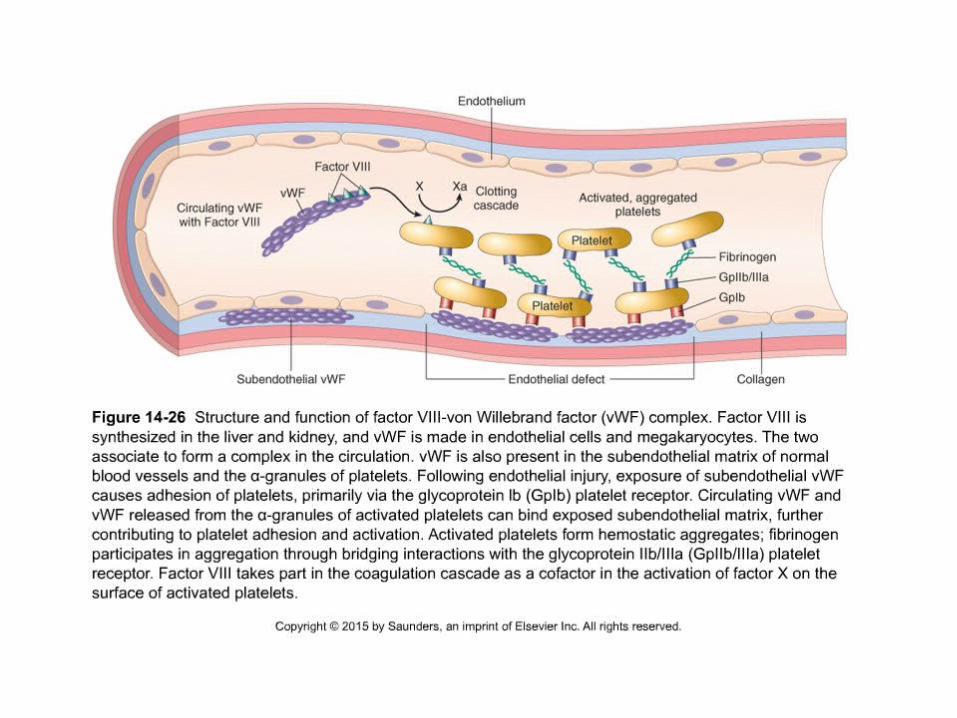
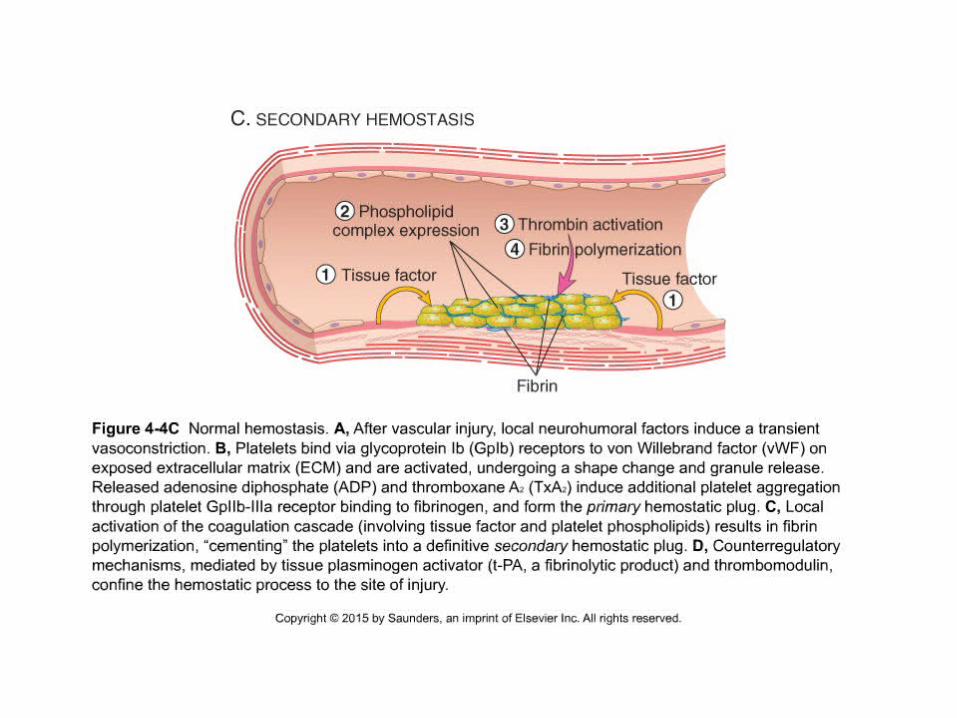
• Adhesion= to the extracellular matrix after vascular injury with vWF (*** vWF - glycoprotein Ib association) and undergo shape change
• Secretion or release reaction= of granule contents soon after adhesion. – Release of calcium and ADP. – Calcium is for coagulation cascade– ADP mediates platelet aggregation
• Aggregation= with platelets via glycoprotein IIb/ IIIa forms the primary hemostatic plug. With platelet contraction, a secondary, irreversible plug is formed. Fibrin cements the plug
Primary Hemostasis Tests
• Platelet counts• Tests of platelet function:– Platelet aggregation test– Von Willebrand factor– Bleeding time
Bleeding Disorders Due to Thrombocytopenia
• 4 major categories:1. Decreased platelet production2. Decreased platelet survival3. Sequestration • Hypersplenism
4. Dilution• Transfusion
Decreased Platelet Production
• Drug-induced• Infections• Nutritional deficiencies (B12; folate)• Bone marrow failure or ineffective
hematopoiesis (aplastic anemia; MDS)• Bone marrow replacement (leukemia;
metastatic carcinoma)
Decreased Platelet Survival
• Immunologic destruction– Primary autoimmune:• Immune thrombocytopenic purpura (ITP)
– Secondary autoimmune:• Systemic lupus erythematosus• Posttransfusion
• Nonimmunologic destruction– Disseminated intravascular coagulation– Thrombotic microangiopathies
25-y.o female with hx of bleeding gums. Sister and uncle also bleed. PT normal, PTT elevated, ristocetin (+). Factor 8 is 30% and mixing studies correct the PTT. DX?
A. Needs allogeneic BMTB. Joints will be deformedC. Needs warfarin (coumadin)D. Might have severe bleed after oral surgeryE. Splenectomy required
Answer D (vWD)
• vWD• Factor VIII low but not at clinically significant
level• No severe bleed unless significant injury- eg,
oral surgery in this case
40-y.o. female has pinpoint hemorrhages on legs. Hct. 43%. Platelets 19,000/mm3. PFA-100 normal. Corticosteroids fail to increase platelets, but splenectomy results in an increase to 150,000 platelets/mm3. Diagnosis?
A. Decreased platelet productionB. Suppressed pluripotent stem cellsC. ITPD. Excessive menstrual bleedingE. Defective platelet-endothelial interaction
Answer C (ITP)
• Patient has antibodies directed against her own platelets. The Ab-coated platelets are removed by the spleen (which also contributes to the Ab production). Corticosteroids fails and splenectomy is an option

Immune Thrombocytopenic Purpura (ITP)
• Cause– Antiplatelet antibodies – Antigen - platelet membrane glycoprotein complexes IIb-
IIIa and Ib-IX• Morphology
– Peripheral Blood• thrombocytopenia, abnormally large platelets
(megathrombocytes or Giant platelets),– Marrow• Normal or Increased magakaryocyte #
• Diagnosis - by exclusion– Bleeding time - prolonged, but PT & PTT - normal
Fatigued 35-y.o. female. Hct. 34%; Plts. 150K; Spherocytes and nucleated RBCs present. Coombs test (+) at 37°C but (-) at 4°C. Diagnosis?
A. Infectious mononucleosisB. Mycoplasma pneumoniaeC. ITPD. E. coli sepsisE. SLE
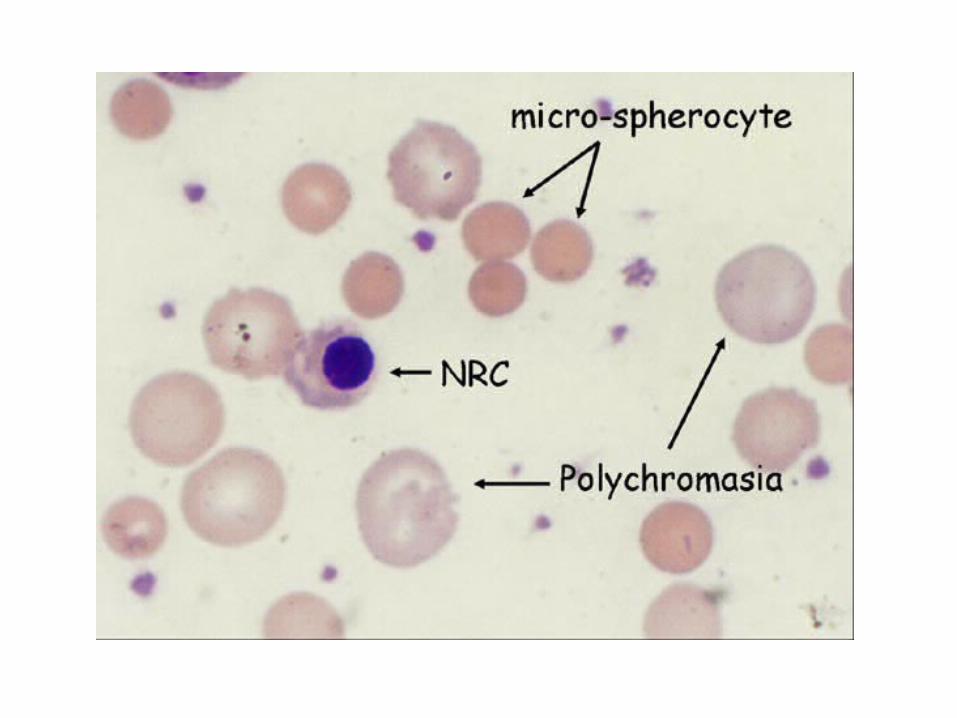
Answer E (SLE with autoimmune hemolytic anemia)
• Warm autoantibody. Anti-RBC-Abs are destroyed in the spleen. Nucleated RBCs indicate a hemolytic anemia
• 4°C agglutination is c/w Mycoplasma infection
60-y.o. female with blurred vision, confusion; 40 C; petechiae; platelets 28,000/mm3; PT, PTT normal; CBC shows fragmented RBCs; BUN 40 mg/dL. Dx?
A. ITPB. TTPC. HUSD. Hemophilia AE. DIC
Answer B (TTP)
• Pentad of TTP– Thrombocytopenia– Fever– Renal disease– CNS disease– MAHA- microangiopathic hemolytic anemia
• Peripheral blood smear shows helmet cells and schistocytes
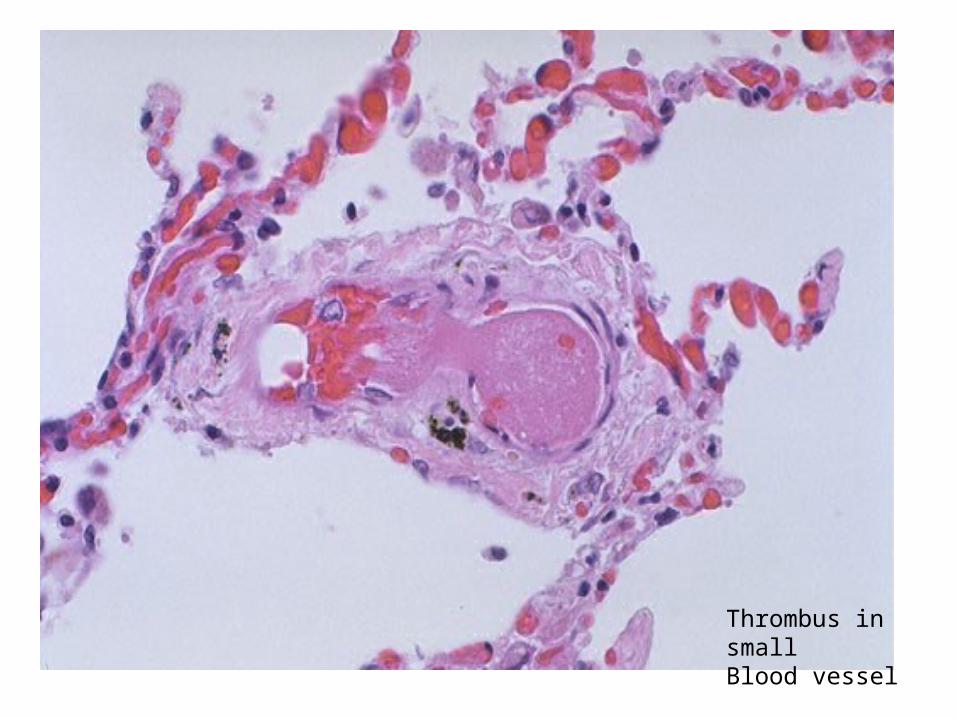
Thrombus in small Blood vessel
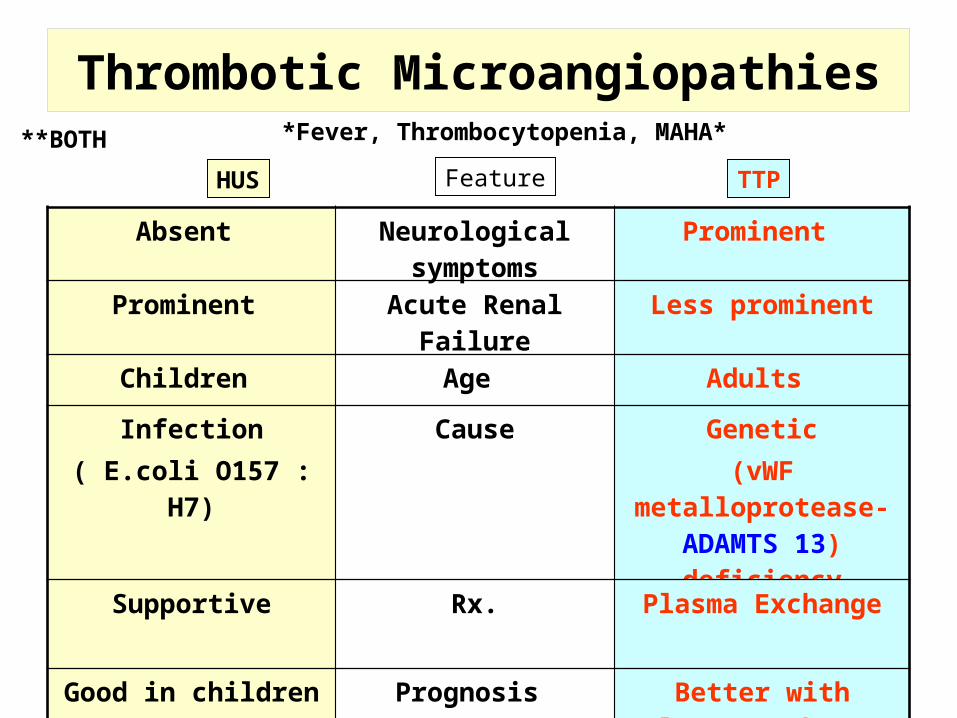
Thrombotic Microangiopathies
HUS TTP
Absent Neurological symptoms
Prominent
Prominent Acute Renal Failure Less prominent
Children Age Adults
Infection( E.coli O157 : H7)
Cause Genetic(vWF metalloprotease-
ADAMTS 13) deficiency
Supportive Rx. Plasma Exchange
Good in children Bad in adults
Prognosis Better with plasma exchange
Feature
*Fever, Thrombocytopenia, MAHA***BOTH
Bleeding Disorders Result From:
• Increased fragility of vessels• Platelet deficiency or dysfunction• Derangement of coagulation
Coagulation pathway
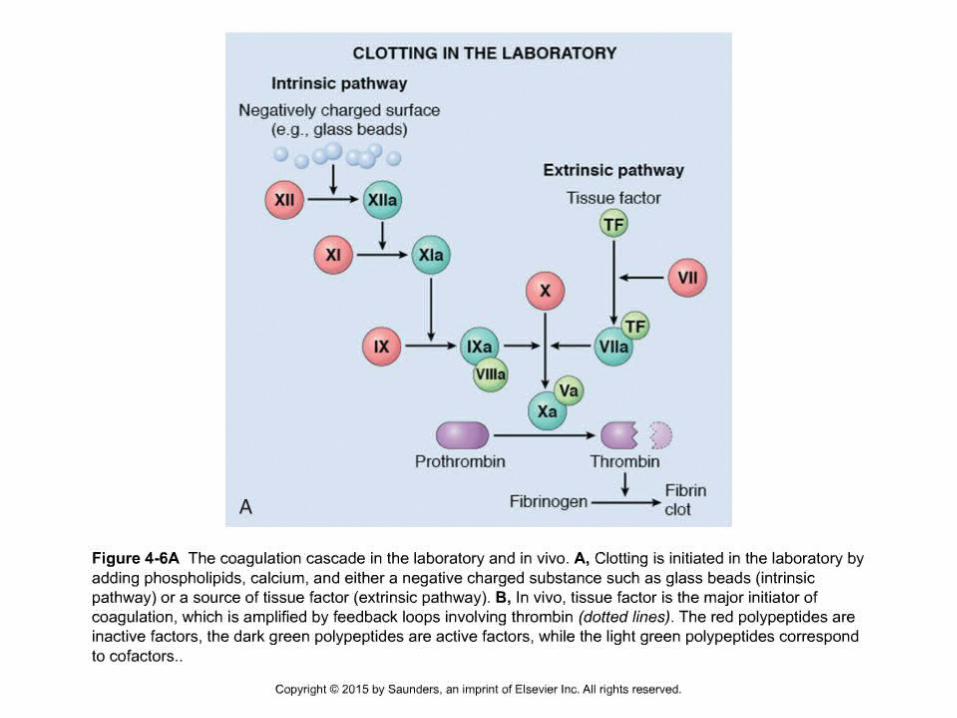
– Two pathways for fibrin clot formation:• Intrinsic– Initiated by negatively charged surface
• Extrinsic– Initiated on tissue injury
– Both pathways converge on a final common pathway• Prothrombin Thrombin (Most critical step )
» Fibrinogen Fibrin Clot
– The pathways are complex and involve many different proteins (called blood clotting factors)
Coagulation Cascade - continued
Control of coagulation • Antithrombins (e.g., antithrombin III)– Proteins C and S– Fibrinolytic cascade • Plasminogen plasmin fibrin break down products
(*FDP or FSP) – d-dimer is most important of the FDPs
*FDP / FSP – Fibrin degradation products / Fibrin split products
Secondary Hemostasis Tests
• Prothrombin time (PT):– Tests extrinsic and common coagulation pathways
• Partial thromboplastin time (PTT):– Tests intrinsic and common coagulation pathways
50-y.o female with Hep C and ALT and AST of 310 and 300 U/L, respectively. Serum ammonia is elevated. What coagulation test is most likely to be abnormal?
A. Von Willebrand Factor assayB. Platelet countC. PTD. D-DimerE. Platelet aggregation
Answer C (PT)
• Evidence of liver failure is present- loss of hepatocytes (and elevated ammonia) and thus decreased clotting factors. vWF is made by endothelial cells.
65-y.o. male with metastatic pancreatic carcinoma shows elevated PT and PTT, platelets 15,000/mm3 and elevated D-Dimer. On a PBS you would see?
A. Howell-Jolly bodiesB. Plasmodium vivaxC. Macro-ovalocytesD. SchistocytesE. Target cells
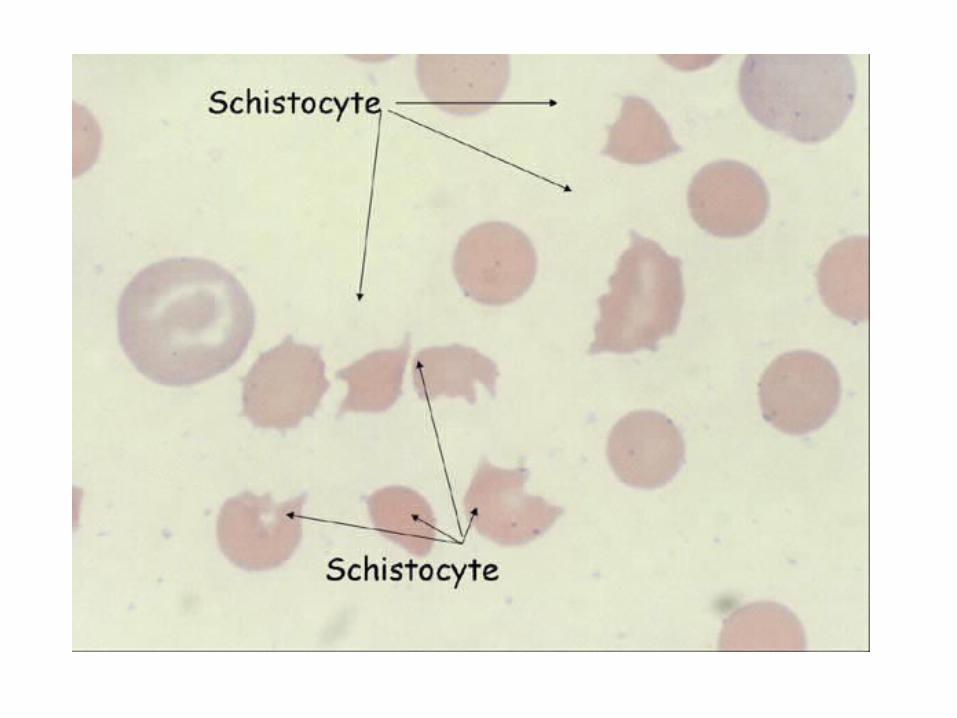
Answer D (schistocytes)
• Fragmented RBCs• Also called helmet cells or schistocytes• Pt has DIC with fibrin strands in small BVs that
slice up the RBCs• Schistocytes also present in TTP and HUS; also
present in artificial heart valves; also seen in APML (acute promyelocytic leukemia)
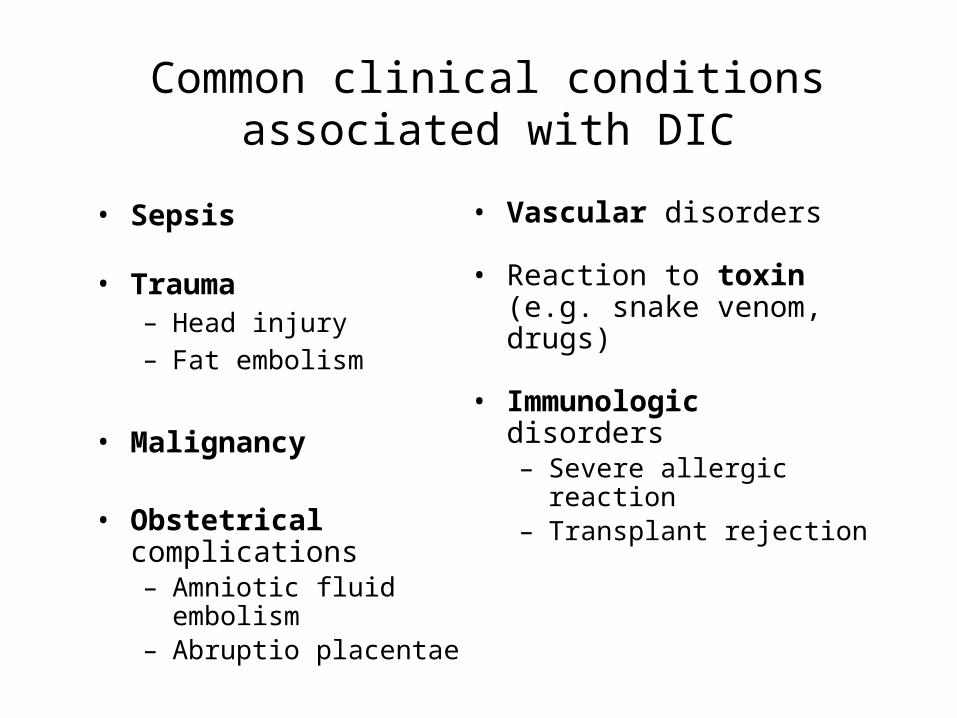
Common clinical conditionsassociated with DIC
• Sepsis
• Trauma– Head injury– Fat embolism
• Malignancy
• Obstetrical complications– Amniotic fluid embolism– Abruptio placentae
• Vascular disorders
• Reaction to toxin (e.g. snake venom, drugs)
• Immunologic disorders– Severe allergic reaction– Transplant rejection
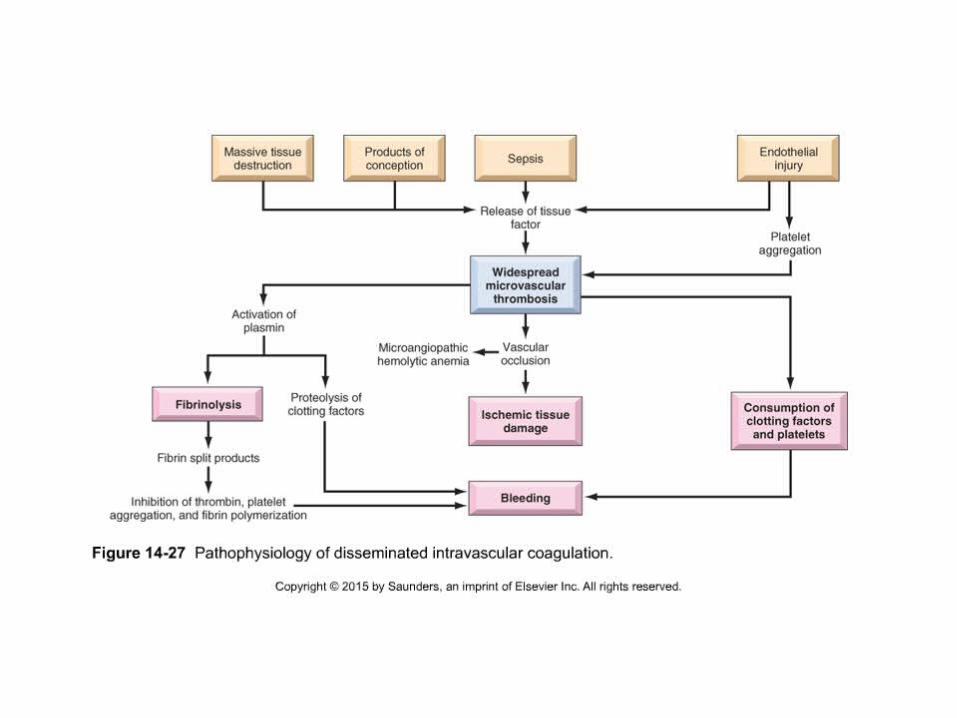
Disseminated Intravascular Coagulationcontinued…
• Lab = PT And PTT Are typically prolonged.– Thrombocytopenia– low Fibrinogen– Elevated plasma Fibrin split products (D-DIMER)
• Prognosis = Highly variable– Depends upon:
• Underlying disorder• Degree of intravascular clotting• Activity of mononuclear phagocytic system• Amount of Fibrinolysis
• Treatment of the underlying disorder is most important!!
13-y.o. boy hx of bruising and deep muscle bleeds; joints abnormal; similar hx for other male family members; Platelets normal; PT normal; PTT elevated. **NOT corrected by mixing study. Dx?
A. Factor V mutationB. DICC. Hemophilia BD. Hemophilia A due to factor 8 inhibitorE. Von Willebrand disease and anti-platelet Abs
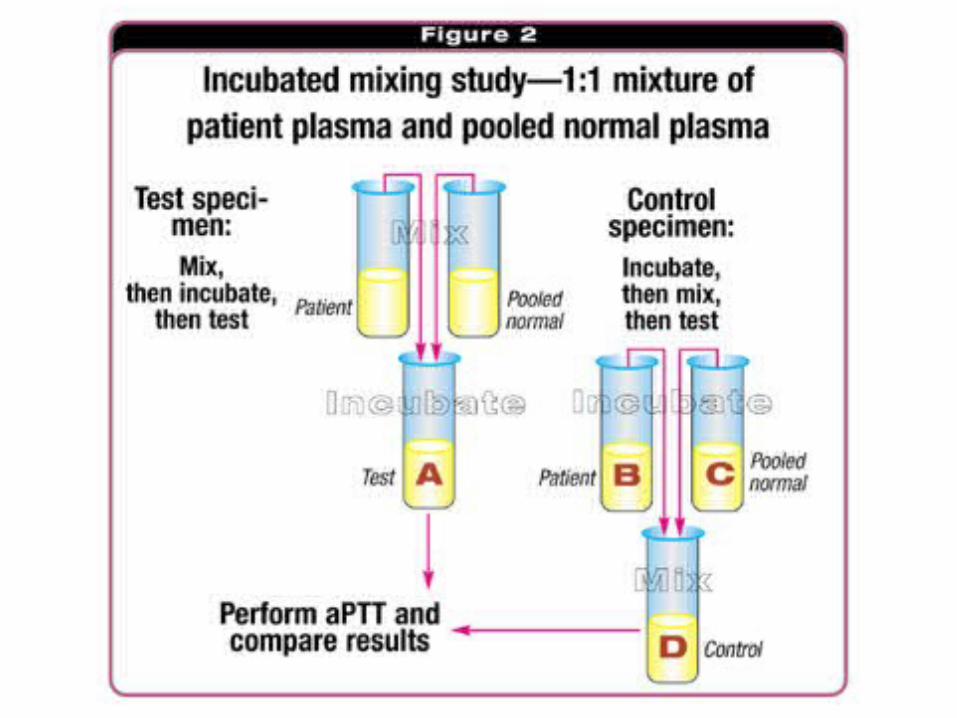
Answer D (inhibitor)
• Hemophilia A due to inhibitor• PTT prolonged• Bleeding time, platelet count, and PT all
normal• Mixing with normal serum does not correct
PTT
Hemophilia A and BHemophilia A (Classic hemophilia)
• Factor VIII deficiency• X-linked recessive• 1/10,000 males
Hemophilia B(Christmas disease)
• Factor IX deficiency• X-linked recessive• 1/50,000 males
*Indistinguishable by clinical presentation or inheritance pattern
Hemophilia continued…
• Severity is related to factor level:o <1% - Severe - spontaneous bleedingo 1-5% - Moderate - bleeding with mild injuryo 5-25% - Mild - bleeding with surgery or trauma
• Bleeding into muscles, subcutaneous tissues, and joints
Pregnant female with fetal death in utero. BP 80/40 mm Hg, blood in stool, elevated D-Dimer, increased PT and PTT, low platelets and fibrinogen. Cause?
A. Vascular fragilityB. Endothelial damageC. Reduced platelet productionD. Consumptive coagulopathyE. Platelet aggregation defect
Answer D (consumptive coagulopathy)
• DIC• Factors and platelets consumed• Thromboplastins from dead fetus (not
ecclampsia as BP is low)

25 year old male with celiac disease presents with hem occult positive stools. What vitamin deficiency should you consider?
A. Vitamin C deficiencyB. Vitamin A deficiencyC. Vitamin K deficiency
Answer C (Vitamin K Deficiency)
• Usually caused by fat malabsorption from pancreatic or small-bowel disease in adults– Celiac disease– Prolonged antibiotic use
• Also seen in neonates breast milk is deficient in vitamin K and the intestine not completely colonized by bacteria that synthesize vitamin K
• Decreased activity of clotting factors II, VII, IX and X prolonged PT and PTT
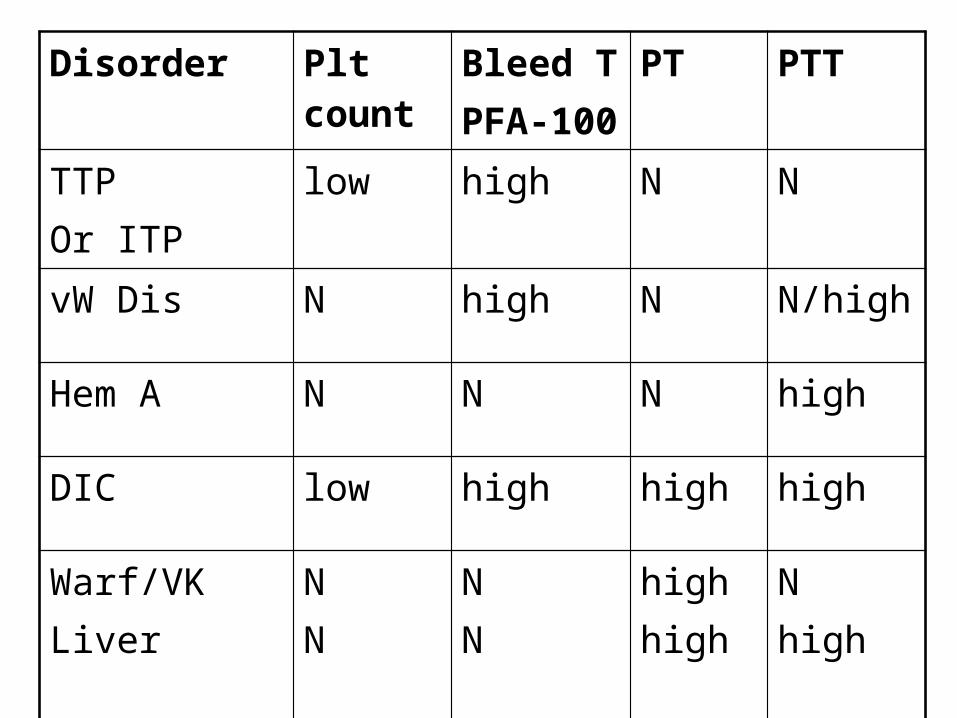
Disorder Plt count
Bleed TPFA-100
PT PTT
TTPOr ITP
low high N N
vW Dis N high N N/high
Hem A N N N high
DIC low high high high
Warf/VKLiver
NN
NN
highhigh
Nhigh
Transfusion Medicine
The blood product that is most likely to be contaminated with bacteria is:
A. Packed RBCsB. Washed RBCsC. Irradiated RBCsD. Fresh Frozen PlasmaE. Platelets
Answer E (platelets)
• Platelets are stored at room temperature• Platelets are tested for bacterial
contamination before administration
IgA deficient female has hx of anaphylaxis after blood transfusions. You should order?
A. Washed RBCsB. Leukocyte-poor RBCsC. Irradiated RBCsD. Whole BloodE. Packed RBCs
Answer A (washed RBCs)
• Washed RBCs have 99% of plasma proteins removed
Saline Washed Red Blood Cells
Indications:
1. History of allergic or febrile reactions secondary to plasma proteins not prevented by pre-transfusion administration of antihistamines and leukocyte reduction
2. IgA deficiency with documented IgA antibodies3. History of anaphylactic reaction to blood components
Transmission of CMV by blood transfusion can be greatly reduced by using?
A. Washed RBCsB. Leukocyte-poor RBCsC. Irradiated RBCsD. Whole BloodE. Packed RBCs

Answer B (leuko-poor)
• Leuko-poor RBCs• CMV infected WBCs are largely removed
Leukocyte-Reduced Red Blood Cells
Indications:
1. Prevention of HLA/WBC alloimmunization2. Prevention of recurrent non-hemolytic febrile reactions3. Prevention of CMV transmission in select groups of patients
Indications: preventing graft versus host disease
1. Immunocompromised patients2. Directed donations from blood relatives3. Premature infants ≤ 1200 gms4. Fetuses receiving intrauterine transfusions5. Neonatal exchange transfusions
Irradiated Blood Products
You have decided to order some cryoprecipitate for a patient because it has high concentrations of?
A. Factors 2,7,9 and 10B. Fibrinogen and factor 8C. PlateletsD. Platelet concentrateE. Neutrophils
Answer B (VIII and fibrinogen)
• Cryo has lots of fibrinogen and also factor 8• Primarily used to replace fibrinogen
Cryoprecipitate
Indications:
1. Hypofibrinogenemia (≤ 100 mg/dl)2. Dysfibrinogenemia3. Factor XIII deficiency - rare
Indications:
1. Treatment of coagulopathy due to clotting factor deficiencies2. Patient is bleeding actively with PT and/or PTT greater than 1.5
normal (INR > 1.8) and platelet count above 50,0003. Coumadin overdose with major bleeding or impending surgery4. Treatment of TTP5. Massive Transfusion Protocol (MTP)
Frozen Plasma
A patient with Hemoglobin of 8.0 g/dL is transfused 2 units of packed RBCs. What will the HCT be after transfusion?
A. 10g/dLB. 11 g/dLC. 30%D. 36%E. 45%
Answer C (30%)
• 10 g/dL hemoglobin• HCT 30 %• 1 g increase for every unit of packed cells or
3% increase in HCT
A 45-year-old male patient dies after an aortic valve replacement that required transfusion of 4 units of packed cells. Transfusion-related deaths are most often caused by which of the following?
A. Hepatitis AB. Hepatitis BC. Hepatitis CD. TRALIE. Anaphylaxis
Answer D (TRALI)
• TRALI is not well understood but appears to be the leading cause of death
• Factors in transfused blood product trigger activation of neutrophils in the lung microvasculature
• Clinically similar to overload, but do not respond to diuretics
• Incidence low (<1 per 10,000 transfusions), but higher in patients with preexisting lung disease
• Higher incidence with fresh frozen plasma and platelets (products that contain higher levels of donor antibodies)
If a patient is blood group AB+. That means they have what antibodies in their serum?
A. Anti-A and Anti-BB. Neither Anti-A nor Anti-BC. Anti-AD. Anti-BE. Anti-D
Answer B (neither)
• AB types have neither anti-A nor anti-B so they make excellent plasma donors; they are called the universal recipient (of red cells)
• AB type RBCs have both A and B antigens• Type O is the universal donor (of red cells) but
they have anti-A and anti-B in plasma
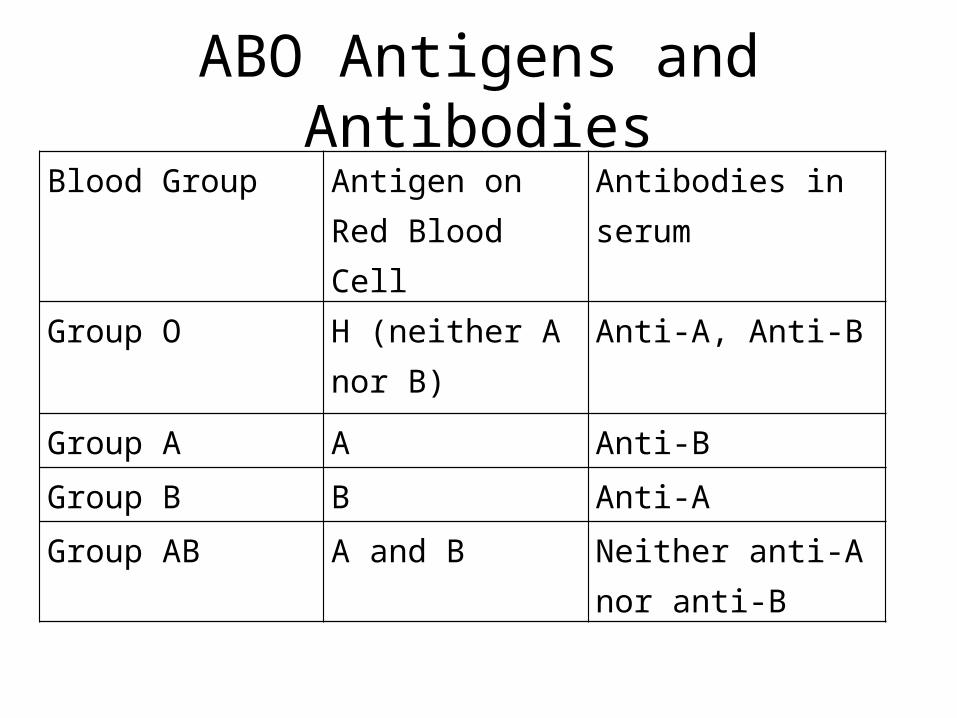
ABO Antigens and AntibodiesBlood Group Antigen on Red
Blood CellAntibodies in serum
Group O H (neither A nor B) Anti-A, Anti-B
Group A A Anti-B
Group B B Anti-A
Group AB A and B Neither anti-A nor anti-B
Mom is type O and baby is type A. HDN is extremely rare because anti-A and anti-B are:
A. IgAB. IgGC. IgMD. IgDE. IgE

Answer C (IgM)
• ABO antibodies are IgM are very rarely cross the placental barrier
• Rh(D) antibodies are IgG and readily cross
• Anti D is given to prevent immunization of Rh(-) moms who give birth to Rh(+) babies. HDN usually occurs in 2nd or 3rd pregnancies after immunization by a prior pregnancy
Hemolytic Disease of the Newborn
• Maternal IgG antibodies cross the placenta and cause hemolytic anemia in the fetus
• Can result in kernicterus and encephalopathy in the newborn or intrauterine fetal demise
• Can be related to ABO or Rh incompatibility • Rh HDN prevented by giving mother anti-D
globulin at 28 weeks gestation
A type O, 50-y.o. male is transfused with 2 units of type AB blood causing an acute hemolytic transfusion reaction. Why did this most likely occur?
A. Delayed hemolytic transfusion reaction due to low titer Abs missed by the crossmatch
B. Use of expired RBCsC. Cross-match error in the blood bank missed high
titer AbsD. Clerical error occurred in the lab or on the floorE. Use of washed RBCs
Answer D (clerical errors)
• Most surveys show the leading cause to be clerical errors
• Mislabeled specimens on floor or in the lab• Blood given to wrong patient due to typing
the wrong blood sample; hanging a unit of blood and giving to the wrong patient
55-y.o female gets 2 units of whole blood and becomes hypoxic. CXR shows total whiteout of both lungs. Diuretics are given, then fever develops and BP collapses. BNP is normal. WBC not elevated. She dies. Autopsy shows no evidence of infection. You suspect?
A. Acute hemolytic transfusion reactionB. TACOC. TRALID. DIC
Answer C (TRALI again)
• TRALI• Hypoxia and lung whiteout but normal BNP• Diuretics worsen the problem
Overall, the most common complication of RBC transfusion is?
A. HIV infectionB. Hepatitis C infectionC. Hepatitis B infectionD. TRALIE. Hives
Answer E (HIVES)
• Allergic reaction but not life-threatening• Type I IgE-mediated hypersensitivity reaction
against proteins in the donor blood• May pretreat with benadryl etc.
A 29-y.o. female is pregnant with child # 2 and in active labor. She has had no prenatal care for this baby and the other child was born in another State. Mom is Rh(-) and baby is Rh(+). Baby #2 is born jaundiced and dies with massive kernicterus. This could be prevented by.
A. anti-D IgGB. anti-D IgM
Answer A (IgG)
• RhoGAM is IgG anti-D prepared from males primed with Rh(+) blood