Embed Size (px)
Citation preview

Heart 1997;77:479-480
CASE REPORT
Transcatheter umbrella closure of aorto-
pulmonary window
Robert M R Tulloh, Michael L Rigby
AbstractAorto-pulmonary window (aorto-pul-monary septal defect) is an uncommoncongenital cardiac malformation which isrepaired using cardiopulmonary bypass.A case is described of an infant with asmall aorto-pulmonary window whichwas closed by transcatheter insertion of adouble umbrella device. Complete occlu-sion of the defect was achieved withoutcomplications. Transcatheter umbrellaclosure of a small aorto-pulmonary win-dow is feasible in infancy and the tech-nique is likely to be applicable in a fewcases.
(Heart 1997;77:479-480)
Keywords: aorto-pulmonary window; double umbrella;congenital heart disease
Department ofPaediatric Cardiology,Royal BromptonHospital, LondonRM R TullohM L RigbyCorrespondence to:Dr R M R Tulloh, Guy's andSt Thomas' Hospital Trust,Guy's Hospital, St ThomasStreet, London SE1 9RT,United Kingdom.Accepted for publication4 September 1996
The first report of an aorto-pulmonary win-dow was that of Elliotson in 1830.' The win-dow is usually a large oval defect between theascending aorta and pulmonary trunk, but inabout 10% of cases it is small. The defect isoften short and is usually a single orifice.2There may be associated anomalies such asanomalous coronary artery origin,3 anomalousorigin of the left or right pulmonary arteryfrom the ascending aorta, or even pulmonaryatresia or aortic atresia. Because in most cases
the defect is large, infants usually present withcongestive heart failure. Other potential prob-lems include the development of pulmonaryvascular disease and bacterial endocarditis. Inmost cases, surgical repair is undertaken dur-ing infancy.We report here the use of the Rashkind
double umbrella (Bard) to close an aorto-pulmonary window in an infant.
Case reportA 9 week old infant was symptom free but pre-sented with a loud continuous murmur thatwas loudest at the upper left sternal edge. Theinitial echocardiogram did not show an arterialduct but did show continuous turbulent flowin the pulmonary trunk and a dilated leftatrium and left ventricle. The electrocardio-gram and chest radiograph were normal.
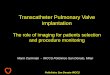
At cardiac catheterisation at the age of sixmonths, the pulmonary artery pressure wasnormal. A selective ascending aortogramshowed a small aorto-pulmonary window3 mm in diameter (fig 1). His parents gaveinformed consent to transcatheter closure with12 mm Rashkind double umbrella fourmonths later, when the infant weighed 8 kg. Aretrograde arterial approach was used to passan end-hole catheter from the aorta throughthe defect and into the pulmonary artery andthen to the superior caval vein through theright ventricle and right atrium. An 0-025 inch
Figure 1 Angiogram inascending aortademonstratingflow ofcontrast in aorto-pulmonary window topulmonary trunk.(A) Anterioposteriorprojection and (B) lateralprojection. (Ao, aorta; PT,pulmonary trunk; APW,aorto-pulmonary window).
A B
.1-
479
.....
on Novem
ber 6, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/H
eart: first published as 10.1136/hrt.77.5.479 on 1 May 1997. D
ownloaded from

Tulloh, Rigby
Figure 2 Angiogram after successful placement of a double umbrella device in aorto-pulmonaty window with contrast in ascending aorta, showing no residual defect.
wire introduced through the catheter wassnared and retrieved to the femoral vein. A12 mm Rashkind double umbrella device wasmodified by bending the arms medially,4 inorder to allow the device to lie flat against theaorto-pulmonary septum. An 8F Mullinssheath was then used to deliver the umbrelladevice. The distal arms were opened in theaorta and the proximal arms were opened inthe pulmonary trunk. The procedure was
uncomplicated and lasted 65 minutes with afluoroscopy time of 26 minutes. After the pro-cedure there was complete occlusion of thedefect as assessed by angiography and echo-cardiography (fig 2). There was no interfer-ence with pulmonary or aortic valve function.The child was reviewed six months after
closure. At that time there was no murmur or
other complication. Echocardiographic assess-
ment showed complete occlusion of thedefect, with resolution of the left atrial and leftventricular enlargement. After Doppler inter-
rogation there was no evidence of stenosisinduced by the umbrella in either the pul-monary trunk or the ascending aorta.
DiscussionThere have been several reports of the surgicalligation of an aorto-pulmonary window, ini-tially with a closed technique which could beapplied to small defects.5 The introduction ofcardiopulmonary bypass allowed for the cor-rection of smaller defects with division,6 how-ever, in most cases the defect is large so thatpatch closure from the aorta is the best treat-ment.7The use of the Rashkind double umbrella
for the closure of a persistent arterial duct iswell established,8 and it has now been used toclose atrial septal defects, baffle fenestrationsafter total cavopulmonary anastomoses,9 andventricular septal defects.4
This case demonstrates a novel use of thedouble umbrella delivery system to close asmall aorto-pulmonary window. There is oneprevious case report of such a technique, butin that case the child was 3 years old and therewas residual left to right shunt after the proce-dure, which meant that the risk of endocarditiswas not avoided.'0Most infants presenting with an aorto-pul-
monary window will require conventional sur-gical repair with the aid of cardiopulmonarybypass. However, we have shown that whenthe defect is small, distant from the semi-lunarvalves, and not associated with anomalous ori-gin of the right or left pulmonary arteries fromthe ascending aorta, transcatheter umbrellaclosure can be effective and safe. It is probablythe best treatment in a few cases.
1 Elliotson J. Case of malformation of the pulmonary arteryand aorta. Lancet 1830;i:247-50.
2 Neufeld HN, Lester RG, Adams P Jr, Anderson RC,Lillehei CW, Edwards JE. Aortico-pulmonary septaldefect. Am Jf Cardiol 1962;9:12-6.
3 Luisi SV, Ashraf MH, Gula G, Radley-Smith R, YacoubM. Anomalous origin of the right coronary artery withaortopulmonary window: functional and surgical consid-erations. Thorax 1980;35:446-52.
4 Rigby ML, Redington AN. Primary transcatheter umbrellaclosure of perimembranous ventricular septal defects. BrHeartJ 1994;72:368-71.
5 Gross RE. Surgical closure of an aortic septal defect.Circulation 1952;5:858-63.
6 Cooley DA, McNamara DG, Latson JR. Aorticopulmonaryseptal defect: diagnosis and surgical treatment. Surgery1957;42:101-8.
7 Deverall PB, Lincoln JCR, Aberdeen E, Bonham-CarterRE, Waterston DJ. Aortopulmonary window. J ThoracCardiovasc Surg 1969;57:479-85.
8 Gatzoulis M, Rigby ML, Redington AN. Umbrella occlu-sion ofpersistent arterial duct in children under 2 years. BrHeartJ 1994;72:364-7.
9 Perry SB, Lock JE. Front loading of the double umbrelladevice, a new technique for umbrella delivery for closingcardiovascular defects. Am J Cardiol 1992;70:917-20.
10 Stamato T, Benson, LN, Smallhom JF, Freedom RM.Transcatheter closure of an aorto-pulmonary windowwith a modified double umbrella occluder system.Catheter Cardiovasc Diagn 1995;35:165-7.
480
on Novem
ber 6, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/H
eart: first published as 10.1136/hrt.77.5.479 on 1 May 1997. D
ownloaded from