Embed Size (px)
Citation preview
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding Applied in Upper Gastrointestinal and Post Partum Bleedings
Lars-Gunnar Eriksson
�
���������� �������� �� ������ �������� � �� �������� ������� � ���������������������� ���������� �� !� "�������� #������ $� %!! �� !&'() *� ��� ������ * ����* +������� ,-������ * .������/0 "�� �������� ���� �� ������� � 1������0
��������
2������ 34�0 %!! 0 "����������� �������� 2����5��� � ��� .������� * 3�*�"�������� 6������ ������� � ���� ������������� �� +�� +����� 6�������00 77 ��0 ������0 �16# & $4&(4)!84(&8(470
"����������� �������� 2����5��� ,"�2/ �� � ����� � ����� � �������� �� ������� �� ������� ���� *������� �������0 6� ���� �������� ���� ������� � �������� ������������� ��� ��������� ��� ������ �� �� ������� �� ��� ������� ������02����� �� ��� �������� * ����� � ����� ������������� ,��/ �������� ��� (!9 �
:!9 * ������� ������� �� ���� ���� �������� ����0 +�� +����� ;�������� ,++;/��� ����� ������� �� �� ����� ��*� ���������0 <���������� �������� ���� ����� ��������� ��� � ��� ����� �������� ������� �� ����� �� � ��� ���� ���� �����������0"�� ������� ��� * ���� ������ ��� � �������� ��� ������� ���*������ ������ ��� "�2
�����=�� �� ������ ��� ����� * "�2 ���� ������� ���� �� >������� �������? �������� ���� ����� �� �������0 2������� "�2 �����=�� �� ��� ��4���� �**��� ����������� ����� �� *�������� � ������ ++;0" �������� ��� ������� ���*����� (: ������� ���� ������� ���� "�2 �*��� �������
�������� *������ �� ) ���� ������� *� �������� ��������� �*��� �������� �������0"�� ������� ����� �� �������� ���� * 7! ������� ������� ���� "�2 ��� ������� ����
)( ������� ������� ���� ������� * ����� �� ��������0� (: ������� ��� ����� ��� ������ ���� �������� * � �������� ���� �� ������ � ��
���� � ����� ��� ����� ���� * ��� ������� ����� ����� ��� "�2 ��������0� ������������ ����� * %! ������� ���� ������ ++; ������� ���� ��������� "�2 * ���
������ ������ ��� ���*����0"�2 ��� *�� � �� �**������ �� � ���������� � �������� ������� *� ���� *
������� ����� �� �������0 "�� :!4��� �������� ��� ���� � ��� "�2 ���� ,:9/ �������� ��� �������� ���� ,(79/06� ������ ��� ������� ����� �� ������ ���� � �������� ���� ��� ���� * ������� ����
�� �����*��� ��������� ������ ����������� * ������ �����0# ���� ������ *�������� � ��������� ����� ��� *�� � ������� ������� ���� "�2
� ++;0 "�2 � ++; �� ��*� �� ���� ���� ��4���� ���� �**���0 6� ���� "�2 � ++;����������� �� �� ������0
������� +�� ������ ���������� ���� ������ ����� �������� "����������� �������������5���� 2������ ��������� 2������ ������� .������� ����
��� ������ ������� ���������� �� ��������� ��������� ��� �������� ����������!�������� "��#���� $����� $��%������ &� '()*( $������ &�����
@ 3���4���� 2����� %!!
�16# & $4&(4)!84(&8(47��'�'��'��'����4$%7$ ,����'AA��0��0��A������B��C��'�'��'��'����4$%7$/
Dedication
“Patients deserve to be treated better than a side of beef”
The “ father” of interventional radiology Charles Dotter (1920-1985)
To my wife Elisabeth and my children Henrik and Martin

List of Original Papers
This thesis is based on the following original papers, which will be referred to in the text by their roman numerals.
I. Ljungdahl M, Eriksson L-G, Nyman R, Gustavsson S.: Arterial embolization in management of massive bleeding from gastric and duodenal ulcers. Eur J Surg 2002; 168(7):384-390.
II. Eriksson L-G, Sundbom M, Gustavsson S, Nyman R.: Endoscopic marking with metallic clip facilitates transcatheter arterial embolization in upper peptic
ulcer bleeding. J Vasc Interv Radiol. 2006 Jun; 17(6): 959-64.
III. Eriksson L-G, Ljungdahl M, Sundbom M, Nyman R.: Transcatheter arterial embolization versus surgery for treatment of upper gastrointestinal bleeding
after therapeutic endoscopy failure. Manuscript
IV. Eriksson. L-G, Lutvica-Mulic A, Jangland L, Nyman R.: Massive post partum haemorrhage treated with transcatheter arterial embolization; long-term effects,
implication on fertility and technical considerations. Acta Radiol. 2007 Jul;48(6):635-42.
Abstract ...................................................................................................................................................... 2Dedication .................................................................................................................................................. 3List of Original Papers ............................................................................................................................... 5Contents ..................................................................................................................................................... 7Abbreviations ............................................................................................................................................. 9Introduction ..............................................................................................................................................11
Historical background ..........................................................................................................................11Transcatheter Arterial Embolization (TAE) ........................................................................................ 12Anatomy ...............................................................................................................................................14Shock caused by hemorrhage (hypovolemic shock) ............................................................................. 19Clinical background ............................................................................................................................. 19
Aims of the thesis ..................................................................................................................................... 23Specific aims of individual studies: ...................................................................................................... 23
Material and methods .............................................................................................................................. 25Study I .................................................................................................................................................. 25Study II ................................................................................................................................................ 25Study III ............................................................................................................................................... 26Study IV ............................................................................................................................................... 26Embolization technique in upper GI bleeding ..................................................................................... 27Embolization technique in PPH ........................................................................................................... 27
Results ...................................................................................................................................................... 29Study I .................................................................................................................................................. 29Study II ................................................................................................................................................ 29Study III ............................................................................................................................................... 30Study IV ................................................................................................................................................31
Discussion ................................................................................................................................................ 33Conclusion ................................................................................................................................................ 35Summary in Swedish ................................................................................................................................ 36Acknowledgements ................................................................................................................................... 39References ................................................................................................................................................ 41
Contents

Abbreviations
PTA Percutaneous Transluminal AngioplastyTAE Transcatheter Arterial Embolization PVA Polyvinyl alcohol particlesGI Gastro IntestinalGDA Gastro Duodenal ArteryLGA Left Gastric ArterySMA Superior Mesenteric ArteryB-II Billroth IIIR Interventional RadiologySD Standard deviationmGY milli-GrayMAST Medical Anti Shock TrousersPPH Post Partum HemorrhageF French


11
Introduction
Historical backgroundThe first contrast enhanced x-ray image of a ves-sel was produced January 1896. Just a month after Wilhelm Conrad Roentgen’s discovery of x-rays, OT Lindenthal injected Teichman’s mixture into the veins of an amputated hand (1). However, many decades passed before angiography played a signif-icant role in medicine.
One of the most important historical landmarks in the latest 50 years is Sven-Ivar Seldinger’s ac-cess technique. In 1953 Dr. Seldinger (1921-1998) published the description of a percutaneous entry technique in the journal, Acta Radiologica (2). In “Pioneers of angiography” (3) he told how this hap-pened. He had been struggling with the problem of developing a better method of catheterization, when he had “a severe attack of common sense”:
“Now! After an unsuccessful attempt to use this technique, I found myself, disap-pointed and sad, with three objects in my hand - a needle, a wire and a catheter - and ... in a split second I realized in what sequence I should use them: Needle in, wire in, needle off, catheter on wire, cath-eter in, catheter advance, wire off.”
The discipline Interventional Radiology (IR) started early in 1960s when the diagnostic x-ray method shifted to a method also to treat. Fluoros-copy and x-ray imaging were used as a diagnos-tic tool followed by “transcatheter” treatment in varied conditions. One of the first interventional radiologists in this field was Charles Dotter (1920-1985). He altered the course of cardiovascular radi-
ology and is considered the father of IR. He began modifying the Seldinger technique for therapeutic purposes and described percutaneous transluminal angioplasty technique (PTA) 1964 (4). The society of Cardiovascular Radiology was founded in 1974. In addition to diagnostic angiography, members of this society were beginning to expand their inter-ventions. In addition to “Dottering” obstructive lesions, they were beginning to treat gastrointesti-nal bleeding and pelvic trauma by pharmacologic infusion and embolization (5).
Another important landmark in IR history was the invention of the PTA balloon 1974 by A Gru-entzig. He developed a new balloon catheter, man-ufactured the device on his kitchen table and used it first on February 12, 1974 in a patient with inter-mittent claudication due to subtotal stenosis of the superficial femoral artery (6, 7).
J Rosch reported the first case of transcatheter arterial embolization (TAE) for acute upper gas-trointestinal bleeding in 1972. He performed a se-lective catheterization of gastroepiploic artery in a patient with a prepyloric bleeding ulcer and inject-ed epinephrine combined with autogenous blood clot as embolic agent (8).
BJ Brown et al reported the first case of emboliza-tion for post partum bleeding in 1979. Three sepa-rate surgical procedures failed to reveal the source of bleeding and standard surgical techniques, in-cluding bilateral ligation of the hypogastric arter-ies were unsuccessful in producing hemostasis. Angiography successfully identified the specific bleeding vessel, and transcatheter embolization with gelatin sponge fragments stopped the hemor-rhage (9).

12
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
Transcatheter Arterial Embolization (TAE)A guidewire and a catheter are inserted into an ar-tery under fluoroscopy guidance. Contrast media is injected into the artery during recording images. The blood flow and the shape of the vessel wall can be evaluated and sources of internal bleeding can be detected. By using material that creates a throm-bus (embolic agent), applied through the catheter into the bleeding site, the vessel will be occluded and the bleeding stopped.
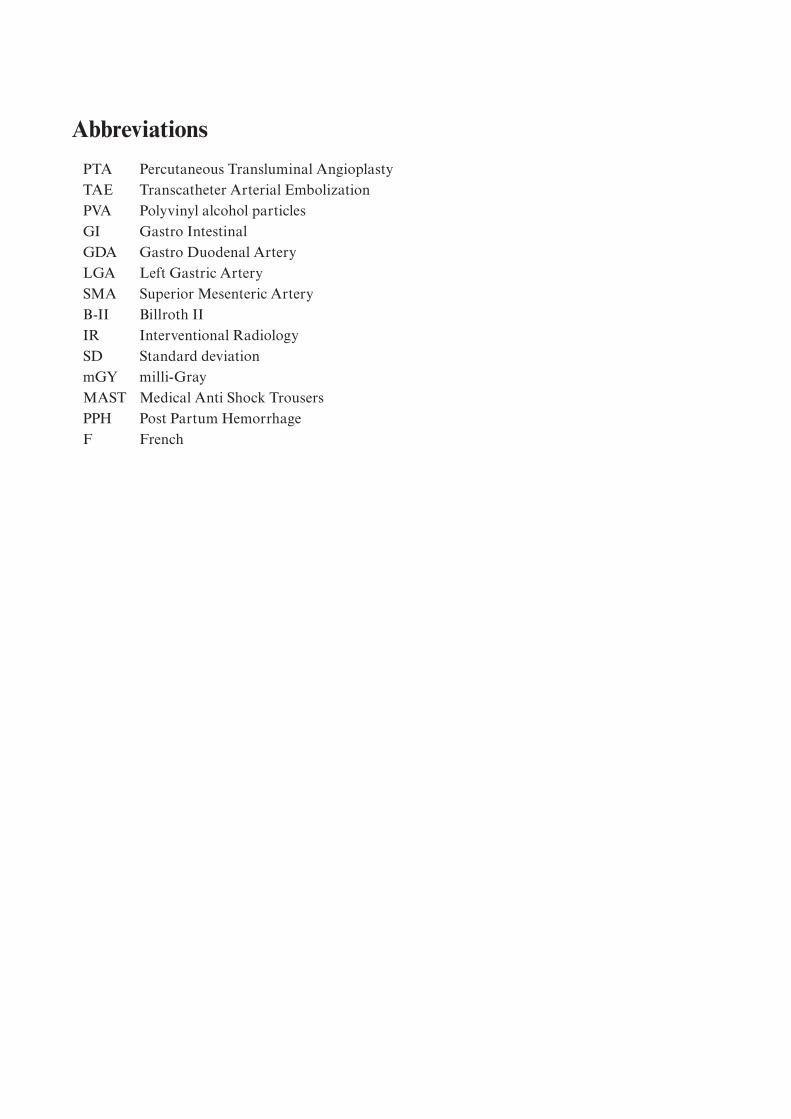
The angiographic sign of ongoing bleeding are contrast media extravasation (fig. 1). It has been shown experimentally that a bleeding rate as low as 0.5 mL/min can be demonstrated angiographically (10). Other useful signs in locating the bleeding site are a “pseudoaneurysm” like lesion in the artery (fig. 2). However, frequently intermittent bleeding brings about difficulties to choose the exact area/site for embolization, when no bleeding signs are identified at angiography. In order to overcome this problem the bleeding can be provoked by injecting vasodilators and/or anticoagulants selectively into the suspected bleeding vessel.
There is a large number of embolic agents i.e. metallic coils, gelatin sponge, polyvinyl alcohol particles (PVA), microspheres, glue, alcohol etc. to chose between.
Large embolic agents such as coils and gelatin sponge pledgets are mostly preferable for large ves-sels. Especially in organs with a rich collateral sup-ply (such as stomach, duodenum and uterus) can proximal vessel be occluded without risk of tissue infarction.
Liquid agents such as alcohol or glue will in most cases embolize the most distal vascular supply and result in ischemia and/or infarcted tissue. Some materials such as gelatin sponge are biodegradable and should be used when recanalization of the em-bolized vessel are desirable.
Gelatin sponge is a water-insoluble hemostatic material prepared from purified skin gelatin, in-tended for application to bleeding surfaces. It is used as a biodegradable, intravascular embo-lic agent. Gelatin sponge promotes hemostasis by development of and providing structural support to thrombus. Pledgets cut from a sheet of gelatin sponge are large and will result in a proximal ar-tery occlusion. An additional technique is to create gelatin sponge slurry by mixing gelatin sponge and contrast media between two syringes via a stop-cock. Gelatin sponge has the potential to induce a short-term occlusion with minimum tissue reac-tion and is absorbed completely, with little tissue reaction. This absorption is dependent on several factors, including the amount used, degree of satu-ration with blood or other fluids, and the site of use. Studies have revealed that the resorption time for gelatin sponge used intravascular occurs within 7-21 day after embolization (11).
Metallic coils were made by cutting pieces of a guide wire. They are now available in different shapes and sizes. Thrombogenic synthetic fiber bundles are attached to the metallic pieces provid-ing structural and chemical support to thrombus causing a permanent occlusion of the vessel. A coil with size 0.018-inch (0.46 mm) in diameter is called “microcoil” and a coil with size 0.035-inch (0.89 mm) in diameter is called “macrocoil” (fig. 3).
13
Introduction
Figure 2. Celiac artery injection (black arrow) shows the GDA with pseudoaneurysm like lesion (white arrow).
Figure 1. Celiac artery injection (black arrow) shows the GDA with extravasation of contrast media (white arrow).
Figure 3. Microcoils in different shapes with trombogenic synthetic fibers.

14
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
AnatomyKnowing the anatomy of the vascular supply of a specific bleeding organ is a prerequisite for a suc-cessful treatment using TAE and to avoid severe complications. A rich collateral network charac-terizes the arterial supply to the upper GI organs as well as the uterus.
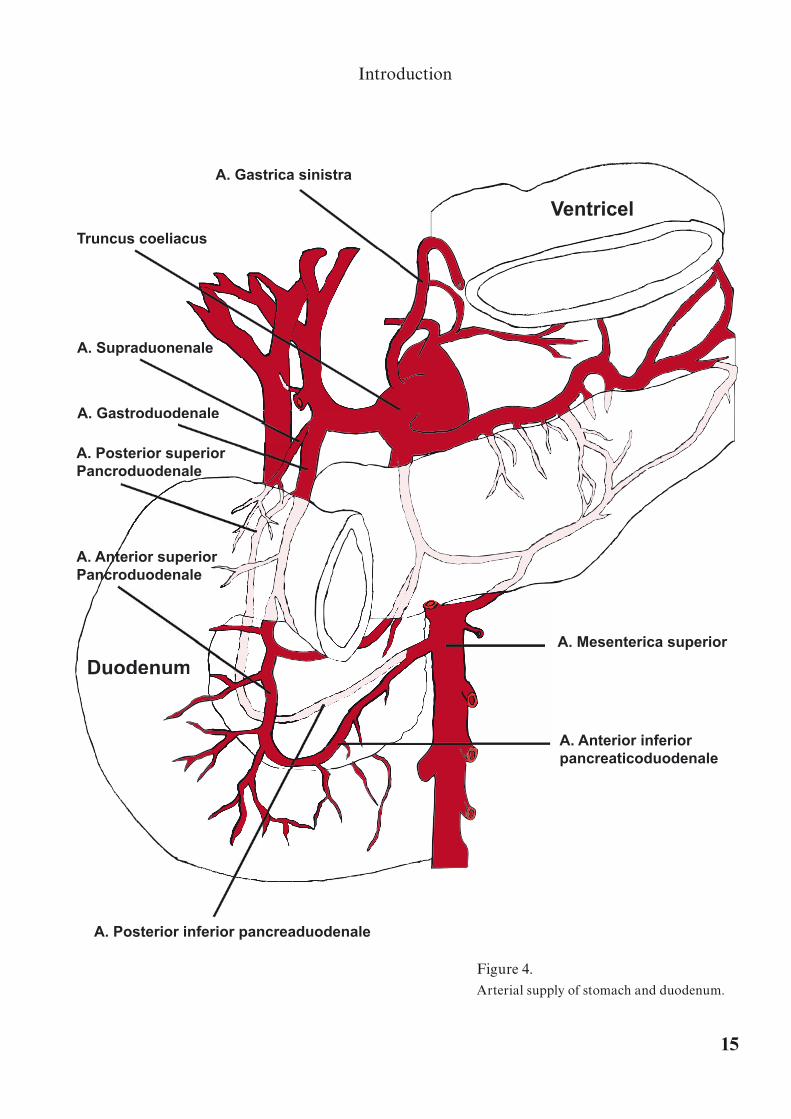
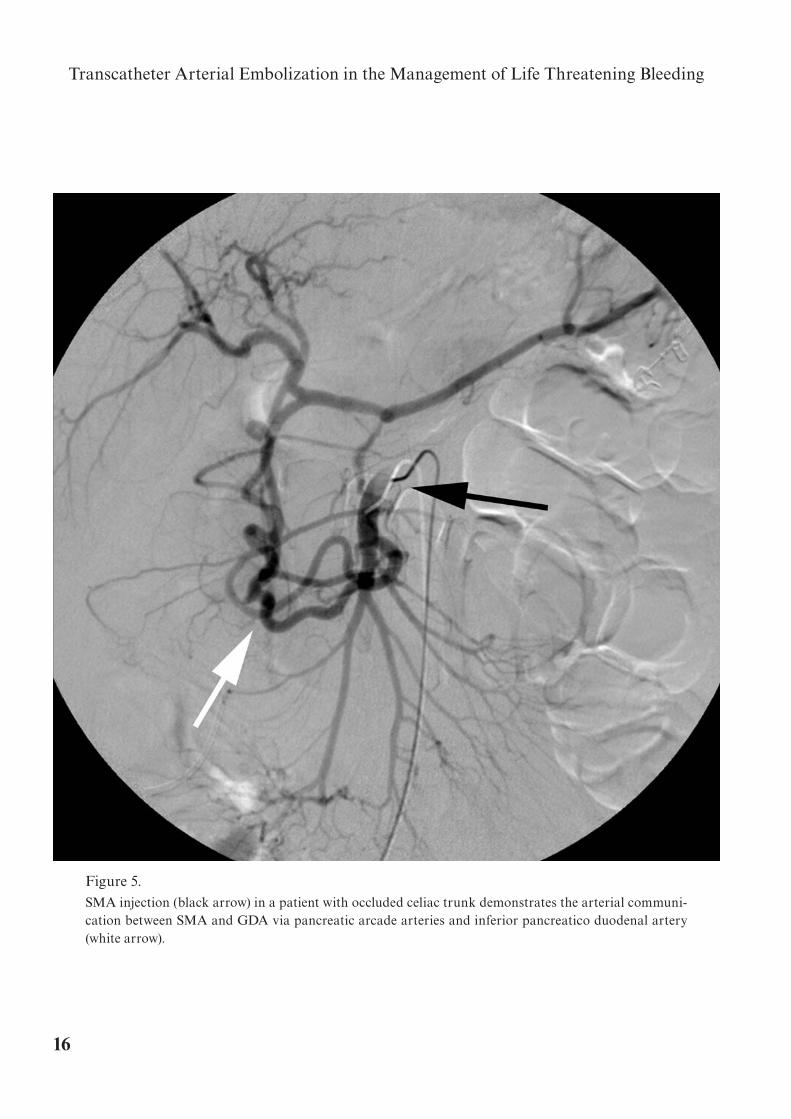
Arterial supply of duodenum reaches the duode-num on its posterior aspects to spread afterwards along its anterior aspect (12) (fig. 4). Both branches from the gastroduodenal artery (GDA) and su-perior mesenteric artery (SMA) and occasionally branches arising from the proper hepatic artery i.e. supraduodenal artery (13) supply the duodenum. A rich arterial communication exists between the GDA and SMA via the pancreatic arcade arteries and inferior pancreatico duodenal artery (14) (fig. 5).
The left gastric artery (LGA) arises from the ce-liac artery it supplies the lower third of the esoph-agus and the upper part of the stomach. The left gastroepiploic artery arises from the splenic artery it supplies the stomach along the upper part of the greater curvature. The right gastroepiploic artery arises from the gastroduodenal branch of the he-patic artery it supplies the lower part of the greater curvature.
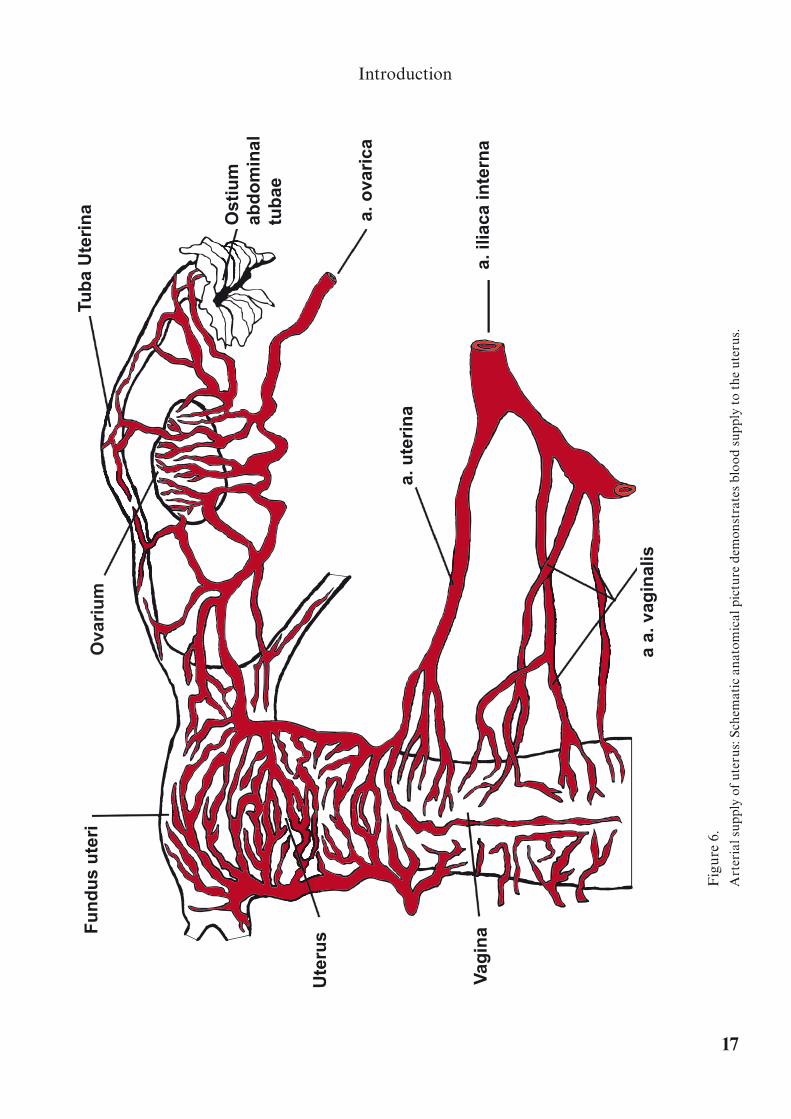
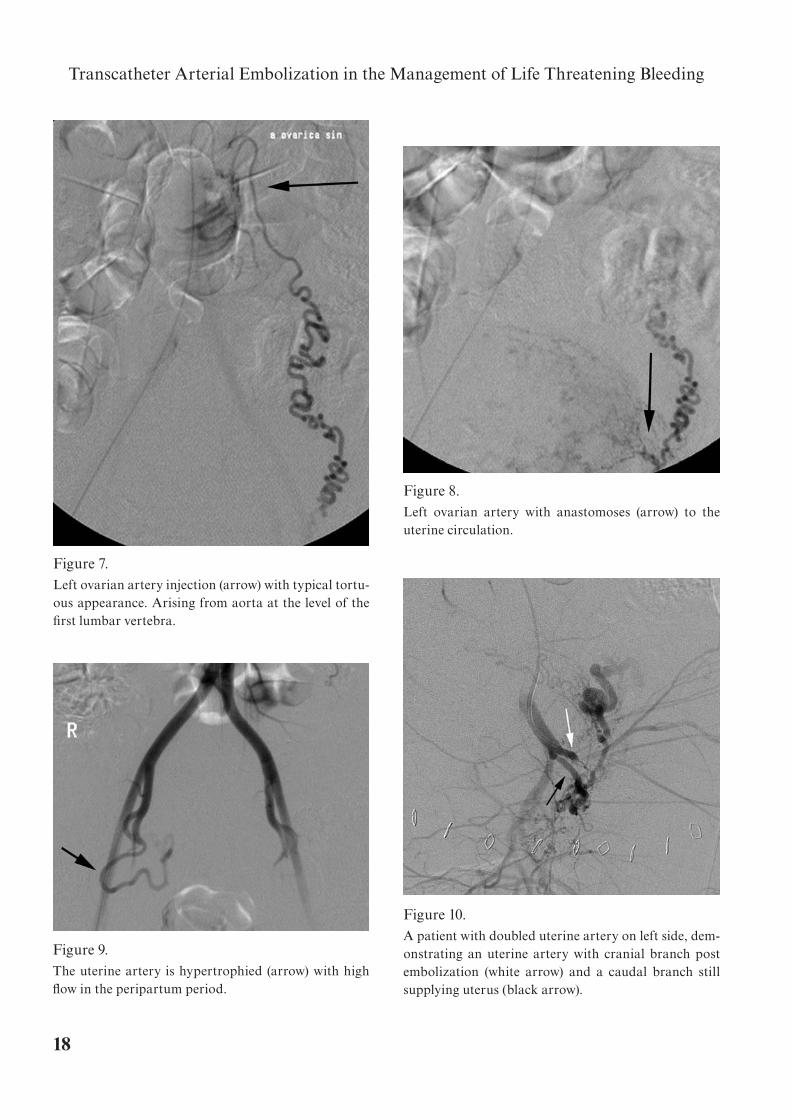
The arterial supply to the uterus (fig. 6) origi-nates mainly from the uterine artery, arising from internal iliac artery, and also some from the ovar-ian artery, arising from aorta at the level of the first lumbar vertebra (fig. 7) (15, 16). The uterine artery and the ovarian artery form anastomoses in the area of the adnexa structures (fig. 8). The uterine artery is hypertrophied with high flow in the peri-partum period (fig. 9). Rarely the uterine arteries are doubled (fig. 10).
15
Introduction
A. Anterior inferiorpancreaticoduodenale
A. Mesenterica superior
Ventricel
A. Posterior inferior pancreaduodenale
Duodenumodenum
A. Anterior superiorPancroduodenale
A. Posterior superiorPancroduodenale
uperiornale
A. Gastroduodenaleoduodenale
A. Supraduonenale
rooduodenale
aduonenale
Truncus coeliacus
A. Gastrica sinistra
Figure 4.Arterial supply of stomach and duodenum.
16
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
Figure 5. SMA injection (black arrow) in a patient with occluded celiac trunk demonstrates the arterial communi-cation between SMA and GDA via pancreatic arcade arteries and inferior pancreatico duodenal artery (white arrow).
17
Introduction
Fig
ure
6.
Art
eria
l sup
ply
of u
teru
s: S
chem
atic
ana
tom
ical
pic
ture
dem
onst
rate
s bl
ood
supp
ly t
o th
e ut
erus
.
a a.
vag
inal
is
a. il
iaca
inte
rna
a. o
vari
ca
Ost
ium
abd
om
inal
tub
ae
a. u
teri
na
Vag
ina
Ute
rus
Tub
a U
teri
na
Ova
riu
mF
un
du
s u
teri
18
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
Figure 7. Left ovarian artery injection (arrow) with typical tortu-ous appearance. Arising from aorta at the level of the first lumbar vertebra.
Figure 8. Left ovarian artery with anastomoses (arrow) to the uterine circulation.
Figure 9. The uterine artery is hypertrophied (arrow) with high flow in the peripartum period.
Figure 10. A patient with doubled uterine artery on left side, dem-onstrating an uterine artery with cranial branch post embolization (white arrow) and a caudal branch still supplying uterus (black arrow).
19
Introduction
Shock caused by hemorrhage (hypovolemic shock)Hemorrhage is the most common cause of hypo-volemic shock. Hemorrhage decreases the mean systemic filling pressure and as a consequence de-creases venous return, cardiac output falls below normal and shock ensues.
Approximately 10% (350-550 mL) of total blood volume can be removed with no significant effect on arterial pressure or cardiac output. Greater blood loss usually diminishes the cardiac output and blood pressure falls (17). Both cardiac output and blood pressure will fall to zero when about 35-45% (1500-2500 mL) of the total blood volume has been removed. The decrease in blood pressure ini-tiates a sympathetic reflex that stimulates the vaso-constrictor system throughout the body resulting in constriction of the arterioles in most parts of the body and thereby greatly increasing the total peripheral resistance (18). The veins and venous reservoirs constrict, thereby helping to maintain adequate venous return despite diminished blood volume. Furthermore, heart rate will increase markedly.
Clinical background
Upper peptic ulcer bleeding is usually presented with hematemesis with bright red blood or brown clumps of partially digested blood similar to coffee grounds and bloody or black faeces combined with low blood pressure, dizziness and fainting.
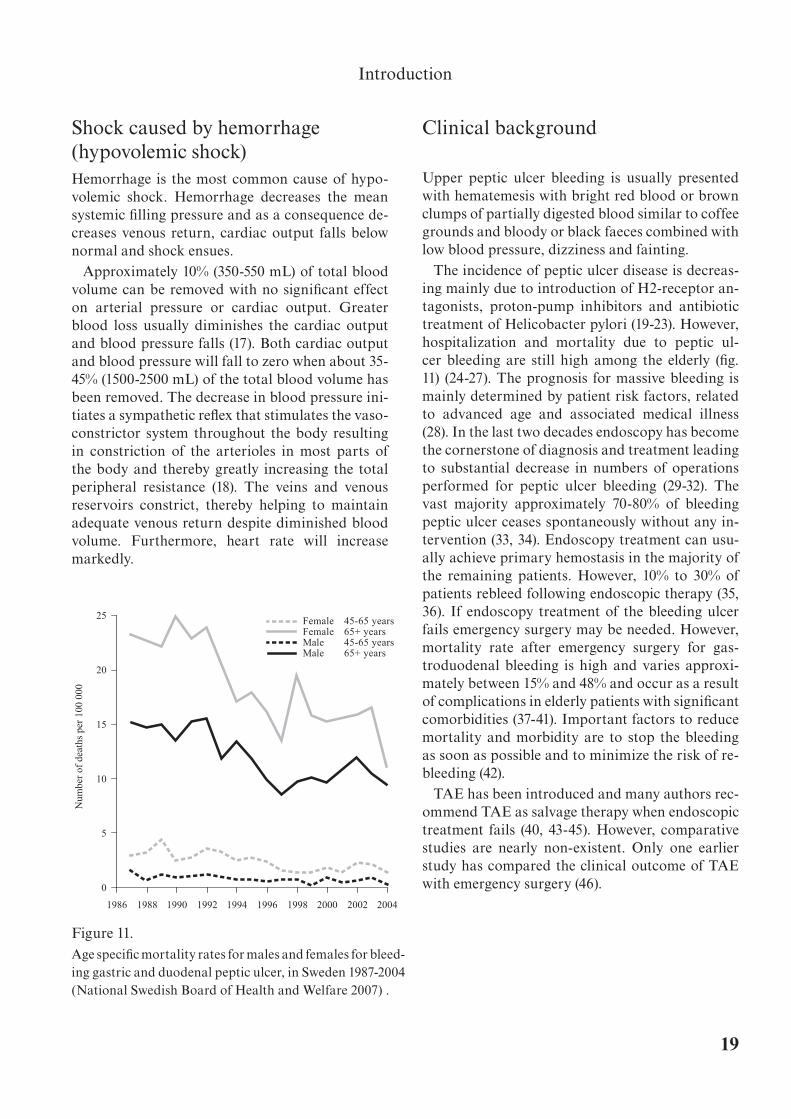
The incidence of peptic ulcer disease is decreas-ing mainly due to introduction of H2-receptor an-tagonists, proton-pump inhibitors and antibiotic treatment of Helicobacter pylori (19-23). However, hospitalization and mortality due to peptic ul-cer bleeding are still high among the elderly (fig. 11) (24-27). The prognosis for massive bleeding is mainly determined by patient risk factors, related to advanced age and associated medical illness (28). In the last two decades endoscopy has become the cornerstone of diagnosis and treatment leading to substantial decrease in numbers of operations performed for peptic ulcer bleeding (29-32). The vast majority approximately 70-80% of bleeding peptic ulcer ceases spontaneously without any in-tervention (33, 34). Endoscopy treatment can usu-ally achieve primary hemostasis in the majority of the remaining patients. However, 10% to 30% of patients rebleed following endoscopic therapy (35, 36). If endoscopy treatment of the bleeding ulcer fails emergency surgery may be needed. However, mortality rate after emergency surgery for gas-troduodenal bleeding is high and varies approxi-mately between 15% and 48% and occur as a result of complications in elderly patients with significant comorbidities (37-41). Important factors to reduce mortality and morbidity are to stop the bleeding as soon as possible and to minimize the risk of re-bleeding (42).
TAE has been introduced and many authors rec-ommend TAE as salvage therapy when endoscopic treatment fails (40, 43-45). However, comparative studies are nearly non-existent. Only one earlier study has compared the clinical outcome of TAE with emergency surgery (46).
Figure 11.Age specific mortality rates for males and females for bleed-ing gastric and duodenal peptic ulcer, in Sweden 1987-2004 (National Swedish Board of Health and Welfare 2007) .
1986 1988 1990 1992 1994 1996 1998 2000 2002 2004
0
5
10
15
20
25
Num
ber
of d
eath
s pe
r 10
0 00
0
Female 45-65 yearsFemale 65+ yearsMale 45-65 yearsMale 65+ years

20
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
The maternal blood volume shortly before deliv-ery is approximately 30% above the normal. The cause of the increased blood volume is mainly hormonal, causing increased fluid retention by the kidneys. The bone marrow becomes increasingly active and produces an excess of red blood cells combined with the excess fluid volume. Therefore, at the time of birth of the baby, the mother has ap-proximately 1 to 2 liters of extra blood volume in her circulation system, allowing the mother to be able to bleed significant with a considerably safety factor.
Severe Post Partum Hemorrhage (PPH) may evolve very rapidly and unexpected and can be-come life threatening within a few minutes. Ob-stetrical mechanical and medical treatment will manage most cases but in some cases emergency surgery is needed and in the worst case can result in hysterectomy. Hysterectomy is a major psycho-logical trauma to a young woman and a high-risk operation following a massive bleeding.
Although maternal mortality rates have declined greatly in the developed countries, post PPH re-mains a leading cause of maternal mortality else-where. According to World Health Organization PPH is considered to be responsible for 25% of ma-ternal death worldwide (47). The mortality rate per million maternities in United Kingdom has more than doubled since the previous triennium 1997-1999 (48) and severe PPH remains a common medi-cal emergency problem even in western countries.
PPH is defined as an estimated blood loss of more than 500 mL with vaginal delivery (49) and more than 1000 mL for cesarean section (50). However, This definition is of limited practical use as accu-rate quantification of blood loss is seldom possible, because of difficulties in evaluation of blood loss with visual observation only. It have been suggest-
ed that PPH should be diagnosed with any amount of blood loss that threatens the hemodynamic sta-bility of the woman. Combs et al defined PPH by a post partum hematocrit drop of 10% or by need for transfusion (49). PPH is classified as early within the first 24 hours and late after 1 day to 6 weeks af-ter delivery (51). The main cause of PPH is uterine atony and retained placental tissue. Other causes are placental abnormalities such as placenta ac-creta, praevia and abruption, lacerations of the perineum, vagina or cervix, vessel malformations, ruptured uterus and coagulations defects.
Extensive blood loss due to PPH can lead to hy-povolemic shock, severe coagulation disorder and serious morbidities such as renal and hepatic fail-ure, adult respiratory distress syndrome and rarely pituitary gland necrosis (52). It is estimated that excessive bleeding complicates 5–15% of delivery (50).
TAE has been developed as an alternative to sur-gery and has been shown to preserve fertility and reduce morbidity (53-56). However, the long-term effect is not well known. A few authors have re-ported data regarding the long-term effect on the menstrual cycle and the possibility of preserved fertility (57-60).
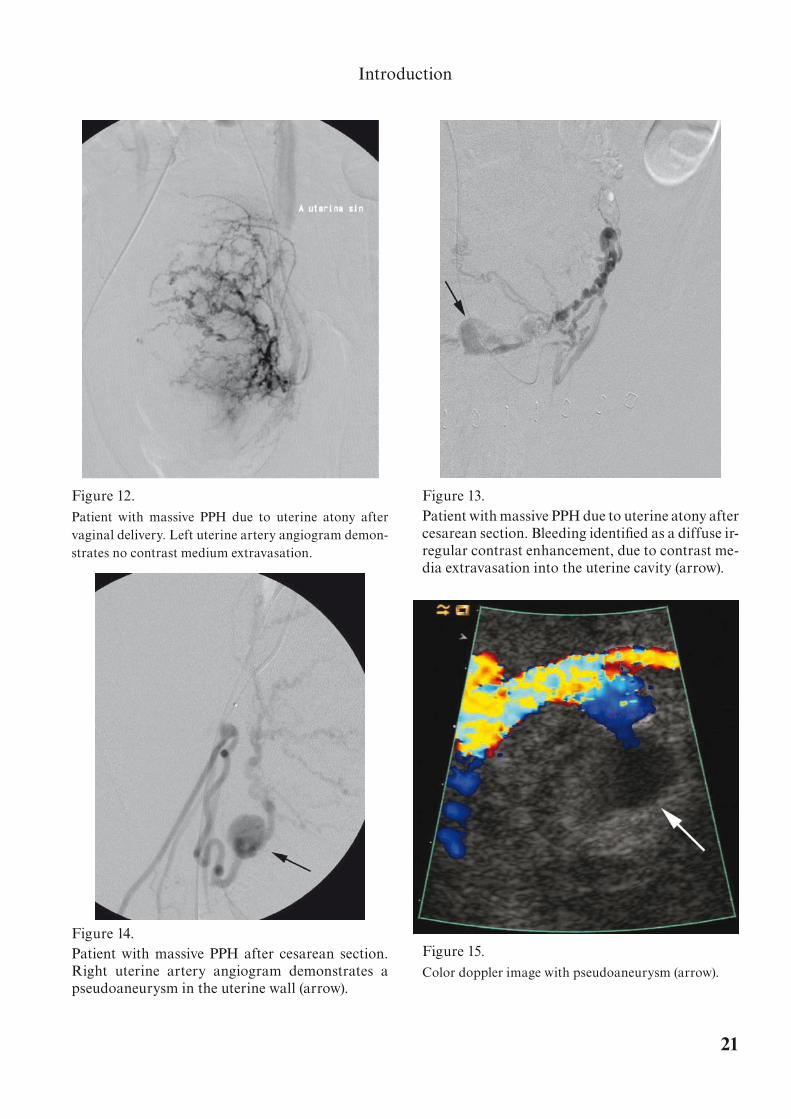
Bleeding caused by uterine atony is often present-ed without contrastmedia extravasation (fig. 12) or identified as a diffuse irregular contrast enhance-ment with tortuous vessels at angiography (fig. 13). Pseudoaneurysm is presented as a rounded well-shaped contrast-enhanced structure in the uterine wall or the cavity of the uterus (fig. 14). On color Doppler images pseudoaneurysm are presented as a rounded anechoic structure with posterior acous-tic enhancement and showing swirling blood flow (fig. 15).
21
Introduction
Figure 12. Patient with massive PPH due to uterine atony after vaginal delivery. Left uterine artery angiogram demon-strates no contrast medium extravasation.
Figure 13. Patient with massive PPH due to uterine atony after cesarean section. Bleeding identified as a diffuse ir-regular contrast enhancement, due to contrast me-dia extravasation into the uterine cavity (arrow).
Figure 14. Patient with massive PPH after cesarean section. Right uterine artery angiogram demonstrates a pseudoaneurysm in the uterine wall (arrow).
Figure 15. Color doppler image with pseudoaneurysm (arrow).

22
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
23
Study aims
Aims of the thesis
Evaluate the clinical usefulness, improve the TAE technique and compare the outcome of TAE with surgery used as “salvage therapy” in patients with upper GI bleeding. Evaluate TAE technique and the long-term effect on the menstrual cycle and fertility in severe PPH.
Specific aims of individual studies:
1. Assess the therapeutic usefulness in patients managed with TAE in non-variceal upper GI-bleeding.
(Study I)
2. Develop a method to mark the bleeding site in upper peptic ulcer bleeding with a metal-lic clip during endoscopy used as a guide in TAE in order to enhance the possibility that the correct area is embolized.
(Study II)
3 Compare the clinical outcome in patients treated with either TAE or surgery in severe upper GI-bleeding after failed endoscopic treatment.
(Study III)
4 To evaluate early and late complications in patients with severe PPH managed with TAE and its influence on menstrual cycle and fertility and to improve the embolization technique.
(Study IV)
24
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding

25
Material and Methods
Material and methods
Study IA study of 18 patients between October 1998 to Sep-tember 2001 (eleven women and seven men, mean age 78 years, range 53 to 94 years). With massive peptic ulcer bleeding treated with TAE. Thirteen patients were treated with TAE after endoscopic treatment failure and 5 patients were treated for recurrent hemorrhage after emergency surgery. All patients were selected to TAE because they were considered poor surgical candidates caused by concurrent diseases and hemodynamic insta-bility. Data recorded were; patient demographics, concurrent diseases, endoscopic diagnosis, surgi-cal report, hemoglobin concentration, and blood pressure, transfusion requirement, angiographic treatment, complications, need for operation and in-hospital mortality.
All angiographic procedures were performed with standard percutaneus transfemoral catheter-ization. The celiac trunk and SMA were selectively examined. Ongoing bleeding was defined as ex-travasation of contrast media or a pseudo-aneu-rysm like lesion. Embolization was performed as close as possibly and on both sides of the bleeding site. If no bleeding site were identified a “blind” embolization of the entire GDA or LGA was per-formed depending of the result of the endoscopic examination. In all patients metallic coils were used as embolic agent.
Study IIA study of 13 patients between September 2003 and February 2005 (five women and eight men, mean age of 75 years, range 30-93 years) with massive upper peptic ulcer bleeding. The bleeding site was identified with endoscopy and treatment performed to stop the bleeding. The ulcer was then marked with placement of a metallic clip at its edge. The purpose was to locate the exact site of the bleeding ulcer at angiography in order to facilitate the TAE procedure. Only ulcers considered by the endosco-pist to present a high risk of recurrent bleeding or hemostasis considered less feasible were marked.
Angiography with TAE was performed if the patient continued to experience bleeding or had a recurrence of bleeding. Guided by the placed metallic clip the catheterization was performed as selectively as possible and the branches closest to the clip were embolized. A transfemoral approach was used in all cases. Both the celiac trunk and SMA were selectively examined. Three patients had definite hemostasis after endoscopy and were not treated with embolization; instead they were examined with plain upper radiography every 24 hours until the clip was found to be dislocated at a maximum of 5 days. Benefit from clip marking was considered when there was no sign of contrast media extravasation before embolization and if the clip made it possible to identify and efficiently em-bolize the vessel close to the clip.

26
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
Study IIIFrom January 1998 to December 2005 a total of 658 patients were diagnosed with upper GI bleed-ing due to gastric or duodenal ulcer, combined gas-tric ulcer and duodenal ulcer, stomal ulcer or Die-lafoys lesion. In 567 (86%) patients who underwent emergency endoscopy, the bleeding had ceased either spontaneously or was successfully stopped by endoscopic treatment (one or two attempts). Ninety-one (14%) patients rebleed or continued to bleed after initial emergency endoscopy treatment and were managed with either surgery or TAE. These 91 patients were included in the study. Forty patients (18 included in paper I) were treated with TAE and 51 patients were treated with surgery.
A retrospective analysis with a review of the medi-cal records was performed. The following variables were recorded: demographic variables, endoscopic diagnoses, comorbidities, the lowest hemoglobin levels, total transfusion requirements, hospitaliza-tion lengths, post procedure complications, and mortality rates. Relative survival rate was calcu-lated. Survival probability was calculated with Ka-plan Meier technique.
The patients were mainly referred to TAE when they were considered as poor surgical candidates because of their high comorbidities. Since 2002, there has been a complete on call system for inter-ventional radiologists in our institution. Emboliza-tion of GDA was performed in 33 patients, embo-lization of LGA in 5 patients and both GDA and LGA in 2 patients.
In the surgical group emergency surgery with a BII-resection was performed in 29, duodenotomy or gastrotomy and over-sewing of the bleeding ul-cer/artery in 14, re-resection after previous B-II resection in 6 and other types in 2 patients (explor-ative laparotomy and small intestine resection).
Study IVA retrospective study of 20 patients (mean age 30 years, range 23-40 years) with severe PPH treated with bilateral TAE of the uterine artery. The pa-tients were treated between 1993 and 2004. Seven patients had vaginal delivery (1 after vacuum ex-ceresis due to miscarriage) and 13 had cesarean section delivery.
If the obstetrical treatment failed with continu-ous bleeding the patient was referred to angiog-raphy and TAE. To determine the long-term side effects and implications on menses and fertil-ity the patients were asked to answer a question-naire regarding their post embolization history. Pregnancies since the embolization, attempting to get pregnant, infertility, miscarriages, number of pregnancies, term or preterm, delivery method, menses, pain history, bladder problems and incon-tinence were asked for. Clinical, biochemical and hematological data were collected from the medi-cal records. Gelatin sponge and coils were used as embolic agent.
The radiation dose was measured in 6 patients and the radiation dose to the ovaries was calcu-lated.

27
Material and Methods
Embolization technique in upper GI bleedingA transfemoral approach was used in all cases by placing a 5F (1.67 mm) introducer into the com-mon femoral artery. The celiac trunk and SMA were selectively examined using a 4F (1.35 mm) catheter (SHK, Cordis, Miami Lakes FL, USA; Cobra, Terumo, Tokyo, Japan). The GDA or LGA was then selectively catheterized using a 3F (1.00 mm) Microcatheter system (Tracker, Boston sci-entific, Natick MA, USA). Iodine contrast media (Omnipaque 200 mgI/mL, Amersham GE Health-care AS, Norway) were injected by hand 5-10 mL/injection.
Depending of the endoscopic findings, extrava-sation of contrastmedia at angiography or the po-sition of a marking metallic clip (a technique to mark the bleeding site at endoscopy used in our in-stitution since 2003 (66)), a selective catheterization of the bleeding branch was performed. When no contrast media extravasation was seen or when no marking clip were placed a “blind” embolization of entire GDA or LGA was performed, depending of the endoscopic findings. Both sides of the bleed-ing site were embolized in order to prevent “back door” bleeding. The endpoint was complete occlu-sion of the target vessel or occlusion of the vessels as near as possible to the extravasation or marking clip. No embolic agents other than coils was used in this study, 0.035-inch (0.89 mm) stainless steel macrocoils (William Cook, Europe, Denmark) or 0.018-inch (0.46 mm) platinum microcoils (Boston scientific, Natick MA, USA). The procedures were performed in local anesthesia in all patients.
Embolization technique in PPH
A catheter was placed into abdominal aorta at the level of the renal arteries. Approximately 20 mL Iodine contrast media (10-15 mL/s) (Omnipaque 200 mgI/mL) were injected. Images of the pelvic region were obtained in order to identify the type of lesion, the position of the uterine arteries and possibly supply from ovarian arteries. Both uter-ine arteries were selectively catheterized from a unilateral transfemoral approach (Cobra catheter, Terumo Tokyo, Japan) and 5-10 mL contrast media were injected by hand to confirm correct position. A piece of gelatin sponge intended for local he-mostasis in surgery (Gelfoam®, Pharmacia & Up-john, Kalamazoo, Mich, USA) was scraped with a scalpel. Approximately 1-3 square centimeters of gelatin sponge was suspended in a solution mixed with 50% saline and 50% contrast media (Omni-paque 200 mgI/mL) to create a slurry by mixing between two syringes via a three-way stopcock. It was then injected into both uterine arteries regard-less if contrast media extravasation was seen or not until circulatory arrest was obtained. If selective catheterization was impossible (i.e. due to spasm) the embolization material were injected at the level of the anterior division of the internal iliac artery. If there was a clear vessel tear micro- or macrocoils were used as embolic agent unilaterally to obtain hemostasis in addition to the gelatin sponge mix.

28
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding

29
Results
Results
Study ISuperselective catheterization and embolization were feasible in all patients. In 9 of 13 patients, treated primarily with TAE, extravasation of con-trast media at angiography indicated continuing bleeding. Immediate hemostasis was achieved in 8 of these patients. One patient continued to bleed after embolization and required an emergency op-eration. One patient needed a reemobilization after 3 days for recurrent bleeding. In 4 patients there were no signs of bleeding at the time of angiog-raphy and the main artery (GDA) was embolized (“blind embolization”) because of the findings at endoscopy. In one patient with a Dieulafoys lesion sclerotherapy and embolization failed to stop the bleeding. This patient had an emergency operation and the lesion was over-sewn but the patient died 18 days postoperatively.
Five patients were treated for recurrent bleeding after surgery. Four of the 5 patients showed signs of continuing bleeding at the time of angiography. Hemostasis was obtained in all 5 after emboliza-tion one needed a reemobilization for recurrent bleeding after 25 days. All patients in this group recovered satisfactorily.
Study IITen of 13 patients underwent angiography. In 8 patients hemostasis was obtained after emboliza-tion. Two patients underwent emergency surgery, 1 with occluded celiac trunk making catheteriza-tion impossible, and 1 with multiple large duodenal ulcers not possible to treat with TAE. In 1 patient reembolization was necessary to obtain final he-mostasis.
The clip stayed in place in 11 patients and was dis-located in 2 patients at the time of x-ray. The result of the embolization procedure benefited from the clip marking in 6 patients. The clip made it easier to identify the suspected bleeding vessel without sign of contrast extravasation. The bleeding vessel was the supraduodenal artery with no connection to GDA in 2 cases and the pancreatic inferior ar-tery with connection with superior mesenteric ar-tery in 1 case. It was possible to reduce the “coiled distance” in 3 cases with suspected bleeding site directly from GDA. In these cases a short distance of GDA were embolized as close as possibly and on both sides of the clip. In 1 case with clear contrast media extravasation there was no benefit from the clip. The extravasation in this case was observed close to the clip. In the 8th case the clip had dislo-cated at the time of TAE.
There were no complications observed and no patient developed signs of ischemia leading to per-foration or problems with gastric emptying.

30
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
Study IIIThe most common causes of bleeding were duo-denal ulcers, 83% in patients referred to TAE and 63% in patients referred to surgery. Patients who underwent TAE were older (76 years, SD 10) and had slightly more comorbidities than the patients who underwent surgery (71 years, SD 13). Hospi-talization time was slightly longer in the surgical group (13 days, range 2-67) compared to the TAE group, (10 days range 3-43). The lowest hemoglo-bin level (median 72 g/L) was equal in both groups. The group treated with TAE required transfusions of median 17 units of packed red cells (range 3-50) compared to 19 (range 0-90) units in the surgical group.
Primary hemostasis was achieved in 30 of 40 (75%) who underwent TAE and 42 of 51 patients (82%) who underwent surgery. Five of 10 patients who rebled or continued to bleed after TAE were treated with a second TAE procedure and hemo-stasis was achieved in all 5 patients. The remaining 5 patients underwent emergency surgery. Hemo-stasis was achieved in 4 patients (3 bleeding ulcers were over-sewn and 1 BII-resection). The 5th pa-tient underwent exploration and no ongoing bleed-ing was identified at the time of surgery. No com-plications related to the embolization procedure, such as groin hematoma or bowel ischemia leading to perforation or problems with gastric emptying, were observed.
Eight of 9 patients who rebleed or continued to bleed after surgery was treated with TAE and he-mostasis were achieved in all 8 patients. One pa-tient was successfully reoperated and the bleeding vessel was over-sewn. Two additional patients in the surgical group, needed a second surgical pro-cedure due leakage with abscess formation after BII-resection.
Thirty-day mortality rate in patients treated with TAE was 1 of 40 (3%) compared to 7 of 51 (14%) in patients treated by surgery (p<0.07). None of these patients who died had a second procedure of either TAE or surgery. The cause of death in the patient who died within 30-days after TAE (age 79 years) was multi organ system failure. All 7 patients who died after surgery were elderly with a mean age of 80 years (range 71-89 years). The causes of death were multiorgan failure in 4 patients, myocardial infarction in 1, respiratory failure in 1 and septice-mia with shock in 1 patient.
The Kaplan-Meier estimate shows that the initial differences in mortality rate between the 2 groups were equalized after 1 year. The relative survival curve demonstrates that both groups have similar mortality rate and somewhat higher than that of an aged matched control group. Around 50% of the patients in both groups were alive 5 years after the actual episode of peptic ulcer bleeding.

31
Results
Study IVHemostasis using TAE was obtained in all 20 pa-tients. In 18 cases selective embolization of the uterine arteries was performed, in 2 cases the ante-rior division of internal iliac was embolized due to spasm of the uterine artery. No bleeding supplied from the ovarian arteries was identified.
Seven patients had vaginal delivery and no sign of contrast media extravasation was observed in this group. Absorbable gelatin sponges were used in all 7 cases as the primary embolic agent and no metallic coils were used. Two patients rebled and were reembolized using gelatin sponge as embo-lic agent. Two patients needed curettage to obtain hemostasis in addition to embolization due to re-tained placental parts.
Thirteen patients had cesarean section delivery. Gelatin sponge were used in all 13 cases as the pri-mary embolic agent, in 2 of these cases coils were added due to massive contrast media extravasa-tion. In this group with obstetric hemorrhage after cesarean section reembolization was necessary in 5 patients. Four had clear signs of contrast me-dia extravasation, primarily only embolized with gelatin sponge. They were all successfully reembo-lized with coils unilaterally One case had no signs
of extravasation of contrast and was successfully reembolized using only gelatin sponge. All the 20 patients who were contacted answered the ques-tionnaire. The only short-term complication reg-istered was a temporary low-grade fever reaction in 7 patients. The average follow-up time was 8.2 years (follow-up range 1.0-12.1 years). The number of registered long-term complications was 6. Endo-metrial infection in 1 patient 3 weeks after embo-lization. Two patients had complained of transient pelvic pain, 2 with transient numbness in legs and 1 patient with reduced tactile sensitivity in right thigh. Normal menses resumed in all patients.
Four patients had a total of 5 full-term and 2 pre-term (gestation week 34 and 35) pregnancies. All delivered healthy infants by cesarean section with no recurrence of PPH. One of these patients had 3 full-term infants and also 1 miscarriage (gestation week 9). They all had a follow-up time longer than 4 years. One patient had six unsuccessful in vitro fertilization attempts. There was no desire and no attempts to get pregnant in the group with follow up time between 1.6-2.6 years.
The mean radiation dose to the ovaries was 586 mGy (range 204-729 mGy).

32
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding

33
Discussion
Discussion
The results in this thesis demonstrate that TAE is a minimal invasive, safe and effective method to treat different life threatening bleedings and should be the method of choice instead of surgery. The method was here applied in upper GI and PPH, but the method has also been found applicable in many other areas. TAE can be used in many situations such as trauma, lower GI, nasal and postoperative hemorrhages (61-63).
Endoscopic therapy is the method of choice in patients with upper GI bleeding. Study I indicat-ed that TAE was effective and an alternative to emergency surgery for control of massive upper GI bleeding, especially in elderly patients with concur-rent diseases and when endoscopic treatment fails. The outcome of an acute GI bleeding in these pa-tients is dependent on a minimal invasive therapy with a low risk of rebleeding. In study III there was a clear trend to lower 30-day mortality in the TEA group despite that the TAE group was older and had slightly more comorbidities than the surgical group. The mortality rate in both groups was some-what higher than that of an aged matched control group. However, almost half of the patients were alive after 5 years, which demonstrate that most patients in this high age group return to a normal life after this life saving treatment. With TAE none of the patients demonstrated any complications in short or long term that could be related to the TAE procedure. Also by using TAE, unnecessary surgi-cal resection of the upper GI tract can be avoided. Another advantage of TAE was that most of the patients suffering from recurrent bleeding after ini-tial treatment with surgery or TAE could be effec-tively treated with TAE and thus avoiding a second surgical procedure. In the long term both TAE and surgery seem to be effective as there was no signs of late rebleeding (>30 days) in any of the groups. These results is also supported by the findings in the study of Ripoll et al (46) who also compared the outcome of TAE and surgery in the treatment of upper peptic ulcer bleeding after failed therapeutic endoscopy. They retrospectively reviewed a group of 70 patients, 31 managed with TAE and 39 with surgery. No differences were found in the incidence of recurrent bleeding, need for additional surgery
or death, despite that the TAE patients were older and had more comorbidities.
The accepted procedure in TAE for peptic ulcer bleeding is selective embolization of at least one vessel, chosen by findings of contrast media ex-travasation, aneurysm formation at angiography or endoscopic findings before angiography. The LGA is chosen as the target vessel for gastric bleed-ing and the GDA and its branches are chosen for duodenal bleeding. Contrast media extravasation is the only direct angiographic criteria to diagnose active bleeding or define the bleeding site. Upper peptic ulcer bleeding is considered to be of arterial origin and is intermittent in nature (64, 65). Com-plex arterial anatomy particular in the bulb and duodenal region in combination with frequently intermittent bleeding bring about difficulties to choose the exact area/site for embolization. In this situation the entire GDA or LGA is recommended to be “blindly” embolized in cases with endoscopic detected duodenal or gastric bleeding (66-68).
The marking technique (study II) with a metallic clip can be used to identify the exact position of the bleeding ulcer even if there is no contrast media ex-travasation. This technique enhances the possibil-ity to choose the right target vessel and to embolize the actually bleeding artery that will most likely reduce the risk of rebleeding. This is especially im-portant when the bleeding artery arises separately from proper hepatic artery i.e. supra-duodenal ar-tery with no connection to GDA and when the ar-tery is in connection with SMA (69). In these cases a “blind” embolization of entire GDA will not be sufficient.
TAE in patients with PPH is safe and have no ma-jor long-term side effect as shown in study IV. No negative effect on menstrual cycle was demonstrat-ed. Four patients had a total of seven pregnancies with normal conception delay, and all delivered healthy infants by cesarean section with no recur-rence of PPH.
No large prospective studies concerning PPH em-bolization are reported in the medical literature. However, in three case series, a total of 38 patients with persistent PPH were embolized with a success rate of 90–95% (56, 70, 71). Successful pregnancies

34
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
have also been reported in other studies in women who had undergone embolization for PPH (57-60). There has been a case report of amenorrhoea fol-lowing embolization for PPH, secondary to necro-sis of the uterine wall and obliteration of the cavity (72).
Cesarean section delivery was high represented in this study. Thirteen of 20 patients had cesarean section and 6 of these had a clear contrast media extravasation indicating a laceration of the uter-ine artery. Four of these, who were primarily em-bolized with only gelatin sponge rebled and the pseudoaneurysm like lesions on the angiograms in-dicated that the cause might have been the surgical trauma. In order to achieve hemostasis they had to be reembolized with coils proximal to the bleeding site. The other 2 patients with clear contrast media extravasation were primarily embolized with coils near the bleeding site, in addition to gelatin sponge bilaterally, to obtain hemostasis. The combina-tion of surgical trauma together with atony of the uterus might be the explanation for the develop-ment of the massive bleeding in these cases. It also demonstrates that gelatin sponge alone as embolic agent might not be sufficient. The hemostasis was only temporary and when the blood pressure and volume raised the gelatin sponge might have been “washed out” causing the bleeding to start again, demonstrating the necessity of use coils in these sit-uations. It is also important to embolize the contra lateral side with gelatin sponge to prevent collateral “feeding” of the bleeding site and to embolize un-til complete circulatory arrest is obtained on both sides in order to minimize the risk of re-bleeding. Extravasation of contrast media seems less com-mon after vaginal delivery and the bleeding is more diffuse and embolization with only gelatin sponge was found to be sufficient in these cases.
The critical condition of the patients with ongo-ing massive PPH often makes the anesthesiologists and the obstetrician reluctant to move the patient outside of the intensive care unit or operating room. However, the risks of transfer have to be weighed against the benefits of embolization in the equipped angiography suite, as the success of the procedure relies on the quality of the fluoroscopy and x-ray images. In order to make the transportation to the angiosuite safer and to gain time medical anti shock trousers (MAST) can be used (73). After in-
sertion of urine catheter the MAST can be applied. The MAST stops the bleeding below renal arteries. In most cases inflation to 25-35 mmHg (millime-ter of mercury) is sufficient. The pressure can be maintained for 4-8 hours. The use of MAST gain time and will enable for the interventionist and the staff to arrive and prepare to treat the patient. The anesthesiologist can concentrate on replacement of blood loss and coagulation disorder and to stabi-lize patient before transfer. The leg compartments of the MAST can remain inflated during the em-bolization procedure and allow access to the femo-ral artery. The advantages of uterine embolization over surgical intervention include the benefit of preserving fertility, the ability to verify the success of procedure with angiography and embolization of collateral vessels and other sources of bleeding such as ovarian arteries, vaginal, cervical branches and rarely inferior epigastric artery (described in study IV).
The radiation doses to the ovaries in study IV exceeded greatly those used in most routine diag-nostic studies (74, 75). Despite the relatively high radiation dose there were no reports of radiation induced skin reactions or children borne with dam-ages or malformations. It is still very important to take every measure to keep the radiation dose as low as possibly to the ovaries. However, to stop the life threatening bleeding in a safe way is the most important task in this situation.
In order to achieve effective results with TAE, it is important with a close multidisciplinary collabo-ration. Concerns have been raised that failed at-tempts at radiological intervention may affect the final outcome by delaying definite surgical therapy (29). Therefore, it is crucial to have an on call sys-tem for interventional radiologist so the TAE pro-cedure can be done quick and effectively at any time during the day and night without unnecessary delay. It is also important to have an equipped an-giosuite at or close to the operation ward, giving the option to perform endoscopy, angiography and TAE or to convert to open surgery, if needed. This setting also allows the anesthesiologist to have a complete intensive care monitoring of the critical-ill patient during the procedures. If these require-ments are fulfilled, TAE can be accepted as an al-ternative to surgery.

35
Conclusion
Conclusion
The use of TAE is a safe and effective method to control severe upper GI-bleeding as well as severe PPH with small risk of complications. TAE in upper GI-bleeding has a lower 30-day mortality rate compared to surgery. Marking the bleeding ulcer with a metallic clip can enhance the safety and effectiveness of TAE. TAE in PPH does not seem to have any major negative effect on menstrual cycle or fertility. The results in this thesis strongly argue for increased use of TAE in upper GI bleeding after therapeutic endoscopy failure and in PPH after conservative obstetrical treat-ment failure as an alternative to surgery.

36
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
Summary in SwedishDetta arbete handlar om kateterburen terapi vid svåra livshotande blödningar. Två typer av blöd-ningar ingår i detta arbete 1: blödande magsår och 2: svåra förlossningsblödningar.
Med interventionell radiologi menas terapi som styrs av röntgengenomlysning och röntgenbilder (kärlröntgen). En kateter förs in i ett kärl över en metalltråd (ledare) och genom katetern injiceras röntgenkontrastmedel samtidigt som röntgenbil-der tas. Man får då en bild av blodkärlen och kan analysera formen av kärlen och identifiera eventu-ell pågående blödning. Genom katetern kan man applicera material (emboliseringsmaterial) som antingen permanent eller tillfälligt stoppar blod-flödet (embolisering).
Förstahandsmetod för diagnostik och behand-ling av blödande magsår är endoskopi (gastro-skopi). De allra flesta blödande magsår slutar att blöda spontant eller efter endoskopisk behandling (ca 70-80%). Dock reblöder 10-30% efter endosko-pisk behandling och då krävs antingen operation eller kateterburen embolisering. Det är ofta äldre patienter med andra samtidiga sjukdomar som drabbas av blödande magsår. För dessa patienter är akut operation påfrestande med hög dödlighet som följd.
Efter genomgången normal vaginal förlossning eller efter kejsarsnitt kan det uppstå svåra blöd-ningar. De allra flesta blödningar kan stoppas med traditionell medikamentell behandling, mekaniska metoder och i sista hand operation. I svåra fall kan man bli tvingad att ta bort livmodern. Som ett al-ternativ till detta kan kateterburen embolisering användas.
Avsikten med denna avhandling var att studera resultaten och att förbättra teknik och logistik vid kateterburen behandling vid dessa två tillstånd. Jämföra det kliniska utfallet och dödligheten hos patienter behandlade för blödande magsår anting-en med kirurgi eller embolisering. Utveckla en me-tod att märka ett blödande magsår vid endoskopi med ett ”metallclips” i syfte att underlätta embo-liseringen vid kärlröntgen. Utvärdera inverkan på menstruationscykeln och fruktsamheten hos pa-tienter behandlade med embolisering för svår for-lossningsblödning.
Studie I avsåg att beskriva tekniken, det kliniska utfallet samt den terapeutiska nyttan med embo-lisering använd vid blödande magsår. Arton pa-tienter behandlades, 13 efter misslyckad endosko-pisk behandling och 5 med fortsatt blödning efter operation för blödande magsår. Det gick att utföra embolisering på alla patienter. Det gick att stoppa blödningen med embolisering hos 17 av 18 patienter, 2 krävde 2 emboliseringstillfällen, en krävde akut operation efter misslyckad embolisering. Resulta-tet indikerade att emboliseringsmetoden är en ef-fektiv metod som alternativ till kirurgi.
Studie 2 avsåg att utveckla en teknik att märka ett blödande magsår vid gastroskopi för att underlätta katetriseringen av rätt kärl vid kateterburen embo-lisering. Det är vanligt att man vid kärlröntgen på en patient med blödande magsår inte ser någon pågående blödning just vid bildtagningstillfället. Man kan då med ledning av gastroskopifyndet ut-föra en ”blind” embolisering av ett kärl som man tror ligger i närheten av det blödande magsåret. Om man märker såret med ett ”metallclips” som kläms fast i kanten av det blödande magsåret vid gastroskopi kan man se dess position vid röntgen och utföra emboliseringen med ledning av detta clips. Resultatet visade att man med detta clips kan välja rätt ”målkärl” med större precision än vid ”blind” embolisering.

37
Summary in Swedish
Studie 3 avsåg att jämföra det kliniska utfallet samt jämföra dödligheten hos patienter som antingen är behandlade med kirurgi eller med kateterburen embolisering för blödande magsår. Under en åt-taårs period diagnostiserades 658 patienter med blödande magsår och 567 (86% ) av dessa slutade blöda spontant eller efter endoskopisk behandling. Nittioen patienter (14%) slutade ej att blöda efter endoskopisk behandling och av dessa behandlades 40 med kateterburen embolisering och 51 med ki-rurgi. Vid jämförelse av dessa två grupper visade resultatet att i gruppen som behandlades med ki-rurgi var 30-dagars dödligheten 14% (7 patienter) mot bara 3% (1 patient) i gruppen som behandlades med embolisering trots att de i emboliseringsgrup-pen var äldre (76 år median mot 71) och något sju-kare. Detta indikerade att emboliseringstekniken var lika effektiv men mer skonsam mot patienten än kirurgi.
Studie 4 var en retrospektiv studie av 20 patienter som genomgått embolisering pga. svår förloss-ningsblödning och som avsåg att utvärdera före-komsten av tidiga och sena komplikationer samt påverkan på menstruationscykeln och fertiliteten. Medeluppföljningstiden var 8,2 år (varierade mel-lan 1,0 - 12,1 år). Resultatet visade att inga tidiga eller sena betydelsefulla komplikationer förekom. Vare sig menstruationscykeln eller fertiliteten på-verkades negativt i den undersökta gruppen em-boliserade kvinnor. Vid embolisering p.g.a förloss-ningsblödning efter kejsarsnitt kunde blödnings-orsaken i åtminstone 6 fall härledas till det kirur-giska traumat
Emboliseringstekniken var effektiv, säker och skonsam både vad gäller behandling av blödande magsår och behandling av svår förlossningsblöd-ning och bör föredras som 1:a metod före kirurgi. Genom att märka det blödande magsåret med me-tallclips kan effektiviteten förbättras med minskad risk för reblödning.
38
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
39
Acknowledgements
Acknowledgements
I wish to express my sincere gratitude to all colleagues who have supported me to complete this thesis and especially to:
Rickard Nyman, my tutor and friend for his inspiring enthusiasm and for his sup-port and encouragement.
Sven Gustavsson my co-tutor for valuable support.
My co-authors Mikael Ljungdahl, Magnus Sundbom, Ajlana Lutvica-Mulic and Lars Jangland, for contributing with your expertise and good advice.
My fellow workers for many years, Lars Strindberg, Länssjukhuset, Gävle and Ann-Marie Löfberg, Akademiska sjukhuset, Uppsala, who invited me to work with interventional radiology at the beginning.
Bengt André at Länssjukhuset, Gävle, who initiated the work with embolization in obstetrical bleedings 1993.
My colleagues Hans Raland, Hampus Eklöf, Mats-Ola Eriksson and Per Gerwins for friendship and support.
Håkan Pettersson and Nora Velastegui for outstanding assistance creating images and layout for this thesis.
All the skilful staff in the angiography department.

40
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
41
References
References
1. Haschek E, Lindenthal OT.: A contribution to the practical use of the photography ac-cording to Röntgen. Wien. Klin. Wschr. 1896; 9:63.
2. Seldinger S.: Catheter replacement of the needle in percutaneous arteriography: a new technique. Acta Radiol 1953; 139:3681.
3. Silvestre ME, Abecasis F, Veiga-Pires JA.: Pio-neers in angiography. A leaf out of the history of angiography. Elseviers Science Publishers. 1987.
4. Dotter CT.: Transluminal treatment of arte-riosclerotic obstruction: description of a new technique and a preliminary report of its ap-plication. Circulation 1964; 30:654-670.
5. Bakal CW.: Vascular and Interventional Radi-ology. Principles and practice. Thieme Medi-cal Publishers 2002.
6. Gruentzig A.: Percutane rekanalisation chro-nischer arterieller Veschlusse mit einem neuen Dilatationskatheter. Deutsche med Wochen-schrift 1974; 290:597-603.
7. Bollinger A, Schlumpf M.: Andreas Gru-entzig’s balloon catheter for angioplasty of peripheral arteries (PTA) is 25 years old. International Journal of Cardiology, 2004; Volume 94, Issue 3, Pages 307-316 Vasa. 1999 Feb;28(1):58-64.
8. Rosch J.: Selective arterial embolization a new method for control of acute gastrointestinal bleeding. Radiology 1972; 102:303-306.
9. Brown BJ, Heaston DK, Poulson AM, et al.: Uncontrollable post partum bleeding: a new approach to hemostasis through angiographic arterial embolisation. Obstet Gynecol 1979; 153:155-157.
10. Baum S, Athanasoulis CA, Waltman AC, et al.: Gastriontestinal hemorrhage: angiograph-ic diagnosis and control. Adv Surg 1973; 7:149-198.
11. Van Allen RJ, Pentecost MJ.: Transcatheter control of hemorrage in cancer patient. Semin Intervent Radiol 1992; 9:38-44.
12. Hentati N, Fournier HD, Papon X, et al.: Ar-terial supply of the duodenal bulb: an anato-moclinical study. Surg Radiol Anat. 1999; 21(3):159-164.
13. Bianchi HF, Albanese EF.: The Supra-duode-nal artery. Surg Radiol Anat 1989; 11:37-40.
14. Song SY, Chung JW, Kwon JW, et al.: Col-lateral pathways in patients with celiac axis stenosis: angiographic-spiral CT correlation. Radiographics. 2002; 22(4):881-893.
15. Pelage JP, Le Dref O, Soyer P, et al.: Arterial anatomy of the female genital tract: variations and relevance to transcatheter embolization of the uterus. AJR Am J Roentgenol. 1999: 172(4):989-994.
16. Worthington-Kirsch RL.: Anatomy of the Uterine Artery. AJR 2000; 174:258.
17. Guyton AC, Crowell JW.: Dynamics of the heart in shock. Fed. Proc 1961; 20:51.
18. Chien S.: Role of the sympathetic nervous sys-tem in hemorrhage. Physiol. Rev.1967; 47:214.
19. Hixson LJ, Kelley CL, Jones WN, et al.: Current trends in the pharmacotherapy for peptic ulcer disease. Arch Intern Med. 1992; 152(4):726-732.
20. Graham DY, Lew GM, Klein PD, et al.: Effect of treatment of Helicobacter pylori infection on the long-term recurrence of gastric or duo-denal ulcer. A randomized, controlled study. Ann Intern Med. 1992; 116(9):705-708.
21. Vakil N, Fennery MB.: Cost-effectiveness of treatment regimens for the eradication of He-licobacter pylori in duodenal ulcer. Am J Gas-troenterol. 1996; 91(2):239-245.
22. Hopkins RJ, Giraldi LS, Turney EA.: Rela-tionship between Helicobacter pylori eradica-tion and reduced duodenal and gastric ulcer recurrence: a review. Gastroenterology. 1996; 110(4):1244-1252.
23. Aabakken L.: Nonvariceal upper gastroin-testinal bleeding. Endoscopy 2005; 37(3):195-200.
42
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
24. Gustavsson S, Kelly KA, Melton LJ 3rd, et al.: Trends in peptic ulcer surgery. A population-based study in Rochester, Minnesota, 1956-1985. Gastroenterology. 1988; 94(3):688-694.
25. Higham J, Kang JY, Majeed A.: Recent trends in admissions and mortality due to peptic ul-cer in England increasing frequency of hae-morrhage among older subjects. Gut 2002; 50:460–464.
26. Andersen IB, Bonnevie O, Jorgensen T, et al.: Time trends for peptic ulcer disease in Den-mark, 1981–1993. Analysis of hospitalization register and mortality data. Scand J Gastro-enterol 1998; 33:260–266.
27. Walt R, Katschinski B, Logan R, et al.: Ris-ing frequency of ulcer perforation in elderly people in the United Kingdom. Lancet 1986; 1:489–492.
28. Coggon D, Lambert P, Langman MJ.: 20 years of hospital admissions for peptic ulcer in Eng-land and Wales. Lancet 1981; 1:1302–1304.
29. Schwesinger WH, Page CP, Sirinek KR, et al.: Operations for peptic ulcer disease: paradigm lost. J Gastrointest Surg. 2001; 5(4):438-443.
30. Paimela H, Paimela L, Myllykangas-Luosu-järvi R, et al.: Current features of peptic ul-cer disease in Finland: incidence of surgery, hospital admissions and mortality for the dis-ease during the past twenty-five years. Scand J Gastroenterol. 2002; 37(4):399-403.
31. Gustavsson S, Nyren O.: Time trends in pep-tic ulcer surgery, 1956 to 1986. A nation-wide survey in Sweden. Ann Surg. 1989; 210(6):704-709.
32. Bjorkman DJ, Zaman A, Fennerty MB, et al.: Urgent vs. elective endoscopy for acute non-variceal upper GI- bleeding: an effectiveness study. Gastrointest Endosc 2004; 60:1-8.
33. Walsh RM, Anain P, Geisinger M, et al.: Role of angiography and embolization for massive gastroduodenal hemorrhage. J Gastrointest Surg. 1999; 3(1):61-65; discussion 66.
34. National Institutes of Health Consensus Con-ference. Therapeutic endoscopy and bleeding ulcers. JAMA 1989; 262:1369-1372.
35. Boonpongmanee S, Fleischer DE, Pezzullo JC, et al.: The frequency of peptic ulcer as a cause of upper-GI bleeding is exaggerated. Gastrointestinal Endosc 2004; 59:788-794.
36. Church NI, Palmer KR.: Diagnostic and ther-apeutic endoscopy. Curr Opin Gastroenterol. 1999; 15(6):504.
37. Lang EV, Picus D, Marx MV, et al.: Massive arterial hemorrhage from the stomach and lower esophagus: impact of embolotherapy on survival. Radiology 1990; 177: 249–252.
38. Lau JYW, Sung JJY, Lam YH, et al.: Endo-scopic retreatment compared with surgery in patients with recurrent bleeding after initial endoscopic control of bleeding ulcers. N Engl J Med 1999; 340:751-756.
39. Kim B, Wright HK, Bordan D, et al.: Risks of surgery for upper gastrointestinal haem-orrhage: 1972 versus 1982. Am J Surg 1985; 149:474-476.
40. Schenker MP, Duszak R, JR, Soulen MC, et al.: Upper Gastrointestinal Hemorrhage and Transcatheter Embolotherapy: Clinical and Technical Factors Impacting Success and Sur-vival. Journal of Vascular and Interventional Radiology 2001; 12:1263-1271.
41. Rockall TA, Logan RFA, Devlin HB, et al.: Incidence of and mortality from acute upper gastrointestinal haemorrhage in the United Kingdom. Steering Committee and mem-bers of the National Audit of Acute Upper Gastrointestinal Haemorrhage. BMJ. 1995; 22;311(6999):222-226.
42. Branicki FJ, Coleman SY, Fok PJ, et al.: Bleeding peptic ulcer: a prospective evalua-tion of risk factors for rebleeding and mortal-ity. World J Surg 1990; 14:262-270.
43. Aina R, Oliva VR, Therasse E, et al.: Arte-rial embolotherapy for upper gastrointestinal hemorrhage: outcome assessment. J Vasc In-terv Radiol 2001; 12(2):195-200.
44. Rafique MZ, Ul Hac T, Ud Din GN, et al.: Transcatheter embolization of acute non-variceal gastrointestinal hemorrhage. J Coll Physicians Surg Pak 2005; 15(2):81-84.
43
References
45. Okazaki M, Higashihara H, Ono H, et al.: Embolotherapy of massive duodenal hemor-rhage. Gastrointest Radiol 1992; 17:319-323.
46. Ripoll C, Banares R, Beceiro I, et al.: Com-parison of transcatheter arterial embolization and surgery for treatment of bleeding peptic ulcer after endoscopic treatment failure. Jour-nal of Vascular and Interventional Radiology 2004; 15:447-450.
47. The world health report 2005 - make every mother and child count. World Health Organ-isation 2005.
48. Department of health, The Sixth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom, “Why Mothers Die 2000-2002”; November 2004, RCOG.
49. Combs CA, Murphy EL, Laros RK Jr.: Fac-tors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol. 1991; 77:69-76.
50. Combs CA, Murphy EL, Laros RK Jr.: Fac-tors associated with hemorrhage in cesarean deliveries. Obstet Gynecol. 1991; 77:77-82.
51. King PA, Duthie SJ, Dong ZG, Ma HK.: Sec-ondary postpartum haemorrhage. Aust N Z J Obstet Gynaecol. 1989; 29:394-398.
52. Kelestimur F.: Sheehan’s syndrome. Pituitary 2003; 6(4):181-188.
53. Pelage JP, Laissy JP.: Management of life-threatening postpartum hemorrhage: indica-tions and technique of arterial embolisation. J Radiol. 2006; 87(5):533-540.
54. Pelage JP, Le Dref O, Mateo J, et al.: Life-threatening primary postpartum hemorrhage: treatment with emergency selective arterial embolization. Radiology 1998; 208(2):359-362.
55. Pelage JP, Le Dref O, Jacob D.: Selective arte-rial embolization of the uterine arteries in the management of intractable post-partum hem-orrhage. Acta Obstet Gynecol Scand. 1999; 78(8):698-703.
56. Vedantham S, Goodwin SC, McLucas B, et al.: Uterine artery embilization: an underused method of controlling pelvic haemorrage. Am J Obstet Gunecol 1997; 176:938-948.
57. Ornan D, White R, Pollak J, et al.: Pelvic em-bolisation for intractable postpartum hemor-rhage: Long-term follow-up and implications for fertility. Obstet Gynecol. 2003; 102(5 Pt 1):904-910.
58. Descargues G, Mauger Tinlot F, Douvrin F, et al.: Menses, fertility and pregnancy after arterial embolisation for the control of post partum haemorrhage. Hum Reprod. 2004; 9(2):339-343.
59. Stancato-Pasik A, Mitty HA, Richard HM, et al.: Obstetric embolotherapy: effect on menses and pregnancy. Radiology 1997; 204:791-793.
60. Salomon LJ, deTayrac R, Castaigne-Meary V, et al.: Fertility and pregnancy outcome fol-lowing pelvic arterial embolization for severe post-partum haemorrhage. A cohort study. Hum Reprod. 2003; 18(4):849-852.
61. Nickel J, Sachs W, Andresen R.: Selective embolisation of posttraumatic intractable epistaxis. Rontgenpraxis 2003; 55(2):72-77.
62. Sun L, Guan YS, Wu H, et al.: Post-traumatic hepatic artery pseudo-aneurysm combined with subphrenic liver abscess treated with embolization. World J Gastroenterol. 2006; 12(17):2798-2799.
63. Iwama Y, Sugimoto K, Zamora CA, et al.: Transcatheter embolization of splenic artery pseudo-aneurysm rupturing into colon after post-operative pancreatitis. Cardiovasc Inter-vent Radiol. 2006; 29(1):133-136.
64. Toyoda H, Nakano S, Takeda I, et al.: Tran-scatheter arterial embolization for massive bleeding from duodenal ulcers not controlled by endoscopic hemostasis. Endoscopy 1995; 27(4):304-307.
65. De Wispelaere JF, De Ronde T, Trigaux JP, et al.: Duodenal ulcer haemorrhage treated by embolization: results in 28 patients. Acta Gas-troenterol Belg. 2002; 65(1):6-11.
66. Defreyne L, Vanlangenhove P, De vos M, et al.: Embolization as a first approach with en-doscopically unmanageable acute nonvariceal gastrointestinal hemorrage. Radiology 2001; 218:739-748.
44
Transcatheter Arterial Embolization in the Management of Life Threatening Bleeding
67. Lang EV, Picus D, Marx MV, et al.: Mas-sive upper gastrointestinal hemorrhage with normal findings on arteriography: value of prophylactic embolization of the left gastric artery. AJR Am J Roentgenol 1992; 158:547-549.
68. Morris DC, Nichols DM, Connell DG, et al.: Embolization of the left gastric artery in the absence of angiographic extravasation. Car-diovasc Intervent Radiol 1986; 9:195-198.
69. Eriksson L-G, Sundbom M, Gustavsson S, et al: Endoscopic marking with a metallic clip facilitates transcatheter arterial embolization in upper peptic ulcer bleeding. J Vasc Interv Radiol. 2006; 17(6):959-964.
70. Corr P.: Arterial embolisation for haemor-rhage in the obstetric patient. Best Practice and Research. Clinical Obstetrics and Gy-naecology 2001; 15:557–561.
71. Deux J-F, Bazot M, Le Blanche AF, et al.: Is selective embolisation of uterine arteries a safe alternative to hysterectomy? American Journal of Roentgenology 2001; 177:145–149.
72. Chitrit Y, Zafy S, Pelage JP, et al.: Amenor-rhea due to partial uterine necrosis after uter-ine artery embolization for control of refrac-tory postpartum hemorrhage. Eur J Obstet Gynecol Reprod Biol. 2006; 127(1):140-142.
73. Andrae B, Eriksson L-G, Skoog G.: Anti-shock trousers (MAST) and transcatheter embolization in the management of massive obstetrics hemorrhage. A report of two cases. Acta Obstet Gynecol Scand. 1999; 78(8):740-741.
74. Andrews RT, Brown PH.: Uterine arterial em-bolization: factors influencing patient radia-tion exposure. Radiology 2000; 217:713-722.
75. Valentin J.: Pregnancy and Medical Radia-tion. Annals of the ICRP. 2000; 30,1:1-39.





























