Embed Size (px)
Citation preview

tPA In Acute Ischemic Stroke: Con
Reuben StrayerR4McGill Emergency Medicine
For Neurological Emergencies / RVH DayMarch 29, 2006
IntroThe use of tPA in acute ischemic stroke is controversial
CAEP: "Further evidence is necessary to support the widespread application of stroke thrombolysis outside research settings."
ACEP: "Further studies are needed to define more clearly those patients most likely to benefit from fibrinolytic therapy in acute ischemic stroke."
SAEM: "It is not yet clear whether the treatment risk is outweighed by the likely therapeutic benefit.""Currently insufficient data exist to mandate thrombolytic therapy as the standard of care for acute
ischemic stroke for all patients across all medical treatment settings."
AAEM: "Objective evidence regarding the efficacy, safety, and applicability of tPA for acute ischemic stroke is insufficient to warrant its classification as standard of care."
References 1-4
2

Intro
Thrombolysis for stroke versus thrombolysis for MI
3
Randomized Data
It is impossible to prove a therapy doesn’t work
Predicted arrangement of multiple trials:a bell-shaped curve
6:1
4
Randomized Data
ECASS-I 1995
MAST-I 1995
ASK 1996
MAST-E 1996
ECASS-II 1998
ATLANTIS 1999
Clark, JAMA 1999
Hacke, Lancet 1998
MAST-E Study Group, NEJM 1996
Donnan, JAMA 1996
MAST-I Study Group, Lancet 1995
Hacke, JAMA 2005
5
Randomized DataExplanations for discrepant results in NINDS
tPA vs. streptokinase
Lower tPA does in NINDS vs. ECASS
The 3 hour cutoff
Chance
Hoffman, EMAC Essays 1996
6

7

8
NINDS“2 Trials”
NINDS Investigators, NEJM 1995
3 month mRS 0-1: tPA 39%, placebo 26%
Symptomatic ICH: tPA 6.4%, placebo .6%
9

NINDSNNT 8
NNH 17NNK 34
NINDS Investigators, NEJM 1995
10

NINDS
49% in the very early group
Marler, Neurology 2000
Failure of randomization in the 91-180 minute group
11
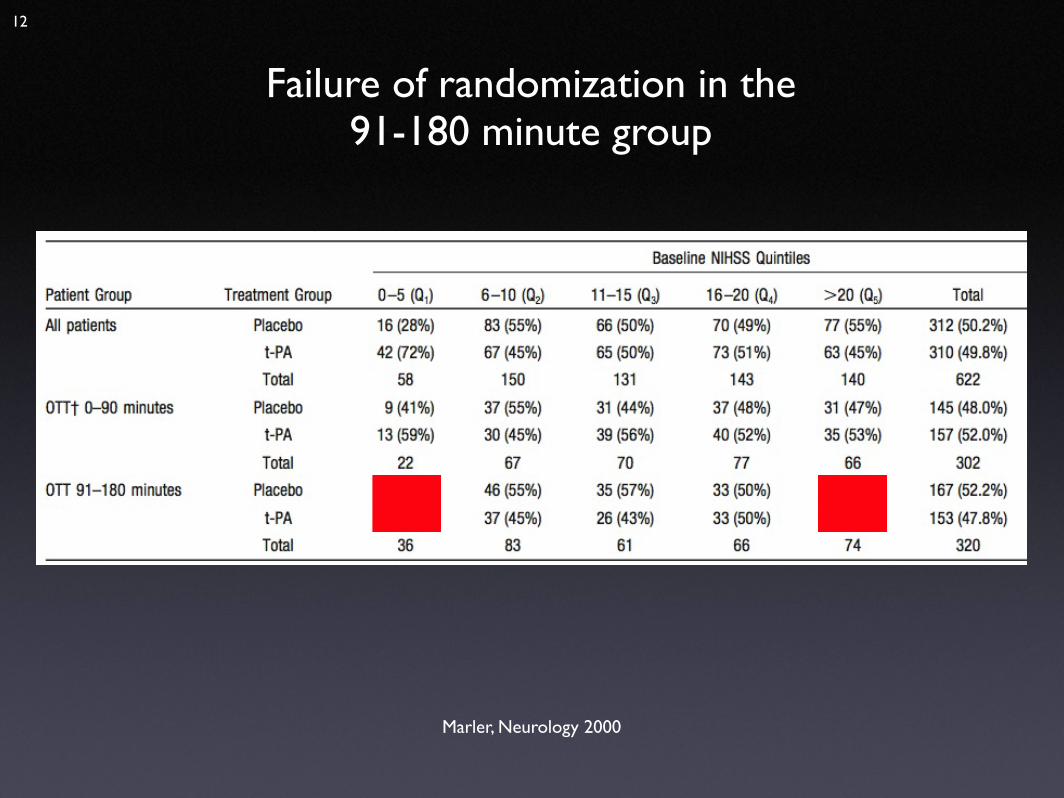
Marler, Neurology 2000
Failure of randomization in the 91-180 minute group
12
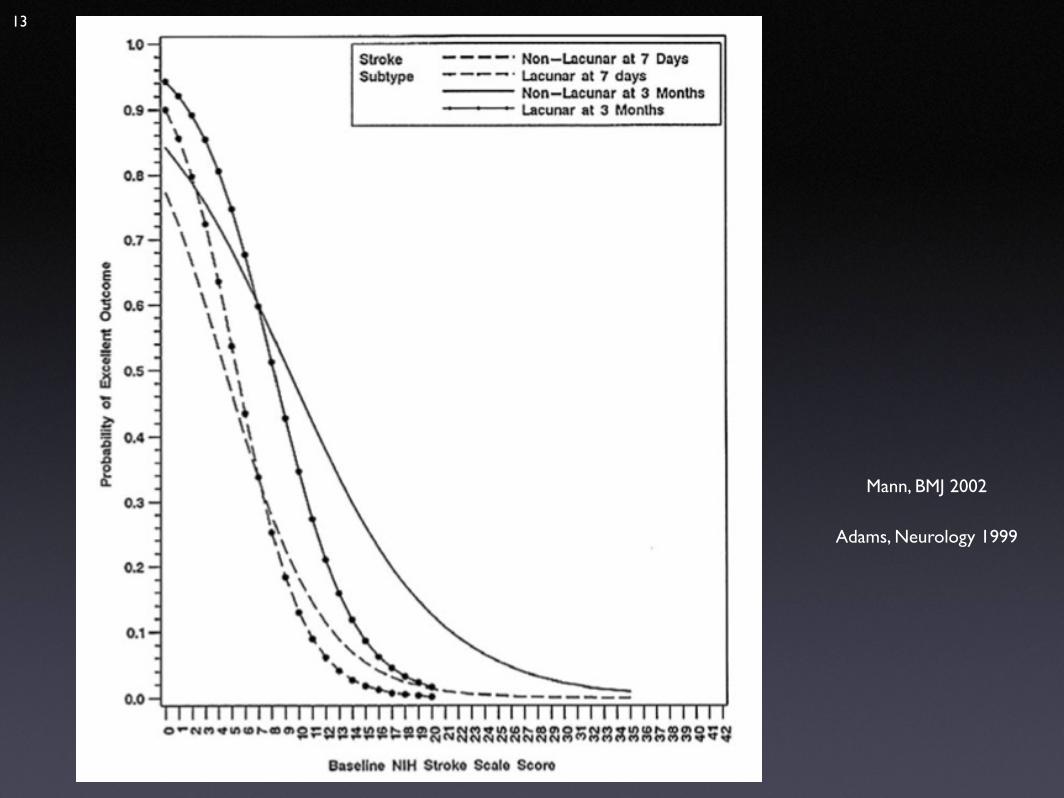
Adams, Neurology 1999
Mann, BMJ 2002
13
NINDS
The two part trial
No difference at 24h:A face validity question
14
Misdiagnosis
Magnitude of benefit
Libman, Arch Neurol. 1995 Kahn, J Emerg Med 2005 Bateman, Stroke 2006
15
Reanalyses
Cochrane Review 2003
Pooled Analysis of NINDS, ECASS, and ATLANTIS
Wardlaw, Cochrane Database 2003
Wardlaw, West J Med 2002
Hacke, Lancet 2004
Lenzer, Healthy Skepticism 2005
16

Usage Studies
Saposnik, JAMA 2004: Prospective UWO registry 1999-2003. Rate of cerebral hemorrhage at 36 hours was 10.4%.
Hill, CMAJ 2005: Selective CASES registry 1999-2001: Excellent clinical outcome of treated patients 31.8%, closer to NINDS placebo, though reported as 37%, which is closer to NINDS treatment arm.
Katzan, JAMA 2000, The Cleveland Cohort. Inclusive review of all patients with stroke in the city except for the VA over a one year period. Treatment rate was 1.8%. 15.7% symptomatic ICH, 50% protocol violations. In-hospital mortality 15.7% vs. 5.1%.
Albers, JAMA 2000, STARS cohort. Selective review of 57 expert-based american centers that participated in the ATLANTIS study. 389 patients, 3.3% symptomatic hemorrhage rate with a high proportion of positive outcomes.
Heuschmann, JAMA 2004, German Stroke Registry 57,000 strokes from 2000-2003. tPA treatment rate 3%. Inhospital mortality 10% tPA vs. 4.6% no tPA.
Tanne, Neurology 1999, Henry Ford Review: 13/16 hospitals identified as high-volume specialty centers from select cities, most of which used a stroke team. 136 patients, 6% symptomatic ICH, but 11% where there were protocol violations, which occurred 30% of the time
in these specialty centers.
Szoeke, MJA 2003, Royal Melbourne Hospital, all diagnosed ischemic stroke patients over 3 years. Treatment rate 3.2%, protocol violation rate with dedicated stoke unit with stroke neurologist, stroke fellow, and stroke RN was 23%.
Bravata, Arch Int Med 2002, The Connecticut Cohort. An inclusive review of all patients in the state over 2.5 years. Treatment rate was .6%. In-hospital mortality was 25% (vs. NINDS 13%).
Bateman, Stroke 2006: In this inclusive database the thrombolysis cohort had a higher in-hospital mortality rate compared with the nonthrombolysis patients (11.4% versus 6.8%).
17
How it happened
Big Pharma & the media frenzy
Expert effect
Bandwagon bias
Desire to do something
Trotter, West J Med 2002 Woods 2006
18

Conclusions
There is one randomized trial that demonstrates a modest benefit for IV tPA in acute ischemic stroke.
This trial is at odds with almost all of the other randomized data on the subject, and suffers from a
number of internal and external validity problems that can explain its discrepant results.
19
Conclusions
If thrombolysis is considered in the most conceivably generous light, it benefits an absurdly small number of
stroke patients, and the present expenditure of resources on this agent that could be diverted to therapies of unquestionably greater value–such as
stroke units–is irresponsible.
Donnan, Med J Aust 2003
20

Conclusions
The logical conclusion to draw from the available data is that tPA does not work; the optimistic view is that tPA might work for a yet-unidentified subset of patients. It is
clear that if the trial results pattern were switched (such that NINDS were the only trial that didn't show a benefit), NINDS would have been ignored, and it is also
clear that the focus on tPA as a therapy for stroke is driven by forces other than the data.
21

Conclusions
A therapy as dangerous as tPA must conclusively demonstrate benefit before it can be considered for routine use. That tPA has been adopted in some settings as standard of care, and that it is being touted as a cure for stroke to a
public unversed in its limitations and consequences, and that an entire "brain attack" industry and regional stroke system
is being implemented before more convincing data is available is at best uninformed and at worst shameful. At this
time, the use of any intravenous thrombolytic should be confined to rigorously controlled settings where it can be administered as part of a research effort to determine in
which patients, if any, the benefit outweighs the risk.
22
References
1 http://www.caep.ca/002.policies/002-01.guidelines/thrombolytic.htm
2 http://www.acep.org/webportal/PracticeResources/PolicyStatements/pracmgt/UseofIntravenoustPAforAcuteStroke.htm
3 http://saem.org/publicat/optcare.htm
4 http://www.aaem.org/positionstatements/thrombolytictherapy.shtml
5 Hacke, W., et al, JAMA 274(13):1017, October 4, 1995. Intravenous Thrombolysis With Recombinant Tissue Plasminogen Activator For Acute Hemispheric Stroke, The European Cooperative Acute Stroke Study (ECASS).
6 Multicenter Acute Stroke Trial-Italy (MAST-I) Study Group. Randomized controlled trial of streptokinase, aspirin, and combination of both in treatment of acute ischemic stroke. Lancet 1995;346:1509-1514.
7 Donnan GA. Streptokinase for acute ischemic stroke with relationship to time of administration: Australian Streptokinase (ASK) Trial Study Group. JAMA. 1996 Sep 25;276(12):961-6.
8 MAST-E Thrombolytic Therapy with Streptokinase in Acute Ischemic Stroke, The Multicenter Acute Stroke Trial - Europe Study Group, NEJM 335(3):145, July 18, 1996
9 Hacke W. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet. 1998 Oct 17;352(9136):1245-51.
10 Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study: a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. JAMA. 1999 Dec 1;282(21):2019-26.

References11 Hoffman, JR. Thrombolytic Therapy For Strokes, Part II. Emergency Medicine and Acute Care Essays, Volume 20, Number 12 December 1996.
12 NINDS Investigators. Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995 Dec 14;333(24):1581-7.
13 Marler, J.R., et al. Early Stroke Treatment Associated With Better Outcome: The Ninds Rt-Pa Stroke Study. Neurology 55:1649, December 2000
14 Mann, J. BMJ 2002: "Rapid Responses" to Lezner, http://bmj.bmjjournals.com/cgi/eletters/324/7339/723.
15 Adams, H. P. Jr. MD. Davis, P. H. MD. Leira, E. C. MD. Chang, K.-C. MD. Bendixen, B. H. PhD, MD. Clarke, W. R. PhD. Woolson, R. F. PhD. Hansen, M. D. MS. Baseline NIH Stroke Scale score strongly predicts outcome after stroke: A report of the Trial of Org 10172 in Acute Stroke Treatment (TOAST). Neurology. 53(1):126-131, July 13, 1999
16 Libman RB, Wirkowski E, Alvir J, Rao TH.Conditions that mimic stroke in the emergency department–Implications for acute stroke trials. Arch Neurol. 1995 Nov;52(11):1119-22.
17 Kahn, J.H., et al. The Use Of Intravenous Recombinant Tissue Plasminogen Activator In Acute Ischemic Stroke. J Emerg Med 29(3):273, October 2005.
18 Bateman BT, Schumacher HC, Boden-Albala B, Berman MF, Mohr JP, Sacco RL, Pile-Spellman J. Factors associated with in-hospital mortality after administration of thrombolysis in acute ischemic stroke patients: an analysis of the nationwide inpatient sample 1999 to 2002. Stroke. 2006 Feb;37(2):440-6.
19 Wardlaw JM, del Zoppo G, Yamaguchi T, Berge E. Thrombolysis for acute ischaemic stroke. The Cochrane Database of Systematic Reviews 2003, Issue 3. Art. No.: CD000213. DOI: 10.1002/14651858.CD000213.
20 Wardlaw JM, Lindley RI, Lewis S. Thrombolysis for acute ischemic stroke: still a treatment for the few by the few. West J Med. 2002 May;176(3): 198-9.
References
21 Hacke W, Donnan G, Fieschi C, Kaste M, von Kummer R, Broderick JP, Brott T, Frankel M, Grotta JC, Haley EC Jr, Kwiatkowski T, Levine SR, Lewandowski C, Lu M, Lyden P, Marler JR, Patel S, Tilley BC, Albers G, Bluhmki E, Wilhelm M, Hamilton S; ATLANTIS Trials Investigators; ECASS Trials Investigators; NINDS rt-PA Study Group Investigators. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004 Mar 6;363(9411):768-74.
22 Lenzer, Jeanne. The new alchemy: Mixing doctors and journalists to spin gold. Healthy Skepticism International News 2005 Apr; 23: 4.
23 Tanne D, Bates VE, Verro P, Kasner SE, Binder JR, Patel SC, Mansbach HH, Daley S, Schultz LR, Karanjia PN, Scott P, Dayno JM, Vereczkey-Porter K, Benesch C, Book D, Coplin WM, Dulli D, Levine SR. Initial clinical experience with IV tissue plasminogen activator for acute ischemic stroke: a multicenter survey. The t-PA Stroke Survey Group. Neurology. 1999 Jul 22;53(2):424-7.
24 Albers GW, Bates VE, Clark WM, Bell R, Verro P, Hamilton SA.Intravenous tissue-type plasminogen activator for treatment of acute stroke: the Standard Treatment with Alteplase to Reverse Stroke (STARS) study. JAMA. 2000 Mar 1;283(9):1145-50.
25 Katzan IL, Furlan AJ, Lloyd LE, et al. Use of tissue-type plasminogen activator for acute ischemic stroke: the Cleveland area experience. JAMA 2000; 283: 1151- 1158.
26 Bravata DM, Kim N, Concato J, Krumholz HM, Brass LM. Thrombolysis for acute stroke in routine clinical practice. Arch Intern Med. 2002 Sep 23;162(17):1994-2001.
References
27 Szoeke CE, Parsons MW, Butcher KS, Baird TA, Mitchell PJ, Fox SE, Davis SM. Acute stroke thrombolysis with intravenous tissue plasminogen activator in an Australian tertiary hospital. Med J Aust. 2003 Apr 7;178(7):324-8.
28 Heuschmann PU, Kolominsky-Rabas PL, Roether J, Misselwitz B, Lowitzsch K, Heidrich J, Hermanek P, Leffmann C, Sitzer M, Biegler M, Buecker-Nott HJ, Berger K; German Stroke Registers Study Group. Predictors of in-hospital mortality in patients with acute ischemic stroke treated with thrombolytic therapy. JAMA. 2004 Oct 20;292(15):1831-8.
29 Hill MD, Buchan AM; Canadian Alteplase for Stroke Effectiveness Study (CASES) Investigators. Thrombolysis for acute ischemic stroke: results of the Canadian Alteplase for Stroke Effectiveness Study. CMAJ. 2005 May 10;172(10):1307-12.
30 Saposnik G, Young B, Silver B, Di Legge S, Webster F, Beletsky V, Jain V, Nilanont Y, Hachinski V. Lack of improvement in patients with acute stroke after treatment with thrombolytic therapy: predictors and association with outcome. JAMA. 2004 Oct 20;292(15):1839-44.
31 Trotter G. Why were the benefits of tPA exaggerated? West J Med. 2002 May;176(3):194-7.
32 Woods, Dirk. Personal communication, 2006.
33 Donnan GA, Davis SM, Levi CR. Strategies to improve outcomes after acute stroke. Med J Aust 2003; 178: 309-310.