Embed Size (px)
Citation preview

British Journal of Anaesthesia 1995; 74: 123-128
CLINICAL INVESTIGATIONS
Total i.v. anaesthesia with propofol and the laryngeal mask fororthopaedic surgery
R. A. DYER, R. L. LLEWELLYN AND M. F. M. JAMES
Summary
One hundred ASA I orthopaedic surgical patients(four randomized groups) were anaesthetized usingcontinuous propofol and intermittent fentanyl(TIVA), with controlled ventilation via a trachealtube in groups 1 and 2, and a laryngeal mask airway(LMA) in groups 3 and 4. Neuromuscular blockerswere used in groups 1 and 3 only. There were nosignificant differences between groups in totalanaesthetic requirements, as assessed by cardio-vascular variables and movement. Coughing inter-fered with surgery and made controlled ventilationdifficult to manage. In contrast, movement notassociated with coughing did not impair surgery orventilation. Patients in group 2 (tracheal tube, noneuromuscular blocker) required more interven-tions for coughing than the other groups, whilepatients in group 4 (LMA, no neuromuscularblocker) needed more boluses for movement thangroups 1 and 3. Groups 1 and 2 (tracheal tube) hadsignificantly higher heart rates and mean arterialpressures than groups 3 and 4 for varying periodsup to 5 min after insertion of the airway man-agement device. There was no correlation betweenmean arterial pressure and plasma concentrations ofcatecholamines related to insertion of either thetracheal tube or LMA. The LMA was found to be ahighly effective device for controlled ventilation inTIVA and easier to manage than the tracheal tubein the absence of neuromuscular blockers. (Br. J.Anaesth. 1995; 74: 123-128)
Key wordsAnaesthetic techniques, i.v. infusion. Anaesthetics i.v., propofol.Surgery, orthopaedic. Equipment, masks anaesthesia.
Propofol is regarded currently as the most suitableanaesthetic agent for total i.v. anaesthesia (TIVA); itallows for rapid changes in anaesthetic depth and arapid, clear-headed recovery [1]. Also, low context-sensitive half-time [2] makes it theoretically the bestavailable agent for long procedures under TIVA.Furthermore, propofol attenuates airway reflexes tothe extent that the laryngeal mask airway (LMA)may be positioned easily without neuromuscularblock [3]. Propofol may even allow for insertion of atracheal tube (TT) without neuromuscular block [4,5]. Neuromuscular blocking drugs are used widely inanaesthesia in association with controlled ventilationwhen the surgical site does not require muscularparalysis. This may increase the danger of awareness
and expose patients to risks of ventilatory failure inthe event of equipment malfunction or inadvertentdisconnection from the ventilator circuit.
It was therefore decided to evaluate the practicalityof TIVA using the LMA as an alternative airwaymanagement device to the TT in peripheral or-thopaedic surgical procedures, during controlledventilation using propofol and fentanyl. In order tostudy the effect of neuromuscular blocking agents onanaesthetic requirements and the practicality ofTIVA, both the LMA and TT were studied withand without neuromuscular block. Furthermore, acomparison was made between the LMA and TT onthe basis of the effect of neuromuscular blockers onthe feasibility of the technique. Finally, the effect ofthe different anaesthetic techniques on serum con-centrations of catecholamines was also studied.
Patients and methods
We studied ASA I patients undergoing orthopaedicsurgery. The study was approved by the Universityof Cape Town Ethics Committee and informedconsent was obtained from all patients.
Premedication comprised oral temazepam 20-30 mg, 2 h before operation. An i.v. cannula and a22-gauge arterial cannula were inserted under localanaesthesia and a 10-ml arterial blood sample wasobtained for measurement of plasma concentrationsof catecholamines. Patients were allocated randomlyto one of four groups. All groups received a standardinduction (see below), and the individual groupswere treated as described below.
Group 1 received vecuronium O.lmgkg"1, thetrachea was intubated and the lungs ventilatedmechanically throughout the procedure. Neuro-muscular block was monitored using the Relaxographand maintained at T l > 9 0 % depression, withincremental boluses of vecuronium 1 mg as required.At the end of the procedure, residual neuromuscularblock was antagonized with neostigmine and glyco-pyrronium. Intubation in group 2 was undertakenusing fentanyl and propofol alone, with no neuro-muscular block and the lungs were ventilatedmechanically. In group 3 an LMA was insertedunder propofol anaesthesia and neuromuscular
R. A. DYER, BSC(HONS), MB, CHB, FFA(SA), R. L. LLEWELLYN, MB,CHB, FFA(SA), M. F. M. JAMES, PHD, MB, CHB, FRCA, Department ofAnaesthesia, Groote Schuur Hospital and University of CapeTown, Observatory, 7925 Cape Town, Republic of South Africa.Accepted for publication: July 11, 1994.
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/2/123/452180 by guest on 02 January 2022

124 British Journal of Anaesthesia
blockers administered as in group 1. Patients ingroup 4 were treated as those in group 2 except thatthey received an LMA instead of a TT.
All subjects received glycopyrronium 0.2 mg fol-lowed by fentanyl 2 ng kg"1 2 min before induction.Induction was performed with propofol ad-ministered from a standard syringe driver (Ohmeda900) at a rate of 600 ml h"1 (10 ml min"1), until theeyelash reflex was lost and then another 2 ml wasinfused. At this point patients in groups 1 and 3received vecuronium O.lmgkg"1 and the othersubjects received an equivalent volume of saline;propofol was continued at a rate of 10 mg kg"1 h"1
for 3 min until intubation or placement of the LMAhad been performed. In groups 2 and 4 insertion ofthe airway device (TT or LMA) took place im-mediately on completion of induction of anaesthesia.In all cases the anaesthetist performing the in-tubation and conducting the remainder of theanaesthetic was blinded as to the use of neuro-muscular blockers.
In all patients anaesthesia was maintained with acontinuous infusion of propofol on a step-downregimen as follows: lOmgkg"1^1 for 15 min (in-cluding preintubation time), 8 mg kg"1 h~' for 15 minand then a target rate of 6 mg kg"1 h"1, the preciserate being determined by clinical signs of depth ofanaesthesia. These signs were as follows: purposefulor non-purposeful movement, change in arterialpressure greater than 20 % of the baseline value, orchange in heart rate greater than 20 % of baseline (ifaccompanied by a similar trend in arterial pressure),sweating or lacrimation. Alterations in anaestheticdepth were made in a stepwise manner as follows: ifthe patient was too lightly anaesthetized (see above),a bolus of propofol 0.5 mg kg"1 was administered,followed by a second bolus if needed within 5 min.After two such boluses, the infusion rate wasincreased by 2 mgkg"1 h"1. Further increases weremade in this manner until a stable state wasestablished. If the patient was too deeply anaes-thetized, as judged by a decrease in heart rate,arterial pressure, or both, of > 20 % of baseline inthe absence of other causes of hypotension, theinfusion rate was stepped down by 2 mg kg"1 h"1
until satisfactory depth was established, at 10-minintervals.
All patients received fentanyl 1 ug kg"1 repeated at30-min intervals until the end of the procedure; thelast dose was not given within 15 min of theanticipated end of the procedure. The inhaled gasmixture was oxygen in air, with an FIO J of 30 % orgreater as necessary to maintain arterial saturationgreater than 95 %. All subjects' lungs were ventilatedmechanically with a tidal volume of 7 ml kg"1 at arate necessary to maintain expired PECC>2 at 4—5 kPa.At the end of the procedure, in groups 1 and 3,neuromuscular block was antagonized and afteradequate tidal volumes were attained, the airwaymaintenance device was removed when the patientwas sufficiently wide awake to maintain an un-supported airway. In the two other groups theairway maintenance device was removed when thepatient could maintain an unsupported airway.
The cardiovascular changes during the induction
sequence were noted. Intubation conditions wereassessed in groups 1 and 2 as follows: at laryn-goscopy, the position of the vocal cords was notedand recorded on the following scale: 1 = cords fullyopen and stationary, 2 = cords partially open andstationary, 3 = cords partially open and moving and4 = cords closely opposed. In group 2, suxa-methonium 1 mg kg"1 was administered before in-tubation if the vocal cord score was 3 or 4. Afterinsertion of the TT or LMA, the insertion conditionswere assessed as follows: 1 = device easily inserted,2 = device inserted with slight resistance, 3 = deviceinserted with difficulty, or repeated attempts requiredand 4 = insertion abandoned. The response of thepatient was graded as follows: 1 = no response, 2 =slight bucking, 3 = coughing and 4 = gross bodymovements. In all four groups cardiovascular statuswas recorded every minute for 5 min after com-pletion of intubation and thereafter at 5-minintervals.
Ventilatory function was monitored by recordingpeak airway pressures, end-tidal carbon dioxidepartial pressures and airway leaks at 10-min intervals.The latter was monitored by gentle auscultation ofthe neck adjacent to the thyroid cartilage.
Anaesthetic requirements were noted by recordingthe infusion rates and total dose requirements(mg kg"1 h"1) of propofol. Baseline plasma cate-cholamines were measured from the arterial cannula5 min after insertion of the radial artery cannula.Subsequent samples were obtained after inductionand at 2 and 5 min after intubation. Concentrationswere measured by electrochemical detection afterseparation with reverse phase HPLC with dihydro-benzylamine as internal standard using a methoddescribed previously [6]. The lower limit of sen-sitivity of this method is 20 pg ml"1 for bothnoradrenaline and adrenaline and the coefficient ofvariation of the assay was 8.6 % for noradrenaline(mean standard concentration 861.5 pg ml"1) and5.0% for adrenaline (mean standard concentration1047.0 pg ml"1). At the end of the procedure, bloodsamples were obtained before extubation and at 2and 5 min after removing the TT or LMA, andcardiovascular data were recorded at the same timesas for the intubation response. During operationventilatory frequency and tidal volume were recordedat 5-min intervals and blood-gas estimations per-formed at 30-min intervals. Oxygen saturation andend-tidal Pco2 were monitored continuously. Failureof any technique at any time (e.g. inability tomaintain adequate ventilation with the LMA,unresponsive hypotension) resulted in conclusionof the study in that subject, and the use ofalternative anaesthetic techniques as indicated. Suchwithdrawal was regarded as a technical failure, butdid not result in exclusion of the patient from thestudy.
In the recovery room, cardiovascular data wererecorded at 5-min intervals for the first hour, andoxygen saturation was monitored continuously. Theincidence of nausea and vomiting in the four groupswas noted and the time taken to full recovery, asjudged by ability to remember date of birth and theday's date. At a postoperative visit within 24 h of the
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/2/123/452180 by guest on 02 January 2022
TIVA and the LMA in orthopaedics
conclusion of the study, every patient was questionedregarding recall of operative events.
Numerical data were analysed by analysis ofvariance with multiple range testing to identifysignificantly different groups. Qualitative data werecompared using chi-square analysis, and where non-parametric scoring systems were used, the Kruskal-Wallis non-parametric analysis of variance was used.Categorical data were analysed using chi-square andFisher's exact tests as appropriate. All statisticaltests were conducted using Statgraphics version 5statistical package running on an IBM-compatible386 machine under MS-DOS version 6. The nullhypothesis was rejected at P < 0.05.
125
2 were significantly greater than those in group 1,and insertion response score was higher in group 2compared with groups 1, 3 and 4. In 11 patients in
Table 3 Mean (SD) duration of anaesthesia, surgery andtourniquet time. No significant differences between groups
Group
1234
Duration ofanaesthesia(min)
87 (43)81 (34)87 (46)79 (31)
Duration ofsurgery(min)
69 (44)63 (32)72 (46)67 (33)
Tourniquet(No.)
21212319
Tourniquettime (min)
60 (40)55 (31)67 (36)61 (32)
Results
Patient characteristics are shown in table 1. Therewere no significant differences in age, sex distri-bution, weight or height. The various populationgroups presenting for surgery at Groote SchuurHospital were distributed evenly between the studygroups. The distribution of surgical procedures,(mostly lower limb orthopaedic) is shown in table 2and data pertaining to surgical, anaesthesia andtourniquet times are shown in table 3. There were nosignificant differences between groups.
An average rank analysis of laryngoscopy andintubation conditions, and intubation response areshown in table 4. The laryngoscopy scores in group
Table 1 Patient characteristics (mean (SD or range) or number)
Group
1234
Table 2
n
25252624
Age (yr)
29.1 (18-53)31.8 (19-56)29.3 (18-51)31.3 (19-65)
Surgical procedure
Operation Group 1
Sex(M/F)
17/820/521/517/7
Group 2
Weight(kg)
66.1 (9.6)69.1 (12.2)64.6 (11.0)63.9 (9.2)
Group 3
Height(cm)
167 (9.3)169 (10.7)169 (10.4)167 (9.7)
Group 4
ArthroscopyArthroscopy andligament repair
Arthroscopy andmeniscectomy
PatellectomyStabilization ofknee
High tibialosteotomy
Zimmer pin andplate
Open reductionand fixation/graft
ForearmLower limb
Arthrodesis andbone graft
ExoskeletonLower limbnailing
Sequestrectomytibia
Remove tibialplate
BunionectomyTotal
65
3
11
1
1
321
10
0
0
025
74
3
11
2
0
011
04
1
0
025
53
2
00
0
0
391
01
1
1
026
44
1
10
1
0
310
15
1
0
224
Laryngoscopyscore
18.532.5*—
Insertionconditions
49515151
Insertionresponse
4971*4043
Table 4 Average ranks of the scores for laryngoscopy andintubation conditions. *P < 0.05
Group
1234
120-i
100-
°>80-
E
£ 60-
§ 40 -
20 -
I—Int
i
1 2i3
Time
i
4(min)
i
5i
10—I 1—Pre Ind
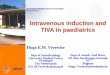
Figure 1 Mean arterial pressure (MAP) in groups 1 ( • ) , 2(O). 3 (*•) and 4 ( • ) (mean, SD). Pre = Preinduction; Ind =after induction; Int = after intubation. Significant differences(P < 0.05): * groups 1 and 2 compared with groups 3 and 4;t group 1 compared with group 4.
120-,
100-
Tc 80 -
Era 6 0 -CQ
oc 4 0 - |
20 -
Pre Ind Int 3 4Time (min)
10
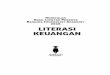
Figure 2 Heart rate (HR) in groups 1 ( • ) , 2 (O), 3 (*) and 4( • ) (mean, SD). Pre = Preinduction; Ind = after induction; Int= after intubation. Significant differences (P < 0.05): * groups1 and 2 compared with groups 3 and 4; t group 2 comparedwith groups 3 and 4.
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/2/123/452180 by guest on 02 January 2022

126 British Journal of Anaesthesia
1000-
800-
Q . 600 -
£ 400 -• a
200 -
0 J
Prel Post 2 min 5 min 2 min 5 min
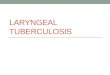
Figure 3 Noradrenaline concentrations in groups 1 ( • ) , 2 (0 j , 3 (\J), and 4 ( • ) (mean, SD). Prel =Preinduction; Post = after induction; Pre = before extubation. *P < 0.05 compared with group 1. No significantwithin-group differences.
200 - |
150 -
E
2
c91
100 -
50 -
0 - 1
Prel Post 2 min 5 min 2 min 5 min
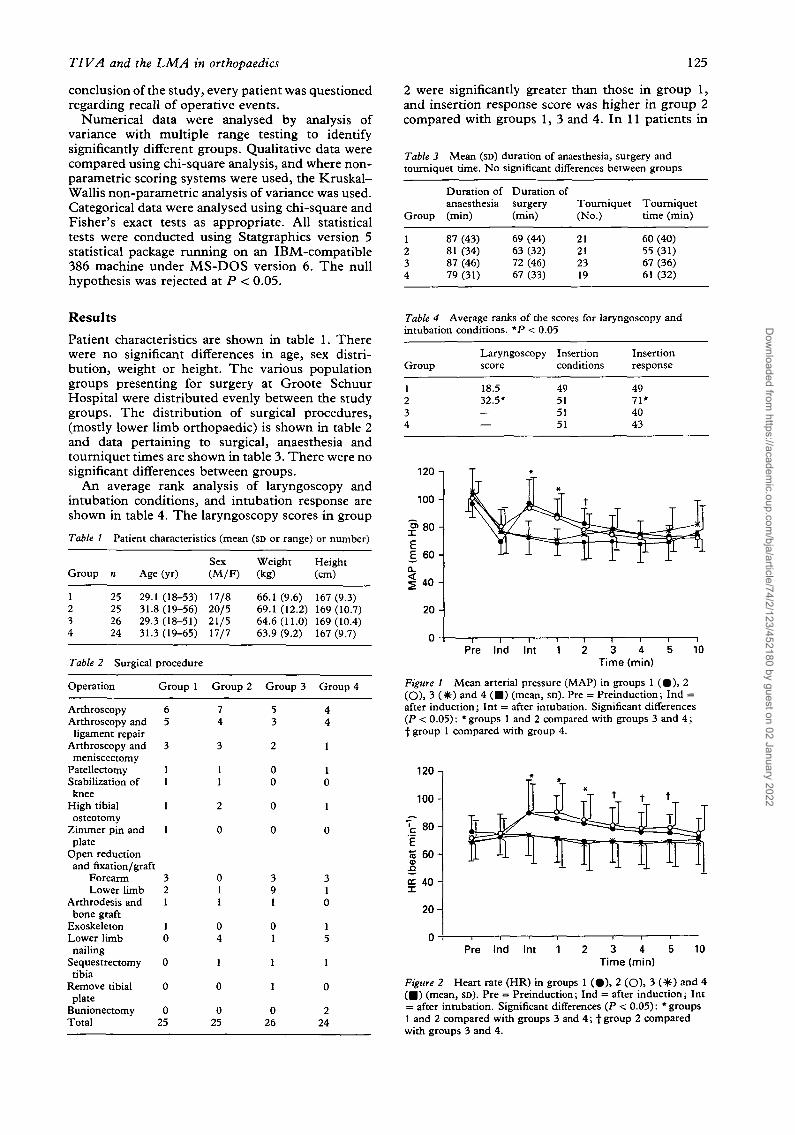
Figure -4 Adrenaline concentrations in groups 1 ("B), 2 10) , 3 i\J) and 4 i • . ) mean, SD,. Prel = Preinduction;Post = after induction; Pre = before extubation. Significant differences (P < 0.05): * within-group differencesfrom baseline values; f within-group differences from all other measurement times; i group 3 compared withgroup 2; ', group 3 compared with group 4.
group 2 laryngoscopy scores were greater than 2 andthis necessitated suxamethonium before intubation.Consequently, insertion conditions were similar forall groups.
Haemodynamic data for the first 10 min afterinsertion of the airway management device are shownin figures 1 and 2. Groups 1 and 2 had significantlyhigher heart rates and mean arterial pressures thangroups 3 and 4 for varying periods up to 5 min afterintubation. Baseline plasma catecholamine con-centrations were not significantly different betweengroups. Changes in plasma concentrations of cate-cholamines during and after induction and extuba-tion are shown in figures 3 and 4. No consistentwithin- or between-group trends could be demon-strated. There was no significant increase in cate-cholamine concentrations in response to either TTor LMA insertion.
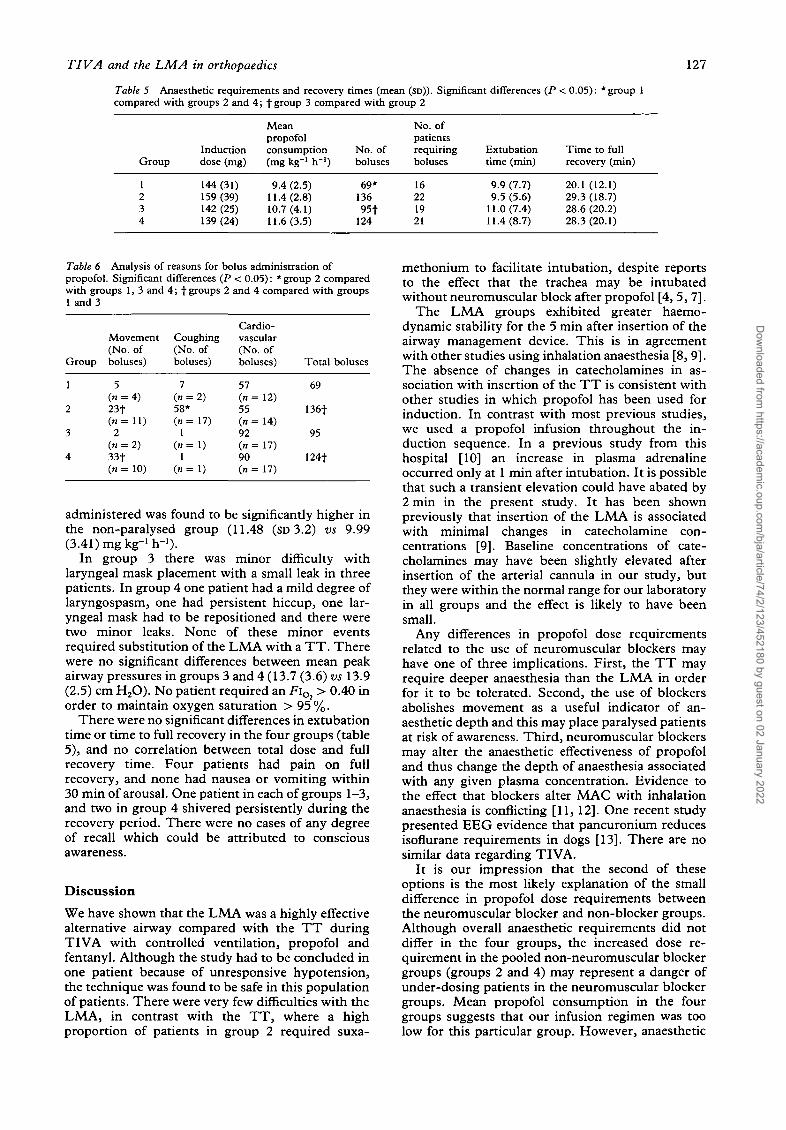
Table 5 shows data on anaesthetic requirements.There was no significant difference between groupsin induction dose or total dose. Groups 2 and 4required significantly more bolus doses of propofolthan group 1, and group 3 required significantlyfewer boluses than group 2. The percentage of druggiven as boluses was relatively small (10.1 %, 17.4 %,11.8% and 17.0% in groups 1 ^ , respectively). Thecommonest indication for bolus administration ingroups 1, 3 and 4 was a change in heart rate orarterial pressure (table 6). Patients in group 2required significantly more interventions forcoughing than groups 1, 3 and 4; groups 2 and 4required more boluses for movement than groups 1and 3. The total anaesthetic requirement was similarin all groups. However, when groups 1 and 3 (withneuromuscular block) were pooled and comparedwith groups 2 and 4, the total dose of propofol
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/2/123/452180 by guest on 02 January 2022
TIVA and the LMA in orthopaedics 127
Table 5 Anaesthetic requirements and recovery times (mean (SD)). Significant differences (P < 0.05): * group 1compared with groups 2 and 4; f group 3 compared with group 2
Group
1234
Inductiondose (mg)
144(31)159 (39)142 (25)139 (24)
Meanpropofolconsumption(mg kg"1 h"1)
9.4 (2.5)11.4(2.8)10.7(4.1)11.6(3.5)
No. ofboluses
69*13695t
124
No. ofpatientsrequiringboluses
16221921
Extubationtime (min)
9.9 (7.7)9.5 (5.6)
11.0(7.4)11.4(8.7)
Time to fullrecovery (min)
20.1 (12.1)29.3 (18.7)28.6 (20.2)28.3(20.1)
Table 6 Analysis of reasons for bolus administration ofpropofol. Significant differences (P < 0.05): * group 2 comparedwith groups 1, 3 and 4; f groups 2 and 4 compared with groups1 and 3
Group
1
2
3
4
Movement(No. ofboluses)
5(« = 4)23t( n = l l )
2(n = 2)33f(n = 10)
Coughing(No. ofboluses)
7(« = 2)58*(« = 17)
1(«=1)
1(«=1)
Cardio-vascular(No. ofboluses)
57(n = 12)55(n = 14)92(« = 17)90(n = 17)
Total boluses
69
136f
95
124t
administered was found to be significantly higher inthe non-paralysed group (11.48 (SD 3.2) vs 9.99
ggIn group 3 there was minor difficulty with
laryngeal mask placement with a small leak in threepatients. In group 4 one patient had a mild degree oflaryngospasm, one had persistent hiccup, one lar-yngeal mask had to be repositioned and there weretwo minor leaks. None of these minor eventsrequired substitution of the LMA with a TT. Therewere no significant differences between mean peakairway pressures in groups 3 and 4 (13.7 (3.6) vs 13.9(2.5) cm H2O). No patient required an FiO2 > 0.40 inorder to maintain oxygen saturation > 95 %.
There were no significant differences in extubationtime or time to full recovery in the four groups (table5), and no correlation between total dose and fullrecovery time. Four patients had pain on fullrecovery, and none had nausea or vomiting within30 min of arousal. One patient in each of groups 1-3,and two in group 4 shivered persistently during therecovery period. There were no cases of any degreeof recall which could be attributed to consciousawareness.
DiscussionWe have shown that the LMA was a highly effectivealternative airway compared with the TT duringTIVA with controlled ventilation, propofol andfentanyl. Although the study had to be concluded inone patient because of unresponsive hypotension,the technique was found to be safe in this populationof patients. There were very few difficulties with theLMA, in contrast with the TT, where a highproportion of patients in group 2 required suxa-
methonium to facilitate intubation, despite reportsto the effect that the trachea may be intubatedwithout neuromuscular block after propofol [4, 5, 7].
The LMA groups exhibited greater haemo-dynamic stability for the 5 min after insertion of theairway management device. This is in agreementwith other studies using inhalation anaesthesia [8, 9].The absence of changes in catecholamines in as-sociation with insertion of the TT is consistent withother studies in which propofol has been used forinduction. In contrast with most previous studies,we used a propofol infusion throughout the in-duction sequence. In a previous study from thishospital [10] an increase in plasma adrenalineoccurred only at 1 min after intubation. It is possiblethat such a transient elevation could have abated by2 min in the present study. It has been shownpreviously that insertion of the LMA is associatedwith minimal changes in catecholamine con-centrations [9]. Baseline concentrations of cate-cholamines may have been slightly elevated afterinsertion of the arterial cannula in our study, butthey were within the normal range for our laboratoryin all groups and the effect is likely to have beensmall.
Any differences in propofol dose requirementsrelated to the use of neuromuscular blockers mayhave one of three implications. First, the TT mayrequire deeper anaesthesia than the LMA in orderfor it to be tolerated. Second, the use of blockersabolishes movement as a useful indicator of an-aesthetic depth and this may place paralysed patientsat risk of awareness. Third, neuromuscular blockersmay alter the anaesthetic effectiveness of propofoland thus change the depth of anaesthesia associatedwith any given plasma concentration. Evidence tothe effect that blockers alter MAC with inhalationanaesthesia is conflicting [11, 12]. One recent studypresented EEG evidence that pancuronium reducesisoflurane requirements in dogs [13]. There are nosimilar data regarding TIVA.
It is our impression that the second of theseoptions is the most likely explanation of the smalldifference in propofol dose requirements betweenthe neuromuscular blocker and non-blocker groups.Although overall anaesthetic requirements did notdiffer in the four groups, the increased dose re-quirement in the pooled non-neuromuscular blockergroups (groups 2 and 4) may represent a danger ofunder-dosing patients in the neuromuscular blockergroups. Mean propofol consumption in the fourgroups suggests that our infusion regimen was toolow for this particular group. However, anaesthetic
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/2/123/452180 by guest on 02 January 2022

128 British Journal of Anaesthesia
depth was adjusted easily by bolus administration ofpropofol. There were more interventions in the formof bolus administration of propofol in the non-paralysed groups compared with the paralysedgroups. Analysis of the reasons for these inter-ventions gave some insight into the clinical feasibilityof the technique. Coughing generally interfered withsurgery and made controlled ventilation difficult tomanage. In contrast, movement not associated withcoughing did not interfere with surgery or impairventilation. Thus the increased number of bolusesrequired in response to coughing in group 2 vs group4 suggests that if neuromuscular blocking drugs arenot used, the LMA is an easier airway managementdevice during TIVA than the TT. Although therewere no increased anaesthetic requirements if neuro-muscular blockers were omitted while using theLMA, patients in group 4 required more inter-ventions for movement than group 3. It is alsonoteworthy that the increased incidence of move-ment in group 4 did not make controlled ventilationmore difficult to manage than in group 3 (furthersupported by the similar mean peak airwaypressures). Moreover, movement provided an addedindication of wakefulness, and suggests some benefitin the omission of neuromuscular blockers if thesurgical site does not require paralysis. This isparticularly relevant in routine clinical anaesthesia,where the average anaesthetist has no access tosophisticated indicators of intraoperative awareness,such as the processed EEG and evoked potentials,and must be guided by cardiovascular responses andmovement.
Although there were differences in the number ofbolus doses between groups, the relatively smallpercentage of drug administered as a bolus accountsfor the absence of significant differences in totaldoses. Lacrimation and sweating were absent in thisstudy; glycopyrronium 0.2 mg given to preventbradycardia was probably inadequate to explainthis finding, and it may be a feature of propofolanaesthesia.
AcknowledgementsWe thank Sr E. Thomas for her assistance, and Zeneca Pharma-ceuticals for their advice and sponsorship.
References1. Rajah A, Morgan M. Non-barbiturate drugs for the induction
and maintenance of anaesthesia. Bailliere's Clinical Anaes-thesiology 1991; 5: 425-452.
2. Hughes MA, Glass PSA, Jacob JR. Context-sensitive half-time in multicompartment pharmacokinetic models for in-travenous anesthetic drugs. Anesthesiology 1992; 76: 334-341.
3. Hickey S, Cameron AE, Asbury AJ. Cardiovascular responseto insertion of Brain's laryngeal mask. Anaesthesia 1990; 45:629-633.
4. Mulholland D, Carlisle RJT. Intubation with propofolaugmented with intravenous lignocaine. Anaesthesia 1991;46: 312-313.
5. Keaveny JP, Knell PJ. Intubation under induction doses ofpropofol. Anaesthesia 1988; 43: S80-S81.
6. Weicker H, Ferandi N, Haegele H, Pluto R. Electrochemicaldetection of catecholamines in urine and plasma afterseparation with HPLC. Clinica Chemica Ada 1984; 141:17-25.
7. Beck GN, Masterson GR, Richards J, Bunting P. Comparisonof intubation following propofol and alfentanil with in-tubation following thiopentone and suxamethonium. An-aesthesia 1993; 48: 876-880.
8. Braude N, Clements EAT, Hodges VM, Andrews BP. Thepressure response and LMA insertion. A comparison withtracheal intubation. Anaesthesia 1989; 44: 551-554.
9. Lamb K, James MFM, Janicki PK. The laryngeal maskairway for intraocular surgery: effects on intraocular pressureand stress responses. British Journal of Anaesthesia 1992; 69:143-147.
10. Brossy MJ, James MFM, Janicki PK. Haemodynamic andcatecholamine changes after induction of anaesthesia witheither thiopentone or propofol with suxamethonium. BritishJournal of Anaesthesia 1994; 72: 596-598.
11. Forbes AR, Cohen NH, Eger El II. Pancuronium reduceshalothane requirement in man. Anesthesia and Analgesia1979; 58: 497^199.
12. Foley MR, Sessler DI, Cannon JE, Brody K, Stoen R, MillerRD. Atracurium, vecuronium and pancuronium do not alterthe minimum alveolar concentration of halothane in humans.Anesthesiology 1989; 71: 53-56.
13. Schwartz AE, Navedo AT, Berman MF. Pancuroniumincreases the duration of electroencephalogram burst sup-pression in dogs anaesthetized with isoflurane. Anesthesiology1992; 77: 686-690.
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/2/123/452180 by guest on 02 January 2022