Embed Size (px)
Citation preview

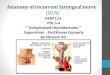
Laryngeal Cancer
Anh Q. TruongMS-4
University of Washington, SOM

Anatomy

Vaezi, MF . Nature Clinical Practice Gastroenterology & Hepatology (2005) 2, 595-603
Anatomy – cont’

Anatomy – subdivision
Source: AJCC Cancer Staging Manual, 6th Ed (2002)

Most common head and neck CA (excluding skin) 12,250 new cases/yr Male : Female = 4 : 1 > 90% squamous cell cancer Glottic CA more common in Caucasian (in US) Glottic CA = supraglottic in African American (in US) Variation of ratio around world
Incidence by Site
Supraglottic 40%
Glottic 59%
Subglottic 1%
Epidemiology
American Cancer Society: Cancer Facts and Figures 2008. Atlanta, Ga: American Cancer Society, 2008.

Tobacco smoking, bidi smoking, alcohol.
MJ smoking correlation HPV, GERD implicated Possibly perchloroethylene
Risk Factors

Signs and symptoms Mass effect: hoarseness, dysphagia, hemoptysis, neck
mass, airway compromise (difficulty breathing), aspiration
Throat pain, ear pain (referred through CN X branch) Suggests advanced stage
Hoarseness = allow for early detection of glottic cancer
Supraglottic CA = tend to present later Usually present w/bulkier tumors before Si/Sx present
More likely to present w/node mets d/t richer lymphatics
Weight loss
Clinical Presentation

Clinical Presentation – cont’
Physical Exam Complete head and neck exam
Palpation for nodes; restricted laryngeal crepitus. Quality of voice
Breathy voice = cord paralysis Muffled voice = supraglottic lesion
Laryngoscopy Laryngeal mirror Fiberoptic exam (lack depth perception) Note: contour, color, vibration, cord mobility, lesions.
Stroboscopic video laryngoscopy Highlights subtle irregularities: vibration, periodicity, cord closure

Differential Diagnosis
Infectious Inflammatory Granulomatous disease (TB, sarcoidosis) Papillomatosis Lymphoma

Imaging
CT or MRI Evaluate pre-epiglottic or paraglottic space Laryngeal cartilage erosion Cervical node mets
PET Role under investigation, currently not standard of care Specific application
Identifying occult nodal mets Distinguish recurrence vs radionecrosis or other prior tx sequalae
Ultrasound In Europe: used to identify cervical mets and laryngeal abn.

Biopsy and Histology
Direct laryngoscopy with biopsy Histologic subtypes
Squamous cell carcinoma > 90% of causes Characterized by nl hyperplasia dysplasia CIS
invasive CA Invasive CA characterized by: well, moderately, or poorly
differentiated Nest of malig epi cells, desmoplastic & inflammatory stroma,
keratin pearls (in well and mod dif CA). Linked to tobacco and excessive alcohol Variance: verrucous, spindle cell carcinoma, & basaloid.

Biopsy and Histology – cont’
Histologic subtypes - cont’ Salivary gland
Adenoid cystic carcinoma Mucoepidermoid carcinoma Surgery is preferred w/guidelines for adjuvant XRT
Sarcomas (mainly chondrosarcoma) Most commonly from cricoid cartilage Nonaggressive, preferably tx with partial laryngeal surgery XRT viewed as ineffective
Others: carcinoid tumors, lymphoma, mets.

Supraglottis Tis: CA in-situ T1: limited to subsite of
supraglots w/normal cord mobility
T2: invade mucosa of > 1 subsite of supraglottis, glottis, or outside of supraglottis w/out fixation of the larynx
T3: limited to larynx w/vocal cord fixation and/or invades postcricoid area, pre-epiglottic tissues, paraglottic space, and/or minor thyroid cartilage erosion
T4a: invades thyroid cartilage and/or tissues beyond larynx
T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures
• Glottis– Tis: CA in-situ– T1: limited to cord;
T1a: one cord; T1b: two cords– T2: extends to supraglottis,
and/or subglottis, and/or w/impaired cord mobility
– T3: limited to larynx w/vocal cord fixation and/or invades paraglottic space, and/or minor thyroid cartilage erosion
– T4a: invades thyroid cartilage and/or tissues beyond larynx
– T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures
• Subglottis– Tis: CA in-situ– T1: limited to subglottis– T2: extends to vocal cord with
normal or impaired mobility – T3: limited to larynx w/vocal cord
fixation– T4a: invades cricoid or thyroid
cartilage, and/or invades tissues beyond the larynx
– T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures
Staging
Source: AJCC Cancer Staging Manual, 6th Ed (2002)

• Subglottis– Tis: CA in-situ– T1: limited to subglottis– T2: extends to vocal cord with
normal or impaired mobility – T3: limited to larynx w/vocal cord
fixation– T4a: invades cricoid or thyroid
cartilage, and/or invades tissues beyond the larynx
– T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures
Staging• Nodes
– N0: no regional node mets– N1: single ipsilateral node, ≤ 3
cm– N2a: single ipsilateral node, > 3
cm, ≤ 6 cm– N2b: multiple ipsilateral nodes, ≤
6 cm– N2c: bilateral or contralateral
nodes, ≤ 6 cm– N3: node > 6 cm
• Mets– Mx: unknown– M0: no distant mets– M1: distant mets
Source: AJCC Cancer Staging Manual, 6th Ed (2002)

Stage Grouping
Stage 0 Tis N0 M0
Stage I T1 N0 M0
Stage II T2 N0 M0
Stage IIIT3 N0 M0
T1-3 N1 M0
Stage IVAT4a N0-1 M0
T1-4a N2 M0
Stage IVBT4b any N M0
any T N3 M0
Stage IVC any T any N M1
Earlystage
Advanced stage

Surgery Microlaryngeal surgery Hemilargyngectomy Supraglottic laryngectomy Near-total laryngectomy Total laryngectomy
Photodynamic Therapy Radiation Chemothrapy
Cisplatin + 5-fluorouracil
Treatments – Options

Current therapeutic options Laser microsurgery (transoral) Open partial laryngectomy Radiation therapy
No RCT to compare surgery w/XRT Rate of local control similar between surgery and
radiation Current recommendations, XRT with surgery reserved
for salvage therapy with local recurrence
Treatment – Early Stage (I/II)
Mendenhall WM et al., Cancer. 2004 May 1;100(9)

Dose Fractionation
Yu et al., 1997 [1] Retrospective study – 5 yr local ctr rate of XRT on T1 glottic CA Daily fx > 2 Gy (50 Gy/2.5Gy QD & 65.25Gy/2.25 Gy QD) had 5
yr local ctr rate of 84% Daily fx = 2 Gy had 5 yr local ctr 65.6%
Andy Trotti, RTOG 95-12 – closed [2] Randomized pts with T2 glottic cancer to 70Gy/2Gy QD vs 79.2
Gy/1.2 Gy BID
1Yu E. et al., Int J Radiat Oncol Biol Phys. 1997 Feb 1;37(3):587-91.2www.rtog.org/members/protocols/95-12/95-12.pdf

Dose Fractionation
Yamazaki et al., 2006 RTC – 5 yr local ctr rate of XRT on T1 glottic CA 2 Gy/fx (60Gy/30 fx or 66Gy/33fx): 5 yr local ctr rate = 77% 2.25 Gy/fx (56.25Gy/25fx or 63 Gy/28fx): 5 yr local ctr rate = 92%
Yamazaki H et al., Int J Radiat Oncol Biol Phys. 2006 Jan 1;64(1):77-82

Treatment – Advanced Stage (III/IV) – VA Study
Dept of VA Laryngeal CA Study Group, 1991 RCT: Induction chemo XRT vs laryngectomy post-op
XRT Chemo arm = cisplatin + 5-FU x 2c if partial/complete
response 3rd cycle XRT*, else salvage surgery
Surgery arm = total laryngectomy (partial if poss) XRT*
*XRT = definitive: 66 Gy – 76 Gy; post-op: 50.4Gy (+10Gy if high risk of local recurrence)
Department of Veterans Affairs Laryngeal Cancer Study Group, N Engl J Med 1991;324:1685-90.

Treatment – Advanced Stage (III/IV) – VA Study cont’
Department of Veterans Affairs Laryngeal Cancer Study Group, N Engl J Med 1991;324:1685-90.
Overall Survival
Surg + XRT
Chemo + XRT
2 yr OS = 68% in both groups, P = 0.9846
Surg + XRT
Chemo + XRT
Chem + XRT shorter disease free interval, but dif not significant
Disease Free Survival

Treatment – Advanced Stage (III/IV) – VA Study cont’
Department of Veterans Affairs Laryngeal Cancer Study Group, N Engl J Med 1991;324:1685-90.
Site of recurrence
Surgery
(N = 166)
Chemotherapy (N=166)
Primary 4 (2%) 20 (12%)
Regional 9 (5%) 14 (8%)
Distant 29 (17%) 18 (11%)
All 42 (25%) 52 (31%)
No difference in rate of recurrence, significant difference in site of recurrence, significant difference in development of a 2nd primary CA (surg 6%, chemo 2%)

Treatment – Advanced Stage (III/IV) – VA Study cont’
Of the 166 pts in the chemo arms - 107 (64%) patients had preserved larynx - 30 patients (18%) laryngectomy before definitive XRT - 29 patients (18%) laryngectomy after definitive XRT
Department of Veterans Affairs Laryngeal Cancer Study Group, N Engl J Med 1991;324:1685-90.

Treatment – Advanced Stage (III/IV) – RTOG 91-11 Study
Forastiere et al, (RTOG 91-11), 2003 RCT: XRT alone vs induction chemo XRT vs concurrent
chemoXRT, primary endpoint = larynx perservation
XRT: 70Gy/35fx in all arms
Induction – cisplatin + 5 FU x 2c if complete or partial response, w/out neck progression 3rd cycle XRT; else laryngectomy XRT
Concurrent – cisplatin x 3c + XRT
Forastiere AA et al, N Engl J Med 2003;349:2091-8.

Treatment – Advanced Stage (III/IV) – RTOG 91-11 Study Induction Chemotherapy
173 assigned 168 completed chemo x 2c 144 complete or partial response 134 completed 3rd chemo cycle
84% of pts received ≥ 67 Gy
Concurrent Chemoradiation 172 assigned 120 (70%) completed cisplatin x 3 cycle, 40
(23%) completed cisplatin x 2 cycles. 91% of pts received ≥ 67 Gy
Radiation alone 95% of pts received ≥ 67 Gy
Forastiere AA et al, N Engl J Med 2003;349:2091-8.

Treatment – Advanced Stage (III/IV) – RTOG 91-11 Study
2 yr 3.8 yr 5 yr updateA
- induction chemo XRT: 75% 72% 70.5% - concurrent chemoXRT : 88%* 84%* 83.6% - XRT alone : 70% 67% 65.7%
Laryngeal Preservation
Forastiere AA et al, N Engl J Med 2003;349:2091-8.
AForastiere AA et al, Journal of Clinical Oncology, Vol 24, No. 18S(June 20 Supplement),2006:5517.

Treatment – Advanced Stage (III/IV) – RTOG 91-11 Study
2 yrs 5 yr updateA
- induction chemo XRT: 64% 54.9% - concurrent chemoXRT : 80% 68.8% - XRT alone : 58% 51%
Locoregional Control
Forastiere AA et al, N Engl J Med 2003;349:2091-8.
AForastiere AA et al, Journal of Clinical Oncology, Vol 24, No. 18S(June 20 Supplement),2006:5517.

Treatment – Advanced Stage (III/IV) – RTOG 91-11 Study
Concurrent chemoXRT
Induction chemo XRT
XRT alone
2 yrs 5 yrs 2 yrs 5 yrs 2 yrs 5 yrs
Dz Free SurvivalA
61% 36% 52% 38% 44% 27%
Overall SurvivalB
74% 54% 76% 55% 75% 56%
Distant metsC
8% 12% 9% 15% 16% 22%
AChemo therapy significant decreased in dz free survival compared to XRT alone (P =0.02 compared w/induction, P = 0.06 compared w/conccurent Tx)BNo significant differenceCDifference only significant comparing concurrent chemoXRT vs XRT alone.
Forastiere AA et al, N Engl J Med 2003;349:2091-8.

Treatment – Advanced Stage (III/IV) – cont’
Forastiere AA et al, N Engl J Med 2003;349:2091-8.

Hypothyroidism Mucositis Dermatitis Xerostomia Fibrosis Fistulas Dysgeusia
Anticipated Toxicities

Take Home Points
Most laryngeal CA are SCC Low stage can be tx by different modalities
Fraction size ≥ 2.25 Gy/fx may increase local ctr OS similar b/w surgery + XRT vs chemo +
XRT in advanced stage, but organ preservation better with chemo + XRT
Organ preservation: concurrent XRT > chemo XRT = XRT alone
Don’t smoke or drink too much alcohol

An Actual Picture of a Laryngeal Cancer
(L) Source: http://www.medscape.com/content/2002/00/44/25/442595/442595_fig.html
(R) Source: http://www.som.tulane.edu/classware/pathology/medical_pathology/New_for_98/Lung_Review/Lung-62.html

Questions?







![Aquaporins as diagnostic and therapeutic targets in cancer ...cancer, Laryngeal cancer, Lung cancer [43], Nasopharyngeal cancer, Ovarian cancer [37] Tumor grade, prognosis, tumor angiogenesis,](https://img.dokumen.tips/doc/110x75/5ffa8fafa51a2a21db58011f/aquaporins-as-diagnostic-and-therapeutic-targets-in-cancer-cancer-laryngeal.jpg)

![Cancer Research - Characterization of Human Laryngeal ......(CANCER RESEARCH 49. 6098-6107, November 1, 1989] Characterization of Human Laryngeal Primary and Metastatic Squamous Cell](https://img.dokumen.tips/doc/110x75/605796831b34e0624044f1b9/cancer-research-characterization-of-human-laryngeal-cancer-research-49.jpg)


















