Embed Size (px)
Citation preview

Tobacco Cessation Quitlines: A Platform for Behavior Change Research
Society for Behavioral MedicinePre-conference Seminar
April 7, 2010

Overview• Introduction• Quitline “Nuts and Bolts”• Examples of Quitline Research• Unanswered Questions and Areas of Interest• Practical Tips• Wrap-up and Discussion

Introductions
• Jessie Saul, Ph.D., Director of Research, North American Quitline Consortium
• Paula Keller, M.P.H., Senior Policy Advisor, University of Wisconsin Center for Tobacco Research and Intervention
• Susan Zbikowski, Ph.D., Vice President, Clinical and Behavioral Sciences, Free & Clear, Inc.
• Cindy Haugland, B.S., Manager of Business Development, National Jewish Health

Quitline “Nuts and Bolts”

Why should Behavioral Medicine think about Quitlines?
• Over 440,000 people die every year in the United States from tobacco use.1
• For every person who dies from smoking, 20 more people, more than 8.5 million people, suffer from a smoking-related illness every year. 2
1 The health consequences of smoking: a report of the Surgeon General. [Atlanta, Ga.]: DHHS, CDC, OSH; Washington, D.C.: U.S. G.P.O., 2004.
2 Hyland, A., et al, ”Cigarette Smoking – Attributable Morbidity – United States 2000,”Morbidity and Mortality Weekly Report, September 5, 2003 / 52(35);842-844.

Why should Behavioral Medicine think about Quitlines?• Quitlines are effective interventions for helping people quit 1,2
• Quitlines are available to all tobacco users in the U.S. and Canada
• Quitlines are easily accessible• Lessons learned from Quitlines can be translated to other
areas of behavioral medicine• Behavioral medicine questions can be tested in real-world
environments through Quitlines
1 Fiore MC et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service. 2008.
2 Stead LF, Perera R, Lancaster T. A systematic review of interventions for smokers who contact quitlines. Tob Control. 2007 Dec;16 Suppl 1:i3-8.

What is a Quitline?

What is a Quitline? (cont.)
• Multiple proactive (outbound) calls (100%)
• Single call protocols (66%)
• Internet-based cessation services (42%)
• Fax referrals from health care providers (93%)
• Referrals to other services (93%)
2008 NAQC Annual Survey data (N=53 quitlines)

Who is served by Quitlines?
In Fiscal Year 2009, most U.S. Quitline clients were:• Cigarette smokers (96%)• Everyday smokers (95%)• Female (57%)• White (79%)• Straight (96%)• Had a HS education or less (55%)• Were uninsured or had government-sponsored
insurance (e.g., Medicare or Medicaid) (63%)2009 Annual Survey data - PRELIMINARY
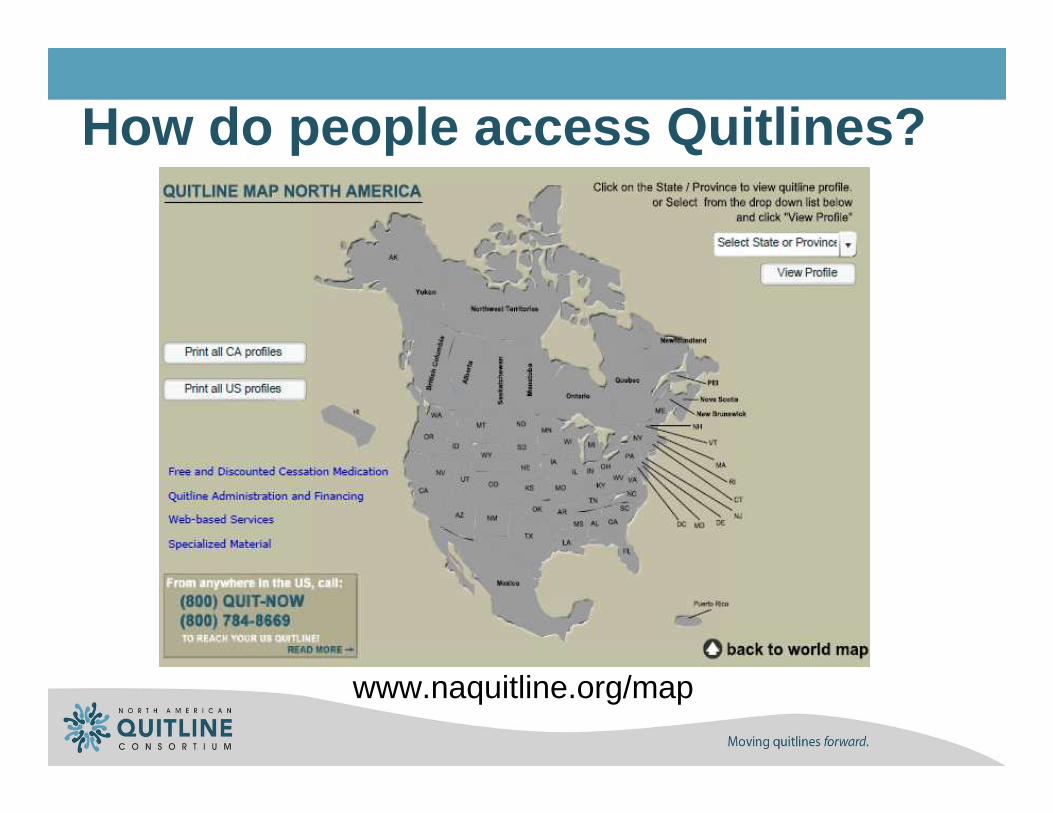
How do people access Quitlines?
www.naquitline.org/map

Promotion and referral mechanisms
• Mass media advertising – Quitline specific• Mass media advertising – general cessation• Earned media (e.g., mention of 1-800-QUIT-
NOW on the Today show)• Health care provider referrals, including fax
referrals• Community organization partnerships• Word of mouth
What happens during counseling?
• Counseling interaction based on theory1
• All quitline protocols incorporate evidence-based interventions, Clinical Practice Guideline recommendations2
• Many have been tested in RCTs
1 Bandura A. (1977) Self-efficacy: toward a unifying theory of behavioral change. Psychological Review,84:191-215. Bandura A. (1986) Social foundations of thought and action: a social cognitive theory. Englewood Cliffs, NJ: Prentice Hall.
2 Fiore MC et al. Treating Tobacco Use and Dependence: 2008 Update Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service; 2008.

Sample calls
Donna Robert
Sample calls available at www.freeclear.com/quit-for-life/

QUESTIONS?

Tools and Resources

Tools for conducting Quitline research
• Minimal Data Set for Quitlines• Standard set of intake and follow-up questions asked of all
callers• Created 2005, revised 2009• Intake: Caller demographics, tobacco use history, intention
to quit• Follow-up: satisfaction, quitting behaviors, tobacco use
status, future intentions• MDS materials available at www.naquitline.org/MDS
Tools (cont.)
• Standardized measures for reach and quit rates for Quitlines• Developed with NAQC members
• Designed to provide “apples-to-apples”comparisons
• Descriptions available at www.naquitline.org/?page=qiiissuepapers
• Existing infrastructure

Funding Announcements
• Multiple opportunities• Federal and non-federal• Many public health and behavior-change
opportunities fit well with quitline research• Health disparities• Intervention projects
• Dissemination projects

Examples of funded research• NIH RePORTER – searched “tobacco and quitline”• 40 research projects funded from FY 2008-FY 2010• Topics include:
• “Efficacy of a smoking quitline in the military”• “Effectiveness of proactive tobacco treatment in diverse low income
smokers”• “Telephone and web-based teen tobacco cessation in HMOs”• “Relapse-prevention booklets as adjunct to a tobacco quitline”• “Using email to enhance counseling services at NCI’s smoking
cessation quitline”• “The impact of smoke-free policy on quitline utilization and smoking
outcomes”• “Ask, Advise, Refer: Promoting pharmacy-based referrals to tobacco
quitlines”

Quitline-specific research findings• PubMed search “quitline” and “tobacco and quitline”• 2005 publication and later• 112 articles• Topics:
• Intervention studies• Medications• Specific populations• Descriptive studies• Promotion and integration• Policy studies

Examples of Quitline Research

QuitLines for many types of studies

UW-CTRI Quitline Research Projects
• Improving the population-wide effectiveness of U.S. tobacco cessation quitlines
• Stevens Smith, PhD, PI; Paula Keller, MPH, Co-Investigator & Project Director
• Aims:• Test promising cessation medication and counseling
enhancements that can be added to existing quitline services to increase quit rates, and
• Identify those quitline treatments that produce the largest and most cost-effective increases in smoking cessation success
• Partners: UW-CTRI, Free & Clear, Inc.• Funder: National Cancer Institute (Challenge grant –
RC1)
• Fax to Quit: Linking smokers visiting clinics to state quitlines• Michael C. Fiore, MD, MPH, MBA, PI; Megan Sheffer, PhD,
Project Director• Aims:
• Test whether “Fax to Quit” increases both contacts and “quality contacts” among quitlines and smokers receiving care in primary care clinics.
• Evaluate whether “Fax to Quit” plus Enhanced Academic Detailing increases successful contact rates and quitline enrollment rates.
• Estimate the incremental costs and yields of this promotional strategy and compare with the costs and yields compared to other promotional strategies
• Partners: UW-CTRI, Free & Clear, Inc., North American QuitlineConsortium, Wisconsin Department of Health Services
• Funder: Centers for Disease Control and Prevention (Innovations in Applied Public Health Research)
UW-CTRI Quitline Research Projects (cont.)

UW-CTRI Quitline Research Projects (cont.)
• Evaluating the Impact of the National Tobacco QuitlineNetwork
• Michael C. Fiore, MD, MPH, MBA, PI; Paula A. Keller, MPH, Co-PI and Project Director
• Aims:• Evaluate changes in quitline organization, financing and
services over time• Identify state-level factors that may influence quitline funding
levels, evaluate whether they are influential, and measure whether these factors change over time
• Partners: UW-CTRI, North American QuitlineConsortium
• Funder: Robert Wood Johnson Foundation, Substance Abuse Policy Research Program

Examples of ResearchStudy State(s) Description
NCI ORQL OR Intensity counseling with medication
OREO OR Effect of free NRT promotion
WI Youth RCT WI Intensity of counseling
OK Wt Concern OK Enhanced counseling
Young Adult Quit Study Multiple Recruitment for intervention testing phone, web, materials
Ask, Advise, Refer CT, WA Comparison of academic detailing vs. none on pharmacist's QL referrals
Fax2Quit WI Comparison of academic detailing vs. none on Fax Referrals
WI Prepare WI Predicting smokers relapse
Low SES IVR WA Does proactive outreach increase QL re-engagement
Oral Health WA Are smokers interested in learning about oral health concerns
Enhanced NRT WI Intensity of medication and enhanced medication counseling
Smoking & Obesity Multiple Determine the effectiveness of cessation for over weight and obese smokers

National Jewish HealthSample Research Studies
Smoking Cessation for Persons with Mental Illnesses: 6-Month Results from Community-Based Interventions
Salish Kootenai College – working with Native American college student who enrolled in both the QuitLine and a Face-to-Face program
Characteristics and abstinence outcomes among tobacco quitline enrollees using Vareniclineor Nicotine Replacement Therapy
Improving Delivery of Smoking Cessation Guidelines in Hospitalized Veterans
The Effectiveness of Smoking Cessation Guidelines in the Emergency Department
Providing Fax referrals from a Pediatric Emergency Room for Parents of Children admitted with Asthma/Allergies
A cost-effectiveness study of nicotine patches distributed through a QuitLine 8 vs. 4 week supply of free NRT among callers who smoke 16-20 cigarettes at QuitLine enrollment

A Randomized Trial of Internet and Telephone Treatment for Smoking Cessation
NIH funded 3 year collaboration between• Brown University
• American Legacy Foundation
• National Jewish Health• QuitNet
Primary question studied • Quit rates at 3, 6, 12 and 18 months for
• Those enrolled over the Internet• Control Group• Internet Enhanced (QuitNet)• Internet Enhanced Plus QuitLine (QuitNet and National Jewish)

A Randomized Trial of Internet and Telephone Treatment for Smoking Cessation
Recruitment through Internet (Google, Yahoo, MSN and AOL)
• N = 2,005 who were randomized to 3 groups • All interventions free of charge to participants
• Telephone assessments for quit rates
– With incentives and Internet option for completion of assessment
Primary Outcome• 30-day point prevalence abstinence measured at 12 months• Data indicate that Internet program provides positive smoking cessation
benefit that was statistically enhanced by QuitLine participation
National Jewish now offers an Internet program to supplement its QuitLineprogram

Randomized Trial Testing a Web-based Quit
Smoking ProgramNIH funded multi- year collaboration between
• Klein Buendel• National Jewish Health• Cancer Control Research Institute - Australia
Primary question• A cost effectiveness analysis comparison between a newly developed Internet smoking
cessation program and the QuitLine in smokers between 20 and 30 years of age.
Analyses will be performed in two methods• One including the cost of building the Internet smoking cessation program and the
QuitLine (considered “developmental costs”)• One excluding the cost of building the Internet smoking cessation program and the
QuitLine
The study is now closed and the data are being analyzed at this time.

NAQC Collaborative Research Project
KIQNIQ: Knowledge Integration in Quitlines: Networks that Improve Cessation
Scott Leischow, PhD, PIAims:
• Investigate the social network structure of quitlines in the US and Canada, and its role on dissemination and implementation of new quitline practices.
• Investigate the potential moderating role of decision-making norms, organizational learning characteristics, and quitlinecharacteristics on adoption of new quitline practices
Partners: North American Quitline ConsortiumFunder: National Cancer Institute

BREAK

Quitline Research: Unanswered Questions and Areas of Interest

Quitline Research Themes
• Who uses Quitlines?• How to best reach diverse communities?• What behavioral interventions hold promise in
a Quitline environment?• Are innovations in service delivery models
needed?• How to best provide cessation medications
through Quitlines?

Research themes (cont.)• How to best integrate Quitline services with
other technology?• What are best practices for promoting
Quitlines?• Are Quitlines cost-effective?• Can effective public-private financing models
be developed?• How can lessons learned from tobacco
quitlines inform other quitline services?

Who Uses Quitlines?
• Who calls Quitlines?• Age, gender, race/ethnicity, insurance
status, education, level of dependence
• Changes in caller demographics• Does the population of callers reflect the
population of tobacco users in the state?

How to Best Reach Diverse Communities?
• How well are Quitlines serving diverse communities?• May require aggregating data across
multiple Quitlines to study some populations
• Are there cultural barriers to accessing services?
• Evaluating culturally tailored protocols/services for diverse communities, or for communities at high risk of tobacco use (e.g., young adults).

What Behavioral Interventions hold Promise in a Quitline Environment?
• Formative analysis of smokers’experiences to identify influencers of success and relapse
• Adherence interventions (for counseling and medication use)
• Theoretical frameworks for counseling• Number and length of calls• Practice quit attempts

Are Innovations in Service Delivery Models Needed?• Proactive outreach to smokers
• All smokers?
• High-risk populations?
• Long-term follow-up to improve long-term cessation outcomes
• Matching services to caller’s needs/risk factors
• Integrating Quitline services within health care systems

How to Best Provide Cessation Medications through Quitlines?
• Optimal medication duration to achieve best outcomes
• Cost-effectiveness of various types and durations of medication
• Comparisons of the use of medication as a promotional strategy compared to costs and outcomes resulting from paid media or other promotional strategies

How to Best Integrate Quitline Services with Other Technology?
• Web-based coaching• Other online interaction (gaming, chat)• Email messaging• Interactive voice response (IVR)• Text messaging
What are Best Practices for Promoting Quitlines?
• Paid media/advertising• Direct mail/direct outreach to smokers• Earned media• Fax referral• Social networking
Are Quitlines Cost-Effective?
• Cost-effectiveness of:• Service delivery models
• Promotional strategies• Types and duration of medications
• Yield/Return on investment from providing services to specific populations (e.g., pregnant women, people with COPD, diabetes or other co-morbid conditions)
Can Effective Public-Private Financing Models be Developed?
• How to leverage government investment in Quitline services• Does government support lessen the private
sector’s interest in financing such services?
• Risk-based sharing of financing for services and promotion among different institutions

How Can Lessons Learned from Tobacco Quitlines Inform other Quitline Services?
• How to apply a Quitline model to other health risk behaviors• Weight gain• Multiple risk factor interventions (e.g., tobacco
use and weight gain)
• Others?

QUESTIONS?

Practical Tips

Studies Typically Impact
• Protocols• Scripts and materials• Data collection• Staff training
Checklist of discussion items
• Research question• Appropriate partners (state funder vs. service
provider)• Timeline• Needed modifications to existing protocols• Cost of necessary modifications• IRB approval• Data ownership and publication
Partnering with States• States are interested in improving services through
innovation that is evidence-based
• Understand the Quitline on all levels (operational, financial, etc.)
• Interested in cost savings & sharing
• Understand implications of adding research to the Quitline procedures
• Creative problem solvers
• Access to State Collaboratives that are dedicated to working on multi-systemic health problems

Effectiveness of Trainings for Referrals
Purpose: Increase Utilization of QL via “Provider” training

Lessons Learned

Addressing Weight Concerns of Smokers
Purpose: Testing the Effectiveness of Enhanced Services for Smokers with Weight Concerns
1. Increased Cessation2. Reduced Weight Gain

Lessons Learned

Best Practices

Challenges

Independent QuitLine Research Study

Independent QuitLine Research Study
A Randomized Trial of Internet and Telephone Treatme nt for Smoking Cessation
Purpose
•To compare effectiveness of Internet Program and Internet Combined with Telephonic QuitLine Program
•Quit Rates at 3, 6 , 12 and 18 months

Changes to Normal Conduct of Business
•Business Agreements• Medical Director as Co-Investigator• Pricing for the Program
• Working with Grant Budgets and Billing Processes• Additional Costs for Coordination/Implementation of the Program• Not Per Call or Participant Pricing
• %’s of Employees working on this project• Indirect and Direct Overhead• Grant Rates – defined by NIH
A Randomized Trial of Internet and Telephone Treatment for Smoking Cessation

Changes to Normal Conduct of Business• Enrollment
• Recruitment for the Study• Advertising on Google and other Websites
• Directed to a phone # for screening – consent and randomization
• Email list to NJ
• Independent toll free number for these callers• Informed Consents for the Study• New questions for the Intake

Changes to Normal Conduct of Business
•IRB Requirements• Multiple IRB’s
•Brown University and NJ
•HIPAA Compliance• BAA’s
•Programming of CMS• Costs and Time required for programming• Staff used 2 systems – entered data in a system at Brown University also
Changes to Normal Conduct of Business
•Staffing• Dedicated staff to study – Supervisor and Coaches• Training (PI to provide all details)• Call Volume in Department during specific times – no change for
this study
•Reporting Requirements• Data Collection from both systems and the Telephony system• Aggregate vs. Individual data• Outcomes – timing/process
•Transitioning from Study Outcomes to Daily Practice• Following this study National Jewish implemented QuitLogix.com
as an additional resource for QuitLine participants
WRAP-UP AND DISCUSSION
Resources
• North American Quitline Consortium Website (www.naquitline.org)
• University of Wisconsin, Center for Tobacco Research and Intervention (www.ctri.wisc.edu)
• Free & Clear, Inc. (www.freeclear.com)• National Jewish Health (www.njh.com)

More resources
Telephone Quitlines: A resource for development, implementation, and evaluation (www.cdc.gov/tobacco/quit_smoking/cessation/quitlines/index.htm)
NAQC collection of documents describing “what is a quitline” and other resources – get notification of updates by signing up atwww.naquitline.org/sustainability
Still more resources
http://www.enqonline.org/
http://www.trdrp.org/Index.asp

Contact InformationJessie [email protected]
Paula [email protected]
Susan ZbikowskiFree & Clear, [email protected]
Cindy HauglandNational Jewish [email protected]