Embed Size (px)
Citation preview

INVITED REVIEW
Tibial Osteotomies for Cranial Cruciate Ligament Insufficiency in Dogs
STANLEY E. KIM, BVSc, ANTONIO POZZI, DMV, MS, Diplomate ACVS, MICHAEL P. KOWALESKI, DVM, Diplomate ACVS,and DANIEL D. LEWIS, DVM, Diplomate ACVS
Objective—To review the biomechanical considerations, experimental investigations, and clinicaldata pertaining to tibial osteotomy procedures for treatment of cranial cruciate ligament (CrCL)insufficiency in dogs.Study Design—Literature review.Methods—Literature search through Pub Med, Veterinary Information Network, CommonwealthAgricultural Bureau Abstracts, and conference proceedings abstracts (November 1977 to March2007).Results—Reported tibial osteotomy procedures attempt to eliminate sagittal instability (cranialtibial thrust) in CrCL-deficient stifles by altering the conformation of the proximal tibia. Functionalstability can be achieved by decreasing the tibial plateau slope (cranial tibial closing wedgeosteotomy [CTWO], tibial plateau leveling osteotomy [TPLO], combined TPLO and CTWO,proximal intraarticular osteotomy, chevron wedge osteotomy), altering the alignment of the patellartendon (tibial tuberosity advancement), or both (triple tibial osteotomy). Clinical reports assessingthe efficacy of these procedures frequently use subjective outcome measures, and the periods offollow-up evaluation are highly variable. Satisfactory results have been reported in most (475%)dogs irrespective of the type of tibial osteotomy procedure.Conclusions—Currently available data does not allow accurate comparisons between different tibialosteotomy procedures, or with traditional methods of stabilizing the CrCL-deficient stifle. Carefullydesigned long-term clinical studies and further biomechanical analyses are required to determine theoptimal osteotomy technique, and whether these procedures are superior to other stabilizationmethods.Clinical Relevance—Limb function in dogs with CrCL insufficiency can be improved using thecurrently described tibial osteotomy techniques.r Copyright 2008 by The American College of Veterinary Surgeons
INTRODUCTION
CRANIAL CRUCIATE ligament (CrCL) insufficien-cy is one of the most common causes of lameness
in dogs.1 Rupture of the CrCL can be caused entirelyby trauma; however, in most dogs rupture is a conse-quence of mid-substance, progressive, pathologic fa-tigue.2 Subsequent instability invariably leads to
development of progressive stifle osteoarthritis (OA)and often results in secondary meniscal damage.This debilitating condition commonly affects youngadult large breed dogs and frequently affects both stifleswithin a year of the initial diagnosis.3 The economic im-pact of treating dogs with CrCL insufficiency in theUnited States has been estimated in 2003 at just over$1 billion.4
Address reprint requests to Dr. Antonio Pozzi, Department of Small Animal Clinical Sciences, College of Veterinary Medicine,
University of Florida, Gainesville, FL 32610. E-mail: [email protected].
Submitted May 2007; Accepted November 2007
From the Department of Small Animal Clinical Sciences, University of Florida, Gainesville, FL; and the Department of Clinical
Sciences, Tufts Cummings School of Veterinary Medicine, North Grafton, MA.
r Copyright 2008 by The American College of Veterinary Surgeons
0161-3499/08
doi:10.1111/j.1532-950X.2007.00361.x
111
Veterinary Surgery
37:111–125, 2008

Treatment of CrCL insufficiency aims to resolve lame-ness caused by joint instability and provide good long-term function of the affected hindlimb. Conservativemanagement of dogs weighing o15kg typically results inacceptable limb function, with reported success ratesranging from 84% to 90%.5,6 Surgical intervention is,however, recommended for most dogs with CrCLinsufficiency to reestablish joint stability, mitigate second-ary degenerative joint disease, and address any concur-rent meniscal injury.6,7 Over the past 50 years, a plethoraof surgical techniques have been reported for treatmentof this condition. This evolution of surgical proceduresreflects the controversy about optimal management ofCrCL insufficiency, and to date, no one pro-cedure has consistently demonstrated superior clinicalefficacy.
Traditional surgical techniques attempt to impart sta-bility using an autogenous, allogenic, or synthetic structureplaced within or about the stifle that mimics the function ofthe normal CrCL. Extraarticular techniques use periartic-ular heavy gauge suture or wires,8,9 or the transposition ofsoft tissues10 to reduce stifle laxity, whereas intraarticulartechniques attempt to anatomically reconstruct the CrCLusing autogenous tissues,11 allografts,12 or synthetic mate-rials.13 Most authors cite good to excellent limb function inmost of dogs that have had extra- or intraarticular proce-dures.14,15 Yet despite these reported satisfactory results,traditional methods are generally considered to yield sub-optimal long-term outcomes, as these techniques fail toconsistently maintain stability, arrest the progression ofOA, and prevent late meniscal damage.9,16,17
As surgical techniques continue to evolve, the focushas shifted to the concept of creating dynamic stability inthe CrCL-deficient stifle by altering bone geometry. In1984, Slocum described the cranial tibial wedge osteo-tomy (CTWO), a surgical procedure that attempts toeliminate cranial subluxation of the tibia during weight-bearing by reducing the caudally directed slope of thetibial plateau.18 By establishing dynamic stability of theCrCL-deficient stifle, passive restraint against laxity is notrequired. Recognition that stabilization could be achievedin this manner led to the development of several proximaltibial osteotomy procedures, such as tibial plateau level-ing osteotomy (TPLO)19; combined TPLO/CTWO20;proximal tibial intraarticular osteotomy (PTIO)21; tripletibial osteotomy (TTO)22; and chevron wedge osteotomy(CVWO).23 The more recently described tibial tuberosityadvancement (TTA) procedure attempts to dynamicallyneutralize craniocaudal instability by altering the relativealignment of the patellar tendon to the tibial plateau.24
Although there are few studies evaluating long-termfunctional outcomes of any of these tibial osteotomytechniques, most have been associated with favorableclinical results.18–22,24–26
Our purpose was to review the biomechanical consid-erations, experimental investigations, and clinical datapertaining to tibial osteotomy procedures for treatingCrCL insufficiency in dogs.
CrCL BIOMECHANICS
Because of the high prevalence of CrCL insufficiency,and because CrCL transection in dogs is frequently usedas an experimental model to induce OA,27 the structureand function of the CrCL has been extensively investi-gated.28–32 Cadaveric experiments, in vivo kinematic an-alyses and theoretical models have contributed tounderstanding of CrCL biomechanics and subsequentlylead to the development of tibial osteotomy techniques.
Using a cadaver model, Arnoczky and Marshall dem-onstrated that the CrCL contributes to passive restraintspecifically limiting cranial translation of the tibia relativeto the femur, excessive internal rotation of the tibia, andhyperextension of the stifle.29 Other structures that pro-vide passive restraint of the canine stifle include the cau-dal cruciate ligament (CaCL), the collateral ligaments,and menisci.29,33,34 The loss of a passive supportingstructure about a joint may increase laxity, but does notnecessarily result in clinically relevant instability.35 Dur-ing in vivo activity, joints are subject to other importantdynamic restraint mechanisms, such as those producedby muscular force.35 For instance, electromyographicstudies have shown that humans with anterior cruciateligament rupture can inhibit anterior tibial translation byincreasing hamstring tone and decreasing quadriceps ac-tivity.36 Further, the magnitude of forces applied to ajoint to demonstrate and quantify joint laxity in vitromay be considerably different than the physiologic loadsthat are sustained in vivo. Therefore, results of cadaverexperiments such as those reported by Arnoczky andMarshall do not fully define whether or not the CrCL is aprimary stabilizer of the canine stifle.
Kinematic studies in dogs, using stereo radio-photogrammetry and/or instrumented spatial linkage,were able to confirm that CrCL transection results insubstantial cranial tibial subluxation during the stancephase of gait.30,31 These findings demonstrate that mus-cular forces are unable to compensate for the loss of re-straint provided by the CrCL. In all but 1 dog, cranialtibial translation did not occur during the swing phase ofgait. Thus, the authors concluded that the stability of thestifle during the stance phase of gait is dependent on theCrCL, whereas stability during the swing phase of gait isnot dependent on the integrity of the CrCL. These ob-servations are in agreement with findings from a study ingoats that measured dynamic CrCL strain in vivo, wheremaximum CrCL force occurred in early stance phase, and
112 TIBIAL OSTEOTOMIES FOR CRANIAL CRUCIATE LIGAMENT INSUFFICIENCY IN DOGS

dropped to zero during the swing phase of gait.37 Con-versely, neither kinematic study found significant differ-ences in peak internal rotation magnitude between CrCL-deficient dogs and normal dogs,30,31 suggesting that eitherthe CrCL is a secondary stabilizer against internal tibialrotation, or that nominal internal tibial torques are gen-erated while walking.
In the clinical setting, diagnosis of complete CrCLrupture is made by detection of craniocaudal joint laxity,which can be elicited by applying a cranially directed loadon the proximal tibia. The ‘‘cranial drawer’’ test can beconsidered a ‘‘static’’ clinical test and is analogous to thecadaver experiment performed by Arnoczky and Mar-shall, because eliciting cranial drawer relies on displace-ment of a bone in the direction of an applied force.35
‘‘Dynamic’’ tests, on the other hand, aim to mimic theforces and dynamic instabilities that normally occur dur-ing weight bearing.35 The ‘‘tibial compression’’ test, de-scribed by Henderson and Milton38 in 1978, attempts toreplicate a weight-bearing force on the limb by flexing thehock. With the stifle at a standing angle, the tensiongenerated in the gastrocnemius muscle creates strongcaudodistal traction of the femur and consequently acranioproximal shear force on the tibia.38 This force isnormally counteracted by the CrCL, so cranioproximaltranslation of the tibia will result if the CrCL is ruptured.The tibiofemoral shear force that occurs during weight-bearing was termed ‘‘cranial tibial thrust’’ by Slocum in1983.32
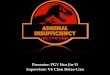
Slocum also presented a theoretical model that pro-posed the magnitude of cranial tibial thrust was depen-dent on the degree of the caudodistally directed slope ofthe tibial plateau.32 Quantification of the tibial plateauslope, the tibial plateau angle (TPA), is defined by theangle formed between the slope of the medial tibial con-dyle and the perpendicular to the longitudinal axis of thetibia.18 Reported mean TPAs in clinically normal dogsrange from 18 to 241.39–41 According to Slocum, thecompressive forces of weight-bearing, assumed to beparallel to the axis of the tibia, can be resolved into acranially directed component (the cranial tibial thrust)responsible for cranial tibial translation, and a jointcompressive force (Fig 1).32 A correlation between tibialplateau slope and anterior or cranial tibial thrusthas been confirmed in human and animal in vitromodels.42–44 It is, however, important to note that thereis no definitive evidence substantiating that dogs withhigher than average TPAs are at greater risk for devel-oping CrCL insufficiency.39,40
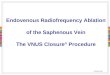
More recent biomechanical theories argue that thetibia is not axially loaded as proposed by Slocum. Rather,Tepic suggests that the total tibiofemoral joint forces invivo are directed parallel to the patellar tendon.28,45 Cra-nial tibial thrust, according to this model, is then depen-
dent on the angle between the tibial plateau and thepatellar tendon (Fig 2).28 This model also predicts thatcranial tibial translation should not occur when a CrCL-deficient stifle is flexed beyond 901.28
Based on the predominant craniocaudal instabilitygenerated by CrCL transection in vivo; it is reasonable toconclude that neutralization of cranial tibial thrust islikely the most important function of the CrCL.30 Ac-cordingly, current tibial osteotomy techniques primarilyaim to address the sagittal plane instability that occurs asa result of weight-bearing. Because these procedures donot provide a passive restraint against internal tibialrotation, excessive internal tibial rotation may still occur(e.g. during certain vigorous activities that involve piv-oting on the pelvic limb), and rotational instability maypotentially contribute to the subsequent development ofOA and meniscal injury.
CTWO
CTWO was the first reported procedure that attempt-ed to eliminate cranial tibial thrust by reducing TPA.18
Initially recommended as an adjunct to procedures thatimpart passive stabilization (such as fascial imbrication),CTWO involves leveling the TPA by resecting a cranially
Fig 1. Slocum theorized that, during weight bearing, the joint
reaction force (magenta arrow) is approximately parallel the
longitudinal axis of the tibia. In the CrCL-deficient stifle (A),
the joint reaction force can be resolved into a cranially directed
tibiofemoral shear component (parallel to tibial plateau) and a
joint compressive force (perpendicular to tibial plateau). By
leveling the tibial plateau (B), the joint reaction force is per-
pendicular to the tibial plateau, thus can only be resolved into
a joint compressive force; cranial tibial thrust is eliminated.
CrCL, cranial cruciate ligament.
113KIM ET AL

based wedge of bone from the proximal tibia, apposingthe margins of the ostectomy site, then stabilizing the 2bone segments with a medially applied bone plate usingAO-ASIF principles (Fig 3). The ostectomy is performedas proximally as feasible while preserving a large enoughproximal bone segment to allow for fixation with at least3 screws in each segment.46
Recent biomechanical studies suggest that to achieve apostoperative TPA of 51, and thereby neutralize cranialtibial thrust, the angle of the wedge to be excised shouldequal the measured preoperative TPA.47 Intuitively, itwould seem that a wedge angle equal to the TPA wouldresult in a postoperative TPA of 01. Performing aCTWO, however, induces tibial longitudinal axis shift,which is responsible for inadequate leveling of the tibialplateau slope.46,48 After CTWO, the proximal landmarkfor defining the tibial longitudinal axis of the tibia, theintercondylar tubercles, is shifted cranially.46,48 To com-pensate for this change in position, ‘‘over-rotation’’ of thetibial plateau is necessary to achieve the expected TPA of51. The postoperative TPA will be larger than anticipatedif calculations do not account for the shift of the longi-tudinal axis of the tibia.46
Wide discrepancies in the postoperative TPAs havebeen reported after CTWO.18,49,50 For instance, within asingle case series reported by Macias et al49, postopera-tive TPAs ranged from 7 to 211. Difficulty in attaining thetarget TPA may be attributed to variability in size andposition of the ostectomy, and tibial longitudinal axisshift.46 Resecting a wedge equal to the TPA, performingthe ostectomy as proximal as practical, and aligning thecranial cortices is recommended to improve the accuracyof the procedure.46,47 Intraoperative calculation of thewedge angle should be precise and methodical to furtherminimize variability in the postoperative TPA. A trigo-nometric method,20 or a sterilized template of the desiredwedge made from radiographic film can be used for thispurpose.
CTWO may be indicated in dogs with certain types ofproximal tibial conformation. Although no causal rela-tionship between a high TPA and CrCL insufficiency hasbeen established, abnormally steep tibial plateau slopeshave been implicated as the underlying cause of CrCLrupture in several case series.20,49–51 Exceedingly steeptibial plateau slopes secondary to alterations in proximaltibial physeal growth may be most amenable to treatmentwith a CTWO.52 Osmond et al52, attempted to charac-terize anomalies of the proximal portion of the tibia bycorrelating the morphometry of the proximal tibia inclinical CrCL insufficiency cases with computer-generat-ed models that mimicked different tibial morphologies.
Fig 2. An alternate theory, proposed by Tepic, suggests that
the joint reaction force (magenta arrow) is approximately par-
allel to the patellar tendon, not the tibial long axis. In the
CrCL-deficient stifle (A), the joint reaction force can be re-
solved into a cranially directed tibiofemoral shear component
and a joint compressive force (yellow arrows). By advancing
the tibial tuberosity cranially, the patellar tendon is perpen-
dicular to the tibial plateau during stance phase of gait (B). The
joint reaction force, therefore, becomes perpendicular to the
tibial plateau during weight bearing, thus can only be resolved
into a joint compressive force; cranial tibial thrust is eliminat-
ed. CrCL, cranial cruciate ligament.
Fig 3. Position of the osteotomies and postoperative illustra-
tion of cranial tibial wedge ostectomy.
114 TIBIAL OSTEOTOMIES FOR CRANIAL CRUCIATE LIGAMENT INSUFFICIENCY IN DOGS

The authors identified a subset of CrCL-deficient dogswith steep TPAs attributed to proximal shaft deformities,and theorized that the tibia would assume a more ana-tomically correct alignment after CTWO, as the proce-dure tilts the distal portion of the tibial shaft in relation tothe proximal portion.52 In our experience (A.P.), correc-tion of substantial proximal tibial varus or torsion arealso more easily addressed by CTWO compared withother tibial osteotomy techniques.
Although dynamic stabilization of CrCL-deficient sti-fles is receiving considerable attention, reports document-ing clinical outcomes after CTWO are sparse. In apreliminary study of the CTWO involving 17 dogs, Slo-cum and Devine reported rapid return to function andclinical union of the osteotomy for most dogs by 6 weeksafter surgery.18 All 9 dogs evaluated at 12 months aftersurgery had limb function that was subjectively consid-ered indistinguishable from normal. Radiographic evi-dence of OA did not progress in any of the stifles;however, objective, quantitative assessment of stifle OAwas not performed. The dogs also had semitendinosus,gracilis, and biceps femoris muscle advancement to re-duce laxity, confounding the assessment of the CTWOprocedure. In a retrospective analysis of 91 dogs treatedwith CTWO, 86% of the dogs were considered to havegood-to-excellent limb function based on the results of aclient survey and physical examination.25 Two case seriesreported the results of CTWO in small breeds dogs withproximal tibial deformities.49,50 Subjective lameness grad-ing or owner satisfaction was used to gauge the efficacy ofthe procedure. All dogs (13 overall) in both studies hadgood-to-excellent limb function within 6 weeks after sur-gery, and maintained good limb use with an averagefollow-up of 1 year. In 1 of these reports, CTWO wascombined with lateral suture stabilization, making itdifficult to ascertain the efficacy of CTWO alone in thisgroup of dogs.50
Reported complications have been principally associatedwith failure of fixation and nonunion.18,25,49,50,53 In a directclinical comparison of TPLO and CTWO, the second-sur-gery rate for CTWO was 11.9%, nearly twice the second-surgery rate for TPLO (4.5%).51 Of the 12 dogs requiringsurgical revision after CTWO, 9 were considered to havecatastrophic tibial fractures requiring multiple plating.51
CTWO has the advantage of not requiring patentedspecialized equipment.53 Other advantages include theability to address exceedingly steep tibial plateau slopes,as well as tibial varus and torsion. Because CTWO causesdistal displacement of the patellar tendon insertion, theprocedure may be used to treat concurrent patella alta.20
Disadvantages include: variability in postoperative TPAs,potential for creating patella baja and limb shorten-ing.20,49,50 Also, inducing longitudinal tibial axis shiftmay result in esthetically undesirable craniocaudal an-
gulation of the tibia.20 With the growing recognition ofproximal tibial angular limb deformities inducing steepTPAs, CTWO may gain wider acceptance in the treat-ment of CrCL insufficiency.
TPLO
Like CTWO, TPLO aims to provide dynamic cranio-caudal stifle stability during the stance phase of gait byreducing the slope of the tibial plateau. Proposed bySlocum in 1993, TPLO involves performing a radialosteotomy of the proximal tibia with subsequent rotationof the proximal segment to enable precise manipulationof the tibial plateau slope.19 Based on the radius of theosteotomy and the preoperative TPA, the exact amountof rotation of the proximal segment is calculated toachieve a postoperative angle of 51.54 The procedure isperformed by a medial approach to the proximal tibia.54
A biradial saw blade is used to create a crescent-shapedosteotomy; compression of the osteotomy results in com-plete congruency, as the inner and outer edges of the sawblade are of the same diameter.54 A custom-jig that isapplied medially maintains alignment of the bonesegments while allowing for rotation of the proximalsegment.54 The osteotomy should be centered over theintercondylar tubercles to ensure accurate rotation andmaintain enough bone in the proximal segment for ad-equate purchase during internal fixation of the osteotomy(Fig 4).54 Imprecise positioning of the osteotomy mayresult in an inaccurate tibial plateau leveling and com-plications such as angular and rotational deformities, andtibial tuberosity fracture.55–57
Biomechanical studies have demonstrated that aftertibial plateau rotation, the tibiofemoral shear force shiftsfrom cranial to caudal when the limb is loaded.42,43 Thus,it has been postulated that joint stability is dependent onthe CaCL neutralizing caudal tibial translation afterTPLO.42 The recommended postoperative TPA was de-fined as 0 and 51 when the procedure was first describedin 1993 and in the TPLO licensing course, respective-ly.18,54 Despite these specific guidelines, the optimal TPAis still a contentious subject. In vitro studies demonstratethat cranial tibial thrust is effectively neutralized at amean angle of 6.51.42,43 Three-dimensional computermodeling of the canine stifle, on the other hand, foundthat rotation to 51 only marginally decreased the tensileforce acting on the CrCL.58 Both in vitro analyses andtheoretical modeling, however, can fail to reliably predictclinical outcome.59 Limitations associated with cadaverexperiments include the difficulty of replicating naturallyoccurring disease and the inability to simulate all themuscular forces acting on the joint. Inaccuracies of com-puter modeling can arise from multiple assumptions, suchas disregarding muscular compensation, and simplifying
115KIM ET AL

joint geometry. Data from in vitro and computer-mod-eling investigations should be interpreted and applied toclinical cases with caution because of these limitations. Ina clinical study by Robinson et al60, there was no statis-tically significant relationship between TPA and groundreaction forces after TPLO, where the postoperativeTPAs were between 0 and 141. Satisfactory results ofunder-rotated stifles, which were indistinguishable fromthe outcome of dogs that had ‘‘optimal’’ postoperativeTPAs, may be indicative of complete elimination of cra-nial tibial thrust in vivo over a wide range of angles.Optimal TPAs may vary between breeds, or indeed be-tween individual dogs. Chronically affected stifles maynot require as much rotation as stifles with acute rupture,because periarticular fibrosis can contribute substantiallyto joint stability.7 Alternatively, the presence of residualcranial tibial thrust after TPLO may not result in lame-ness.19 Precise in vivo kinematic analyses are required toidentify the optimal TPA and further understand thebiomechanics of the TPLO.
Results for dogs treated with TPLO have so far beenencouraging, although there are no studies documentingobjective data with follow-up 417 months (mean).60
Subjective evaluation of limb function suggests earlierreturn to weight-bearing after TPLO when comparedwith the intra- and extracapsular forms of stabilization.61
Beyond the initial recovery period, however, convincingproof that the TPLO results in superior limb function
currently does not exist. In Slocum’s original study,which included 394 dogs, outcomes at follow-up evalu-ations 46 months after surgery were reported as excel-lent for 73%, good for 21%, and fair for 3%.19 Anotherstudy with a follow-up ranging from 6 months to 4 yearsreported that 93% of owners were satisfied with the out-come after TPLO, which is similar to the proportion ofowner satisfaction after other techniques.57 Good to ex-cellent long-term function, based on owner evaluation,has also been reported in most dogs (25 cases, 50 stifles)treated with single-session bilateral TPLOs.62
In an in vivo experiment by Ballagas et al63, experi-mentally induced CrCL-deficient pelvic limbs were treat-ed with TPLO and evaluated with force plate analysispreoperatively, at 8 and 18 weeks after surgery. By 18weeks, peak vertical force and vertical impulse were notsignificantly different when compared with preoperativevalues, although a subjective mild lameness was still ev-ident in 4 of 6 dogs. Conzemius et al64 in a prospectiveclinical study in Labrador Retrievers with CrCL insuffi-ciency compared limb function after lateral suture stabi-lization, intracapsular stabilization, and TPLO usingforce platform gait analysis. Contrary to the conclusionsdrawn by some studies that evaluated outcomes subjec-tively, these investigators found no difference in groundreaction forces or peak vertical impulse between TPLOand lateral suture stabilization treated dogs at 2 and 6months after surgery. Moreover, only 10.9% of TPLO-treated dogs obtained comparable limb function to clin-ically normal dogs compared with 14.9% of dogs withlateral suture stabilization and 15% of dogs with intra-capsular stabilization evaluated in the same study.
There are several reports that have investigated theprogression of stifle OA after TPLO. A prospective ra-diographic study of 40 dogs showed a significant overallincrease in mean osteophyte scores 6 months afterTPLO.65 Interestingly, progression of osteophytosis wasnot evident in most (57.5%) of dogs, and radiographicparameters of OA were improved in 2 dogs.65 A com-parison of long-term radiographic changes after TPLOand lateral suture stabilization revealed that whereasTPLO did not prevent progression of OA, rate of pro-gression was � 3-fold less than stifles that had lateralsuture stabilization.66 Studies assessing the efficacy ofTPLO based on radiographic OA assessment should beinterpreted with caution, as soft tissue (e.g. cartilage,synovium, menisci, periarticular tissues) changes are notreadily identifiable with this imaging modality, and 1study has shown that radiographic OA changes in thestifle are not predictive of limb function.67
Numerous intra- and postoperative complicationshave been reported in dogs undergoing TPLO. The rel-ative high frequency of complications reported for TPLOmay be because of the large number of cases that have
Fig 4. Position of the osteotomy and postoperative illustra-
tion of tibial plateau leveling osteotomy.
116 TIBIAL OSTEOTOMIES FOR CRANIAL CRUCIATE LIGAMENT INSUFFICIENCY IN DOGS

been evaluated in the literature, and many of these studieswere documenting initial experience with this technique.The overall complication rate is reportedly 26–34%, withtibial tuberosity fracture, implant failure, patellar ten-donitis, subsequent meniscal tear after TPLO and infec-tion reported most frequently.57,68–72 Whereas most areimplant or fracture-related complications, others havebeen attributed to abnormal stifle biomechanics inducedby TPLO.57,68–72 Tibial tuberosity fracture occurs in 3–7% of TPLO cases.68–70 Most of these fractures are non-or minimally displaced and do not require surgical inter-vention.57 Fracture of the tibial tuberosity may be causedby a stress riser effect at the site of Kirschner wire place-ment used to maintain the rotation of the tibial plateausegment, or at the narrow isthmus of the tibial tuberositycreated by a cranially positioned osteotomy.68,69 Thermalnecrosis, vascular compromise secondary to soft tissuedissection, increased strain in the patellar tendon afterTPLO and large rotations of the tibia plateau segmenthave also been cited as potential predisposing fac-tors.20,57,68 A retrospective analysis by Kergiosen et al57
identified age, weight, single session bilateral TPLO sur-gery and tibial tuberosity width as potential risk factorsfor tibial tuberosity fractures. Prophylactic pin and ten-sion bands have been used in an attempt to decrease therisk of tibial tuberosity fractures.62
Patellar tendonitis is also common, and may causelameness within the first 2 months after TPLO.68,69,71,72
Clinical signs are usually self-limiting. Patellar tendonthickening, visible on radiographs or by ultrasonography,is most commonly noted distally.72 Possible causes in-clude trauma to the patellar tendon sustained duringsurgery because of excessive retraction, or thermal dam-age associated with saw blade contact.71,72 Histopatho-logic changes in the tendon are noninflammatory andsimilar to those identified in humans with patellar tendonstrain, hence excessive loading of patellar tendon second-ary to altered biomechanics after TPLO has also beenimplicated as a possible underlying cause.55,71 Rotationof the tibial plateau segment may result in a decreasedmoment arm if the distance between the patellar tendoninsertion and instant center of rotation of the stifle isreduced; in turn, greater forces in the quadriceps mech-anism may be required to generate the same extensormoment about the stifle.55,71 This theory is corroboratedby findings from a radiographic study by Mattern et al72,where lower postoperative TPAs (o61) were associatedwith more severe ultrasonographic changes in the patellartendon.
Recurrent lameness after TPLO may indicate subse-quent meniscal injuries. Although meniscal tears occur-ring after stabilization of CrCL-deficient stifles have beenreported as a complication associated with several pro-cedures,73,74 it is proposed that there is a high risk of
developing meniscal injuries after TPLO because passivejoint stability is not restored.19 The caudal pole of themedial meniscus acts as a wedge between the femoral andthe tibial condyles and may become crushed during cra-nial tibial translation.34 TPLO places the stifle joint in agreater angle of flexion during weight bearing, whichmight result in excessive loading of the caudal pole of themedial meniscus.28 Slocum and others have advocatedcomplete radial transection of the medial meniscus,termed meniscal release, to allow caudal displacementof the caudal pole of the medial meniscus during cranialtibial translation, thereby preventing subsequent meniscaltears.19,68 In vitro studies have, however, shown thatmeniscal release impairs load transmission and stabilityof the stifle.34,75 The adverse consequences of releasingthe meniscus were corroborated by a radiographic studydemonstrating greater progression of OA in dogs thathad meniscal release.76 Furthermore, there is no evidenceto suggest that meniscal release eliminates the risk ofsubsequent meniscal tears.77 A recent retrospective studyreported a 3.5% incidence of subsequent meniscal injuryin stifles that underwent arthrotomy with meniscalrelease.77 Meniscal release did not reduce the rate ofsubsequent meniscal tearing when compared with casestreated arthroscopically without meniscal release.77
Whereas traditionally, stifle arthrotomy has been con-sidered as an accurate method for assessing the menisci,78
the data suggest that lack of identification of meniscaltears at the time of TPLO may play an important role inthe development of recurrent lameness because of men-iscal pathology.77 Indeed, a recent cadaver study foundthat meniscal examination by arthrotomy had significant-ly lower sensitivity and specificity than arthroscopy fordiagnosing meniscal tears.79 When meniscal pathologycannot be comprehensively assessed in the CrCL-deficientstifle, releasing the medial meniscus is advocated to de-crease the incidence of subsequent meniscal tears.77,79 Ifthe medial meniscus is thoroughly evaluated at the time ofTPLO, and cranial tibial thrust is effectively neutralized,meniscal release may not be warranted.77,79
The decision to release an intact meniscus remainscontroversial, and the issue is further complicated by theapparent nominal impact meniscal release has on limbfunction.77 Further studies are necessary to determine thelong-term effects of meniscal release on joint function. Itis important to note that although meniscal release ismost commonly referenced to TPLO, performing a men-iscal release is not restricted to this procedure becausepassive joint laxity is a consistent feature of all tibialosteotomy techniques.
CaCL injury is cited as a potential complication afterTPLO.19 Because TPLO is postulated to induce caudaltibial thrust, over-rotation increases strain on the CaCL.42
Whereas increased strain has been demonstrated in
117KIM ET AL

cadaver studies,42 clinical cases with postoperative lame-ness definitively attributed to CaCL strain or rupturehave not been reported, even in cases where TPAs havebeen as low as �71.68
Neoplasia developing at the TPLO surgical site hasbeen documented; however, a direct causal relationshiphas not been proven.80 Boudrieau et al80 recently de-scribed a dog with an histiocytic sarcoma involving theproximal portion of the tibia 5 years after TPLO. Visual,microscopic, chemical and metallographic analysis of theTPLO plate retrieved from this dog revealed corrosion;poor resistance to corrosion was attributed to the castingmanufacturing process of the implant. Implant corrosionwas implicated as a potential cause of tumor develop-ment, and 3 additional dogs were identified that hadpreviously undergone TPLO and developed osseous ne-oplasia of the proximal tibia. These findings promptedfurther investigations; metallurgic analyses of both newand previously implanted Slocum TPLO plates revealedthese plates had unusual surface irregularities and poros-ity.81,82 Aluminum and silicon residua and inclusions,which were thought to have originated from the castmoulds, were also identified.81
Conflicting results exist regarding corrosion of retrie-ved implants.81–83 Although investigations have focusedon corrosion as a potential cause for neoplasia, othercausative factors that are not specific to the SlocumTPLO plate, such as the osteotomy itself, have not beeneliminated. Moreover, TPLO is almost exclusively rec-ommended to a population of dogs that are at risk fordeveloping primary osseous neoplasia, of which the prox-imal tibia is a common site of occurrence.84 Further workis warranted to determine whether the TPLO procedure,or the specific implants used, increase the risk of tumordevelopment.
Infection, manifesting as septic arthritis, osteomyelitis,or superficial wound infection is reported with a rate of3–7%, which is greater than the infection rate previouslyreported for other clean surgical procedures.68–70,85 Septicarthritis is considered one of the most serious complica-tions encountered after TPLO.68 The cause of higher in-fection rate after TPLO is likely multifactorial. Infectionafter open reduction and internal fixation of proximaltibial fractures in human patients is attributed to poor softtissue coverage and blood supply.86 Poor soft tissue cov-erage of the surgical site may play a role in migration ofbacteria through the surgical wound from the externalenvironment.86 Extensive soft tissue dissection around theproximal tibia, poor tissue handling, prolonged surgicaltime, surface plate characteristics87, and thermal necrosisat the osteotomy site may also contribute to infection.
TPLO is currently the most common tibial osteotomyperformed, and widely regarded by many veterinary sur-geons as the best surgical option for CrCL insufficiency in
medium to large breed dogs.64 Advantages includegeometric precision, maintenance of the original positionof the tibial tuberosity and patellofemoral joint.20 Dis-advantages include the technical difficulty and complica-tions of the surgical procedure, including iatrogenicangular and torsional deformities, as well as the poten-tial adverse affects on stifle biomechanics.56,57,69,70,72
TTA
TTA, first described by Montavon et al24 in 2002, at-tempts to dynamically stabilize the CrCL-deficient stiflewithout leveling the tibial plateau. As previously dis-cussed, theoretical models of the stifle predict that thetotal joint forces are approximately parallel to the patel-lar tendon.28 Thus, if the patellar tendon is orientedperpendicular to the tibial plateau, there is no shearcomponent of the total joint force. During the stancephase of gait, where the stifle angle is 1351 of extension,the angle between the patellar tendon and the tibial pla-teau is approximately 1051.45 Accordingly, reducing thisangle to 901 should stabilize the CrCL-deficient stifle (Fig2). This anatomic conformation can be achieved by per-forming a TTA (Fig 5). The procedure involves making alongitudinal osteotomy subjacent to the tibial tuberosity.An appropriately sized spacer-cage is implanted at theproximal extent of the osteotomy to secure the tibial
Fig 5. Position of the osteotomy and postoperative illustra-
tion of tibial tuberosity advancement.
118 TIBIAL OSTEOTOMIES FOR CRANIAL CRUCIATE LIGAMENT INSUFFICIENCY IN DOGS

tuberosity in a cranial position. The width of the cage,available in 3, 6, 9, and 12mm sizes, is determined bymeasurements made from preoperative lateral pelvic limbradiographs with the stifle at � 1351 extension.24 A ten-sion-band bone plate is applied to the medial aspect ofthe tibia, and autogenous or allogenic bone graft is placedin the resulting defect to accelerate bone union.24
Theoretical reduction of tibiofemoral shear forces byadvancing the insertion of the patellar tendon has beensubstantiated in both cadaver and computer-modelingstudies.88–90 Maquet’s procedure in human patients in-volves anterior advancement of the tibial tuberosity,which is advocated for treatment of patellofemoralpain.91 In a cadaver study of Maquet’s procedure, themagnitude of tibiofemoral forces in a direction tangentialto the joint surfaces consistently decreased after incre-mental advancement, provided the knee angle was atnear-to-full extension.90 Similarly, finite element analysisof the human knee found that, at near full extension, an-terior cruciate ligament and tibiofemoral contact forcessubstantially decreased after advancement of the tibial tu-berosity.89 A recent in vitro study performed in caninecadaver pelvic limbs also demonstrated neutralization oftibiofemoral shear forces by advancing the tibial tubero-sity, where the mean patellar tendon-to-tibial plateau anglerequired to eliminate cranial tibial thrust was 90� 91.88
Clinical outcomes after TTA are currently document-ed in a small number of preliminary reports only 2 ofwhich are still in abstract form.24,92,93 In a prospectiveclinical trial of 40 CrCL-deficient stifles treated withTTA, mean peak vertical force was 32% of body weightpreoperatively, and doubled to 64% of body weight at afinal examination performed between 4 and 12 monthsafter surgery.92 This was still significantly lower than amean peak vertical force of 74% in clinically normaldogs, although the results are comparable with the find-ings in a similar study evaluating pelvic limb functionbefore and after TPLO.92 In a retrospective report, 38 of40 owners (95%) were satisfied with the long-term out-come of TTA, and the author’s clinical impression wasthat the postoperative recovery with this technique wasvery rapid.93 Hoffman et al26, found that, with a medianfollow-up of 24 weeks, owners assessed the overall out-come of the procedure good to excellent in 90% of cases.These initial results appear promising; however, accurateassessment of outcome after TTA is not currently pos-sible because of a lack of reported clinical studies.
Reported complications associated with TTA includeimplant failure, tibial tuberosity fracture, medial patellarluxation, CaCL injury because of excessive advancement,and subsequent meniscal injury.26,92,93 Implant failure,reported to occur in 1–5% of operated limbs, was attrib-uted to either technical error or earlier implant designs thatwere considered too weak; the implants have been subse-
quently modified. Excessive postoperative activity has alsoresulted in complete implant failure.26 Partial CaCL rup-ture diagnosed 4 months after surgery in 1 dog was attrib-uted to excessive advancement of the tibial tuberosity.92
Indeed, in the cadaver study by Apelt et al88, caudal tibialtranslation was found to occur when the tibial tuberositywas advanced beyond the defined angle required to neu-tralize cranial tibial thrust, presumably placing excessivestrain on the CaCL. Postoperative meniscal injuries werefrequent in 1 study, occurring in 7 of 24 cases that hadintact medial menisci at surgery.93 It is difficult to ascertainwhether this was an accurate reflection of the true prev-alence of late meniscal injury associated with the TTA, ifmeniscal lesions were the result of unfavorable biomechan-ics, if meniscal lesions were missed at the primary surgery,or if meniscal lesions were caused by insufficient advance-ment of the tibial tuberosity after TTA.
From a biomechanical perspective, TTA may have 2principal advantages over TPLO. TTA preserves the nat-ural tibiofemoral articulation because the tibial plateau isnot repositioned. In doing so, and provided that the TTAis equally as effective as the TPLO in neutralizing cranialtibial thrust, natural load transmission across the stifle(and menisci) is less likely to be altered. TTA also in-creases the extensor moment arm of the stifle and thus themechanical advantage of the patellar tendon, therebytheoretically reducing the forces acting along the patellartendon.28 TPLO, on the other hand, appears to increasethe strain on the extensor mechanisms of the stifle, re-sulting in clinically relevant complications.55,71 At thisstage, these potentially advantageous features of TTA arepurely speculative, and future biomechanical analyses willhopefully provide information that allows objective com-parisons between TTA and TPLO.
Purported advantages of TTA include being less in-vasive and technically less demanding than other tibialosteotomies, an ability to effectively treat concurrent pa-tellar luxation,94 short operative time, and low postop-erative morbidity.92 Disadvantages include the potentialto cause iatrogenic patellar luxation, requirement forspecialized implants, and potentially high rate of latemeniscal injuries. Because the technique is a new proce-dure, the true benefits and complications are yet to besubstantiated by sufficient clinical or biomechanical data.
OTHER TIBIAL OSTEOTOMY TECHNIQUES
Several other tibial plateau leveling techniques havebeen described. Whereas information regarding theseprocedures is limited, each procedure presents uniquemethods developed to circumvent certain limitations ofconventional tibial osteotomies described above, and maygain further attention in the future.
119KIM ET AL

Combination Closing Wedge Osteotomy and TPLO
Combination TPLO and CTWO is primarily used totreat CrCL-deficient stifles with excessive TPAs (4341).20
Reducing TPA by using both methods concurrently ispurported to diminish the risk of complications encoun-tered when either procedure is performed alone, such aspatella baja and tibial tuberosity fracture.20 The magni-tude of rotation and wedge angle is determined by stan-dardizing 1 measurement (e.g. wedge angle 101), thencalculating the remainder of tibial plateau levelingwith the other measurement (e.g. tibial plateau rota-tion¼TPA–5–wedge angle) to achieve a postoperativeTPA of 51. The radial osteotomy is positioned in thesame location as a standard TPLO, and the craniallybased closing wedge ostectomy is placed such that theapex is at the caudal cortical margin of the TPLO. Ex-tensive rigid internal fixation using interfragmentaryKirschner wires, tension-band wire, and single or doubleplating is required to stabilize all 3 bone segments (Fig 6).
In a clinical series of 15 dogs with excessive TPAs, amean postoperative TPA of 81 was achieved with com-bination TPLO/CTWO.20 At a mean final follow-up of23 weeks, no lameness was observed in 73%, only a mildlameness was noted in the remaining 27%, and all ownerswere satisfied with the overall outcome. Postoperativecomplications were, however, common, occurring in 78%
of cases. Most notably, implant failure necessitating asecond procedure occurred in more than 1 in 4 cases, andmean time to complete radiographic healing was pro-longed at 18 weeks.
CrCL insufficiency in dogs with exceedingly largeTPAs remains a challenging orthopedic problem, anddespite a high complication rate, combination TPLO/CTWO may be one of few surgical procedures resultingin an acceptable outcome. Dogs with excessive TPAs mayalso have concurrent pelvic limb conformational abnor-malities,51 and proponents of combining TPLO withCTWO suggest many of these conditions can be ad-dressed with this technique.20 It is arguably the mosttechnically demanding procedure of all described tibialosteotomies and should thus be performed by only ex-perienced veterinary orthopedic surgeons.
PTIO
PTIO is another tibial plateau leveling technique thatinvolves making a wedge ostectomy with the base of thewedge located between the bursa of the patellar tendonand the cranial aspect of the menisci (Fig 7).21,95 A biaxialapproach is required: tibial osteotomies are performedfrom the medial surface; laterally the craniolateral crusmuscles area is elevated off the proximal tibia and a fibulaostectomy is made to facilitate reduction of the ostectomysite. Both medial and lateral arthrotomies are recom-
Fig 6. Position of the osteotomies and postoperative illustra-
tion of tibial plateau leveling osteotomy and cranial tibial
wedge ostectomy.
Fig 7. Position of the osteotomies and postoperative illustra-
tion of proximal tibial intraarticular osteotomy.
120 TIBIAL OSTEOTOMIES FOR CRANIAL CRUCIATE LIGAMENT INSUFFICIENCY IN DOGS

mended to inspect the stifle and excise the infrapatellar fatpad for adequate visualization during the procedure. Theangle of the wedge to be excised is determined from pre-operative radiographs, but descriptions of calculating thisangle are vague. The margins of the osteotomies are re-duced with reduction forceps and stabilization is achievedwith screws inserted in lag fashion craniocaudally, with orwithout augmentation using a medially positioned 6-holeplate applied in buttress fashion. The medial and lateralfascia may be imbricated to reduce passive instability.
In the original description of this procedure, 75 of 87dogs (86%) were considered to have a sound gait at fol-low-up assessments 4 months postoperatively, but 7 dogs(8%) were still moderately lame.21 Slightly better out-comes were reported by Jerram et al95, where lamenesswas not apparent in 54 of 57 (95%) operated limbs whenexamined 6 months after surgery. The remaining 3 (5%)operated limbs had intermittent, mild, weight-bearinglameness with exercise.95 Although the overall proportionof dogs with satisfactory results is comparable with othertibial osteotomy procedures, multiple complications maypreclude PTIO from gaining wide acceptance.21 A highrate of subsequent meniscal injuries has been observed.Of 57 stifles with an intact medial meniscus, subsequentmeniscal injury requiring surgical intervention occurredin 10 stifles (17.5%).21 Induced tibial valgus deformitywas observed in both reports, occurring in 3–12% ofoperated limbs. Other reported complications includedlong digital extensor trauma or fibrosis, requiring a sec-ond surgery and intensive physical therapy, superficialperoneal nerve injury, laceration of the cranial tibial ar-tery, tibial fracture, osteomyelitis, and implant failure.21,95
The main advantage of PTIO is that it can be per-formed without need for specialized surgical equip-ment.21,95 Disadvantages include long operative time,apparent necessity for medial meniscal release, and oc-currence of complications, such as valgus deformities andlong digital extensor tendon injury that often require sur-gical revision. The requirement for extensive arthrotomiesis unfavorable when compared with other techniques, asstudies have demonstrated acceleration of OA when a fullarthrotomy is performed.96,97 At present, PTIO cannot beadvocated as a valid alternative to TPLO.
Chevron Wedge Tibial Osteotomy
A cranially based tibial wedge ostectomy can be per-formed using chevron kerfs.23 The rationale behind usingmore complex osteotomies stems from the perceptionthat opposed V-shaped osteotomy surfaces resist cranio-caudal shear and torsional forces better than conven-tional linear osteotomies (Fig 8).23 Planning of CVWO issimilar to CTWO: tibial longitudinal axis shift should betaken into consideration when calculating the wedge an-
gle, the osteotomies should be positioned as proximally aspossible, and the ostectomy site is stabilized with a me-dially applied bone plate. Accurate execution of theosteotomies may be facilitated with the use of a saw-bladeguide jig, and stability of the construct can be enhancedby use of a cranially placed screw inserted in lag fashion,directed caudad and proximad.
Clinical outcomes of CVWO for treatment of CrCLinsufficiency in dogs have not been reported, and thus thecomplication rate is unknown. In an in vitro geometricstudy of 5 different tibial osteotomy techniques,23 CVWOinduced the greatest amount of tibial valgus deformity,and postoperative valgus has also been observed anec-dotally in clinical cases (Denis J. Marcellin-Little, 2007,personal communication). Because of the paucity of in-formation available, it is uncertain whether CVWO hasany clinically relevant benefit over other tibial plateauleveling procedures.
TTO
TTO, like TTA, is a procedure that aims to result in aproximal tibial conformation so that the patellar tendonis oriented perpendicular to the tibial plateau when thestifle is at a weight-bearing angle.22 First, a partial frontalplane osteotomy of the tibial tuberosity is made, leavingthe distal cortex intact. A partial wedge ostectomy, with a
Fig 8. Position of the osteotomies and postoperative illustra-
tion of chevron wedge osteotomy.
121KIM ET AL

wedge angle equal to two-thirds of angle between thepatellar tendon and a line perpendicular to the tibial pla-teau slope, is then performed caudal to the tibial tubero-sity osteotomy. Specialized TTO instrumentation iscommercially available to facilitate accurate positioningof the osteotomies. Reduction of the wedge ostectomysite simultaneously reduces the tibial plateau slope andshifts the tibial tuberosity in a cranial direction (Fig 9).Application of a 3.5mm T-plate is recommended to sta-bilize the wedge ostectomy site.
In a prospective clinical study of TTO in 64 dogs with amean follow-up of 15 months, no lameness was observedin most dogs at final examination.22 Significant increasesin thigh circumference and stifle range of motion were alsonoted. All owners assessed their dog as being normal ornear normal for all physical activities except sitting (2%mildly abnormal) and standing (4% mildly abnormal).Complications were encountered in 36% of cases, includ-ing tibial tuberosity fractures, infection, and subsequentmeniscal injury. The most common complication was in-traoperative tibial tuberosity fracture necessitating ten-sion-band wire fixation, which occurred in 23% of dogs.
Proposed advantages of TTO include minimal changeto the orientation of the tibiofemoral articulating surfac-es, a relatively small osteotomy gap caudal to the tibialtuberosity, no loss of limb length, and low technicaldifficulty when the appropriate instrumentation is used.Potential disadvantages include variability of the post-
operative patellar tendon-to-TPA when using the recom-mended calculations, and questionable protective effectsagainst medial meniscal injury.
CONCLUSIONS
By addressing the cranially directed shear force leadingto cranioproximal tibial translation that occurs duringweight-bearing, tibial osteotomy techniques have beenclinically successful in improving pelvic limb function indogs with CrCL insufficiency. Despite their popularity,differences in long-term outcome between tibial osteo-tomies and traditional methods of repair are not appar-ent.64 As highlighted in a recent metaanalysis evaluatingsurgical procedures used in dogs with CrCL insufficiency,this may reflect the lack of objective clinical data report-ed.98 Likewise, the current body of information isinsufficient to validate 1 tibial osteotomy technique overanother. Individual and interbreed differences in mor-phology, kinematics and kinetics may also influence thefinal outcome after surgery, and some osteotomy proce-dures may be more suitable than others in certain breedsof dogs or tibial conformations. Specific indications foreach individual technique remain to be determined. Con-cerns common to all tibial osteotomies for treating CrCLinsufficiency include the sparing effect on the meniscus,the progression of OA after surgery and the correlationbetween clinical outcome and postoperative TPA orpatellar tendon-to-tibial plateau angle. Future clinicalstudies need to adopt reliable, validated and standardizedoutcome measures to permit fair and direct comparisonsbetween the various techniques.
The problems encountered in the surgical managementof CrCL insufficiency are undoubtedly a reflection of thecomplexity of the structure and function of the stifle joint.Future studies should not only focus on the clinical re-sults of different surgical procedures; a clearer under-standing of the biomechanics of the canine stifle and theetiopathogenesis of the disease is also required to deter-mine whether tibial osteotomy techniques are superior toother treatment modalities for managing CrCL insuffi-ciency in dogs.
ACKNOWLEDGMENTS
The authors thank Drs. Jimi L. Cook, Denis J. Marcellin-
Little, Warwick J. Bruce, and Randy J. Boudrieau for their
contributions. The assistance of Tim Vojt in producing the
figures is gratefully acknowledged.
REFERENCES
1. Johnson JA, Austin C, Breur GJ: Incidence of canine ap-
pendicular musculoskeletal disorders in 16 veterinary
Fig 9. Position of the osteotomies and postoperative illustra-
tion of triple tibial osteotomy.
122 TIBIAL OSTEOTOMIES FOR CRANIAL CRUCIATE LIGAMENT INSUFFICIENCY IN DOGS

teaching hospitals from 1980 through 1989. Vet Comp
Orthop Traumatol 7:56–69, 1994
2. Hayashi K, Manley PA, Muir P: Cranial cruciate ligament
pathophysiology in dogs with cruciate disease: a review.
J Am Anim Hosp Assoc 40:385–390, 2004
3. Doverspike M, Vasseur PB, Harb MF, et al: Contralateral
cranial cruciate ligament rupture: incidence in 114 dogs. J
Am Anim Hosp Assoc 29:167–170, 1993
4. Wilke VL, Robinson DA, Evans RB, et al: Estimate of the
annual economic impact of treatment of cranial cruciate
ligament injury in dogs in the United States. J Am Vet Med
Assoc 227:1604–1607, 2005
5. Pond MJ, Campbell JR: The canine stifle joint: I. Rupture of
the anterior cruciate ligament: An Assessment of conserva-
tive and surgical treatment. J Small Anim Pract 13:1, 1972
6. Vasseur PD: Clinical results following nonoperative manage-
ment for rupture of the cranial cruciate ligament in dogs.
Vet Surg 13:243–246, 1984
7. Piermattei DL, Flo GL, DeCamp CE: The stifle joint, in
Piermattei DL, Flo GL, DeCamp CE (eds): Brinker, Pier-
mattei, and Flo’s Handbook of Small Animal Orthopedics
and Fracture Repair (ed 4). Philadelphia, PA, Saunders,
2006, pp 562–632
8. Flo GL: Modification of the lateral retinacular imbrication
technique for stabilizing cruciate ligament injuries. J Am
Anim Hosp Assoc 11:570–576, 1975
9. Gambardella PC, Wallace LJ, Cassidy F: Lateral suture
technique for management of anterior cruciate ligament
rupture in dogs: a retrospective study. J Am Anim Hosp
Assoc 17:33–38, 1981
10. Smith GK, Torg JS: Fibular head transposition for repair of
cruciate-deficient stifle in the dog. J Am Vet Med Assoc
187:375–383, 1985
11. Arnoczky SP, Tarvin GB, Marshall JL, et al: The over-the-
top procedure: a technique for anterior cruciate ligament
substitution in the dog. J Am Anim Hosp Assoc 15:283–
290, 1979
12. Curtis RJ, Delee JC, Drez DJ: Reconstruction of the anterior
cruciate ligament with freeze dried fascia lata allografts in
dogs. A preliminary report. Am J Sports Med 13:408–14,
1985
13. Denny HR, Goodship AE: Replacement of the anterior
cruciate ligament with carbon fibre in the dog. J Small
Anim Prac 21:279–286, 1980
14. Mullen HS, Matthiesen DT: Complications of transposition
of the fibular head for stabilization of the cranial cruciate-
deficient stifle in dogs: 80 cases (1982–1986). J Am Vet Med
Assoc 195:1267–1271, 1989
15. Elkins AD, Pechman R, Kearney MT, et al: A retrospective
study evaluating the degree of degenerative joint diseases in
the stifle joint of dogs following surgical repair of anterior
cruciate ligament rupture. J Am Anim Hosp Assoc 27:
533–540, 1991
16. Chauvet AE, Johnson AL, Pijanowski GK, et al: Evaluation
of fibular head transposition, lateral fabellar suture, and
conservative treatment of cranial cruciate ligament rupture
in large dogs: a retrospective study. J Am Anim Hosp As-
soc 32:247–255, 1996
17. Vasseur PB, Berry CR: Progression of stifle osteoarthrosis
following reconstruction of the cranial cruciate ligament in
21 dogs. J Am Anim Hosp Assoc 28:129–136, 1992
18. Slocum B, Devine T: Cranial tibial wedge osteotomy: a
technique for eliminating cranial tibial thrust in cranial
cruciate ligament repair. J Am Vet Med Assoc 184:564–
569, 1984
19. Slocum B, Slocum TD: Tibial plateau leveling osteotomy
for repair of cranial cruciate ligament rupture in the
canine. Vet Clin North Am Small Anim Pract 23:777–795,
1993
20. Talaat MB, Kowaleski MP, Boudrieau RJ: Combination
tibial plateau leveling osteotomy and cranial closing wedge
osteotomy of the tibia for the treatment of cranial cruciate
ligament-deficient stifles with excessive tibial plateau angle.
Vet Surg 35:729–739, 2006
21. Damur DM, Tepic S, Montavon PM: Proximal tibial osteo-
tomy for the repair of cranial cruciate-deficient stifle joints
in dogs. Vet Comp Orthop Traumatol 16:211–216, 2003
22. Bruce WJ, Rose A, Tuke J, et al: Evaluation of the triple tibial
osteotomy (TTO): a new technique for the management of
the canine cruciate-deficient stifle. Proceedings, European
Society of Veterinary Orthopaedics and Traumatology
Congress, Munich, Germany, pp. 214–215, 2006 (abstract).
23. Hildreth BE, Marcellin-Little DJ, Roe SC, et al: In vitro
evaluation of five canine tibial plateau leveling methods.
Am J Vet Res 67:693–700, 2006
24. Montavon PM, Damur DM, Tepic S: Advancement of the
tibial tuberosity for the treatment of cranial cruciate deficient
canine stifle. Proceedings, 1st World Orthopedic Veterinary
Congress, Munich, Germany, p. 152, 2002 (abstract).
25. Watt PR: Tibial wedge osteotomy for treatment of cranial
cruciate rupture. Vet Surg 29:478, 2000 (abstract)
26. Hoffman DE, Miller JM, Ober CP, et al: Tibial tuberosity
advancement in 65 canine stifles. Vet Comp Orthop Trau-
matol 19:219–227, 2006
27. Pond MJ, Nuki G: Experimentally-induced osteoarthritis in
the dog. Ann Rheum Dis 32:387–388, 1973
28. Tepic S, Damur DM, Montavon PM: Biomechanics of the
stifle joint. Proceedings, 1st World Orthopaedic Veterinary
Congress, Munich, Germany, pp 189–190, 2002 (abstract).
29. Arnoczky SP, Marshall JL: The cruciate ligaments of the ca-
nine stifle: an anatomical and functional analysis. Am J Vet
Res 38:1807–1814, 1977
30. Korvick DL, Pijanowski GJ, Schaeffer DJ: Three-dimension-
al kinematics of the intact and cranial cruciate ligament-
deficient stifle of dogs. J Biomech 27:77–87, 1994
31. Tashman S, Anderst W, Kolowich P, et al: Kinematics of the
ACL-deficient canine knee during gait: serial changes over
two years. J Orthop Res 22:931–941, 2004
32. Slocum B, Devine T: Cranial tibial thrust: a primary force in
the canine stifle. J Am Vet Med Assoc 183:456–459, 1983
33. Vasseur PB, Arnoczky SP: Collateral ligaments of the canine
stifle joint: anatomic and functional analysis. Am J Vet Res
42:1133–1137, 1981
34. Pozzi A, Kowaleski MP, Apelt D, et al: Effect of medial
meniscal release on tibial translation after tibial plateau
leveling osteotomy. Vet Surg 35:486–494, 2006
123KIM ET AL

35. Bull AM, Amis AA: The pivot-shift phenomenon: a clinical
and biomechanical perspective. Knee 5:141–158, 1998
36. Limbird TJ, Shiavi R, Frazer M, et al: EMG profiles of knee
joint musculature during walking: changes induced by an-
terior cruciate ligament deficiency. J Orthop Res 6:630–
638, 1988
37. Holden JP, Grood ES, Korvick DL, et al: In vivo forces in
the anterior cruciate ligament: direct measurements during
walking and trotting in a quadruped. J Biomech 27:517–
526, 1994
38. Henderson RA, Milton JL: The tibial compression mecha-
nism: a diagnostic aid in stifle injuries. J Am Anim Hosp
Assoc 14:474–479, 1978
39. Reif U, Probst CW: Comparison of tibial plateau angles in
normal and cranial cruciate deficient stifles of Labrador
retrievers. Vet Surg 32:385–389, 2003
40. Wilke VL, Conzemius MG, Besancon MF, et al: Comparison
of tibial plateau angle between clinically normal grey-
hounds and labrador retrievers with and without rupture of
the cranial cruciate ligament. J Am Vet Med Assoc
221:1426–1429, 2002
41. Morris E, Lipowitz AJ: Comparison of tibial plateau angles
in dogs with and without cranial cruciate ligament injuries.
J Am Vet Med Assoc 218:363–366, 2001
42. Warzee CC, Dejardin LM, Arnoczky SP, et al: Effect of tibial
plateau leveling on cranial and caudal tibial thrusts in
canine cranial cruciate-deficient stifles: an in vitro experi-
mental study. Vet Surg 30:278–286, 2001
43. Reif U, Hulse DA, Hauptman JG: Effect of tibial plateau
leveling on stability of the canine cranial cruciate-deficient
stifle joint: an in vitro study. Vet Surg 31:147–154, 2002
44. Griffin JR, Vogrin TM, Zantop T, et al: Effects of increasing
tibial slope on the biomechanics of the knee. Am J Sports
Med 32:376–382, 2004
45. Dennler R, Kipfer NM, Tepic S, et al: Inclination of the
patellar ligament in relation to flexion angle in stifle joints
of dogs without degenerative joint disease. Am J Vet Res
67:1849–1854, 2006
46. Bailey CJ, Smith BA, Black AP: Geometric implications of
tibial wedge osteotomies. Proceedings, 30th Annual Con-
ference of the Veterinary Orthopedic Society, Steamboat
Springs, CO, p. 60, 2003 (abstract).
47. Apelt D, Kowaleski MP, Pozzi A, et al: The effect of tibial
closing wedge angle on cranial tibial subluxation. Proceed-
ings, 32nd Annual Conference of the Veterinary Orthope-
dic Society, Snowmass, CO, p. 3, 2005 (abstract).
48. Kowaleski MP, McCarthy RJ: Geometric analysis evaluating
the effect of tibial plateau leveling osteotomy position on
postoperative tibial plateau slope. Vet Comp Orthop Trau-
matol 17:30–34, 2004
49. Macias C, McKee WM, May C: Caudal proximal tibial de-
formity and cranial cruciate ligament rupture in small-
breed dogs. J Small Anim Pract 43:433–438, 2002
50. Selmi AL, Padilha Filho JG: Rupture of the cranial cruciate
ligament associated with deformity of the proximal tibia in
five dogs. J Small Anim Pract 42:390–393, 2001
51. Read RA, Robins GM: Deformity of the proximal tibia in
dogs. Vet Rec 111:295–298, 1982
52. Osmond CS, Marcellin-Little DJ, Harrysson OL, et al: Mo-
rphometric assessment of the proximal portion of the tibia
in dogs with and without cranial cruciate ligament rupture.
Vet Radiol Ultrasound 47:136–141, 2006
53. Holsworth IG: Clinical comparison of TPLO vs tibial closing
wedge osteotomy. Proceedings, 12th European Society of
Veterinary Orthopaedics and Traumatology, Munich, Ger-
many, p. 62, 2004 (abstract).
54. Dejardin LM: Tibial plateau leveling osteotomy, in Slatter D
(ed): Textbook of Small Animal Surgery (ed 3, Vol. 2.
Philadelphia, PA, Saunders, 2003, pp 2133–2143
55. Kowaleski MP, Apelt D, Mattoon JS, et al: The effect of tibial
plateau leveling osteotomy position on cranial tibial sub-
luxation: an in vitro study. Vet Surg 34:332–336, 2005
56. Wheeler JL, Cross AR, Gingrich W: In vitro effects of osteo-
tomy angle and osteotomy reduction on tibial angulation
and rotation during the tibial plateau-leveling osteotomy
procedure. Vet Surg 32:371–377, 2003
57. Kergosien DH, Barnhart MD, Kees CE, et al: Radiographic
and clinical changes of the tibial tuberosity after tibial pla-
teau leveling osteotomy. Vet Surg 33:468–474, 2004
58. Shahar R, Milgram J: Biomechanics of tibial plateau leveling
of the canine cruciate-deficient stifle joint: a theoretical
model. Vet Surg 35:144–149, 2006
59. Williams A, Logan M: Understanding tibio-femoral motion.
Knee 11:81–88, 2004
60. Robinson DA, Mason DR, Evans R, et al: The effect of tibial
plateau angle on ground reaction forces 4–17 months after
tibial plateau leveling osteotomy in labrador retrievers. Vet
Surg 35:294–299, 2006
61. Schwarz PD: Tibial plateau leveling osteotomy (TPLO): a
prospective clinical comparative study. Proceedings of the
9th American College of Veterinary Surgeons Symposium,
San Francisco, CA, p. 379, 1999 (abstract).
62. Barnhart MD: Results of single-session bilateral tibial plateau
leveling osteotomies as a treatment for bilaterally ruptured
cranial cruciate ligaments in dogs: 25 cases (2000–2001). J
Am Anim Hosp Assoc 39:573–578, 2003
63. Ballagas AJ, Montgomery RD, Henderson RA, et al: Pre- and
postoperative force plate analysis of dogs with experimen-
tally transected cranial cruciate ligaments treated using tib-
ial plateau leveling osteotomy. Vet Surg 33:187–190, 2004
64. Conzemius MG, Evans RB, Besancon MF, et al: Effect of
surgical technique on limb function after surgery for rup-
ture of the cranial cruciate ligament in dogs. J Am Vet Med
Assoc 226:232–236, 2005
65. Rayward RM, Thomson DG, Davies JV, et al: Progression
of osteoarthritis following TPLO surgery: a prospective
radiographic study of 40 dogs. J Small Anim Pract 45:92–
97, 2004
66. Lazar TP, Berry CR, deHaan JJ, et al: Long-term radio-
graphic comparison of tibial plateau leveling osteotomy
versus extracapsular stabilization for cranial cruciate liga-
ment rupture in the dog. Vet Surg 34:133–141, 2005
67. Gordon WJ, Conzemius MG, Riedesel E, et al: The rela-
tionship between limb function and radiographic
osteoarthrosis in dogs with stifle osteoarthrosis. Vet Surg
32:451–454, 2003
124 TIBIAL OSTEOTOMIES FOR CRANIAL CRUCIATE LIGAMENT INSUFFICIENCY IN DOGS

68. Priddy NH, Tomlinson JL, Dodam JR, et al: Complications
with and owner assessment of the outcome of tibial plateau
leveling osteotomy for treatment of cranial cruciate liga-
ment rupture in dogs: 193 cases (1997–2001). J Am Vet
Med Assoc 222:1726–1732, 2003
69. Pacchiana PD, Morris E, Gillings SL, et al: Surgical and
postoperative complications associated with tibial plateau
leveling osteotomy in dogs with cranial cruciate ligament
rupture: 397 cases (1998–2001). J Am Vet Med Assoc
222:184–193, 2003
70. Stauffer KD, Tuttle TA, Elkins AD, et al: Complications
associated with 696 tibial plateau leveling osteotomies
(2001–2003). J Am Anim Hosp Assoc 42:44–50, 2006
71. Carey K, Aiken SW, DiResta GR, et al: Radiographic and
clinical changes of the patellar tendon after tibial plateau
leveling osteotomy 94 cases (2000–2003). Vet Comp Ort-
hop Traumatol 18:235–242, 2005
72. Mattern KL, Berry CR, Peck JN, et al: Radiographic and
ultrasonographic evaluation of the patellar ligament
following tibial plateau leveling osteotomy. Vet Radiol
Ultrasound 47:185–191, 2006
73. Flo GL: Meniscal injuries. Vet Clin North Am Small Anim
Pract 23:831–843, 1993
74. Metelman LA, Schwarz PD, Salman M, et al: An evalua-
tion of three different cranial cruciate ligament surgical
stabilization procedures as they relate to postoper-
ative meniscal injuries. Vet Comp Orthop Traumatol 8:
118–123, 1995
75. Pozzi A, Litsky A, Field JR, et al: Meniscal release impairs
load transmission and joint stability in the canine stifle. Vet
Comp Orthop Traumatol 2:A36, 2005 (abstract).
76. Matis U, Brahm-Jorda T, Jorda C, et al: Radiographic eval-
uation of the progression of osteoarthritis after tibial pla-
teau leveling osteotomy in 93 dogs. Proceedings, 12th
European Society of Veterinary Orthopaedics and Trau-
matology, Munich, Germany, p. 250, 2004 (abstract).
77. Thieman KM, Tomlinson JL, Fox DB, et al: Effect of men-
iscal release on rate of subsequent meniscal tears and own-
er-assessed outcomes in dogs with cruciate disease treated
with tibial plateau leveling osteotomy. Vet Surg 35:705–
710, 2006
78. Jackson J, Vasseur PB, Griffey S, et al: Pathologic changes in
grossly normal menisci in dogs with rupture of the cranial
cruciate ligament. J Am Vet Med Assoc 218:1281–1284,
2001
79. Pozzi A, Hildreth BE, Rajala-Schultz PJ: Comparison of ar-
throscopy and arthrotomy for the diagnosis of meniscal
pathology: an in vitro study. Proceedings of the 34th An-
nual Conference Veterinary Orthopaedic Society, Sun Val-
ley, ID, p. 48, 2007 (abstract).
80. Boudrieau RJ, McCarthy RJ, Sisson RD Jr: Sarcoma of the
proximal portion of the tibia in a dog 5.5 years after tibial
plateau leveling osteotomy. J Am Vet Med Assoc
227:1613–1617, 2005. Comment in: J Am Vet Med Assoc.
2006 Jan 15;228(2):194–5; author reply 195
81. Boudrieau RJ, McCarthy RJ, Sprecher CM, et al: Material
properties of and tissue reaction to the Slocum TPLO
plate. Am J Vet Res 67:1258–1265, 2006
82. Charles AE, Ness MG: Crevice corrosion of implants recov-
ered after tibial plateau leveling osteotomy in dogs. Vet
Surg 35:438–444, 2006
83. Crooks R, Lackowski B, Vasilyeva Y, et al: Material analysis
of the Slocum TPLO bone plate. Proceedings of the 32nd
Annual Conference Veterinary Orthopaedic Society, Snow-
mass, CO, p. 55, 2005 (abstract).
84. Wolke RE, Nielsen SW: Site incidence of canine osteosarco-
ma. J Small Anim Pract 7:489–492, 1966
85. Vasseur PB, Levy J, Dowd E, et al: Surgical wound infection
rates in dogs and cats. Data from a teaching hospital. Vet
Surg 17:60–64, 1988
86. Papagelopoulos PJ, Partsinevelos AA, Themistocleous GS, et
al: Complications after tibial plateau fracture surgery. In-
jury 37:475–484, 2006
87. Harris LG, Richards RG: Staphylococci and implant surfac-
es: a review. Injury 37(Suppl 2): S3–S14, 2006
88. Apelt D, Kowaleski MP, Boudrieau RJ: Effect of tibial
tuberosity advancement on cranial tibial subluxation in
canine cranial cruciate deficient stifle joints: an in vitro
experimental study. Vet Surg 36:170–177, 2007
89. Shirazi-Adl A, Mesfar W: Effect of tibial tubercle elevation
on biomechanics of the entire knee joint under muscle
loads. Clin Biomech 22:344–351, 2007
90. Nakamura N, Ellis M, Seedhom BB: Advancement of the
tibial tuberosity. A biomechanical study. J Bone Joint Surg
Br 67:255–260, 1985
91. Maquet P: Advancement of the tibial tuberosity. Clin Orthop
Relat Res 115:225–230, 1976
92. Damur DM: Tibial tuberosity advancement: clinical results.
Proceedings of the 15th Annual American College of Vet-
erinary Surgeons Symposium, San Diego, CA, pp 441–442,
2005 (abstract).
93. Boudrieau RJ: Tibial tuberosity advancement (TTA): clinical
results. Proceedings of the 15th Annual American College
of Veterinary Surgeons Symposium, San Diego, CA, pp
443–445, 2005 (abstract).
94. Fitzpatrick N, Yeadon R, Kowaleski M: Tibial tuberosity
transposition-advancement for treatment of medial patellar
luxation and concomitant cranial cruciate ligament disease
in the dog. Proceedings of the 34th Annual Conference
Veterinary Orthopaedic Society, Sun Valley, ID, p. 68,
2007 (abstract).
95. Jerram RM, Walker AM, Warman CG: Proximal tibial in-
traarticular ostectomy for treatment of canine cranial
cruciate ligament injury. Vet Surg 34:196–205, 2005
96. Lineberger JA, Allen DA, Wilson ER, et al: Comparison of
radiographic arthritic changes associated with two varia-
tions of tibial plateau leveling osteotomy. Vet Comp Ort-
hop Traumatol 18:13–17, 2005
97. Hoelzler MG, Millis DL, Francis DA, et al: Results of ar-
throscopic versus open arthrotomy for surgical manage-
ment of cranial cruciate ligament deficiency in dogs. Vet
Surg 33:146–153, 2004
98. Aragon CL, Budsberg SC: Applications of evidence-based
medicine: cranial cruciate ligament injury repair in the dog.
Vet Surg 34:93–98, 2005
125KIM ET AL