Embed Size (px)
DESCRIPTION
PANCREAS INSUFFICIENCY. Lipase. Bile acids (Conc. >CMC). Micelles. Fatty acid or monoglyceride. Polar end of bile acid. Hydroxyl groups of bile acids. Bile acid. HUMAN PANCREATIC LIPASE. Interfacial enzyme,active in the lipid-water interface - PowerPoint PPT Presentation
Citation preview

PANCREAS INSUFFICIENCY

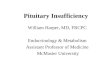
Fatty acid or monoglyceridePolar end of bile acidHydroxyl groups of bile acidsBile acid
Bile acids(Conc. >CMC)Micelles
Lipase

HUMAN PANCREATIC LIPASE Interfacial enzyme,active in the lipid-
water interface Dependent on clean interface for lipolysis Colipase binds to lipase in presence of
bile salts Lipase is specific for primary esterbond Lipase is rapidly and irreversibly
inactivated at pH<4

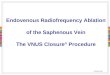
Chylomicron Formation and Secretion
NucleusNucleus
Granular-Granular-endoplasmicreticulumendoplasmicreticulum
MitochondriaMitochondria
EsterificationEsterificationSurfaceSurfacestabilizationstabilizationAddition ofAddition oflipoproteinlipoprotein
ChylomicronChylomicronformationformation
Uptake fromUptake frommicellar solutionmicellar solutionFA and MGFA and MG
Secretion viaSecretion viaintercellular spacesintercellular spacesinto lactealsinto lacteals
Golgi materialGolgi material

Pancreatic Exocrine Function Normal post-prandial pancreatic secretion is ±70% of maximal
secretory capacity or 4–5 times the basal rate Post-prandial secretion lasts for about 4 hours Total intraduodenal lipase output varies from
300,000 to 500,000 U/meal Minimum pancreatic function of 10% of normal is necessary for
adequate lipid digestion, correspondingto ± 30,000–50,000 U lipase in the duodenum
Amount of lipase, to be added to meals, varies depending upon degree in insufficiency and degree of gastric/duodenal denaturation

Pancreatic Exocrine Insufficiency Steatorrhea (mild:7–10 g/d; moderate: 10–
20 g/d; severe: >20 g/d) Bile salt precipitation due to low duodenal
pH (bicarbonate deficiency)→increased fecal bile salt loss
Impaired CCK and GIP release→sluggish gallbladder emptying
Malabsorption of lipid-soluble vitamins,cholesterol

SYMPTOMATOLOGY OF EXOCRINE PANCREATIC INSUFFICIENCY Steatorrhea and creatorrhea causes -Abdominal complaints
-bloating,pain,cramps-urgency,diarrhea,foul smelling stools
-Generalised symptoms-weight loss -fatigue,loss of energy-sympoms related to vitamin deficiencies

Exocrine Pancreatic InsufficiencyDiagnosis
• Suspicion because of associated medical condition and: clinical history of steatorrhea weight loss
• Laboratory tests fat balance test (not specific) non-invasive pancreatic function test
• fecal elastase, fecal chymotrypsin, PABA test invasive direct pancreatic function test (gold standard)
• secretin test

Indications for Pancreatic Enzyme Therapy
Exocrine pancreatic insufficiency causing–any moderate / severe steatorrhea–any steatorrhea with weight loss–chronic / watery diarrhea–dyspeptic symptoms
Unrelenting pain in chronic pancreatitis(inhibition of pancreatic secretory drive by negative feedback) (non-enteric coated preparations)

Pancreatic Enzyme PreparationsNon-Enteric Coated PreparationsPancreatin powder / granulate blends well with food unpalatable denaturation in acid / peptic milieu hyperuricosuriaPancreatin tablet / capsule inadequate dispersion into the meal neutral taste denaturation in acid / peptic milieu

Pancreatic Enzyme PreparationsEnteric Coated PreparationsEnteric-coated tablet / capsule (dissolving at pH >5) prolonged gastric retention causing de-synchronisation failed or delayed dissolution when duodenal pH is low (lack
of bicarbonate)
Enteric-coated microspheres (dissolving at pH >5) premature gastric dissolution when pH >5 during early
phase of meal delayed gastric emptying of particles >1.4 mm failed or delayed dissolution when duodenal pH is low

Enteric Coated Mini-Doses PreparationGalenic aspects
gelatin capsule
pancreatin
pH dependent enteric coated layer

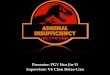
Creon 8,000 9,000 450 1.4 (1.2–1.7)Pancrease 5,000 2,900 330 2.0 (1.7–2.2)Panzytrat 25,000 22,500 1,250 2.0Creon forte 25,000 18,000 1,000 1.4 (1.2–1.8)
Lipase Amylase Protease sphere diam.
Microsphere Pancreatic Enzyme Preparations
microspheres larger than 1.4 mm empty more slowly than solid phase of the meal
release of enzymes from microspheres is slow, depending upon pH and ionic strength of medium

Pancreatic Enzyme PreparationsCourse of dissolution of enteric oat
0102030405060708090
100
5,0 5.2 5.4 5.6 5.8 6.0
CreonCreon FortePancreasePancrease HLPanzytrat

• Enzyme supplementation during all meals
• Main meal: 25.000 to 75.000 FIP units lipase of EC preparation
• In-between snacks: 5.000 to 25.000 FIP lipase of EC preparation
• Dosage should be adjusted for individual patient
• Addition of H2-receptor blocker or protonpump inhibitor
Pancreatic Enzyme PreparationsDosage recommendations

Pancreatic Exocrine InsufficiencyDietary recommendations
Abstinence from alcohol In principle NO limitation of fat content of food (<60 g/d)
(unpalatable; risk of deficit of essential fatty acids e.g. linoleic acid) except therapy failure
Frequent small meals Reduction in fiber content (fiber inhibits
pancreatic enzymes) Medium chain triglycerides (C6-C12)
(80–120 g/d) in case of insufficiently corrected steatorrhea and weight loss

Therapy of Pancreatic InsufficiencyTreatment failure
• Acid related– inactivation of lipase– precipitation of bile salts– enteric coat dissolves too distally
• Related to the use of medication– too low dose– noncompliance– incorrect timing or mode of ingestion
• False diagnosis or concomitant disease– celiac disease– bacterial overgrowth