Embed Size (px)
Citation preview
Thrombose-Prophylaxe und OAK 2011
Scuol 4.9.11
0920-0945
JH Beer

Zukunft: Individualisierte und auf den Pat.
massgeschneiderte Antikoagulation
•Dabigatran-Pradaxa
•Rivaroxaban-Xarelto
•Apixaban-Eliquis
•Edoxaban
•Betrixaban
•Markoumar
•Heparine
•Kombinationen, u.a. mit
•Plättchenhemmern
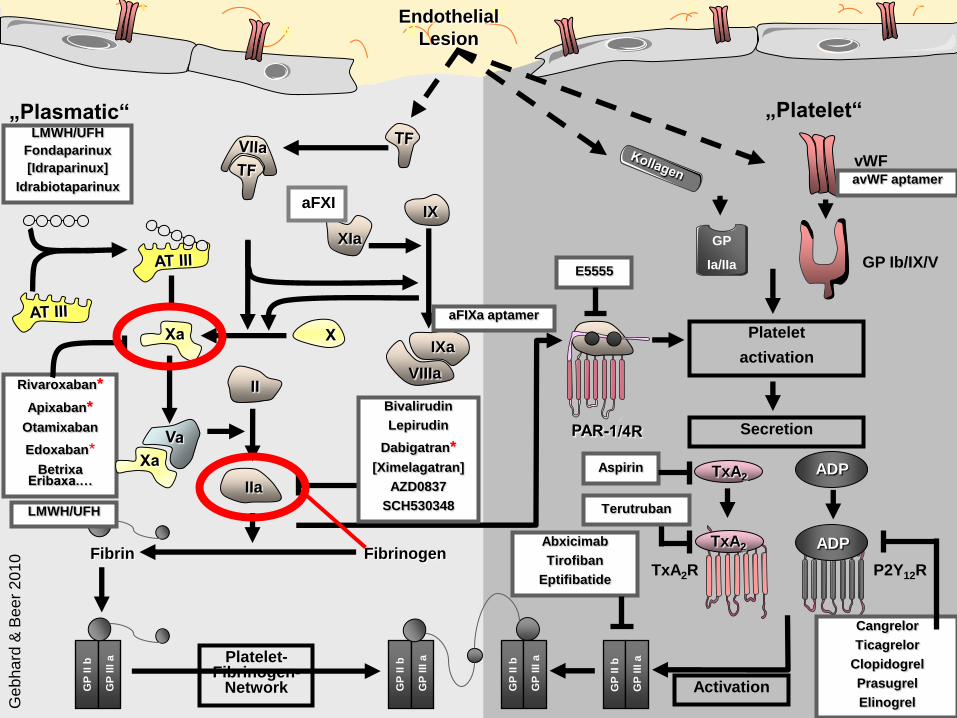
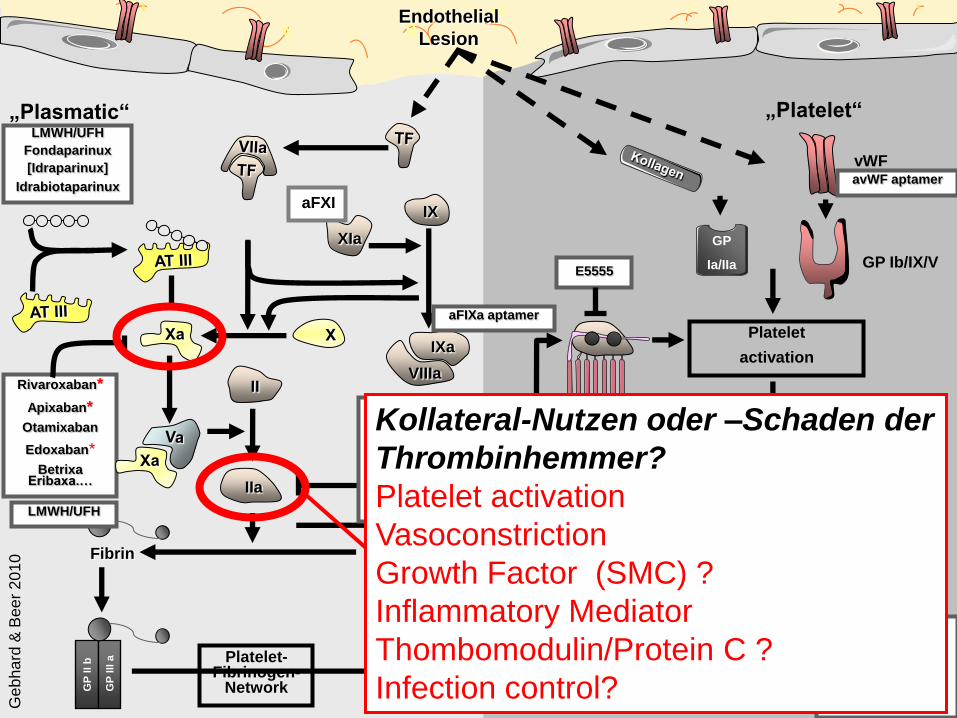
„Plasmatic“ „Platelet“
Rivaroxaban*
Apixaban*
Otamixaban
Edoxaban*
Betrixa Eribaxa.…
vWF
ADP
LMWH/UFH
Fondaparinux
[Idraparinux]
Idrabiotaparinux
Aspirin
Platelet
activation
Secretion
P2Y12R
TxA2
TxA2R
Endothelial
Lesion
GP
II b
GP
III
a
Activation
Cangrelor
Ticagrelor
Clopidogrel
Prasugrel
Elinogrel
GP
II b
GP
III
a
GP
II b
GP
III
aPlatelet-Fibrinogen-
Network
Fibrin FibrinogenAbxicimab
Tirofiban
Eptifibatide
IX
IXa
VIIIa
XIa
GP
II b
GP
III
a
II
IIa
LMWH/UFH
Bivalirudin
Lepirudin
Dabigatran*
[Ximelagatran]
AZD0837
SCH530348
ADP
TxA2
Terutruban
E5555
GP
Ia/IIa GP Ib/IX/V
Ge
bh
ard
& B
ee
r 2
01
0
aFIXa aptamer
avWF aptamer
aFXI
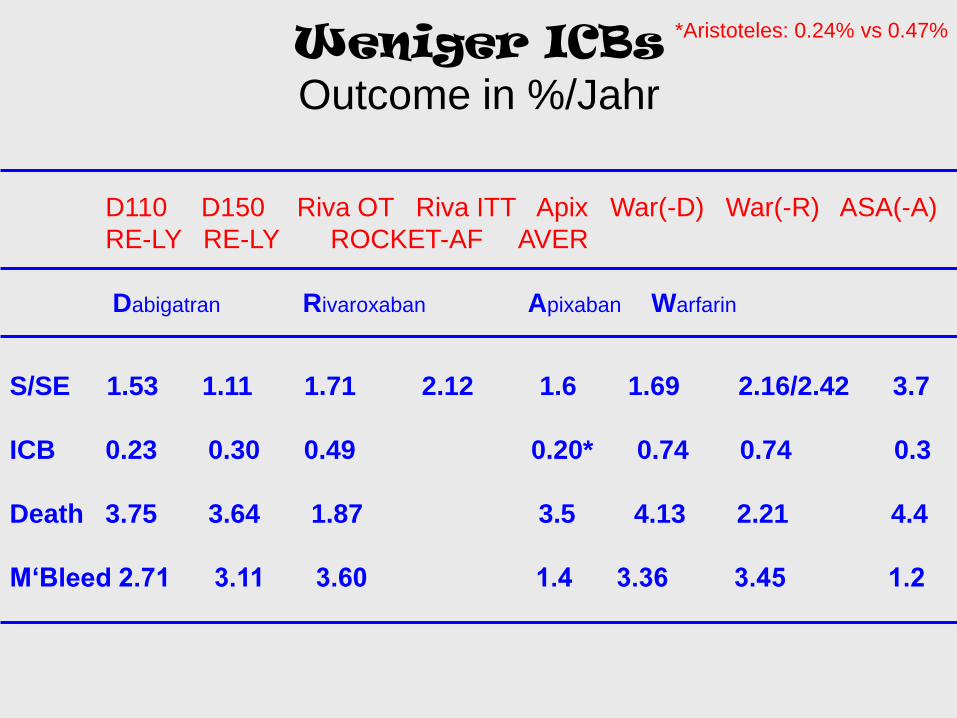
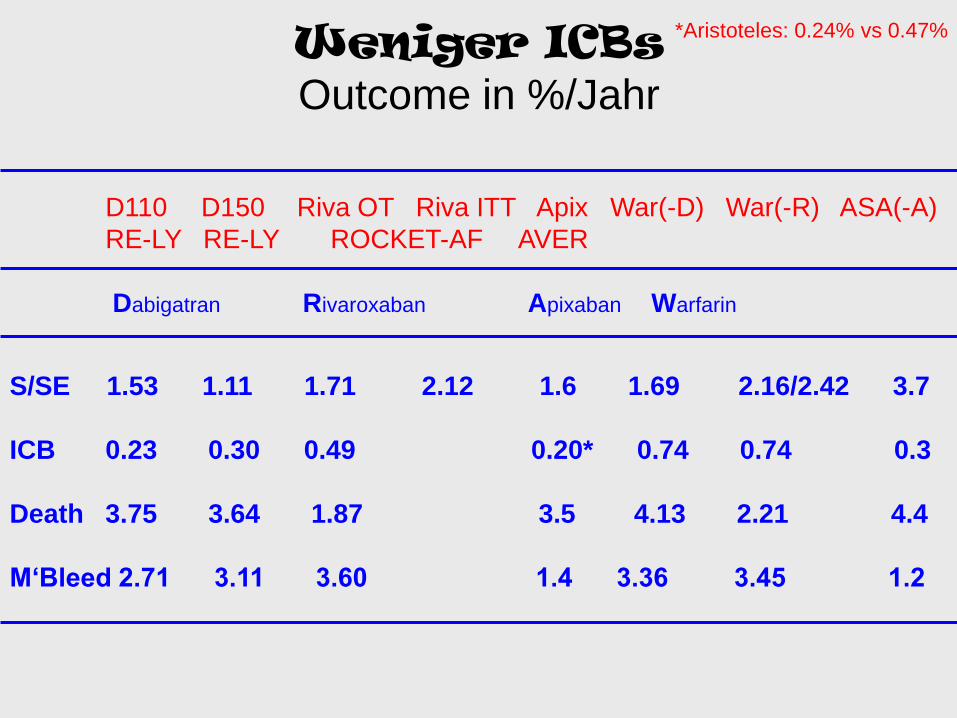
Weniger ICBs Outcome in %/Jahr
D110 D150 Riva OT Riva ITT Apix War(-D) War(-R) ASA(-A)
RE-LY RE-LY ROCKET-AF AVER
Dabigatran Rivaroxaban Apixaban Warfarin
S/SE 1.53 1.11 1.71 2.12 1.6 1.69 2.16/2.42 3.7
ICB 0.23 0.30 0.49 0.20* 0.74 0.74 0.3
Death 3.75 3.64 1.87 3.5 4.13 2.21 4.4
M‘Bleed 2.71 3.11 3.60 1.4 3.36 3.45 1.2
*Aristoteles: 0.24% vs 0.47%

Pharmakologische Eigenschaften neuerer Antikoagulantien
Annu Rev Med 2011; 62:41

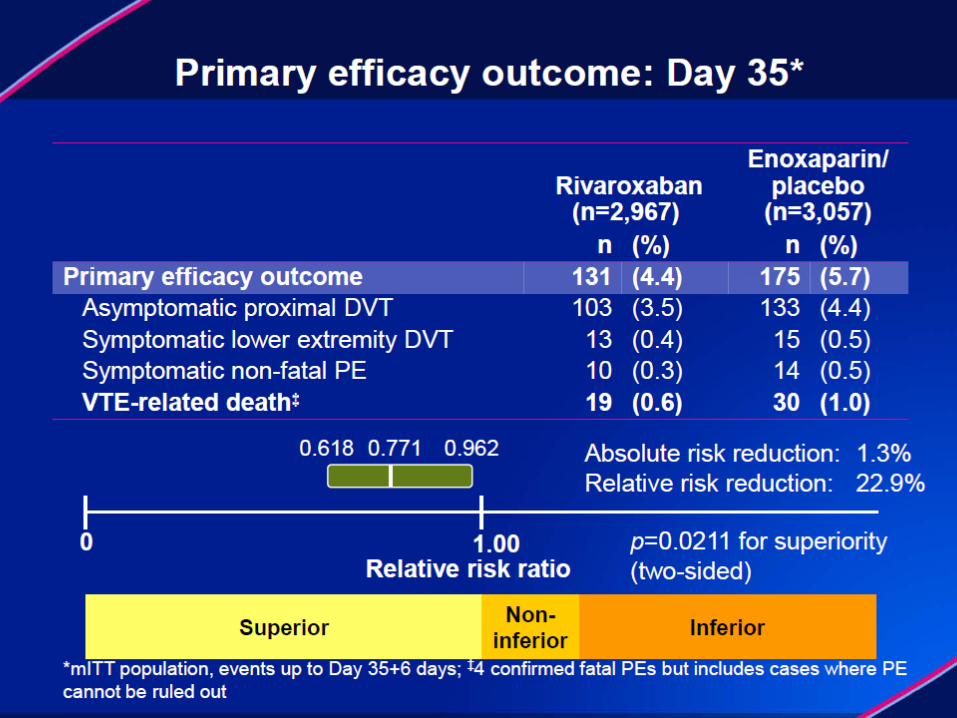
Prophylaxe

Rivaroxaban in der orthopädischen
Chirurgie: 4 Studien zusammengefasst
Symptomatic VTE and
all-cause mortality
Major bleeding
1.3%
0.6%
0.2%0.4%
ARD=–0.8%
p<0.001
ARD=0.2%
p=0.076
13/6,200 24/6,18382/6,200 35/6,183
p-values analyzed using a Cox regression model; safety population, n=12,383
0
0.5
1.0
1.5
2.0
Incid
en
ce
(%)
Enoxaparin regimens
Rivaroxaban regimens
Primary populationfor analysis
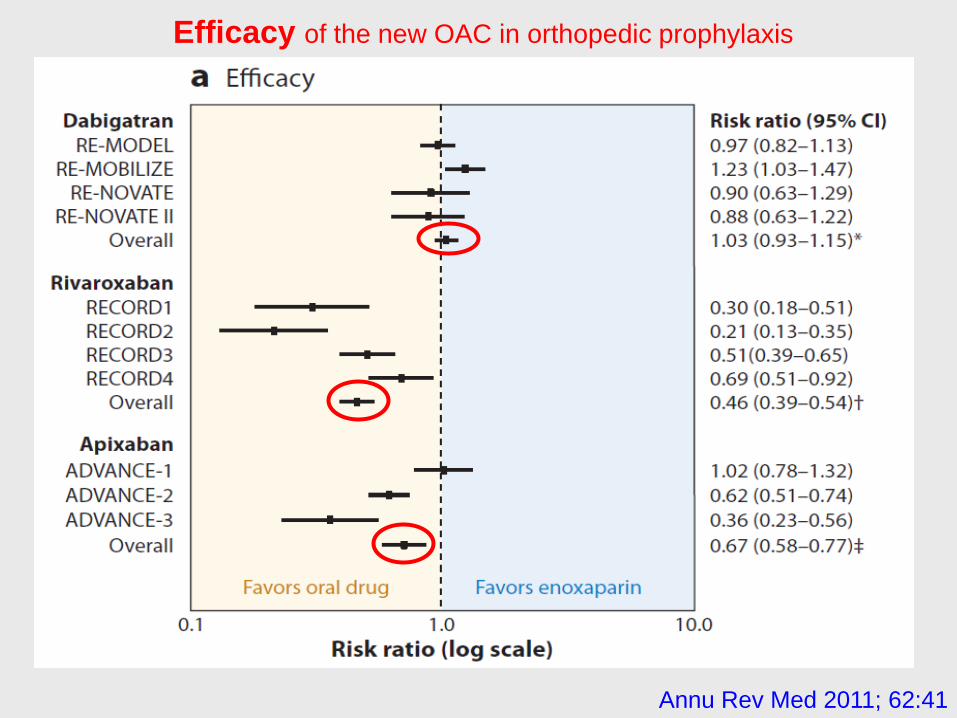
Efficacy of the new OAC in orthopedic prophylaxis
Annu Rev Med 2011; 62:41

Bleeding Risk of the new OAC in orthopedic prophylaxis
Annu Rev Med 2011; 62:41
Kollege D. fragt, ob diese erfolgreiche orthopädische
Prophylaxe auf die multimorbiden medizinischen
Patienten übertragbar sei?
(Magellan)
Fall 2a

TVT
NEJM 2009; 361:2342
Re-Cover: Dabigatran
NEJM 2009; 361:2342
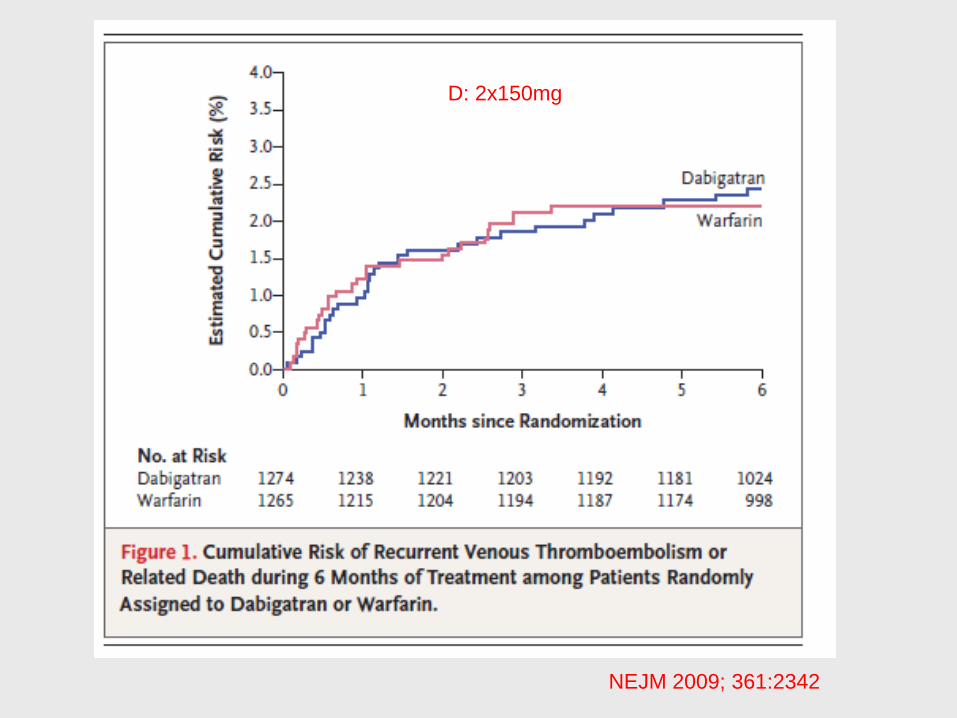
D: 2x150mg

NEJM 2009; 361:2342
NEJM 2010; 363:2495
NEJM 2010; 363:2495
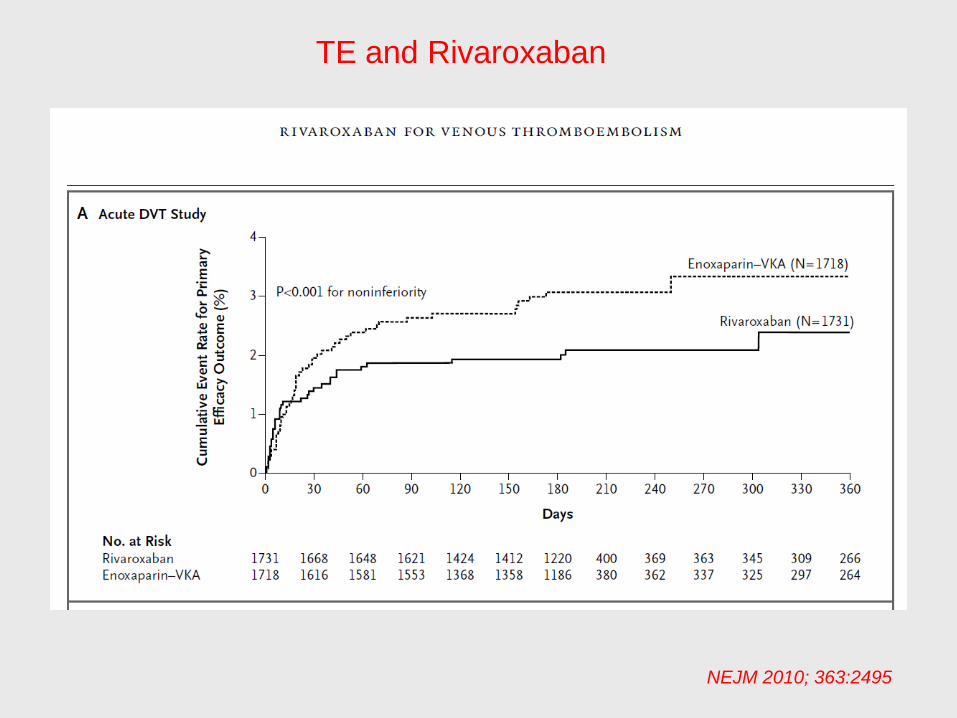
TE and Rivaroxaban

NEJM 2010; 363:2495
Einstein Extension

Einstein-Extension

VHFli

JACC 2010; 56:2067
150 Net difference -0.58%
110 Net difference -0.16%
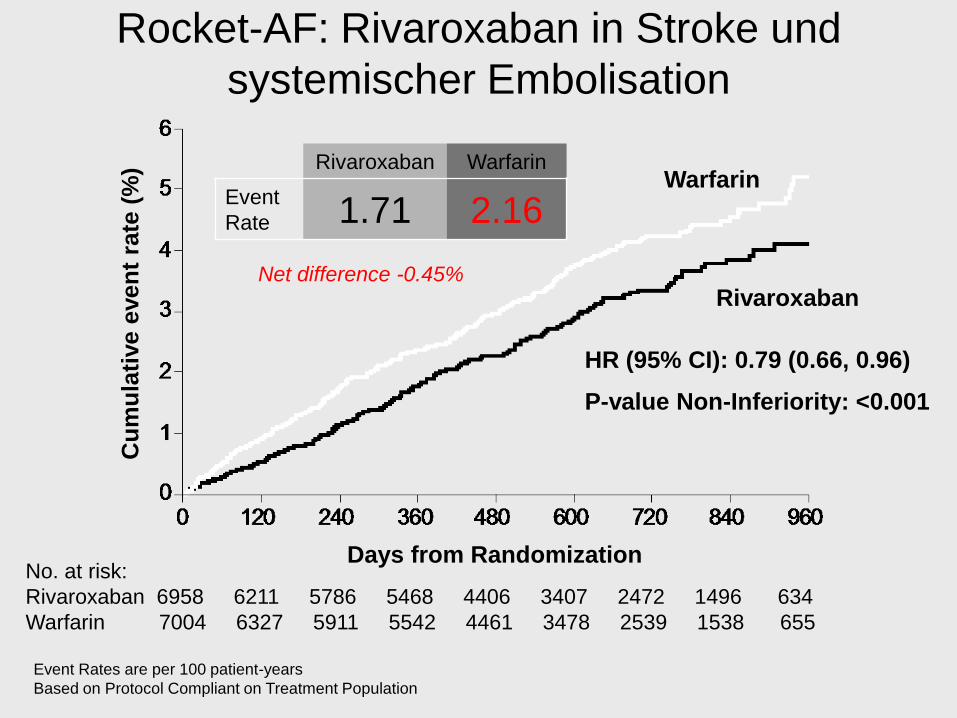
Rocket-AF: Rivaroxaban in Stroke und
systemischer Embolisation
Event Rates are per 100 patient-years
Based on Protocol Compliant on Treatment Population
No. at risk:
Rivaroxaban 6958 6211 5786 5468 4406 3407 2472 1496 634
Warfarin 7004 6327 5911 5542 4461 3478 2539 1538 655
Warfarin
HR (95% CI): 0.79 (0.66, 0.96)
P-value Non-Inferiority: <0.001
Days from Randomization
Cu
mu
lati
ve e
ven
t ra
te (
%)
Rivaroxaban
Rivaroxaban Warfarin
Event
Rate 1.71 2.16
Net difference -0.45%
Rivaroxaban Warfarin
Event
Rate
Event
Rate
HR
(95% CI)P-value
On
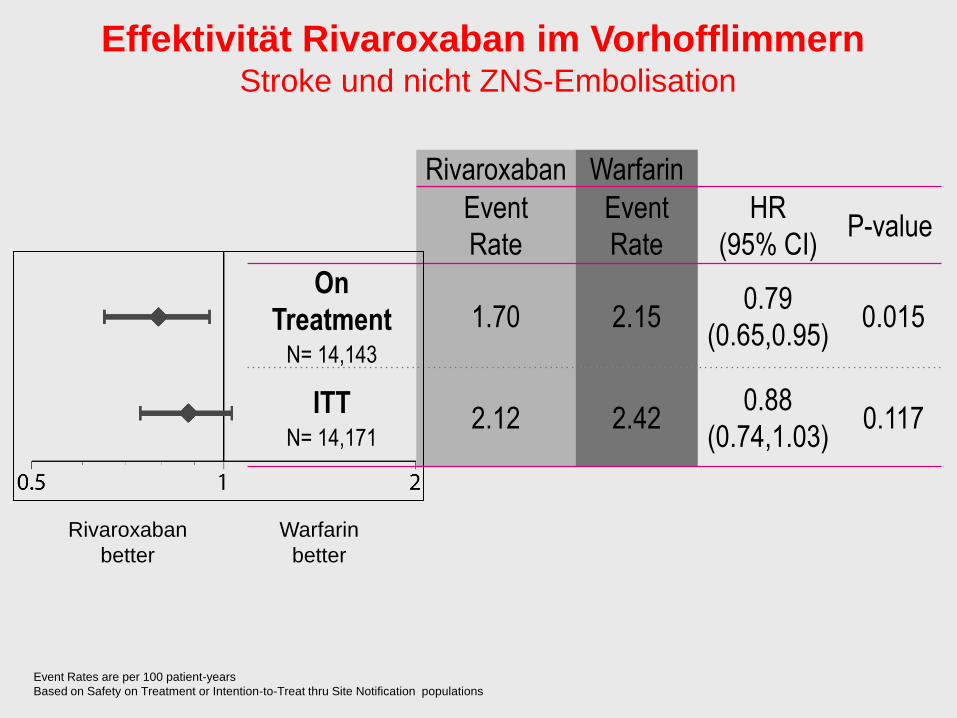
TreatmentN= 14,143
1.70 2.150.79
(0.65,0.95)0.015
ITTN= 14,171
2.12 2.420.88
(0.74,1.03)0.117
Rivaroxaban
better
Warfarin
better
Effektivität Rivaroxaban im VorhofflimmernStroke und nicht ZNS-Embolisation
Event Rates are per 100 patient-years
Based on Safety on Treatment or Intention-to-Treat thru Site Notification populations
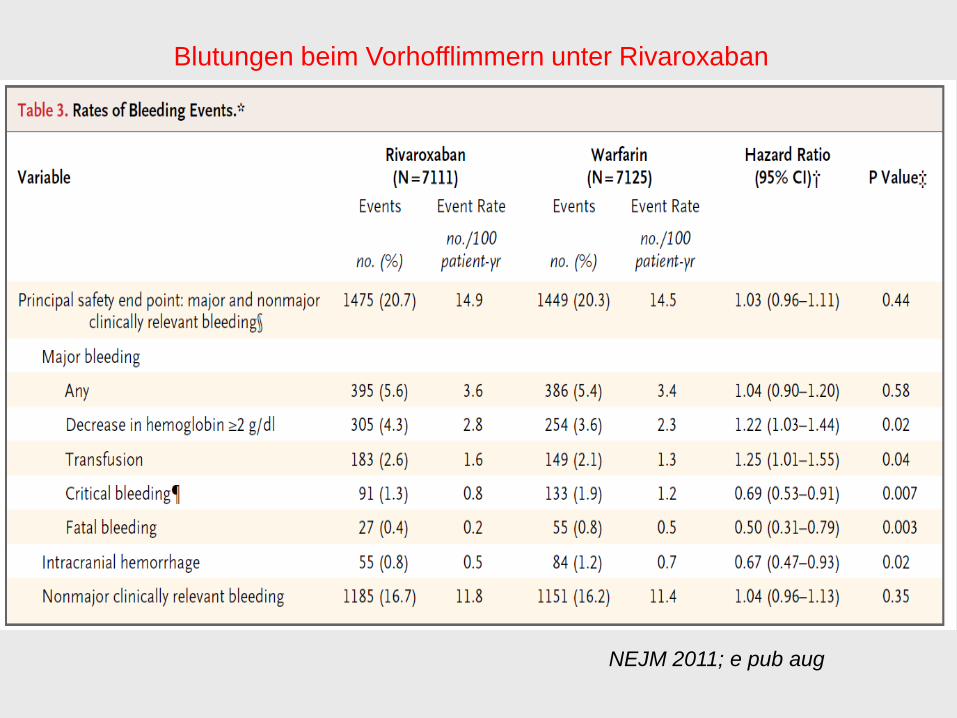
Blutungen beim Vorhofflimmern unter Rivaroxaban
NEJM 2011; e pub aug
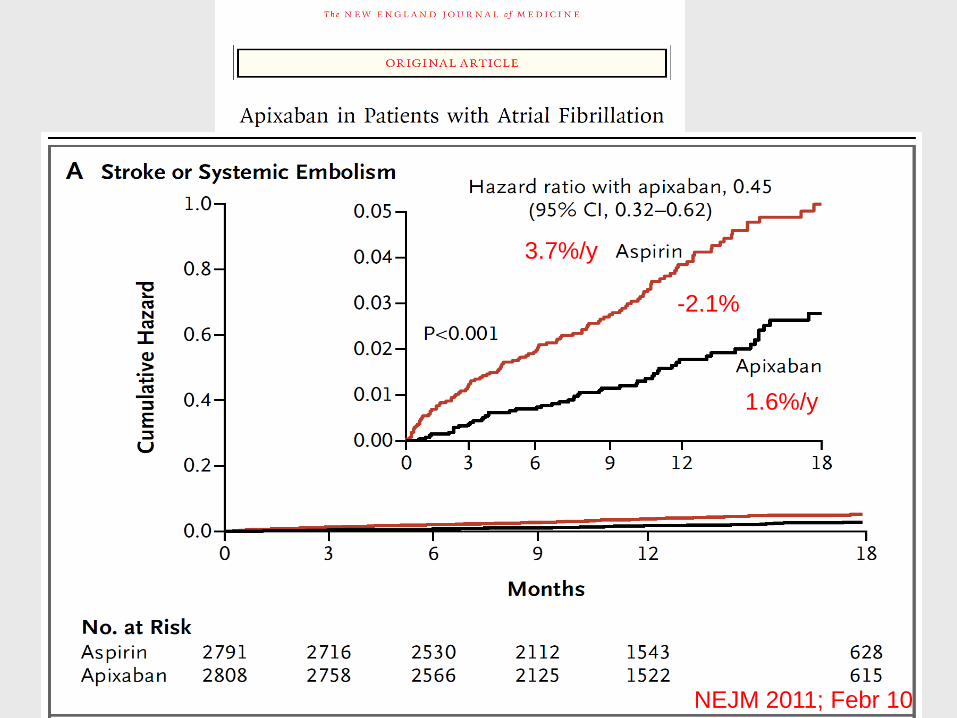
NEJM 2011; Febr 10
3.7%/y
1.6%/y
-2.1%
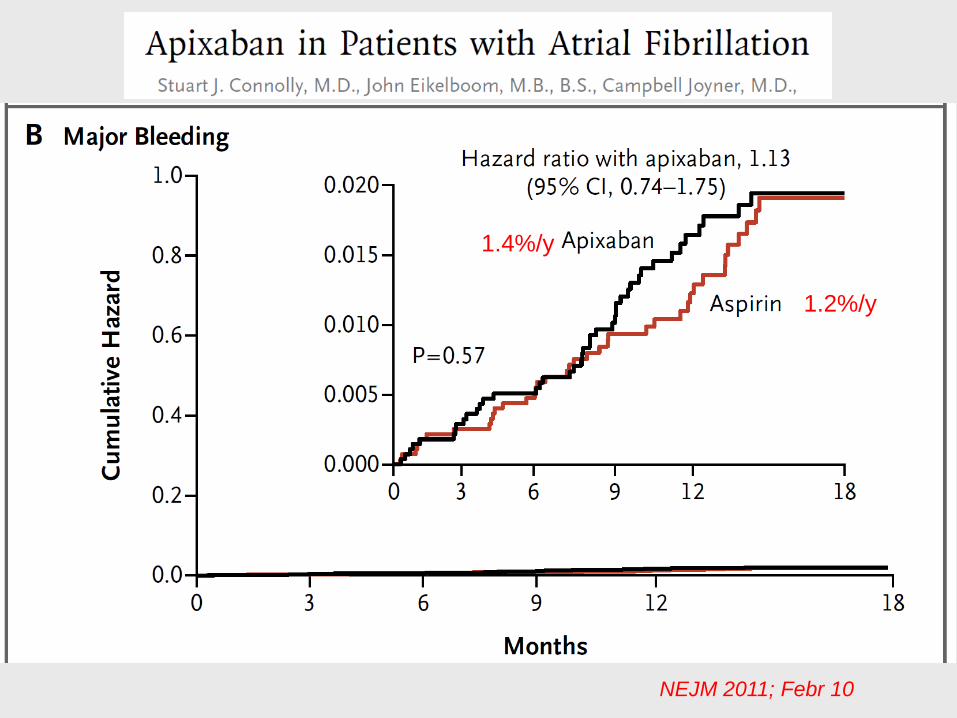
NEJM 2011; Febr 10
1.2%/y
1.4%/y
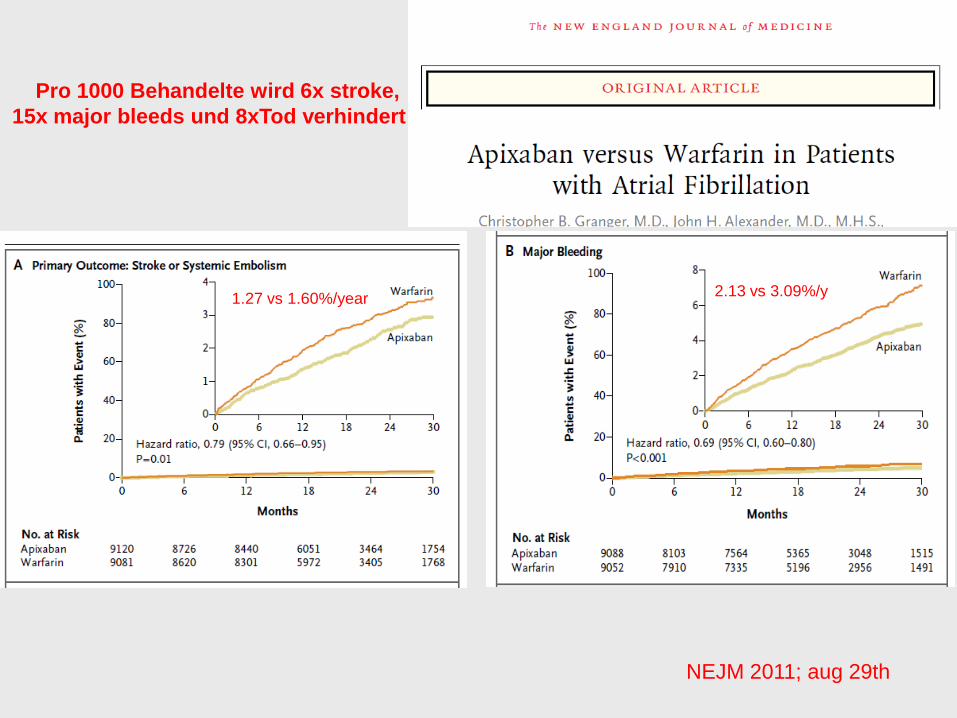
NEJM 2011; aug 29th
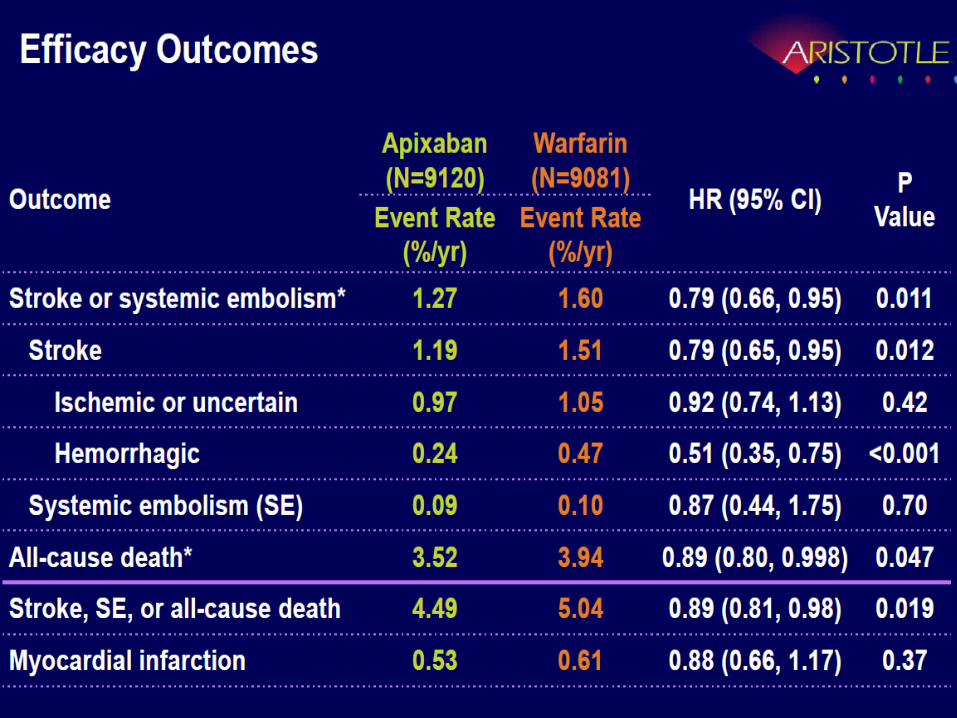
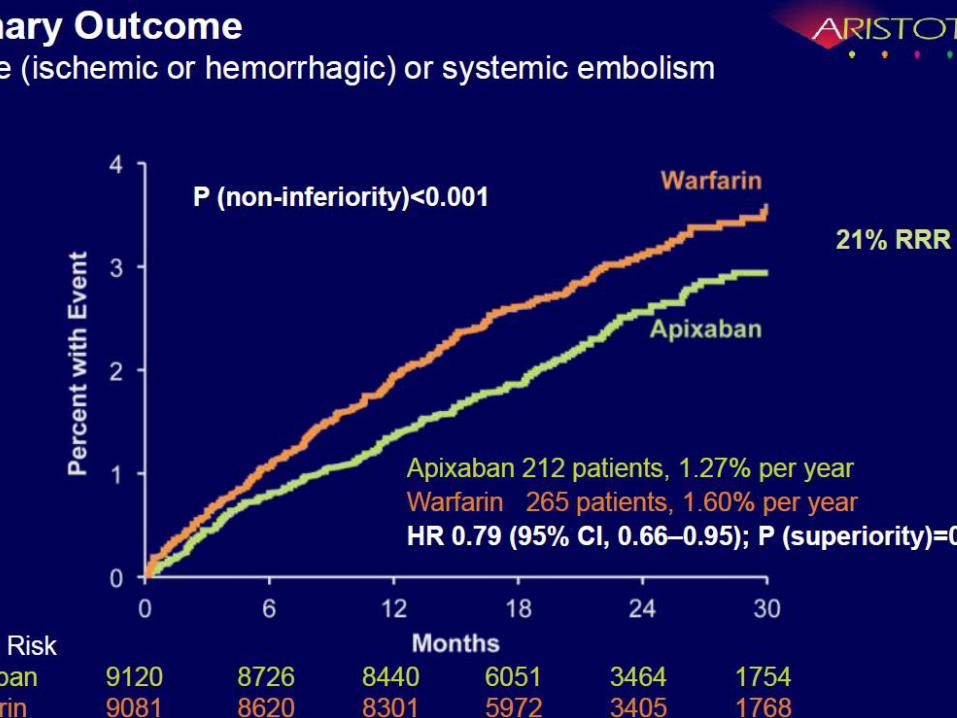
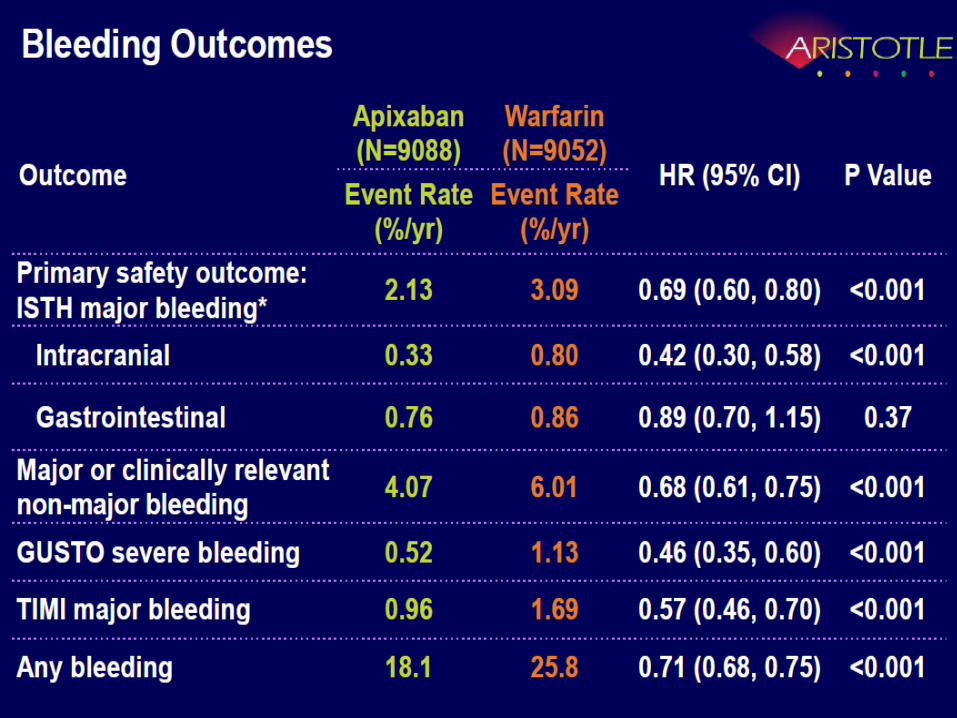
2.13 vs 3.09%/y1.27 vs 1.60%/year
Pro 1000 Behandelte wird 6x stroke,
15x major bleeds und 8xTod verhindert
Das Dabigatran wird ja demnächst zugelassen in der
CH, es wurde in 2 Dosierungen zugelassen in Can, JPN,
in der höheren -2x150mg (und einer wesentlich tieferen
– 2x75mg) in den USA.
Gibt es Daten, die meiner Risikokategorie, meinem
Alter und meiner Co-Medikation gerecht werden?
Patienten und Hausarzt-Fragen

Clinical Chemistry, Vol.57, Nr.4,
April 2011
Neue Antikoagulantien: Die Fragen von
Patienten und ihren Aerzten

Zusammenfassung
1. Wirksamkeit: Mind gleich gut (in einigen Situationen besser)
2. ICB: Besser
3. Kein Lebersignal (bis jetzt)
4. Möglichkeit der Individualisierung / Wahl bzgl Risiko und Metabolismus
5. p.o.!
6. Nahrungsunabhängig? – weniger nahrungsabhängig!
7. Weniger Medikamenteninteraktionen
8. Monitorisierung? Patientenentscheid.
9. Antagonisierung? Aber kurze Halbwertszeit.
10.Compliance/Therapie-Unterbrüche?
11.Bridging?
12.Gut und sehr gut INR-Eingestellte zurückhaltend wechseln!
13. „Das Spiel dauert 90 min“
Kriterien für Auswahl: Niereninsuffizienz/ Schlechte Compliance:1xtägl/
Dyspepsie/ Medikamenteninteraktionen/Risikoprofil/
Aber ich bin doch perfekt eingestellt und „zu fast 100%“
im therapeutischen Bereich mit dem Marcoumar, ich
weiss, dass es fast nie blutet. Wie gross ist unter diesen
perfekten Bedingungen die Hirnschlag- und Hirn-
Blutungsgefahr wirklich?
Patienten Fragen
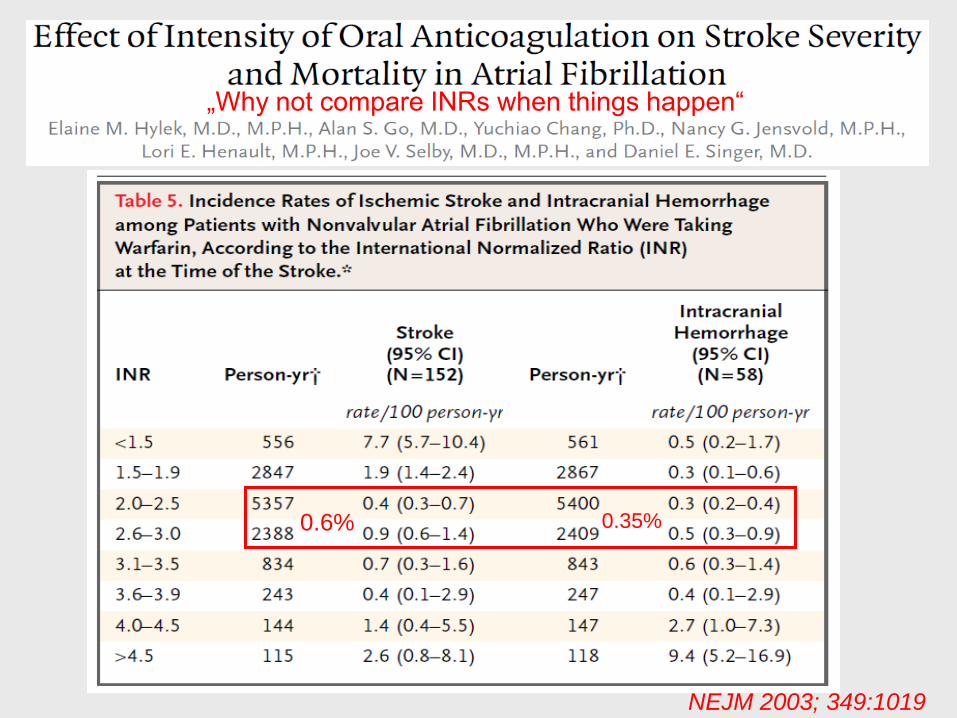
NEJM 2003; 349:1019
„Why not compare INRs when things happen“
0.6% 0.35%
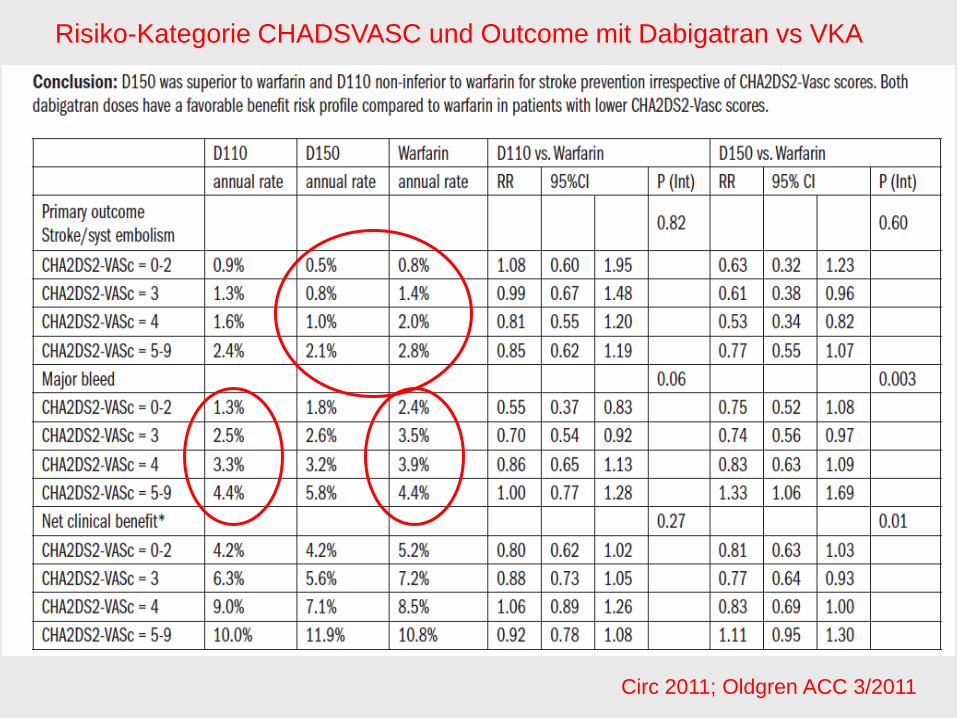
Circ 2011; Oldgren ACC 3/2011
Risiko-Kategorie CHADSVASC und Outcome mit Dabigatran vs VKA

Circ 2011; 123: 2363 (mai 31)
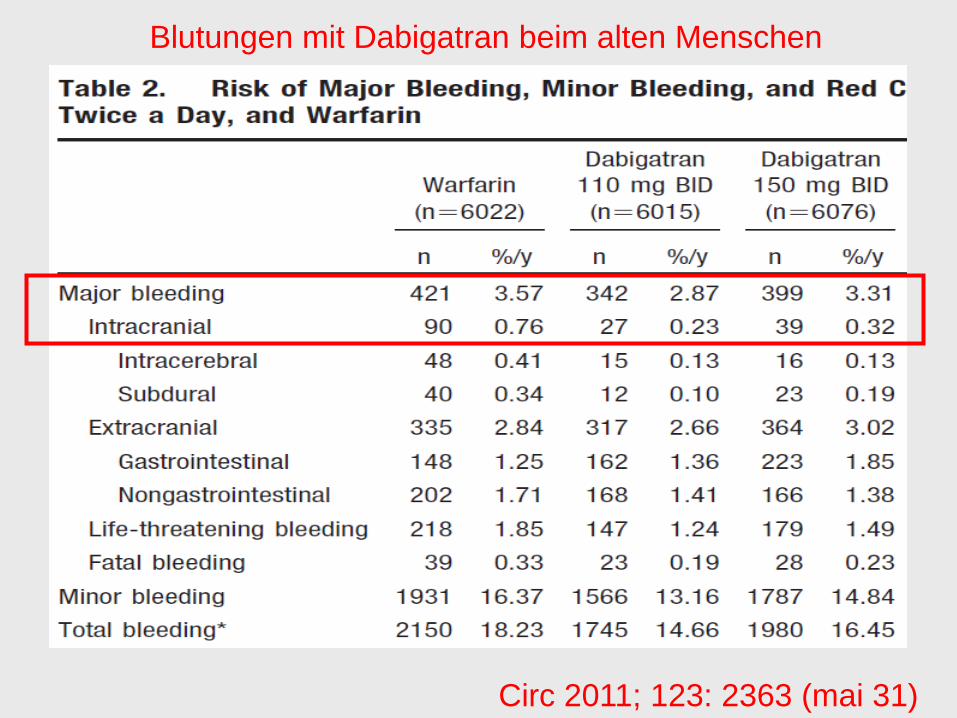
Blutungen mit Dabigatran beim alten Menschen
Circ 2011; 123: 2363 (mai 31)
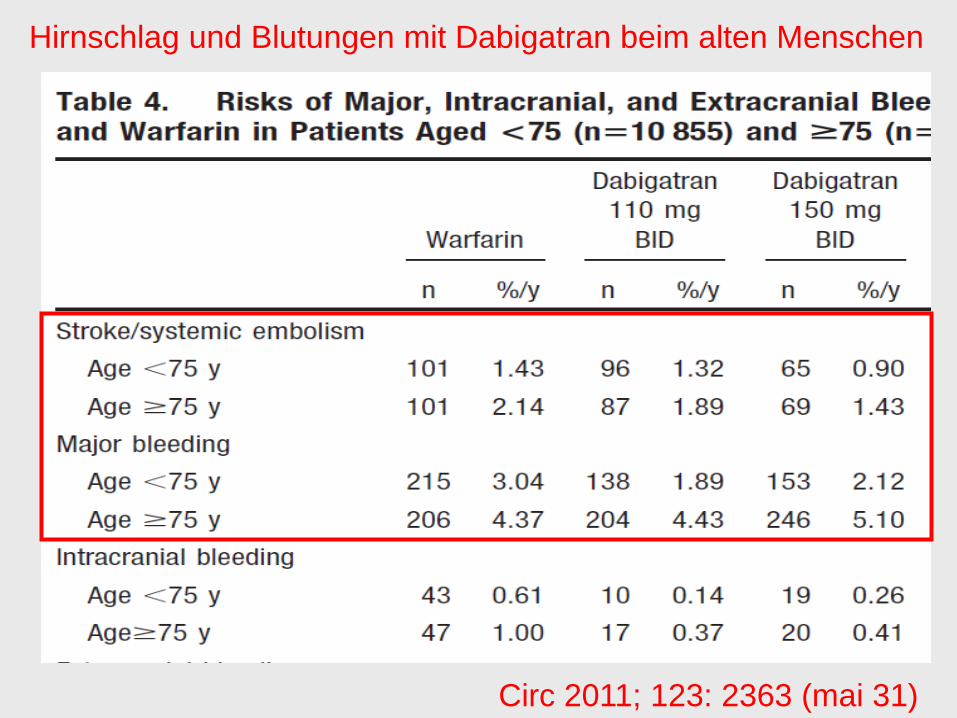
Hirnschlag und Blutungen mit Dabigatran beim alten Menschen
Circ 2011; 123: 2363 (mai 31)
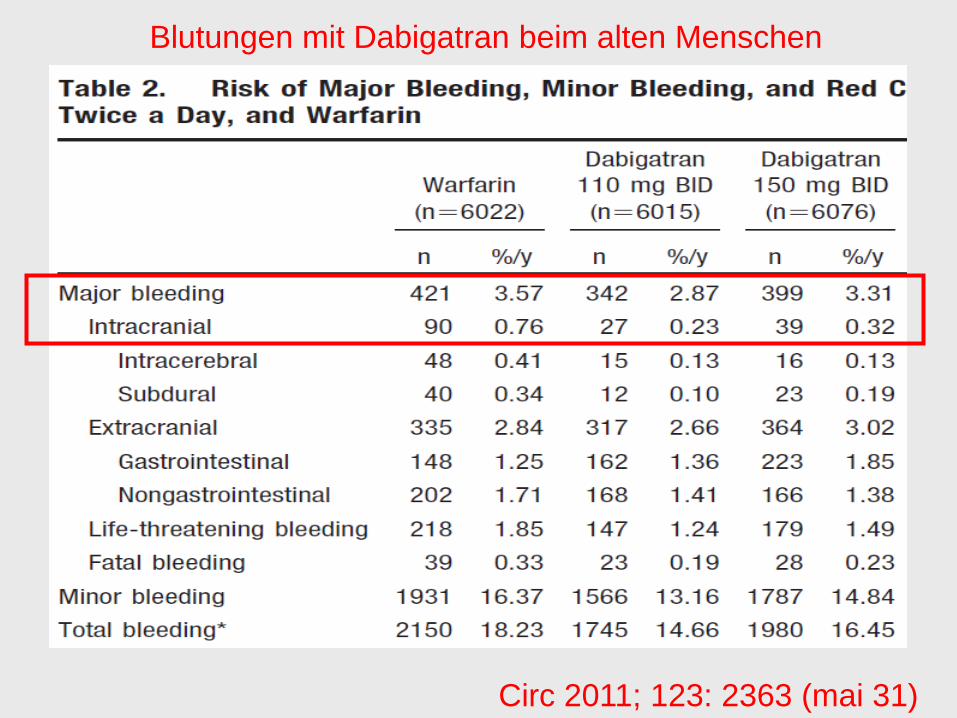
Blutungen mit Dabigatran beim alten Menschen
Circ 2011; 123: 2363 (mai 31)
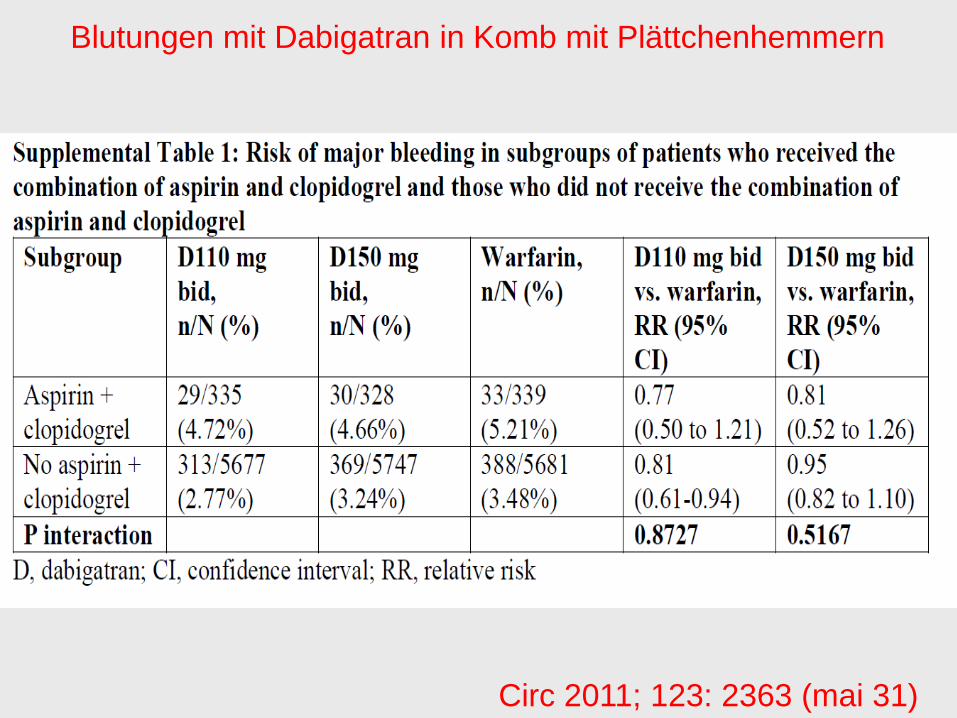
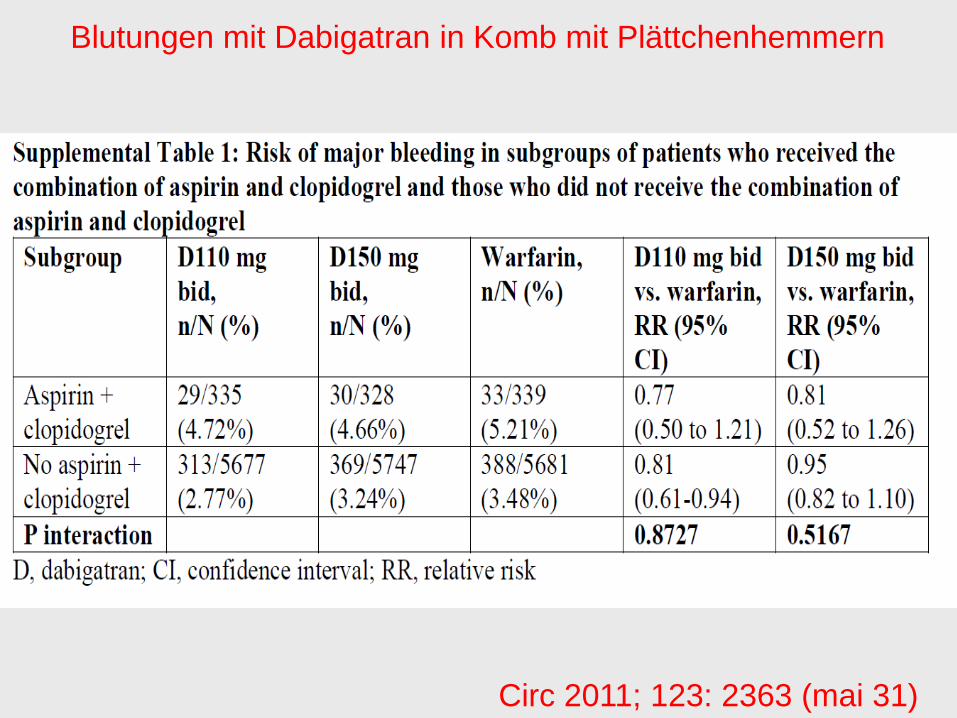
Blutungen mit Dabigatran in Komb mit Plättchenhemmern
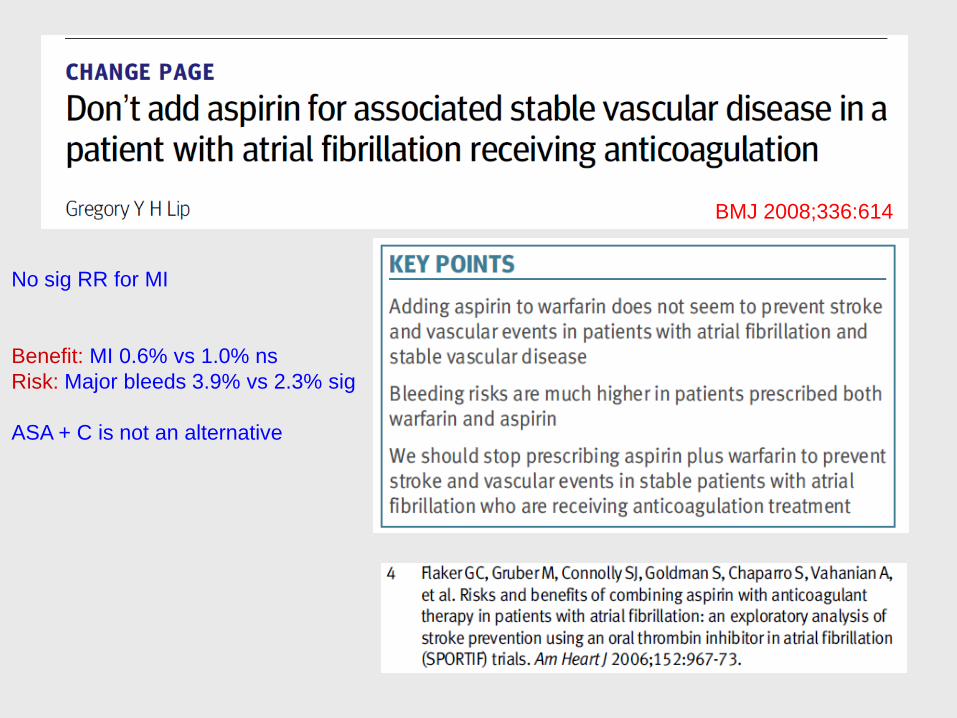
BMJ 2008;336:614
No sig RR for MI
Benefit: MI 0.6% vs 1.0% ns
Risk: Major bleeds 3.9% vs 2.3% sig
ASA + C is not an alternative

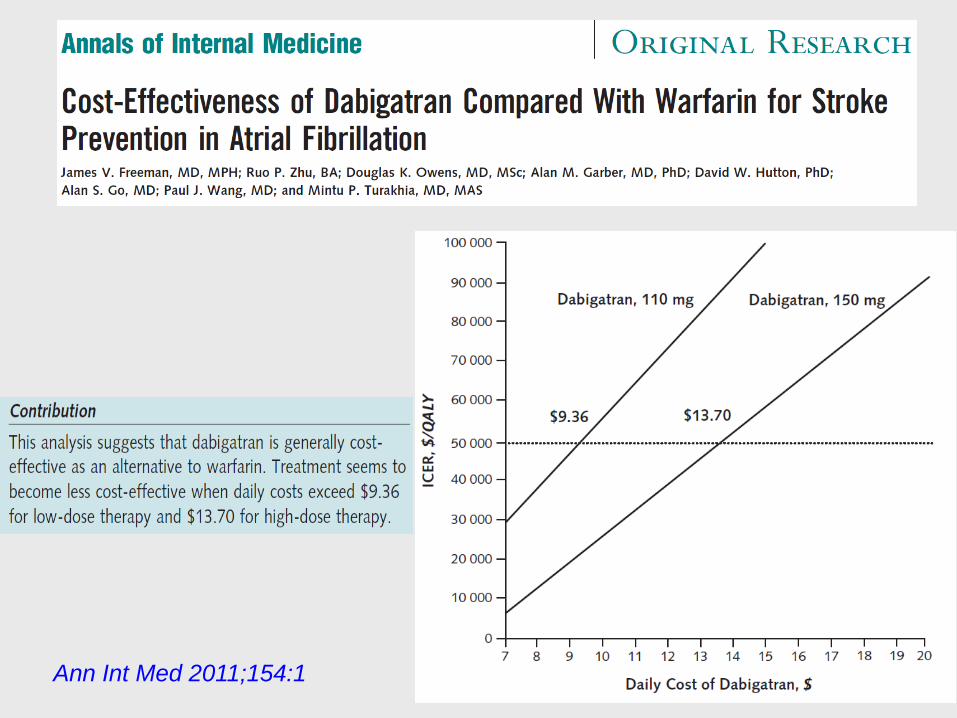
Ann Int Med 2011;154:1

TTR in EINSTEIN
NEJM 2010; 363:2495

Stroke und TE-Ereignisse beim Vorhofflimmern unter Rivaroxaban
NEJM 2011; e pub aug
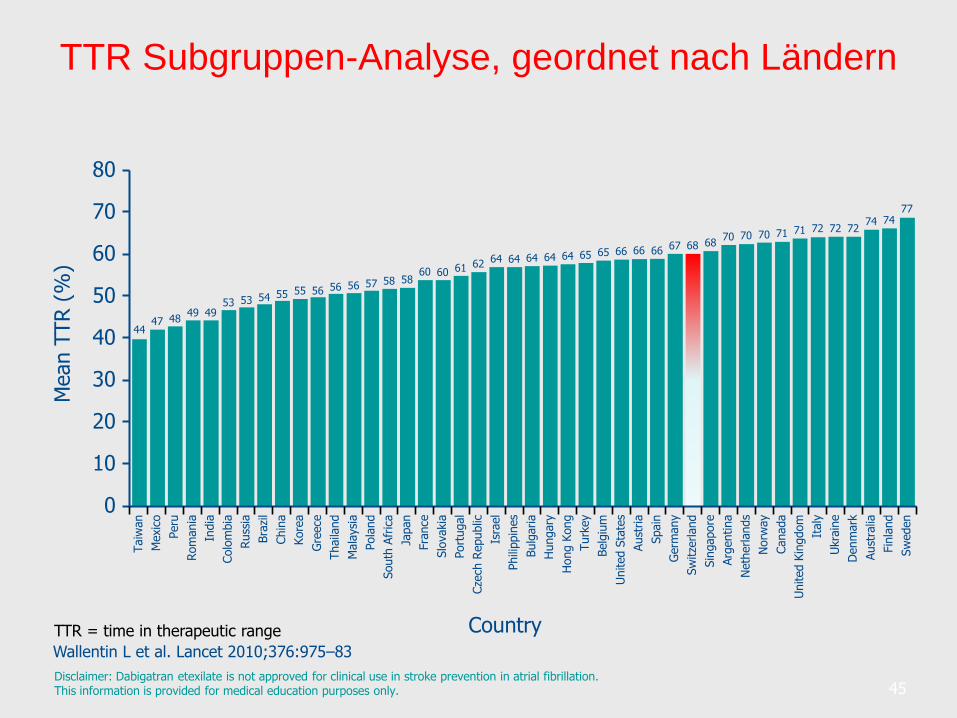
TTR Subgruppen-Analyse, geordnet nach Ländern
45Disclaimer: Dabigatran etexilate is not approved for clinical use in stroke prevention in atrial fibrillation.This information is provided for medical education purposes only.
TTR = time in therapeutic range
Wallentin L et al. Lancet 2010;376:975–83
Mean T
TR (
%)
10
30
50
60
70
80
0
Country
20
40
Taiw
an
Mexic
o
Peru
Rom
ania
India
Colo
mbia
Russ
ia
Bra
zil
Chin
a
Kore
a
Gre
ece
Thaila
nd
Mala
ysi
a
Pola
nd
South
Afr
ica
Japan
Fra
nce
Slo
vakia
Port
ugal
Cze
ch R
epublic
Isra
el
Phili
ppin
es
Bulg
aria
Hungary
Hong K
ong
Turk
ey
Belg
ium
United S
tate
s
Aust
ria
Spain
Germ
any
Sw
itze
rland
Sin
gapore
Arg
entina
Neth
erlands
Norw
ay
Canada
United K
ingdom
Italy
Ukra
ine
Denm
ark
Aust
ralia
Fin
land
Sw
eden
4447 48
49 4953 53 54 55 55 56 56 56 57 58 58
60 60 61 62 64 64 64 64 64 65 65 66 66 66 67 68 6870 70 70 71 71 72 72 72
74 7477
Ich bin schlecht einstellbar mit meinem
Quickwert. Profitiere ich nun mehr oder weniger
von einer Umstellung auf die Neuen?
Patienten-Frage:
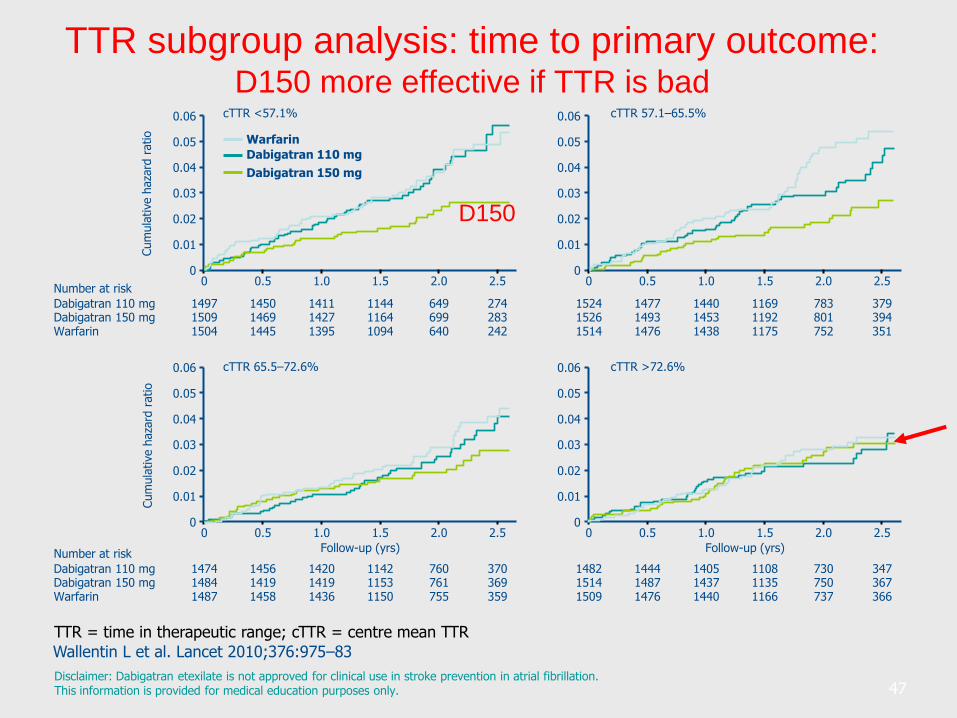
TTR subgroup analysis: time to primary outcome:D150 more effective if TTR is bad
Disclaimer: Dabigatran etexilate is not approved for clinical use in stroke prevention in atrial fibrillation.This information is provided for medical education purposes only.
TTR = time in therapeutic range; cTTR = centre mean TTR
Wallentin L et al. Lancet 2010;376:975–83
Dabigatran 110 mg
Dabigatran 150 mg
WarfarinCum
ula
tive h
aza
rd r
atio
0.01
0.03
0.04
0.05
0.06
0
0.02
0 0.5 1.0 1.5 2.0 2.5
1497 1450 1411 1144 649 274Dabigatran 110 mg1509 1469 1427 1164 699 283Dabigatran 150 mg1504 1445 1395 1094 640 242Warfarin
Number at risk
cTTR <57.1%
0.01
0.03
0.04
0.05
0.06
0
0.02
0 0.5 1.0 1.5 2.0 2.5
1524 1477 1440 1169 783 3791526 1493 1453 1192 801 3941514 1476 1438 1175 752 351
cTTR 57.1–65.5%
Cum
ula
tive h
aza
rd r
atio
0.01
0.03
0.04
0.05
0.06
0
0.02
0
Follow-up (yrs)
0.5 1.0 1.5 2.0 2.5
1474 1456 1420 1142 760 370Dabigatran 110 mg1484 1419 1419 1153 761 369Dabigatran 150 mg1487 1458 1436 1150 755 359Warfarin
Number at risk
cTTR 65.5–72.6%
0.01
0.03
0.04
0.05
0.06
0
0.02
0 0.5 1.0 1.5 2.0 2.5
1482 1444 1405 1108 730 3471514 1487 1437 1135 750 3671509 1476 1440 1166 737 366
Follow-up (yrs)
cTTR >72.6%
47
D150
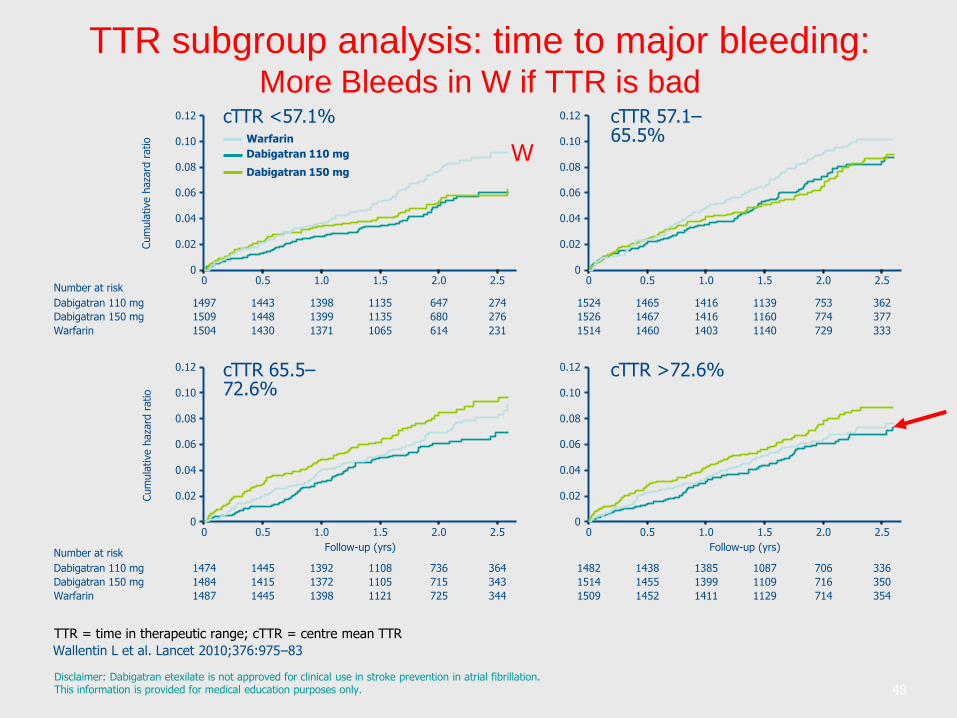
TTR subgroup analysis: time to major bleeding:More Bleeds in W if TTR is bad
Disclaimer: Dabigatran etexilate is not approved for clinical use in stroke prevention in atrial fibrillation.This information is provided for medical education purposes only.
TTR = time in therapeutic range; cTTR = centre mean TTR
Wallentin L et al. Lancet 2010;376:975–83
Cum
ula
tive h
aza
rd r
atio
0.02
0.06
0.08
0.10
0.12
0
0.04
0 0.5 1.0 1.5 2.0 2.5
1497 1443 1398 1135 647 274Dabigatran 110 mg
1509 1448 1399 1135 680 276Dabigatran 150 mg
1504 1430 1371 1065 614 231Warfarin
Number at risk
cTTR <57.1%
0.02
0.06
0.08
0.10
0.12
0
0.04
0 0.5 1.0 1.5 2.0 2.5
1524 1465 1416 1139 753 362
1526 1467 1416 1160 774 377
1514 1460 1403 1140 729 333
cTTR 57.1–65.5%
Cum
ula
tive h
aza
rd r
atio
0.02
0.06
0.08
0.10
0.12
0
0.04
0
Follow-up (yrs)
0.5 1.0 1.5 2.0 2.5
1474 1445 1392 1108 736 364Dabigatran 110 mg
1484 1415 1372 1105 715 343Dabigatran 150 mg
1487 1445 1398 1121 725 344Warfarin
Number at risk
cTTR 65.5–72.6%
0.02
0.06
0.08
0.10
0.12
0
0.04
0 0.5 1.0 1.5 2.0 2.5
1482 1438 1385 1087 706 336
1514 1455 1399 1109 716 350
1509 1452 1411 1129 714 354
Follow-up (yrs)
cTTR >72.6%
Dabigatran 110 mg
Dabigatran 150 mg
Warfarin
48
W
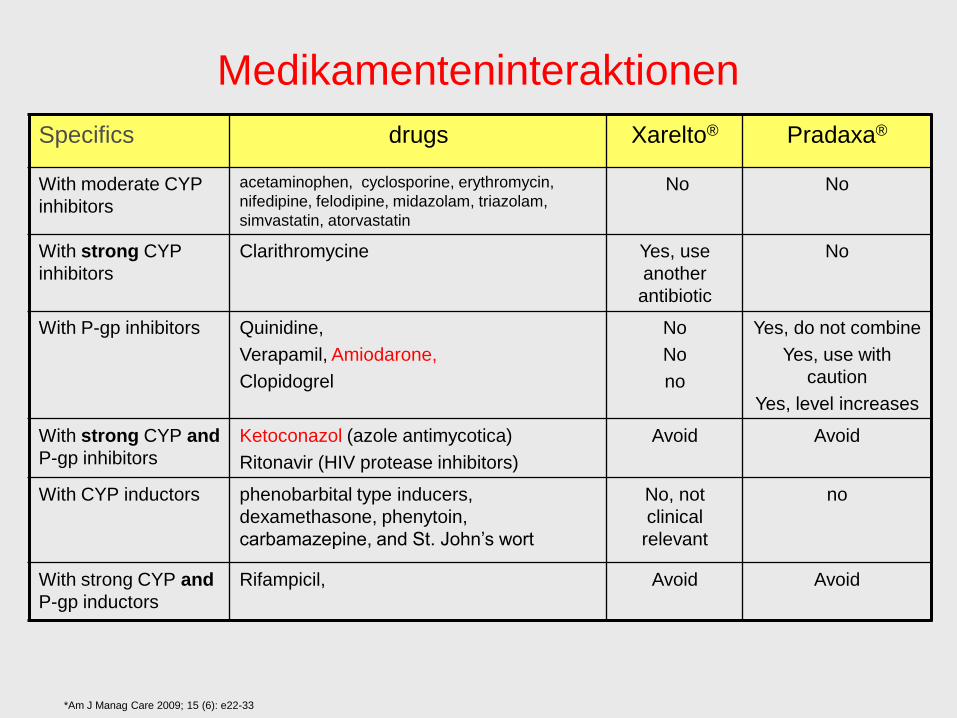
Medikamenteninteraktionen
Specifics drugs Xarelto® Pradaxa®
With moderate CYP
inhibitors
acetaminophen, cyclosporine, erythromycin,
nifedipine, felodipine, midazolam, triazolam,
simvastatin, atorvastatin
No No
With strong CYP
inhibitors
Clarithromycine Yes, use
another
antibiotic
No
With P-gp inhibitors Quinidine,
Verapamil, Amiodarone,
Clopidogrel
No
No
no
Yes, do not combine
Yes, use with
caution
Yes, level increases
With strong CYP and
P-gp inhibitors
Ketoconazol (azole antimycotica)
Ritonavir (HIV protease inhibitors)
Avoid Avoid
With CYP inductors phenobarbital type inducers,
dexamethasone, phenytoin,
carbamazepine, and St. John’s wort
No, not
clinical
relevant
no
With strong CYP and
P-gp inductors
Rifampicil, Avoid Avoid
*Am J Manag Care 2009; 15 (6): e22-33
Wie steht es mit der Niereninsuffizienz?
Hausarzt-Frage:
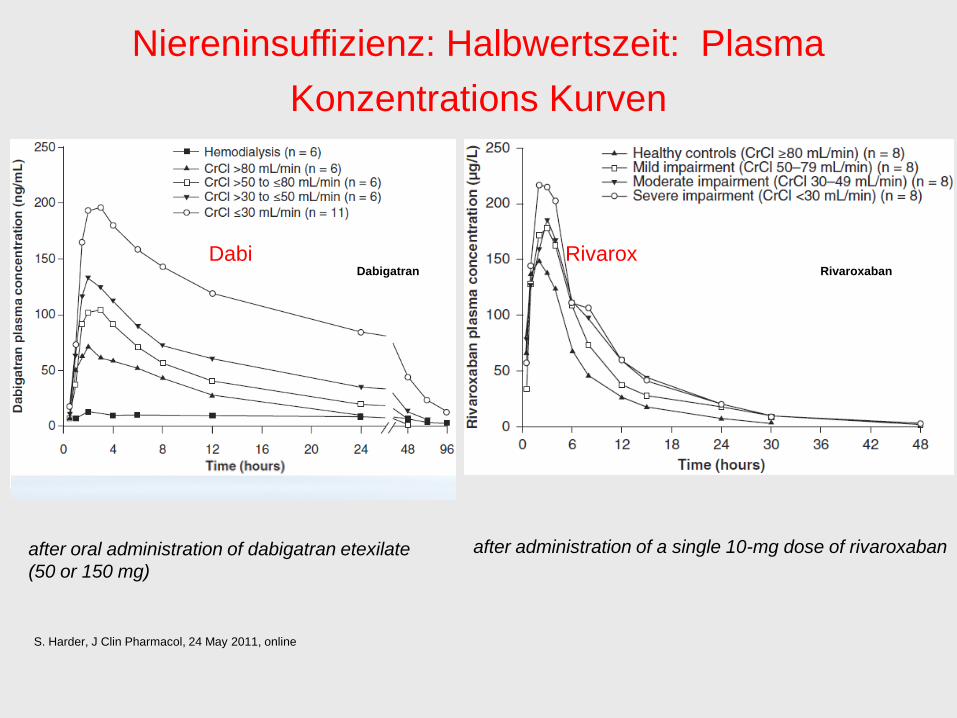
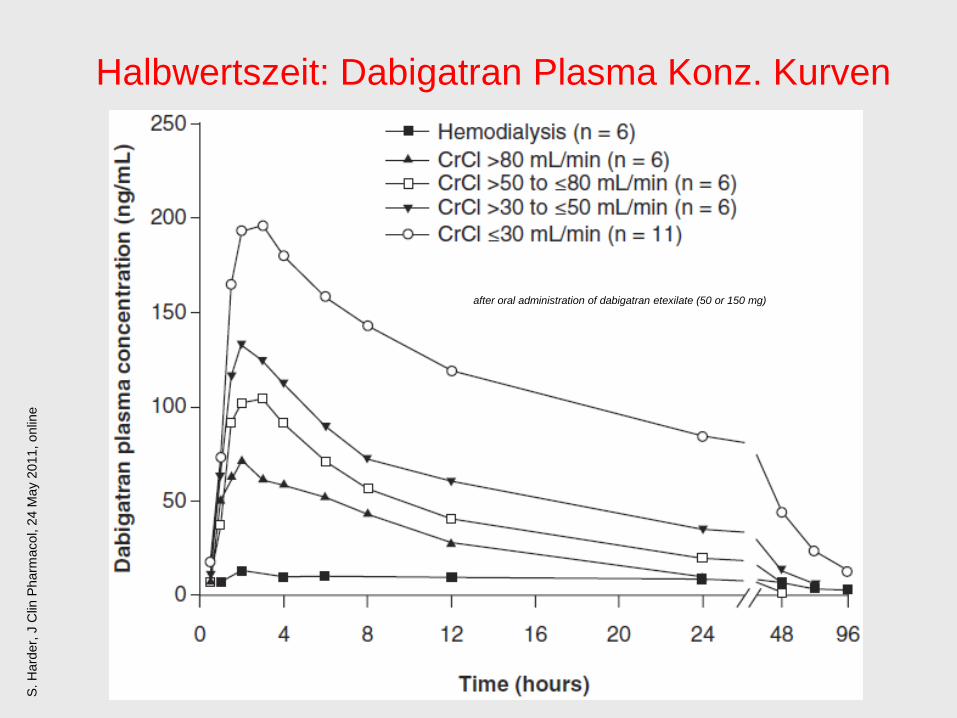
Niereninsuffizienz: Halbwertszeit: Plasma
Konzentrations Kurven
S. Harder, J Clin Pharmacol, 24 May 2011, online
Dabigatran Rivaroxaban
after oral administration of dabigatran etexilate
(50 or 150 mg)
after administration of a single 10-mg dose of rivaroxaban
Dabi Rivarox
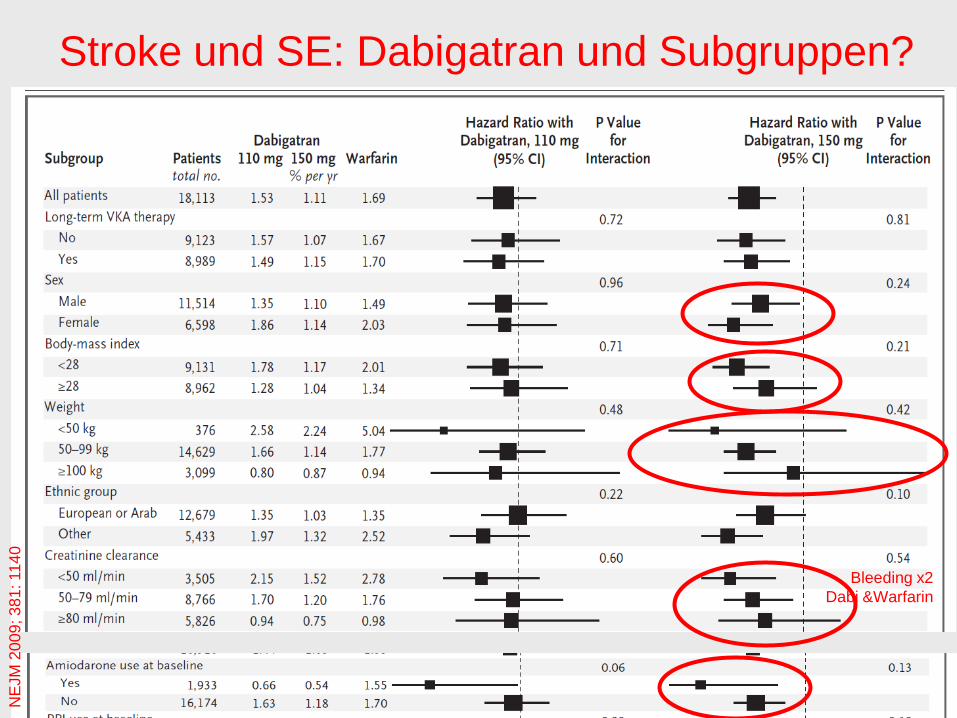
Stroke und SE: Dabigatran und Subgruppen?
NEJM 2009; 381: 1140
NE
JM
20
09
; 3
81
: 11
40
Bleeding x2
Dabi &Warfarin

Wie steht es mit dem Körpergewicht?
Hausarzt-Frage:
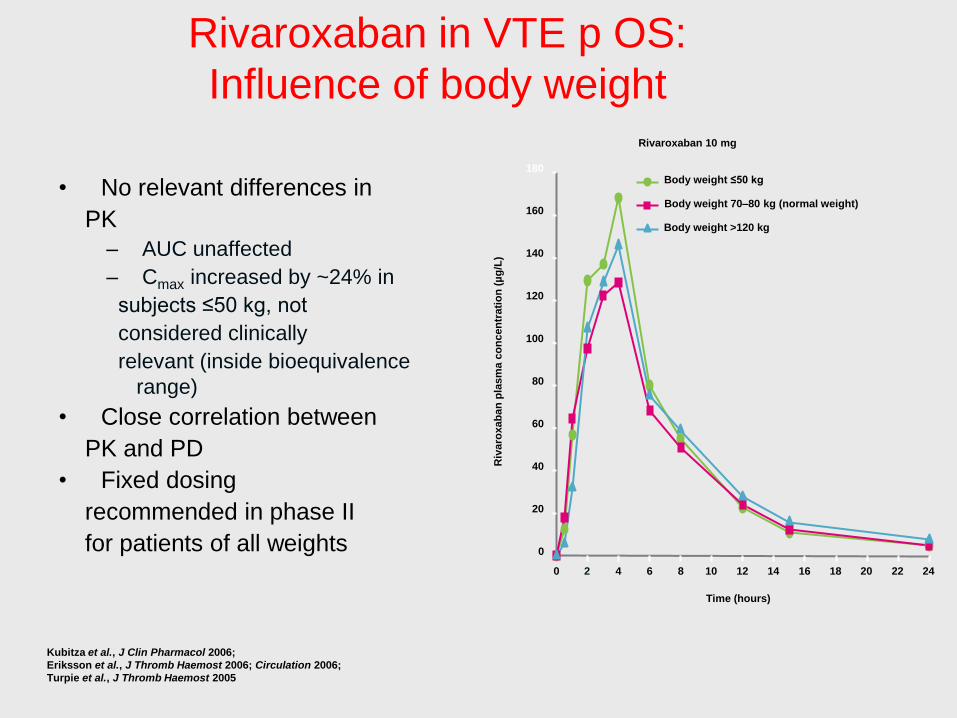
Rivaroxaban in VTE p OS:
Influence of body weight
• No relevant differences in
PK
– AUC unaffected
– Cmax increased by ~24% in
subjects ≤50 kg, not
considered clinically
relevant (inside bioequivalence
range)
• Close correlation between
PK and PD
• Fixed dosing
recommended in phase II
for patients of all weights
Time (hours)
Body weight ≤50 kg
Body weight 70–80 kg (normal weight)
Body weight >120 kg
0
20
40
60
80
100
120
140
160
180
0 2 4 6 8 10 12 14 16 18 20 22 24
Riv
aro
xab
an
pla
sm
a c
on
cen
trati
on
(µ
g/L
)
Rivaroxaban 10 mg
Kubitza et al., J Clin Pharmacol 2006;
Eriksson et al., J Thromb Haemost 2006; Circulation 2006;
Turpie et al., J Thromb Haemost 2005
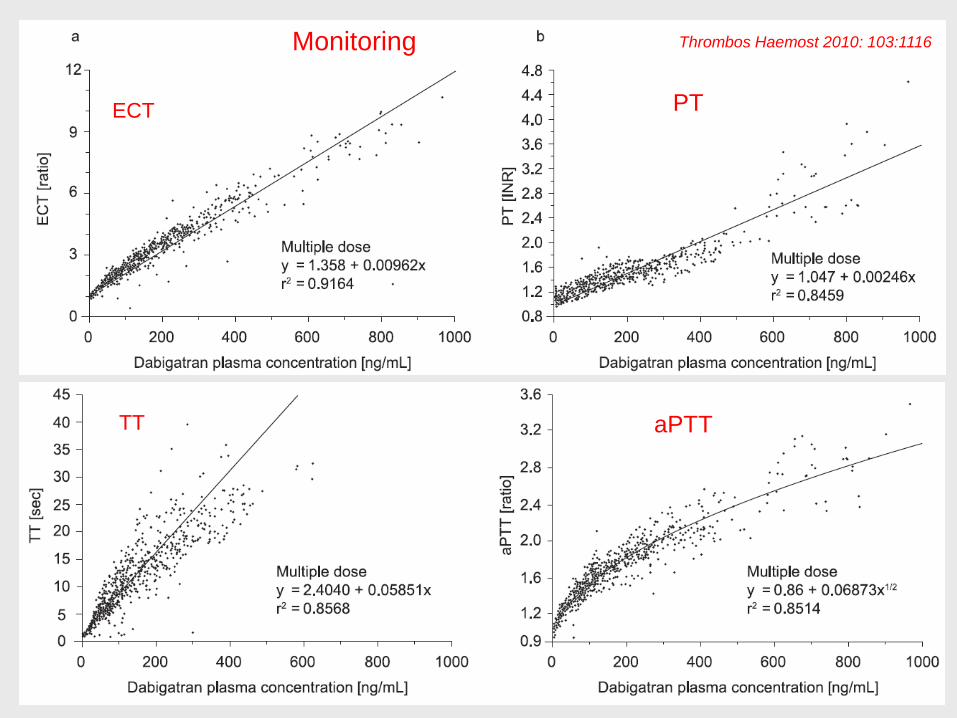
Wie steht es mit dem Monitoring?
Hausarzt-Frage:
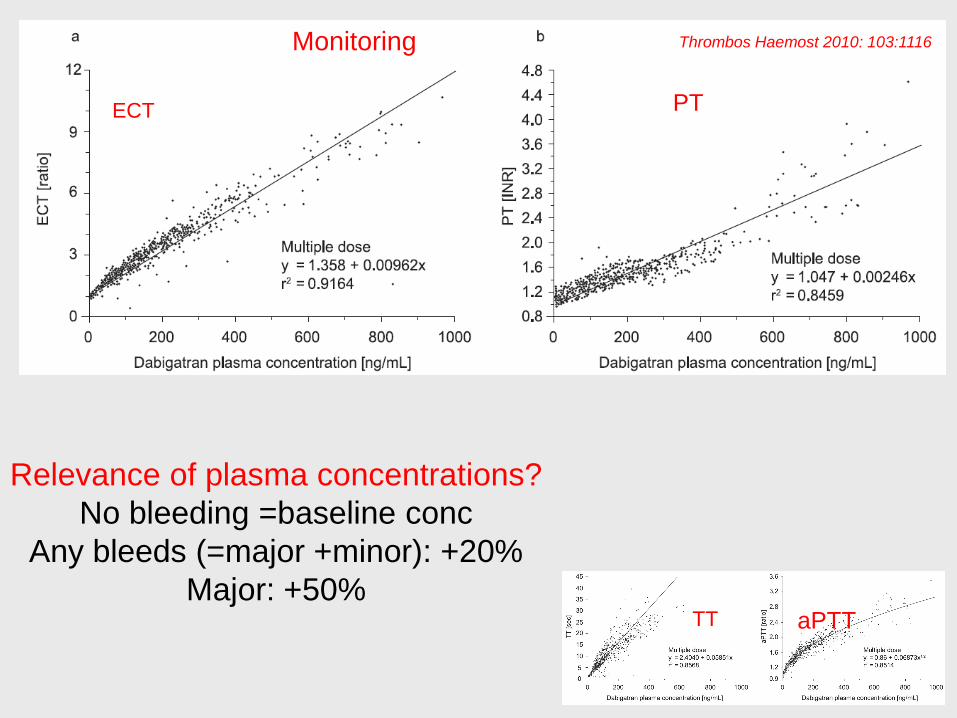
Monitoring
aPTT
PTECT
TT
Thrombos Haemost 2010: 103:1116
Relevance of plasma concentrations?
No bleeding =baseline conc
Any bleeds (=major +minor): +20%
Major: +50%
Bedeutung der Compliance bei kurzen
Halbwertszeiten?
1x täglich oder 2x täglich?
Hausarzt-Frage:
Weniger ICBs Outcome in %/Jahr
D110 D150 Riva OT Riva ITT Apix War(-D) War(-R) ASA(-A)
RE-LY RE-LY ROCKET-AF AVER
Dabigatran Rivaroxaban Apixaban Warfarin
S/SE 1.53 1.11 1.71 2.12 1.6 1.69 2.16/2.42 3.7
ICB 0.23 0.30 0.49 0.20* 0.74 0.74 0.3
Death 3.75 3.64 1.87 3.5 4.13 2.21 4.4
M‘Bleed 2.71 3.11 3.60 1.4 3.36 3.45 1.2
*Aristoteles: 0.24% vs 0.47%
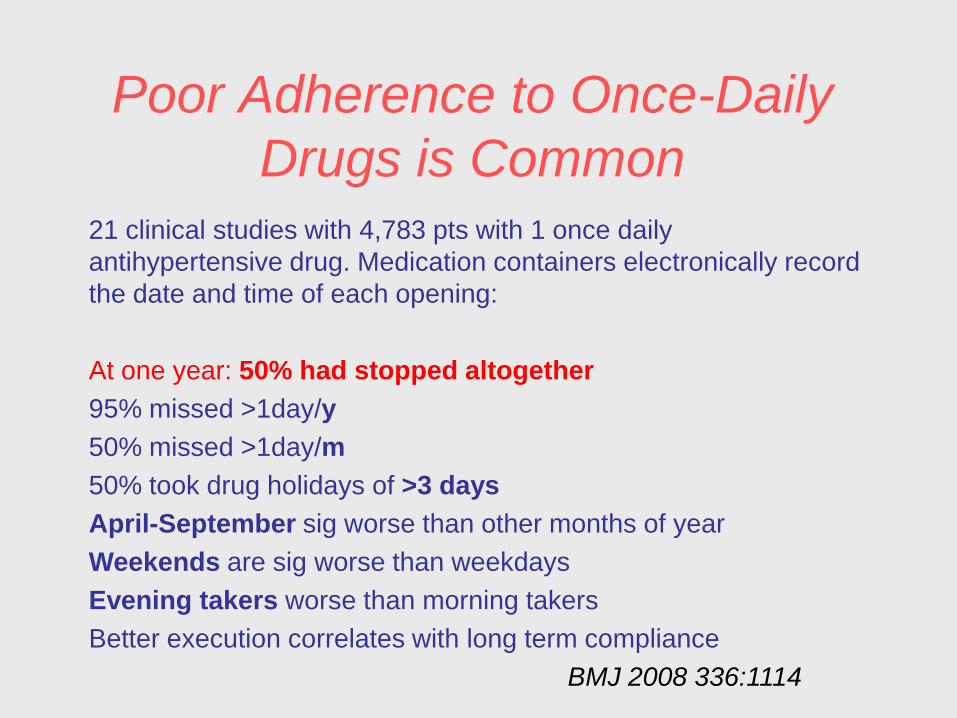
Poor Adherence to Once-Daily
Drugs is Common
21 clinical studies with 4,783 pts with 1 once daily
antihypertensive drug. Medication containers electronically record
the date and time of each opening:
At one year: 50% had stopped altogether
95% missed >1day/y
50% missed >1day/m
50% took drug holidays of >3 days
April-September sig worse than other months of year
Weekends are sig worse than weekdays
Evening takers worse than morning takers
Better execution correlates with long term compliance
BMJ 2008 336:1114
Pharmakokinetik?
Hausarzt-Frage:
…und wenns blutet?
Hausarzt-Frage:
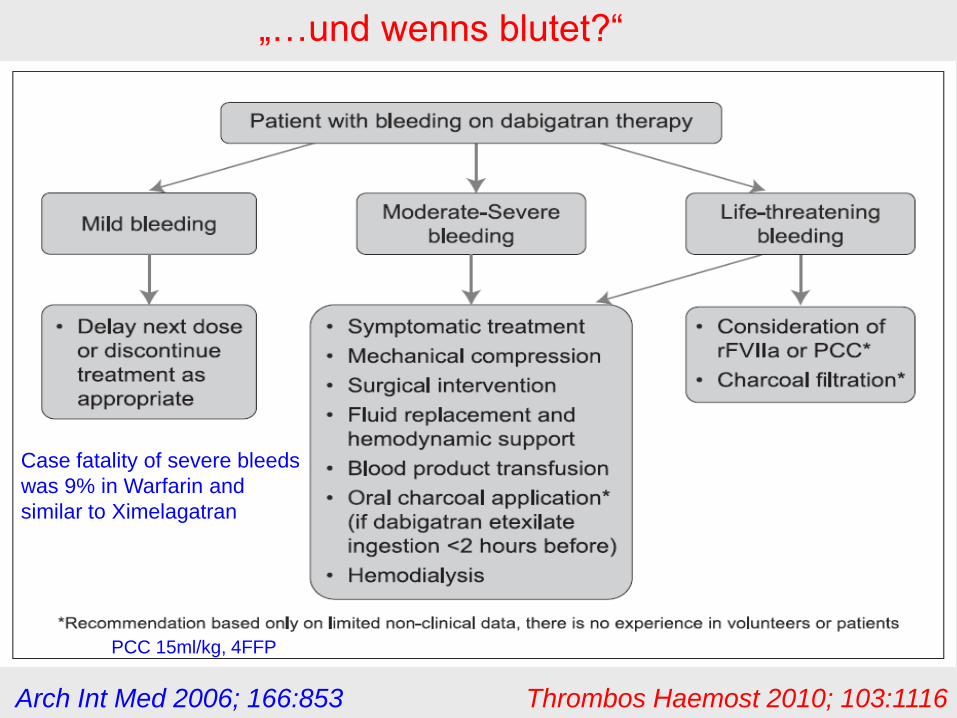
Arch Int Med 2006; 166:853 Thrombos Haemost 2010; 103:1116
„…und wenns blutet?“
Case fatality of severe bleeds
was 9% in Warfarin and
similar to Ximelagatran
PCC 15ml/kg, 4FFP

Bridging –Procedere?
Hausarzt-Frage:
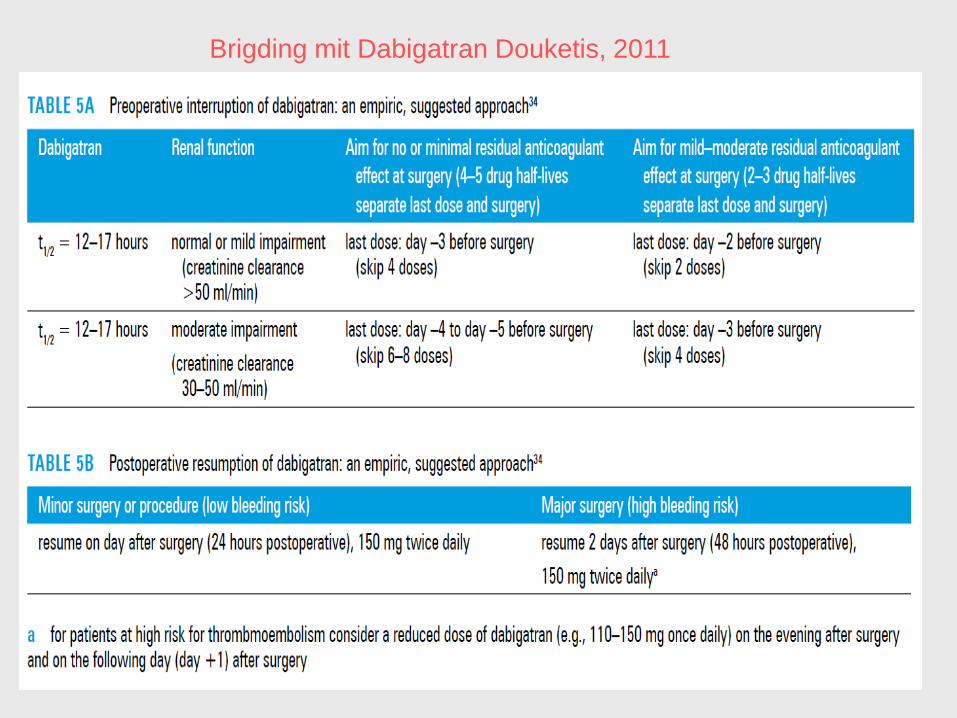
Brigding mit Dabigatran Douketis, 2011

Ich bin schlecht einstellbar mit meinem
Quickwert. Profitiere ich nun mehr oder weniger
von einer Umstellung auf die Neuen?
Patienten-Frage:

Rivaroxaban (Xarelto)
Oraler und direkter Factor-Xa-Inhibitor
Hohe orale Bioverfügbarkeit (80 - 100%)
Sofort aktiv: Cmax= 2 - 4 h (ähnlich LMWH)
Halflife: 5 - 9h (Aeltere Pat.: 11 - 13 h)
Dualer Eliminationsweg 1/3 renale Elimination
2/3 Metabolisierung durch die Leber
Fixe Dosis – unabhängig von Ernährung, Körpergewicht, Geschlecht und Alter (in
klinischen Studien)
Kein Monitoring erforderlich (spez anti-Xa assay). PT, aPTT werden
Medi-Interaktionen: CYP3A4-Hemmer erhöhen die Konzentration: Ketokonazol,
Ritonavir; p-gp Inhibitoren: Clarithromycin
CYP3A4 Induktoren erniedrigen die Konz.:Rifampicin Phenobarbital, Phenytoin,
Carbamacepin, Johanniskraut.
Perzborn E et al. J Thromb Haemost 2005;3:514–521. Kubitza D et al. Eur J Clin Pharmacol 2005;61:873–880. Kubitza D et al. J Clin Pharmacol 2006;46:981–990. Kubitza D et al. Br J Clin Pharmacol 2007;63:469–476.Kubitza D et al. J Clin Pharmacol 2007;47:218–226. Kubitza D et al. Blood 2006;108:Abstract 905.
Rivaroxaban
N NO
NH
O
S
ClO
O
O
Aber ich bin doch perfekt eingestellt und zu fast 100% im
therapeutischen Bereich mit dem Marcoumar, ich weiss,
dass es fast nie blutet.
Patienten Fragen
Hausarzt Dr K. ruft mich an, er habe soeben einem 60 j.
Patienten mit Status 2J. nach TVT Xarelto 10mg für die
Reise nach S.F. (9h) und zurück mitgegeben. „Ob das in
meinem Sinne sei“? Der Pat möchte nicht spritzen und
doch „etwas tun“ und sein „Nachbar habe es doch
problemlos erhalten…“
Fall 2

A) Nein, keine Studien
B) Ja, ws wirksam und NW-arm, ähnliche T1/2 wie LMWH
C) Mechanische Prophylaxe hätte genügt
D) Wird nie Studien geben (?) Analogie-Schluss ziehen?
E) Warte mind auf Studien bei andern ortho-Eingriffen,
allg-chi Populationen, med. Patienten-Kollektiven*
*Magellan?
Fall 2
Halbwertszeit: Dabigatran Plasma Konz. Kurven
S. H
ard
er,
J C
lin P
harm
acol, 2
4 M
ay 2
011, onlin
e
after oral administration of dabigatran etexilate (50 or 150 mg)

The „DEAR“ Trials in AF
RE-LY ENGAGE AVERROES ARISTOTLE ROCKET-
Dabigatran Edoxaban Apixaban Apixaban Rivaroxaban
110/150 bid 5mg bid 5mg bid 30/60mg od 20mg od
INR 2-3 INR 2-3 ASA INR 2-3 INR 2-3
18,000pts 20,500 5,600 18,000 14,000
1 RF moderate R >/= 1RF 1 RF moderate-
CHADS 1: 32% CHADS >=2 „unsuitable“ high risk
CHADS 2: 35% „intolerant“ CHADS 2: 10%
CHADS 3: 33% CH >/=3: 90%
50% VK naive
W:open label Stopped premat DD S-INR; Neur. DD; Sham INR
S/SE S/SE S/SE S/SE S/SE
Published 3/2012 Published 4/2011 (Abstr)
Event d:450 Time 24m Event d 36m Event d 448 Event d 405
>12m >14m

Bleeding
Comp EP.:TE, death
66j. Patientin mit TVT Oberschenkel links, unprovoziert,
schlecht einstellbar mit Markoumar (TTR<50%),
trotz häufiger INR, zT 2x/Woche, „will nicht mehr recht“.
Sie möchte nach 3 Monaten absetzen.
TTR?
Compliance?
Interaktionen, Medi?
Essen?
Co Diagnosen?
…
Risiko-Analyse: Blutungsgefahr, Rezidivgefahr?
Fall 3b

Time in Therapeutic Range (TTR)
INR Data (Rocket-AF Nov 2010)
INR range
Warfarin
Median (25th, 75th)
<1.5 2.7 (0.0 – 9.0)
1.5 to <1.8 7.9 (3.5 – 14.0)
1.8 to <2.0 9.1 (5.3 – 13.6)
2.0 to 3.0 57.8 (43.0 – 70.5)
>3.0 to 3.2 4.0 (1.9 – 6.5)
>3.2 to 5.0 7.9 (3.3 – 13.8)
>5.0 0.0 (0.0 – 0.5)
Based on Rosendaal method with all INR values included
Based on Safety Population
“Taken together, the key message appears that Dabigatran
has clear advantages over warfarin in terms of its efficacy
(with the 150mg dose) and safety (with the 110mg dose)
but that the net benefit is attenuated (and possibly nullified),
when there is good or excellent anticoagulation control with
Warfarin, as defined by a TTR of >72% “.
Douketis 2011
Kennen Sie Ihren TTR?
66j. Patientin mit TVT Oberschenkel links, unprovoziert
schlecht einstellbar mit Markoumar (TTR<50%),
trotz häufiger INR, zT 2x/Woche, „will nicht mehr“.
Nach einem Canada-Aufenthalt in Vancouver kommt sie
mit einer Packung Dabigatran (2x150 mg) zurück („sei ja
auch wirksam und brauche keinen Quick (Cousine in
Vancouver habe Vorhofflimmern…)“
Dabigatran?
(Pradaxa)
Rivaroxaban
(Xarelto)
Fall 3c
Hausarzt Dr A.K. fragt ob er einen Pat mit unprovozierter
TVT nach 1 Monat umstellen solle und dürfe: Der TTR
sei sehr mit >75% sehr gut und der HA ruft mich an,
Umstellung auf das Dabigatran ?
Pat habe von der neuen Medikation gehört und möchte umstellen. Wie?
Timing?
Wie lange?
Monitoring?
Gerinnungstests? Reversibilität?
Dialyse?
Bleeding?
Fall 3 (Frage 2011/12)

Monitoring
aPTT
PTECT
TT
Thrombos Haemost 2010: 103:1116
Wenn die Thrombinzeit normal ist,
hats sicher kein Dabigatran an Bord
Monitoring
aPTT
PTECT
TT
Thrombos Haemost 2010: 103:1116

Does Benefit/Risk Support Exploration of Higher
Doses of Dabigatran? The FDAs View
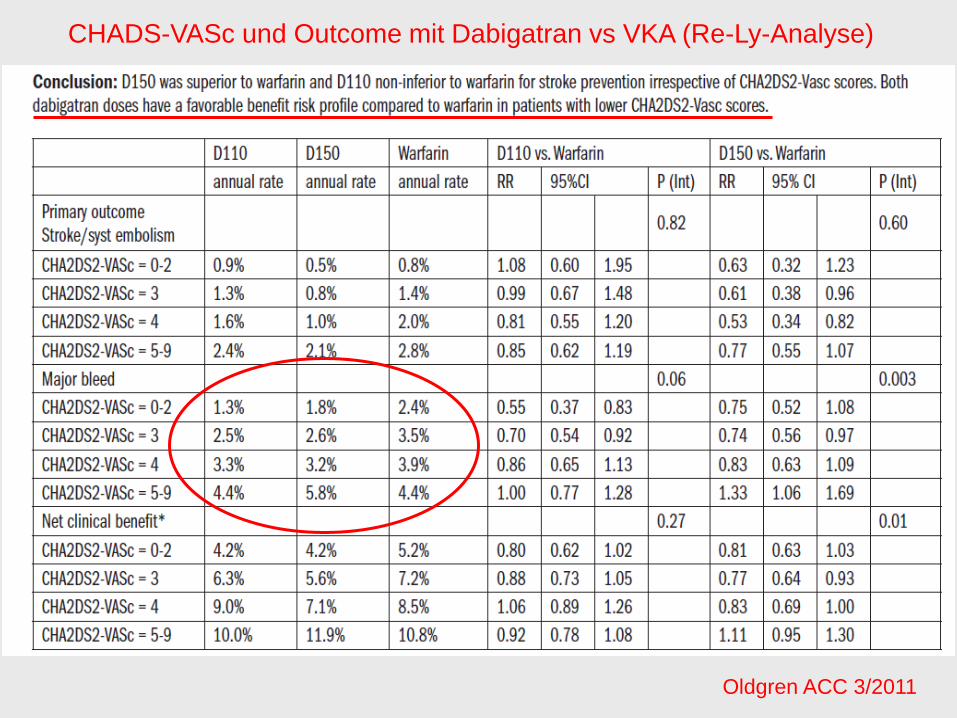
Oldgren ACC 3/2011
CHADS-VASc und Outcome mit Dabigatran vs VKA (Re-Ly-Analyse)

Circ 2011; 123: 2363 (mai 31)
Blutungen mit Dabigatran beim alten Menschen
Circ 2011; 123: 2363 (mai 31)
Blutungen mit Dabigatran beim alten Menschen

Circ 2011; 123: 2363 (mai 31)
Blutungen mit Dabigatran beim alten Menschen
Circ 2011; 123: 2363 (mai 31)
Blutungen mit Dabigatran in Komb mit Plättchenhemmern
Circ 2011; 123: 2363 (mai 31)
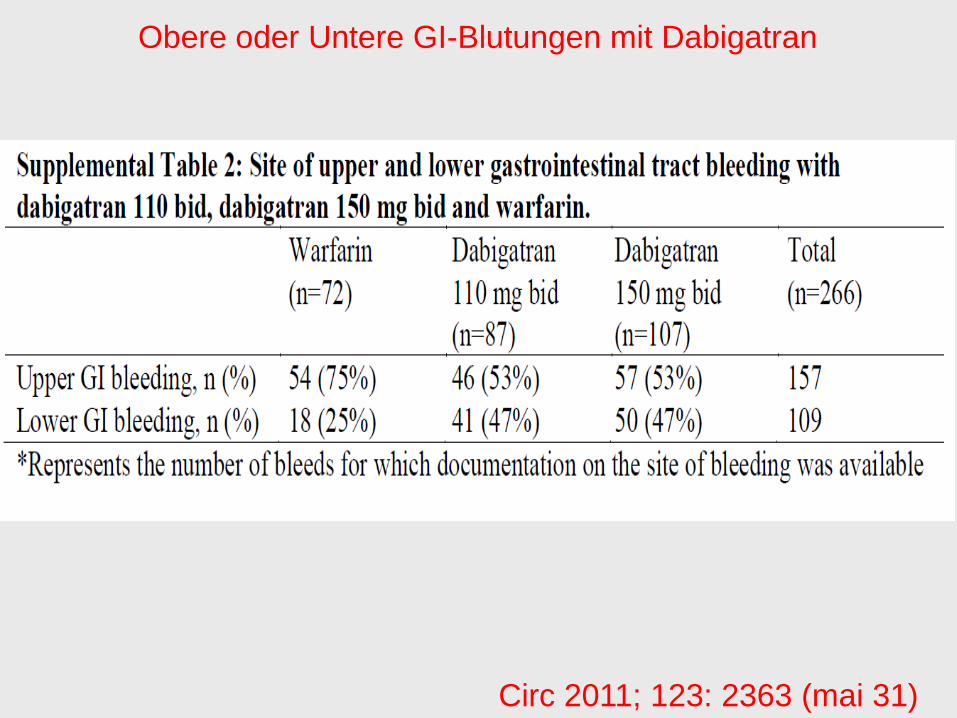
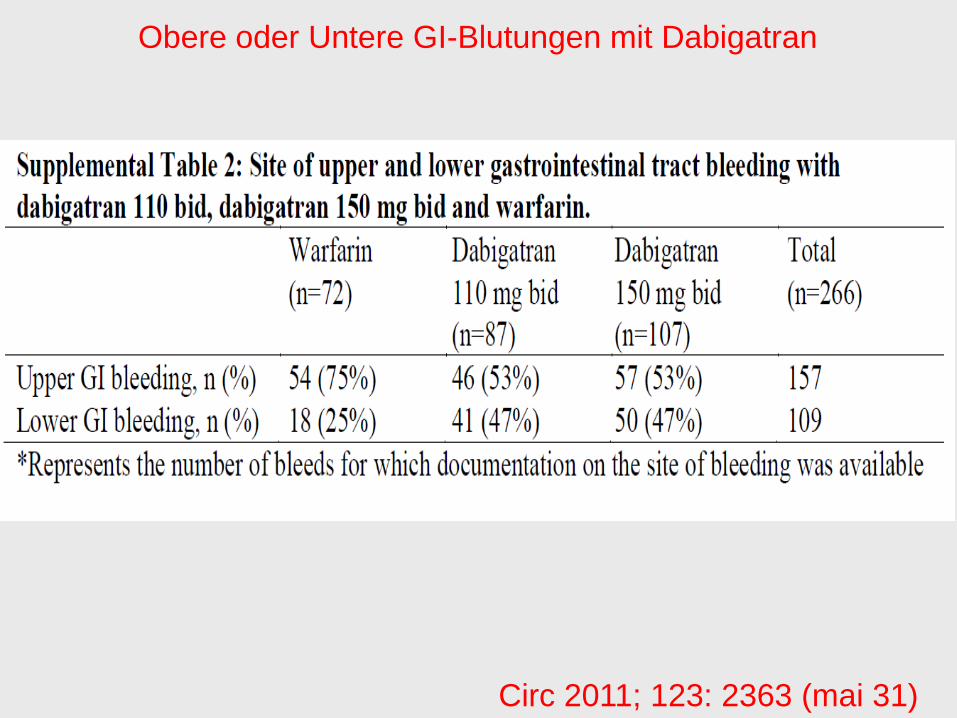
Obere oder Untere GI-Blutungen mit Dabigatran
Ann Int Med 2011;154:1

Die FDA Meinung
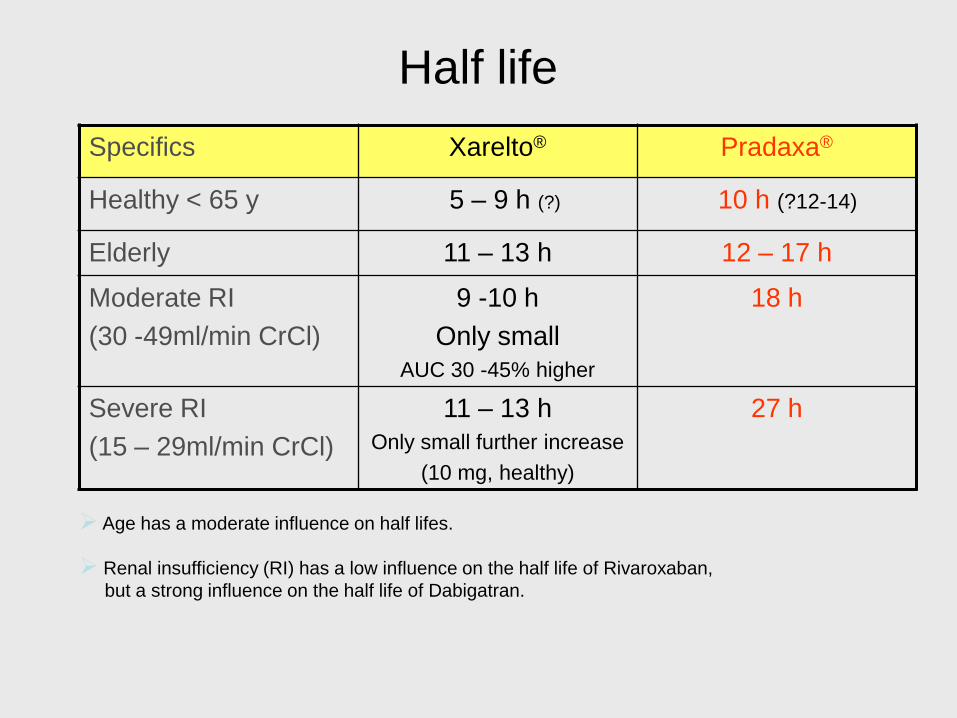
Half life
Specifics Xarelto® Pradaxa®
Healthy < 65 y 5 – 9 h (?) 10 h (?12-14)
Elderly 11 – 13 h 12 – 17 h
Moderate RI
(30 -49ml/min CrCl)
9 -10 h
Only small
AUC 30 -45% higher
18 h
Severe RI
(15 – 29ml/min CrCl)
11 – 13 h
Only small further increase
(10 mg, healthy)
27 h
Age has a moderate influence on half lifes.
Renal insufficiency (RI) has a low influence on the half life of Rivaroxaban,
but a strong influence on the half life of Dabigatran.

Half life: Dabigatran plasma
conc. curves
S. Harder, J Clin Pharmacol, 24 May 2011, online
after oral administration of dabigatran etexilate (50 or 150 mg)
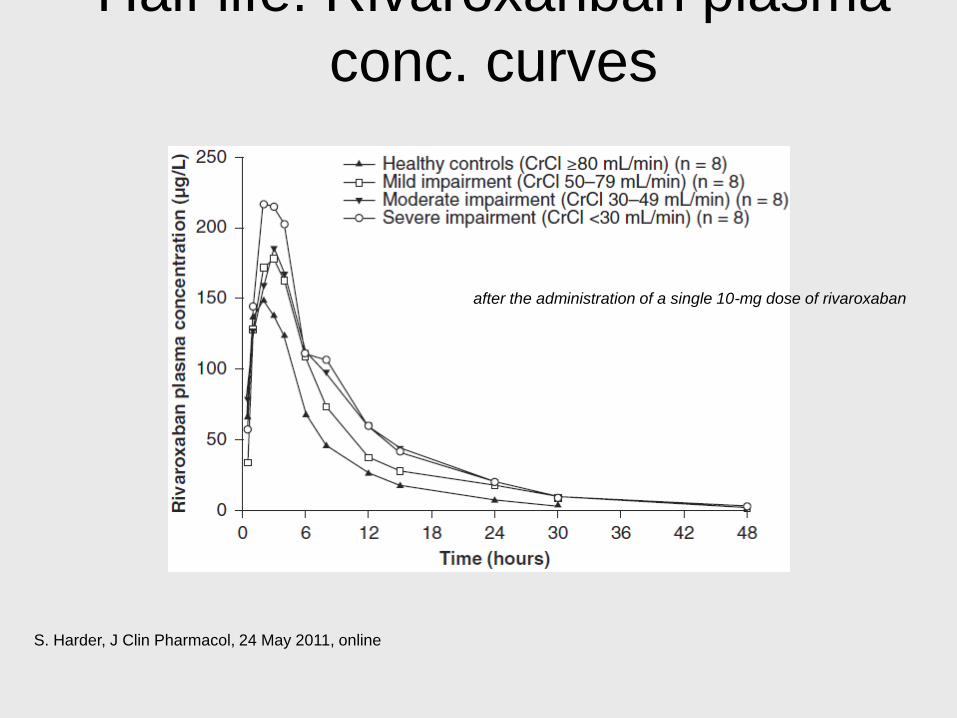
Half life: Rivaroxanban plasma
conc. curves
S. Harder, J Clin Pharmacol, 24 May 2011, online
after the administration of a single 10-mg dose of rivaroxaban
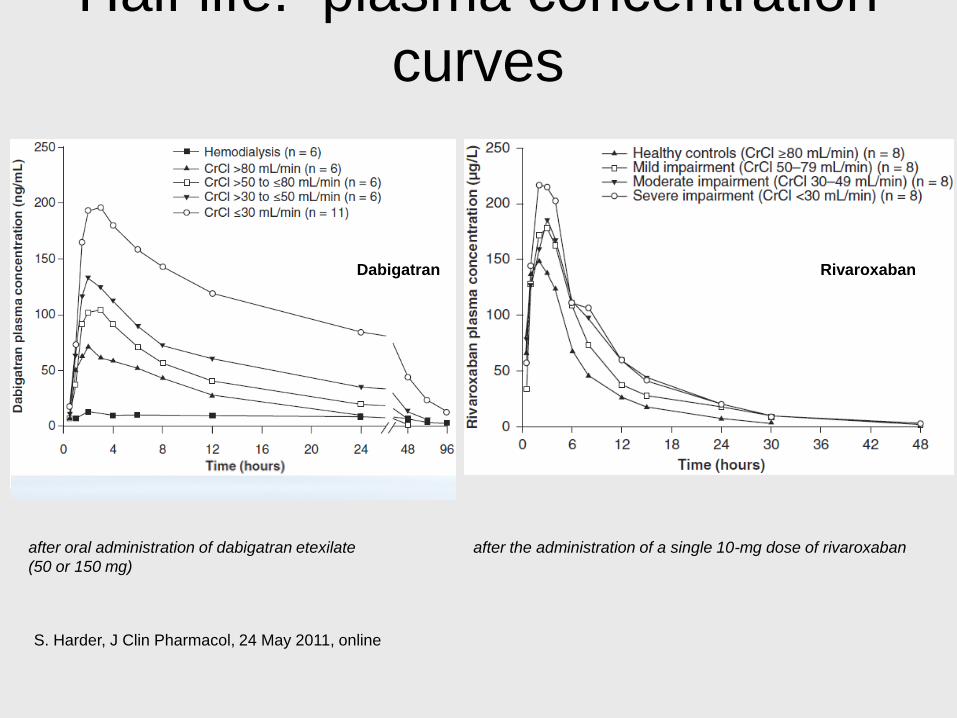
Half life: plasma concentration
curves
S. Harder, J Clin Pharmacol, 24 May 2011, online
Dabigatran Rivaroxaban
after oral administration of dabigatran etexilate
(50 or 150 mg)
after the administration of a single 10-mg dose of rivaroxaban
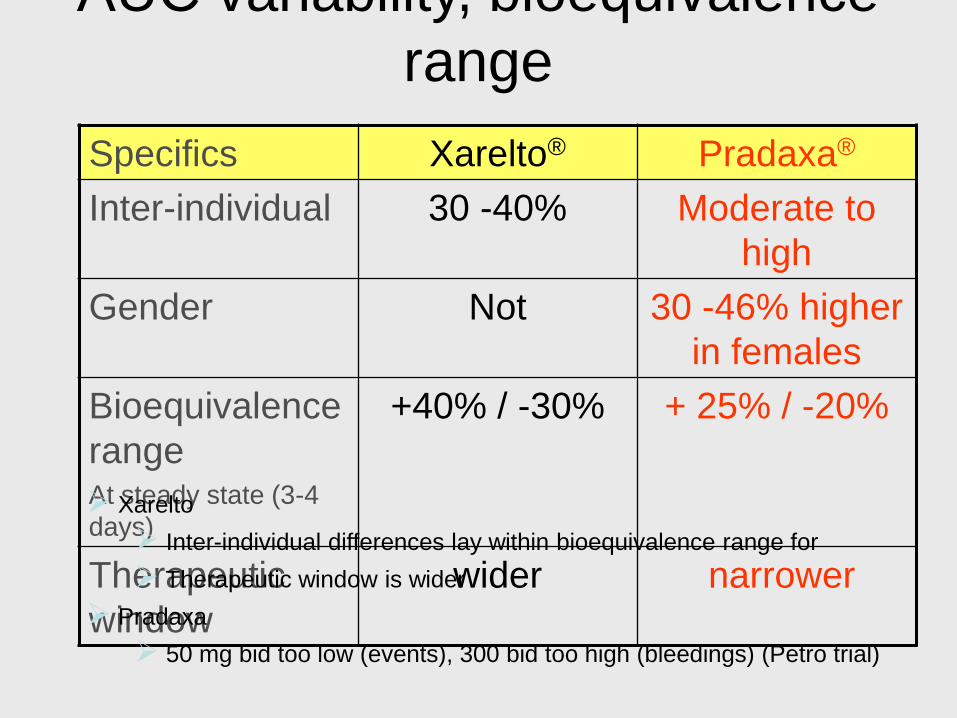
AUC variability, bioequivalence
range
Specifics Xarelto® Pradaxa®
Inter-individual 30 -40% Moderate to
high
Gender Not 30 -46% higher
in females
Bioequivalence
rangeAt steady state (3-4
days)
+40% / -30% + 25% / -20%
Therapeutic
window
wider narrower
Xarelto
Inter-individual differences lay within bioequivalence range for
Therapeutic window is wider
Pradaxa
50 mg bid too low (events), 300 bid too high (bleedings) (Petro trial)

Shallower dose–response
curve of Factor Xa suggests
wider safety margin• Thrombin only
activates clotting
over a narrow
concentration range;
Factor Xa functions
over a wider range.
– Dose–response
curves for DTIs and
direct Factor Xa
inhibitors would Esmon, ISTH 2005
0
20
40
60
80
100
120
0 50 100 150 200 250
Clo
ttin
g tim
e (
s)
Thrombin
Factor Xa
Enzyme dilution
These findings suggest that maintaining the appropriate dose
range for Factor Xa inhibitors may be easier than for DTIs

Phase II studies in VTE p OS:Low correlation of dose with efficacy,
all doses better than Enoxaparin
Eriksson et al. Circulation 2006;114:2374–2381.
40
30
20
10
0
0 5 10 20 30 40
Incid
ence –
effic
acy (
%)
Rivaroxaban (mg total daily dose)Enoxaparin
40 mg od
Shallow dose efficacy curve
En
ox
ap
arin
Riv
aro
xa
ba
n
Wide therapeutic window
Incidence of DVT, PE, and all-cause mortality
p=0.0852
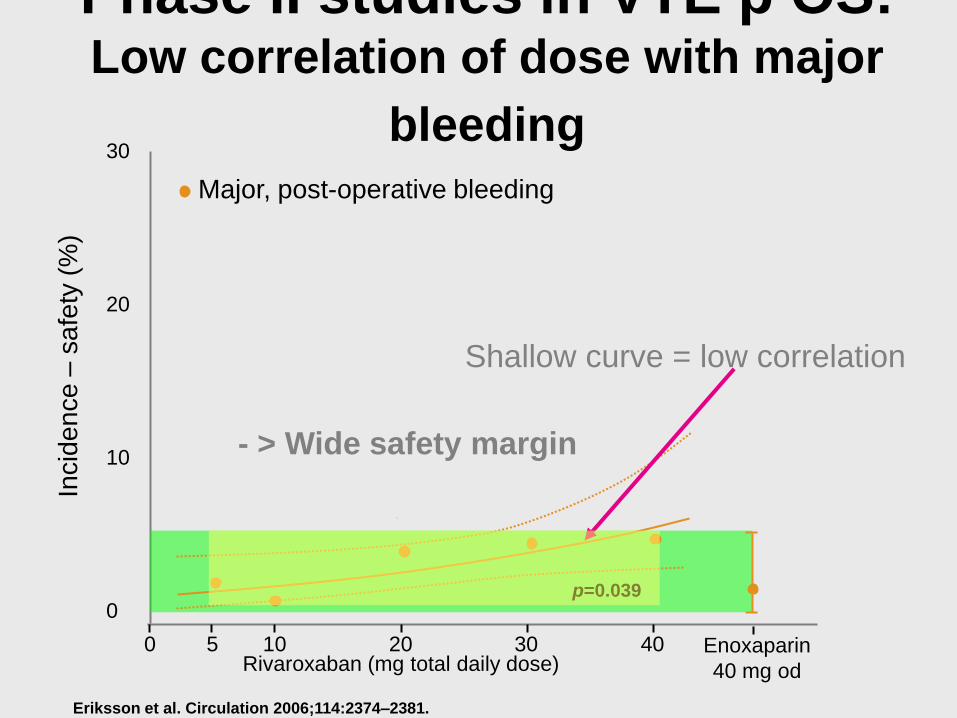
Phase II studies in VTE p OS:Low correlation of dose with major
bleeding
Eriksson et al. Circulation 2006;114:2374–2381.
30
20
10
0
0 5 10 20 30 40Rivaroxaban (mg total daily dose)
Enoxaparin
40 mg od
Incid
en
ce
–sa
fety
(%
)
p=0.039
Major, post-operative bleeding
Shallow curve = low correlation
- > Wide safety margin
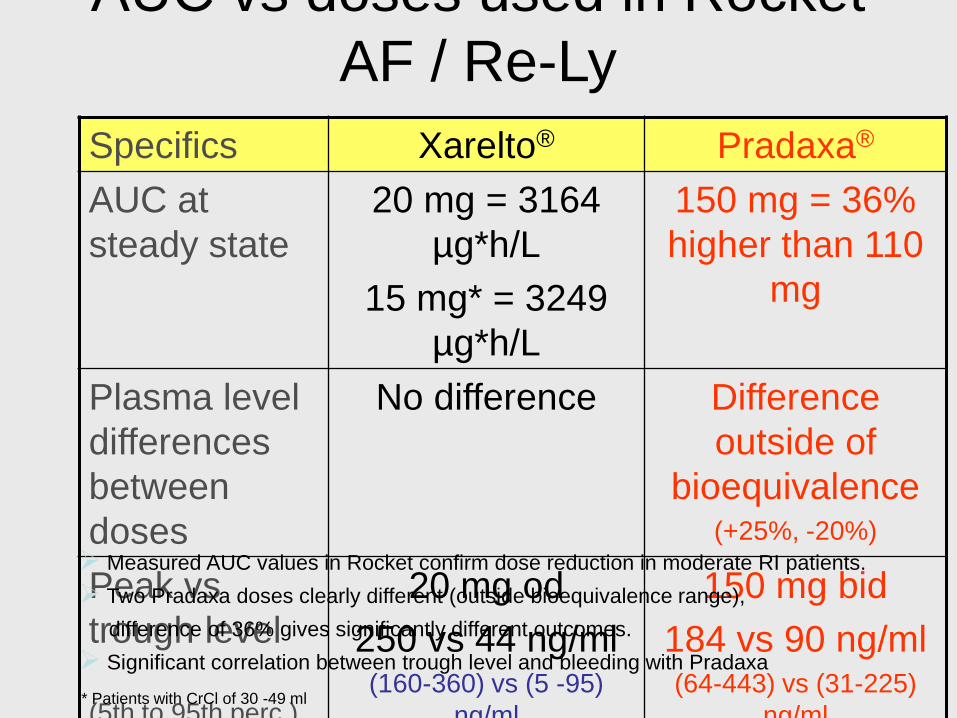
AUC vs doses used in Rocket
AF / Re-Ly
Specifics Xarelto® Pradaxa®
AUC at
steady state
20 mg = 3164
µg*h/L
15 mg* = 3249
µg*h/L
150 mg = 36%
higher than 110
mg
Plasma level
differences
between
doses
No difference Difference
outside of
bioequivalence(+25%, -20%)
Peak vs
trough level
(5th to 95th perc.)
20 mg od
250 vs 44 ng/ml (160-360) vs (5 -95)
ng/ml
150 mg bid
184 vs 90 ng/ml(64-443) vs (31-225)
ng/ml
Measured AUC values in Rocket confirm dose reduction in moderate RI patients.
Two Pradaxa doses clearly different (outside bioequivalence range),
difference of 36% gives significantly different outcomes.
Significant correlation between trough level and bleeding with Pradaxa
* Patients with CrCl of 30 -49 ml
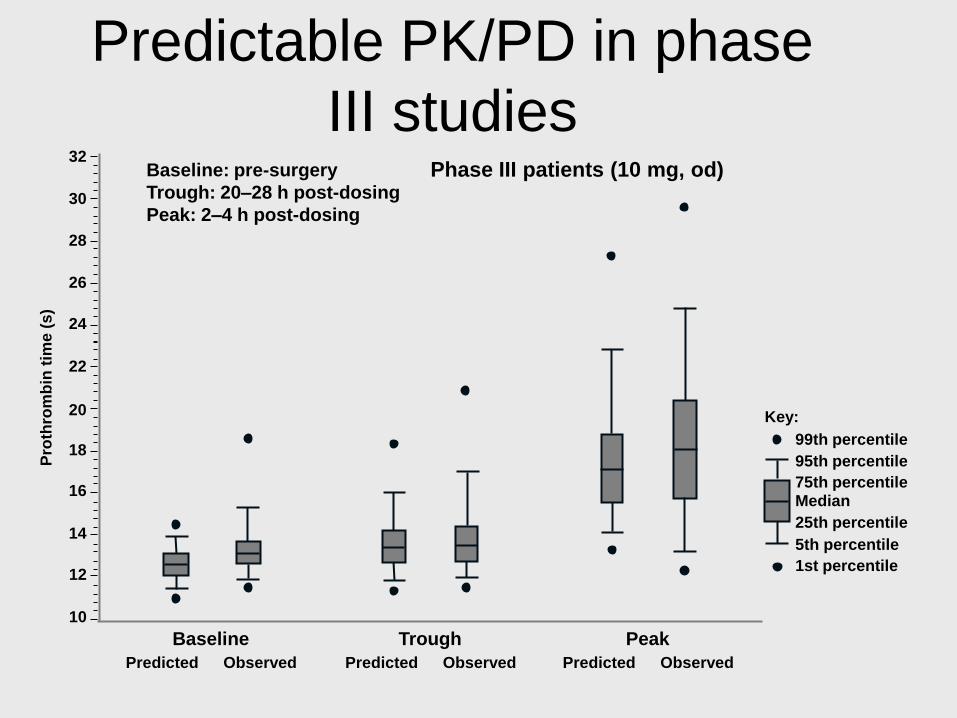
99th percentile
95th percentile
75th percentileMedian
25th percentile
5th percentile
1st percentile
Key:
Phase III patients (10 mg, od)
10
12
14
16
18
20
22
24
26
28
30
32
Baseline
Predicted Observed
Trough
Predicted Observed
Peak
Predicted Observed
Pro
thro
mb
in t
ime
(s)
Baseline: pre-surgery
Trough: 20–28 h post-dosing
Peak: 2–4 h post-dosing
Predictable PK/PD in phase
III studies

Bioavailability
Specifics Xarelto® Pradaxa®
Healthy subjects 80-100 % 3-7%
pH dependent No Yes, plasma level
reductions with PPIs
Food dependent? 10 mg no,
15-20 mg with food
(39% AUC incr.)
No, but with food 2h
longer to Cmax
Dyspesia stronger
without food
Linear up take? No, ceiling >50 mg Yes, up to 600 mg
Greater variability in bioavailability with Pradaxa

Metabolism / elimination
Specifics Xarelto® Pradaxa®
Prodrug No, active substance Yes, hydrolized by
esterases
Liver, CYP 450 system 66% (CYP 3A4 u.a.) No hepatic
metabolization
Liver, glucuronidation Not observed Yes, into 4 different
substances
Liver interaction Not an inducer or a
inhibitor of the CYP
system
Not an inducer or a
inhibitor of the CYP
system
Kidney 33% active substance,
33% inactive metabolites
>85% active substance
Xarelto
dual mode of elimination
no surprises due to polymorphism in prodrug metabolization
Renal elimination only modest -> less accumulation in RI

Relevant interactions with other drugs
Specifics drugs Xarelto® Pradaxa®
With moderate CYP
inhibitors
acetaminophen, cyclosporine, erythromycin,
nifedipine, felodipine, midazolam, triazolam,
simvastatin, atorvastatin
No No
With strong CYP
inhibitors
Clarithromycine Yes, use
another
antibiotic
No
With P-gp inhibitors Quinidine,
Verapamil, Amiodarone,
Clopidogrel
No
No
no
Yes, do not combine
Yes, use with
caution
Yes, level increases
With strong CYP and
P-gp inhibitors
Ketoconazol (azole antimycotica)
Ritonavir (HIV protease inhibitors)
Avoid Avoid
With CYP inductors phenobarbital type inducers,
dexamethasone, phenytoin,
carbamazepine, and St. John’s wort
No, not
clinical
relevant
no
With strong CYP and
P-gp inductors
Rifampicin, Avoid Avoid
*Am J Manag Care 2009; 15 (6): e22-33
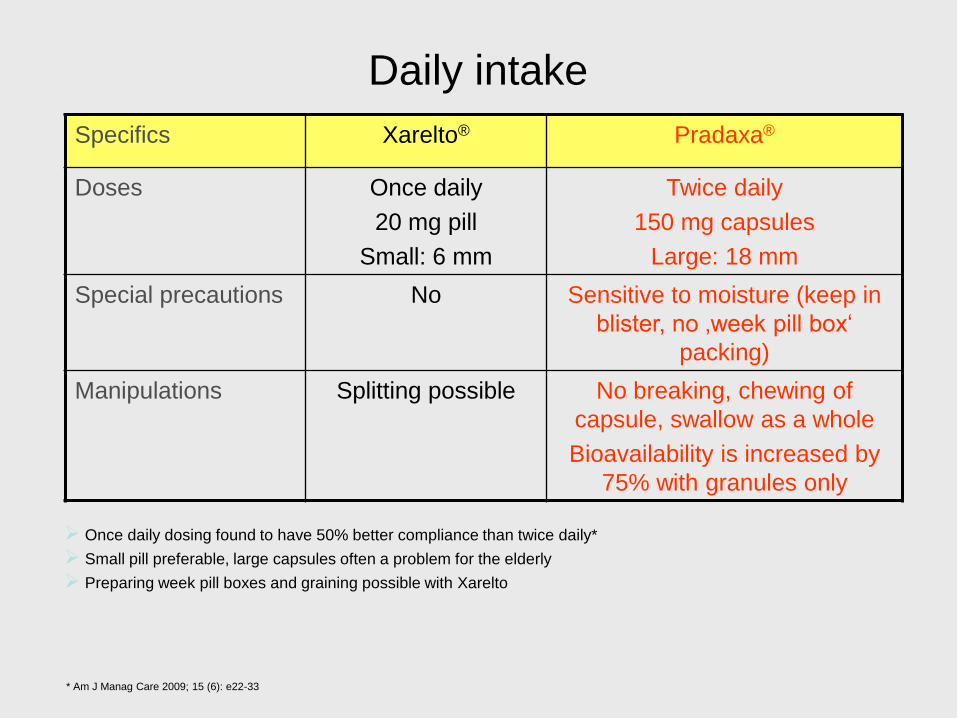
Daily intake
Specifics Xarelto® Pradaxa®
Doses Once daily
20 mg pill
Small: 6 mm
Twice daily
150 mg capsules
Large: 18 mm
Special precautions No Sensitive to moisture (keep in
blister, no ‚week pill box‘
packing)
Manipulations Splitting possible No breaking, chewing of
capsule, swallow as a whole
Bioavailability is increased by
75% with granules only
Once daily dosing found to have 50% better compliance than twice daily*
Small pill preferable, large capsules often a problem for the elderly
Preparing week pill boxes and graining possible with Xarelto
* Am J Manag Care 2009; 15 (6): e22-33
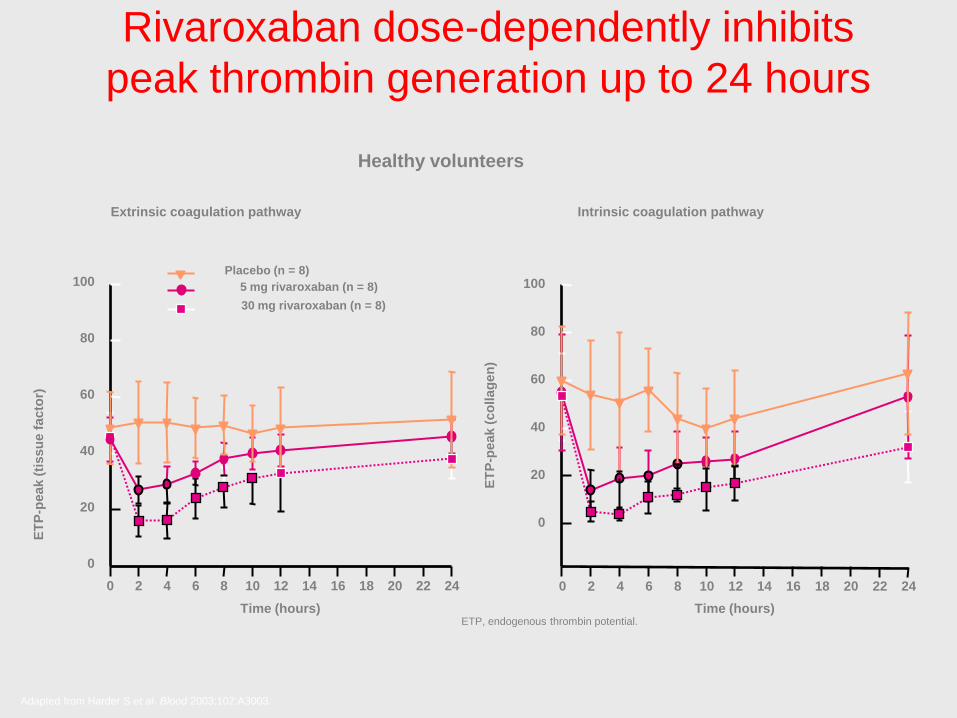
Rivaroxaban dose-dependently inhibits
peak thrombin generation up to 24 hours
Healthy volunteers
ETP, endogenous thrombin potential.
0 2 4 6 8 10 12 14 16 18 20
ET
P-p
eak (
co
llag
en
)
0
20
40
60
80
100
Time (hours)
0 2 4 6 8 10 12 14 16 18 20 22 24
ET
P-p
eak (
tissu
e f
acto
r)
0
20
40
60
80
100
Time (hours)
30 mg rivaroxaban (n = 8)
5 mg rivaroxaban (n = 8)
Placebo (n = 8)
Intrinsic coagulation pathwayExtrinsic coagulation pathway
Adapted from Harder S et al. Blood 2003;102:A3003.
22 24

One dose for all patients?
Specifics Xarelto® Pradaxa®
Age (>18y) No age limit (97y max)
Low influence so fare
Further analysis needed
71y (+/-8.8)
Bleeding pattern
significantly different in
age goups
Weight Low influence so far
VTEp OS
>100 kg, trend to VKA
better (110 significantly
better than 150)
Co-medications More bleeding with
ASS, but similar in both
arms
Most other common
drugs have low
influence
More bleeding with
ASS, but similar in both
arms, use ASS with
caution
PPI, Amiodarone,
Quinidine influence
plasma conc, trend to
worser outcome
*Am J Manag Care 2009; 15 (6): e22-33

Dose adjustements in renal insufficiency
Specifics Xarelto® Pradaxa®
>50 – 80 ml / Cr Cl No, 20 mg; od No, 150 mg; bid
30 -49 ml / Cr Cl Yes, SPAF 15 mg; od No, 150 mg; bid
15 – 29 ml CrCL 15 mg (very few
patients)
VTE p OS (10 mg) use
with caution
75 mg only in US,
Contra-indicated in
VTE p OS
< 15 ml CrCl Not recommended Contra-indicated
Dose adjustements in ROCKET AF by intention to get homegeneous
AUC down to 30 ml CrCl. All patient can be pooled.
Unclear situation with Pradaxa, different dose recommendations in US
(75 mg), CAN and EU likely
75 mg Pradaxa dose not studied
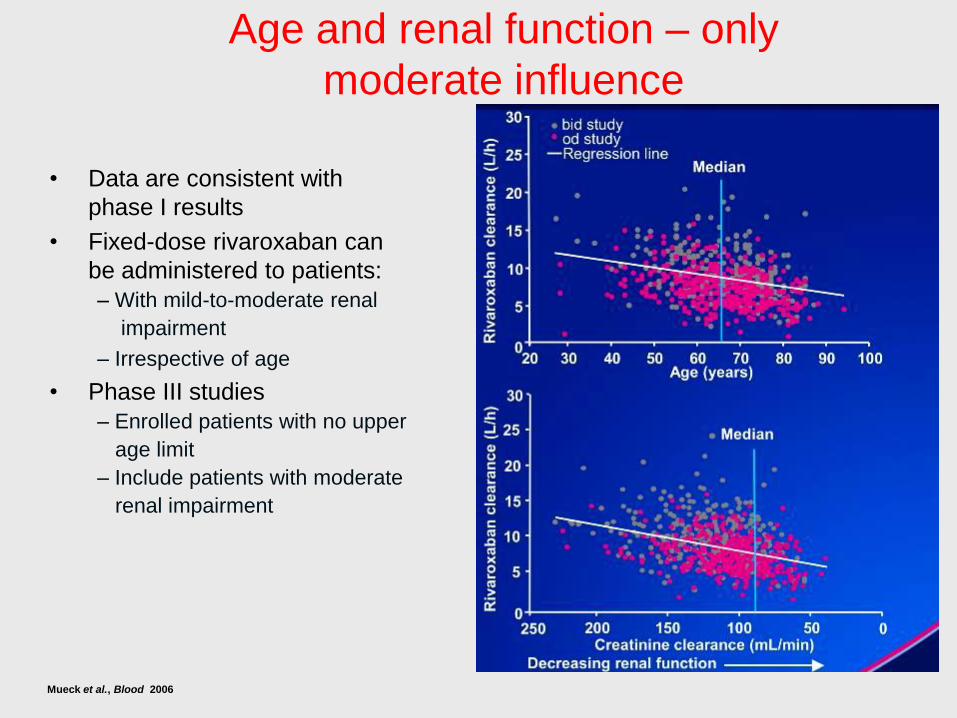
Age and renal function – only
moderate influence
• Data are consistent with
phase I results
• Fixed-dose rivaroxaban can
be administered to patients:
– With mild-to-moderate renal
impairment
– Irrespective of age
• Phase III studies
– Enrolled patients with no upper
age limit
– Include patients with moderate
renal impairment
Mueck et al., Blood 2006
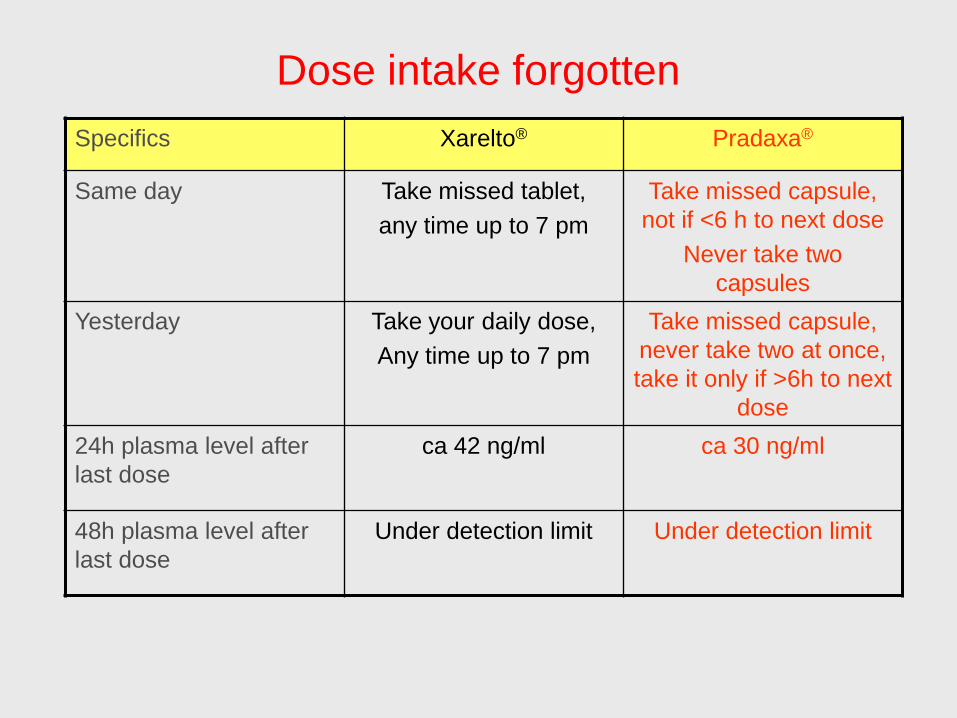
Dose intake forgotten
Specifics Xarelto® Pradaxa®
Same day Take missed tablet,
any time up to 7 pm
Take missed capsule,
not if <6 h to next dose
Never take two
capsules
Yesterday Take your daily dose,
Any time up to 7 pm
Take missed capsule,
never take two at once,
take it only if >6h to next
dose
24h plasma level after
last dose
ca 42 ng/ml ca 30 ng/ml
48h plasma level after
last dose
Under detection limit Under detection limit
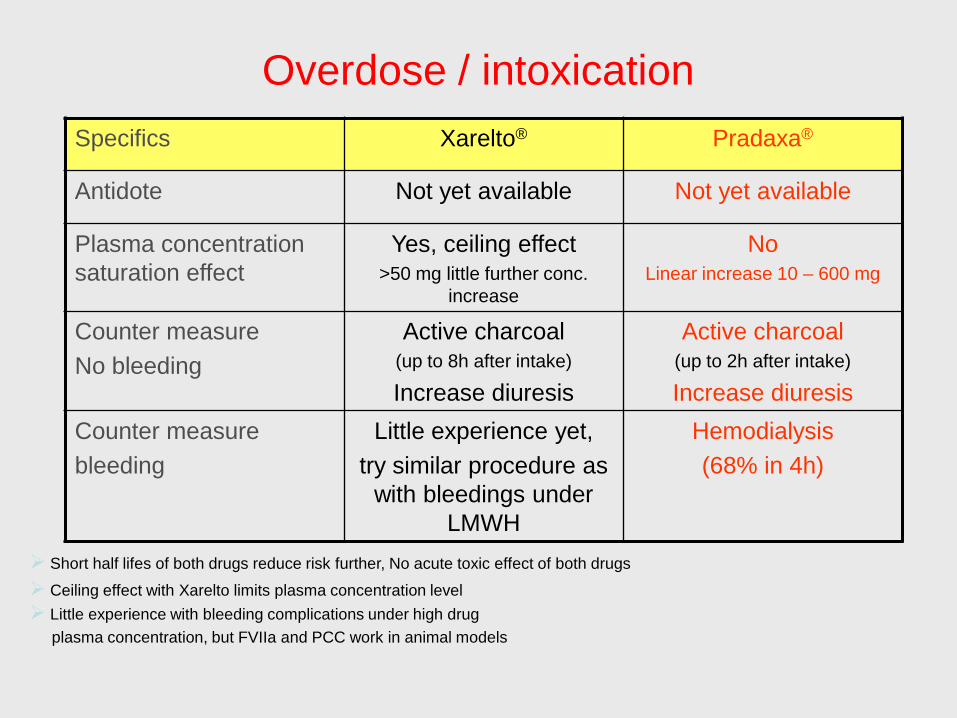
Overdose / intoxication
Specifics Xarelto® Pradaxa®
Antidote Not yet available Not yet available
Plasma concentration
saturation effect
Yes, ceiling effect>50 mg little further conc.
increase
NoLinear increase 10 – 600 mg
Counter measure
No bleeding
Active charcoal (up to 8h after intake)
Increase diuresis
Active charcoal(up to 2h after intake)
Increase diuresis
Counter measure
bleeding
Little experience yet,
try similar procedure as
with bleedings under
LMWH
Hemodialysis
(68% in 4h)
Short half lifes of both drugs reduce risk further, No acute toxic effect of both drugs
Ceiling effect with Xarelto limits plasma concentration level
Little experience with bleeding complications under high drug
plasma concentration, but FVIIa and PCC work in animal models
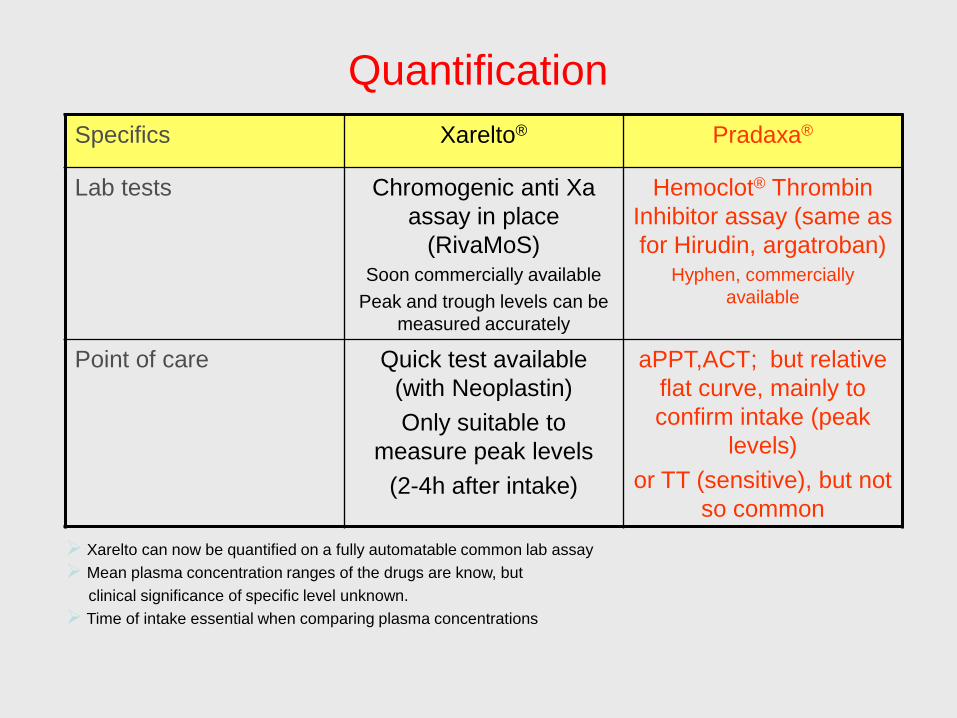
Quantification
Specifics Xarelto® Pradaxa®
Lab tests Chromogenic anti Xa
assay in place
(RivaMoS)Soon commercially available
Peak and trough levels can be
measured accurately
Hemoclot® Thrombin
Inhibitor assay (same as
for Hirudin, argatroban) Hyphen, commercially
available
Point of care Quick test available
(with Neoplastin)
Only suitable to
measure peak levels
(2-4h after intake)
aPPT,ACT; but relative
flat curve, mainly to
confirm intake (peak
levels)
or TT (sensitive), but not
so common
Xarelto can now be quantified on a fully automatable common lab assay
Mean plasma concentration ranges of the drugs are know, but
clinical significance of specific level unknown.
Time of intake essential when comparing plasma concentrations
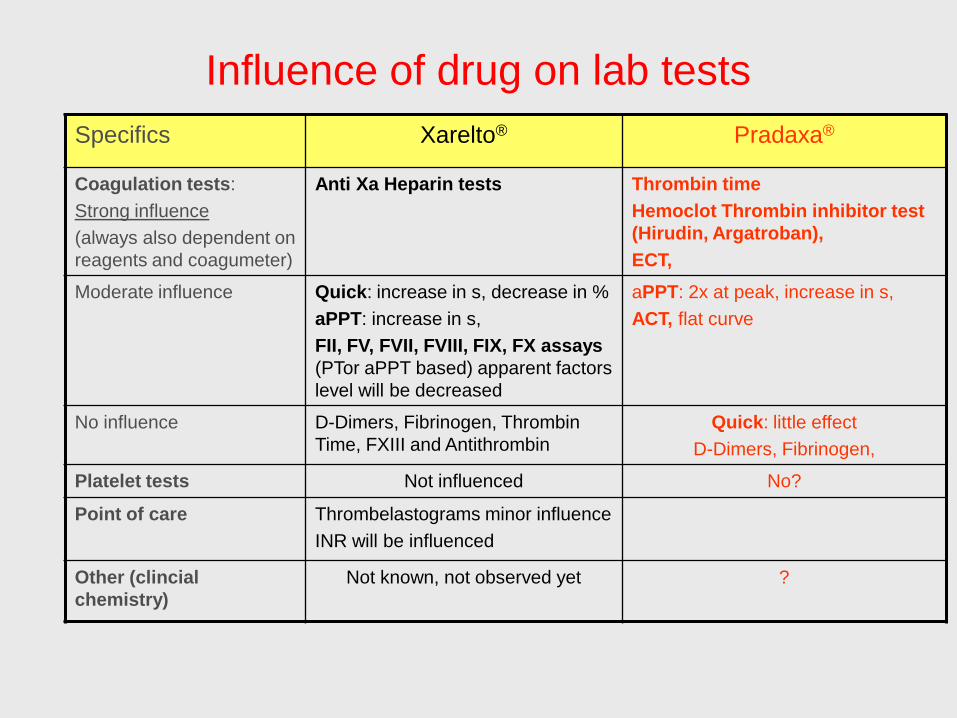
Influence of drug on lab tests
Specifics Xarelto® Pradaxa®
Coagulation tests:
Strong influence
(always also dependent on
reagents and coagumeter)
Anti Xa Heparin tests Thrombin time
Hemoclot Thrombin inhibitor test
(Hirudin, Argatroban),
ECT,
Moderate influence Quick: increase in s, decrease in %
aPPT: increase in s,
FII, FV, FVII, FVIII, FIX, FX assays
(PTor aPPT based) apparent factors
level will be decreased
aPPT: 2x at peak, increase in s,
ACT, flat curve
No influence D-Dimers, Fibrinogen, Thrombin
Time, FXIII and Antithrombin
Quick: little effect
D-Dimers, Fibrinogen,
Platelet tests Not influenced No?
Point of care Thrombelastograms minor influence
INR will be influenced
Other (clincial
chemistry)
Not known, not observed yet ?

Baseline Demographics
Topic specifics Xarelto 20 mg Pradaxa 150 mg
Rocket AF Re-Ly
Age years 73 71.5
>75 years 43.80%
Females 40% 36.80%
Race white 83% 70.20%
Asian 13%
Region North America 19% 36%
Latin America 13% 5.30%
Asia Pacific 15% 15.40%
Central EU 38% 11.60%
Western EU 15% 25.60%
VKA naive 37.70% 49.80%
never used 31.40%
CrCL median 67 ml 67.9 ml
31- 50 ml 21%
50-80 ml 47%
>80 ml 32%
AF type persistent/permanent 81% 67.40%
paroxysmal 18% 32.60%
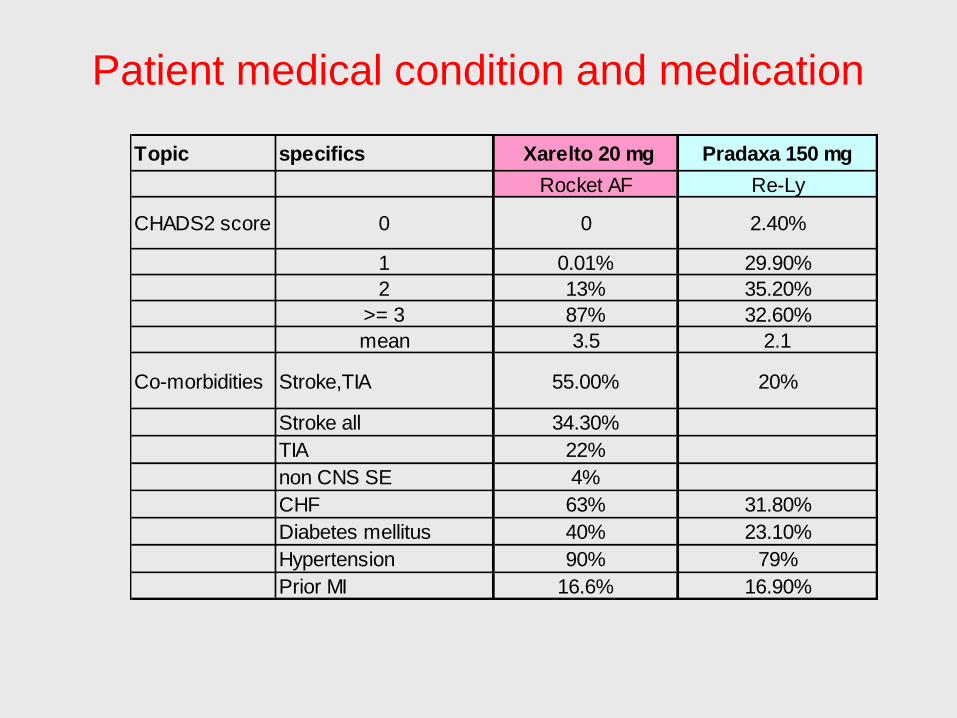
Patient medical condition and medication
Topic specifics Xarelto 20 mg Pradaxa 150 mg
Rocket AF Re-Ly
CHADS2 score 0 0 2.40%
1 0.01% 29.90%
2 13% 35.20%
>= 3 87% 32.60%
mean 3.5 2.1
Co-morbidities Stroke,TIA 55.00% 20%
Stroke all 34.30%
TIA 22%
non CNS SE 4%
CHF 63% 31.80%
Diabetes mellitus 40% 23.10%
Hypertension 90% 79%
Prior MI 16.6% 16.90%

Patient medical condition and medication – ctd.
Topic specifics Xarelto 20 mg Pradaxa 150 mg
Rocket AF Re-Ly
Co-Medication ASA during study 35% (relevant)39% (any time)
19.6% (always)
ASA prior study 37% 38.50%
Clopidogrel prior study 2.3% 5.50%
Clopidogrel during
study3.4% 2.20%
ASS & Clopidogrel prior
study3.50%
ASS & Clopidogrel
during study1.10%

Patient flow
Topic specifics Xarelto 20 mg Pradaxa 150 mg
Rocket AF Re-Ly
Number of
patientsScreeing 17'232 20'382
total ITT population 14'264 18'113
total Safety population 14'236 18'040
total Per-protocol
population14'054 17'630
on study drug 7'008 6'059
on Warfarin 7'046 5'998
Completed on study
medication4'591 4'627
stopped study
medication, but
completed study
2520 (35.4%) 1197 (19.8%)
stopped on warfarin 2468 (34,6%) 907 (15%)
Difference in early
discontinuation vs
warfarin
no difference
about 4.8% higher in
the DE arm than
warfarin

NEJM 2003; 349:1019
0.6 0.35



Neue Antikoagulantien:
Heutige Ziele:
1. Update 7. Monitoring
2. Off-label 8. 3.Welt
3. Compliance vs TTR 9. Zulassungen
4. Bleeds: ICB and GI 10. Kosten
5. 80+ 11. Triple Therapie m PH
6. CCreat 12. Individuelles Massschneidern
ZusammenfassungDer Zug hat die Station verlassen
Individualisierte Therapien möglich
Effektivere Antikoagulantien sind bereits zugelassen
Weitere werden folgen. Patienten und Aerzte haben schon entschieden.
Bedeutung der
Compliance bei
kurzen
Halbwertszeiten
1x/d oder 2x/d?

Markoumar
und…ASA etc?

Circ 2011; 123: 2363 (mai 31)
Obere oder Untere GI-Blutungen mit Dabigatran
Pat mit Vorhofflimmern: Welches ist mein alljährliches
Risiko, eine intracerebrale Blutung unter diesen
Antikoagulantien zu erleiden?
Patienten Fragen
Anti IIa und anti Xa vs VKAHeutige Ziele: Einsatz beim Vorhofflimmern
(Prophylaxe und Therapie der TE)1. Der alte Mann und das Meer (von neuen Medikamenten)
2. Tod, TE vs Blutungen, ICB
3. Kombinationen mit P-Hemmern
4. NW, Hepatotoxizität
5. Nahrung, Medikamenteninteraktionen
6. Monitoring?
7. Antagonisierung/Procedere bei Blutungen
8. Neueste Daten
9. TTR des INR als allg Qualitätsmarker –
10.T ½, Dosis-Intervall, und Compliance
11.Langzeiteffekt und Sicherheit
12.Preis
13.Individualisierung der Therapie
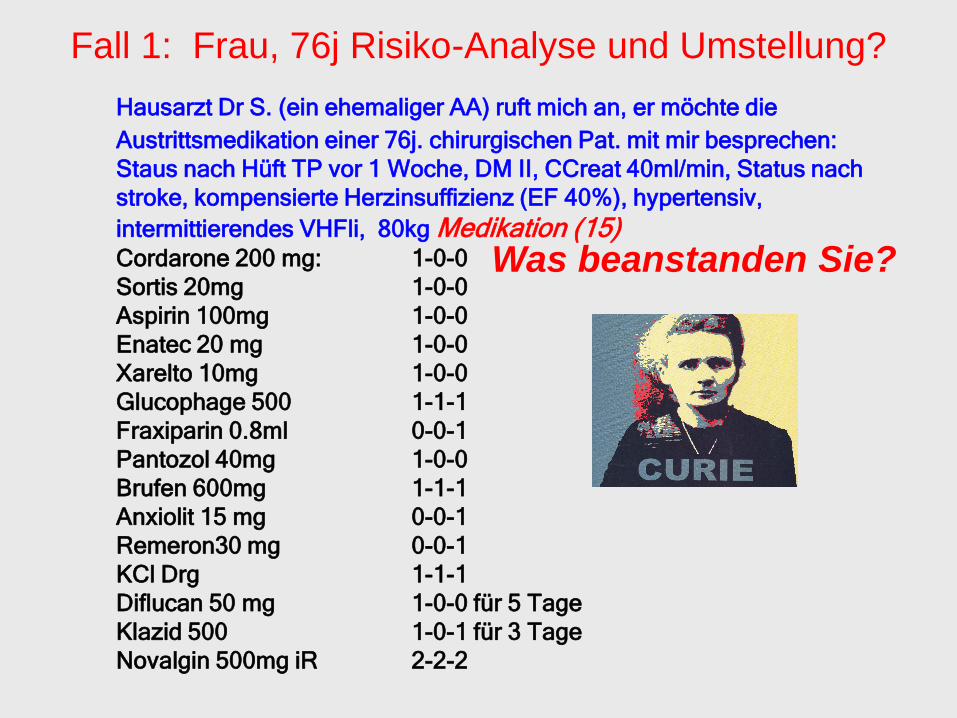
Hausarzt Dr S. (ein ehemaliger AA) ruft mich an, er möchte die
Austrittsmedikation einer 76j. chirurgischen Pat. mit mir besprechen:
Staus nach Hüft TP vor 1 Woche, DM II, CCreat 40ml/min, Status nach
stroke, kompensierte Herzinsuffizienz (EF 40%), hypertensiv,
intermittierendes VHFli, 80kg Medikation (15) Cordarone 200 mg: 1-0-0
Sortis 20mg 1-0-0
Aspirin 100mg 1-0-0
Enatec 20 mg 1-0-0
Xarelto 10mg 1-0-0
Glucophage 500 1-1-1
Fraxiparin 0.8ml 0-0-1
Pantozol 40mg 1-0-0
Brufen 600mg 1-1-1
Anxiolit 15 mg 0-0-1
Remeron30 mg 0-0-1
KCl Drg 1-1-1
Diflucan 50 mg 1-0-0 für 5 Tage
Klazid 500 1-0-1 für 3 Tage
Novalgin 500mg iR 2-2-2
Fall 1: Frau, 76j Risiko-Analyse und Umstellung?
Was beanstanden Sie?

Scientific American 2011
Fall 1: Die Limiten der Intelligenz
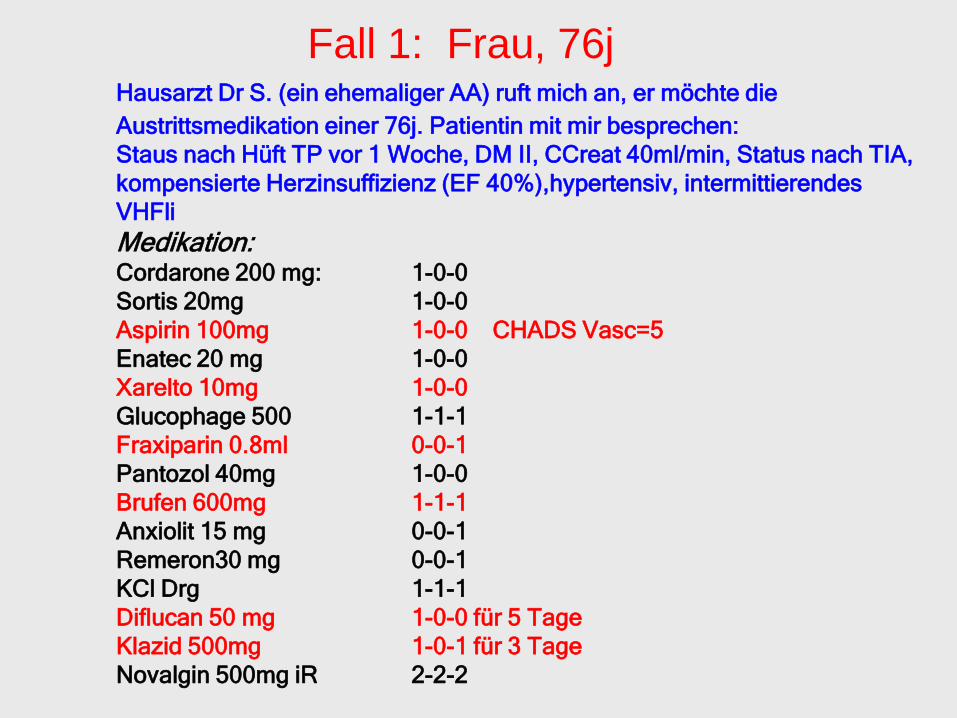
Hausarzt Dr S. (ein ehemaliger AA) ruft mich an, er möchte die
Austrittsmedikation einer 76j. Patientin mit mir besprechen:
Staus nach Hüft TP vor 1 Woche, DM II, CCreat 40ml/min, Status nach TIA,
kompensierte Herzinsuffizienz (EF 40%),hypertensiv, intermittierendes
VHFli
Medikation:Cordarone 200 mg: 1-0-0
Sortis 20mg 1-0-0
Aspirin 100mg 1-0-0 CHADS Vasc=5
Enatec 20 mg 1-0-0
Xarelto 10mg 1-0-0
Glucophage 500 1-1-1
Fraxiparin 0.8ml 0-0-1
Pantozol 40mg 1-0-0
Brufen 600mg 1-1-1
Anxiolit 15 mg 0-0-1
Remeron30 mg 0-0-1
KCl Drg 1-1-1
Diflucan 50 mg 1-0-0 für 5 Tage
Klazid 500mg 1-0-1 für 3 Tage
Novalgin 500mg iR 2-2-2
Fall 1: Frau, 76j
Welches ist mein alljährliches Risiko, einen Hirnschlag
oder eine Embolie zu erleiden?
Patienten Fragen
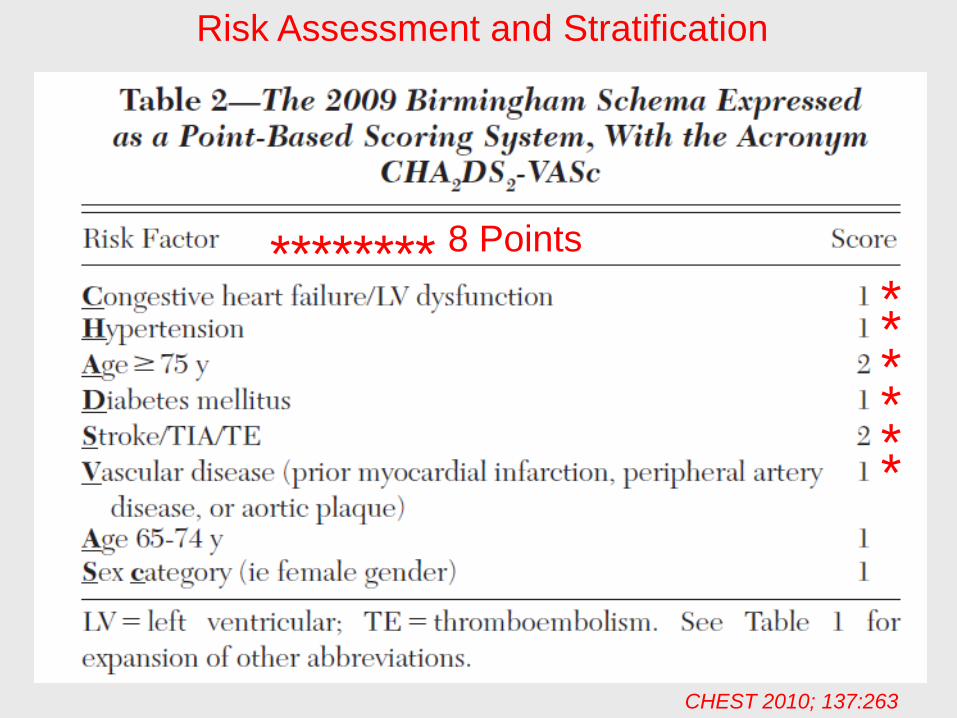
Risk Assessment and Stratification
CHEST 2010; 137:263
8 Points**************

Risk Assessment and Stratification: CHADS-VASc
CHEST 2010; 137:263
Ca 10%

Welches ist mein alljährliches Risiko, eine schwere
Blutung zu erleiden?
Patienten Fragen

Def Major Bleeds: Any bleed requiring hospitalisation, decrease of Hb >2g% or transfusion
CHEST 2010/3/18 online
Our Patient:4-5 points
*
*
**
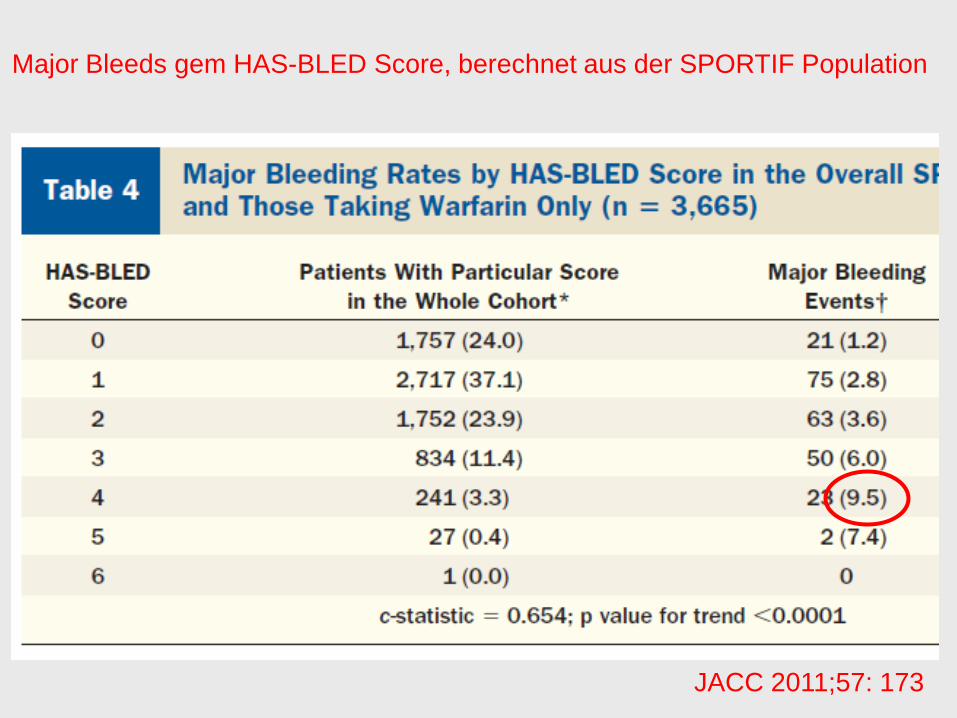
Major Bleeds gem HAS-BLED Score, berechnet aus der SPORTIF Population
JACC 2011;57: 173
Wie ist denn das Nutzen-Risikoverhältnis bei den
Neueren AK resp. auf welches sollte ich denn
umstellen?
Patienten Fragen
„Plasmatic“ „Platelet“
Rivaroxaban*
Apixaban*
Otamixaban
Edoxaban*
Betrixa Eribaxa.…
vWF
ADP
LMWH/UFH
Fondaparinux
[Idraparinux]
Idrabiotaparinux
Aspirin
Platelet
activation
Secretion
P2Y12R
TxA2
TxA2R
Endothelial
Lesion
GP
II b
GP
III
a
Activation
Cangrelor
Ticagrelor
Clopidogrel
Prasugrel
Elinogrel
GP
II b
GP
III
a
GP
II b
GP
III
aPlatelet-Fibrinogen-
Network
Fibrin FibrinogenAbxicimab
Tirofiban
Eptifibatide
IX
IXa
VIIIa
XIa
GP
II b
GP
III
a
II
IIa
LMWH/UFH
Bivalirudin
Lepirudin
Dabigatran*
[Ximelagatran]
AZD0837
SCH530348
ADP
TxA2
Terutruban
E5555
GP
Ia/IIa GP Ib/IX/V
Ge
bh
ard
& B
ee
r 2
01
0
aFIXa aptamer
avWF aptamer
aFXI
Kollateral-Nutzen oder –Schaden der
Thrombinhemmer?
Platelet activation
Vasoconstriction
Growth Factor (SMC) ?
Inflammatory Mediator
Thombomodulin/Protein C ?
Infection control?

Orale Bioverfügbarkeit ~6.5%
Mittlere Halbwertszeit 14–17h in
Gesunden unabhängig von der Dosis
NH2
N
NH
N
N
CH3
N
OO
O
N
O
O CH3
CH3
Dabigatran etexilate
Nicht metabolisiert durch CYP450 Enzyme, und interferiert nicht mit dem
Metabolismus anderer Medi, die dieses System brauchen.
Medi-Interferenzen; GP1 (Cordarone +50%) Rifampicin, Tenofivir,
Clarithromycin, Verapamil und Chinidin
80% renale Ausscheidung
Keine Interferenz mit Nahrungsmitteln
Bisher kein spezifisches Antidot verfügbar ****
Kontraindiziert bei CCr < 30 ml/min
Dyspepsie in 5%
Dabigatran etexilate
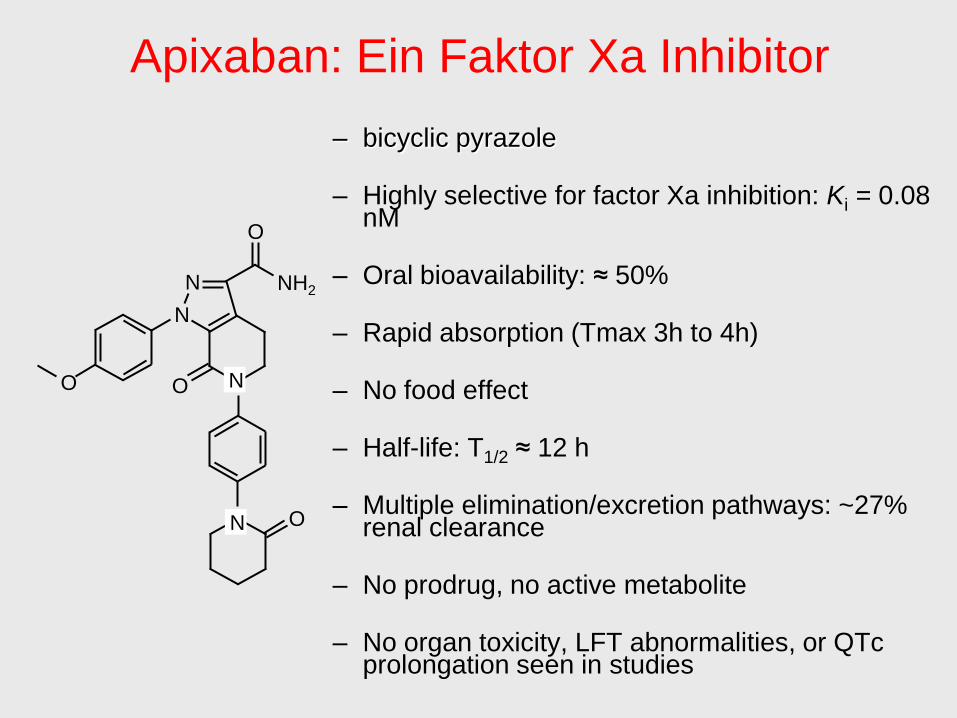
Apixaban: Ein Faktor Xa Inhibitor
– bicyclic pyrazole
– Highly selective for factor Xa inhibition: Ki = 0.08 nM
– Oral bioavailability: ≈ 50%
– Rapid absorption (Tmax 3h to 4h)
– No food effect
– Half-life: T1/2 ≈ 12 h
– Multiple elimination/excretion pathways: ~27% renal clearance
– No prodrug, no active metabolite
– No organ toxicity, LFT abnormalities, or QTc prolongation seen in studies
N
N
O
NH2
O N
N O
O