Embed Size (px)
Citation preview

Thoracic TraumaThoracic TraumaChristopher McPeak, Christopher McPeak,
MDMDDepartment of Emergency Department of Emergency
MedicineMedicine
Albany Medical CenterAlbany Medical Center

Thoracic TraumaThoracic Trauma
Second leading cause of trauma Second leading cause of trauma deaths after head injurydeaths after head injury
Cause of about 10-20% of all trauma Cause of about 10-20% of all trauma deathsdeaths
Many deaths due to thoracic trauma Many deaths due to thoracic trauma are preventableare preventable

Thoracic TraumaThoracic Trauma
Prevention StrategiesPrevention Strategies Gun Safety EducationGun Safety Education Sports Training & Protective EquipmentSports Training & Protective Equipment Seat Belt & Air Bag UseSeat Belt & Air Bag Use

Thoracic TraumaThoracic Trauma
Mechanisms of InjuryMechanisms of Injury Blunt InjuryBlunt Injury
DecelerationDeceleration CompressionCompression
Penetrating InjuryPenetrating Injury

Thoracic TraumaThoracic Trauma
Anatomical InjuriesAnatomical Injuries Thoracic Cage (Skeletal)Thoracic Cage (Skeletal) CardiovascularCardiovascular Pleural and PulmonaryPleural and Pulmonary MediastinalMediastinal DiaphragmaticDiaphragmatic EsophagealEsophageal Penetrating CardiacPenetrating Cardiac
Thoracic TraumaThoracic Trauma Often result in:Often result in:
HypoxiaHypoxia
HypercarbiaHypercarbia
Acidosis Acidosis hypoperfusion of tissues (metabolic)hypoperfusion of tissues (metabolic)

Thoracic Trauma--CardiacThoracic Trauma--Cardiac
Impairments to cardiac outputImpairments to cardiac output blood lossblood loss increased intrapleural pressuresincreased intrapleural pressures blood in pericardial sacblood in pericardial sac myocardial valve damagemyocardial valve damage vascular disruptionvascular disruption

Thoracic Trauma--Thoracic Trauma--RespiratoryRespiratory
Impairments in ventilatory efficiencyImpairments in ventilatory efficiency chest excursion compromisechest excursion compromise
painpain air in pleural spaceair in pleural space asymmetrical movementasymmetrical movement
bleeding in pleural spacebleeding in pleural space ineffective diaphragm contractionineffective diaphragm contraction

Thoracic Trauma--Thoracic Trauma--RespiratoryRespiratory
Impairments in gas exchangeImpairments in gas exchange atelectasisatelectasis pulmonary contusionpulmonary contusion respiratory tract disruptionrespiratory tract disruption

Thoracic Trauma--ExamThoracic Trauma--Exam Initial exam directed toward life Initial exam directed toward life
threatening:threatening: InjuriesInjuries
Open pneumothoraxOpen pneumothorax Flail chestFlail chest Tension pneumothoraxTension pneumothorax Massive hemothoraxMassive hemothorax Cardiac tamponadeCardiac tamponade
ConditionsConditions ApneaApnea Respiratory DistressRespiratory Distress

Thoracic Trauma--ExamThoracic Trauma--Exam
Assessment FindingsAssessment Findings Mental Status (decreased)Mental Status (decreased) Pulse (absent, tachy or brady)Pulse (absent, tachy or brady) BP (narrow PP, hyper- or hypotension, BP (narrow PP, hyper- or hypotension,
pulsus paradoxus)pulsus paradoxus) Ventilatory rate & effort (tachy- or Ventilatory rate & effort (tachy- or
bradypnea, labored, retractions)bradypnea, labored, retractions) Skin (diaphoresis, pallor, cyanosis, open Skin (diaphoresis, pallor, cyanosis, open
injury, ecchymosis)injury, ecchymosis)

Thoracic Trauma--ExamThoracic Trauma--Exam
Assessment FindingsAssessment Findings Neck (tracheal position, SQ emphysema, Neck (tracheal position, SQ emphysema,
JVD, open injury)JVD, open injury) Chest (contusions, tenderness, asymmetry, Chest (contusions, tenderness, asymmetry,
absent or decreased lung sounds, bowel absent or decreased lung sounds, bowel sounds, abnormal percussion, open injury, sounds, abnormal percussion, open injury, impaled object, crepitus, hemoptysis)impaled object, crepitus, hemoptysis)
Heart Sounds (muffled, distant, regurgitant Heart Sounds (muffled, distant, regurgitant murmur)murmur)
Upper abdomen (contusion, open injury)Upper abdomen (contusion, open injury)

Thoracic Trauma--ExamThoracic Trauma--Exam
Assessment FindingsAssessment Findings ECG (ST segment abnormalities, ECG (ST segment abnormalities,
dysrhythmias)dysrhythmias) HistoryHistory
DyspneaDyspnea PainPain Past hx of cardiorespiratory diseasePast hx of cardiorespiratory disease Restraint devices usedRestraint devices used Item/Weapon involved in injuryItem/Weapon involved in injury

Thoracic Thoracic TraumaTraumaSpecific InjuriesSpecific Injuries

Rib FractureRib Fracture
Most common chest wall injury Most common chest wall injury from direct traumafrom direct trauma
More common in adults than More common in adults than childrenchildren
Especially common in elderlyEspecially common in elderly Ribs form ringsRibs form rings
Possibility of break in two placesPossibility of break in two places Most commonly 5th - 9th ribsMost commonly 5th - 9th ribs
Poor protectionPoor protection

Rib FractureRib Fracture
Fractures of 1st and 2nd second Fractures of 1st and 2nd second require high forcerequire high force Frequently have injury to aorta or bronchiFrequently have injury to aorta or bronchi Occur in 90% of patients with tracheo-Occur in 90% of patients with tracheo-
bronchial rupturebronchial rupture May injure subclavian artery/veinMay injure subclavian artery/vein May result in pneumothoraxMay result in pneumothorax
30% will die30% will die

Rib FractureRib Fracture
Fractures of 10 to 12th ribs can cause Fractures of 10 to 12th ribs can cause damage to underlying abdominal solid damage to underlying abdominal solid organs:organs: LiverLiver SpleenSpleen KidneysKidneys

Rib FractureRib Fracture Assessment FindingsAssessment Findings
Localized pain, tendernessLocalized pain, tenderness Increases on palpation or when patient:Increases on palpation or when patient:
CoughsCoughs MovesMoves Breathes deeplyBreathes deeply
““Splinted” RespirationsSplinted” Respirations Instability in chest wall, CrepitusInstability in chest wall, Crepitus Deformity and discolorationDeformity and discoloration Associated pneumo or hemothoraxAssociated pneumo or hemothorax

Rib FractureRib Fracture ManagementManagement
High concentration OHigh concentration O22
Positive pressure ventilation as neededPositive pressure ventilation as needed Splint using pillow or swathesSplint using pillow or swathes Encourage pt to breath deeplyEncourage pt to breath deeply
Helps prevent atelectasisHelps prevent atelectasis Analgesics for isolated traumaAnalgesics for isolated trauma Non-circumferential splintingNon-circumferential splinting
Rib FractureRib Fracture ManagementManagement
Monitor elderly and COPD patients closelyMonitor elderly and COPD patients closely Broken ribs can cause Broken ribs can cause
decompensationdecompensation Patients will fail to breathe deeply Patients will fail to breathe deeply
and cough, resulting in poor and cough, resulting in poor clearance of secretionsclearance of secretions
Usually Non-Emergent TransportUsually Non-Emergent Transport

Sternal FractureSternal Fracture
Uncommon, 5-8% in blunt chest traumaUncommon, 5-8% in blunt chest trauma Large traumatic forceLarge traumatic force Direct blow to front of chest byDirect blow to front of chest by
DecelerationDeceleration steering wheelsteering wheel dashboarddashboard
Other objectOther object

Sternal FractureSternal Fracture 25 - 45% mortality due to associated trauma:25 - 45% mortality due to associated trauma:
Disruption of thoracic aortaDisruption of thoracic aorta Tracheal or bronchial tearTracheal or bronchial tear Diaphragm ruptureDiaphragm rupture Flail chestFlail chest Myocardial traumaMyocardial trauma
High incidence of myocardial contusion, High incidence of myocardial contusion, cardiac tamponade or pulmonary contusioncardiac tamponade or pulmonary contusion

Sternal FractureSternal Fracture
Assessment FindingsAssessment Findings Localized painLocalized pain Tenderness over sternumTenderness over sternum CrepitusCrepitus Tachypnea, DyspneaTachypnea, Dyspnea ECG changes with associated ECG changes with associated
myocardial contusionmyocardial contusion Hx/Mechanism of blunt chest traumaHx/Mechanism of blunt chest trauma

Sternal FractureSternal Fracture ManagementManagement
Establish airwayEstablish airway High concentration oxygenHigh concentration oxygen Assist ventilations with BVM as neededAssist ventilations with BVM as needed IV NS/LRIV NS/LR Emergent TransportEmergent Transport
Trauma centerTrauma center

Flail ChestFlail Chest
Two or more adjacent ribs Two or more adjacent ribs fractured in two or more fractured in two or more places producing a free places producing a free
floating segment of the chest floating segment of the chest wallwall

Flail ChestFlail Chest Usually secondary to Usually secondary to
blunt traumablunt trauma Most commonly in MVCMost commonly in MVC Also results fromAlso results from
falls from heightsfalls from heights industrial accidentsindustrial accidents assaultassault birth traumabirth trauma
More common in More common in older patientsolder patients

Flail ChestFlail Chest
Mortality rates 20-40% due to Mortality rates 20-40% due to associated injuriesassociated injuries
Mortality increased withMortality increased with advanced ageadvanced age seven or more rib fracturesseven or more rib fractures three or more associated injuriesthree or more associated injuries shockshock head injurieshead injuries

Flail ChestFlail Chest Consequences of flail chestConsequences of flail chest
Respiratory failure due toRespiratory failure due to pulmonary contusionpulmonary contusion intrathoracic injuryintrathoracic injury inadequate diaphragm movementinadequate diaphragm movement
Paradoxical movement of the chestParadoxical movement of the chest must be large to compromise ventilationmust be large to compromise ventilation Increased work of breathingIncreased work of breathing
Pain, decreased chest expansionPain, decreased chest expansion leading decreased ventilationleading decreased ventilation

Flail ChestFlail Chest
Consequences of flail chestConsequences of flail chest Contusion of lungContusion of lung
decreased lung compliancedecreased lung compliance intra alveolar-capillary hemorrhageintra alveolar-capillary hemorrhage
Decreased ventilationDecreased ventilation HypercapneaHypercapnea HypoxiaHypoxia

Flail ChestFlail Chest
Assessment FindingsAssessment Findings Chest wall contusionChest wall contusion Respiratory distressRespiratory distress Pleuritic chest painPleuritic chest pain Splinting of affected sideSplinting of affected side CrepitusCrepitus Tachypnea, TachycardiaTachypnea, Tachycardia Paradoxical movement (possible)Paradoxical movement (possible)

Flail ChestFlail Chest ManagementManagement
Suspect spinal injuriesSuspect spinal injuries Establish airwayEstablish airway High concentration oxygenHigh concentration oxygen Assist ventilation with BVMAssist ventilation with BVM
Treat hypoxia from underlying contusionTreat hypoxia from underlying contusion Promote full lung expansionPromote full lung expansion
Consider need for intubation and PEEPConsider need for intubation and PEEP Mechanically stabilize chest wallMechanically stabilize chest wall
questionable valuequestionable value

Flail ChestFlail Chest ManagementManagement
IV of LR/NSIV of LR/NS Avoid rapid replacement in Avoid rapid replacement in
hemodynamically stable patienthemodynamically stable patient Contused lung cannot handle fluid loadContused lung cannot handle fluid load
Monitor EKGMonitor EKG Chest trauma can cause dysrhythmiasChest trauma can cause dysrhythmias
Emergent TransportEmergent Transport Trauma centerTrauma center

Simple PneumothoraxSimple Pneumothorax IncidenceIncidence
10-30% in blunt chest 10-30% in blunt chest traumatrauma
almost 100% with almost 100% with penetrating chest penetrating chest traumatrauma
Morbidity & Mortality Morbidity & Mortality dependent ondependent on
extent of atelectasisextent of atelectasis associated injuriesassociated injuries

Simple PneumothoraxSimple Pneumothorax CausesCauses
Commonly a fx rib lacerates lungCommonly a fx rib lacerates lung May occur spontaneously in tall, thin May occur spontaneously in tall, thin
young males following:young males following: ExertionExertion CoughingCoughing Air TravelAir Travel

Simple PneumothoraxSimple Pneumothorax PathophysiologyPathophysiology
Air enters pleural space causing partial lung Air enters pleural space causing partial lung collapsecollapse
small tears self-sealsmall tears self-seal larger tears may progresslarger tears may progress
Usually well-tolerated in the young & healthyUsually well-tolerated in the young & healthy Severe compromise can occur in the elderly Severe compromise can occur in the elderly
or patients with pulmonary diseaseor patients with pulmonary disease Degree of distress depends on amount and Degree of distress depends on amount and
speed of collapsespeed of collapse

Simple PneumothoraxSimple Pneumothorax Assessment FindingsAssessment Findings
Tachypnea, TachycardiaTachypnea, Tachycardia Difficulty breathing or respiratory distressDifficulty breathing or respiratory distress Pleuritic painPleuritic pain
may be referred to shoulder or arm on affected may be referred to shoulder or arm on affected sideside
Decreased or absent breath soundsDecreased or absent breath sounds not always reliablenot always reliable
if patient standing, assess apices first if patient standing, assess apices first if supine, assess anteriorlyif supine, assess anteriorly
patients with multiple ribs fractures may patients with multiple ribs fractures may splint injured side by not breathing deeplysplint injured side by not breathing deeply

Simple PneumothoraxSimple Pneumothorax ManagementManagement
Establish airwayEstablish airway High concentration OHigh concentration O22 with NRB with NRB Assist with BVMAssist with BVM IV of LR/NSIV of LR/NS Monitor for progressionMonitor for progression Monitor ECGMonitor ECG Usually Non-emergent transportUsually Non-emergent transport
Open Open PneumothoraxPneumothoraxHole in chest wall that allows air to Hole in chest wall that allows air to
enter pleural space. enter pleural space.
Larger the hole the more likely air Larger the hole the more likely air will enter there than through the will enter there than through the
trachea. trachea.
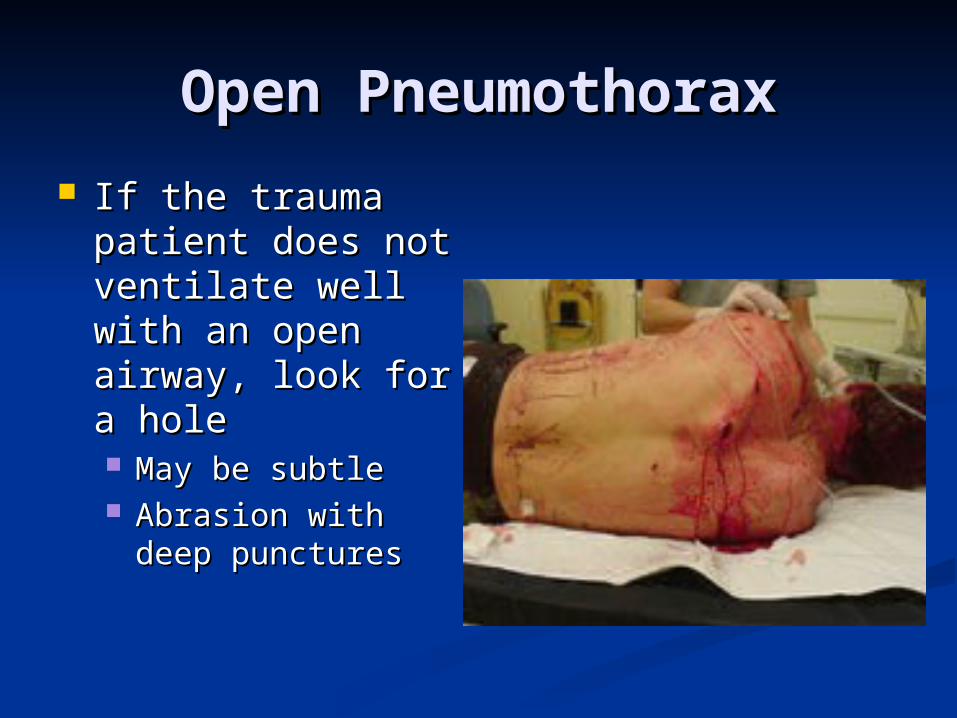
Open PneumothoraxOpen Pneumothorax
If the trauma If the trauma patient does not patient does not ventilate well with ventilate well with an open airway, an open airway, look for a holelook for a hole May be subtleMay be subtle Abrasion with deep Abrasion with deep
puncturespunctures
Open PneumothoraxOpen Pneumothorax
PathophysiologyPathophysiology Result of penetrating traumaResult of penetrating trauma Profound hypoventilation may occurProfound hypoventilation may occur Allows communication between pleural Allows communication between pleural
space and atmospherespace and atmosphere Prevents development of negative Prevents development of negative
intrapleural pressureintrapleural pressure Results in ipsilateral lung collapseResults in ipsilateral lung collapse
inability to ventilate affected lunginability to ventilate affected lung

Open PneumothoraxOpen Pneumothorax PathophysiologyPathophysiology
V/Q MismatchV/Q Mismatch shuntingshunting hypoventilationhypoventilation hypoxiahypoxia large functional dead spacelarge functional dead space
Pressure may build within pleural spacePressure may build within pleural space Return from Vena cava may be impairedReturn from Vena cava may be impaired
Open PneumothoraxOpen Pneumothorax
Assessment FindingsAssessment Findings Opening in the chest wallOpening in the chest wall Sucking sound on inhalationSucking sound on inhalation TachycardiaTachycardia TachypneaTachypnea Respiratory distressRespiratory distress SQ EmphysemaSQ Emphysema Decreased lung sounds on affected sideDecreased lung sounds on affected side

Open PneumothoraxOpen Pneumothorax ManagementManagement
Cover chest opening with occlusive dressingCover chest opening with occlusive dressing High concentration OHigh concentration O22
Assist with positive pressure ventilations prnAssist with positive pressure ventilations prn Monitor for progression to tension Monitor for progression to tension
pneumothoraxpneumothorax IV with LR/NSIV with LR/NS Monitor ECGMonitor ECG Emergent TransportEmergent Transport
Trauma CenterTrauma Center
Tension PneumothoraxTension Pneumothorax IncidenceIncidence
Penetrating TraumaPenetrating Trauma Blunt TraumaBlunt Trauma
Morbidity/MortalityMorbidity/Mortality Severe hypoventilationSevere hypoventilation Immediate life-threat if not managed earlyImmediate life-threat if not managed early

Tension PneumothoraxTension Pneumothorax PathophysiologyPathophysiology
One-way valve forms in lung or chest wall One-way valve forms in lung or chest wall Air enters pleural space, but cannot leaveAir enters pleural space, but cannot leave
Air is trapped in pleural spaceAir is trapped in pleural space Pressure collapses lung on affected sidePressure collapses lung on affected side Mediastinal shift to contralateral sideMediastinal shift to contralateral side
Reduction in cardiac outputReduction in cardiac output Increased intrathoracic pressureIncreased intrathoracic pressure deformed vena cava reducing preloaddeformed vena cava reducing preload

Tension PneumothoraxTension Pneumothorax Assessment Findings - Most LikelyAssessment Findings - Most Likely
Severe dyspnea Severe dyspnea extreme resp distress extreme resp distress Restlessness, anxiety, agitationRestlessness, anxiety, agitation Decreased/absent breath soundsDecreased/absent breath sounds Worsening or Severe Shock / Worsening or Severe Shock /
Cardiovascular collapseCardiovascular collapse TachycardiaTachycardia Weak pulseWeak pulse HypotensionHypotension Narrow pulse pressureNarrow pulse pressure

Tension PneumothoraxTension Pneumothorax Assessment Findings - Less LikelyAssessment Findings - Less Likely
Jugular Vein DistensionJugular Vein Distension absent if also hypovolemicabsent if also hypovolemic
Hyperresonance to percussion Hyperresonance to percussion Subcutaneous emphysemaSubcutaneous emphysema Tracheal shift Tracheal shift awayaway from injured side (late) from injured side (late) Cyanosis (late)Cyanosis (late)

Tension PneumothoraxTension Pneumothorax ManagementManagement
Recognize & Manage Recognize & Manage earlyearly
Establish airwayEstablish airway High concentration OHigh concentration O22 Positive pressure Positive pressure
ventilations w/BVM prnventilations w/BVM prn Needle thoracostomyNeedle thoracostomy IV of LR/NSIV of LR/NS Monitor ECGMonitor ECG Emergent TransportEmergent Transport
Consider need to Consider need to intubateintubate
Trauma Center preferredTrauma Center preferred
Tension PneumothoraxTension Pneumothorax ManagementManagement
Needle Thoracostomy ReviewNeedle Thoracostomy Review Decompress with 14g (lg bore), 2-inch Decompress with 14g (lg bore), 2-inch
needleneedle Midclavicular line: 2nd intercostal Midclavicular line: 2nd intercostal
spacespace Midaxillary line: 4-5th intercostal spaceMidaxillary line: 4-5th intercostal space Go over superior margin of rib to avoid Go over superior margin of rib to avoid
blood vesselsblood vessels Be careful not to kink or bend needle Be careful not to kink or bend needle
or catheteror catheter If available, attach a one-way valveIf available, attach a one-way valve
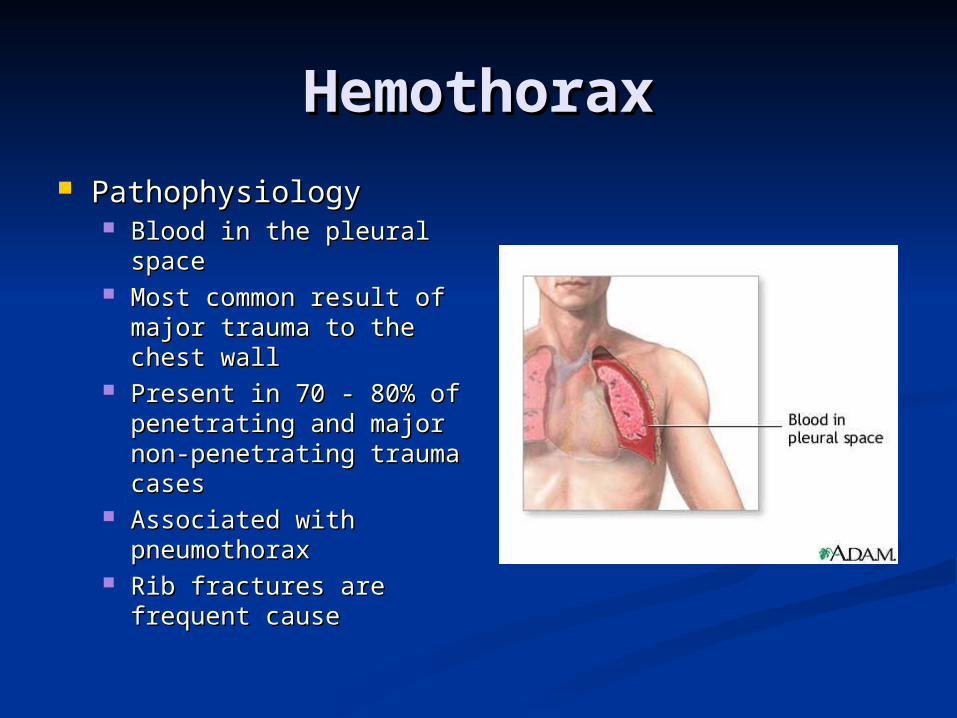
HemothoraxHemothorax PathophysiologyPathophysiology
Blood in the pleural Blood in the pleural spacespace
Most common result of Most common result of major trauma to the major trauma to the chest wallchest wall
Present in 70 - 80% of Present in 70 - 80% of penetrating and major penetrating and major non-penetrating trauma non-penetrating trauma casescases
Associated with Associated with pneumothoraxpneumothorax
Rib fractures are Rib fractures are frequent causefrequent cause
HemothoraxHemothorax PathophysiologyPathophysiology
Each can hold up to 3000 cc of bloodEach can hold up to 3000 cc of blood Life-threatening often requiring chest tube Life-threatening often requiring chest tube
and/or surgeryand/or surgery If assoc. with great vessel or cardiac injuryIf assoc. with great vessel or cardiac injury
50% die immediately50% die immediately 25% live five to ten minutes25% live five to ten minutes 25% may live 30 minutes or longer 25% may live 30 minutes or longer
Blood loss results inBlood loss results in HypovolemiaHypovolemia Decreased ventilation of affected lungDecreased ventilation of affected lung

HemothoraxHemothorax PathophysiologyPathophysiology
Accumulation of blood in pleural spaceAccumulation of blood in pleural space penetrating or blunt lung injurypenetrating or blunt lung injury chest wall vesselschest wall vessels intercostal vesselsintercostal vessels myocardiummyocardium
Massive hemothorax indicates great vessel Massive hemothorax indicates great vessel or cardiac injuryor cardiac injury
Intercostal artery can bleed 50 cc/minIntercostal artery can bleed 50 cc/min Results in collapse of lungResults in collapse of lung

HemothoraxHemothorax PathophysiologyPathophysiology
Accumulated blood can eventually produce Accumulated blood can eventually produce a tension hemothorax a tension hemothorax
Shifting the mediastinum producingShifting the mediastinum producing ventilatory impairmentventilatory impairment cardiovascular collapsecardiovascular collapse

HemothoraxHemothorax Assessment FindingsAssessment Findings
Tachypnea or respiratory distressTachypnea or respiratory distress ShockShock
Rapid, weak pulseRapid, weak pulse Hypotension, narrow pulse pressureHypotension, narrow pulse pressure Restlessness, anxietyRestlessness, anxiety Cool, pale, clammy skinCool, pale, clammy skin ThirstThirst
Pleuritic chest painPleuritic chest pain Decreased lung soundsDecreased lung sounds Collapsed neck veinsCollapsed neck veins Dullness on percussionDullness on percussion

HemothoraxHemothorax ManagementManagement
Establish airwayEstablish airway High concentration OHigh concentration O22
Assist Ventilations w/BVM prnAssist Ventilations w/BVM prn Needle thoracostomy if tension & unable to Needle thoracostomy if tension & unable to
differentiate from Tension Pneumothoraxdifferentiate from Tension Pneumothorax IVs x 2 with LR/NSIVs x 2 with LR/NS Monitor ECGMonitor ECG Emergent transport to Trauma CenterEmergent transport to Trauma Center

Pulmonary ContusionPulmonary Contusion PathophysiologyPathophysiology
Blunt trauma to the chestBlunt trauma to the chest Rapid deceleration forces cause lung to Rapid deceleration forces cause lung to
strike chest wallstrike chest wall high energy shock wave from explosionhigh energy shock wave from explosion high velocity missile woundhigh velocity missile wound low velocity as with ice picklow velocity as with ice pick
Most common injury from blunt thoracic Most common injury from blunt thoracic traumatrauma
30-75% of blunt trauma30-75% of blunt trauma mortality 14-20%mortality 14-20%
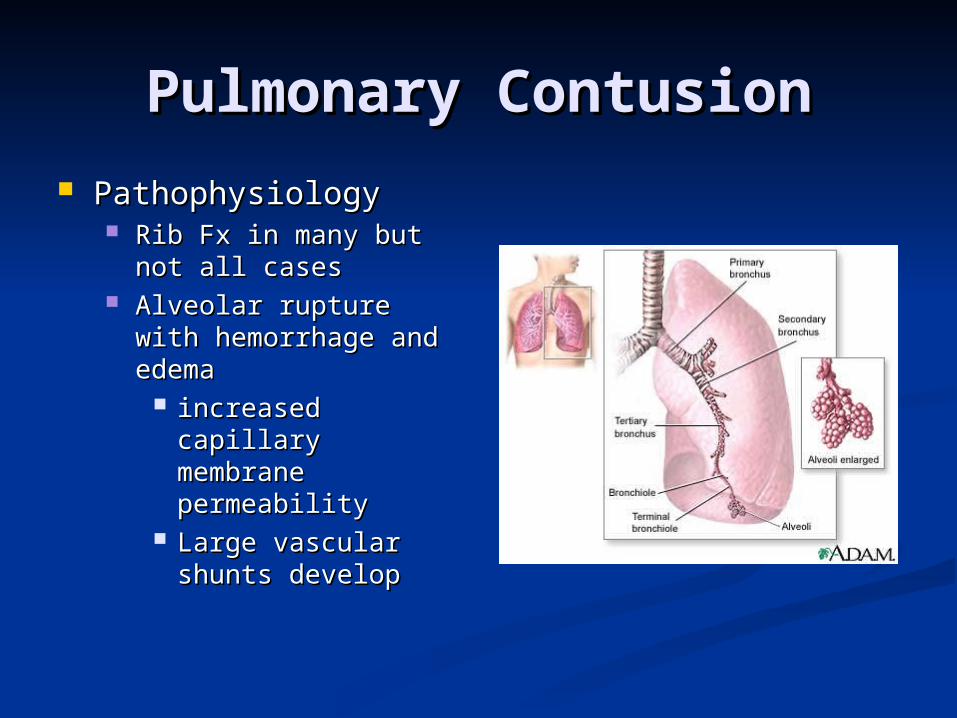
Pulmonary ContusionPulmonary Contusion PathophysiologyPathophysiology
Rib Fx in many but not Rib Fx in many but not all casesall cases
Alveolar rupture with Alveolar rupture with hemorrhage and edemahemorrhage and edema
increased capillary increased capillary membrane membrane permeabilitypermeability
Large vascular Large vascular shunts developshunts develop

Pulmonary ContusionPulmonary Contusion Assessment FindingsAssessment Findings
Tachypnea or respiratory distressTachypnea or respiratory distress TachycardiaTachycardia Evidence of blunt chest traumaEvidence of blunt chest trauma Cough and/or HemoptysisCough and/or Hemoptysis ApprehensionApprehension CyanosisCyanosis

Pulmonary ContusionPulmonary Contusion ManagementManagement
Supportive therapySupportive therapy Early use of positive Early use of positive
pressure ventilation pressure ventilation reduces ventilator reduces ventilator therapy durationtherapy duration
Avoid aggressive Avoid aggressive crystalloid infusioncrystalloid infusion
Severe cases may Severe cases may require ventilator require ventilator therapytherapy
Emergent TransportEmergent Transport Trauma CenterTrauma Center

Cardiovascular Cardiovascular TraumaTrauma
Any patient with significant Any patient with significant blunt or penetrating trauma blunt or penetrating trauma
to chest has heart/great to chest has heart/great vessel injury until proven vessel injury until proven
otherwiseotherwise

Myocardial ContusionMyocardial Contusion
Most common blunt injury to heartMost common blunt injury to heart Usually due to steering wheelUsually due to steering wheel Significant cause of morbidity and Significant cause of morbidity and
mortality in the blunt trauma patientmortality in the blunt trauma patient

Myocardial ContusionMyocardial Contusion PathophysiologyPathophysiology
Behaves like acute MIBehaves like acute MI Hemorrhage with edemaHemorrhage with edema
Cellular injuryCellular injury vascular damage may occurvascular damage may occur
Hemopericardium may occur from Hemopericardium may occur from lacerated epicardium or endocardiumlacerated epicardium or endocardium
May produce arrhythmiasMay produce arrhythmias May cause hypotension unresponsive to May cause hypotension unresponsive to
fluid or drug therapyfluid or drug therapy

Myocardial ContusionMyocardial Contusion Assessment FindingsAssessment Findings
Cardiac arrhythmias following blunt chest Cardiac arrhythmias following blunt chest traumatrauma
Angina-like pain unresponsive to Angina-like pain unresponsive to nitroglycerinnitroglycerin
Precordial discomfort independent of Precordial discomfort independent of respiratory movementrespiratory movement
Pericardial friction rub (late)Pericardial friction rub (late)
Myocardial ContusionMyocardial Contusion Assessment FindingsAssessment Findings
ECG ChangesECG Changes Persistent tachycardiaPersistent tachycardia ST elevation, T wave inversionST elevation, T wave inversion RBBBRBBB Atrial flutter, Atrial fibrillationAtrial flutter, Atrial fibrillation PVCsPVCs PACsPACs

Myocardial ContusionMyocardial Contusion ManagementManagement
Establish airwayEstablish airway High concentration OHigh concentration O2 2
IV LR/NSIV LR/NS Cautious fluid administration due to injured Cautious fluid administration due to injured
myocardiummyocardium ECGECG
Standard drug therapy for arrhythmiasStandard drug therapy for arrhythmias 12 Lead ECG if time permits12 Lead ECG if time permits
Consider vasopressors for hypotensionConsider vasopressors for hypotension Emergent TransportEmergent Transport
Trauma CenterTrauma Center

Pericardial TamponadePericardial Tamponade IncidenceIncidence
Usually associated with penetrating Usually associated with penetrating traumatrauma
Rare in blunt traumaRare in blunt trauma Occurs in < 2% of chest traumaOccurs in < 2% of chest trauma GSW wounds have higher mortality GSW wounds have higher mortality
than stab woundsthan stab wounds Lower mortality rate if isolated Lower mortality rate if isolated
tamponadetamponade

Pericardial TamponadePericardial Tamponade PathophysiologyPathophysiology
Space normally filled with 30-50 ml of Space normally filled with 30-50 ml of straw-colored fluidstraw-colored fluid
lubricationlubrication lymphatic dischargelymphatic discharge immunologic protection for the heartimmunologic protection for the heart
Rapid accumulation of blood in the inelastic Rapid accumulation of blood in the inelastic pericardiumpericardium
Pericardial TamponadePericardial Tamponade PathophysiologyPathophysiology
Heart is compressed decreasing blood Heart is compressed decreasing blood entering heartentering heart
Decreased diastolic expansion and fillingDecreased diastolic expansion and filling Hindered venous return (preload)Hindered venous return (preload)
Myocardial perfusion decreased due toMyocardial perfusion decreased due to pressure effects on walls of heartpressure effects on walls of heart decreased diastolic pressuresdecreased diastolic pressures
Ischemic dysfunction may result in injuryIschemic dysfunction may result in injury Removal of as little as 20 ml of blood may Removal of as little as 20 ml of blood may
drastically improve cardiac outputdrastically improve cardiac output

Pericardial TamponadePericardial Tamponade Signs and SymptomsSigns and Symptoms
Beck’s TriadBeck’s Triad Resistant hypotensionResistant hypotension Increased central venous Increased central venous pressure (distended neck/arm pressure (distended neck/arm veins in presence of decreased veins in presence of decreased arterial BP)arterial BP)
Small quiet heart (decreased Small quiet heart (decreased heart sounds)heart sounds)

Pericardial TamponadePericardial Tamponade
Signs and SymptomsSigns and Symptoms Narrowing pulse pressureNarrowing pulse pressure Pulsus paradoxicusPulsus paradoxicus
Radial pulse becomes weak or Radial pulse becomes weak or disappears when patient inhalesdisappears when patient inhales
Increased intrathoracic Increased intrathoracic pressure on inhalation causes pressure on inhalation causes blood to be trapped in lungs blood to be trapped in lungs temporarilytemporarily

Pericardial TamponadePericardial Tamponade ManagementManagement
Secure airwaySecure airway High concentration OHigh concentration O22
PericardiocentesisPericardiocentesis Out of hospital, primarily reserved for Out of hospital, primarily reserved for
cardiac arrestcardiac arrest Rapid transportRapid transport
Trauma CenterTrauma Center IVs of LR/NSIVs of LR/NS
Pericardial TamponadePericardial Tamponade ManagementManagement
Definite treatment is pericardiocentesis Definite treatment is pericardiocentesis followed by surgeryfollowed by surgery
Pericardial WindowPericardial Window Tamponade is hard to diagnosisTamponade is hard to diagnosis
Hypotension is common in chest traumaHypotension is common in chest trauma Heart sounds are difficult to hearHeart sounds are difficult to hear Bulging neck veins may be absent if Bulging neck veins may be absent if
hypovolemia is presenthypovolemia is present High index of suspicion is requiredHigh index of suspicion is required
Traumatic Aortic Traumatic Aortic Dissection/RuptureDissection/Rupture
Caused By:Caused By: Motor Vehicle Motor Vehicle
CollisionsCollisions Falls from heightsFalls from heights Crushing chest traumaCrushing chest trauma Animal KicksAnimal Kicks Blunt chest traumaBlunt chest trauma
15% of all blunt 15% of all blunt trauma deathstrauma deaths
Traumatic Aortic Traumatic Aortic Dissection/RuptureDissection/Rupture
1 of 6 persons dying in MVC’s has 1 of 6 persons dying in MVC’s has aortic ruptureaortic rupture 85% die instantaneously85% die instantaneously 10-15% survive to hospital10-15% survive to hospital
1/3 die within six hours1/3 die within six hours 1/3 die within 24 hours1/3 die within 24 hours 1/3 survive 3 days or longer1/3 survive 3 days or longer
MustMust have high index of suspicion have high index of suspicion
Traumatic Aortic Traumatic Aortic Dissection/RuptureDissection/Rupture
Separation of the aortic intima and mediaSeparation of the aortic intima and media Tear 2° high speed deceleration at points of relative Tear 2° high speed deceleration at points of relative
fixationfixation Blood enters media through a small intima Blood enters media through a small intima
teartear Thinned layer may ruptureThinned layer may rupture
Descending aorta at the isthmus distal to left Descending aorta at the isthmus distal to left subclavian artery most common site of subclavian artery most common site of rupturerupture ligamentum arteriosomligamentum arteriosom

Traumatic Aortic Traumatic Aortic Dissection/Rupture Dissection/Rupture
Assessment FindingsAssessment Findings Retrosternal or interscapular painRetrosternal or interscapular pain Pain in lower back or one legPain in lower back or one leg Respiratory distressRespiratory distress Asymmetrical arm BPsAsymmetrical arm BPs Upper extremity hypertension withUpper extremity hypertension with
Decreased femoral pulses, ORDecreased femoral pulses, OR Absent femoral pulses Absent femoral pulses
DysphagiaDysphagia

Traumatic Aortic Traumatic Aortic Dissection/Rupture Dissection/Rupture
ManagementManagement Establish airwayEstablish airway High concentration oxygenHigh concentration oxygen Maintain minimal BP in dissectionMaintain minimal BP in dissection
IV LR/NS TKOIV LR/NS TKO minimize fluid administrationminimize fluid administration
Avoid PASGAvoid PASG Emergent TransportEmergent Transport
Trauma CenterTrauma Center Vascular Surgery capabilityVascular Surgery capability
Diaphragmatic RuptureDiaphragmatic Rupture Usually due to blunt trauma but may Usually due to blunt trauma but may
occur with penetrating traumaoccur with penetrating trauma Usually life-threateningUsually life-threatening Likely to be associated with other Likely to be associated with other
severe injuriessevere injuries

Diaphragmatic RuptureDiaphragmatic Rupture PathophysiologyPathophysiology
Compression to abdomen resulting in Compression to abdomen resulting in increased intra-abdominal pressureincreased intra-abdominal pressure
abdominal contents rupture through abdominal contents rupture through diaphragm into chestdiaphragm into chest
bowel obstruction and strangulationbowel obstruction and strangulation restriction of lung expansionrestriction of lung expansion mediastinal shiftmediastinal shift
90% occur on left side due to protection of 90% occur on left side due to protection of right side by liverright side by liver

Diaphragmatic RuptureDiaphragmatic Rupture
Assessment FindingsAssessment Findings Decreased breath soundsDecreased breath sounds
Usually unilateralUsually unilateral Dullness to percussionDullness to percussion
Dyspnea or Respiratory DistressDyspnea or Respiratory Distress Scaphoid Abdomen (hollow appearance)Scaphoid Abdomen (hollow appearance) Usually impossible to hear bowel soundsUsually impossible to hear bowel sounds

Diaphragmatic RuptureDiaphragmatic Rupture ManagementManagement
Establish airwayEstablish airway Assist ventilations with high concentration OAssist ventilations with high concentration O2 2
IV of LRIV of LR Monitor EKGMonitor EKG NG tube if possibleNG tube if possible AvoidAvoid
MASTMAST Trendelenburg positionTrendelenburg position
Diaphragmatic Diaphragmatic PenetrationPenetration
Suspect intra-abdominal trauma Suspect intra-abdominal trauma with any injury below 4th ICSwith any injury below 4th ICS
Suspect intrathoracic trauma with Suspect intrathoracic trauma with any abdominal injury above any abdominal injury above umbilicusumbilicus

Esophageal InjuryEsophageal Injury Penetrating Injury most frequent causePenetrating Injury most frequent cause
Rare in blunt traumaRare in blunt trauma Can perforate spontaneouslyCan perforate spontaneously
violent emesisviolent emesis carcinomacarcinoma
Esophageal InjuryEsophageal Injury Assessment FindingsAssessment Findings
Pain, local tendernessPain, local tenderness Hoarseness, DysphagiaHoarseness, Dysphagia Respiratory distressRespiratory distress Resistance of neck on passive motionResistance of neck on passive motion Mediastinal esophageal perforationMediastinal esophageal perforation
mediastinal emphysema / mediastinal crunchmediastinal emphysema / mediastinal crunch mediastinitismediastinitis SQ EmphysemaSQ Emphysema splinting of chest wallsplinting of chest wall
ShockShock

Esophageal InjuryEsophageal Injury ManagementManagement
Establish AirwayEstablish Airway Consider early intubation if possibleConsider early intubation if possible IV LR/NS titrated to BP 90-100 mm HgIV LR/NS titrated to BP 90-100 mm Hg Emergent TransportEmergent Transport
Trauma CenterTrauma Center Surgical capabilitySurgical capability

Tracheobronchial Tracheobronchial RuptureRupture
Uncommon injury Uncommon injury less than 3% of chest traumaless than 3% of chest trauma
Occurs with penetrating or blunt Occurs with penetrating or blunt chest traumachest traumaHigh mortality rate (>30%)High mortality rate (>30%)May involve fracture of upper 3 May involve fracture of upper 3 ribsribs

Tracheobronchial Tracheobronchial RuptureRupture
PathophysiologyPathophysiology Majority (80%) occur at or near carinaMajority (80%) occur at or near carina rapid movement of air into pleural spacerapid movement of air into pleural space Tension pneumothorax refractory to needle Tension pneumothorax refractory to needle
decompressiondecompression continuous flow of air from needle of continuous flow of air from needle of
decompressed chestdecompressed chest
Tracheobronchial Tracheobronchial RuptureRupture Assessment FindingsAssessment Findings
Respiratory DistressRespiratory Distress DyspneaDyspnea TachypneaTachypnea
Obvious SQ emphysemaObvious SQ emphysema HemoptysisHemoptysis
Especially of bright red bloodEspecially of bright red blood Signs of tension pneumothorax Signs of tension pneumothorax
unresponsive to needle decompressionunresponsive to needle decompression
Tracheobronchial Tracheobronchial RuptureRupture ManagementManagement
Establish airway and ventilationsEstablish airway and ventilations Consider early intubationConsider early intubation
intubating right or left mainstem may be intubating right or left mainstem may be life savinglife saving
Emergent TransportEmergent Transport Trauma CenterTrauma Center

Pitfalls to AvoidPitfalls to Avoid
Elderly do not tolerate relatively minor Elderly do not tolerate relatively minor chest injurieschest injuries Anticipate progression to acute respiratory Anticipate progression to acute respiratory
insufficiencyinsufficiency Children may sustain significant Children may sustain significant
intrathoracic injury w/o evidence of intrathoracic injury w/o evidence of thoracic skeletal traumathoracic skeletal trauma Maintain a high index of suspicionMaintain a high index of suspicion
Pitfalls to AvoidPitfalls to Avoid
Don’t overlook the Obvious!Don’t overlook the Obvious! Be suspicious of the non-obvious!Be suspicious of the non-obvious!