Embed Size (px)
Citation preview
This is the most comprehensive compilation of epidemiological
information on Hepatitis C
Graciously provided by the
University Hepatitis Center
(last updated 2008)

Hepatitis C Update 2008
Tanya Schreibman, MD
University Hepatitis Center
Bradenton, Fl

Hepatitis C Update 2008
• Epidemiology
• Natural History and Clinical Presentation
• Diagnosis, Screening and Barriers
• Treatment
• Final Comments

Hepatitis C Update 2008: Epidemiology


Hepatitis C Virus InfectionMagnitude of the Problem
• Nearly 4 million persons in United States infected• Approximately 35,000 new cases yearly• 85% of new cases become chronic• Leading cause of
Chronic liver disease Cirrhosis Liver cancer Liver transplantation
Centers for Disease Control and Prevention. Hepatitis C fact sheet. Available at: http://www.cdc.gov/ncidod/diseases/hepatitis/c/fact.htm. Accessed February 1, 2006.
True or False?
• You can only get hepatitis C by injecting drugs.

Answer: False
• It is true that you can get Hepatitis C by sharing needles or injecting drugs.
• However, this is not the only way that you can get Hepatitis C.


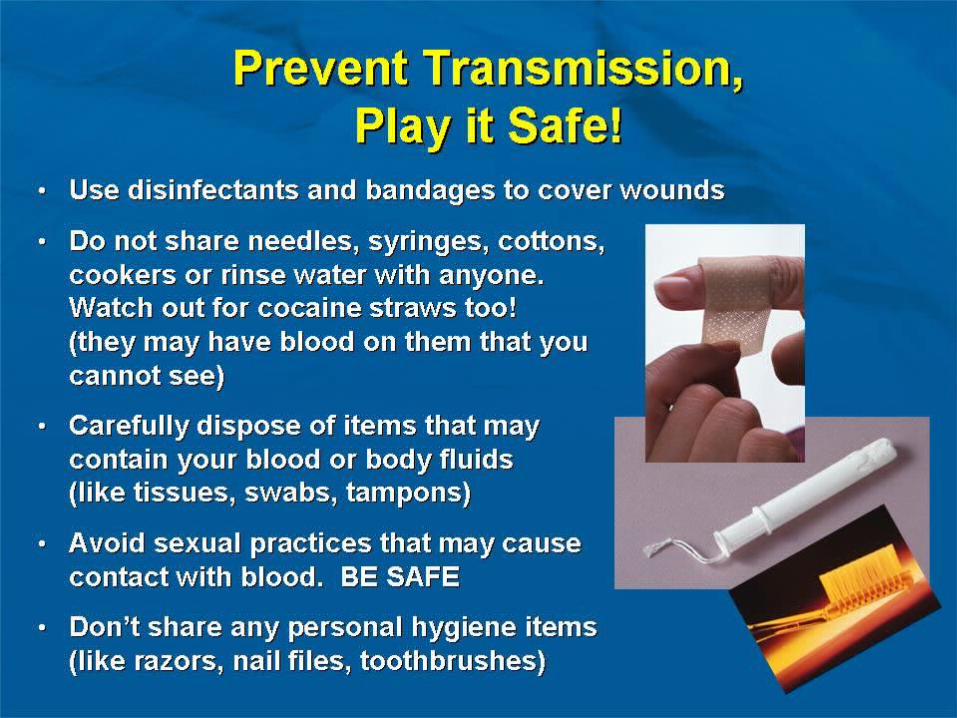
Hepatitis C Virus InfectionPopulation at Risk
• Transfusion of blood products before 1992
• Intravenous drug use
• Nasal inhalation of cocaine
• Chronic renal failure on dialysis
• Incarceration
• Occupational exposure to blood products
• Transplantation of an organ/tissue graft from an HCV-positive donor
• Body piercing and potentially tattoo
Centers for Disease Control and Prevention. Hepatitis C fact sheet. Available at: http://www.cdc.gov/ncidod/diseases/hepatitis/c/fact.htm. Accessed February 1, 2006.



HCV Sexual TransmissionUnlikely in Heterosexual
Monogamous Couples• 895 monogamous heterosexual partners of
HCV infected patients– Ten year prospective follow up study
• 3 HCV infections during followed up– None were sexually transmitted from partner– In one couple,partners were different genotypes– In two couples, partners had same genotypes
but different strains


Hepatitis C Update 2008: Natural History and Clinical Presentation of Hepatitis C
Infection



4 Stages of Liver DamageStage 1 (F1)
Beginning of liver damageDamage has started with some slight
scarring
Stage 2 (F2)Moderate liver damage scarring advances in the liver & surrounding blood vessels
4 Stages of Liver DamageStage 3 (F3)
Significant liver damage; the liver becomes fibrotic (scarred) and connects
with other scarred areas.
Stage 4 (F4)Final stage of liver damage, also called cirrhosis; the liver is severely damaged
and no longer functions properly


Hepatitis C VirusFate of Acute Infection
15%
Chronic85%
Spontaneousresolution
Alter MJ, et al. N Eng J Med. 1999;341:556-562.

Hepatitis C Virus InfectionNatural History
Stable80% (68%)
HCCLiver failure25% (4%)
Slowlyprogressive75% (13%)
Resolved15% (15%)
Acute HCV
Cirrhosis20% (17%)
Chronic HCV85% (85%)
HCC, hepatocellular carcinoma

True or False?
• You can get hepatitis C and not even feel sick?

Answer: True
• You can have Hepatitis C for many years and not even feel sick or have any symptoms.
• The only way for you to know if you have Hepatitis C is to test your blood.

Chronic HCV InfectionSymptoms
Asymptomatic
Symptomatic
Cirrhosis
0
20
40
60
80
100
Fatigue
Per
cen
tag
e o
f P
atie
nts
37%
7%
56%
Unpublished data from MCV Hepatitis Program, 1995.




Alcohol and HCV: Is a little bit OK?• 800 patients – alcohol questionnaire
– Alcohol intake = lifetime ETOH/time drinking
• Fibrosis increased with > 50 g/day
Monto A et al. Hepatology 2004;39:826 - 834

g/Drinkg/Drink Drinks/50 gDrinks/50 g
BeerBeer12 oz at 12 oz at 4%4%
1111 4.54.5
Wine 5 oz Wine 5 oz at 11%at 11% 1313 3.83.8
MartiniMartini3 oz at 3 oz at 40%40%
2828 1.81.8
Alcohol content in specific beverages



Hepatitis C Update 2008:Screening and Diagnosis





Testing for Hepatitis C VirusAnti-HCV Antibodies
• ELISA screening test
– Sensitivity: 97%
– Detects circulating HCV antibodies
• False positive reactions may occur
– Cross-reacting circulating antibodies
• Positive predictive value
– 95% with risk factors and elevated ALT
– 50% without risk factors and normal ALTIllustration by Mitchell L. Shiffman, MD.


Hepatitis C VirusGenotypes in the USA
All others1%
Type 310%
Type 217%
Type 172%
McHutchinson JG, et al. N Engl J Med. 1998;339:1485-1492.


Chronic HCV InfectionNormal vs Elevated Serum ALT
Normal ALT Elevated ALT
Portal26%
No fibrosis
23%
Mild39%
Cirrhosis6%
Bridging6%
Portal20%
No fibrosis
16% Mild33%
Cirrhosis18%
Bridging13%
Shiffman ML, et al. J Infect Dis. 2000;182:1595-1601.

Hepatitis C Virus InfectionLiver Biopsy
• Only test that can accurately assess– Severity of inflammation– Degree of fibrosis
• Determines the following– Risk for developing cirrhosis in future– Need for therapy– Need for ongoing therapy when initial
treatment has failed


Hepatitis C Update 2008: Treatment


True or False?
• HIV related disease is the number one cause of death in HIV patients co-infected with hepatitis C.

Answer: False
• Liver-related death is the number one cause of death in co-infected patients. That is why it is important to talk to your healthcare provider about treatment.





Current Treatment Recommendations
• Combination therapy for 6-12 months of pegylated interferon plus ribavirin is the standard of care
• Pegylated interferon (injection) helps fight the virus in two ways:– It helps healthy cells defend themselves against
the virus– It strengthens the immune system, which helps
to stop the virus from growing in number

Ribavirin
• Ribavirin is a pill, that when taken with pegylated interferon, helps the pegylated interferon do its job. It helps slow down the replication of hepatitis C. It is usually taken as long as you are taking pegylated interferon.
• Ribavirin cannot fight HCV on its own.

Treatment of Chronic HCVPeginterferon and Ribavirin
0
20
40
60
80
100
1 2-3
Genotype
Su
stai
ned
Vir
olo
gic
Res
po
nse
(%
)
PegIFN-2a/RBVPegIFN-2b/RBV
Fried MW, et al. N Eng J Med. 2002;347:975-982. Manns MP, et al. Lancet 2001;358:958-965.



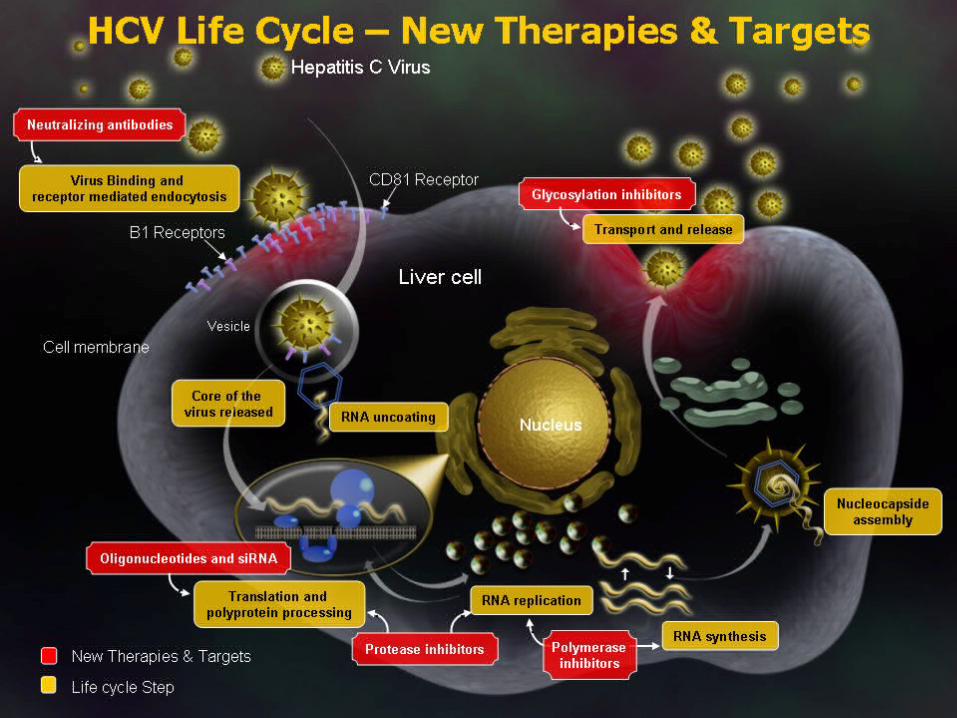


Protease Inhibitor: Protease Inhibitor: Telaprevir(VX-950)Telaprevir(VX-950)
Courtesy of Dr. J-M Pawlotsky.


Hepatitis C Update 2008: Final Comments



Hepatitis C Virus Infection Prevalence by Age
0
1.0
2.0
3.0
4.0
5.0
< 11 11-19 20-29 30-39 40-49 50-59 60-69 ≥ 70
Age Group
An
ti-H
CV
Po
siti
ve (
%)
Alter MJ, et al. N Eng J Med. 1999;341:556-562.

Armstrong GL, et al. Hepatology. 2000;31:777-782.
Hepatitis C Virus InfectionThe Burden of Disease
0
1.0
2.0
3.0
1960 1980 2000 2020
Year
All patients
Infection for> 20 years
An
ti-H
CV
Po
siti
ve (
%)
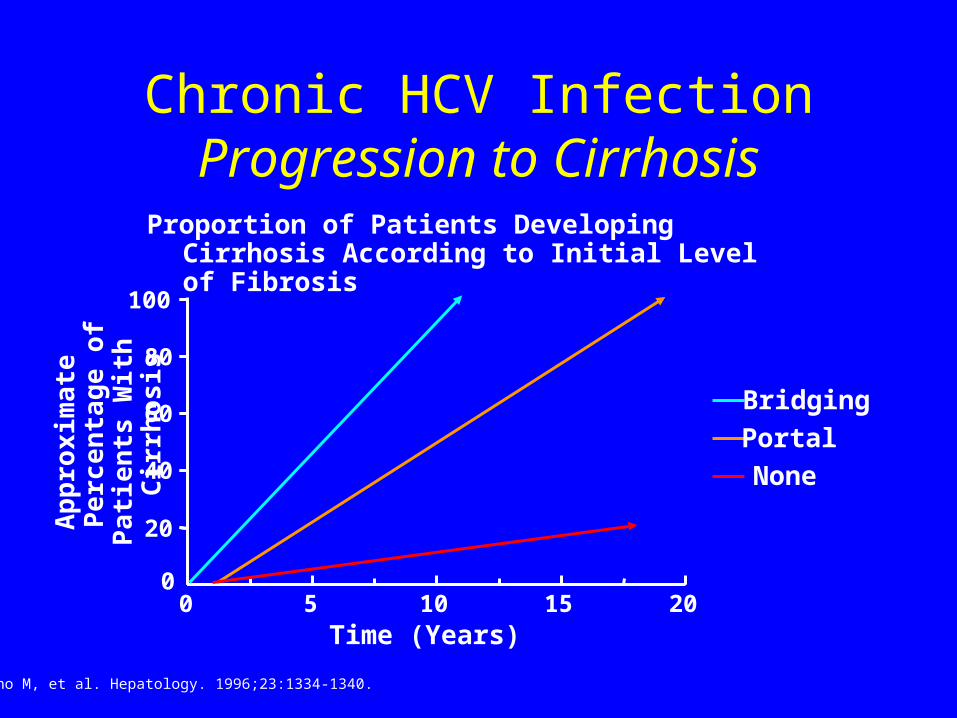
Chronic HCV InfectionProgression to Cirrhosis
0
20
40
60
80
100
0 5 10 15 20Time (Years)
Bridging
Portal
None
Ap
pro
xim
ate
Pe
rce
nta
ge
of
Pa
tie
nts
Wit
h C
irrh
osi
s
Yano M, et al. Hepatology. 1996;23:1334-1340.
Proportion of Patients Developing Cirrhosis According to Initial Level of Fibrosis

Zein CO, et al. Am J Gastroenterol. 2005;100:48-55.
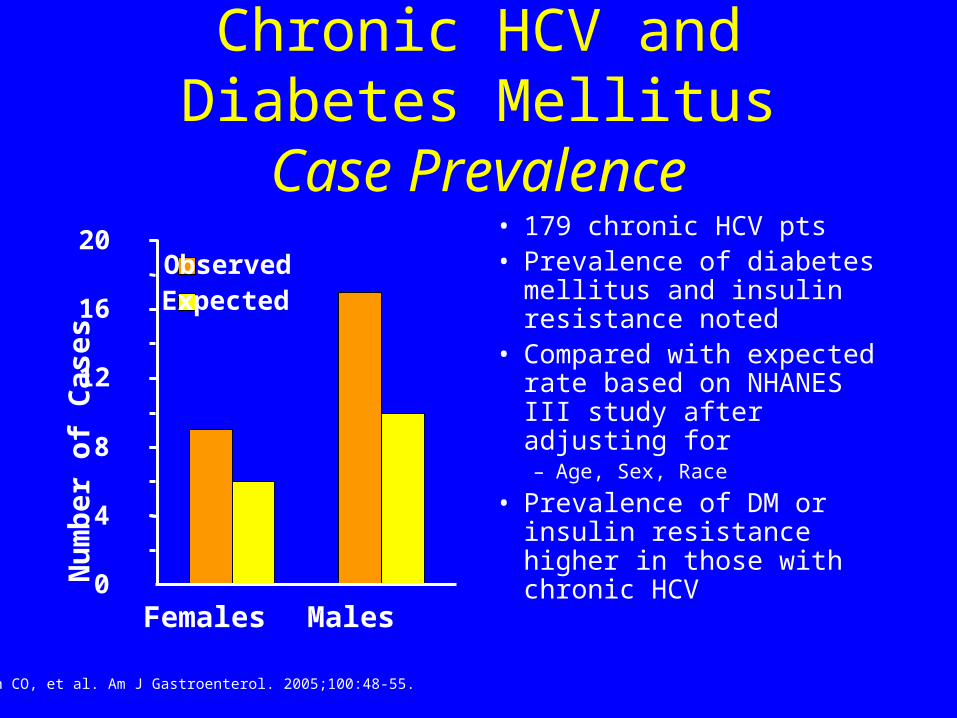
Chronic HCV and Diabetes Mellitus
Case Prevalence• 179 chronic HCV pts• Prevalence of diabetes
mellitus and insulin resistance noted
• Compared with expected rate based on NHANES III study after adjusting for– Age, Sex, Race
• Prevalence of DM or insulin resistance higher in those with chronic HCV
0
4
8
12
16
20
Females Males
Nu
mb
er o
f C
ases
ObservedExpected
Zein CO, et al. Am J Gastroenterol. 2005;100:48-55.
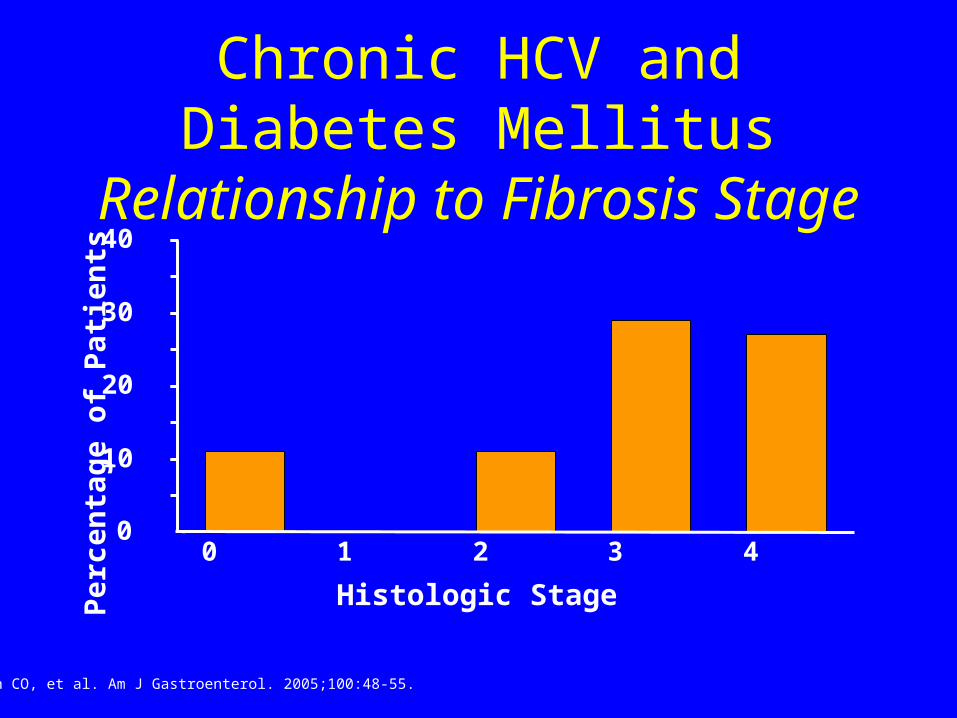
Chronic HCV and Diabetes Mellitus
Relationship to Fibrosis Stage
0
10
20
30
40
0 1 2 3 4
Histologic Stage
Per
cen
tag
e o
f P
atie
nts
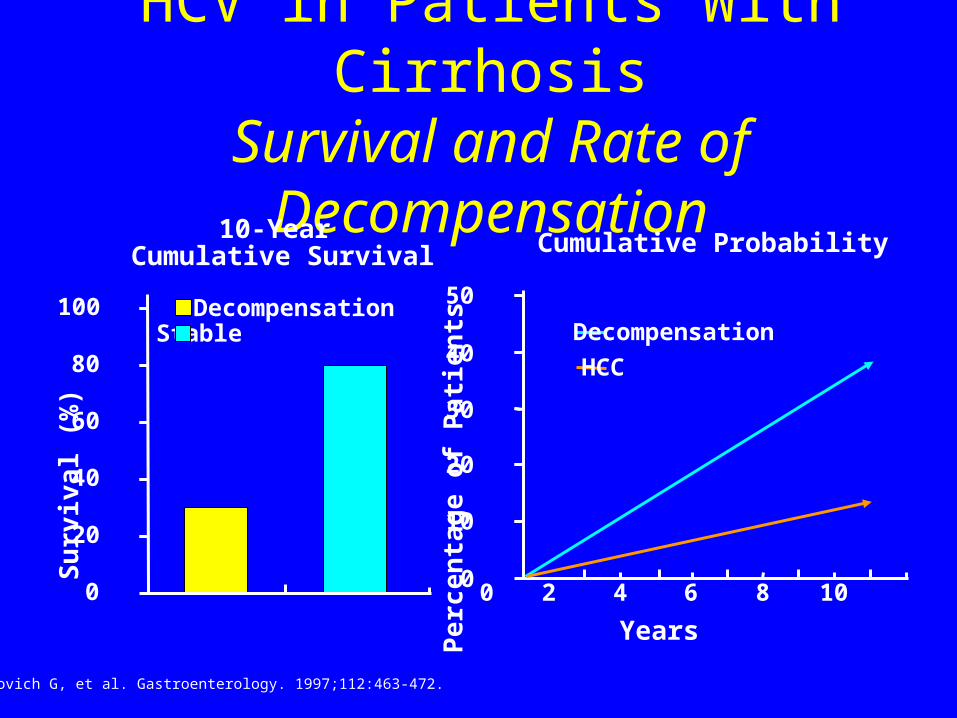
Fattovich G, et al. Gastroenterology. 1997;112:463-472.
HCV in Patients With CirrhosisSurvival and Rate of
Decompensation
0
20
40
60
80
100
Su
rviv
al (
%)
StableDecompensation
10-Year Cumulative Survival
0
10
20
30
40
50
0 2 4 6 8 10
Years
Pe
rce
nta
ge
of
Pa
tie
nts
Decompensation
HCC
Cumulative Probability

HCV RNA and Liver HistologyFibrosis
Genotype
NoFibrosis
PortalFibrosis
BridgingFibrosis
Cirrhosis
Serum HCV RNA does not correlate with level of fibrosis
0
2
4
6
8
Lo
g H
CV
RN
A(c
op
ies/
mL
)
1
2
3
4
Ferreira-Gonzalez A, et al. Semin Liver Dis. 2004;24:9-18.