Embed Size (px)
Citation preview

Ronald Chrisbianto Gani405090223
Faculty of MedicineTarumanagara University
EMERGENCY MEDICINE BLOCK
THERMAL BURNS

THERMAL BURNS

THERMAL BURNS
• Injuries to the skin resulting from contact with heat, electrical current, radiation, or chemical agents
• Less than 44oC well tolerated• Above 60oC denaturation of protein
Rosen’s Emergency Medicine 7th Ed

EPIDEMIOLOGY
• American Burn Association– 500.000 burn injuries, 40.000 admissions– 4.000 deaths– Caused by : Fire (46%), scalds (32%), hot objects
(8%), electricity (4%), chemical agents (3%)– 38% >10% TBSA, 10% >30% TBSA– Age 19-44– Location : UE (41%), LE (26%), Head & Neck (17%)– <5% full thickness
Rosen’s Emergency Medicine 7th Ed

PATHOPHYSIOLOGY
• Three concentric zone– Zone of irreversible coagulative necrosis– Zone of ischemia– Zone of hyperemia
• Regeneration comes from– Basal layer of cells– Dermal skin appendages (hair follicles and
sebaceous glands)
Rosen’s Emergency Medicine 7th Ed

PATHOPHYSIOLOGY
• Clotting inflammatory cells recruitment (B2-
integrins, CD11b, CD18) cells marginate to vessel walls (ICAM-1) release of mediators and cytokines (cytotoxic reactive oxygen and nitrogen species) lipid peroxidation accumulation of leukocytes, RBC, platelet microthrombi reduce local perfusion
Rosen’s Emergency Medicine 7th Ed

PATHOPHYSIOLOGY• Inhalation injury– Caused by steam, aldehydes, oxides of sulfur and
nitrogen, PVC, Hydrochloric Acid, CO– Airway edema & de-epithelization of injured
mucosa necrotic lining pseudomembranous cast airway obstruction
– Edema & congestion of pulmonary parenchyma bronchospasm, inflammation, destruction decreased lung compliance microatelectasis progressive hypoxemia ARDS
Rosen’s Emergency Medicine 7th Ed
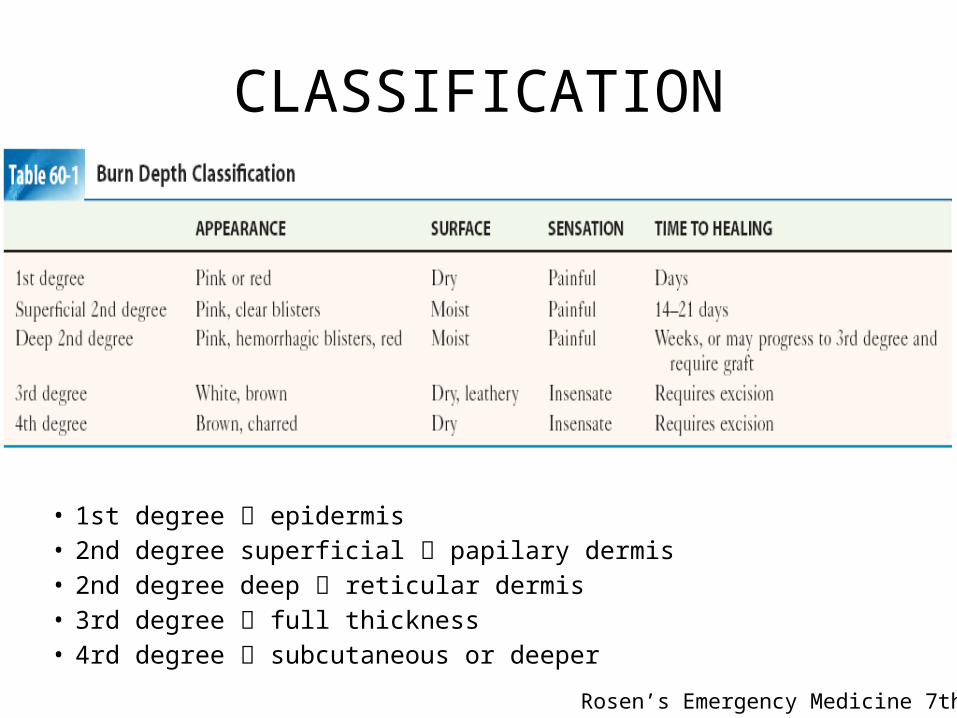
CLASSIFICATION
• 1st degree epidermis• 2nd degree superficial papilary dermis• 2nd degree deep reticular dermis• 3rd degree full thickness• 4rd degree subcutaneous or deeper
Rosen’s Emergency Medicine 7th Ed

CLASSIFICATION• Percentage of TBSA involved– Rules of nine : 18% front trunk, 18% back trunk,
18% each LE, 9% each UE, 9% head & neck, 1% perineal
Rosen’s Emergency Medicine 7th Ed

CLASSIFICATION
LUND-BROWDER CHART
Rosen’s Emergency Medicine 7th Ed

1ST & 2ND DEGREE BURN INJURY
1st degree
Rosen’s Emergency Medicine 7th Ed
Fitzpatrick’s Dermatology in General Medicine 7th Ed

3RDDEGREEBURN
INJURY
Rosen’s Emergency Medicine 7th Ed
Fitzpatrick’s Dermatology in General Medicine 7th Ed

4TH DEGREE BURN INJURY
Fitzpatrick’s Dermatology in General Medicine 7th Ed

MANAGEMENT
• Prior to ED arrival– Stop burning process, extinguish flame, chemical
injury tap water wash– Protect from additional injury– Adequacy of airway and ventilation intubation– CO poisoning 100% oxygen – Extensive burns IV fluid LR, Parkland Formula– Morphine sulfate 2-4mg IV bolus– Cover burns with clean dressing– Prevent hypotermia
Rosen’s Emergency Medicine 7th Ed
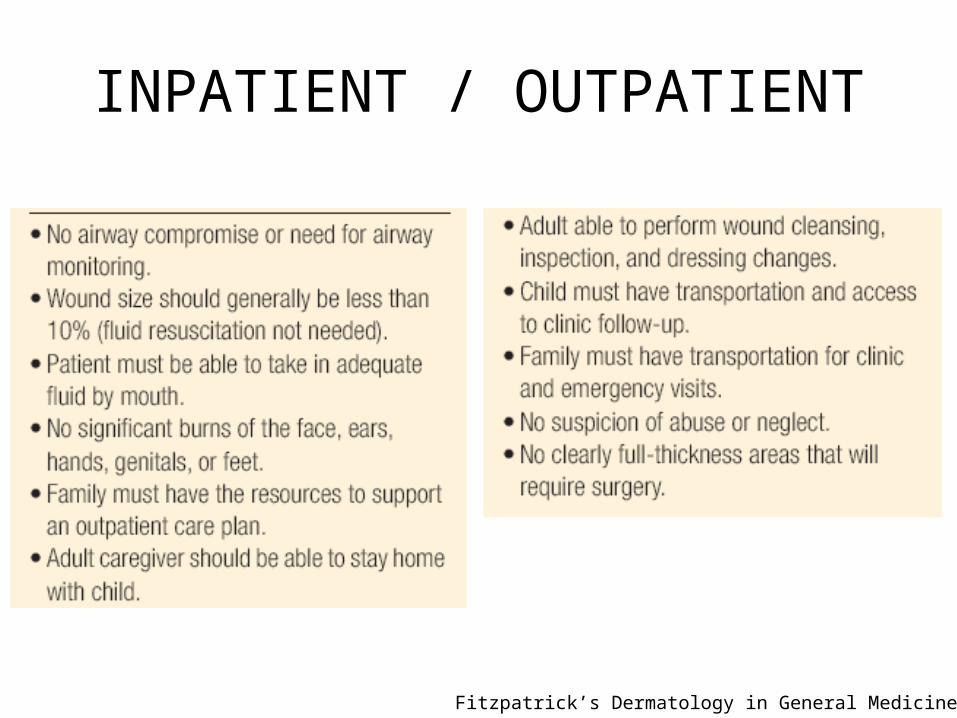
INPATIENT / OUTPATIENT
Fitzpatrick’s Dermatology in General Medicine 7th Ed

MANAGEMENT
• At Emergency Department (ABC!!)– Airway • Check for upper airway edema fiberoptic
laryngoscopy• Endotracheal intubation or crycothyrotomi if needed• Escharotomies if needed• Maintain PO2 >92%• Urethral catheter monitor urine output and eval for
rhabdomiolysis and myoglobinuria• NGT prevent gastric distention
Rosen’s Emergency Medicine 7th Ed

MANAGEMENT
– Inhalation Injury• Fiberoptic laryngoscope & bronchoscopy soot,
charring, inflammation, edema, necrosis• Injury to parenchyma xenon ventilation (RARE)• Other : CO and cyanides• Treatment : mechanical ventilation, aleveolar lavage,
PO2 >92%, airway pressure <35cm H2O, pH >7,25• Bronchospasm bronchodilators + suctioning• N-acetylsistein with/without heparin aerosolized
breakdown thick mucous
Rosen’s Emergency Medicine 7th Ed

Rosen’s Emergency Medicine 7th Ed

MANAGEMENT
– Circulation and Fluid Resuscitation• Burn injury activate PG, Histamine, LT Intravascular
fluid extravasation fluid depletion + soft tissue edema• Small burns oral fluid, Large burns IV fluids• Volume Parkland Formula + adjustment as needed• Adjustment criteria : HR, BP, Conciousness, Capilarry
Refill, urine output.• Additional fluid : inhalation injury, electrical burn• Excessive fluid pneumonia, sepsis, ARDS, death
Rosen’s Emergency Medicine 7th Ed
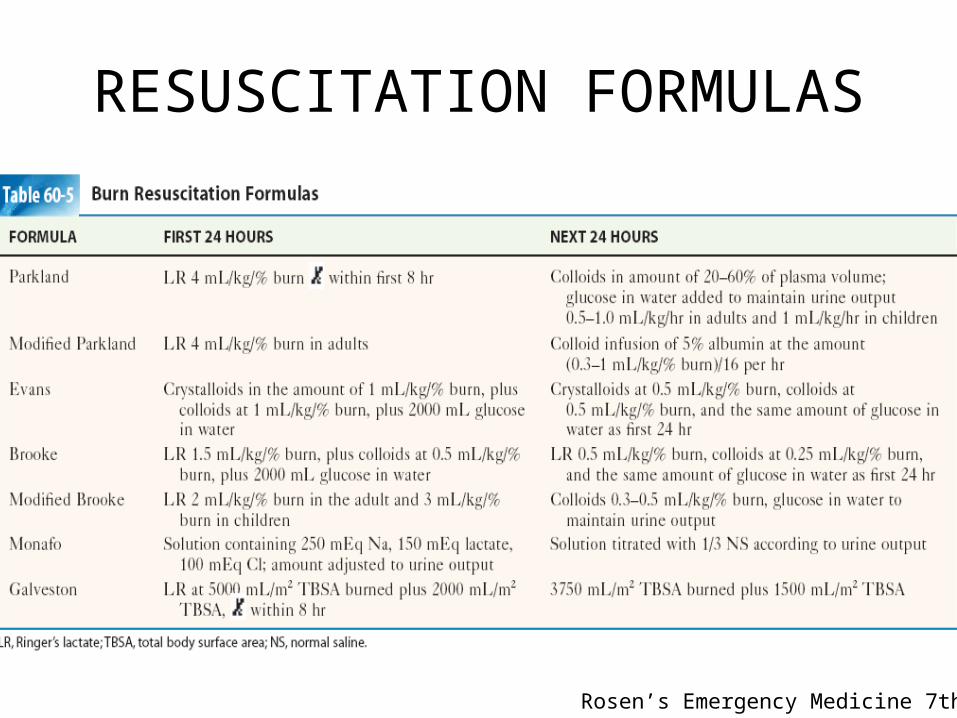
RESUSCITATION FORMULAS
Rosen’s Emergency Medicine 7th Ed

MANAGEMENT
• Local Wound Care– Cleansing with soap + water, removal of debris
and necrotic tissue, TT booster– Cooling : tap water 10o-25o C up to 30mins after
injury, avoid hypothermia, ice/ice water contraindicated
– Burn Blisters : Fluid confined by necrotic skin heal faster less infection, 2nd degree debridement + intact less scaring, heal faster
Rosen’s Emergency Medicine 7th Ed

MANAGEMENT
– Burn dressing• Open method : antimicrobial topical until skin is re-
epithelialized. Used on exudative burn. Mostly used silver sulfadiazine and mafenide acetate. Daily removed• Closed method : moist wound healing environment
heal faster. Mostly used : Nanocrystalline silver. • At home : washing, apply topicals. Occlusive should not
be opened unless saturated or malodorous go to ER. If swelling of fever go to ER
Rosen’s Emergency Medicine 7th Ed

BURN DRESSINGS
Rosen’s Emergency Medicine 7th Ed

MANAGEMENT
• Escharotomy– Releasing constriction of burn eschar with scalpel– Eschar constriction interrupts arterial outflow
pain, loss of sensation, delayed capilarry refill. – Indication: Doppler Signal & Pulse oximetry <90% – Avoid to cut underlying vessels and nerves
Rosen’s Emergency Medicine 7th Ed
MANAGEMENT
• Pain Types and Management– 3 phases of burn recovery• Emergency / Resuscitative Phase• Healing Phase• Rehabilitative Phase
– In Emergency Phase, there are 3 kinds of pain• Background Pain• Breakthrough Pain• Procedural Pain
Rosen’s Emergency Medicine 7th Ed

MANAGEMENT– Non pharmacologic• Cooling, tap water 10o-25oC• Moist occlusive dressing
– Pharmacologic• Morphine Sulfate (0,05-0,1mg/kg) titrated• Acetaminophen (1g adults, 15mg/kg child) /4-6h• Ibuprofen (400-800mg adults, 10mg/kg child) / 6-8h• Fentanyl 0,5-1mg/kg• Lidocaine• Anxyolytics : benzodiazepin (Lorazepam)• Others : gabapentin, stimulants, B-Blockers, antidepressants
Rosen’s Emergency Medicine 7th Ed

COMPLICATION
Fitzpatrick’s Dermatology in General Medicine 7th Ed

COMPLICATIONStreptococcal Cellulitis
Fitzpatrick’s Dermatology in General Medicine 7th Ed
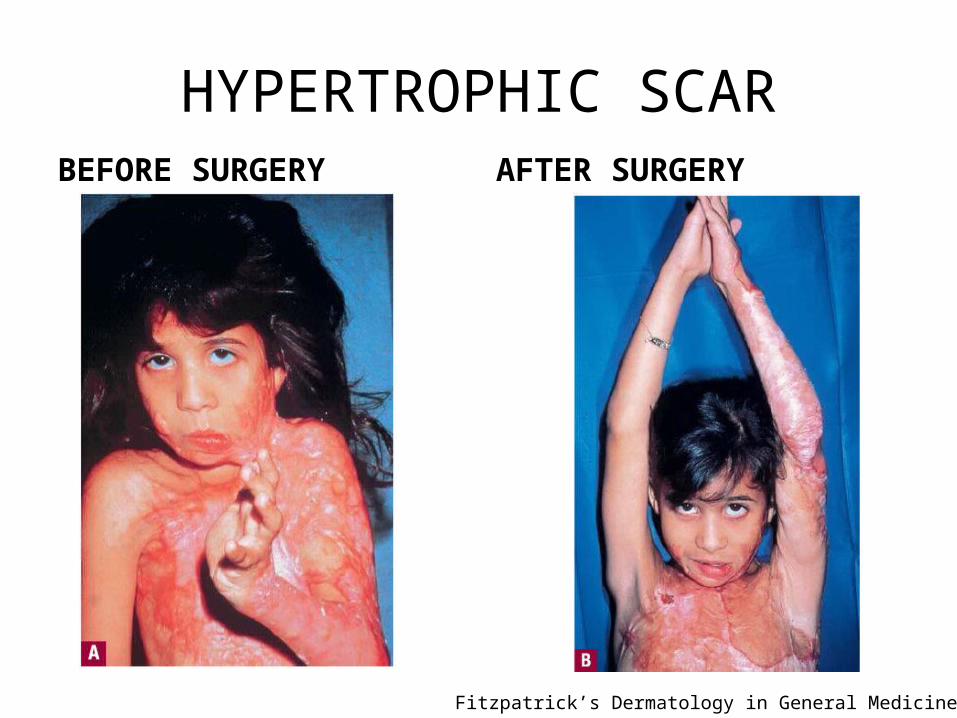
HYPERTROPHIC SCARBEFORE SURGERY AFTER SURGERY
Fitzpatrick’s Dermatology in General Medicine 7th Ed

BURN PREVENTION
Rosen’s Emergency Medicine 7th Ed

REFERENCES
• Marx JA, Hockberger RS, Walls RM, Adams JG, editors. Rosen’s Emergency Medicine Concepts and Clinical Practice. 7th Ed. Philadelpia : Mosby Elsevier, 2010
• Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, editors. Fitzpatrick’s Dermatology in General Medicine. 7th Ed. New York : McGraw-Hill, 2008





























