Embed Size (px)
Citation preview

www.mjms.usm.my © Penerbit Universiti Sains Malaysia, 2013 For permission, please email:[email protected]
Introduction
Hotwaterfacialscaldingleadingtoblindnessisrareamongadults.However,itcanresultfromassault and accidents (1). A hotwater burn is athermalinjury,anddirectcontactwiththeeyemayresult inblindnessifnotproperlymanaged.Thethermal burn causes superficial epithelium celldeath,althoughthermalnecrosisandpenetrationcan occur (1,2). Thermal eye injury triggers aninflammatory response by various inflammatorycells,whichresults in therapidaccumulationofextravascular fluid in the ocular tissue (3). Theocular effect dependson the temperature of thewater, and the final visual outcome dependson many factors, including the promptness ofpresentation to the hospital (1), severity of theburn, application of traditional medication(4–8),andavailableexpertise.Thispaperreportsa 23-year-old woman who sustained a facialor ocular scald, used traditional medicationand presented late to the hospital, resulting inuniocularblindness.
Case Report A 23-year-old breast-feeding motherpresented to our hospital following a facial hotwater injury that occurred three days prior.Thebucketofhotwater shewascarrying to the
Case Report
Submitted: 22Jun2012Accepted: 26Jul2012
Uniocular Blindness Following Thermal Injury
Abdulkabir Ayansiji AyAnniyi1, Monsudi Kehinde FAsAsi2
1 Department of Ophthalmology, College of Health Sciences, University of Abuja, P.M.B 117 Abuja 902101, Nigeria
2 Department of Ophthalmology, Federal Medical Centre, Birnin Kebbi, Nigeria
Abstract Ahotwaterburnisathermalinjurythatresultsincelldeath.Thermaleyeinjurytriggersinflammatory processes, including inflammatory cell influx and/or the activation of variousinflammatorycells,whichresultintherapidaccumulationofextravascularfluidintheoculartissue.Theoculareffectdependsonthetemperatureofthewater,andthefinalvisualoutcomedependsontheseverityof thedamageto the intraocularstructures.Wereporta23-year-oldwomanwhoexperienceda facialhotwaterburn that resulted inblindness.Thepatientpresented late to thehospital after theunsuccessful use of traditionalmedication. Facial burns are a known causeofblindness.Publichealtheducationonprompthospitalpresentation,andresistance to theuseofpotentiallyharmfultraditionalmedicineinfacialburnsissuggested.
Keywords: herpes zoster ophthalmicus, hot water burn, traditional eye medication
bathroom fell, and the hot water splashed intoher face.Sheexperiencedassociated; facialpainand swelling, and right eye (RE) symptomsincluding pain, redness, tearing, photophobia,andareductioninvision.Sheenjoyedgoodvisionbilaterallypriortotheincident.Sheimmediatelyirrigatedherfacewithwater,andapproximatelyfive minutes later, she applied traditionalmedication (TM) to her face and RE. Two daysafter the incident,shenoticedREdischargeandvery poor vision. The patient had no significantpast medical or ocular history. At the time ofpresentationtotheaccidentandemergency(A&E)unit, the medical officer on duty admitted thepatient for anophthalmologist review, as a caseofherpes zosterophthalmicus (HZO).Ageneralexaminationrevealedadepressedyoungwoman,whowasafebrilewithafacialscald(mainlyrighthemifacial)thatwascoveredbyblackconcoctionextending from her forehead to her chin(Figure1).Anocularexaminationdemonstratedthat her visual acuity (VA)was countingfingers(CF) intheREand6/6inthe lefteye(LE).TheRE showed the presence of lid scald/periorbitaledema, complete mechanical ptosis, purulenteye discharge, diffuse conjunctival hyperemia,180degreelimbalischemia(3–9o’clock),ahazycornea, a normal anterior chamber depth, a
88Malays J Med Sci. Jan-Mar 2013; 20(1): 88-91

Case Report |Facialburnassociatedblindness
www.mjms.usm.my 89
glimpseofroundpupilandiris,andapoorviewof the fundus.A slit lamp examination revealeda central corneal ulcer approximately 4 mm indiameter.Herlefteye(LE)wasessentiallynormal.Adiagnosisofaright-sidedsuperficialfacialhotwater burnwithRE involvementwasmade. Allof the laboratory investigations, including a fullblood count and fasting blood sugar, revealedno abnormalities. Right eye swab microscopy,culture,andsensitivitywerenotremarkable.Thepatient was admitted, and facial debridementwas performed. The patient was treated withintravenousciproxin,200mgevery12hoursfor48 hours, and metronidazole, 500 mg every8 hours for 48 hours. Anti-tetanus serum(750IU)wasalsoadministeredintramuscularly.Additionally, thepatientwastreatedwithguttaeatropine (1%) every 12 hours, ciprofloxacinevery 4 hours, flurbiprofen every 6 hours andchloramphenicol eye ointment. Furthermore,the patient received tablet cataflam, 50 mgevery 12 hours for 5 days, and ascorbic acid,
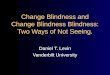
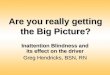
100 mg every 8 hours for 7 days. Dermacerinecream was applied to the facial wound every6–8 hours for 10 days. At 48 hours afteradmission, the intravenous antibiotics werechanged to oral antibiotics (tablet ciprotab,500 mg every 12 hours, and metronidazole,400mgevery8hoursforoneweek).Onthe3rddayafteradmission,thefacialburnshowedsignsofhealing,andthelidswellinghadreduced,buttherewasstillcompletemechanicalptosisoftheRE.Anexaminationonthe5thdayafteradmissionrevealed rapid healing of the facial burn withright lower lid ectropion, a reduced intensity ofcornealstainingwitharedreflex,andaglimpseofasuperiorretinaonfundoscopy(Figure2).Theectropionwasmanagedbyplastertapping. The patient recovered well and wasdischarged two weeks after admission with anRE visual acuity of CF, diffuse central cornealopacity (Figure 3) and an intraocular pressureof 14mmHg. The patient was lost to follow upfollowingdischarge.
Figure2:Thepatienton the5thday followingadmission.
Figure 1:The patient at presentation (3rd dayafterthescald).

90 www.mjms.usm.my
Malays J Med Sci. Jan-Mar 2013; 20(1): 88-91
Discussion
This paper reported a 23-year-old womanwho sustained a facial or ocular burn leadingto uniocular blindness. An ocular burn is anophthalmic emergency (9), whether it is achemicalor radiant injury,because rapidoculartissue damage occurs. Radiant injuries caninvolvehot liquids,hotgases,moltenmetals,orultraviolet rays. The severity of an ocular burnis related to the duration of exposure, and theoffending agent. Burns inflict damage primarilyby denaturing and coagulating tissue proteins,and secondarily through ischemic vasculardamage. Typically, thermal burns are limitedto the superficial epithelial cells, but thermalnecrosisandpenetrationmayoccur(9). The proportion of ocular burns among eyeinjuries ranges between 7%–18% (10), and eyeinjuries account for 3%–4% of all occupationalinjuries (11). Most (84%) are chemical burns,whilethermalburnsrepresent16%ofocularburncases. Approximately 15%–20% of facial burncases have a secondary ocular injury. Burns arenotageorgenderspecific,butyoungeragegroups
andmalesappeartobemoreatrisk.Thesegroupsmay bemore exposed to/engaged in situations/vocationswithahighriskforocularinjury. It is of note that complications sometimesfollowocularburns,includingeyelidcontractures,conjunctivitis,cornealdefects(epithelialdefects/ulcer, conjunctival cells invasion, perforation,scarring), cataracts, raised intraocularpressure/glaucoma, retinal detachment and impairedvision/blindness(12,13). Theprognosisofanocularburndependsonthedepthoftheinjury.Inmildtomoderatecases,the outcome is good, while severe cases mayrequire serious intervention, including cornealtransplant or rehabilitation services (14). Themajorconcernswithocularburnsarefinalvisualacuityandcosmesis.Withprompttreatmentandearlyophthalmologicintervention,thermalburnsgenerallyhavegoodvisualoutcomes(9). Thiscaseoccurredduringthecoldseasonofharmattan, and it is a common practice amongpeople to warm up ‘harmattan cold’ water withhot water for a bath. This case illustrates thetypical rural management of health conditions,including hot water burns, and their oculareffects, inagreementwithaprevious report (2).Many health conditions are first managed withtraditional medications, and orthodox care isonly soughtwhen thecondition fails to improveor deteriorates. Early presentation would haveimproved the visual prognosis, and reduced thedurationofhospitalstayinthispatient,asreportedelsewhere(1).Additionally,thiscaseillustratestheoculareffectoftraditionaleyemedication(TEM),and agrees with similar studies in developingcountries (4–8). The corneal ulcer may havebeenduetothehotwaterburn,theTEMorboth.Although theeye swab testwasnot remarkable,an eye infection was suspected and manageddue to the breach of the epithelium (from theburn),andpossibleinoculationwithaninfectingorganism by TEM, which has been reported invariousstudies(4,5,8).Thehemifacialaffectationof the burn resulted in the inclusion of herpeszosterophthalmicus in thedifferentialdiagnosisof this patient. However, a carefully takenmedical history (clerking) should have assistedthemedical officer in the A&E unit to correctlydiagnose this patient even without any medicalinvestigation. The right hemifacial affectationwas remarkable, and it could be reasoned thatthebucketcontaininghotwaterwascarriedwithher right hand and was closer to the right sideof her face when the accident occurred. Plastertapping corrected the right lower lid ectropion.Theanti-tetanusprophylaxiswasjustifiedinthis
Figure3: The patient at discharge (2weeks oftreatment).

Case Report |Facialburnassociatedblindness
www.mjms.usm.my 91
patient because of the epithelial breach by theburn andbecauseTEM is potentially infectious.Welostthebenefitofassessingthevisualacuityintheaffectedrighteyeafterdischargefromthehospital because the patient was lost to followup.Losingpatientstofollowupisachallengetohealth care in our health facility and elsewhere(8).Nonetheless, shouldhervisualacuity fail toimprove,thispatientmaybenefitfromacornealtransplant in the future.However, judging fromthepatient’ssocialindices,shemaynothavebeenbotheredbytheblindnessinherrighteyeaslongasherlefteyeremainedvisuallyfunctional.Evenif an improvement in her right eye vision wasdesired,shemaynothavebeenabletoaffordtheexpenseswithoutassistance.Suchchallengesfacemanyacrosstheglobewhosufferfromavoidableblindness.
Conclusion
In conclusion, the late presentation to thehospitalandtheuseoftraditionalmedicineledtoblindnessinthispatient.Facialburnsareacauseofblindness.Theneedforpublichealtheducationonprompthospitalpresentationandresistancetotheuseofpotentiallyharmfultraditionalmedicinein facial injuries is suggested. Precautionarymeasuresagainsthomeaccidentsleadingtofacialburnswouldreduceavoidableblindness.
Acknowledgement
This study was sponsored by the authors;therewasnoexternalfinancialassistance.
Authors’ Contributions
Conceptionanddesign,analysisandinterpretationof the data, drafting and final approval of thearticle,criticalrevisionofthearticleforimportantintellectualcontent,provisionofstudymaterialsor patients, statistical expertise, obtaining offunding, administrative, technical or logisticsupport, and collection and assembly of data:AAA,MKF
CorrespondenceDrAyanniyiAbdulkabirAyansijiMBBS(Ibadan),FMCOpthal(Nigeria)DepartmentofOphthalmologyCollegeofHealthSciences,UniversityofAbujaP.M.B117Abuja902101,NigeriaTel:+23-48058548765Fax:+09-8821380Email:[email protected]
References
1. Monsudi KF, Ayanniyi AA. A 14-year-old girlwho regained normal vision after bilateral visualimpairment following hot water injury to the eye.Saudi J Ophthalmology. 2011;25(2):2207–2210.
2. MelsaetherCN,RosenCL.Burn,ocular:differentialdiagnoses and work up, treatment and medication,followup2009.Medscape Ref.2011.Availablefrom:http://emedicine.medscape.com/article/798696.
3. deBandtJP,Chollet-MartinS,HernvannA.Cytokineresponse to burn injury: relationship with proteinmetabolism.J Trauma. 1994;36(5):624–648.
4. Catherine UU, Nanaiashat M. Incidence andComplications of Traditional Eye Medications inNigeria in a Teaching Hospital. Middle East Afr J Ophthalmol. 2010;17(4):315–319.
5. Baba I.TheRedEye:First aid at theprimary level.Community Eye Health.2005;18(53):70–72.
6 Courtright P, Lewallan S, Kanjaloti S, Divala DJ.Traditional eye medicine use among patients withcorneal disease in rural Malawi. Br J Ophthalmol. 1994;78(11):810–812.
7. Prajna VN, Plllai MR, Manimegalai IK, SrinivasanM. Use of traditional eye medications by cornealulcerpatientspresentinginahospitalinSouthIndia.Indian J Ophthalmol. 1999;47(1):15–18.
8. Ayanniyi AA. A 39-year-old man with blindnessfollowing the application of raw cassava extractsto the eyes. Digital J Ophthalmology. 2009;5(2).Availablefrom:www.djo.harvard.edu/site.php?url=/physicians/gr/1328.
9. WeaverCNM,RosenCL.OcularBurns.Medscape Ref:2011. Available from: http://emedicine.medscape.com/article/798696-overview.
10. MerleH, GerardM, SchrageN. Ocular burns. J Fr Ophtalmol.2008;31(7):723–734.
11. XiangH,StallonesL,ChenG,SmithGA.Work-relatedeyeinjuriestreatedinhospitalemergencydepartmentsintheUS.AmJIndMed.2005;48(1):57–62.
12. Stern JD, Goldfarb IW, Slater H. Ophthalmologicalcomplications as a manifestation of burn injury.Burns.1996;22(2):135–136.
13. Kuckelkorn R, Schrage N, Keller G, Redbrake C.Emergency treatment of chemical and thermal eyeburns.Acta Ophthalmol Scand. 2002;80(1):4–10.
14. WagonerMD. Chemical injuries of the eye: currentconcepts in pathophysiology and therapy. Surv Ophthalmol. 1997;41(4):275–313.