Embed Size (px)
Citation preview

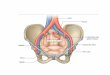
Removal of the Uterus and Its Appendages for PelvicInflammatory Disease. 1
J., M. BALDY, M.D.,
Professor of Gyncecology in the Philadelphia Polyclinic ; Surgeon to theGynecean Hospital.
It was supposed when we had alllearned the lesson that Mr. Taitfought so long and valiantly to teachus, that the question of the treatmentof pelvic inflammations and theirravages had been finally settled. Theremoval of the displaced and adherentFallopian tubes and ovaries, whichcontained pus or whose tissues werehypertrophied and infiltrated withchronic inflammatory products, soonbecame a common procedure and thetechnique of the operation was sorapidly pushed to perfection thatmany operators arose whose resultssuccessfully rivaled those of Taithimself. Large numbers of womenwho had formerly been doomed to ahopeless invalidism were now restored
1 Read before the Obstetrical Society of Phila-delphia, October $, 1893.
to health and useful lives. So fre-quently were these happy results ob-tained and reported to an expectantprofession that sight was lost alto-gether, for the time, of certain cases,afflicted with these same diseases, onwhom the same operation had beenperformed, but who were not blessedwith the same good results as theirmore fortunate sisters. The glamorof success of an entirely new andbrilliant procedure so greatly over-shadowed these poor sufferers thattime was necessary before attentioncould be directed towards them. Asis often the case the enemies of thenew procedure were the first to pointout this class, not from any particulardesire to aid in the complete solutionof the problem, but from a spirit ofcriticism which says, “ Lo and behold!

J. M. BALDY.2
thy vaunted remedy has failed.” Ithad failed to a certain extent, it istrue, and the taunt sufficed to drawcloser attention to the failures and adeeper study as to why they hadfailed.
You are all of you cognizant ofpatients in your practice on whom anabdominal section has been performedfor pelvic inflammatory disease, whoconsults you for continued bleeding,leucorrhoeal discharges (often pro-fuse) and pain—women who havehad the operation performed for thesesymptoms and who complain now,three months, six months, a yearafter the operation, of the same kindand the same amount of suffering.You are familiar with such cases,coming both from your own practiceand that of your neighbor. Theycome into the public clinics in consid-erable numbers complaining of theoperator and refusing to return tohim for the reason that they hadthought the operation would curethem, and because it had not theirdoctor was to blame, as usual, and asa matter of course. These are thesame patients who are held up to usas a proof that our method of treat-ment is wrong and has failed andshould, therefore, be condemned intoto. The time has not even yetpassed when we must submit to justsuch spurious criticism.
But, as a matter of fact, a certaintoo large proportion of our patientsstill remain uncured by a simpleremoval of the uterine appendages;and let me emphasize the fact that Iam now discussing a class of patientswho have an easily demonstrableamount of disease of these organs—-no reference is intended to that toonumerous class on whom operations
are performed for symptoms alone,no disease being found by a physicalexamination and none capable of cleardemonstration even after the organshave been removed.
Local applications to the uterusafter a coeliotomy for removal of theappendages has been tried, with nogreater success than the same amountof treatment before the surgical pro-cedure. Curettement of the wombhas been followed with little moreencouraging results. I have adoptedthis course in some six or ten cases,and have not been able in a singleone to say that I had cured thewoman. The majority of them ceasedcoming for treatment long before anydecided result had been obtained.During the past winter it was mymisfortune to see a number of thesewomen who had been unrelieved oronly partially relieved in spite of thefact that a complete and clean re-moval of both appendages had beenmade and that the remaining uteriwere freely movable. No troublecould be detected in the pelvis by amost careful and repeated physicalexamination.
After applying local and generaltreatment to several of these women,until we were both discouraged anddisgusted, I, in despair, suggestedthat the womb itself be removed. Iwas led to this decision from the factthat I had known some months be-fore of a case on whom my colleague,Dr. Baer, had performed several ab-dominal sections in, I think, a neu-rotic case, without obtaining much re-lief, and upon whom he had finallyperformed hysterectomy with an ex-tremely satisfactory result. This, inaddition to the work being done inFrance in the way of hysterectomy

REMOVAL OF UTERUS AND ITS APPENDAGES. 3
for pelvic abscesses, evidently influ-enced my thoughts in this direction.The woman to whom I proposed theoperation had had her original opera-tion for suppurating uterine append-ages. Months after her operationshe still had a large uterus, irregularbleeding, profuse leucorrhoeal dis-charges, great backache and pelvicbearing-down pains. The uterus wasremoved by supra-vaginal amputationlow down into the cervix, and drop-ping the stump back into the pelvis.Her recovery was an uninterruptedone. The bleeding and leucorrhoealdischarges ceased at once, and thepelvic pains and backache almost en-tirely disappeared, the little that re-mained of them being evidently dueto the menopause. Encouraged bythis result, I have continued this lineof treatment up to the present time,and have now had sufficient experi-ence to feel warranted in recommend-ing the procedure to your carefulconsideration and trial. In two caseshave I removed the uterus subsequentto a simple removal of the append-ages. Six times have I removed itat the primary operation.
It is well known that in pelvic in-flammation the disease first affectsthe womb, and secondarily invadesthe Fallopian tubes and the pelvicperitoneum. Not only is the endo-metrium affected, but the inflamma-tory products invade the deeperstructures which go to make up theuterine walls. If a suppurative pro-cess follows, these infiltrates undergothe same changes as do the same ele-ments in the walls of the Fallopiantubes. The ease with which a liga-ture cuts through uterine tissue,when applied at the cornua in casesof pus tubes, is a well-known demon-
stration of the truth of this. With aFallopian tube and uterus, both ofwhich are diseased by the same fac*tor and to the same extent, is itrational to suppose that a cure is tobe always obtained by the removal ofthe tube alone? Is it not commonsense to remove the whole of the dis-ease, and not only a part ? Theoryand practice both combine in thismatter to force the conclusion.
It must not be understood that Irecommend the removal of the uterustogether with the Fallopian tubes andovaries in all cases of pelvic inflam-matory disease. In many cases theuterus has succeeded in throwing offthe original infection, and is compara-tively healthy. Under such circum-stances the procedure is not indi-cated. But where an abdominal sec-tion is performed for the removal ofthe uterine appendages, and thewomb is found enlarged and diseased,especially if it has been surroundedby extensive adhesions, and the free-ing of it leaves large areas of " °dperitoneum, hysterectomy should oethe operation of choice. But a singleobjection can be raised to this propo-sition, viz., the mortality of the opera-tion. Can, then, hysterectomy beperformed as safely as ovariotomy ?
Unhesitatingly I answer in theaffirmative. My own hysterectomiesnow number more than eighty, withseven deaths. These deaths includethe accidents incident to acquiringthe skill and perfecting the tech-nique ; in a similar series the resultswill be infinitely better.
Beyond the question of mortalitythere can be no doubt as to the ad-visability of removing the diseaseduterus. With its appendages gone itis an altogether useless organ, and

J. M. BALD Y4
even the old, familiar cry of mutila-tion and unsexing the patient hasno place.
I am free to confess that sinceadopting this method of practice thefield for hysterectomy has greatlywidened. For instance, I assentedand assisted in an operation for theremoval of the uterus in a womanupon whom seven abdominal sectionshad been performed without givingher relief. The uterus was enlarged,and was found to contain severalsmall fibroid nodules, as large as ahickory nut, which had undergonecalcareous degeneration. The patientwas relieved at once, and continuedso for some months, when she dis-appeared from observation.
Only last Sunday I performed anabdominal section for double ovariancysts. One cyst proved to havegrown into the broad ligament, while
the second one was free. The uteruswas very large, half as large again asnormal. The operation was finishedby making a clean sweep of bothtumors, Fallopian tubes and uterus.The patient is convalescent, and is, Ithink, distinctly better without thewomb, which I exhibit to you.
Looking at this matter as I do, ithas been no great matter of surpriseto me to find other operators adopt-ing this procedure. Last spring,while visiting in New York, I foundthat Krug had arrived at much thesame conclusion, and was followinga like practice. During a recentvisit to Chicago I discovered thatHeurotin was working on the samelines, and I have no doubt but thatafter a winter’s agitation on thesubject most of the profession willbe won over to a similar manner ofthinking and to the same practice.