Embed Size (px)
Citation preview

Pédiatrie Dentistry
The treatment of nonvital immature teeth with calcium hydroxide-sterilewater paste: Two case reports
Gamze Erdogan, DDS, PhD*
Abstract Death of the dental pulp before completion of rool development results in a toolhwith an open apex. During endodontic treatment, the open apex makes obturationdifficult, because there is no apical stop against which iheJUling can be packed andcondensed. For many years, open apices have been treated by root canal fillingsor by periapical surgery wilh or without a reverse seat. Currently. Ihe conservativeapproach is preferred over surgical management, to avoid the physical andpsychological trauma ofsttrger}- to a young patient. Two patients were treated bycalcium hydroxide-sterile water paste to promote the apexification of the nonvitalteeth with an Incompletely formed apex. Nortnal endodontic preparation of thecanal had been carried out in the Immature tooth. Radiologie examination after6 to 9 months showed that the apex of the maxillary incisors was completed bynewly formed tisstie. (Quintessence Int 1997;28:681-686.)
Clinical relevance
Calcium hydroxide might be a good choice forinducing apical closure in young patients because ofits antibacterial and calcification-inducing proper-ties.
Introduction
The teeth most commonly traumatized in children arethe maxillary central incisors. The peak incidence fortrauma occurs between 8 and 10 years of age, when theroots of the incisors are developing. If. during thistime, the pulp becomes nonvital as a consequence ofthe traumatic episode, no ftirther development andmaturation of the root will take place, resulting in anonvital incisor with an open apex and incompleteroot development.'
' Chief, Dental Pédiatrie Clinics of Marly and Villars-s-Olâne.Fribourg,Switzerland.
Repritit requests: Dr Gamze Erdogan. 3, tue du Leman, 1301 Geneva,Swit¿er!and, Fax: 41-22-738-7544.
Apexification is a method of inducing apical closurethrough the formation of mineralized tissue in theapical pulp region of a non-vital tooth with anincompletely formed root and an open apex.- Variousclinical techniques have been aimed at inducingapexificalion in immature permanent teeth with necro-tic pulps.- Inducing apical closure by the formation ofan apical stop, generally with calcium hydroxide,[Ca(OH,)] is one of the most widely used methods oftreating a tooth that has a necrotic pulp and an openapex.-"-"
Calcium hydroxide (Caixyl) was introduced byHermann in the 1920s for endodontic treatment. In1930, Hermann'- advocated using Caixyl (OCODirmslein) for pulp capping, pulpotomy. pulpectomy,and treatment of infected canals. In 1938. Teuscherand Zander" atid Zander''' introdttced calcium hydrox-ide in the United States as a pulpotomy agent. Theinduction technique was first addressed in the UnitedStates in 1964 with separate presentations by Kaiser(Scientific session, Washington DC. 17 Apr 1964) andFrank (Table clinic, Washington DC. 19 Apr 1964) atthe 21st annual meeting of the American Associationof Endotdoctists. It was presented in the literature in1966 and popularized as the Frank technique.^^
Quintessence International... dumber 10/1997 681

Erdogan
The use of calcium hydroxide paste to promote theformation of a calcific apical barrier prior to theplacement of a gulta-percha root filling has becomewell accepted.** In 1972, Cvek" reported periapicalhealing and closure ofthe immature apical foramen byhard tissue in 90% of nonvital permanent incisorstreated with calcium hydroxide. When Andreasen'^reviewed the literature, he found that barrier formationoccurred in 74% to 94% of teeth treated with calciumhydroxide. Ghose et al'*' reported that apical closureoccurred in 96% of nonvital immature incisor teeth.
In 1988. Mackie and coworkers' reported a tech-nique using calcium hydroxide paste, which alsoproduced apical barrier formation in 96% of teethtreated. Meanwhile, Yates'^ and KJeier and Barr.'̂using various calcium hydroxide pastes, reported100% success in achieving apical barrier formation.Treatment was regarded as successful if hard tissue hadformed and closed the root canal apically and provideda base for a later permanent root filling.'' Apicalclosure that was observed after treatment in teeth inwhich the development of the root had ceased wasdescribed as a hard tissue barrier, varying in radio-graphic density, position in the canal, and the time itrequired to form.'''
Steiner and Vim Hassel-" have found Ihe formationof cementlike hard tissue after treatment of artificiallyinfected monkey teeth with calcium hydroxide mixedwith camphorated monochlorophenol. The formationof such hard tissue is believed to occur only in theabsence of microorganisms.-' -- Heithersay-' exam-ined the newly formed apex histoiogically and foundthat it consists mainly of irregular dentin. He theorizedthat the alkalinity ofthe material may have acted as abuffer to acidic inflammatory reactions. Accordirtg toKlein and coworkers.^ the histologie finding of newbone and cementum in the apical area is evidence ofsuccessHil treatment, but the mechanism of apicalclosure is still in question. Frank-'' postulated thatHenwig's sheath may play a role in root apexformation once the infection has subsided. Seltzer-^has found that, after deposition of root dentin.Hertwig"s sheath disintegrales in a coronal directionfollowing the ingrowth ofthe connective tissue ofthedental sac. When the root sheath begins to disinte-grate, cells ofthe connective tissue differentiate intocementoblasts. and cementum is deposited on thedentin. Stanley^ suggests that if the root has notcompleted its formation, in some cases, the cells ofthedental sac surrounding the wide-opened apex retainthe genetic code that predisposes them to diflerentiateinto cementoblasts.
Tronstad and coworkers"*" have shown thai the pHof untreated teeth with pulpal necrosis is between 6.0and 7,4, Teeth with complete root formation have a pHbetween 7.4 and 9.6 in the dentin away from the pulpand from 8.0 to 11.1 in the dentin next to the pulp.These investigators maintain that Ca( OH )-, neutralizesacids produced by osteoclasts.-'' Anthony and co-workers'* concluded that the alkaline environmentwould favor the formation of calcium phosphate[Ca(PO) I complexes, which would, in turn, serve asa stimulus for further calcification. Studies by Abiko-'suggest that the presence of calcium ion may activateadenosine triphosphate activity, which in turn mayaccelerate the mineralization of hard tissue such asdentin or bone, Javelet and coworkers-" also indicatedthat the alkalinity is a significant feature in the abilityof Ca(OH)., to induce hard tissue formation. Vaes'̂and Bourne-̂ " contended that CaiOH), creates anunfavorable environineni for osteoclastic activity orcan activate alkaline phosphatase enzymes,
Binnie and Rowe" compared periapical healing ofexperimentally infeeted dogs' teeth after filling theroot canals with Grossman's sealer. Calxyl. andCa(OH ), mixed with water. The Ca(OH),-waterpastedid equally well in teeth that were closed and in teeththat were left open to the oral environment.
In previous investigations, calcium hydroxide hasbeen mixed with camphorated monochlorophenol.camphorated paracholorophenol, sterile water.'- Rin-ger's solution, methyl cellulose, or iodoform''chloro-thymonal.-''' To provide opacity and thus aid in radio-graphic interpretation of the extent of the calciumhydroxide paste in the root canal system, bariumsulfate powder is added to the paste. The purpose ofthe present article is to describe results in two patientswho were treated with calcium hydroxide mixed withdistilled water.
Case reports
Case I
The maxillary left central incisor ofa 7-year-old girlhad suffered a traumatic incident 5 months previouslyThis tooth had been fractured without any obviouspulpal exposure, and the fractured surface area hadbeen covered with Dyca! (DeTrey Dentsply-Kon-stanz) and a basket crown by the general dentist towhom she had been referred. She complained thatintermittent aching had been present in the tooth forIhe previous month. Pulp testing confirmed that themaxillar>' right incisor was nonvital. and a radiographrevealed an incompletely formed apex (Fig la).
682 Quintessence International Volume 28, Number 10/1997

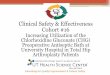
Fig 1a The Ieit central incisor had ahistory of trauma that had resulted in anecrotic pulp. The fractured area hadbeen covered with Dycal and a basketcrown 5 monfhs previously. The canalwas debrided and obturated with cal-cium hycfroxide-sterile water paste.(arrows) Immature apical formation.
Fig fb Apical development has con-tinued after the pulpecfomy procedurewith calcium hydroxide (6-month inter-val).
During the patient's first appointment, a rubber damwas placed to isolate the involved tooth, the basketcrown was removed, and the access opening into thepulp chamber was prepared. The access, through thelingtial surface of the incisor, was accomplished byremoving all impinging tooth structure at the rootcanal orifice. After the root canal was debridedbiomechanically, it was irrigated with sodium hypo-ehlorite and dried with an inverted coarse paper point,
A ratio of one part barium sulfate to eight partscalcium hydroxide was mixed with distilled water, andthe paste was placed into the root canal. The canal wasfilled with the aid ofa lentulo needle, and the paste waspressed toward the apex with cotton wool pellets ( Figlb). The paste filling in the canal was then coveredwith IRM cement (DeTrey Dentsply),
Monthly appointments revealed no clinical symp-toms, and the radiograph taken after 6 monthsrevealed the closure of the apex. The final apicalclosure permitted a fitted gutta-percha point withetidomethasone to fili the canal adequately (Fig lc).
Fig 1c Adequate penapical closurehas taken place to allow permanentendodonfic therapy
i Nlir 10/1997 683

Ef dogan
Fig 2a The maxillary right incisor had a history of traumaresulting in a necrotic pulp. As a result, the apex isincompletely formed
Figs 2b and 2c Nine months after the übturation v./\'\i calcium hydroxide paste, apicalclosure is adequate to permit root canal obturation wifh gutta-percha and endamethasone.
Case 2
An 8-year-old girl was referred for therapy on hermaxillary right central incisor, which had been frac-tured in an accident 4 months previously. The toothgave no response to vitality and thermal lests. Theradiographie examination revealed an incompletelyformed apex (Fig 2a),
Access to the root canal was accomplished byremoving all carious tissue, and therapy was initiatedwith biomechanical instrumentation ofthe root canal.After irrigation of the canal, the canal space wasobturated with a paste of calcium hydroxide.
Nine months after the first visit, apical closure wasadequate to allow permanent root catiai ñlling wilhgutta-percha and endamethasone (Figs 2b and 2c),
684 Quintessence International Volurne 28, Nutnber 10/1997

Erdogan
Discussion
Necrosis or the dental pulp before completion ofroot(development results in a lootli with an open apex.^ Thetreatment of nonvitiil teeth in children can present theclinician with a challenge because ofthe immature rootformation.^ According to Frank,^•" successful endo-dontic treatment requires that the apex ofthe treatedtooth be completely and densely sealed with root canalfilling material.
Currently there are at least five methods of treating atooth thai has a necrotic pulp and an open apex.According to Morse and coworkers,- these methodsare 11) filling the root canal wilh the large end of agutta-percha cone or customized gutta-percha conesand a sealer; (2) filling the root canal well short oftheapex (before the walls have divei^ed) wilh gutta-percha and sealer or zinc oxide-eugenol alone: (3)filling the root canal with gutta-percha and sealer aswell as possible and then performing periapical surgerywith or without a reverse amalgam seal; (4) inducingapical closure by the formation of an apical stop(calcium hydroxide is generally used) against which apermanent root canal filling can subsequently beinserted; and (5) placing a biologically acceptablesubstance in the apical portion of the root canal(dentinai chips or tricalcium phosphate has been used )thus forming an apical barrier; which is followed byfilling ofthe root canal with gutta-percha sealer.
Techniques that induce apical closure have beendeveloped to provide a calcule barrier at the end oftheroot, to act as a stop against which a gutta-percha rootfilling can be condensed. The most frequently usedprocedure appears tobeapexification with CaiOH),."Although calcium hydroxide possesses many proper-ties that infiuence induction of apical closure, apexifi-cation has also been successful without the use of anymedicament in some cases.- Experimental endodonticwork carried out by Torneck and Smith'" on partiallydeveloped incisor teeth in young monkeys showedhistologically the process of root development thatoccurred after pulpotomies and pulpectomies. Theaccess cavities were sealed with amalgam, but rootfillings were not inserted. The conclusion reached wasthat root formation may continue after such treatmentwithout remedial therapy, but growth is retarded^andirregular.'̂ According to Morse and coworkers,- thecommon aspects of all apexification procedures aredebridement. cleaning, and reduction of the root canalspace with a material, thus leading to a favorableperiapicai environment.
The two cases presented are examples of closure of
immature root apices subsequent to treatment withcalcium hydroxide mixed with sterile water. Thismaterial was left in the root canal in two patients untiladequate apical closure occurred through continuedapical development. The process of apical develop-ment continued to its potential after routine endodon-tic therapy with gutta-percha and cndamethasone. Atthe end ofthe treatment, the apices were closed anddid not allow excess gutta-percha to be expressedperiapically. In these two patients, no periapicalpathosis or root résorption was recorded.
Cvek'' suggested that the effect ofthis material mightbe explained by the assumption that calcium hydroxideacts as a long-lasting antibacterial agenl. He alsoindicated that once the infection is eliminated andperiapical tissues reorganize, it is possible for calculedevelopment to take place.-"'
The mechanism of action of this paste may bepartially dependent on its high pH; thus, one ofthemost important reasons for mixing calcium hydroxidewith a physiologic vehicle such as sterile water is itsexpected alkaline pH.
Conclusion
The literature is replete with articles offering additionalmodes of therapy for a nonvital tooth with an openapex. Two case reports have shown thai the techniqueof apical closure with calcium hydroxide-sterile waterpaste proved highly successful. Results related closelyto data obtained in the past. This method is easy tocarry out and is well accepted by patients. For thoseclinical situations in which apexification or barrierformation is necessary, calcium hydroxide-sterile waterpaste might be a good choice, especially in childrenwho are anxious about surgical procedures.
References
1. Mackie IC, Bentley EM. Wonhingtnn HV. The closure of openapices in non-vital inimaUire ineisor teeth Br Dent J 1988; 165:169-173.
2. Morse DR, OXarnie J, Yesilsoy C. Apexificalion: Review of Iheliterature. Quintessence lnt 1990:21:589-598.
3. Barker BCW Maync JR. Some unubual cases of apexifieationsubsequent to trauma. Oral Surg Oral Med Oral Pathol 1975;39;I44-I5O.
4. Anthony DR, GordonTM, del RIO CE. The effect of Iliree vehicleson the pH of calcium hydro.^ide. Oral Surg Oral Med Oral Patholl982;54;56O-565.
5. Klein SH. Levy BA. H i sto logic evaluation of indtieed apical closureof !i human pulptess tooth Oral Surg Oral Med Oral Palhol1974:38:954-959.
»,3a. Number 10/1997 685

Erdogan
6. Cvek M, Treatment of non-vital permanent lntlsor^ with calciumhydroxide. I, Follow-up of periapical repair and apical closure ofimmature roots. Oiioiitol Rev 1972;23:27-44.
7. Frank AL. Calcium hydroxide: The ultimate medicament? Dent ClinNorth Am 1979-:3691-703.
8. Maekie It". Worthington HV. Hill FJ. A follow-up study of Incisiirteeth which had been treated l>y apical closure and root Tilling. BrDent J l993il75:99-IOI.
9. Duell RC. Conservative endodontic treatment of the open ape\ inthree dimensions. Dunt Clin North Am 1973:17:125-1.'4.
1(1, Webber RT Ape\ogenesis versus apevificiition. Dent Clin NorthAm I984;2K 669-697.
11. Frank AL, Therapy for the divergent puiplcss tooth by continuedapical formation. J Am Dent Assoc l966;72rS7-93.
12. Hermann BW. Dentinobliteration der Wurielkanäle naeh derBehandlung mil Kaicium. Zaiinärzti Rundschau 193O;59:88S.
13. Teuscher GW, Zander HA. A preliminary report on pulpotomy.Northwestern Univ 0 Bull 1938:39:4.
14. Zander HA. Reaction of the dental pulp to calcium hydroxide JDent Res 19.19: IS:373.
15. Andreaien JO. Traumatic In.iurics of the Teeth. Copenhagen:Munksgaard. 19Sl:.15i..
16. Ghose LJ. Baghdady VS, Hikmat BYM. ApesiTieation of immatureapices of pulpless permanent anterior teeth with calcium hydroxide.J Endod I9K7;I3 2S5-290.
17. Yates JA, Barrier formation time in non-vital teeth with open apiees,Int EndodJ l98Si21:3l3-319.
IS. Kleier DJ, Barr ES. A study of endodontically apcsificd teetli.Endod Dent Traumalol 1991:7:112-117.
19. Steiner JC. Dow PR, Cathey CM. Inducing root and ciosure ofnon-vital permanent teeth. J Dent (h i ld 1968:35:47.
20. Steiner JC, Van Hassel HJ. Experimental root apesiTication inprimates. Oral Surg I97I;31:4O9.
21. Boyle FP. Kronfeld's H i sto pathology of the Teeth and TheirSurrounding Struetures. Philadelphia: Lea & Ferbiger, 1955:339.
22. CrabbHSM The basis of root-canal therapy. Dent Pract Dent ResI965:I5:.197
23. Heithersay GS. Stimulation of root formation in incompletelydeveloped pulpless teeth. Orai Surg Oral Med Oral Patho! I97t):29:620.
;4 I rank A Endodontic therapy for the wide-open i.psx. Dent Clin
North Am 19h7:11;(i75-7OU,
25. Seltzer S. E n dodo n to I (lu y-Bio logic Considerations in EndodontitProcedures. New York: McGrjw-Hill, 1971 :Z-4.
;(.. Tronstad L, Andreasen JO. Hasselgren C. et al. pH changes indental tissues after root canal Tilling with calcium hydrcnide. JEndoil I98I;7:I7-21,
27. Abiko YStudiesoncüIcium-stimulatedadenosinetriphosphataseinthe albino rabbit dental pulp: Its subcellular distribution andproperties.J Dunt Res 1977:56.1558-I56S.
28. JüveletJ,Torabinejad M, Bakland LK.. Comparison pH levels for theinduction of apical barriers in immature leeth of monkeys. J Endodl985;il:375-378,
29 Vaes G. Lysosomes and cellular physiology of bone résorption. In:Dingies J[, Fell HE (cds). Lysosomes in Biology and Pathology,Amsterdam' North Holland, 1969:216-353
30. Bourne HG, Phosphatase and ealcification In. Bourne HG (edl.The Biochemistry and Physiology of Bone, New York: AcademicPress, 1972:79-120,
31. Binnie WH, Rowe AHR. A hiitological study of the periapicaltissues of ineompleleiy formed pulplcss teeth Tilled with calciumhydroxide. J Dent Res 197.!:5:r I i 10- 1116.
32. Wechsler SM.FishelbergG.Opdevaluable and etfeetive clinical proc
,.'3, Holland R,DüSouzaLD,TagliavinniRL. etal A histological studyof the effect of calcitim hydroxide in the treatment of pulpless teeth ofdogs. J Br Endod Soc I979J2:15-23.
.'4 StewartGG, Gautier RF Reduced inflaminatory root canal medica-tion. Oral Surg Oral Med Oral Pathol I962;15 715-7:0.
35. Torneck CD, Smith J. Biological effects of endodnntic procedureson developing incisor teeth. Oral Surg Oral Med Oral Pathol
ck WR, et al, ApesiTieation: Aire. Gen Dent 1978:26:40-43.
36. Cvek M. C?linical procedures promoting apical ciosure and arrest ofexternal root résorption in non-vital permanent incisors, InrGrossman L (ed). Transactions of the Fifth International Con-ference on Endodontics. Philadelphia: üniversit> of PennsylvaniaPress, 1973:30-44, •
686 Quintessence Iniernational Volume 28, Number 10/1997