Embed Size (px)
Citation preview

The Synapse
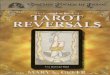
Neurons generate action potentials which consist of brief reversals in the polarity (electrical state) of the axon (transmitting region) of the cell. These action potentials cause the release of a chemical messenger from a storage vesicle in the axon terminal. The chemical messenger (called a neurotransmitter) travels across a synapse to bind to a postsynaptic receptor protein. The act of binding to the receptor protein sets in motion a series of events which eventually brings about a change in the electrical state of the postsynaptic cell. Some neurotransmitter-receptor bindings excite the cell and others inhibit it. At any given moment a neuron receives thousands of these messages and integrates this input to bring about only one of two possible outcomes - the neuron stays in a resting state or it generates an action potential to communicate with another neuron.

The Synapse1.....Postsynaptic Neuron2.....Presynaptic Neuron3.....Vesicle with Neurotransmitter (NT)
Molecules4.....Mitochondrion (for energy production
from glucose)5.....Synaptic Cleft6.....Neurotransmitter (NT) Molecules7.....Postsynaptic Membrane (with NT
receptors)Neurotransmitters are released from storage vesicles and diffuse across the synaptic cleft to bind to a specific receptor site on the postsynaptic neuron. The neurotransmitter then activates (excites or inhibits) the next neuron and is then reuptaken into the sending neuron or destroyed either in the cleft or in the presynaptic neuron. It is at the synapse that most drugs or chemicals work to alter the brain and thus the mental state of the person.

The Synapse
Presynaptic Axon
Postsynaptic SpinePostsynaptic
Density
Active Zone
Astrocyte
Coated Vesicle
Dense Core Vesicle
Double-Walled Vesicle
Endoplasmic Reticulum
Mitochondrion
Punctum Adhaerens
Synaptic Cleft
Synaptic Vesicles

The Synapse
Dendritic Spine

Active Zones and the Postsynaptic Density (PSD)
Active Zone
Synaptic Cleft

Astrocytes

Vesicles
Coated vesicles are pieces of membrane retrieved from the
plasmalemma throughendocytosis.
Synaptic Vesicles
Coated Vesicles

Neurotransmitter Release:A nerve impulse that reaches a presynaptic ending produces a transient depolarization of the presynaptic membrane, which activates voltage-sensitive calcium channels. Calcium ions flow across the membrane. Increased calcium levels cause vesicles that store the chemical transmitters to move toward the synaptic cleft (the space between pre- and postsynaptic cells). The vesicles fuse with the inner surface of this region, and the transmitters are transported across the membrane and released into the cleft region. The transmitter molecules diffuse across the cleft. Some bind to receptor molecules on the postsynaptic membrane, changing the permeability of the membrane.

Presynaptic Receptors & the control of NT release.

Presynaptic Receptors & the control of NT release.

Vesicle release

Vesicle release

The EPSP
Squid Mouse

Calcium Channel Blockers & the CNS: L-type
Dihydropyridines: Blockers of L-type VSCCs
L-type VSCCs found on Neurons, but also on vascular smooth muscle & other muscle cells throughout the body.

Calcium Channel Blockers & the CNS: N-type
Omega-conotoxin MVIIa (SNX-111): A selective blocker for N-type calcium channels from the cone snail Conus magus
Conus Geographicus

Conus Geographicus

Na Channel Blocker: TTX
Blocks voltage-gated sodium channels
Commonly used in labs around the world
Fugu Poisoning: Estimates as high as 200 cases per year have been reported with mortality approaching 50%

Neurotransmitters
A neurotransmitter is a chemical compound, secreted by a neuron, that either stimulates or inhibits the flow of an impulse between neurons. Shortly after a neurotransmitter completes its action, it is taken up or brokendown by an enzyme. Acetylcholine , norepinephrine are examples of stimulatory neurotransmitters; gamma aminobutyric acid is an example of an inhibitor. Two other neurotransmitters, sertonin and dopamine, are stimulatory in some parts of the brain but inhibitory in others. Acetylcholine also stimulates muscle contraction wherevera neuron connects with a muscle.

NeurotransmittersDetailed Notes
Provided

Catecholamines: Synthesis

Catecholamines: Metabolism

Catecholamines: Projections

Acetylcholine

Acetylcholine

Parkinson’s Disease
Described > 180 Yrs ago by James Parkinson
Affects > 1 million people in North America
Prevalence increases with increasing age
Shortens life & increases disability

Parkinson’s Disease
Characterized by the progressive death of selected neurons
• Dopaminergic neurons of the pars compacta of the substantia nigra•Selected aminergic brainstem nuclei (catecholaminergic and serotoninergic)
• Cholinergic nucleus basalis of Meynert
Results in a loss of dopamine in the striatum

Parkinson’s Disease:
Characterized by
T remor
R igidity
A kinesia
P ostural Instability
Which are due to an imbalance in
the excitatory and inhibitory circuitry
of the basal ganglia –
Structures responsible for motor control.

Parkinson’s Disease:
Treated with L-dopa
(metabolized in the CNS to dopamine)

Parkinson’s Disease:
Treated surgically by lesioning the
globus pallidus
(pallidotomy) or
subthalamic nucleus

GABA Receptors
There are two basic subtypes, GABA-a and GABA-b. GABA-a is the most prevalent in the mammalian brain. The GABA-a receptor is similar to acetylcholine receptor in that it is related to an ion channel. In the case of GABA-a it is the chloride ionophore. Binding of GABA to this receptor increases the permeability to chloride ion which causes a hyperpolarization of the neuron or inhibition. The GABA-a receptor has four basic subunits, 2-alpha and 2 beta peptides which surround a chloride channel.
There are three basic binding sites on this complex. The first is the GABA site. The second is a benzodiazepine site. The third is in the channel and is essentially a barbiturate site.

Glutamate receptors
Responsible for mediating Rapid Synaptic Excitation in the CNS

Back to the patient:
Enhance GABAA
+
Block EAA Receptors
=
Anesthesia

Evoked Potentials Monitoring

Evoked Potentials

Somatosensory Evoked Potentials
The SSEP assesses the pathways from the nerves in the arms or legs, through the spinal cord to the brain. Electrodes are placed on the scalp. A small electrical current is applied to the skin near nerves on your arms or legs. The evoked potential is measured from the scapl. This test can also be used to monitor coma patients, and test hearing in infants and others whose hearing cannot be tested in standard ways.

Succinylcholine
Succinylcholine chloride is an ultra short-acting, depolarizing-type, skeletal muscle relaxant for intravenous administration
It is a depolarizing skeletal muscle relaxant. It competes with acetylcholine for the cholinergic receptors of the motor endplate, and, like acetylcholine, it combines with these receptors to produce depolarization.
Succinylcholine, however, causes a more prolonged depolarization than acetylcholine because it has a high affinity for thecholinergic receptor and a strong resistance to acetylcholinesterase. Depolarization results in fasciculation of the skeletal muscles followed by muscle paralysis. Neuromuscular transmission is inhibited as long as an adequate concentration of succinylcholine remains at the receptor site.

Pancuronium
Pancuronium bromide is a nondepolarizing neuromuscular blocking agent. It is similar to, but five times as potent as, tubocurarine. Pancuronium is used to induce relaxation of the skeletal muscles during surgery and to facilitate pulmonary compliance during mechanical ventilation
Nondepolarizing agents produce skeletal muscle paralysis by blockade at the myoneural junction. Pancuronium competes with acetylcholine for cholinergic receptor sites. Unlike depolarizing agents, pancuronium has little agonist activity, having no depolarizing effect at the motor endplate. Skeletal muscle relaxation proceeds in predictable order, starting with muscles associated with fine movements, e.g., eyes, face, and neck. These are followed by muscles of the limbs, chest, and abdomen and, finally, the diaphragm. Larger doses increase the risk of respiratory depression due to relaxation of the intercostal muscles and diaphragm. Muscle tone returns in the reverse order.

How to Gauge Depth of Neuromuscular Relaxation:

One last look…