Embed Size (px)
Citation preview

Food Quality and Preference 39 (2015) 62–72
Contents lists available at ScienceDirect
Food Quality and Preference
journal homepage: www.elsevier .com/locate / foodqual
The spirit is willing, but the flesh is weak: The moderating effectof implicit associations on healthy eating behaviors
http://dx.doi.org/10.1016/j.foodqual.2014.06.0140950-3293/� 2014 Elsevier Ltd. All rights reserved.
⇑ Corresponding author. Tel.: +49 431 880 3614; fax: +49 431 880 3349.E-mail addresses: [email protected] (R. Mai), stefan.hoffmann@bwl.
uni-kiel.de (S. Hoffmann), [email protected] (K. Hoppert), [email protected] (P. Schwarz), [email protected] (H. Rohm).
1 Tel.: +49 431 880 4737; fax: +49 431 880 3349.2 Tel.: +49 351 463 32754; fax: +49 351 463 37761.3 Tel.: +49 351 458 2715; fax: +49 351 458 7319.4 Tel.: +49 351 463 32420; fax: +49 351 463 37761.
Robert Mai a,⇑, Stefan Hoffmann a,1, Karin Hoppert b,2, Peter Schwarz c,3, Harald Rohm b,4
a Christian-Albrecht-University of Kiel, Faculty of Business, Economics and Social Sciences, Department of Marketing, 24098 Kiel, Germanyb Dresden University of Technology, Institute of Food Technology and Bioprocess Engineering, 01062 Dresden, Germanyc Department of Internal Medicine III, Clinic for Endocrinology, Diabetes and Metabolism, Dresden University of Technology, 01069 Dresden, Germany
a r t i c l e i n f o
Article history:Received 9 January 2014Received in revised form 22 June 2014Accepted 24 June 2014Available online 2 July 2014
Keywords:HealthFoodNutrition self-efficacyImplicit Association TestMediated moderation
a b s t r a c t
This paper examines how implicit processes shape consumer’s food decision making. A series of threeempirical studies combines questionnaire data with the Implicit Association Test to demonstrate thatthe effect of nutrition self-efficacy on behavioral intentions and eating behavior is moderated by foodassociations that are activated automatically and unconsciously. The Main Study provides evidence thatconsumers with a low ability to adopt a healthy diet behave according to their self-efficacy if implicitassociations are negatively connoted (e.g., ‘‘healthy food products are less tasty’’). A mediated moderationmodel shows that the interaction effect exerts its influence via intentions to adopt a healthy diet. Repli-cation Study A confirms that this interaction effect even shapes the consumption patterns of at-risk con-sumers who have received nutritional counseling. Study B confirms the moderating role of implicitassociations in a different setting and for different implicit associations. The article reveals that solelyincreasing consumer’s self-efficacy will not result in substantial changes towards a more healthy diet.By addressing implicit processes, food producers and policy makers can improve the effectiveness of theirefforts to induce changes in consumers’ food consumption patterns.
� 2014 Elsevier Ltd. All rights reserved.
Introduction
Changing food consumption is considered the key to solvemany of the current diet-related health problems, e.g., diabetesmellitus type 2, coronary heart disease, and overeating (Haws &Winterich, 2013; Marteau, Hollands, & Fletcher, 2012). Policy mak-ers have launched numerous educational campaigns, e.g., ‘‘Five ADay campaign’’, (Consumers Union, 2005) and initiated severalchanges in the food consumption environments, e.g., school lunchprograms (Grainger, Senauer, & Runge, 2007) and serving sizes(Grynbaum, 2013). While many consumers now agree that healthynutrition is crucial for their well-being, food choices often do notmatch the rise in problem awareness and a substantial reverse inthe obesity epidemic has not been achieved so far (Frieden,
Dietz, & Collins, 2010; Swinburn et al., 2011). Hence, the crucialquestion is how the health concerns can be translated into action.
Previous research emphasized the role of cognitive abilities,such as the consumer’s belief in his/her ability to achieve andmaintain a healthy diet; referred to as nutrition-related self-effi-cacy (Anderson, Winett, Wojcik, Winett, & Bowden, 2001; Mai &Hoffmann, 2012; Rimal, 2000). Yet, purely cognitive explanationsfall short of expectations, and there is still an enormous gapbetween the increased health concern and self-efficacy of consum-ers and their actual food consumption choices. There is a growingconsensus among scholars that rational cognitive processes in fooddecisions cannot sufficiently explain why some consumers act con-trary to their convictions (Kidwell, Hardesty, & Childers, 2008;Köster, 2009; Mai, Zahn, Hoppert, Hoffmann, & Rohm, 2014;Marteau et al., 2012; Yang et al., 2012). Researchers thus need toshift the focus from consumer’s motivation and ability, to factorswhich lie outside rational decision making. This research claimsthat unconscious and automatically activated processes (referredto as implicit processes) shape cognitive reasoning when makinga food decision or when consuming food.
Recent findings provide indications that implicit and explicitprocesses are not necessarily in line, and implicit processes domi-nate consumer’s food preferences (Raghunathan, Walker Naylor, &

R. Mai et al. / Food Quality and Preference 39 (2015) 62–72 63
Hoyer, 2006). The interplay between both processes may helpexplain why some consumers eat in accordance to their healthgoals and why others do not. This article reports three empiricalinvestigations that combine questionnaire data with the ImplicitAssociation Test (IAT; Greenwald, Nosek, & Banaji, 2003) to analyzethe interaction effects of implicit and explicit processes. The MainStudy investigates how implicit food associations shape the influ-ence of nutrition self-efficacy on intentions to change nutritionhabits and food consumption patterns (Fig. 1). This study empiri-cally tests a mediated moderation model that demonstrates howthe catalyzing effects of implicit associations work along theprocess from self-efficacy via intentions to behavior. Pivotalsocial-cognitive predictors of health behavior and several controlvariables are included to ensure the stability of the model.
Two conceptual replications support the robustness of themodel. Replication Study A examines the interaction effect for at-risk consumers who have undergone medical treatment andnutritional counseling. Replication Study B finally confirms theinterplay of self-efficacy and implicit associations for specific foodproducts, namely fat- and sugar-reduced foods. In sum, this paperoutlines a highly relevant interaction effect that is stable across dif-ferent settings. Implications are developed for how policy makerscan foster healthy food consumption by addressing implicit atti-tudes to overcome the mind-behavior gap.
Theoretical background
Healthy consumer behavior
Research has examined a wide range of food constituents andaspects of labeling (e.g., Balcombe, Fraser, & Falco, 2010; Hoegg &Alba, 2007; Howlett, Burton, Bates, & Huggins, 2009), as well as awhole host of consumer characteristics that guide food consump-tion (e.g., Mai & Hoffmann, 2012; Roberts & Pettigrew, 2013).Despite the vast body of literature, a review by Block et al.(2011) leads to the conclusion that knowledge on how to effec-tively induce changes in eating behaviors is scarce. There is ampleevidence that the actual behavior of many consumers does notnecessarily live up to their intentions (Webb & Sheeran, 2006).Even though some consumers are motivated and capable of adopt-ing a healthy diet, they do not behave in the intended way. Otherseat a healthy diet, although they do not intend to do so. Somerecent approaches suggest that this gap may be overcome by nudg-ing consumers and designing appropriate choice architectures(Marteau et al., 2012; van Ittersum & Wansink, 2012). While suchattempts are rather context-based, knowledge on sustainable
Nutrition self-efficacy
Implicit food associations
Intention to a healthy
Socio-demographics/psychographics
Social-cognitive predictors of health behavior change
- Outcome expectancies- Risk perception
Control variables
MediatedModeration
- Sex- Hunger- Diet- Education
- Positive feelings- Impulsiveness- Household size
Fig. 1. Concept
individual-based mechanisms of behavioral change is urgentlyneeded. In a longitudinal intervention-based field study, for exam-ple, Patrick and Hagtvedt (2012) reveal that verbal aspects can behelpful in self-regulation. It is of pivotal importance to unravelfurther factors that help empower the consumer in goal pursuit.
Nutrition self-efficacy
Self-efficacy describes ‘‘the belief in one’s competence to copewith a broad range of stressful or challenging demands’’(Luszczynska, Scholz, & Schwarzer, 2005). According to Social Cog-nitive Theory (Bandura, 1977, 1986), a person is more likely toadopt a specific behavior, the higher his/her degree of self-efficacy.The relevance of self-efficacy has also been confirmed in the field ofhealth behavior and health promotion (cf. Baranowski et al., 2003;Holden, 1991; Judge, Jackson, Shaw, Scott, & Rich, 2007). This arti-cle considers self-efficacy as a domain-specific construct because itis reasonable to assume that its predictive power is greater thanthat of a general conceptualization (Kidwell et al., 2008;Lastovicka & Joachimsthaler, 1988). The research group aroundRenner and Schwarzer (e.g., Renner, Knoll, & Schwarzer, 2000;Renner & Schwarzer, 2005) has established the construct of nutri-tion self-efficacy that captures a person’s beliefs to cope with theobstacles that are linked to a healthy nutrition. Prior research hasdemonstrated that nutrition self-efficacy influences certain foodpatterns, such as weight control, fruit and vegetable consumption,or fat and sugar intake (e.g., Anderson, Winett, & Wojcik, 2000; Mai& Hoffmann, 2012; Schwarzer & Renner, 2000).
Implicit food associations
Rational consumer theories and explicitly measured conceptssuch as self-efficacy are unable to fully explain food consumptionpatterns because the mechanisms guiding food choices are oftenoutside the consumer’s awareness and/or control (Köster, 2009;Morewedge, Huh, & Vosgerau, 2010). Consumers choose food prod-ucts, for example, on the basis of eating habits, gut feelings and othernon-conscious factors. Even emotions were shown to play a role infood choice (Kidwell et al., 2008). The literature distinguishes twobasic cognitive modes of decision making and choice under uncer-tainty (e.g., Kahneman, 2003; Stanovich & West, 2000; Yang et al.,2012). Intuitions (System 1) tend to operate quickly, automatically,and effortlessly. They are not available to introspection. Intuitionsare implicit, often emotionally charged, and usually governed byhabits. Consequently, the individual can control and modify themonly with great difficulty (Kahneman, 2003, p.698). Reasoning
Food consumption
Main Study: Menu choiceReplication Study A: Adherence to nutrition
guidelinesReplication Study B: Low-fat/sugar product
consumption
adopt diet
ual model.

64 R. Mai et al. / Food Quality and Preference 39 (2015) 62–72
(System 2), on the other hand, is slow, controlled, effortful, andrule-governed as it reflects more in-depth logic.
Food choices very often operate on the unconscious level (e.g.,Cervellon, Dubé, & Knäuper, 2007; Marteau et al., 2012;Raghunathan et al., 2006), unless they are overridden or modifiedby the more deliberate mode of mental operation. Even thougheveryday eating and drinking are actions that are open to aware-ness, it seems plausible that the control over eating habits is notnecessarily explicit. Some researchers even claim that food choicesare mostly unconsciously driven, often guided by heuristics andnot carefully scrutinized (Mai et al., 2014; Yang et al., 2012). Withrespect to ‘‘eating and drinking, intuitive thinking is rule ratherthan exception’’ (Köster, 2009, p.76).
Empirical studies revealed that implicit and explicit associa-tions diverge significantly (Czyzewska & Graham, 2008; Roefs &Jansen, 2002) and may even conflict (Hoefling & Strack, 2008;Ratliff, Swinkels, Klerx, & Nosek, 2012). In the context of food deci-sion making, many consumers non-consciously assess the taste ofhealthy items as negative. This implicit link between unhealthyand tasty is so pervasive that even the behaviors of those consum-ers who show no explicit belief in this unhealthy = tasty intuitionare affected (Raghunathan et al., 2006).
Hypotheses and flow of studies
This paper aims to answer the fundamental question of whysome consumers translate their abilities to achieve a healthy dietinto practice while others do not. Building on the dichotomy ofcognitive modes, we expect that favorable implicit associationsbuild the basis on which explicit processes guide healthy foodchoices. Studies have shown that implicit taste evaluations maybe an important barrier to healthy eating (Raghunathan et al.,2006). We suggest that strong nutrition self-efficacy only trans-lates into intentions to eat healthy if the intuitive belief thathealthy foods lack in taste is no (or only a small) implicit barrier.
Hypothesis H1. The influence of nutrition self-efficacy on theintention to adopt a healthy diet is moderated by the implicit linkbetween unhealthy food and taste: The more favorable implicittaste associations, the more likely nutrition self-efficacy influencesintentions to adopt a healthy diet.
Following the rationale underlying H1, a consumer’s intentionto adopt a healthy diet may not necessarily result in an actuallyhealthier diet. If implicit associations with healthy food are unfa-vorable, optimistic intentions have no substantial and lasting effect(e.g., New Year’s resolution to lead a healthier lifestyle). We there-fore suggest that intentions exert their influence on eating behav-iors only if there are no implicit barriers.
Hypothesis H2. The influence of the intention to adopt a healthydiet is moderated by the implicit link between unhealthy food andtaste: The more favorable the implicit taste associations, the morelikely consumers translate their intentions to adopt a healthy dietinto healthier food choices.
Taken together, this framework suggests a mediated modera-tion (Muller, Judd, & Yzerbyt, 2005): The joint effect of self-efficacyand implicit associations on intentions is passed on to food con-sumption patterns. If the interaction effect between nutritionself-efficacy and implicit associations has a strong impact, it hasto be reflected in several related domains of healthy food con-sumption, such as the adherence to nutrition guidelines or the con-sumption of fat- and sugar-reduced products.
Hypothesis 3a,b. The interaction effect of nutrition self-efficacyand implicit associations on intentions to eat healthy are reflectedin several aspects of food consumption, such as (a) eating
behaviors in accordance to nutrition guidelines or (b) preferencesfor fat- and sugar-reduced products.
This article reports three empirical studies to answer ourhypotheses. The Main Study tests the proposed mediated modera-tion model that explains how implicit associations shape the pro-cess from self-efficacy via intentions (H1) to behavior (H2).Several control variables are included to ensure the stability ofthe model. Since improvements in eating behaviors have the great-est economic and social effects over the lifespan, the Main Studyfocuses on young consumers. While young consumers may be lessconcerned with adopting a healthy diet, Replication Study A exam-ines if the moderating role of implicit processes is evident even forconsumers with a high risk of type II diabetes (and who havereceived nutritional counseling). Besides their intentions to adopta healthy diet, we examine whether the at-risk consumers’ eatingis in accordance with nutrition guidelines (H3a). To rule out alter-native explanations, the study contrasts implicit and explicit mea-sures of taste. Replication Study B then aims to corroborate thefindings by focusing on fat- and sugar-reduced food products (H3b).
Main Study
Objective
The Main Study tests the basic premise that implicit food asso-ciations shape the influence of self-efficacy on the intention toadopt a healthy diet and, subsequently, food consumption pat-terns. This study includes several control variables to ensure thestability of the mediated moderation model.
Design
Owing to the distinct nature of the focal constructs (implicit vs.explicit) and to avoid common method variance, a multi-methodapproach was used employing highly diverse instruments, suchas reaction time tests and self-reporting scales. Implicit associa-tions cannot be assessed with self-reporting scales because sub-jects are unable to verbalize such cognitions. Instead, thisresearch applied the Implicit Association Test (IAT; Greenwaldet al., 2003; Gregg & Klymowsky, 2013; for a review see Dimofte,2010) as implemented in the application Inquisit by MillisecondSoftware. This instrument measures implicit attitudes on the basisof a multiple-step procedure of computer-based reaction-timetests. The present study measured the strength of the participant’simplicit taste associations with (un)healthy foods (adopting theprocedure by Raghunathan et al., 2006). In the course of the IAT,target concepts (e.g., pictures of healthy or unhealthy food) or eval-uative attributes (e.g., tasty or not tasty) are presented on a com-puter screen (see Appendix A for target concepts and evaluativeattributes). We developed the pictures of the target concepts in apretest. From a large set of pictures of various food items, a groupof five interdisciplinary researchers (from marketing, psychology,and nutrition sciences) chose six items that are rather healthyand six items that are generally considered unhealthy when con-sumed heavily. To minimize bias of the stimulus materials, theitems varied systematically across different food categories (e.g.,beverages: mineral water vs. cola; snacks: dried banana chips vs.potato chips). In addition, the researchers made sure that the pic-tures are similar regarding size, visual complexity and salience(Rothermund & Wentura, 2004). As evaluative attributes for the‘tasty’ and ‘not tasty’ categories, we adapted a word list that wasused in prior research (Raghunathan et al., 2006).
Participants are asked to sort these pictures or words rapidlyinto categories on the left side (e.g., ‘‘healthy food’’ and ‘‘tasty’’)or the right side of the screen (e.g., ‘‘unhealthy food’’ and ‘‘not

R. Mai et al. / Food Quality and Preference 39 (2015) 62–72 65
tasty’’). After several trials (Table 1), the positions of the target con-cepts are interchanged (e.g., left side: ‘‘unhealthy food’’ and‘‘tasty’’). The IAT is based on the assumption that differences inreaction times between both task conditions reveal easier pairings(indicated by faster responses), which can be interpreted as twocategories that are more closely associated than more difficultpairings (indicated by slower responses). For example, the moretime the participants take to pair pictures of unhealthy food prod-ucts with tastiness in comparison to pictures of healthy food prod-ucts, the weaker they associate ‘‘unhealthy food’’ and ‘‘tasty’’. Thisresearch applied the improved scoring algorithm suggested byGreenwald et al. (2003) to assess the IAT D effect.
Different self-reporting scales that are widely used in consumerresearch were applied to measure the explicit constructs (Appen-dix B). Nutrition self-efficacy was operationalized by a four-itemseven-point Likert scale (M = 4.37, SD = .77, Cronbach’s a = .70)taken from Schwarzer and Renner (2000) and Renner et al.(2008) who originally distinguished the facets of pre-action andpost-intention. Since this paper examines whether individualstranslate goals into action, only action-related nutrition self-effi-cacy is measured. Consumer’s intention to adopt a healthy dietwas measured with a four-item Likert scale (M = 4.68, SD = 1.03,a = .78) from Schwarzer and Renner (2000). To assess the subjects’food consumption pattern, this research assessed their choicesfrom menus. The subjects were asked to select one of three proto-typical menus that reflect their eating patterns best. One of thethree menu options is healthier compared to the other two options.The participants were asked to pick one prototypical menu forbreakfast (light menu: e.g., cereals, fruits; sweet menu: e.g., jam,honey, croissants; savory menu: cheese, eggs or sausages), onefor lunch (light menu: e.g., salad, soup or chicken; sweet menu:e.g., rice pudding or pancake; savory menu: steak, meat and sidedish) and one for supper (light menu: e.g., salad, vegetables, crispor whole-grain bread; sweet menu: e.g., pancake, chocolate breador fruit yoghurt; savory menu: pizza, sausages or cold meat). Thechoice of the light menu option is coded with 1 (0 = other choice).The three choices were combined to an index (M = 1.15, SD = .73).
Several control variables were added. From Schwarzer andRenner (2000), we took outcome expectancies which refer toexpected benefits of adopting a healthy diet (three-item seven-point Likert scale, M = 5.05, SD = 1.33, a = .73), and risk perceptionwhich refers to perceived vulnerability of possible negative conse-quences (three-item seven-point semantic differential scale withthe anchors ‘‘much below/above average’’, M = 3.11, SD = 1.29,a = .79). These two factors are widely discussed and included inestablished models of health behavior and behavioral change,such as the Health Action Process Approach (Schwarzer &Renner, 2000). The latter has successfully been applied in thecontext of nutrition behavior. In addition, we measured impul-siveness (three-item seven-point Likert scale, M = 4.91, SD = 1.06,a = .70), positive mood (four-item five-point Likert scale,M = 4.35, SD = .48, a = .67), and hunger (one-item five-point Likertscale, M = 3.02, SD = 1.16). The questionnaire also checkedwhether the participants were on a diet using a 0/1-question(8.9% on a diet).
Table 1Procedure of the IAT.
Block Trials Function Tasks main
1 20 Practice Healthy vs2 20 Practice Tasty vs. n3 20 Critical block for analysis Healthy + t4 40 Critical block for analysis Healthy + t5 20 Practice Unhealthy6 20 Critical block for analysis Unhealthy7 40 Critical block for analysis Unhealthy
The internal consistency of all reflectively measured multi-itemscales is high (see Appendix B). A confirmatory factor analysis(maximum likelihood estimation; AMOS 21.0) including themulti-item scales confirms the measurement models (v2/d.f. = 1.30, p 6 .01; CFI = .90, IFI = .91, RMSEA = .058). The Fornelland Larcker (1981) test provides evidence for discriminant validity.That is, the maximum of the squared correlation among the scalesis lower than the average variance extracted.
We applied several measures before (‘ex ante’) and after thestudy was run (‘ex post’) to avoid common method variance(Podsakoff, MacKenzie, Lee, & Podsakoff, 2003). Ex ante, we useddifferent instruments (reaction time measurement and question-naire) to methodologically separate the measurements. Weemployed different scaling formats for the survey data (five- andseven-point Likert scales as well as semantic differential scalesand dichotomous questions). We added some conceptually unre-lated items to psychologically and temporally separate the mea-surements. As an ex post means of control, the single-factor testwas run. An exploratory factor analysis including all indicatorsreveals that one general factor explains 17.1% of the variance only.By contrast, many factors explain 70.8% of the variance. FollowingLindell and Whitney (2001), the questionnaire also included anunrelated marker variable (‘‘I usually buy branded products.’’).Since there are no statistically significant relationships betweenthis marker variable and the focal scales (|r| 6 .184, p > .05), com-mon method variance did not distort the results.
The study was part of a larger research project which examinedimplicit product-based and personality-based obstacles to healthyfood consumption (another part unrelated to this study was pub-lished in Hoppert, Mai, Zahn, Hoffmann, & Rohm, 2012). Respon-dents were recruited via notice boards and posts in newspapers.In all, 91 subjects participated in the IAT and filled in the briefquestionnaire in a laboratory at the authors’ university. The sub-jects received 10€ for their participation. On average, the subjectswere 24.15 years old (SD = 3.8), 64% were female and they hadan average Body Mass Index (BMI) of 23.19 (SD = 3.52).
Results
The analysis of implicit taste evaluations reveals that partici-pants perceive unhealthy food products as less tasty than healthyproducts. The subjects paired unhealthy foods with not tasty(and healthy foods with tasty) much more easily (820.84 ms) thanhealthy foods with not tasty (and unhealthy foods with tasty)(1,478.51 ms). The IAT effect (MD-schore = 1.08, SD = .32) is highlysignificant (t = 32.451, p < .001).
Regression analyses (one-tailed) provide empirical evidence thatimplicit taste evaluations moderate the influence of nutrition self-efficacy on food consumption patterns. While nutrition self-efficacyexerts a main effect on the subjects intention to adopt a healthy diet(b = .23, t = 2.256, p < .05), there is no main effect of implicit tasteevaluations (p > .05). Yet, implicit associations strongly moderatethe influence of self-efficacy on intentions (b = �.30, t = �2.960,p < .01). The interplay between self-efficacy and implicit associationaccounts for an increase in explained variance of 8.8%. This change in
study and Replication Study A Tasks Replication Study B
. unhealthy products Diet vs. regular food productsot tasty Positive vs. negativeasty vs. unhealthy + not tasty Diet + positive vs. regular + negativeasty vs. unhealthy + not tasty Diet + positive vs. regular + negativevs. healthy products Regular vs. diet food products+ tasty vs. healthy + not tasty Regular + positive vs. diet + negative+ tasty vs. healthy + not tasty Regular + positive vs. diet + negative

66 R. Mai et al. / Food Quality and Preference 39 (2015) 62–72
R2 is highly significant (F = 8.76, p < .01). Spotlight analysis demon-strates that for consumers who only weakly associate healthy foodwith tastiness (�1 SD below mean), low self-efficacy significantlyreduces intentions to adopt a healthy diet (b = .53, t = 3.502,p < .001). This influence is smaller for consumers with moderatetastiness associations towards healthy food items (0 SD: b = .23,t = 2.256, p < .05). However, for subjects with most favorable tasteassociations (+1 SD), intentions are high, regardless of nutritionself-efficacy (p > .05). A flood light analysis (Spiller, Fitzsimons,Lynch, & McClelland, 2013) identified regions where the influenceof self-efficacy on intention formation is significant. This Johnsonand Neyman (1936) significance region is below a moderate IATscore of D = 1.11.
In the next step, the analysis examines how the interplay ofintentions to adopt a healthy diet and implicit associations affectthe menu choices. Implicit associations determine whether inten-tions to adopt a healthy diet are reflected in healthier menuchoices. While this interaction effect is significant (b = �.27,t = �2.522, p < .05), there are no significant main effects (bothp > .05). Only for subjects with weak associations between healthyfood and tastiness, there are significant relationships (�1 SD:b = .24, t = 2.491, p < .05). The Johnson–Neyman significance regionis D 6 .89. Again, including the interaction effect strongly increasesexplained variances by 6.7% (F = 6.36, p < .05).
In sum, the results illustrate that implicit evaluations moderatethe impact of self-efficacy on intention to adopt a healthy diet andthey moderate the effect of these intentions on food menu choice.The Sobel test provides evidence that the mediation of the self-effi-cacy � implicit association interaction via the subject’s intention issignificant, confirming the mediated moderation model (one-tailed,indirect effect IE = .06, Z = 1.67, p 6 .05). To assess conditionaleffects, the Preacher and Hayes (2008, 2004) bootstrapping proce-dure with 1,000 samples is applied. This procedure helps to spot-light the different levels of implicit associations (one standarddeviation above/below the mean) and generates a bias-corrected95% confidence interval for the specific indirect effects. Given thatthe confidence interval (CI) does not include zero, the analysis sub-stantiates this paper’s basic assumption that nutrition self-efficacyis passed onto menu choice. The mediating effect is prominent forsubjects with less favorable tastiness associations towards healthyfood (�1 SD: IE = .12, CI = .01 to .33). For subjects who more closelyassociate healthy food with taste, however, there are no indirecteffects via the subject’s intentions (the CI includes 0). Given themore favorable implicit evaluation of healthy foods, they chosehealthier menus, regardless of perceived nutrition self-efficacyand explicitly formed intentions.
Table 2Regression of intention to adopt healthier eating behaviors (Main Study).
Model 1
b t p
Nutrition self-efficacy (NSE) .23 2.26*
Implicit taste associations .06 .54NSE � implicit taste associations �.30 �2.96**
Outcome expectanciesRisk perceptionSexImpulsivenessPositive moodHungerDiet
R2 (adjusted R2) .13 (.10)R2 increase by NSE � implicit taste .09 (.08)
Note: Significance of OLS regression (one-tailed).* p 6 .05.
** p 6 .01.*** p 6 .001.
Robustness test
The robustness of the findings were checked in two steps. First,risk perception and outcome expectancies are added to the analy-sis as these two variables are widely used to predict behavioralchange (e.g., Health Action Process Approach). Regression analysesdemonstrate that the interaction effect of self-efficacy and implicitassociations on the intention to eat healthy is stable after havingintroduced both variables (Table 2, Model 2). Analyses of condi-tional effects confirm the expected patterns. The indirect effect ofoutcome expectancies on menu choice via intention is solely sig-nificant for subjects with weaker healthiness/tastiness associations(�1 SD: IE = .13, CI = .01 to .36; 0 and +1 SD: p > .05). The indirecteffect of risk perception is significant as well for this group only(�1 SD: IE = .06, CI = .01 to .21 0 and +1 SD: p > .05).
Second, further socio-demographic and psychographic controlvariables were included: sex, impulsiveness, positive mood, hun-ger, and being on a diet. Still, regression analysis confirms thatthe key findings are stable for the comprehensive models (Table 2,Model 3). Both the main effects of the socio-cognitive predictorsand the interaction effects with implicit associations remain signif-icant. Finally, analyses of conditional effects for the extendedmodel shows that the indirect effect of nutrition self-efficacy viaintentions to eat healthy stays significant for subjects who lessstrongly associate healthy foods with tasty (IE = .10, CI = .01 to.31), whereas this influence is not significant for subjects withstronger implicit taste associations.
Discussion
This study reveals that the consideration of explicit nutritionself-efficacy and intentions is insufficient to explain why someconsumers make healthy nutrition choices and others do not. Con-sumer’s automatic associations towards healthy products’ tasti-ness are a crucial boundary condition because they are able tooverride the reasoned and intentional processes that are addressedby many informational and educational campaigns or interven-tions. The results show that implicit taste associations moderatethe influence of one’s perceived self-efficacy on intentions to eathealthy and, even more importantly, they have the potential to off-set their impact. For that reason, nutrition patterns of those withmore favorable taste associations are healthier, regardless of theirintentions to achieve or maintain a healthy eating behavior. Thiskey finding largely overlaps with previous research on the moder-ating role of habits, which can be considered as automatic
Model 2 Model 3
b t p b t p
.24 2.65* .22 2.44*
�.00 �.25 .02 .22�.26 �2.85** �.24 �2.57*
.36 4.06*** .30 3.03**
.25 2.74** .22 2.33*
�.11 �1.04.06 .66�.04 �.40�.12 �1.29
.12 1.22
.34 (.30) .38 (.30)
.06 (.06) .05 (.05)

R. Mai et al. / Food Quality and Preference 39 (2015) 62–72 67
responses to environmental cues (Brug, Kremers, Lenthe, Ball, &Crawford, 2008). Behaviors are only significantly shaped by inten-tions if habit strength is weak (Webb & Sheeran, 2006, p. 252).When habits are increasing in strength, subsequent behaviors areless likely guided by rational and conscious intentions. This wasconfirmed for different behaviors such as dietary intake (e.g., fruitconsumption, De Bruijn et al., 2007) or physical activity (Kremers,Dijkman, de Meij, Jurg, & Brug, 2008).
Overall, nutrition self-efficacy and implicit food associationsjointly determine the intention to adopt healthy eating habits and,in turn, food choices. The analysis further supports the mediatedmoderation model: Implicit associations determine whether ornot there is an effect of nutrition self-efficacy on the subject’s inten-tion to adopt a healthy diet which is passed to menu choice. In addi-tion, particularly for consumers with a weak belief in the notion thathealthy foods are tasty, low intentions to eat healthy result inunhealthier choices. Those with more favorable implicit taste asso-ciations eat more healthy, even if their explicit intentions are low.
This study confirms the expected moderating role of implicitassociations. Given that the interaction effect’s direction is oppo-site to our expectations, the results only partly confirm hypothesesH1 and H2. While implicit associations obviously moderate theinfluence of self-efficacy on eating intentions and behaviors, theshape of the moderating influence may vary across several bound-ary variables. Thus, it is advisable to test this effect for other sam-ples and in a different context.
Replication Study A
Objective
The Main Study is a rather conservative test of our assumptionsbecause the study was based on a sample of young consumers. Thisgroup is generally less concerned about their health and nutritionalstatus. To test for generalizability and to assess the robustness ofthe observed interplay between explicit and implicit drivers, thisfollow-up-study aims to replicate the main findings for older andhealth-concerned consumers who have undergone preventivenutritional counseling. As a second goal, this study addresses alter-native explanations. By including explicit measures of taste impor-tance, the incremental influence of implicit measures is isolated.
Design
Replication Study A applies a similar design as the Main Study.The respondents were asked to complete a brief questionnairewhich covered the previously used measures of nutrition self-effi-cacy (M = 4.89, SD = .70, a = .78), the intention to adopt a healthierdiet (M = 5.50, SD = 1.02, a = .87), outcome expectancies (M = 5.67,SD = 1.02, a = .78), and risk perception (M = 3.82, SD = 1.53,a = .86). To measure healthy nutrition behavior, participants wereasked to what extent their food consumption is in accordance withten guidelines for healthy nutrition released by the German Nutri-tion Society DGE (e.g., vegetables and fruit – take ‘5 a day’). Theanswers on the ten items (‘‘My nutrition behavior is – knowinglyor unknowingly – consistent with this rule’’; three-point scale withthe anchors 0 ‘no’, 1 ‘yes’) were combined to an index ranging from0 to 10 (M = 5.56, SD = 1.93). The study also employed explicitmeasures assessing the importance of taste (M = 4.51, SD = 1.04,a = .63) (three-items seven-point Likert scales suggested byScholderer, Brunsø, Bredahl, & Grunert, 2004). The questionnairemeasured several controls, such as hunger, positive mood, house-hold size (number of persons in household) and education (dichot-omous variable with 1 ‘apprenticeship training or similar’ and 2‘academic studies’). In addition, the subjects completed the IAT of
the Main Study employing the targets ‘unhealthy vs. healthy’ andthe evaluative attributes ‘tasty vs. not tasty’.
Participants were recruited from the diabetes genetic studydatabase (DIAGEN). These subjects have a considerable risk of typeII diabetes and they have received medical treatment as well asnutritional counseling in a prevention program (Schwarz et al.,2006). The study was part of a larger project (Hoppert et al.,2014). Seventy-one subjects participated in this study (61% female,56 years, SD = 17.76, BMI = 28.98, SD = 5.28). Compared to theMain Study’s sample, these subjects have much greater abilitiesto maintain healthy eating (MMain Study = 4.37, MReplication Study A =4.89, t = 4.429, p < .001) and significantly higher intentions toadopt a healthy diet (MMain Study = 4.68, MReplication Study A = 5.50,t = 5.088, p < .001).
Results
We applied a hierarchical approach to analyze the influence onintentions to eat healthy (Models 1–3) and adherence to nutritionguidelines (Models 4–6). In step 1, the analysis of reaction timesreveals a highly significant IAT effect (MD-schore = .95, SD = .43,t = 17.97, p < .001). This implicit belief that unhealthy food itemsare less tasty moderates the impact of nutrition self-efficacy onthe consumer’s intention to adopt a healthy diet (Table 3, Model1). Model 4 demonstrates that implicit taste associations qualifywhether the subject’s diet is in line with nutrition guidelines.Including the implicit measure helps increase the explained vari-ance of intentions as well as that of adherence to nutrition guide-lines by six percent. Consistent with the results of the Main Study,the analyses of conditional effects confirm that nutrition self-effi-cacy guides intentions and adherence to nutrition guidelines, par-ticularly for consumers with less favorable taste associations (�1SD) (Table 3). The impact of self-efficacy is lower for moderate tast-iness associations and insignificant for strong implicit taste associ-ations. In step 2, the models included the explicit measure of tasteimportance and its interaction with nutrition self-efficacy. For bothintentions (Model 2) and adherence to nutrition guidelines (Model5), we observe no additional significant coefficients and the inter-action between the implicit measure and nutrition self-efficacyremains stable. The interactive effect holds when including thesocial cognitive predictors of health behavior change and the con-trols (hunger, positive mood, household size, education) in thethird step (Models 3 and 6).
Finally, we estimate the mediated moderation model, accordingto which implicit taste associations moderate the influence ofnutrition self-efficacy on the intention to eat healthy and examineif this moderation is passed on to food consumption consistentwith nutrition guidelines. The procedure proposed by Mulleret al. (2005) supports this pattern and the mediated interactioneffect via intentions is significant (one-tailed, Z = 1.66, p 6 .05).Spotlighting the conditional effects confirms that there is an indi-rect effect of nutrition self-efficacy on the criterion variable viaintentions for subjects with low implicit tastiness associationstowards healthy foods (�1 SD, IE = .34, CI .06 to .69). For those withmore favorable implicit associations, this indirect effect is weaker(0 SD, IE = .16, CI .01 to .44) or insignificant (+1 SD, IE = .04, CIincludes 0).
Discussion
This study supports the generalizability of our central premise.Including the moderating influence of implicit associationsimproves the accuracy of health behavior models. The questionof whether nutrition self-efficacy is helpful in stimulating healthierconsumption patterns is dependent upon implicit associations.Remarkably, our study confirms the crucial role of implicit barriers
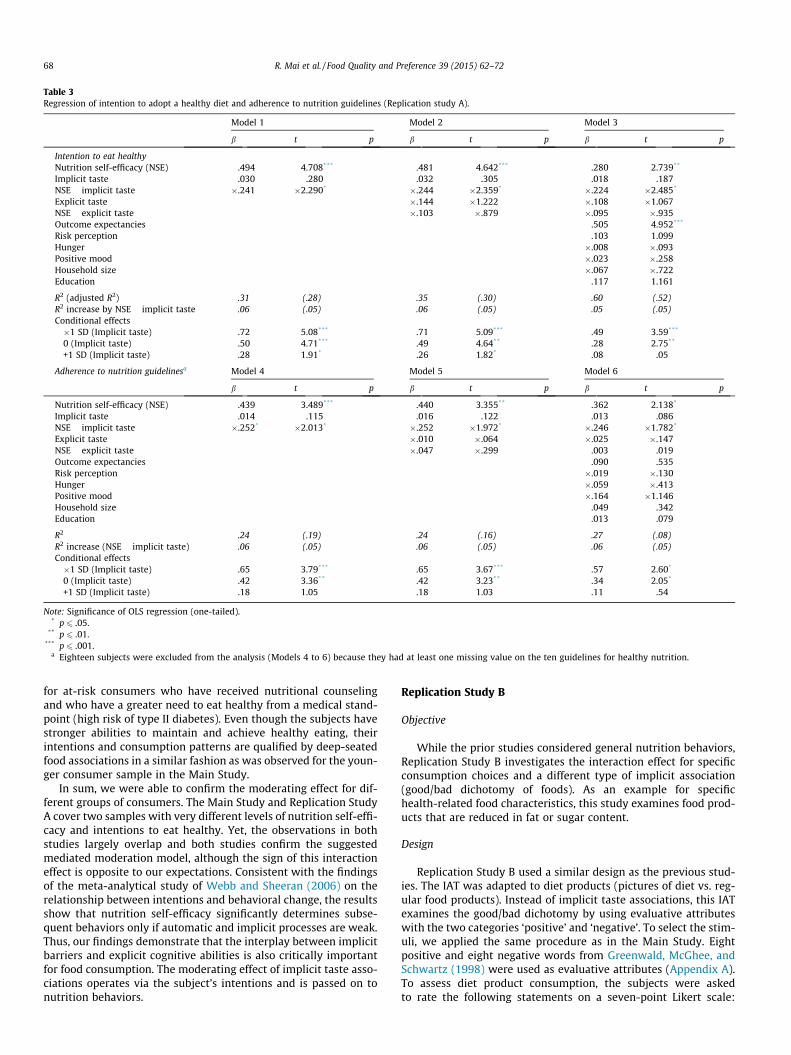
Table 3Regression of intention to adopt a healthy diet and adherence to nutrition guidelines (Replication study A).
Model 1 Model 2 Model 3
b t p b t p b t p
Intention to eat healthyNutrition self-efficacy (NSE) .494 4.708*** .481 4.642*** .280 2.739**
Implicit taste .030 .280 .032 .305 .018 .187NSE � implicit taste �.241 �2.290* �.244 �2.359* �.224 �2.485*
Explicit taste �.144 �1.222 �.108 �1.067NSE � explicit taste �.103 �.879 �.095 �.935Outcome expectancies .505 4.952***
Risk perception .103 1.099Hunger �.008 �.093Positive mood �.023 �.258Household size �.067 �.722Education .117 1.161
R2 (adjusted R2) .31 (.28) .35 (.30) .60 (.52)R2 increase by NSE � implicit taste .06 (.05) .06 (.05) .05 (.05)Conditional effects�1 SD (Implicit taste) .72 5.08*** .71 5.09*** .49 3.59***
0 (Implicit taste) .50 4.71*** .49 4.64** .28 2.75**
+1 SD (Implicit taste) .28 1.91* .26 1.82* .08 .05
Adherence to nutrition guidelinesa Model 4 Model 5 Model 6
b t p b t p b t p
Nutrition self-efficacy (NSE) .439 3.489*** .440 3.355** .362 2.138*
Implicit taste .014 .115 .016 .122 .013 .086NSE � implicit taste �.252* �2.013* �.252 �1.972* �.246 �1.782*
Explicit taste �.010 �.064 �.025 �.147NSE � explicit taste �.047 �.299 .003 .019Outcome expectancies .090 .535Risk perception �.019 �.130Hunger �.059 �.413Positive mood �.164 �1.146Household size .049 .342Education .013 .079
R2 .24 (.19) .24 (.16) .27 (.08)R2 increase (NSE � implicit taste) .06 (.05) .06 (.05) .06 (.05)Conditional effects�1 SD (Implicit taste) .65 3.79*** .65 3.67*** .57 2.60*
0 (Implicit taste) .42 3.36** .42 3.23** .34 2.05*
+1 SD (Implicit taste) .18 1.05 .18 1.03 .11 .54
Note: Significance of OLS regression (one-tailed).* p 6 .05.
** p 6 .01.*** p 6 .001.
a Eighteen subjects were excluded from the analysis (Models 4 to 6) because they had at least one missing value on the ten guidelines for healthy nutrition.
68 R. Mai et al. / Food Quality and Preference 39 (2015) 62–72
for at-risk consumers who have received nutritional counselingand who have a greater need to eat healthy from a medical stand-point (high risk of type II diabetes). Even though the subjects havestronger abilities to maintain and achieve healthy eating, theirintentions and consumption patterns are qualified by deep-seatedfood associations in a similar fashion as was observed for the youn-ger consumer sample in the Main Study.
In sum, we were able to confirm the moderating effect for dif-ferent groups of consumers. The Main Study and Replication StudyA cover two samples with very different levels of nutrition self-effi-cacy and intentions to eat healthy. Yet, the observations in bothstudies largely overlap and both studies confirm the suggestedmediated moderation model, although the sign of this interactioneffect is opposite to our expectations. Consistent with the findingsof the meta-analytical study of Webb and Sheeran (2006) on therelationship between intentions and behavioral change, the resultsshow that nutrition self-efficacy significantly determines subse-quent behaviors only if automatic and implicit processes are weak.Thus, our findings demonstrate that the interplay between implicitbarriers and explicit cognitive abilities is also critically importantfor food consumption. The moderating effect of implicit taste asso-ciations operates via the subject’s intentions and is passed on tonutrition behaviors.
Replication Study B
Objective
While the prior studies considered general nutrition behaviors,Replication Study B investigates the interaction effect for specificconsumption choices and a different type of implicit association(good/bad dichotomy of foods). As an example for specifichealth-related food characteristics, this study examines food prod-ucts that are reduced in fat or sugar content.
Design
Replication Study B used a similar design as the previous stud-ies. The IAT was adapted to diet products (pictures of diet vs. reg-ular food products). Instead of implicit taste associations, this IATexamines the good/bad dichotomy by using evaluative attributeswith the two categories ‘positive’ and ‘negative’. To select the stim-uli, we applied the same procedure as in the Main Study. Eightpositive and eight negative words from Greenwald, McGhee, andSchwartz (1998) were used as evaluative attributes (Appendix A).To assess diet product consumption, the subjects were askedto rate the following statements on a seven-point Likert scale:

R. Mai et al. / Food Quality and Preference 39 (2015) 62–72 69
‘‘For many food products, I regularly choose the diet variant’’, and‘‘I usually buy the ‘light’ version of a food product’’ (M = 3.61,SD = 1.49, a = .92). Nutrition self-efficacy was measured with theinstrument used in the Main Study (M = 4.30, SD = 1.09, a = .70).Thirty-six young consumers (75% female, mean age 25.0 years,SD = 2.56, BMI = 22.31, SD = 2.77) took part in the study.
Results
The analysis shows that respondents’ implicit evaluations ofproducts which are reduced in fat or sugar content are much moreheterogeneous than the taste evaluations of healthy food productsobserved in the Main Study. The IAT effect is significant (MD-score = .20, t = 2.058, p < .05), suggesting that fat-/sugar-reducedproducts, on average, are evaluated positively. Yet, the relativelywide range of IAT effects from -1.03 to 1.08 indicates that implicitevaluations of such products can be rather negative for some con-sumers and rather positive for others.
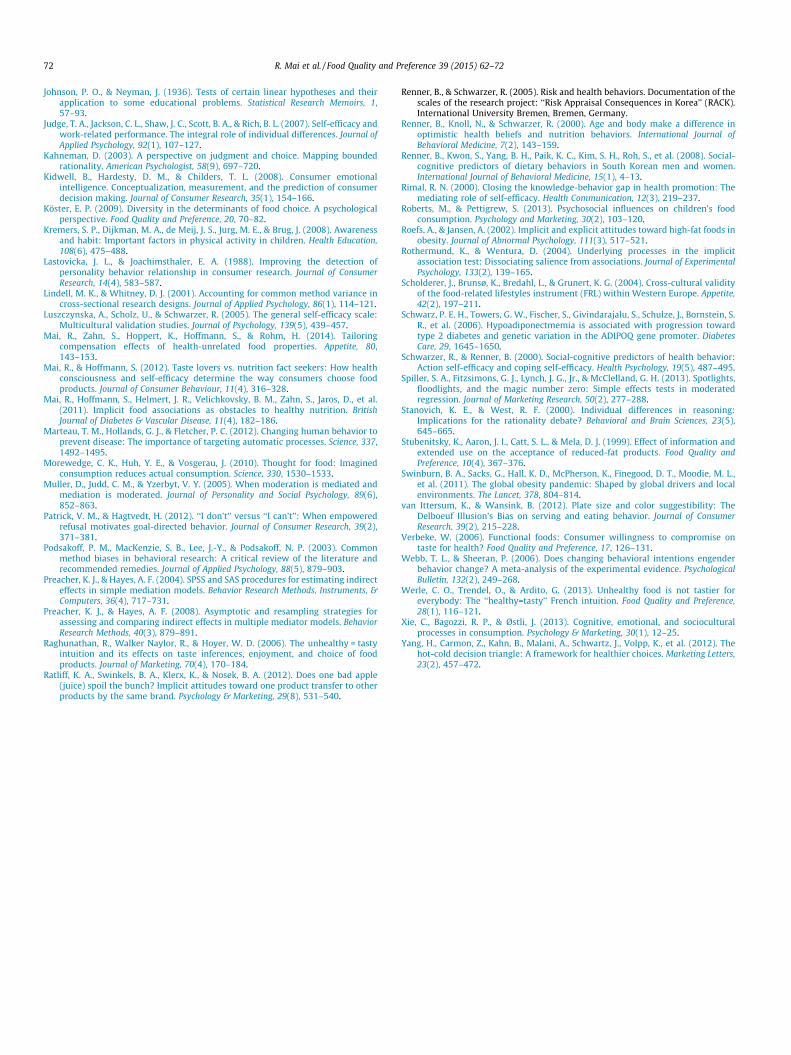
Regression analysis confirms that implicit associations moder-ate the impact of nutrition self-efficacy on diet food product con-sumption (interaction: b = .38, t = 2.395, p < .05). Both nutritionself-efficacy (b = .35, t = 2.076, p < .05) and implicit associations(b = .36, t = 2.212, p < .05) exert significant main influences as well(R2 = 0.25). As in the Main Study, including the interaction termresults in a considerable gain in explained variance of 13.4%(F = 5.73, p < .05). The analysis of conditional effects demonstratesthat diet product consumption is driven by perceived self-efficacyprimarily for those with a rather positive implicit evaluation (+1SD: b = .75, t = 2.787, p < .01; 0: b = .35, t = 2.076, p < .05; �1 SD:p > .05). The Johnson–Neyman significance region is D P �.01. Ifimplicit associations towards diet food products are positive, sub-jects with high self-efficacy significantly consume more diet foodproducts than subjects with lower self-efficacy (Fig. 2). For subjectswith negative implicit evaluations, the consumption of fat-/sugar-reduced products is low, regardless of perceived nutrition self-efficacy.
Discussion
The second Replication Study supports hypothesis H3b and con-firms that the interplay between implicit and explicit processesaffects the consumption of specific products as well. Again, nutri-tion self-efficacy alone cannot predict healthy food consumptionsufficiently. Scholars need to consider the moderating role of impli-cit food associations to improve the prediction. Our study hasrevealed that including the interactive term helps increaseexplained variance in diet food product consumption by 13%, whichis a strong effect according to the conventions of Cohen (1988). Rep-lication Study B thus contributes to the robustness of our claim andreveals an important observation. Unlike for implicit taste associa-tions measured in the previous studies, this study’s IAT effect ismuch more heterogeneous and much closer to the measure’s
Consumption of fat/sugar-reduced products
Nutrition self-efficacy
low high
Index score
1
3
5
76
4
2
Implicit associations
positivenegative
Fig. 2. Consumption of fat/sugar-reduced products as a func
absolute zero point. This may explain why the interaction effectof Study B has a different pattern. As a bottom line, across all stud-ies, we find that favorable implicit associations are crucial for stim-ulating healthier food consumption and eating behaviors.
General discussion
Implications for future research
A series of three studies provides evidence that the influence ofnutrition self-efficacy is moderated by associations that are acti-vated automatically. This finding is robust across different samples,settings, and dependent variables. Yet, the shape of this interactioneffect varies with the type of implicit associations considered. Weshow that favorable implicit taste associations are able to attenu-ate the negative consequences of low nutrition self-efficacy andlow intentions to eat healthy. Regarding implicit good/bad associ-ations towards diet food products, positive implicit evaluations ofdiet products are the basis on which nutrition self-efficacy can betranslated into action.
This paper’s findings provide a basis for future research and the-ory development. We demonstrate that it is particularly insightfulto study more deeply the implicit processes of food choice. Takinginto account deep-seated barriers can help bridge the gap betweenhealthy food attitudes/intentions and eating behaviors to someextent. Accordingly, our findings suggest adding implicit associa-tions to the widely used social-cognitive models of health behaviorin order to increase their predictive power. In the Main Study, forexample, it was shown that the influences of the three major pre-dictors (self-efficacy, outcome expectancies, risk perception) andthe key mediator (intention to adopt a healthy diet) of the estab-lished Health Action Process Approach model can be explained bet-ter when including implicit taste associations. This research callsfor further investigations to test such extensions. Also consumerpsychology models that are centered on goal conflicts (e.g., ethicsvs. prices, sustainable consumption vs. convenience) and goal-directed behavior (e.g., Xie, Bagozzi, & Østli, 2013) should beextended to include implicit barriers.
As with all empirical investigations, this research has somemethodological limitations. In our series of studies, we examineda specific facet of nutrition self-efficacy that is particularly relevantin the pre-actional stage. It might be interesting to examine impli-cit influences also in the post-intentional phases when the individ-ual aims to sustain a healthier lifestyle over a long period. At thisstage of behavioral change, ‘coping-self-efficacy’ is the better pre-dictor (which may depend on implicit processes as well). In thisregard, longitudinal studies may be helpful to examine how theimplicit mechanisms change over time. Note, we applied thewidely used measurement suggested by Schwarzer and Renner(2000). To support the generalizability of our findings, scholarsshould employ alternative measures of self-efficacy (e.g.,Anderson et al., 2000). We also call for more research that modifies
Regression results
Notes. OLS regression (one-tailed), *p < .05.
β (p) t- value
Nutrition self-efficacy (S) .35* 2.076Implicit associations (I) .36* 2.212
S I .38* 2.395
R2 interaction effect = .13 (R2full model = .25)
tion of nutrition self-efficacy and implicit associations.

Healthy food items Unhealthy food items
Tasty Not tasty
deliciousyummy
appetizingflavorfulappealingenjoyable
mouthwateringpalatable
dislikedless enjoyableunappealing
blandflavorless
unappetizingunpalatableunsavory
Positive Negative
pleasurecheerhappygentlelove
caresslucky
laughter
murderassault
jailhatredvomitdeathkill
divorce
70 R. Mai et al. / Food Quality and Preference 39 (2015) 62–72
the setting (e.g., smoking, physical activity, addiction to alcohol),other types of implicit associations and dependent variables, suchas actual eating or choices in a real shopping environment (e.g.,grocery store).
Our Main Study and Replication Study A recruit consumers withrather low and rather high nutrition self-efficacy scores and inten-tions to eat healthy. While both studies cover the more extremepoints, it would be interesting to investigate the full range ofself-efficacy and intentions, employing a larger and more heteroge-neous sample. In addition, priming studies should aim to manipu-late the subject’s implicit associations systematically.
As regards to Replication Study B, it is important to note thatthe associations with fat- and sugar-reduced products are hetero-geneous. While some subjects view such products positively, oth-ers have more negative associations. Also prior research observeda mild negative effect of a ‘‘reduced in fat’’-information on con-sumer acceptance (e.g., chocolate snack bars, Stubenitsky, Aaron,Catt, & Mela, 1999). Future research should explore the underlyingreasons as to why the subjects’ opinions diverge. Are diet productsevaluated negatively by some consumers because they are per-ceived less palatable than the conventional variant? Are consumersconcerned with supplements or substitutions (e.g., artificial sweet-eners) that may have unfavorable side-effects? In addition, futurestudies should elaborate on the distinct interaction patterns ofthe different types of implicit associations. In this regard, it wouldbe insightful to scrutinize more closely the relationship betweentastiness and healthiness, because recent findings (Werle,Trendel, & Ardito, 2013) have sparked a debate about whether bothcomponents are inversely related. For example, unlike for the U.S.-American-based sample of the original study (Raghunathan et al.,2006), healthy is considered tastier in France (Werle et al., 2013).Our results confirm the latter observation. Future studies shouldexamine the meaningfulness of the IAT measure’s zero point(Blanton & Jaccard, 2006) and they should validate the locationof the threshold value (the cutoff value for that region of IAT scoreswhere healthy foods are considered tastier than unhealthy foodsand that region where unhealthy foods are considered tastier).
Finally, and most importantly, future research should answerthe fundamental question of how implicit automatic associationstowards healthy foods can be changed. For example, Horcajo,Briñol, and Petty (2010) showed that this may be achieved withthe help of ad messages or feedback. In addition, there are indica-tions that the link between tastiness and healthiness depends onindividual consumer characteristics, such as culture and socializa-tion, see the above-mentioned difference between US-American(Raghunathan et al., 2006) and French consumers (Werle et al.,2013). Irmak, Vallen, and Robinson (2011) hint that this implicitlink between taste and healthiness also depends on motivationalfactors, such as weight loss. The findings of Verbeke (2006) suggestthat one’s health orientation may correlate with taste associations,because consumers with a strong health orientation are more will-ing to accept a worse taste of functional foods with benefits fortheir future health.
Since insights into how to change implicit associations is lim-ited, future research should aim to develop interventions targetingimplicit aspects as well. Knowledge is also needed on the consumersegments with the most unfavorable implicit associations as wellas demographic or psychographic correlates to identify the mostimportant targets for a successful intervention campaign. Beyondinformational and educational campaigns, alternative ways shouldbe explored to compensate for unfavorable taste associations.Recent findings hint that optimizing food products can helpincrease the attractiveness of healthier product variants (Maiet al., 2014). Future studies should explore how to elicit such com-pensation effects for consumer’s with unfavorable implicit associ-ations and how to tailor compensation effects most effectively.
Conclusions
Although there is evidence that intuitive thinking is highly rel-evant in a food consumption context (and even more relevant thanrational considerations), automatic reactions and implicit pro-cesses have been largely disregarded (e.g., Köster, 2009; Marteauet al., 2012). This investigation provides an answer to the questionof why increasing nutrition self-efficacy is not sufficient to stimu-late healthy food consumption for some consumer segments. Thechallenge now is to find feasible ways to target consumers’ implicitassociations. The key findings reported in this paper encourageresearchers, practitioners and public policy makers to take intoaccount implicit associations towards healthy food products and/or health care services if they aim at changing food choices. Forexample, research on nudging and designing effective choice archi-tectures should incorporate such implicit processes. Based on thekey findings, policy makers are well advised to tackle implicit asso-ciations in social marketing campaigns because enhancing knowl-edge and motivation (e.g., self-efficacy, expectancy value, goalsetting) are only one side of the coin (Block et al., 2011).
This paper’s findings hopefully motivate managers to nuancetheir products and services to the customer’s deep-seated prefer-ences and they should track their implicit attitudes, for example,by applying the IAT. Firms that are targeting consumers with a highlevel of healthy eating behavior should keep in mind that theseconsumers have specific preferences. On the contrary, such mea-sures are deemed inefficient once targeting consumers with lowerbeliefs in their ability to maintain a healthy diet. When focusing onthis consumer segment, pinpointing the healthy nature of the foodserved or highlighting comprehensive product information in themenu or food packaging may be even counterproductive. Hence,overcoming the implicit barriers is a major challenge for research-ers, companies and policy makers.
Acknowledgement
This research project approach was supported by the GermanFederal Ministry of Education and Research, Berlin, Germany (grant01EA1325).
Appendix A. Stimuli and evaluative attributes used in the IATs
R. Mai et al. / Food Quality and Preference 39 (2015) 62–72 71
Appendix B. Measurement of the explicit latent constructs
Wording
FactorloadingsNutrition self-efficacy (M = 4.37, SD = .77,EV = 52%, a = .70)
I can manage to stick to a healthy diet. . .. . . even if I have to learn much aboutnutrition
.75
. . . even if I have to watch out in manysituations
.70
. . . even if I have to make a detailed plan
.68. . . even if I have to rethink my entire way ofnutrition
.76
Intention to adopt a healthy diet (M = 4.68, SD = 1.03,EV = 61%, a = .78)
I intend to live a healthier life .78 I intend to eat healthful foods over the nextmonths.86
I intend to eat only a very small amount of fat(such as saturated fat, cheese, butter) over thenext months
.54
I intend to invest more into my health
.89Risk perception (M = 3.11, SD = 1.29, EV = 72%,a = .79)
If I compare myself with others of my age andgender, I estimate the likelihood ofexperiencing. . .1. . . heart disease
.87
. . . high blood pressure
.77. . . a stroke
.91Outcome expectancies (M = 5.05, SD = 1.33,
EV = 65%, a = .73) If I stick to a low-fat, high-fiber diet, then . . .. . . I would feel physically more attractive
.87. . . I would feel better mentally
.68. . . I would have no (or fewer) weight problems
.86 Impulsiveness (M = 4.91, SD = 1.06, EV = 63%,a = .70)
I do things without thinking .82 I plan tasks carefullyr .85 I am self-controlledr .71Positive mood (M = 4.35, SD = .48, EV = 50%,a = .67)
How do you feel at the moment?.... . . Content
.74. . . Happy
.66. . . Sadr
.75. . . Disappointedr
.68Hunger (M = 3.02, SD = 1.16)
How do you feel at the moment? Hungry –Diet (8.9% on a diet)
Are you on a diet right now? –Notes: Explorative factor analysis (PCA, Varimax-rotation).EV = explained variance, a = Cronbach’s alpha, M = Mean,SD = Standard deviation. r = reversely coded. 1 = seven-pointsemantic differential scale anchored at ‘‘much below average’’and ‘‘much above average’’.
References
Anderson, E. S., Winett, R. A., & Wojcik, J. R. (2000). Social-cognitive determinants ofnutrition behavior among supermarket food shoppers: A structural equationanalysis. Health Psychology, 19(5), 479–486.
Anderson, E. S., Winett, R., Wojcik, J., Winett, S., & Bowden, T. (2001). A computerizedsocial cognitive intervention for nutrition behavior: Direct and mediated effects onfat, fiber, fruits, and vegetables, self-efficacy, and outcome expectations amongfood shoppers. Annals of Behavioral Medicine, 23(2), 88–100.
Balcombe, K., Fraser, I., & Falco, S. D. (2010). Traffic lights and food choice. A choiceexperiment examining the relationship between nutritional food labels andprice. Food Policy, 35(3), 211–220.
Bandura, A. (1977). Self-efficacy: The exercise of control. New York: Freeman.Bandura, A. (1986). Social foundations of thought and action. Englewood Cliffs:
Prentice Hall.Baranowski, T., Baranowski, J. C., Cullen, K. W., Marsh, T., Islam, N., Zakeri, I., et al.
(2003). Squire’s quest! Dietary outcome evaluation of a multimedia game.American Journal of Prevention Medicine, 24, 52–61.
Blanton, H., & Jaccard, J. (2006). Arbitrary metrics in psychology. AmericanPsychologist, 61(1), 27–41.
Block, L. G., Grier, S. A., Childers, T. L., Davis, B., Ebert, J. E. J., Kumanyika, S., et al.(2011). From nutrients to nurturance. A conceptual introduction to food well-being. Journal of Public Policy & Marketing, 30(1), 5–13.
Brug, J., Kremers, S. P., Lenthe, F. V., Ball, K., & Crawford, D. (2008). Environmentaldeterminants of healthy eating: In need of theory and evidence. Proceedings ofthe Nutrition Society, 67, 307–316.
Cervellon, M.-C., Dubé, L., & Knäuper, B. (2007). Implicit and explicit influences onspontaneous and deliberate food choices. Advances in Consumer Research, 31,104–109.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ:Lawrence Erlbaum.
Consumers Union (2005). Marketing of soda, candy, snacks and fast foods drowns outhealthful messages, <http://www.consumersunion.org/pdf/OutofBalance.pdf>.
Czyzewska, M., & Graham, R. (2008). Implicit and explicit attitudes to high- andlow-calorie food in females with different BMI status. Eating Behaviors, 9(3),303–312.
De Bruijn, G. J., Kremers, S. P., De Vet, E., De Nooijer, J., Van Mechelen, W., & Brug, J.(2007). Does habit strength moderate the intention–behaviour relationship inthe theory of planned behaviour? The case of fruit consumption. Psychology andHealth, 22(8), 899–916.
Dimofte, C. V. (2010). Implicit measures of consumer cognition: A review.Psychology & Marketing, 27(10), 921–937.
Fornell, C. A., & Larcker, D. F. (1981). Evaluating structural equation models withunobservable variables and measurement error. Journal of Marketing Research,18(1), 39–50.
Frieden, T. R., Dietz, W., & Collins, J. (2010). Reducing childhood obesity throughpolicy change: Acting now to prevent obesity. Health Affair, 29(3), 357–363.
Grainger, C., Senauer, B., & Runge, C. F. (2007). Nutritional improvements andstudent food choices in a school lunch program. Journal of Consumer Affairs,41(2), 265–284.
Greenwald, A. G., McGhee, D. E., & Schwartz, J. L. (1998). Measuring individualdifferences in implicit cognition: The implicit association test. Journal ofPersonality and Social Psychology, 74(6), 1464–1480.
Greenwald, A. G., Nosek, B. A., & Banaji, M. R. (2003). Understanding and using theimplicit association test: I. An improved scoring algorithm. Journal of Personalityand Social Psychology, 85(2), 197–216.
Gregg, A. P., & Klymowsky, J. (2013). The Implicit Association Test in marketresearch: Potentials and pitfalls. Psychology and Marketing, 30(7), 588–601.
Grynbaum, M. M. (2013). Judge blocks New York City’s limits on big sugary drinks.The New York Times, (March 11), <http://www.nytimes.com/2013/03/12/nyregion/judge-invalidates-bloombergs-soda-ban.html?pagewanted=all>Accessed 24.05.13.
Haws, K. L., & Winterich, K. P. (2013). When value trumps health in a supersizedworld. Journal of Marketing, 77(3), 48–64.
Hoefling, A., & Strack, F. (2008). The tempting effect of forbidden foods: High caloriecontent evokes conflicting implicit and explicit evaluations in restrained eaters.Appetite, 51(3), 681–689.
Hoegg, J., & Alba, J. W. (2007). Taste perception: More than meets the tongue.Journal of Consumer Research, 33(4), 490–498.
Holden, G. (1991). The relationship of self-efficacy appraisals to subsequent healthrelated outcomes: A meta-analysis. Social Work in Health Care, 16(1), 53–93.
Hoppert, K., Mai, R., Zahn, S., Hoffmann, S., & Rohm, H. (2012). Integrating sensoryevaluation in adaptive conjoint analysis to elaborate the conflicting influence ofintrinsic and extrinsic attributes on food choice. Appetite, 59(3), 949–965.
Hoppert, K., Mai, R., Zahn, S., Schwarz, P. E., Hoffmann, S., & Rohm, H. (2014). Is therea fit in cognitive and sensory evaluation of yogurt? The moderating role ofnutrition training. Food Quality and Preference, 31, 65–68.
Horcajo, J., Briñol, P., & Petty, R. E. (2010). Consumer persuasion: Indirect changeand implicit balance. Psychology & Marketing, 27(10), 938–963.
Howlett, E. A., Burton, S., Bates, K., & Huggins, K. (2009). Coming to a restaurant nearyou? Potential consumer responses to nutrition information disclosure onmenus. Journal of Consumer Research, 36, 494–503.
Irmak, C., Vallen, B., & Robinson, S. R. (2011). The impact of product name on dieters’and nondieters’ food evaluations and consumption. Journal of ConsumerResearch, 38(2), 390–405.
72 R. Mai et al. / Food Quality and Preference 39 (2015) 62–72
Johnson, P. O., & Neyman, J. (1936). Tests of certain linear hypotheses and theirapplication to some educational problems. Statistical Research Memoirs, 1,57–93.
Judge, T. A., Jackson, C. L., Shaw, J. C., Scott, B. A., & Rich, B. L. (2007). Self-efficacy andwork-related performance. The integral role of individual differences. Journal ofApplied Psychology, 92(1), 107–127.
Kahneman, D. (2003). A perspective on judgment and choice. Mapping boundedrationality. American Psychologist, 58(9), 697–720.
Kidwell, B., Hardesty, D. M., & Childers, T. L. (2008). Consumer emotionalintelligence. Conceptualization, measurement, and the prediction of consumerdecision making. Journal of Consumer Research, 35(1), 154–166.
Köster, E. P. (2009). Diversity in the determinants of food choice. A psychologicalperspective. Food Quality and Preference, 20, 70–82.
Kremers, S. P., Dijkman, M. A., de Meij, J. S., Jurg, M. E., & Brug, J. (2008). Awarenessand habit: Important factors in physical activity in children. Health Education,108(6), 475–488.
Lastovicka, J. L., & Joachimsthaler, E. A. (1988). Improving the detection ofpersonality behavior relationship in consumer research. Journal of ConsumerResearch, 14(4), 583–587.
Lindell, M. K., & Whitney, D. J. (2001). Accounting for common method variance incross-sectional research designs. Journal of Applied Psychology, 86(1), 114–121.
Luszczynska, A., Scholz, U., & Schwarzer, R. (2005). The general self-efficacy scale:Multicultural validation studies. Journal of Psychology, 139(5), 439–457.
Mai, R., Zahn, S., Hoppert, K., Hoffmann, S., & Rohm, H. (2014). Tailoringcompensation effects of health-unrelated food properties. Appetite, 80,143–153.
Mai, R., & Hoffmann, S. (2012). Taste lovers vs. nutrition fact seekers: How healthconsciousness and self-efficacy determine the way consumers choose foodproducts. Journal of Consumer Behaviour, 11(4), 316–328.
Mai, R., Hoffmann, S., Helmert, J. R., Velichkovsky, B. M., Zahn, S., Jaros, D., et al.(2011). Implicit food associations as obstacles to healthy nutrition. BritishJournal of Diabetes & Vascular Disease, 11(4), 182–186.
Marteau, T. M., Hollands, G. J., & Fletcher, P. C. (2012). Changing human behavior toprevent disease: The importance of targeting automatic processes. Science, 337,1492–1495.
Morewedge, C. K., Huh, Y. E., & Vosgerau, J. (2010). Thought for food: Imaginedconsumption reduces actual consumption. Science, 330, 1530–1533.
Muller, D., Judd, C. M., & Yzerbyt, V. Y. (2005). When moderation is mediated andmediation is moderated. Journal of Personality and Social Psychology, 89(6),852–863.
Patrick, V. M., & Hagtvedt, H. (2012). ‘‘I don’t’’ versus ‘‘I can’t’’: When empoweredrefusal motivates goal-directed behavior. Journal of Consumer Research, 39(2),371–381.
Podsakoff, P. M., MacKenzie, S. B., Lee, J.-Y., & Podsakoff, N. P. (2003). Commonmethod biases in behavioral research: A critical review of the literature andrecommended remedies. Journal of Applied Psychology, 88(5), 879–903.
Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirecteffects in simple mediation models. Behavior Research Methods, Instruments, &Computers, 36(4), 717–731.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies forassessing and comparing indirect effects in multiple mediator models. BehaviorResearch Methods, 40(3), 879–891.
Raghunathan, R., Walker Naylor, R., & Hoyer, W. D. (2006). The unhealthy = tastyintuition and its effects on taste inferences, enjoyment, and choice of foodproducts. Journal of Marketing, 70(4), 170–184.
Ratliff, K. A., Swinkels, B. A., Klerx, K., & Nosek, B. A. (2012). Does one bad apple(juice) spoil the bunch? Implicit attitudes toward one product transfer to otherproducts by the same brand. Psychology & Marketing, 29(8), 531–540.
Renner, B., & Schwarzer, R. (2005). Risk and health behaviors. Documentation of thescales of the research project: ‘‘Risk Appraisal Consequences in Korea’’ (RACK).International University Bremen, Bremen, Germany.
Renner, B., Knoll, N., & Schwarzer, R. (2000). Age and body make a difference inoptimistic health beliefs and nutrition behaviors. International Journal ofBehavioral Medicine, 7(2), 143–159.
Renner, B., Kwon, S., Yang, B. H., Paik, K. C., Kim, S. H., Roh, S., et al. (2008). Social-cognitive predictors of dietary behaviors in South Korean men and women.International Journal of Behavioral Medicine, 15(1), 4–13.
Rimal, R. N. (2000). Closing the knowledge-behavior gap in health promotion: Themediating role of self-efficacy. Health Communication, 12(3), 219–237.
Roberts, M., & Pettigrew, S. (2013). Psychosocial influences on children’s foodconsumption. Psychology and Marketing, 30(2), 103–120.
Roefs, A., & Jansen, A. (2002). Implicit and explicit attitudes toward high-fat foods inobesity. Journal of Abnormal Psychology, 111(3), 517–521.
Rothermund, K., & Wentura, D. (2004). Underlying processes in the implicitassociation test: Dissociating salience from associations. Journal of ExperimentalPsychology, 133(2), 139–165.
Scholderer, J., Brunsø, K., Bredahl, L., & Grunert, K. G. (2004). Cross-cultural validityof the food-related lifestyles instrument (FRL) within Western Europe. Appetite,42(2), 197–211.
Schwarz, P. E. H., Towers, G. W., Fischer, S., Givindarajalu, S., Schulze, J., Bornstein, S.R., et al. (2006). Hypoadiponectmemia is associated with progression towardtype 2 diabetes and genetic variation in the ADIPOQ gene promoter. DiabetesCare, 29, 1645–1650.
Schwarzer, R., & Renner, B. (2000). Social-cognitive predictors of health behavior:Action self-efficacy and coping self-efficacy. Health Psychology, 19(5), 487–495.
Spiller, S. A., Fitzsimons, G. J., Lynch, J. G., Jr., & McClelland, G. H. (2013). Spotlights,floodlights, and the magic number zero: Simple effects tests in moderatedregression. Journal of Marketing Research, 50(2), 277–288.
Stanovich, K. E., & West, R. F. (2000). Individual differences in reasoning:Implications for the rationality debate? Behavioral and Brain Sciences, 23(5),645–665.
Stubenitsky, K., Aaron, J. I., Catt, S. L., & Mela, D. J. (1999). Effect of information andextended use on the acceptance of reduced-fat products. Food Quality andPreference, 10(4), 367–376.
Swinburn, B. A., Sacks, G., Hall, K. D., McPherson, K., Finegood, D. T., Moodie, M. L.,et al. (2011). The global obesity pandemic: Shaped by global drivers and localenvironments. The Lancet, 378, 804–814.
van Ittersum, K., & Wansink, B. (2012). Plate size and color suggestibility: TheDelboeuf Illusion’s Bias on serving and eating behavior. Journal of ConsumerResearch, 39(2), 215–228.
Verbeke, W. (2006). Functional foods: Consumer willingness to compromise ontaste for health? Food Quality and Preference, 17, 126–131.
Webb, T. L., & Sheeran, P. (2006). Does changing behavioral intentions engenderbehavior change? A meta-analysis of the experimental evidence. PsychologicalBulletin, 132(2), 249–268.
Werle, C. O., Trendel, O., & Ardito, G. (2013). Unhealthy food is not tastier foreverybody: The ‘‘healthy=tasty’’ French intuition. Food Quality and Preference,28(1), 116–121.
Xie, C., Bagozzi, R. P., & Østli, J. (2013). Cognitive, emotional, and socioculturalprocesses in consumption. Psychology & Marketing, 30(1), 12–25.
Yang, H., Carmon, Z., Kahn, B., Malani, A., Schwartz, J., Volpp, K., et al. (2012). Thehot-cold decision triangle: A framework for healthier choices. Marketing Letters,23(2), 457–472.