Embed Size (px)
Citation preview

brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by Elsevier - Publisher Connector
Canadian Association of Radiologists Journal 63 (2012) 5e11www.carjonline.org
Critically Appraised Topic / �Evaluation critique
The Spectrum of Imaging Findings of Brucellosis: A Pictorial Essay
Nizar A. Al-Nakshabandi, MD, FRCPC*
Department of Radiology and Diagnostic Imaging, King Khalid University Hospital, College of Medicine, King Saud University, Riyadh, Saudi Arabia
Introduction
Human brucellosis is a multisystemic disease. The diseaseis caused by a gram-negative coccobacilli of the genusBrucella [1]. There are 4 types of species that cause brucel-losis in humans: Brucella melitensis, found in camels andsheep; Brucella abortus in cattle; Brucella canis in dogs; andBrucella suis in hogs. B. melitensis is the most virulent andinvasive [1]. Brucellosis is endemic in Saudi Arabia.Morbidity in the Saudi population continues to be reportedwith increasing frequency from various regions of the country,particularly in the rural areas. The reported human infectionrange is 1.6%-2.6% [1]. The disease can present in any sex orage with varied manifestation. Any body part can be involved,but the musculoskeletal system, particularly the spine, is mostcommonly affected. Brucellosis remains a huge problem anda public health issue in many regions, particularly in theMediterranean, the Middle East, parts of South and CentralAmerica, and many parts of Western Africa [2]. It has alsobeen reported to have involved multiple organ systems in1 patient in whom there had been Brucella hepatitis,myocarditis, acute disseminate encephalitis, and renal failure,with low attenuating, low agglutinating titers [2].
Brucellosis is an important concern in first-world countriesbecause of issues surrounding immigration and the impact ofthe disease on the economy. The radiologist plays a major rolein raising the suspicion of a brucellosis diagnosis in patientsfrom high-risk demographics in nonendemic countries.
Brucellosis in Saudi Arabia
Morbidity in the Saudi population still continues to bereported, with human infection in the range of 1.6%e2.6%[1]. There was an increase in the rate of annual admission ofbrucellosis in the 1980s [1]. During this period, brucellosis in
* Address for correspondence: Nizar A. Al-Nakshabandi, MD, FRCPC,
Department of Radiology and Diagnostic Imaging (40), King Khalid
University Hospital, College of Medicine, King Saud University, P.O. Box
7805, Riyadh 11472, Saudi Arabia.
E-mail address: [email protected] (N. A. Al-Nakshabandi).
0846-5371/$ - see front matter � 2012 Canadian Association of Radiologists. A
doi:10.1016/j.carj.2010.09.011
animals and humans has been thoroughly linked to theuncontrolled deportation of animals potentially infected withbrucellosis, widespread animal husbandry, and the prevailinghabit among the nomadic population of ingesting raw milk orits products.
There has been a steady increase in the incidence ofBrucellainfections in animals. In 1977, the incidence of brucellosis in thesouthern region had been documented to be 0.8% in goats, 0.5%in sheep, 2.8% in camels, and 3.6% in cows. Ten years later, theincidence rate had gone up to 18.2% in goats, 12.3% in sheep,and 22.6% in camels, and 15.5% in cows [1].
Discussion
Brucellosis can involve various body parts.
The Brain
In brucellosis, the central and peripheral nervous systemsare involved in 3.5%e13% of patients [3]. These patientsusually exhibit symptoms such as headache and neuropsy-chiatric complaints related to neurologic disorders [3].Magnetic resonance (MR) spectroscopy has been used inbrucellosis, because brucellosis may cause subtle cerebralalterations that are only discernible in MR spectroscopybecause of its ability to detect the increased choline-to-creatineratio, which represents an initial phase of inflammation anddemyelination process of brucellosis [3]. Brucellosis in thebrain has been reported to have extensive white matterchanges, particularly on the fluid attenuated inversion recovery(FLAIR) sequences as well as involvement of the meninges.When gadolinium is given, the meninges and the white matterchanges can be enhanced (Figure 1). Other manifestations ofa neurobrucellosis range from cerebral infarction to whitematter changes to peripheral nerve palsies [4,5].
The Spine
Two forms of spinal brucellosis are known: the focal andthe diffuse [6]. In the focal form, the organisms are
ll rights reserved.

Figure 1. (A, B) Axial T1- and T2-weighted image in a 32-year-old woman, showing high signal intensity in the right posterior aspect of right parietal lobe. (C)
Fluid attenuated inversion recovery sequence, showing focal high signal intensity in the same region. (D) Axial T1 after gadolinium infusion, showing focal
enhancement in the white matter and the meninges (arrows).
6 N. A. Al-Nakshabandi / Canadian Association of Radiologists Journal 63 (2012) 5e11
transferred by the hematogenous route and localized in theanterior aspect of the superior end plate, which is known forits rich blood supply. The disks and paraspinal soft tissues atthe level of focal disease are usually within normal limits.Late changes will be definitely identified on bone scans andMR imaging (Figure 2). In diffuse disease, the infection isusually more severe and involves the epidural space at times;even in severe cases, the changes are not usually seen onplain radiographs. MR is usually needed to identify thesechanges, which are identified by areas of loss of signalintensity on T1-weighted images that become hyperintenseon T2-weighted magnetic resonance imaging (MRI)sequences when using a low, long TR and TE, and, aftergadolinium administration, avid enhancement usually occurs(Figure 3) [6,7].
Figure 2. Focal form of spinal brucellosis in a 26-year-old woman with systemic
between L4-L5 and an anterior osteophyte (arrow), sclerosis. (B) Scintigram, show
the anterior view. (C) Fat-suppressed T1-weighted magnetic resonance image (T
gadolinium, showing focal enhancement of the anterior aspect of the superior end
of the L4 and L5 disks (arrow). (Case courtesy of Dr Fatima Abdulla, Manama
Bone scans are an important diagnostic tool for detectingspinal involvement of brucellosis. However, MRI is themethod of choice for diagnosing Brucella spondylodiscitisand gives the added benefit of seeing paraspinal or epiduralabscess involvement, particularly when cord or nervecompression is in question [7].
Diffusion weighted imaging (DWI) has a valuable role indetecting vertebral brucellar spondylodiscitis. DWI isa sensitive and fast sequence that can differentiate acute fromchronic forms of spondylodiscitis, which is at times crucialin imaging the spine [8]. The acute form of brucellosis of thevertebral bodies and end plates will be hyperintense, whereasit will be hypointense in the chronic form on DWI [9].
The issue of differentiating brucellar spondylitis fromtuberculo-spondylitis remains a conundrum. However,
brucellosis and low back pain. (A) Radiograph, showing loss of disk height
ing focal increased uptake in the bodies of L4 and L5. This was seen only on
R was 500 msec; TE was 18 msec [500/18]) obtained after administration of
plate of L4 and L5 (arrows). Also note the enhancement of the anterior aspect
General Hospital, Manama, Kingdom of Bahrain.)

Figure 3. A 60-year-old woman with neck pain and a diffuse form of brucellosis. (A) Sagittal turbo spin echo image, showing destruction of the C5 and C6, and
involvement of the disk space (arrow). (B) Sagittal T1-weighted image with intravenous gadolinium, showing an enhancing mass with destruction of the
vertebral bodies of C5 and C6 as well as enhancement of the disk space (arrow). (C) Coronal weighted image with intravenous gadolinium, showing an
enhancing mass with destruction of the vertebral bodies of C5 and C6 as well as enhancement of the disk space (arrow).
7Imaging findings of brucellosis / Canadian Association of Radiologists Journal 63 (2012) 5e11
multiple reports claim that involvement of the multiplevertebral bodies with the involvement of the disk space andGibbus deformity usually suggests tuberculo-spondylitis [8].In addition, brucellar serology, in most cases by using theagglutination test, is positive in brucellar spondylodiscitisand not often the case in tuberculo-spondylitis.
The Breast
There are at least 7 published cases of brucellar mastitis inthe literature [9]. Brucellar mastitis is not seen primarily inwomen who are lactating but can be seen in women withbreast implants [10]. It is seen on ultrasound as oedema
Figure 4. (A) A 38-year-old non-pregnant woman with right breast redness, tend
showing oedema of the breast consistent with diffuse mastitis and a complex m
(FSPGR) with gadolinium infusion, showing avid enhancement of the oedemato
along the mammary ducts, with abscess formation (Figure4A). MR elegantly demonstrates this oedema and abscessformation, which demonstrates avid contrast enhancement(Figure 4B).
The Musculoskeletal System
Any joint can be involved, with affinity to large joints, butall joints have been involved, including sternoclavicularjoints and sacroiliac joints. Brucella has also been reported tocause avascular nephrosis in the femoral head in long-standing and neglected cases [11,12]. Joints involved ina great majority of patients show an increased uptake on
erness, and a positive Brucella titer. Ultrasound by using a 10-MHz probe,
ass (arrow). (B) The same patient in (A). Fat sat fast spoiled echo gradient
us tissue and mass, extending to the nipple (arrow).
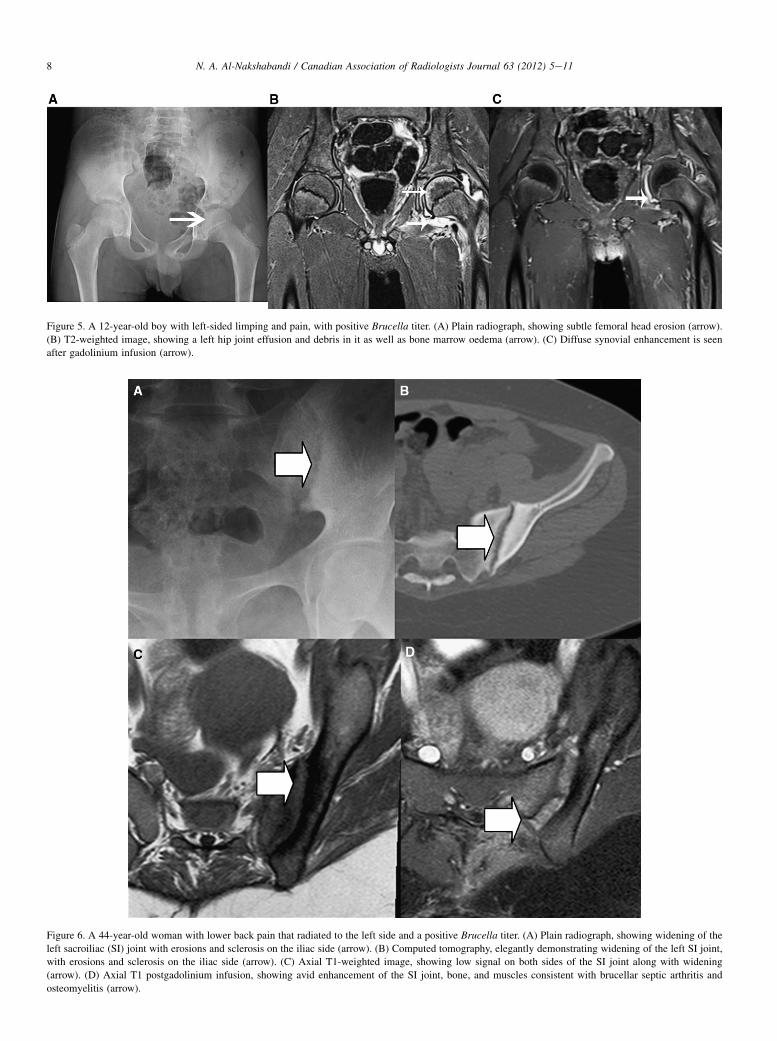
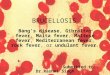
Figure 5. A 12-year-old boy with left-sided limping and pain, with positive Brucella titer. (A) Plain radiograph, showing subtle femoral head erosion (arrow).
(B) T2-weighted image, showing a left hip joint effusion and debris in it as well as bone marrow oedema (arrow). (C) Diffuse synovial enhancement is seen
after gadolinium infusion (arrow).
Figure 6. A 44-year-old woman with lower back pain that radiated to the left side and a positive Brucella titer. (A) Plain radiograph, showing widening of the
left sacroiliac (SI) joint with erosions and sclerosis on the iliac side (arrow). (B) Computed tomography, elegantly demonstrating widening of the left SI joint,
with erosions and sclerosis on the iliac side (arrow). (C) Axial T1-weighted image, showing low signal on both sides of the SI joint along with widening
(arrow). (D) Axial T1 postgadolinium infusion, showing avid enhancement of the SI joint, bone, and muscles consistent with brucellar septic arthritis and
osteomyelitis (arrow).
8 N. A. Al-Nakshabandi / Canadian Association of Radiologists Journal 63 (2012) 5e11
Figure 7. A 39-year-old woman with fever, positive Brucella titer, and
a newly diagnosed murmur. Long-axis transesophageal echo, showing
vegetations on the ventricular surface of the aortic valve (arrow), an aortic
regurgitation, and chamber enlargement as a result. (Case courtesy of Dr
Rajaa Mestady, Riyadh, Saudi Arabia.)
Figure 8. A 50-year-old man with a positive Brucella titer was having
abdominal pain and pulsating abdominal mass. (A) A computed tomography
(CT) of the aorta at the level of a destructed L3, with erosions of the body
and extension of the inflammatory process into the aorta, which caused
a mycotic aneurysm (arrow). (B) Sagittal CT of the same patient, elegantly
showing the extent of destruction and aneurysm formation (arrow). (C, D)
Coronal T2-weighted image of the lumbar spine, showing destruction of the
disk space between L3 and L4, with spread of the phlegmon to the
abdominal aorta, which caused a mycotic aneurysm (arrow). (Case courtesy
of Dr Khalid Alismail, King Faisal Specialist Hospital, Riyadh, Saudi
Arabia.)
Figure 9. A 27-year-old man with brucellosis and abdominal pain. (A) Plain
abdominal radiograph, showing an enlarged liver shadow (arrow). (B)
Coronal T2-weighted image, confirming the plain radiograph suspicion of
hepatomegaly (arrow).
9Imaging findings of brucellosis / Canadian Association of Radiologists Journal 63 (2012) 5e11
bone scans. In addition, an increase of synovial fluid isevident on MRI, with evidence of bone marrow oedema(Figure 5). The joints are presumed to have only a synovialdisease [6]. However, aspiration of the joints almost always

Figure 10. A 33-year-old woman with severe diarrhoea and abdominal pain
after drinking unpasteurized milk. (Arrow A) points to dilated severely
inflamed loop of bowel. (Arrow B) points to ascites and nodular peritonitis.
(Arrow C) points to reactive lymphadenopathy.
Figure 11. A 29-year-old man with testicular pain and a high Brucella titer. (A) Transverse sonogram of the testis, showing an enlarged and predominantly
hypoechoic epididymis, with a reactive hydrocele in a patient with acute epididymitis. (B, C) Colour-flow sonogram, showing increased vascularity in the
epididymis. An enlarged epididymis with increased vascularity in the appropriate clinical setting is diagnostic of acute epididymitis. This figure is available in
colour online at http://carjonline.org/.
10 N. A. Al-Nakshabandi / Canadian Association of Radiologists Journal 63 (2012) 5e11
yields sterile serosanguineous fluid. The sacroiliac joint isanother favorite location for brucellar septic arthritis andosteomyelitis. Sacroiliac joint involvement can extend tobone and muscle involvement in the region [8].
One of the hallmarks of Brucella septic arthritis is that itaffects both joint spaces in the sacroiliac joint and causeserosive and bony destruction of the sacroiliac joint, withenhancement (Figure 6). This feature is similarly seen inpsoriatic gout and arthropathy [13].
The Cardiovascular System
Brucella endocarditis is a rare manifestation of brucellosis[14]; in imaging, usually thickening of the myocardium aswell as vegetation on valves can be seen in cases of endo-carditis (Figure 7) and thickening of the pericardium in casesof pericarditis, with a pericardial effusion. Brucella endo-carditis is a diagnosis based on a positive titer and blood
culture, along with visualization of vegetations on a cardiacvalve [14]. In addition, direct spread of the spinal brucellarphlegmon can encase the major vessels, for example, theaorta, and cause mycotic aneurysms (Figure 8).
The Gastrointestinal System
Brucella can cause local infections in the gastrointestinalsystem, for example, hepatitis that leads to hepatomegaly(Figure 9), cholecystitis, and pancreatitis [15]. Colitis,spontaneous bacterial peritonitis, and adenopathy (Figure 10)have also been reported with Brucella [15].
The Genitourinary System
Scrotal infections are generally diagnosed by clinicalfeatures. Ultrasound and Doppler are helpful in confirming thediagnoses and detecting complications such as abscesses ortesticular torsion [16]. The imaging features of heterogeneity
differences in the testicle and thickening of the scrotum as wellas hydrocele and enlargement of the epididymal head are seenon ultrasound. In addition, Doppler interrogation usuallydemonstrates an increase in flow to the inflamed regions inpatients who have a positive Brucella titer (Figure 11).
Summary
Brucellosis remains a major health and economic problemin some parts of theworld. The radiologist plays amajor role inits diagnosis and management. Brucellosis is an importantconcern in first-world countries because of issues surroundingimmigration and the impact of the disease on the economy.
References
[1] Al Eissa YA. Brucellosis in Saudi Arabia: past, present and future. Ann
Saudi Med 1999;19:403e4.

11Imaging findings of brucellosis / Canadian Association of Radiologists Journal 63 (2012) 5e11
[2] Khorvash F, Keshteli AH, Behati M, et al. An unusual presentation of
brucellosis, involving multiple organ systems, with low agglutinating
titers: a case report. J Med Case Reports 2007;1:53.
[3] Kayabas U, Alkan A, Kemat FA, et al. Magnetic resonance spectros-
copy features of normal-appearing white matter in patients with acute
brucellosis. Eur J Radiol 2008;65:417e20.
[4] Al-Sous MW, Bohlega S, Al-Kawi MZ, et al. Neurobrucellosis:
clinical and neuroimaging correlation. Am J Neuroradiol 2004;25:
395e401.
[5] €Ozkavukcu E, Tuncay Z, Selcuk F, et al. An unusual case of neuro-
brucellosis presenting with unilateral abducens nerve palsy: clinical
and MRI findings. Diagn Interv Radiol 2009;15:236e8.
[6] Al-Shahed MS, Sharif HS, Haddad MC, et al. Imaging features of
musculoskeletal brucellosis. Radiographics 1994;14:333e48.
[7] Pourbagher A, Pourbagher MA, Savas L, et al. Epidemiologic, clinical,
and imaging findings in brucellosis patients with osteoarticular
involvement. AJR Am J Roentgenol 2006;187:873e80.
[8] Jung NY, Jee WH, Ha KY, et al. Discrimination of tuberculous spon-
dylitis from pyogenic spondylitis on MRI. AJR Am J Roentgenol 2004;
182:1405e10.
[9] Oztekin O, Calli C, Adibelli Z, et al. Brucellar spondylodiscitis:
magnetic resonance imaging features with conventional sequences and
diffusion weighted imaging. Radiol Med 2010;115:794e803.
[10] Jensenius M, Hermansen N, Jahr G, et al. Brucellar mastitis: presentation
of a case and review of the literature. Int J Infect Dis 2008;12:98e113.
[11] Benjamin B, Khan MR. Hip involvement in childhood brucellosis.
J Bone Joint Surg Br 1994;76:544e7.
[12] Gedalia A, Howard C, Einhom M. Brucellosis induced avascular
necrosis of the femoral head in a 7 year old child. Ann Rheum Dis
1992;51:404e6.
[13] Dayan L, Deyev S, Palma L, et al. Long standing, neglected sacroiliitis
with remarked sacro-iliac degenerative changes as a result of Brucella
spp. infection. Spine J 2009;9:e1e4.
[14] Yildiz A, Tufekcioglu O, Aras D, et al. Myocardial noncompaction
presenting with Brucella endocarditis. Int J Cardiol 2009;131:e87e9.
[15] Aziz S, Al-Anazi A, Al-Aska A. A review of gastrointestinal mani-
festations of Brucellosis. Saudi J Gastroenterol 2005;11:20e7.
[16] Ozturk A, Ozturk E, Zeyrek F, et al. Comparison of brucella and non-
specific epididymorchitis: gray scale and color Doppler ultrasono-
graphic features. Eur J Radiol 2005;56:256e62.