Embed Size (px)
Citation preview

The role of hysteroscopy in the diagnosis and treatment of
Adenomyosis
Keith Isaacson, MDAssociate Professor Ob/Gyn
Harvard Medical School

Adenomyosis• Endometrial glands and stroma present with
uterine musculature• Can be focal or diffuse• Incidence 20-30% at time
of hysterectomy

Etiology Theories• Invagination of basalis endometrium
– Loss of tissue cohesion– Tissue trauma injury endometrial lining– Aberrant immune phenomenon
• Stimulation of migratory tissue– High expression of estrogen receptor
• De Novo synthesis of ectopic endometriumwithin the myometrium
Bergon. Pathology and physiology of adenomyosis. Best Pract & Research Clin Obstet & Gyn.
Ferenczy. Pathophysiology of adenomyosis. Human Reproduction Update 1998

Etiology Theories• Lymphatic Spread• Stem cell theory
– Endometrial regeneration after bone marrow transplant
Du H, Taylor H. Stem Cell and female reproduction. Reprod Sci 2009
Sasson I, Taylor. Stem Cells and the Pathogenesis of Endometriosis. Ann. N.Y Acad Sci 2008

Pathophysiology
• Is Adenomyosis the same as endometriosis?• What leads to the clinical presentation?
– Menorrhagia– Dysmenorrhea– Infertility?

Descriptive pathophysiology
• Biological properties– Extrauterine sites
• induction of apoptosis vs. constant proliferation– Reduction in Bcl-2 gene expression
• Different hormonal effects: rare secretory phase– Progesterone resistance
– Growth factors and cytokines• BFgf, VEGF, macrophages
Matsumoto. Apoptosis and Ki-67 expression in adenomyotic lesions and in the corresponding eutopic endometrium. Obstet Gynecol 1999
Ota. Is adenomyosis an immune disease? Hum Repro Update. 1998
Propst. Adenomyosis demonstrates increased expression of the basic fibroblast growth factor receptor/ligand system compared with autologous endometrium. Menopause 2001

Diagnosis
HISTOLOGICIAL
HYSTEROSCOPY RADIOLOGICAL IMAGING

Histological Diagnosis• Ectopic endometrial tissue in myometrium• Smooth muscle cell hyperplasia• Posterior wall• Circumscribed nodular aggregates
– 2% endometrial polyps
Azzi R. Adenomyosis: current perspectives. Obstet Gynecol Clin. N. Am. 1989

Histological Criteria
• One low power field• Foci deeper than 25% of myometrial
thickness• Glandular extension >1-3mm
– 2.5mm used in most studies Incidence 5-70% due to classification

Bazot M, et al. Ultrasound compared with MRI for the diagnosis of adenomyosis: correlation with histopathology. Human Reproduction 2001: 16 (11) p 2427-2433

Histological Diagnosis• Hysterectomy• Biopsy
– 5mm loop electrode with hysteroscopy– Cutting needles at time of laparoscopy– Ultrasound guidance biopsy
McCausland A. Hysteroscopic myometrial biopsy: Its use in diagnosing adenomyosis and its clinical applications. Am J Obstet Gynecol 1992
Popp L. Myometrial biopsy in the diagnosis of adenomyosis uteri. Am J Obstet Gynecol. 1993

Hysteroscopy• Irregular endometrium with superficial openings• Irregular subendometrium• Altered vascularity• Intramural cystic hemorrhagic lesion
Molinas C. Office Hysteroscopy and adenomyosis. Best Pract Res Clin Obstet Gynaecol 2006
Fernandez C. Adenomyosis visualized during hysteroscopy. J Minim Invasive Gynecol 2007

Hysteroscopy

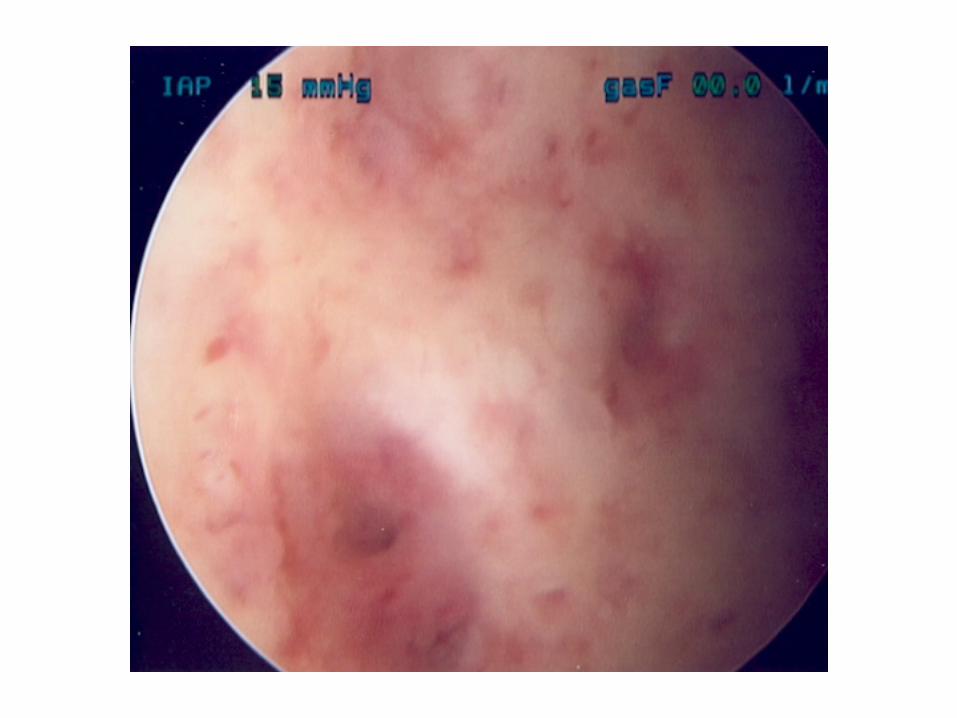

Blood filled cystic lesions
Molinas CR and Campo R
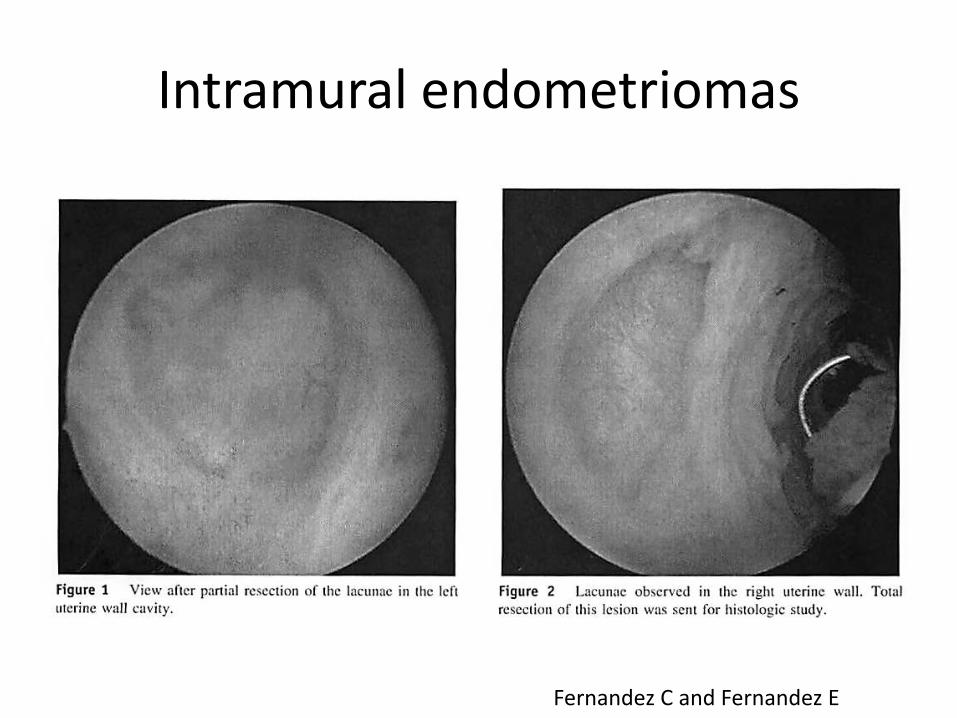
Intramural endometriomas
Fernandez C and Fernandez E

Hysteroscopic biopsy
• McCausland A 1992– 90 patients with menorragia– 50 normal cavities
• 33 (66% with adenomyosis >1 mm)

Hysteroscopic biopsy
• Campo hysteroscope – under development

Hysteroscopic therapy for adenomyosis
McCausland A and McCausland V 1996

Endometrial ablation/resection
• Rollerball electrode– <2mm successful procedures with or without
progesterone therapy– >2mm hysterectomy
• Global ablation– 1.5 increased risk of failure
McCausland A, McCausland V. Depth of endometrial penetration in adenomyosis helps determine outcome of rollerball ablation. Am J Obstet Gynecol 1996
Wood C. Surgical and medical treatment of adenomyosis. Human Reproduction Update 1998
El Nashar S, Prediction of treatment outcomes after global endometrial ablation. Obstet Gynecol 2009





























