Embed Size (px)
Citation preview

Journal of Infection (I992) 25, 39-46
The rapid serological diagnosis o f infect ious m o n o n u c l e o s i s
J. j. Gray,* Jill Caldwellt and Margaret Sill ist
* Clinical Microbiology and Public Health Laboratory, Addenbrooke's Hospital, Cambridge and
t Public Health Laboratory, [Vest Norwich Hospital, Bowthorpe Road, Norwich, U.K.
Accepted for publication 28 November I99I
Summary
A total of i2I samples of serum collected from IOI patients was tested to determine the sensitivity and specificity of a commercial latex agglutination test for detecting infectious mononucleosis heterophile antibody, a commercial immunofluorescence test for detecting antibody to Epstein-Barr virus capsid antigen and a rapid enzyme immunoassay for detecting antibody to Epstein-Barr virus nuclear antigen. Although the Epstein-Barr virus capsid antigen IgM indirect immunofluorescence test proved to be the most sensitive, false-positive reactions were seen when samples collected from patients with cytomegalovirus, hepatitis A virus, parvovirus and leptospira infection were tested. False-positive reactions were also seen with samples containing rheumatoid factor.
Introduction
Infectious mononucleosis (IM), an acute, self-limiting disease characterised by fever, lymphadenopathy and the presence of atypical mononuclear cells in the peripheral blood, is caused by infection with Epstein-Barr virus ( E B V ) . 1
Cytomegalovirus (CMV) and Toxoplasma gondii infections may also produce a mononucleosis. Therefore, any diagnostic test for IM must be able to differentiate the disease from these other infections.
Although the presence of atypical mononuclear cells in the peripheral blood may suggest EBV infection, particularly in young adults, the diagnosis should be confirmed by demonstrating specific antibodies in the patient's serum. The serological diagnosis of IM relies on demonstrating either IgM antibodies to specific EBV antigens or IM heterophile antibody. A rise in IgG antibody may not be detected during the acute phase of the illness since IgG antibody to EBV virus capsid antigen (VCA) usually appears at or soon after the onset of symptoms and IgG antibody to EBV nuclear antigens (EBNA) is not present during the acute phase of the illnessfl
Heterophile antibodies react with surface antigens present on cells of various mammalian species. The IM heterophile antibody reacts with bovine, sheep and horse erythrocytes 3 but does not react with EBV-specific antigens. The Paul-Bunnell test, which detects IM heterophile antibody and includes an adsorption with guinea-pig kidney emulsion to exclude Forssman antibody, is often used for the diagnosis of IM. 4 However, I0--20 °/o adults and > 50 % children under 4 years of age do not produce IM heterophile antibody detectable in the Paul-Bunnell test; some infections may therefore be missed. 5
This study was made in order to determine the sensitivity and specificity of
oi63-4453/9z/o4oo39+o8 $03.00/0 © I992 The British Society for the Study of Infection

40 j . j . GRAY" E T A L .
three commercial assays used for the serological diagnosis of EBV infection. We examined samples of serum, collected from patients with symptoms suggestive of IM, for heterophile antibody by means of the Paul-Bunnell test and a commercial latex agglutination test with purified Paul-Bunnell antigen- coated latex particles (monolatex, biokit, Barcelona--supplied by Launch Diagnostics, Dartford, U.K.). Samples were also tested for the presence of specific antibodies to EBV by means of an immunofluorescence test designed to detect EBV VCA IgM antibody 6 (Gull Laboratories, Utah, U.S.A.) and an E L I S A designed to detect IgM and IgG antibodies to a synthetic peptide (p62) derived from a segment of EBNA-17 (Monolert , Ortho Diagnostics).
Materials and m e t h o d s
S e r u m samples
A total of 92 samples of serum collected from 72 patients with symptoms consistent with infectious mononucleosis was tested for I M heterophile antibody by means of the Paul-Bunnell and latex agglutination tests as well as for EBV VCA IgM and EBNA p62 IgM and IgG. Samples which gave discordant results were tested for EBV VCA IgG and the antibody avidity was determined. 8 The avidity of IgG immediately after the onset of EBV infection is low and increases with the maturat ion of the immune response. Low and high-avidity IgG may be differentiated by incorporating 8 M urea in the antibody assay wash solution. Low-avidity antibody will be eluted from the antigen in the presence of 8 M urea. A further 29 samples, collected from patients with evidence of infection with either T. gondii, CMV, parvovirus, hepatitis A virus, rubella virus or leptospira (infections which may produce symptoms similar to those seen in IM) and five samples known to be rheumatoid factor positive were tested in order to estimate the frequency of non-specific reactions.
EBV serology
All commercial tests were performed according to the manufacturer 's instructions.
P a u l - B u n n e l l test
A I ml volume of guinea-pig kidney suspension (20 %) was centrifuged and the supernatant discarded. A total of I ml of a i in Io dilution of serum in phosphate buffered saline (PBS) (pH 7"2) was added to the deposit, shaken and incubated at room temperature for 5 min. The suspension was centrifuged and doubling dilutions from I in 20 to I in 640 were prepared from the supernatant in Ioo m m × I2 m m tubes in PBS and an equal volume (400 #1) of 2 % sheep red blood cells added. After centrifugation, the red cells were resuspended by flicking the tubes. The antibody titre was expressed as the reciprocal of the highest serum dilution to show macroscopic agglutination.
Latex agglut inat ion test (mono la tex )
A volume of 50/zl undi luted serum was placed on one section of a disposable slide and one drop of Paul-Bunnell antigen-coated latex suspension added. T he serum and latex were mixed and the slide rotated for 3 rain at room
Diagnosis of infectious mononucleosis 4I
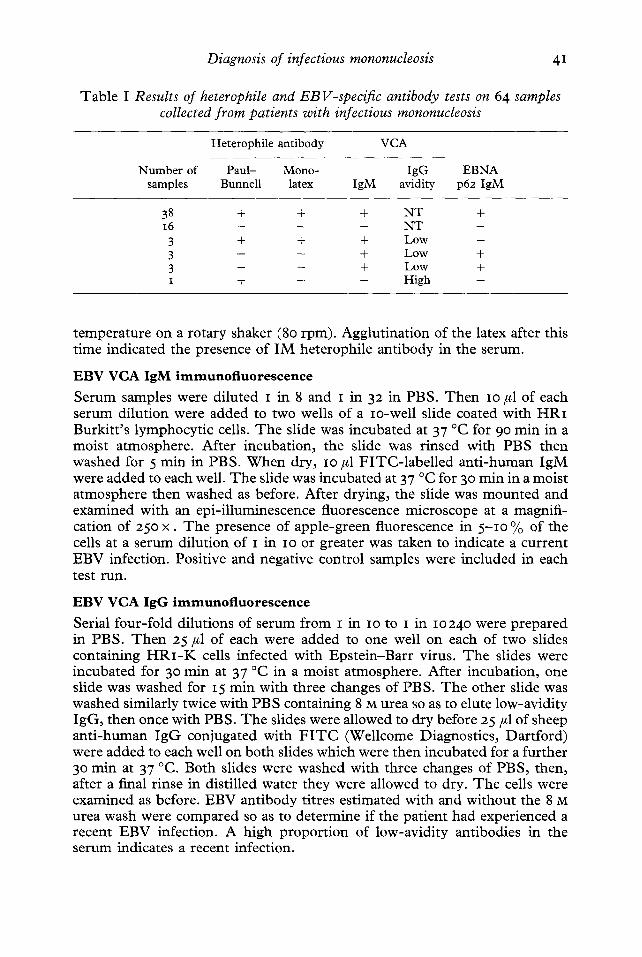
Tab le I Results of heterophile and EBV-specific antibody tests on 64 samples collected from patients with infectious mononucleosis
Heterophile antibody VCA
Number of Paul- Mono- IgG EBNA samples Bunnell latex IgM avidity p62 IgM
38 + + + N T + i6 - - - NT - 3 + + + Low - 3 - + + Low + 3 - - + Low + i + -- - High -
t empera tu re on a rotary shaker (80 rpm). Agglut inat ion of the latex after this t ime indicated the presence of I M heterophi le ant ibody in the serum.
E B V V C A I g M i m m u n o f l u o r e s c e n e e
Serum samples were di luted I in 8 and I in 32 in PBS. T h e n Io #1 of each serum dilut ion were added to two wells of a xo-well slide coated with H R I Burki t t ' s lymphocyt ic cells. T h e slide was incubated at 37 °C for 90 min in a moist a tmosphere . After incubat ion, the slide was r insed with PBS then washed for 5 min in PBS. W h e n dry, Io #1 F I T C - l a b e l l e d an t i -human IgM were added to each well. T h e slide was incubated at 37 °C for 3o min in a moist a tmosphere then washed as before. After drying, the slide was m o u n t e d and examined with an epi- i l luminescence fluorescence microscope at a magnifi- cation of 25o x . T h e presence of apple-green fluorescence in 5 - I o % of the cells at a serum dilut ion of I in Io or greater was taken to indicate a cur ren t EBV infection. Positive and negative control samples were included in each test run.
E B V V C A IgG i m m u n o f l u o r e s c e n c e
Serial four- fo ld dilutions of serum f rom I in Io to I in 10240 were p repared in PBS. T h e n 25 #1 of each were added to one well on each of two slides containing H R I - K cells infected with Eps t e in -Bar r virus. T h e slides were incubated for 30 min at 37 °C in a moist a tmosphere. After incubat ion, one slide was washed for I5 min with three changes of PBS. T h e other slide was washed similarly twice with PBS containing 8 M urea so as to elute low-avidi ty IgG, then once with PBS. T h e slides were allowed to dry before 25 #1 of sheep an t i -human I g G conjugated with F I T C (Wellcome Diagnostics, Dar t ford) were added to each well on both slides which were then incubated for a fu r ther 30 min at 37 °C. Both slides were washed with three changes of PBS, then, after a final rinse in distilled water they were allowed to dry. T h e cells were examined as before. EBV ant ibody titres est imated with and wi thout the 8 M urea wash were compared so as to de termine if the pat ient had exper ienced a recent EBV infection. A high p ropor t ion of low-avidi ty antibodies in the serum indicates a recent infection.

4 2 J . J . GRAY E T A L .
Anti -EBNA-, IgM and IgG ELISA (Monolert)
A volume of 5o #1 serum was added to an equal volume of diluent in each of two wells on a peptide-coated paddle. The paddle was incubated for 2 rain at room temperature then washed by immersion in a washing bath. The paddle was blotted in order to remove excess washing solution and two drops of anti- human IgM monoclonal antibody conjugated to horseradish peroxidase (HRP) were added to one well (M well) while two drops of ant i -human IgG monoclonal antibody conjugated to H R P were added to the other well (G well). After incubation for 2 rain at room temperature, the paddle was washed as before and two drops of 2,2'-azino-di (3-ethylbenzthiazoline-sulphonate) containing hydrogen peroxide were added to each well. The paddle was incubated for a further 2 rain at room temperature before the colour intensity in both wells was compared. A colour in the M well more intense than that seen in the G well indicated an acute or current EBV infection.
Results
Samples from IM patients
A total of 54/64 (84"4 %) single samples collected from patients with IM gave concordant results in all four tests. Evidence of recent EBV infection was found in 38 samples while i6 were negative. Of the remaining 1o samples, three (4"7 %) were Panl-Bunnell , latex agglutination and VCA IgM positive but EBNA IgM-negative, three (4"7 %) were Paul-Bunne11 negative but latex agglutination, VCA IgM and EBNA IgM positive, three (4 '7%) were Pau1-Bunne11 and latex agglutination negative but VCA IgM and EBNA IgM positive. One (v6 %) was Paul-Bunne11 positive but latex agglutination, VCA IgM and EBNA IgM negative (Table I).
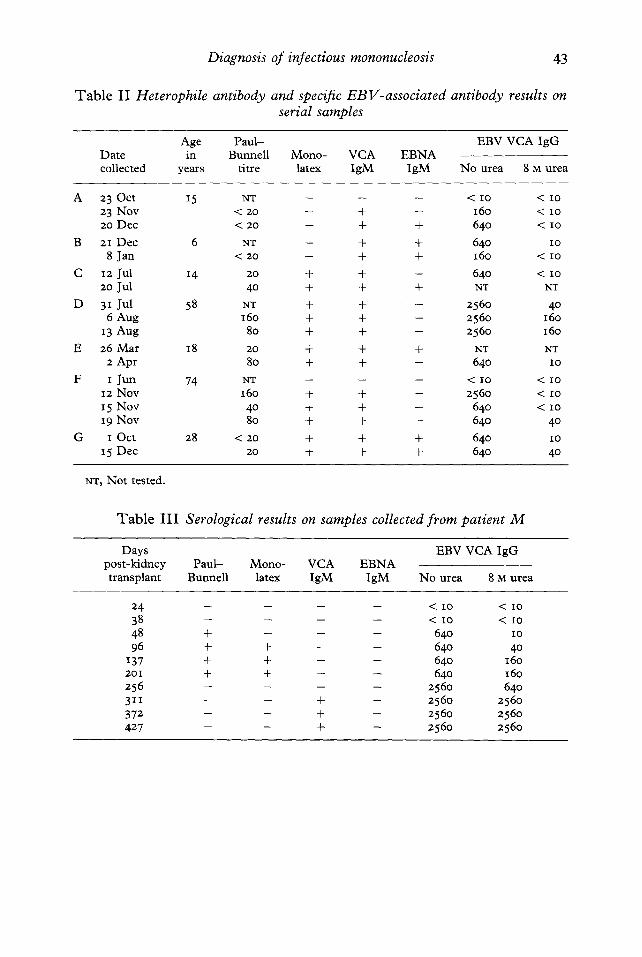
The results of tests performed on serial samples collected from seven patients are shown in Table II. Concordant results in all four assays were obtained in at least one serum sample collected from each of the patients C, E and G. Two patients (A and B) did not have detectable heterophile antibody although results from all other tests indicated recent infection. Samples from two patients (D and F) did not have detectable EBNA IgM although all other tests indicated a recent infection.
EBV VCA IgG antibody tests performed on samples collected from patient M, a kidney transplant recipient, who presented with fever and slight tenderness of the liver 32 days post-transplant, indicated a primary EBV infection less than 48 days post-transplant. This was confirmed by the antibody avidity test. A sample collected on day 48 was Paul-Bunnell positive and one collected on day 96 was monolatex-positive. EBV VCA IgM was not detected until day 311 and EBNA IgM was not detected up to 427 days post- transplant (Table III) .
Non-specific reactions
A total of 3 /4 samples containing CMV IgM antibody and I /5 with rheumatoid factor gave EBNA IgM false-positive results; 2/5 with human parvovirus IgM, 3/5 with hepatitis A IgM and I /5 with leptospira antibody
Diagnosis of infectious mononucleosis 43
Table II Heterophile antibody and specific EBV-associated antibody results on serial samples
A g e P a u l - E B V V C A I g G
D a t e i n B u n n e l l M o n o - V C A E B N A
c o l l e c t e d y e a r s t i t r e l a t ex I g M I g M N o u r e a 8 M u r e a
A 2 3 O c t t 5 N T - - - - - - < I O < I O
2 3 N o v < 20 - + - i 6 o < i o
2 o D e c < 2 0 - + + 640 < i o
B 21 D e c 6 NT -- + + 640 IO 8 J a n < 20 - - + + 16o < IO
C IX Ju l 14 20 + + - 640 < IO
2o J u l 40 + + + NT NT
D 3 1 J u l 58 NT + + -- 2560 4 ° 6 A u g 16o + + -- 256o 16o
I 3 A u g 8o + + - 256o 16o
E 2 6 M a r 18 20 + + + N T N T
2 A p r 8o + + - 640 IO
F I J u n 74 NT - - -- -- < IO < IO
I x N o v 16o + + - 256o < IO
I 5 N o v 4 ° + + - 64o < IO
I 9 N o v 8o + + - 64o 4 °
O I O c t 28 < 20 + + + 640 IO
I 5 D e c 2o + + + 640 4o
NT, N o t t e s t ed .
Table III Serological results on samples collected from patient M
D a y s
p o s t - k i d n e y P a u l - M o n o - V C A E B N A
t r a n s p l a n t B u n n e l l l a t e x I g M I g M
E B V V C A I g G
N o u r e a 8 M u r e a
24 . . . . < IO < IO
38 . . . . < IO < IO
48 + -- -- -- 640 i o
96 + + -- -- 64o 4o I 3 7 + + -- -- 64o i 6 o 2 o i + + -- -- 640 i 6 o
z56 . . . . 256o 64o
3 I I -- -- + - 2560 256o
372 -- - + -- 256o 256o
427 -- - + - 256o 256o
44 j . j . GRAY E T A L .
gave false-positive results in the latex agglutination test while all five samples containing rheumatoid factor gave false-positive results in the VCA IgM immunofluorescence test.
Discuss ion
T he detection of heterophile antibody by means of the Paul-Bunnell test has been the method of choice in many laboratories for the serological diagnosis of IM. Since many children and some young adults, however, do not produce heterophile antibodies after infection with EBV this test has obvious limitations. In this study, detectable EBV VCA IgM and the presence of low- avidity EBV VCA IgG, as indicated by a ~> eight-fold reduction in antibody titre, were used to define a recent EBV infection.
The detection of EBV VCA IgM as a marker of acute or recent infection may be influenced by the presence of EBV VCA IgG3 This antibody may reach maximum titre at or soon after the onset of symptoms and compete with the specific IgM for the available antigen sites on infected cells used in the immunofluorescence test. This competit ion may lead to false-negative EBV VCA IgM results. EBV VCA IgG may also allow the at tachment of IgM anti- IgG rheumatoid factor which, if present in the patient 's serum, will lead to false-positive results. 9
The EBV VCA IgM immunofluorescence test was the most sensitive (Ioo.o %) test used although VCA IgM was detected late after infection in serum collected from the kidney transplant patient (M). The specificity, which was IOO.O % when used to test the serum of patients with I M was reduced to 73"9 % when the results from tests on n o n - I M samples were included. This problem of reduced specificity, caused by the presence of rheumatoid factor may be reduced or eliminated by adsorbing and removing the rheumatoid factor when aggregated IgG or by separating the IgG and IgM serum fractions by chromatography. TM
Heterophile antibody and IgG-avidity tests indicated that patient M experienced an EBV infection approximately 48 days after transplant, but EBV VCA IgM was not detected in the patient 's serum until day 3I I . Al though this may be due to EBV-specific IgG antibody blocking the at tachment of EBV-specific IgM, EBV VCA IgM was not detected even after adsorption with ant i -human IgG (GuUSORB). Ho e t al . 11 reported atypical serological responses to EBV infection in immunosuppressed patients, only 5o % patients with a primary infection having detectable EBV VCA IgM.
Although antibodies to EBNA, detected by ant icomplement immuno- fluorescence, 12 do not appear until the convalescent phase of the disease, an early IgM response to EBNA-specific peptide (p62) has been demonstrated in both heterophile-positive and heterophile-negative I M patients. 1~
The sensitivity and specificity of the EBNA p62 IgM E L I S A for detecting antibodies in serum collected from patients with I M was 9I'6 and IOO'O% respectively. A total of 5/55 patients, with evidence of recent EBV infection, had no detectable EBNA p62 IgM. Four n o n - I M samples were EBNA p62 IgM positive; one was rheumatoid factor positive and three were CMV IgM antibody-positive.

Diagnosis of infectious mononucleosis 45
The latex agglutination test uses a highly purified Paul-Bunnell antigen derived from bovine red cell membranes. The purification should reduce the need for differential adsorption with guinea-pig kidney emulsion necessary in the Paul-Bunnel l test.
When testing samples collected from patients with IM, the latex ag- glutination test was more sensitive (sensitivity 9I-6 %) than the Paul-Bunnell test (sensitivity 87'3 %). False-positive results were not detected in the latex agglutination test giving a specificity of Ioo.o % compared to 94"8 % in the Paul-Bunnel l test for which there was one false-positive result. In contrast, when the latex agglutination test was used to test samples from n o n - I M patients, there were 3/5 false-positive results in respect of samples from patients with recent hepatitis A infection, 2/5 for those with parvovirus infection and I /5 for those with leptospirosis. There were no false-positive Paul-Bunnel l test results in the n o n - I M group. A total of 5/54 (9"3 %) patients with acute EBV infection did not produce detectable heterophile antibody.
A total of seven samples, three EBV IgM positive, two parvovirus IgM positive and two HAV antibody-positive, which were positive in the latex agglutination test, were adsorbed with guinea-pig kidney emulsion. The three EBV VCA IgM positive samples remained positive after adsorption but the other samples were negative when retested in the latex agglutination test. Therefore, false-positive reactions seen in the latex agglutination test may be caused by Forssman antibody in the samples. This antibody is removed in the Paul-Bunnel l test by adsorption with guinea-pig kidney emulsion and although this adsorption is not included in the latex agglutination test protocol, the number of false-positive reactions may be reduced by its inclusion.
This study demonstrates differences in sensitivity between tests that detect I M heterophile antibody and those that detect specific EBV-associated antibodies as well as differences in specificity among tests. The false-positive reactions seen in the EBV VCA IgM immunofluorescence test, caused by rheumatoid factor, may be prevented by pre-treating samples to remove this antibody. The non-specific reactions in the EBNA IgM test, however, can be overcome only by excluding the presence of IgM antibodies to other pathogens. Matheson et al. 1~ reported false-positive reactions in serum samples collected from patients with adenovirus, CMV and Toxoplasma gondii infections when they were tested for EBNA IgM by means of this assay.
Al though detecting heterophile antibody for the diagnosis of EBV infection has its limitations, the latex agglutination test (monolatex) is rapid, technically simple and more sensitive than the Paul-Bunnel l test. When a definitive diagnosis is required, specific EBV antibodies as well as I M heterophile antibody should always be sought.
R e f e r e n c e s
I. Henle G, Henle W, Diehl V. Relation of Burkitt turnout associated herpes-type virus to infectious mononucleosis. Proc Natl Acad Sci USA I968 ; 59: 94-Ioi.
2. Crawford DH, FAwards JMB. Epstein-Barr virus. In: Zuckerman AJ, Banatvala JE, Pattison JR, Eds. Principles and practice of clinical virology. London : John Wiley and Sons, I987: zIZ-I33. ..

46 j . j . GRAY ET AL.
3. Paul JR, Bunnell WW. The presence ofheterophile antibodies in infectious mononucleosis. Am J Med Sci I932; 183:9o-IO4 .
4. Davidsohn I. Serologic diagnosis of infectious mononucleosis. J A M A I937; lO8 : 289-295. 5. Sumaya CV. Infectious mononucleosis and other EBV infections: diagnostic factors. Lab
Manag 1986; 24: 37-45. 6. Henle W, Henle G, Horwitz CA. Epstein-Barr virus specific diagnostic tests in infectious
mononucleosis. Hum Pathol I974; 5:551-565 • 7. Rhodes G, Carson DA, Valbracht J, Houghton R, Vaughan JH. Human immune responses
to synthetic peptides from the Epstein-Barr nuclear antigen. J Immunol I985; 134: 211-216.
8. Gray JJ, Wreghitt TG. Immunogl0bulin G avidity in Epstein-Barr virus infection in organ transplant recipients. Serodiag Immunother Infect Dis 1989; 3: 389-393-
9- Henle G, Lennette ET, Alspaugh MA, Henle W. Rheumatoid factor as a cause of positive reactions in tests for Epstein-Barr virus-specific IgM antibodies. Clin Exp Immunol 1979; 36: 415-422.
IO. Sumaya CV, Ench Y, Carrillo MA, Pope RM. Use of a simple separation column in detection of immunoglobulin M antibody to Epstein-Barr virus. J Clin Microbiol 1984; 2 o :
298-299. II. Ho M, Miller G, Wayne Atchison R et al. Epstein-Barr virus infections and DNA
hybridization studies in posttransplantation lymphoma and lymphoproliferative lesions: the role of primary infection. J Infect Dis 1985; 152: 876-886.
12. Henle G, Henle W, Horwitz CA. Antibodies to Epstein-Barr virus-associated nuclear antigen in infectious mononucleosis. J Infect Dis 1974; 13o: 231-239.
13. Smith RS, Rhodes G, Vaughan JH, Horwitz CA, Geltosky JE, Whalley AS. A synthetic peptide for detecting antibodies to Epstein-Barr virus nuclear antigen in sera from patients with infectious mononucleosis. J Infect Dis 1986; 154: 885-889.
14. Matheson BA, Chisholm SM, Ho-Yen DO. Assessment of rapid ELISA test for detection of Epstein-Barr virus infection. J Clin Pathol 199o; 43: 691-693.












![WORKSHOP SESSIONS DAY 2(October 29[Mon]) · Institute of Infectious Diseases W2-2-08 Oral Neomycin prevents hepatitis of severe infectious mononucleosis-like disease in murine](https://img.dokumen.tips/doc/110x75/6033401d452e3a74a96d5ee1/workshop-sessions-day-2ioctober-29moni-institute-of-infectious-diseases-w2-2-08.jpg)