Embed Size (px)
Citation preview

Restoring the NHS in England as an accountable public service
The proposed
NHS Reinstatement Bill
The proposed National Health Service Reinstatement Bill explained and set out in
this document has been drafted by Peter Roderick with the assistance of Professor
Allyson Pollock, having benefitted from discussions with individuals and
organisations concerned about the increasing role of the market over the last
twenty five years in the NHS in England.
We wish to consult on the Bill with those who share our concern and commitment to
reinstating fully the NHS as an accountable public service as smoothly as possible and
with only a minimal and exceptional role for commercial companies.
Responses can be sent to either or both of us by 15th
December 2014.
Peter Roderick Professor Allyson Pollock
[email protected] [email protected]
Centre for Primary Care and Public Health, Queen Mary, University of London
29th
August 2014

2
Brief summary of the Bill
In short, the Bill proposes to reverse 25 years of marketization in the NHS by abolishing the
purchaser-provider split, re-establishing public bodies and fully restoring the NHS in England
as an accountable public service. It draws on some of the best examples of NHS
administration over its history, retains some features of the 2012 reforms and would be
implemented on a timescale determined by the Secretary of State.
It would:
• reinstate the government’s duty to provide the NHS in England,
• re-establish NHS England as a special health authority with regional committees and
modified functions,
• re-establish District Health Authorities, with Family Health Services Committees to
administer arrangements with GPs, dentists and others,
• abolish marketised bodies such as NHS trusts, NHS foundation trusts and clinical
commissioning groups, as well as Monitor, the regulator of NHS foundation trusts
and commercial companies,
• end virtually all commissioning and allow commercial companies to provide services
only if the NHS could not do so and otherwise patients would suffer,
• abolish competition,
• re-establish Community Health Councils to represent the interest of the public in the
NHS,
• stop licence conditions taking effect which have been imposed by Monitor on NHS
foundation trusts and that will have the effect of reducing by April 2016 the number
of services that they currently have to provide,
• bring the terms and conditions of staff employed in providing NHS services under the
NHS Staff Council,
• prohibit ratification of the Transatlantic Trade and Investment Partnership and other
international treaties without the approval of Parliament (and the devolved bodies)
if they would cover the NHS.
Many further and consequential amendments would also be necessary, for example relating
to public health and GP services, and these are currently covered in Schedules to the Bill.
Part 1 of this document explains the clauses of the Bill. Part 2 provides background notes on some of
the Schedules (page 11 onwards). Part 3 sets out the Bill (page 20 onwards).

3
Part 1: Clause-by-Clause summaries
Clause 1 – Secretary of State’s duties to promote and provide a comprehensive health
service
Clause 1(1) would reinstate the Secretary of State’s legal duty to provide the NHS in
England. It would do so by effectively repealing the abolition of that duty as a result of
section 1 of the Health and Social Care Act 2012, and by reproducing the corresponding
provision that applied from 1946 until 2006.
Until 2006, the government’s overarching duty had been “to provide or secure effective
provision” of services. The NHS Act 2006 deleted the word “effective”, and also de-coupled
this duty from the duty to “promote” a comprehensive service.
The title of section 1 of the 2006 Act ("Secretary of State's duty to promote health service")
would revert to the title of section 1 of the National Health Service Act 1977, which made no
distinction between the connected duties of promotion and provision.
Clause 2 - Abolition of the duties of autonomy
This clause would repeal the two sections inserted into the 2006 Act which require the
Secretary of State and the NHS Commissioning Board, respectively, to have regard to the
desirability of securing, so far as consistent with the interests of the health service, that any
other person exercising functions in relation to the health service or providing services for
its purposes is free to exercise those functions or provide those services in the manner that
it considers most appropriate, and that unnecessary burdens are not imposed on any such
person. These duties are incompatible with a national health service which the Secretary of
State would, under this Bill, again have the duty to provide.
However, certain elements of section 1D of the 2006 Act in relation to the Secretary of
State’s power of directions would be retained under Clause 12 of the Bill.
Clause 3 - Secretary of State's duty to provide certain services
This clause would insert a new section 3 into the NHS Act 2006.
The new section 3(1) would set out the four basic categories of services that it would be the
Secretary of State’s duty to provide or secure the effective provision of:
• the long-standing duty to provide the services listed in new subsection (see new
section 3(2));
• functions relating to high security psychiatric services (see Clause 4);
• duties and powers relating to provision of medical, dental, ophthalmic and
pharmaceutical services (see Parts 4-7); and
4
• functions in relation to other services, for example as regards school children and
blood supplies (see Schedule 1 of the 2006 Act, as amended by Schedule 1 of this
Bill).
The new section 3(2) would reinstate the duty of the Secretary of State to provide
“throughout England” hospital accommodation, services and facilities as in section 3(1) of
the 2006 Act, re-applying the duty as it was before the 2012 Health and Social Care Act. This
would replace the current duty on clinical commissioning groups (CCGs) to arrange provision
for persons for whom they are responsible, and CCGs would be abolished (see Clause 13).
Clause 4 - High security psychiatric services
This would re-establish the Secretary of State’s duty to provide high security psychiatric
hospitals and services under section 4(1) of the NHS Act 2006. The duty would also extend
to maintaining the same, as under the 1977 NHS Act (but which was dropped under section
41 of the Health Act 1999).
Clause 5 (and Schedule 1) - Other services
Schedule 1 of the 2006 Act set out a number of additional services in relation to which the
Secretary of State had obligations, dating back to the 1977 Act and even, in some instances,
the 1946 Act. They covered medical inspection of pupils, contraceptive services, vehicles for
disabled persons, a microbiological service and research. The 2012 Act added provisions
relating to the weighing and measuring of children and the supply of blood and human
tissue.
The obligations for most of these services would revert to the Secretary of State.
Background information on these services is provided below in Part 2.
Clause 6 - Public health functions of the Secretary of State and local authorities
The 2012 Act created public health functions as a new category of services divided between
the Secretary of State and local authorities. Neither of these bodies now have duties to
provide or to secure provision or to make arrangements for provision as regards public
health, only a metaphorically-expressed duty to “take steps” as they consider “appropriate”
for protecting the public from disease or other health dangers or for improving the health of
people. The Bill needs to address these functions (hence the envisaged Schedule 2),
including, for example, whether there is a need to re-establish a health promotion body.
More information is provided below in Part 2.
Clause 7 - Distribution of functions
This Clause would re-establish NHS England as a Special Health Authority – its form before
the 2012 Act - with Regional Committees, along with District Health Authorities (having
Family Health Service Committees).

5
Clause 8 - NHS England and Regional Committees
The National Health Service Commissioning Board – the current NHS England’s formal name
– would be abolished and replaced by The National Health Service England Authority to be
called “NHS England”. It would have a number of Regional Committees covering the whole
of England, and Schedule 3 would provide details of its establishment.
Clause 8(4) would set out the main duty of NHS England. This would be to exercise on behalf
of the Secretary of State some of his duties under the National Health Service Act 2006, by
providing or securing effective provision of the services or facilities referred to in subsection
(5) in accordance with regulations.
The specific services and facilities listed in subsection (5) are those for which the current
NHS England may be required to make arrangements in accordance with regulations under
section 3B of the 2006 Act - dental services; services or facilities for members of the armed
forces, their families or prisoner – as well as others that may be prescribed if more
appropriate for NHS England to provide or secure effective provision of rather than the
Secretary of State or District Health Authorities (or their Family Health Services
Committees). In deciding whether it would be appropriate, the Secretary of State would
have to have regard to the same matters as currently under section 3B(3) and (4).
NHS England would perform its functions through its Regional Committees, save to the
extent that regulations provide otherwise; and regulations could provide otherwise where
the Secretary of State considers that provision is more appropriate on a national basis
rather than on regional bases.
Three preconditions are set out in Clause 8(12), which are intended to have the effect of
entitling NHS England to arrange for service provision outside the NHS exceptionally – but
necessarily to meet all reasonable requirements.
Clause 12 of the Bill covers directions to NHS England.
Clause 9 - District Health Authorities
Under Clause 9, District Health Authorities (DHAs) would become the heart of NHS services
on the ground. They would have the duty to exercise on behalf of the Secretary of State his
duty in section 1(1) of the National Health Service Act 2006 by exercising his or her functions
under specified provisions of that Act, including hospital and other accommodation;
medical, dental, nursing and ambulance services; facilities for the care of expectant and
nursing mothers and young children; facilities for the prevention of illness and the aftercare
of persons who have suffered from illness; and services under Schedule 1 of the 2006 Act
and Schedule 5 of this Bill. So for example, hospitals currently run by NHS trusts and NHS
foundation trusts (which would be abolished) would be transferred to the DHAs.
As for NHS England, DHAs would only be able to arrange for service provision outside the
NHS exceptionally; and would be subject to directions under Clause 12.
6
Schedule 4 of the Bill would set out the basis for the constitution, membership etc. of DHAs,
and the basis for their boundaries needs consultation. The relationship of these boundaries
with those of local government (often referred to as ‘co-terminosity’) will be particularly
important in ensuring the closest cooperation between health and social services.
Schedule 5 would set out the many other functions that were necessarily part of the
Secretary of State’s functions for the running of the NHS, and the list will be finalised after
consultation.
Each DHA would have a Family Health Services Committee having the functions set out in
Clause 10.
Clause 10 - Family Health Services Committees
The duty of each Family Health Services Committee would be, in accordance with
regulations, to administer on behalf of the DHA the arrangements made under Parts 4-7 of
the National Health Service Act 2006 for the provision of medical, dental, ophthalmic and
pharmaceutical services for the district of the Authority, and to perform such other
functions relating to those services as may be prescribed.
Schedule 4, Part 2 makes further provision in respect of Family Health Services Committees
and the discharge of their functions. Background information on the current legal provisions
for medical services is set out in Part 2 below of this document.
Clause 11 - Special health authorities
Clause 11 makes clear that the Secretary of State retains full powers to establish Special
Health Authorities for performing any functions which he may direct the body to perform on
his behalf, or on behalf of NHS England or DHAs. This would be a possible approach to
provide planning for cities such as London, as an alternative, for example, to city-based and
enhanced local government representation on Regional Committees of NHS England.
Section 28A of the National Health Service Act 2006 is repealed, as this limits the duration of
new Special Health Authorities to a maximum period of three years.
Clause 12 – Directions
This clause would give the Secretary of State a general power of giving directions to NHS
England, a DHA, including any Family Health Services Committee, a Special Health Authority,
the National Institute for Health and Care Excellence, the Health and Social Care Information
Centre, and any other persons who are exceptionally providing other prescribed services.
However, this power would not usually be unrestricted. The Secretary of State would be
obliged to have regard to the desirability, so far as consistent with the interests of the
health service and relevant to the exercise of the power in all circumstances, of protecting
and promoting the health of patients and the public, and of the bodies being free to
exercise their functions in the manner that they consider best calculated to promote the
NHS.

7
These directions must be contained in regulations, except in a genuine emergency, so that
the exercise of executive power would be open to Parliamentary scrutiny and procedure.
This provision is a modified version of the duties of autonomy (the hands-off clauses)
introduced by the 2012 Act and which would be abolished by Clause 2.
Clauses 13 – 16 - Abolition of bodies, and staff transfer
Clauses 13 - 15 (and Schedule 6) would make provision for abolishing CCGs, NHS trusts and
NHS foundation trusts. Their property, rights and liabilities would transfer to the Secretary
of State, or to any other NHS body determined by him or her, such as DHAs. Clauses 13(5),
14(5) and 15(4) require regard to be had by the Secretary of State to Schedule 8 in
connection with the abolition of these bodies in order to ensure as smooth a transition as
possible in returning to a fully restored NHS.
Clause 16 would require the Secretary of State, after consultation with trade unions, to
make regulations which would set out the terms and conditions applying to the transfer of
staff from NHS trusts, NHS foundation trusts and CCGs to DHAs, NHS England and other NHS
bodies. These include entitlement to redundancy payments, particularly for senior staff
whose job loss is technical rather than real.
Clause 17 - Community Health Councils
This clause (with Schedule 7) would re-establish Community Health Councils, with the duty
of representing the interests of the local public in the health service. These were initially
established under section 9 of the NHS Reorganisation Act 1973, and were abolished in
England by section 22 of the NHS Reform and Health Care Professions Act 2002.
Clauses 18 and 19 - Abolition of Monitor, transfer to the CQC and Competition
Clause 18 would abolish Monitor, which currently regulates NHS foundation trusts and
licenses commercial companies and voluntary organisations. Many of its functions,
particularly those relating to competition under sections 72-80 of the 2012 Act, would also
be abolished. Those remaining would transfer to the Care Quality Commission (CQC).
The National Health Service (Procurement, Patient Choice and Competition) (No. 2)
Regulations 2013 (SI 2013 No. 500) would be repealed.
Currently, there is no objective underpinning Monitor’s (and under this Bill after transfer the
CQC’s) powers and duties – unlike Ofgem, for example. This Clause would make clear that
the end to which its residual functions under the 2012 Act must be directed is the
comprehensive health service that it is the Secretary of State’s duty to promote and provide
as a service of social solidarity based on cooperation.
By inserting into the 2012 Act a new section 61A(2) and by repealing section 62(9), the duty
of Monitor to act consistently with the Secretary of State’s duties to promote and provide
would be reinstated (and transferred to the CQC). Parliament had imposed that duty on
Monitor both in section 32 of the 2006 Act and in section 3 of the Health and Social Care

8
(Community Health and Standards) Act 2003 (although in those enactments Monitor’s duty
also extended to acting consistently with the Secretary of State’s duty in relation to
university clinical teaching and research). The 2012 Act, in section 62(9), only imposed a
duty on Monitor in relation to the duty to promote under section 1(1) of the 2006 Act,
hence its proposed repeal under this Clause.
Clause 20 Continuity of mandatory services
Monitor has imposed licence conditions on NHS foundation trusts under which currently
mandatory services - basically those which had to be provided, under the old NHS
foundation trust authorisation system - will cease to be mandatory after April 2016, and a
new set of mandatory services will be put in place. Under its associated guidance issued in
March 2013, Monitor asks commissioners to consider the current list, and states that it
expects the number of mandatory services to decrease as a result. Clause 20 would have the
effect of annulling these licence conditions.
Clause 21 National terms and conditions
This Clause is intended to ensure that the UK-wide ‘Agenda for Change’ system under the
auspices of the non-statutory NHS Staff Council that has been in place since 2004 would
apply to all staff employed by those who provide NHS services, regardless of whether the
employer is in the public, commercial or voluntary sector. Currently this system only applies
to NHS trusts, NHS Foundation Trusts, Special Health Authorities, NHS England, CCGs, The
Health and Social Care Information Centre and NICE. Recognising the NHS as a national
service and the desirability of staff being able to move freely between its constituent parts
without suffering detriment would help ensure fairness, equity and equal value for NHS staff
and good patient care. This Clause would not affect those staff not currently covered by the
Agenda for Change system such as hospital doctors and dentists and very senior managers.
Clause 22 – Treaty requirements
25. This Clause follows the spirit of the example of section 6 of the European Assembly
Elections Act 1978 which provided for any increase in the powers of the Assembly, now
called the European Parliament, to be ratified by the United Kingdom only if there had been
prior approval by an Act of Parliament.
26. The Clause would make it impossible for any trade, investment or similar international
agreement – such as the proposed Transatlantic Trade and Investment Partnership (TTIP)
being negotiated between the European Union and the US - in effect to legislate for the NHS
without Parliament (or the relevant devolved legislature) giving its approval prior to
signature or agreement.
Clause 23 - Commencement and transitional arrangements
Clause 23 gives flexibility to the Secretary of State in the way in which the Act, except for
section 1, is brought into effect; and thus the timescale for its implementation. How this
flexibility would be exercised in practice would depend on considering the impact of a

9
further major reorganisation on the appointed day necessary to reinstate the NHS (on the
one hand) and the undesirability of giving vested interests a post-enactment opportunity to
delay implementation (on the other). Transitional arrangements would be set out in
Schedule 8 in order to ensure as smooth a transition as possible in returning to a fully
restored NHS, and Clauses 13(5), 14(5) and 15(4) require regard to be had by the Secretary
of State to Schedule 8 in connection with the abolition of CCGs, NHS trusts and NHS
foundation trusts.

10
Part 2: Schedules - Background Notes
Preliminary
Schedules have been included in the Bill in order to indicate the nature and range of
supplementary issues, transitional and consequential amendments and repeals entailed by a
new Bill. Many of the matters covered could be dealt with in a separate “NHS
(Consequential Provisions) Bill” that would be enacted simultaneously, as happened in 2006.
Some of the “standard” type of Schedules – such as those covering organizational aspects
for NHS England and its Regional Committees (Schedule 3), DHAs (Schedule 4) and
Community Health Councils (Schedule 7) – currently have no content, or indicative content
based on previous legislation.
Amongst the Schedules dealing with services are those relating to the Secretary of State and
other services (Schedule 1), Public Health (Schedule 2) and further functions of the DHAs
(Schedule 5).
Modifications to the provisions and functions relating to medical, dental, pharmaceutical
and ophthalmic services are currently envisaged in Schedule 9, Part 1. After consultation at
least some of these may be relocated to the main body of the Bill.
The notes below provide some background information to assist consideration of the
contents of Schedule 1 and 2 and of Schedule 9, Part 1 as regards medical services.
11
Schedule 1 (Further provision about the Secretary of State and services) and Schedule 2
(Public Health)
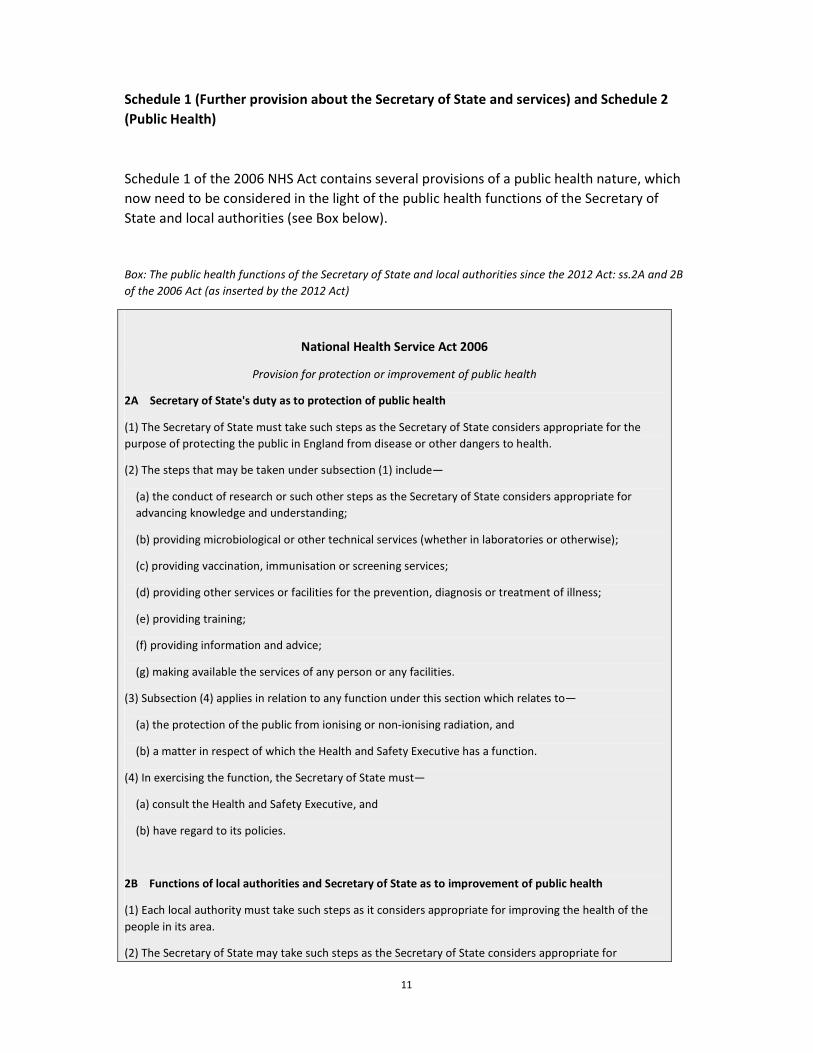
Schedule 1 of the 2006 NHS Act contains several provisions of a public health nature, which
now need to be considered in the light of the public health functions of the Secretary of
State and local authorities (see Box below).
Box: The public health functions of the Secretary of State and local authorities since the 2012 Act: ss.2A and 2B
of the 2006 Act (as inserted by the 2012 Act)
National Health Service Act 2006
Provision for protection or improvement of public health
2A Secretary of State's duty as to protection of public health
(1) The Secretary of State must take such steps as the Secretary of State considers appropriate for the
purpose of protecting the public in England from disease or other dangers to health.
(2) The steps that may be taken under subsection (1) include—
(a) the conduct of research or such other steps as the Secretary of State considers appropriate for
advancing knowledge and understanding;
(b) providing microbiological or other technical services (whether in laboratories or otherwise);
(c) providing vaccination, immunisation or screening services;
(d) providing other services or facilities for the prevention, diagnosis or treatment of illness;
(e) providing training;
(f) providing information and advice;
(g) making available the services of any person or any facilities.
(3) Subsection (4) applies in relation to any function under this section which relates to—
(a) the protection of the public from ionising or non-ionising radiation, and
(b) a matter in respect of which the Health and Safety Executive has a function.
(4) In exercising the function, the Secretary of State must—
(a) consult the Health and Safety Executive, and
(b) have regard to its policies.
2B Functions of local authorities and Secretary of State as to improvement of public health
(1) Each local authority must take such steps as it considers appropriate for improving the health of the
people in its area.
(2) The Secretary of State may take such steps as the Secretary of State considers appropriate for

12
improving the health of the people of England.
(3) The steps that may be taken under subsection (1) or (2) include—
(a) providing information and advice;
(b) providing services or facilities designed to promote healthy living (whether by helping individuals to
address behaviour that is detrimental to health or in any other way);
(c) providing services or facilities for the prevention, diagnosis or treatment of illness;
(d) providing financial incentives to encourage individuals to adopt healthier lifestyles;
(e) providing assistance (including financial assistance) to help individuals to minimise any risks to
health arising from their accommodation or environment;
(f) providing or participating in the provision of training for persons working or seeking to work in the
field of health improvement;
(g) making available the services of any person or any facilities.
(4) The steps that may be taken under subsection (1) also include providing grants or loans (on such terms
as the local authority considers appropriate).
(5) In this section, “local authority” means—
(a) a county council in England;
(b) a district council in England, other than a council for a district in a county for which there is a county
council;
(c) a London borough council;
(d) the Council of the Isles of Scilly;
(e) the Common Council of the City of London.
Medical inspection of pupils
Since the 2012 Act, a local authority has responsibilities for the medical inspection and
treatment of pupils. This was previously the responsibility of the Secretary of State under
the 2006 Act. The Explanatory Notes to the 2012 Act suggest that this transfer is in the
context of the public health functions of local authorities under section 2B.
Under section 48 of the Education Act 1944, local education authorities were given a duty to
provide for medical inspection of pupils, and a duty to make arrangements to secure
“comprehensive facilities for free medical treatment are available”. This duty was repealed
by the 1973 NHS Reorganisation Act, replacing it with a duty on the Secretary of State to
make provision for the medical and dental inspection and treatment of pupils. The NHS Act
1977 replaced this duty with a power for the Secretary of State, by arrangement with the
local authority, to provide for both medical and dental inspections and treatment.

13
Weighing and measuring of children
Since the 2012 Act, local authorities have the power (not duty) to provide for the weighing
and measuring of pupils under 12 at its schools, and the power to arrange the same with
private schools and registered child minders. From 2008 (when these provisions were first
introduced, by section 143 of the Health and Social Care Act 2008) until the 2012 Act, the
Secretary of State had the power to provide by arrangement with local education
authorities, or such private schools and minders.
The Secretary of State has the power to make regulations authorizing disclosure of
information about the children to those carrying out the weighing and measuring,
prescribing how to conduct the activities, authorizing disclosure of the results to parents
and regulating the processing of the results. The current regulations are set out in Part 3 of
The Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny)
Regulations 2013 (S.I. No. 218), which require local authorities to disclose the results to the
Health and Social Care Information Centre, which is given the power to disclose it to any
other person “with a view to enabling further processing of the information for the
purposes of research, monitoring, audit or the planning of services, or for any purpose
connected with public health, subject to the condition that the information may be
disclosed only in a form in which no individual child can be identified”.
From 2008 – 2013, it appears that Primary Care Trusts carried out the weighing and
measuring under the annual National Child Measurement Programme (The National Child
Measurement Programme Regulations 2008 (S.I. No. 3080)).
Supply of blood and other human tissues
The 2012 Act (section 17(9)) imposed a new duty on the Secretary of State to make
arrangements for collecting, screening, analyzing, processing and supplying blood and other
tissues (and related services) and for facilitating organ and tissue transplantation. According
to the Explanatory Notes to the 2012 Act, this new specific duty was needed because the
Secretary of State’s duty to provide under section 3 of the 2006 Act was abolished, along
with other changes to section 2 (general power). Those Notes also state that “[a]s now, the
functions would be performed by NHS Blood and Transplant, a Special Health Authority,
rather than by the Department of Health”.
Contraceptive services
Since the 1973 NHS Reorganisation Act, the Secretary of State has had the duty to arrange
the giving of advice on contraception, the medical examination and treatment of those
seeking such advice and the supply of contraceptive substances and appliances. This duty
remains in place.
Provision of vehicles for disabled persons
Since the 2012 Act, CCGs have a power to make arrangements for providing vehicles
including wheelchairs for persons for whom they are responsible and who appear to have a

14
physical impairment. They also have the power to make arrangements to adapt, maintain,
repair and insure the vehicle, including providing a structure in which to keep it. CCGs are
also enabled to make grants for adapting (etc.), for buying fuel and learning to drive it.
This was previously the power of the Secretary of State under the 2006 Act, which in turn
was an updated version of the power in the 1977 Act (to provide “invalid carriages for
persons appearing to him to be suffering from severe physical defect or disability”).
Provision of a microbiological service by the Secretary of State
Under the 1977 Act, a power was conferred on the Secretary of State to “provide a
microbiological service, which may include the provision of laboratories, for the control of
the spread of infectious diseases (and the Secretary of State may allow persons to use
services provided at such laboratories on such terms, including terms as to charges, as he
thinks fit)”. This service constituted “the public health laboratory service”. The Public Health
Laboratory Service Act 1979 (enacted at the very end of the Callaghan government)
extended this power so that it included the power to “carry on such other activities as in his
opinion can conveniently be carried on in conjunction with that service”, as well as powers
to charge and to exercise the power for non-NHS purposes.
Since the 2012 Act “providing microbiological or other technical services (whether in
laboratories or otherwise)” has been one of the listed “steps that may be taken” pursuant to
the Secretary of State’s duty under section 2A to “take steps as [he] considers appropriate
for the purpose of protecting the public in England from disease or other dangers to health”.
The power in paragraph 12 of Schedule 1 has been modified to reflect that.
Note that the 1977 Act continued the “Public Health Laboratory Service Board”, a body
corporate,” for the purpose of exercising such functions with respect to the administration
of the public health laboratory service”. It was abolished by section 4 of the Health and
Social Care (Community Health and Standards) Act 2003.
[Schedule1 of the 2006 Act also covers research functions]
A historical note on the functions of local authorities under the NHS Act 1946 is included in the
Appendix to this Part 2.

15
Schedule 9, Part 1 - Medical, dental, pharmaceutical and ophthalmic services
This Part of the Bill would contain amendments to those Parts of the 2006 Act that relate to
these services, as they would become administered by a DHA’s Family Health Services
Committee. The remainder of this note relates only to medical services.
Since the 2012 Act, NHS England has an over-arching duty, to the extent that it considers
necessary to meet all reasonable requirements, to exercise its powers so as to provide
primary medical services. (This was a duty previously imposed on area-based Primary Care
Trusts, initially introduced in the 2003 Health and Social Care (Community Health and
Standards) Act 2003.)
NHS England has 3 specific powers in this regard - also previously conferred on PCTs, and
subject to directions from the Secretary of State under s.98A(3) of the 2006 Act as inserted
by s.49 of the 2012 Act – which form the basis for the 3 medical services contract types:
(a) A general and widely-expressed power to make arrangements as it considers
appropriate, including entering contracts with any person, under s.83(2) of the 2006
Act – such as commercial companies or voluntary organisations. These have become
known as Alternative Personal Medical Services (APMS) contracts, though the term
does not appear in primary legislation (nor, it seems, in regulations). This power was
first introduced in the 2003 Act; and is not subject to additional requirements in the
same way as both of the following two powers are (except for directions under
s.98A(3): see the Alternative Provider Medical Services Directions 2013);
(b) A power to enter into a contract with specified persons under ss. 84 et seq., referred
to as general medical services (GMS) contracts. These are subject to several
requirements, set out in the primary Act, in extensive regulations (see the NHS
(General Medical Services Contracts) Regulations 2004, as amended, most recently
last March by the NHS (General Medical Services Contracts and Personal Medical
Services Agreements) Amendment Regulations 2014), and also in directions from the
Secretary of State. GMS contracts can be made with medical practitioners, and also
with (e.g.) companies owned by them, and with NHS trusts. This legal route is not
open to commercial companies such as Virgin or United Health (who can be awarded
APMS contracts).
The statutory origin of this power was the duty imposed (first) on area-based
Executive Councils in s.33 of the 1946 Act and (later) on various health authorities
under 29 of the 1977 Act (since abolished) to make arrangements with medical
practitioners for the provision by them of personal medical services for all persons in
the area who wished to take advantage of the arrangements.
(c) A power to make agreements with specified persons under s.92 et seq., referred to
as “s.92 arrangements) and as personal medical services (PMS) contracts. Similar to
GMS contracts, but offering more local flexibility, PMS contracts are also subject to
several requirements in regulations (see the NHS (Personal Medical Services
Agreements) Regulations 2004, as amended), and in directions. This mechanism was

16
first introduced as a “pilot scheme” in the 1997 NHS (Primary Care) Act – one of the
last Acts of the Major government – and made permanent in the 2003 Act.
It would be consistent with the scheme of the Bill to transfer NHS England’s powers to DHAs
in order for them to be administered by their Family Health Services Committees, and to
permit the power to enter into APMS contracts to be exercised only if it is not reasonably
practicable for a DHA to provide the services, or for a GMS or PMS contract to be entered
into, and if an APMS contract is necessary to meet all reasonable requirements (i.e.,
effectively the same preconditions for commercial company involvement as in Clause 9(4)
for DHAs (and Clause 8(12) for NHS England).

17
Appendix – historical note
The functions of local authorities under the NHS Act 1946
County and borough councils - termed local health authorities (LHAs) - were given a critical role in
the NHS from the start, under ministerial control. (NHS Act 1946, Part III, ss.19-30).
Summary
Scope
They were required under section 20 to submit to the Minister their proposals relating to eight
categories of service which subject to the Minister’s approval it was their duty to carry out. These
categories related to health centres, care of mothers and young children, midwifery, health visiting,
vaccination and immunization (against small pox and diptheria as a minimum), ambulance services
and the prevention of illness, care and after-care. ‘Domestic help’ formed a ninth category.
Charging
Means-tested charges could be made for domestic help and services related to prevention of illness,
care and after-care; and also for “articles” relating to the care of mothers and young children.
Duties
No duty was expressed as having to meet “reasonable requirements”, but the number of midwives
for stated purposes had to be “adequate for the needs of the area”. Only in the case of health
centres was there a direct LHA duty to provide and to employ staff (though not all staff). Midwives,
health visitors, home visitors and ambulance staff could be employees of LHAs or voluntary
organizations. Ambulance staff could also be employed by private companies or other public bodies;
and private companies could also provide vaccines and sera to the Minister for onward supply.
These duties were either transferred or abolished under the NHS Reorganisation Act 1973. More
detail on the nine categories is set out below.
Service categories
Health centres
Amongst these eight categories, the only one which it was the authority’s duty directly to provide
(equip and maintain to the satisfaction of the Minister) was health centres, under section 21. These
were premises at which facilities would be available for at least one of six categories of service -
general medical services, dental and pharmaceutical services; for the provision or organisation of
any of the services which the LHA are required or empowered to provide; services of specialists or
other services provided for outpatients under Part III; or for the exercise of the powers conferred on
the LHA by s.179 of the Public Health Act 1936, or s.298 Public Health (London) Act 1936; for the
publication of information on questions relating to health or disease; and for the delivery of lectures
and the display of pictures or cinematograph films in which such questions are dealt with. The
authority was also obliged to provide staff at the centres to the Minister’s satisfaction (but not
medical and dental staff providing (Part IV services).

18
Care of mothers and young children
The LHA had a duty under section 22 “to make arrangements for the care, including in particular
dental care, of expectant and nursing mothers and of children who have not attained the age of 5
years and are not attending primary schools maintained by a local health authority” – and were
empowered to make reasonable charges (subject to ministerial approval) “in respect of articles
provided” having regard to the means of those persons. They were also empowered with approval
to contribute to any voluntary organization formed for such purposes.
Midwifery
LHAs became the local supervising authority under Midwives Acts 1902-1936, and were given the
duty to “secure” - whether by making arrangements with Boards of Governors of teaching hospitals,
hospital management committees or voluntary organizations for the employment by those Boards,
committees or organizations of certified midwives or by themselves employing such midwives - “that
the number of certified midwives so employed who are available in the authority’s area for
attendance on women in their homes as midwives, or as maternity nurses during childbirth and from
time to time thereafter during a period not less than the lying-in period, is adequate for the needs of
the area”.
Health visiting
LHAs were also given the duty under section 24 “to make provision in their area for the visiting of
persons in their homes by visitors, to be called ‘health visitors’, for the purpose of giving advice as to
the care of young children, persons suffering from illness and expectant or nursing mothers, and as
to the measures necessary to prevent the spread of infection.”. This could be done by making
arrangements with voluntary organizations for the employment by those organizations of health
visitors, or by the LHA itself employing health visitors.
Home nursing
A similar duty was imposed on LHAs under section 25 to “to make provision…for securing the
attendance of nurses on persons who require nursing in their own homes”; again, by making
arrangements with voluntary organizations for the employment by them of nurses or by the LHA
itself employing such nurses.
Vaccination and immunization
Each LHA was obliged to make arrangements with medical practitioners for small pox vaccinations
and diphtheria immunizations, under section 26. They were also empowered to make similar
arrangements against any other disease if approved by the Minister; and were obliged to do so if
directed by him or her. The Minister was empowered – directly or by through arrangements with
such persons as he or she thought fit (so including private companies) – to supply the vaccines, sera
or other preparations free of charge.
Ambulance services
Under section 27, it was the duty of every LHA “to make provision for securing” that ambulances and
other means of transport are available, where necessary, for the conveyance of persons suffering
from illness or mental defectiveness, and of expectant or nursing mothers. This duty could be
performed by the LHA itself providing the necessary ambulances etc. and the necessary staff, or by
making arrangements with voluntary organizations “or other persons” for the provision by them of
such ambulances, transport and staff. Of the LHA services, this is the only instance where it is
19
specified that the arrangements can be made with persons other than voluntary organizations (e.g.,
with private companies).
Prevention of illness, care and after-care
Making arrangements for the purpose of the prevention of illness, the care of persons suffering from
illness or mental defectiveness, or the after-care of such persons, was also a power given to LHAs,
with ministerial approval. (It is curious that section 28 refers expressly to ministerial approval,
because all these LHA services are subject to such approval under section 20, so it might be that this
service was seen particularly as needing central control.) LHAs were empowered to make reasonable
and means-tested charges (subject to ministerial approval); and could with approval contribute to
voluntary organizations formed for these purposes.
Domestic help
An LHA was also empowered to “make such arrangements as the Minister may approve for
providing domestic help for households where such help is required owing to the presence of any
person who is ill, lying-in, an expectant mother, mentally defective, aged, or a child not over
compulsory school age”. Again, reasonable and means-tested charges with ministerial approval
could be made. Proposals for domestic help did not have to be submitted to the Minister under
section 20 along with proposals for the other eight categories of service.
Part 3 follows
20
NHS Reinstatement Bill
CONTENTS
PART 1
SERVICES, ADMINISTRATION AND ACCOUNTABILITY
1 Secretary of State’s duties to promote and provide a comprehensive health service
2 Abolition of the duties of autonomy
3 Secretary of State’s duty to provide certain services
4 High security psychiatric services
5 Other services
6 Public health functions of the Secretary of State and local authorities
7 Distribution of functions
8 NHS England and Regional Committees
9 District Health Authorities
10 Family Health Services Committees
11 Special health authorities
12 Directions
13 Abolition of clinical commissioning groups
14 Abolition of NHS trusts
15 Abolition of NHS foundation trusts
16 Terms and conditions of staff transfers
17 Community Health Councils
PART 2
REGULATION OF HEALTH AND ADULT SOCIAL SERVICES
18 Abolition of Monitor and transfer to the Care Quality Commission
19 Competition
20 Continuity of mandatory services
PART 3
TERMS AND CONDITIONS
21 National terms and conditions
PART 4
TREATIES
22 Treaty requirements

21
PART 5
FINAL PROVISIONS
23 Commencement and transitional arrangements
24 Further and consequential amendments
25 Interpretation
26 Short title and extent
SCHEDULES
Schedule 1 – Further provision about the Secretary of State and services
Schedule 2 – Public Health
Schedule 3 - NHS England and its Regional Committees
Schedule 4 - District Health Authorities
Schedule 5 – District Health Authorities: Additional Functions
Schedule 6 – Repeals
Part 1: Further repeals consequent on abolition of clinical commissioning groups
Part 2: Further repeals consequent on abolition of NHS trusts
Part 3: Further repeals consequent on abolition of NHS foundation trusts
Part 4: Further repeals consequent on the abolition of the National Health Service
Commissioning Board
Part 5: Other miscellaneous repeals
Schedule 7 - Community Health Councils
Schedule 8 – Transitional Arrangements
Schedule 9 – Further and consequential amendments
Part 1: Medical services, dental services, pharmaceutical services, ophthalmic
services
Part 2: Regulation of health and social care
Part 3: Public involvement, local government and scrutiny
Part 4: The National Institute for Health and Care Excellence
Part 5: The Health and Social Care Information Centre
Part 6: Charging
Part 7: Protection of NHS from fraud and other unlawful activities
Part 8: Property and finance
Part 9: Miscellaneous

22
A
B I L L
TO
Re-establish the Secretary of State’s legal duty as to the National Health Service in England;
to halt and reverse marketization; to make provision for the administration and accountability
of the National Health Service; to abolish certain bodies; to protect mandatory services; and
for associated purposes.
Be it enacted by the Queen’s most Excellent Majesty, by and with the advice and
consent of the Lords Spiritual and Temporal, and Commons, in this present
Parliament assembled, and by the authority of the same, as follows:—
PART 1
SERVICES, ADMINISTRATION AND ACCOUNTABILITY
Duties of the Secretary of State
1 Secretary of State’s duties to promote and provide a comprehensive health
service
For section 1 of the National Health Service Act 2006 (Secretary of State’s duty to
promote comprehensive health service) substitute—
“1 Secretary of State’s duty as to the health service
(1) It shall be the duty of the Secretary of State to promote in England a
comprehensive health service designed to secure improvement—
(a) in the physical and mental health of the people of England, and
(b) in the prevention, diagnosis and treatment of illness,
and for that purpose to provide or secure the effective provision of services in
accordance with this Act.

23
(2) The services so provided must be free of charge except in so far as the making
and recovery of charges is expressly provided for, by or under any enactment,
whenever passed.”
2 Abolition of the duties of autonomy
Sections 1D and 13F of the National Health Service Act 2006 (duties as to
promoting autonomy) are repealed.
Duties as to certain services
3 Secretary of State’s duty to provide certain services
(1) For section 3 of the National Health Service Act 2006 (Duties of clinical
commissioning groups as to commissioning certain health services) substitute—
“3 Secretary of State’s duty to provide certain services
(1) The duty of the Secretary of State under section 1(1) to provide or secure
the effective provision of services includes—
(a) the duty of the Secretary of State imposed by subsection (2) below,
(b) duties and powers in relation to high security psychiatric services in
accordance with section 4 below;
(c) duties and powers in Part 4 (medical services), Part 5 (dental services),
Part 6 (Ophthalmic services) and Part 7 (Pharmaceutical services and
local pharmaceutical services) below; and
(d) duties and powers in relation to other services, in accordance with
Schedule 1 of this Act.
(2) It is the Secretary of State’s duty to provide throughout England, to such
extent as he considers necessary to meet all reasonable requirements—
(a) hospital accommodation;
(b) other accommodation for the purpose of any service provided under
this Act;
(c) medical, dental, nursing and ambulance services;

24
(d) such other facilities for the care of expectant and nursing mothers and
young children as he considers are appropriate as part of the health
service;
(e) such facilities for the prevention of illness, the care of persons
suffering from illness and the after-care of persons who have suffered
from illness as he considers are appropriate as part of the health service;
(f) such other services as are required for the diagnosis and treatment of
illness.
(3) The Secretary of State may provide or secure the provision of anything
mentioned in subsection (2) above outside England.
(4) Subsection (2) does not affect the provisions of Parts 4-7 (which relate to
arrangements with practitioners for the provision of medical, dental,
ophthalmic and pharmaceutical services).”
(2) Section 3 (Duties of clinical commissioning groups as to commissioning certain
health services) and section 3A (Power of clinical commissioning groups to
commission certain health services) of the National Health Service Act 2006 are
repealed.
4 High security psychiatric services
In section 4(1) of the National Health Service Act 2006, for the words “The Board
must arrange for the provision of” substitute the words “The Secretary of State's
duty under section 1(1) includes a duty to provide and maintain”.
5 Other services
Schedule 1 of this Act makes further provision about the Secretary of State and
services under the National Health Service Act 2006 and amends Schedule 1 of
that Act.
25
6 Public health functions of the Secretary of State and local authorities
Schedule 2 of this Act shall have effect in relation to section 2A (Secretary of
State’s duty as to protection of public health) and section 2B (Functions of local
authorities and Secretary of State as to improvements of public health) of the
National Health Service Act 2006.
Administration
7 Distribution of functions
There shall be established—
(a) a Special Health Authority to be known as the National Health Service
England Authority, with Regional Committees, in accordance with and having
the functions referred to in section 8 below,
(b) District Health Authorities, with Family Health Service Committees, in
accordance with and having the functions referred to in sections 9 and 10
below.
8 NHS England and Regional Committees
(1) The National Health Service Commissioning Board is abolished.
(2) The Special Health Authority known as The National Health Service England
Authority (referred to in this Act as “NHS England”) established pursuant to section
26
7(a) above shall have a number of Regional Committees covering the whole of
England.
(3) Schedule 3 makes further provision in relation to the establishment of NHS England
and its Regional Committees.
(4) NHS England shall exercise on behalf of the Secretary of State his duty in section
1(1), and, to the extent relevant, his duty under section 3(2), of the National Health
Service Act 2006, by providing or securing effective provision of the services or
facilities referred to in subsection (5) below in accordance with regulations made by the
Secretary of State.
(5) The services or facilities referred to in subsection (4) are—
(a) dental services of a prescribed description;
(b) services or facilities for members of the armed forces or their families;
(c) services or facilities for persons who are detained in a prison or in other
accommodation of a prescribed description;
(d) such other services or facilities as may be prescribed that—
(i) support District Health Authorities (including their Family Health
Services Committees) and other Special Health Authorities in
discharging their functions, or
(ii) are more appropriate for NHS England to provide or secure
effective provision of rather than the Secretary of State or District
Health Authorities (or their Family Health Services Committees).
(6) In deciding for the purposes of subsection (5)(d)(ii) whether it would be
appropriate, the Secretary of State must have regard to—
(a) the number of individuals who require the provision of the service or
facility;
(b) the cost of providing the service or facility;
(c) the number of persons able to provide the service or facility; and
(d) the financial implications of NHS England providing or securing effective
provision of the service rather than any of the other persons or bodies
mentioned in that subsection.
27
(7) Before deciding whether to make regulations under subsection (5), the Secretary of
State must—
(a) obtain advice appropriate for that purpose, and
(b) consult NHS England.
(8) The reference in subsection (5)(b) to members of the armed forces is a reference
to persons who are members of—
(a) the regular forces within the meaning of the Armed Forces Act 2006, or
(b) the reserve forces within the meaning of that Act.
(9) The Secretary of State may also make regulations containing directions to NHS
England relating to their functions under this section in accordance with section
12 below.
(10) NHS England shall perform its functions through its Regional Committees, save
to the extent that regulations provide otherwise.
(11) The Secretary of State may make regulations that provide otherwise where he
considers that it is more appropriate for a service or facility to be provided, or for its
effective provision to be secured, on a national basis rather than on regional bases.
(12) NHS England may make arrangements with any person for the provision of the
services or facilities referred to in subsection (5) provided that—
(a) it is not reasonably practicable for those services or facilities to be provided
directly by—
(i) NHS England (including by one or more of its Regional Committees), or
(ii) by another health service body,
(b) all reasonable requirements for those services or facilities could not
foreseeably be met in the absence of such arrangements, and
(c) the person holds a licence under Chapter 3 of Part 3 of the Health and
Social Care Act 2012.
(13) “Health service body” means any of the following—
(a) NHS England, including one or more of its Regional Committees,
(b) a DHA, including one or more of its Family Health Services Committee,

28
(c) a Special Health Authority,
(d) a Local Health Board,
(e) a Health Board constituted under section 2 of the National Health Service
(Scotland) Act 1978 (c. 29),
(f) a Special Health Board constituted under that section,
(g) a Health and Social Services Board constituted under the Health and
Personal Social Services (Northern Ireland) Order 1972 (S.I. 1972/1265
(N.I.14)),
(h) the Common Services Agency for the Scottish Health Service,
(i) the Wales Centre for Health,
(j) the Care Quality Commission,
(k) NICE,
(l) the Health and Social Care Information Centre,
(m) the Scottish Dental Practice Board,
(n) the Secretary of State,
(o) the Welsh Ministers,
(p) the Scottish Ministers,
(q) Healthcare Improvement Scotland,
(r) the Northern Ireland Central Services Agency for the Health and Social
Services established under the Health and Personal Social Services (Northern
Ireland) Order 1972,
(s) a special health and social services agency established under the Health and
Personal Social Services (Special Agencies) (Northern Ireland) Order 1990
(S.I. 1990/247 (N.I.3)),
(t) a Health and Social Services trust established under the Health and Personal
Social Services (Northern Ireland) Order 1991 (S.I. 1991/194 (N.I.1)),
(u) the Department of Health, Social Services and Public Safety.
(14) An arrangement made by NHS England and another health service body shall not
be regarded as giving rise to contractual rights or liabilities.
29
9 District Health Authorities
(1) It is the duty of the Secretary of State to establish by order in accordance with
Schedule 4 to this Act authorities to be called District Health Authorities (referred to
in this Act as “DHAs”) for districts within regions that—
(a) correspond with those of the Regional Committees of NHS England, and
(b) have Family Health Services Committees with the functions referred to in
section 10.
(2) A DHA shall exercise on behalf of the Secretary of State his duty in section 1(1) of
the National Health Service Act 2006 by exercising his functions under the following
provisions of that Act—
(a) section 3(2)(a) and (b), with respect to the provision of hospital and other
accommodation for the purposes of any service provided under the Act,
(b) section 3(2)(c), with respect to the provision of medical, dental, nursing and
ambulance services,
(c) section 3(2)(d), with respect to the provision of facilities for the care of
expectant and nursing mothers and young children,
(d) section 3(2)(e), with respect to the provision of facilities for the prevention of
illness and the aftercare of persons who have suffered from illness,
(e) section 3(1)(f), with respect to the provision of such other services as are
required for the diagnosis and treatment of illness,
(f) Schedule 1 of that Act (as modified by Schedule 1 of this Act), with respect to
the other services referred to therein, and
(h) Schedule 5 of this Act, with respect to the additional functions set out therein.
(3) The Secretary of State may also make regulations containing directions to District
Health Authorities relating to their functions under this section in accordance with
section 12 below.
(4) A DHA may make arrangements with any person for the provision of the services
or facilities referred to in subsection (2) provided that—
(a) it is not reasonably practicable for those services or facilities to be provided
directly by—
(i) that DHA or by another DHA, or
30
(ii) by another health service body,
(b) all reasonable requirements for those services or facilities could not
foreseeably be met in the absence of such arrangements, and
(c) the person holds a licence under Chapter 3 of Part 3 of the Health and Social
Care Act 2012.
(5) “Health service body” has the same meaning as in section 8(13) above.
(6) An arrangement made by a DHA (including by its Family Health Services Committee
under section 10 below) and another health service body shall not be regarded as
giving rise to contractual rights or liabilities.
10 Family Health Services Committees
(1) It is the duty of each Family Health Services Committee established under section
9(1) above, in accordance with regulations—
(a) to administer, on behalf of the District Health Authority, the arrangements
made under Parts 4-7 of the National Health Service Act 2006 for the provision of
medical, dental, ophthalmic and pharmaceutical services for the district of the
Authority, and
(b) to perform such other functions relating to those services as may be prescribed.
(2) Schedule 4, Part 2 makes further provision in respect of Family Health Services
Committees and the discharge of their functions under subsection (1).
11 Special health authorities
(1) If the Secretary of State considers that a special body should be established for the
purpose of performing any functions which he may direct the body to perform on
his behalf, or on behalf of NHS England (including on behalf of one or more of its
Regional Committees), a District Health Authority (including its Family Health

31
Services Committee), he may by order establish a body for that purpose in
accordance with section 28 (Special Health Authorities) of the National Health
Service Act 2006.
(2) Section 28A of the National Health Service Act 2006 is repealed.
12 Directions
(1) The Secretary of State may direct any of the bodies mentioned in subsection (2) to
exercise any functions relating to the health service which are specified in the
directions, and may also give directions to any such body about its exercise of any
functions or about its provision of services under arrangements referred to in
subsection (2)(f).
(2) These bodies are—
(a) NHS England, including any or all of its Regional Committees,
(b) a DHA, including any Family Health Services Committee,
(c) a Special Health Authority,
(d) the National Institute for Health and Care Excellence,
(e) the Health and Social Care Information Centre, and
(f) any other body or person providing services in pursuance of prescribed
arrangements.
(3) In exercising his power under subsection (1), the Secretary of State must have
regard to the desirability, so far as consistent with the interests of the health service and
relevant to the exercise of the power in all circumstances—
(a) of protecting and promoting the health of patients and the public,
(b) of any bodies mentioned in subsection (2) being free, in exercising its
functions or providing services in accordance with its duties and powers, to do so
in the manner that it considers best calculated to promote the comprehensive
service referred to in section 1 (1) of the National Health Service Act 2006, and
(c) of ensuring co-operation between the bodies mentioned in subsection (2) in the
exercise of their functions or provision of services.
32
(4) If, in having regard to the desirability of the matters referred to in subsection (3) the
Secretary of State considers that there is a conflict between those matters and the
discharge of his duties under section 1 of the National Health Service Act 2006, he must
give priority to the duties under that section.
(5) Directions under this section must be contained in regulations, except in an
emergency, but cannot as directions modify the terms of any enactment.
Abolition of bodies
13 Abolition of clinical commissioning groups
(1) Clinical commissioning groups are abolished.
(2) Chapter A2 of the National Health Service Act 2006 (Clinical Commissioning
Groups) (sections 14A to 14Z24) is repealed.
(3) Schedule 6, Part 1 has effect for the purposes of further consequential repeals.
(4) On the day this section is commenced by order the property, rights and liabilities of
clinical commissioning groups shall vest in the Secretary of State or in any other NHS
body determined by him in accordance with regulations made under this section.
(5) In making such an order and regulations the Secretary of State shall have regard to the
provisions of section 23 and of Schedule 8 (Transitional Arrangements) of this Act.
14 Abolition of NHS trusts
(1) The Secretary of State shall exercise his power under paragraph 28(1) of Schedule 4
of the National Health Service Act 2006 to dissolve by order all NHS trusts.
33
(2) The following provisions of Part 3 of Schedule 4 of the National Health Service Act
2006 (NHS trusts established under section 25: Dissolution) shall apply to dissolution
under subsection (1):
(a) paragraph 28(3) (such prior consultation as may be prescribed),
(b) paragraph 29 (transfer by order of properties, liabilities and employed staff to
himself or an NHS body), and
(c) paragraph 30 (responsibility for continued payment of pension, allowances
and gratuities).
(3) Chapter 3 of Part 2 of the National Health Service Act 2006 (Health Service Bodies:
NHS trusts) (sections 25 to 27) is repealed, including save as aforesaid Schedule 4,
and including Schedule 5 thereof (Financial provision about NHS trusts).
(4) In making an order dissolving an NHS trust under this section the Secretary of State
shall have regard to the provisions of section 23 and of Schedule 8 (Transitional
Arrangements) of this Act.
(5) Schedule 6, Part 2 has effect for the purpose of further consequential repeals.
15 Abolition of NHS foundation trusts
(1) NHS foundations trusts are abolished.
(2) Chapter 5 of Part 2 of the National Health Service Act 2006 (Health Service Bodies:
NHS foundation trusts) (sections 30 – 65) is repealed.
(3) On the day this section is commenced by order the property, rights and liabilities of
NHS foundation trusts shall vest in the Secretary of State or in any other NHS body
determined by him in accordance with regulations made under this section.
(4) In making such an order and such regulations, the Secretary of State shall have regard
to the provisions of section 23 and of Schedule 8 (Transitional Arrangements) of this
Act.
34
(5) Schedule 6, Part 3 has effect for the purpose of further consequential repeals.
16 Terms and conditions of staff transfers
(1) The Secretary of State shall make regulations determining the terms and conditions
relating to the transfer of staff as the result of abolition of any of the bodies referred to
in sections 13, 14 and 15, including terms and conditions relating to eligibility for
redundancy payments.
(2) Before making those regulations, he shall consult with representatives of those staff.
Accountability
17 Community Health Councils
(1) It shall be the duty of the Secretary of State to establish in accordance with this
section a Council for the district of each DHA or separate Councils for such separate
parts of the districts of those Authorities as he thinks fit; and such a council shall be
called a Community Health Council (and is hereafter referred to as a "Council").
(2) It shall be the duty of a Council—
(a) to represent the interests in the health service of the public in its district; and
(b) to perform such other functions as may be conferred on it by virtue of the
following subsection.
(3) Schedule 7 shall have effect.
35
PART 2
REGULATION OF HEALTH AND ADULT SOCIAL SERVICES
18 Abolition of Monitor and transfer to the Care Quality Commission
(1) Subject to subsection (2), Monitor is abolished and its functions and objective at the
date of abolition shall be transferred to the Care Quality Commission.
(2) Subsection (1) shall come into effect by order of the Secretary of State [made no
later than 1st April 2016].
(3) The Health and Social Care Act 2012 is amended as follows.
(4) After section 61 (Monitor) insert—
“61A Monitor’s objective (to be transferred to the Care Quality Commission)
(1) The objective of Monitor is, through the exercise of its functions, to
contribute to the achievement of a comprehensive health service in England as a
service of social solidarity based on cooperation.
(2) In exercising its main duty and other functions Monitor must act in
accordance with that objective and in a manner consistent with the performance
by the Secretary of State of his duties contained in sections 1 and 3 of the
National Health Service Act 2006.
(3) The objective in subsection (1) and the duty in subsection (2) shall transfer
to the Care Quality Commission in accordance with section 18(1) of the NHS
Reinstatement Act 2014.”
(4) In section 62 (General duties), at the end of subsection (1), after “services”,
delete “.” and insert “, where provision of those services is made pursuant to
arrangements under and in accordance with the Emergency NHS Reinstatement
Act”.
(5) Section 62(9) is repealed.

36
19 Competition
(1) Sections 72- 80 (Competition) of the Health and Social Care Act 2012 are repealed.
(2) The National Health Service (Procurement, Patient Choice and Competition)
(No. 2) Regulations 2013 are repealed.
20 Continuity of mandatory services
Conditions in a licence issued to an NHS foundation trust by Monitor pursuant to section
87(3) of the Health and Social Care Act 2012 which purport to have the effect by April
2016 of modifying, de-designating or ceasing services which that trust was obliged to
provide under its previous authorisation given pursuant to section 35 of the National
Health Service Act 2006 shall be void and of no effect.
PART 3
TERMS AND CONDITIONS
21 National terms and conditions
(1) Staff employed in providing NHS services shall be employed on terms and conditions
in accordance with the arrangements of the NHS Staff Council.
(2) Subsection (1) applies regardless of whether the provider is licensed under Chapter 3
of Part 3 of the Health and Social Care Act 2012.
(3) In subsection (1), “NHS services” means health services provided in England for the
purposes of the health service continued under section 1(1) of the National Health
Service Act 2006.
PART 4
TREATIES
22 Treaty requirements
37
(1) No treaty which requires the United Kingdom—
(a) to change; or
(b) to limit the powers of the United Kingdom in respect of
NHS legislation shall be signed or agreed unless any such changes or limits have been
approved by—
(i) in relation to England, an Act of Parliament;
(ii) in relation to Scotland, an Act of the Scottish Parliament;
(iii) in relation to Wales, an Act of the National Assembly for Wales; and
(iv) in relation to Northern Ireland, an Act of the Northern Ireland Assembly.
(2) In subsection (1)—
“to change” means to amend, repeal, introduce or otherwise to change;
“NHS legislation” means any primary legislation passed by Parliament,
the Scottish Parliament, the National Assembly for Wales or the
Northern Ireland Assembly, and any secondary legislation enacted by
the Secretary of State or any of the devolved administrations, relating
to—
(a) as regards England, the comprehensive health service which
must be continued under section 1(1) of the National Health
Service Act 2006;
(b) as regards Scotland, the comprehensive and integrated health
service that must be continued under section 1(1) of the
National Health Service (Scotland) Act 1978;
(c) as regards Wales, the comprehensive health service that must
be continued under section 1(1) of the National Health Service
(Wales) Act 2006; and
(d) as regards Northern Ireland, the integrated health services and
personal social services that must be provided or secured under
Article 4 of the Health and Personal Social Services (Northern
Ireland) Order 1972;
“treaty” means a written agreement between States or between States and
international organisations which is binding under international law
and includes any protocol, annex or schedule to or an amendment or
replacement of such an agreement and includes a regulation, rule,
measure, decision or similar instrument made under a treaty, which has the effect
mentioned in subsection (1).

38
PART 5
FINAL PROVISIONS
23 Commencement and transitional arrangements
(1) Section 1 of this Act, and subsection (3) below, shall come into force on the day on
which this Act is passed.
(2) The other provisions of this Act shall be brought into force on such day as the
Secretary of State may by order appoint that is not later than twelve months from the
day on which this Act is passed; and different days may be appointed for different
provisions and for different purposes (including different areas).
(3) Schedule 8 makes provision about current services during any period before all the
provisions of this Act are brought into force.
(4) In subsection (3), “current services” means health services which are at the time this
section comes into effect are being provided, secured or arranged under the National
Health Service Act 2006 or the Health and Social Care Act 2012.
24 Further and consequential amendments
Schedule 9 shall have effect.
25 Interpretation
Expressions used in this Act which are also in the National Health Service Act
2006 and in the Health and Social Care Act 2012 shall have the same meanings
as the meanings given to those expressions under those Acts.
26 Short title and extent
(1) This Act may be cited as the National Health Service Reinstatement Act 2014.
(2) This Act extends to England, and, in relation to section 22, to Scotland, Wales and
Northern Ireland.

39
SCHEDULES
Schedule 1 – Further provision about the Secretary of State and services
Schedule 2 – Public Health
Schedule 3 - NHS England and its Regional Committees
Schedule 4 - District Health Authorities
Schedule 5 – District Health Authorities: Additional Functions
Schedule 6 – Repeals
Part 1: Further repeals consequent on abolition of clinical
commissioning groups
Part 2: Further repeals consequent on abolition of NHS trusts
Part 3: Further repeals consequent on abolition of NHS foundation
trusts
Part 4: Further repeals consequent on the abolition of the National
Health Service Commissioning Board
Part 5: Other miscellaneous repeals
Schedule 7 - Community Health Councils
Schedule 8 – Transitional Arrangements
Schedule 9 – Further and consequential amendments
Part 1: Medical services, dental services, pharmaceutical services,
ophthalmic services
Part 2: Regulation of health and social care
Part 3: Public involvement, local government and scrutiny
Part 4: The National Institute for Health and Care Excellence
Part 5: The Health and Social Care Information Centre
Part 6: Charging
Part 7: Protection of NHS from fraud and other unlawful activities
Part 8: Property and finance
Part 9: Miscellaneous

40
SCHEDULE 1
Section 5
FURTHER PROVISION ABOUT THE SECRETARY OF STATE AND SERVICES
Medical inspection of pupils
Weighing and measuring of children
Supply of blood and other human tissues
Contraceptive services
Provision of vehicles for disabled persons
Provision of a microbiological service by the Secretary of State
Powers of the Secretary of State in relation to research etc
SCHEDULE 2
Section 6
PUBLIC HEALTH
Part 1
PUBLIC HEALTH PROTECTION
Secretary of State’s duty as to protection of public health
Part 2
PUBLIC HEALTH IMPROVEMENT
Functions of local authorities and Secretary of State as to improvements of public health

41
SCHEDULE 3
Section 8
NHS ENGLAND AND ITS REGIONAL COMMITTEES
Part 1
NHS England
[Corporate status, Membership, Appointments, Pay and Allowances, Staff, Regional
Committees, Other Committees and sub-committees]
Part 2
Regional Committees
[Membership, Power to act on behalf of NHS England, Power to act on behalf of the
Secretary of State or another NHS body, Appointments etc.]
42
SCHEDULE 4
Section 9
Part 1
DISTRICT HEALTH AUTHORITIES
Establishment
1. It is the Secretary of State's duty to exercise the powers conferred on him by section 9(1)
so as to secure—
(a) that the regions determined in pursuance of those provisions together comprise the
whole of England and that no region includes part only of any district; and
(b) that the provision of health services in each region can conveniently be associated
with a university which has a school of medicine or with two or more such
universities.
2. An order made by virtue of section 9(1) shall contain such provisions for the transfer of
officers, property, rights and liabilities as the Secretary of State thinks fit.
3. It is the Secretary of State's duty before he makes an order under section 9(1) to consult
with respect to the order—
(a) such bodies as he may recognise as representing officers who in his opinion are
likely to be transferred or affected by transfers in pursuance of the order; and
(b) such other bodies as he considers are concerned with the order.
Other matters
[Corporate status, Membership, Appointments, Pay and Allowances, Staff, Committees and
sub-committees]
Part 2
FAMILY HEALTH SERVICES COMMITTEES

43
SCHEDULE 5
Section 9(2)(h)
DISTRICT HEALTH AUTHORITIES: ADDITIONAL FUNCTIONS
1. A DHA shall exercise on behalf of the Secretary of State his duty in section 1(1) by
exercising his functions under the provisions referred to in the following paragraphs of this
Schedule.
2. [Section […], with respect to making arrangements for the conduct of, or assistance by
grants or otherwise to any person for the conduct of, research [etc.]]
3. [Section […], with respect to the payment of travelling expenses.]
4. [Section […], with respect to recognition of regional advisory committees.]
5. [Section […], with respect to recognition of district advisory committees.]
6. [Section […], with respect to arranging with any person or body (including a voluntary
organisation) for that person or body to provide or assist in providing any service under the
Act, but subject to the provisions of this Act.]
7. [Section […], with respect to making available to certain persons and bodies (including
voluntary organisations) facilities and services of persons employed in connection with such
facilities]
8. [Section […], with respect to the agreement of terms and the making of payments in
respect of facilities or services provided under section […].]
9. [Section […], with respect to making available (on such terms as to charges as thought fit)
supplies of human blood.]
10. [Section […], with respect to the supply of goods, services and other facilities to local
authorities and other public bodies and carrying out maintenance work in connection with
any land or building the maintenance of which is a local authority responsibility.]
11. [Section […], with respect to the making available to persons providing general medcial
services, general dental services, general opthalmic services or pharmaceutical services such
goods, materials and other facilities as may be prescribed.]
12. [Section […], with respect to making available any services or other facilities and the
services of employed persons to enable local authorities to discharge their functions relating
to social services, education and public health.]
13. [Other powers in relation to local authorities which may or may not continue to be
relevant, such as a power to arrange to make available to local authorities the services of
specified groups of persons (GPs, dentists etc) so far as reasonably necessary and practicable
to enable local authorities to discharge their functions relating to social services, education
and public health; to consult before making persons available and power to agree terms and
payment; and the function of agreeing charges with local authorities where their employed
staff are made available to enable health authorities to exercise their functions.]

44
14. [Section […], with respect to making available in premises provided under the Act, such
facilities as are regarded as required for clinical teaching and for research connected with
clinical medicine or clinical dentistry.]
15. [Section […], with respect to making available [certain accommodation for GPs et al.]]
16. [Section […] with respect to allowing use of and charging for accommodation or services,
including for private patients.]
17. [Section […] with the respect to the disposal of goods and the production and
manufacture of them in excess of that required for the services provided under the other
provisions of the Act.]
18. [Section […], with respect to authorising hospital accommodation to be made available
on payment of charges for part of the cost and recovering those charges.]
19. [Section […], with respect to allowing accommodation and services, authorised to be
made available in connection with the treatment, in pursuance of arrangements made by
medical or dental practitioners, of their private patients as resident patients.]
20. [Various other functions such as those relating to charges to non-residents, charges for
more expensive supplies, charges for replacement or repair of appliances and vehicles, land
acquisition and other property required for the purposes of the Act and use and maintenance
of any property belonging to the Secretary of State by virtue of the Act (but not his or her
compulsory acquisition powers).]
21. [Specified Mental Health Act functions]
22. [Specified social care functions]
23. [Specified provisions of the Health Services and Public Health Act 1968 – such as those
relating to “the instruction of officers of health authorities and other persons employed or
contemplating employment” by health authorities or in authorities connected with health or
welfare.]

45
SCHEDULE 6
REPEALS
Part 1
Further repeals consequent on abolition of clinical commissioning groups
Part 2
Further repeals consequent on abolition of NHS trusts
Part 3
Further repeals consequent on abolition of NHS foundation trusts
Part 4
Further repeals consequent on abolition of The National Health Service Commissioning
Board

46
SCHEDULE 7
Section 17
COMMUNITY HEALTH COUNCILS
1. Provision may be made by regulations as to—
(a) the membership of Councils (including the election by members of a Council of a
chairman of the Council);
(b) the proceedings of Councils;
(c) the staff, premises and expenses of Councils;
(d) the consultation of Councils by DHAs with respect to such matters and on such
occasions as may be prescribed;
(e) the furnishing of information to Councils by DHAs and the rights of members of
Councils to enter and inspect premises controlled by DHAs;
(f) the consideration by Councils of matters relating to the operation of the health
service within their districts and the giving of advice by Councils to DHAs on such
matters;
(g) the preparation and publication of reports by Councils on such matters and the
furnishing and publication by DHAs of comments on the reports; and
(h) the functions to be exercised by Councils in addition to the functions exercisable by
them by virtue of paragraph (a) of the preceding subsection and the preceding
provisions of this subsection;
and the Secretary of State may pay to members of Councils such travelling and other
allowances (including compensation for loss of remunerative time) as he may determine
with the consent of the Minister for the Civil Service.
2. It shall be the duty of the Secretary of State to exercise his power to make regulations in
pursuance of paragraph 1(a) so as to secure as respects each Council that—
(a) at least one member of the Council is appointed by each local authority of which the
district or part of it is included in the Council's district and at least half of the
members of the Council consist of persons appointed by those local authorities;
(b) at least one third of the members of the Council are appointed in a prescribed manner
by bodies (other than public or local authorities) of which the activities are carried on
otherwise than for profit;
47
(c) the other members of the Council are appointed by such bodies, in such manner and
after such consultations as may be prescribed ; and
(d) no member of the Council is also a member of a DHA or Special Health Authority;
but nothing in this subsection shall affect the validity of anything done by or in
relation to a Council during any period during which, by reason of a vacancy in the
membership of the Council or a defect in the appointment of a member of it, a
requirement included in regulations in pursuance of this subsection is not satisfied.
3. The Secretary of State may by regulations—
(a) provide for the establishment of a body—
(i) to advise Councils with respect to the performance of their functions and to
assist Councils in the performance of their functions, and
(ii) to perform such other functions as may be prescribed; and
(b) make provision as to the membership, proceedings, staff, premises and expenses of
the said body;
and the Secretary of State may pay to members of the said body such travelling and other
allowances (including compensation for loss of remunerative time) as he may determine
with the consent of the Minister for the Civil Service.
4. In this Schedule—
“local authority” means in England a county council; a district council, other than a
council for a district in a county for which there is a county council; a London
borough council; the Council of the isles of Scilly; or the Common Council of the
City of London; and
“district” in relation to a Council, means the locality for which it is established,
whether that locality consists of the district or part of the district of a DHA or such a
district or part together with the districts or parts of the districts of other DHAs; and
the district of a Council must be such that no part of it is separated from the rest of it
by territory not included in the district,
and section 25 shall be construed accordingly.

48
SCHEDULE 8
Section 23(3)
TRANSITIONAL ARRANGEMENTS
[Provisions to ensure continuity of services during the transition]
SCHEDULE 9
Section 24
FURTHER AND CONSEQUENTIAL AMENDMENTS
Part 1
MEDICAL SERVICES, DENTAL SERVICES, PHARMACEUTICAL SERVICES,
OPHTHALMIC SERVICES
[Amendments to Parts 4-7 of the National Health Service Act 2006 consequential to these
services under this Act becoming administered by a District Health Authority’s Family
Health Services Committee]
Part 2
REGULATION OF HEALTH AND SOCIAL CARE
[Further amendments to Part 3 of the Health and Social Care Act 2012 consequential to
commissioning ending under this Act, and private companies providing services only
exceptionally as set out in sections 8(12) and 9(4).]
49
Part 3
PUBLIC INVOLVEMENT, LOCAL GOVERNMENT AND SCRUTINY
[Amendments to various enactments (such as the Health and Social Care Act 2008, the Local
Government and Public Involvement in Health Act 2007 and Part 12 of the National Health
Service Act 2006) consequential to the re-establishment under this Act of Community Health
Councils.]
Part 4
THE NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
[Amendments to Part 8 of the Health and Social Care Act 2012 relating to the general duties,
other functions and operation of NICE]
Part 5
HEALTH AND SOCIAL CARE INFORMATION CENTRE
[Amendments to Part 9 of the Health and Social Care Act 2012 consequential to abolition of
the NHS Commissioning Board and in order to protect the confidentiality of patient
information]
Part 6
CHARGING
[Amendments to Part 9 of the National Health Service Act 2006 relating to charging, such as
the power to charge generally; charging for dental services; charging for local pharmaceutical
services; charging for optical appliances and exemptions]

50
Part 7
PROTECTION OF NHS FROM FRAUD AND OTHER UNLAWFUL ACTIVITIES
[Amendments to Part 10 of the National Health Service Act 2006 relating to disclosure
notices and offences]
Part 8
PROPERTY AND FINANCE
[Amendments to Part 11 of the National Health Service Act 2006 relating to property and
finance issues, such as acquisition and use of property, transfers, raising money, the
formation of companies, finance, accounts and audit]
Part 9
MISCELLANEOUS
[Amendments to miscellaneous provisions contained in Part 13 of the National Health
Service Act 2006, such as those relating to independent advocacy services, joint working
with the prison service, emergencies, local social services authorities, community services,
university teaching and research, sale of medical practices, price of medical supplies, and use
of facilities in private practice]





























