Embed Size (px)
Citation preview

Ken HoChair, Centres for Health Research, Princess Alexandra Hospital
Professor of Medicine, University of QueenslandAdjunct Professor, QUT
Princess AlexandraHospital
The performance/adequacy of current laboratory assays
for GH and IGF-1

Clinical Utility of GH and IGF-1 Assays
Is there a problem?
What is the source?
How to fix it?

What I expect from laboratories providingGH and IGF-1 results
1. Clear what are normal and abnormal
2. Make clinical decisions against published data or guidelines
3. Does not matter which laboratory provides the results

Diagnosis Treatment MonitoringGHDeficiency
GH
IGF-1
< 3 ug/L to ITT*< 6 ug/L to arg-GHRH*< 3 ug/L to glucagon*
Normal range
Acromegaly GH <1ug/L to OGTT†
IGF-1 Elevated Normal range
Clinical Utility of GH and IGF-1 Assays
* Consensus Guidelines of Endocrine Society and GRS† Consensus Guidelines of Endocrine Society and Pituitary Society

A 24 year old man, previously treated in childhood with GH for short stature,is assessed for GH replacement in adult life. He underwent normal pubertaldevelopment at the expected age.
He complains of being overweight, lethargic and lacking energy but otherwiseis in good health.
His height is 166 cm, weight 75 kg and BMI 28 kg/m².
Results from an ITT: BSL mmol/L 4.6 2.0
GH mIU/L 2.6 9.1 (Guidelines < 3 ug/L)
Should he be replaced with GH?
Case 1

Case 2
A 64 year old woman presents with 20 year history of progressive weightgain (70 to 90 kg), lethargy, arthralgia and daytime sleepiness.
Her husband complains of heavy snoring and increasing frequency of chokingduring sleep. She had previously seen an endocrinologist who considered adiagnosis of acromegaly unlikely. An oral GTT revealed the following:
Blood glucose mmol/L 6.4 10.8
GH mIU/L 7.2, 6.6, 5.4, 3.5, 2.5, 2.5, 2.4
IGF-1 ng/mL 280 (RR 110 – 350)
Does she have acromegaly?
Case 2

7
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
00 1 2 3 4 5 6 7 8 9 10 11 12 13 14
GH (m
U/L
)
Method
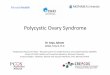
Pokrajac A et al. Clin Endocrinol (Oxf) 2007;67:65–70
The choice assay determines whether theGH nadir is normal
Interpreting GH nadirs from 14 assaysfor diagnosis of acromegaly

Reference Ranges

GH Reference Ranges
Beckman Coulter Males < 1.4 ug/LFemales < 5.2 ug/L
Roche < 2.5 ug/L
Immulite Males < 3.1 ug/LFemales < 8.1 ug/L

GH Normal Ranges
PLATFORMSEndo QAP Cycle 43
#BC Access 1BC Unicel 2IDS iSyS 0Immulite 40Liaison 3Roche 9
UNITSEndo QAP Cycle 43
mU/L (primary unit) 34ug/L 21
REFERENCE INTERVAL SURVEY
BC (1) 0 - 10Roche (3) 0 - 2.5Immulite (11) 0 - 10
<5.9 - >13.9
<5.9 8.4 9.9 11.4 >13.9
Reference Interval Survey - hGH
GH (mU/L)Reproduced with permission from RCPAQAP

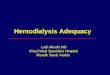
GH secretion
0
10
20
30
40
50
Clocktime
Sleep
0
10
20
30
40
50
GH
mIU
/L
GH
mIU
/L
0800 2000 0800 0800 2000 0800
Sleep
Normal Acromegaly
Clocktime
Reference Ranges provided by kits and labs are meaningless

Case 2
A 64 year old woman presents with 20 year history of progressive weightgain (70 to 90 kg), lethargy, arthralgia and daytime sleepiness.
Her husband complains of heavy snoring and increasing frequency of chokingduring sleep. She had previously seen an endocrinologist who considered adiagnosis of acromegaly unlikely. An oral GTT revealed the following:
Blood glucose mmol/L 6.4 10.8
GH mIU/L 7.2, 6.6, 5.4, 3.5, 2.5, 2.5, 2.4
IGF-1 ng/mL 280 (RR 110 – 350)
Does she have acromegaly?
Case 2

IGF-I Reference range
13
Brabant G. et al. / Horm Res 2003
Details of RR from commercial kits are obscureBroad adult RRs are providedAge/gender stratified RR are not provided

What is a “normal” IGF-I?
03 March 2015 Bidlingmaier - How do I interpret GH andIGF-I assays? 14August 13 201414
Ranke et al., Clin Chem Lab Med 2003
700 samples from healthy adultsmeasured by 4 IGF-I assays
Values cannot be transfered between IGF assaysReference intervals need to be method specific!

Adopted Reference Ranges

Conclusion1. Must be physiologically meaningful
2. Must be method-specific
3. Established from large normative data
4. If “adopted or adapted” must be undertaken byvalidated harmonisation methods
Reference Ranges

Is the performance of current laboratory
assays for GH and IGF-1 adequate?
NO!

Sources of discourdance between Assays
Units of measurementStandardsCalibratorsAntibodyMatrixBinding Protein(s)

Units of Measurement
GH mIU/L, ug/L
IGF-1 U/mL, ug/L, nmol/L
What is the conversion factor?

International Standards
GH 1969 66/217 Pituitary 2.0 U/mg1982 80/585 Pituitary 2.6 U/mg1994 88/624 rec 22k 3.0 U/mg1998 98/574 rec 22k 3.0 U/mg
IGF-1 1990 87/518 ?2008 02/254 rec IGF-1

Issues in Quantification of GH
Heterogeneity: isoforms, dimers, post-translational, bound forms of GH in blood
Standards: Does using pure rh22k GH appropriate for the heterogeneityof GH in blood
Antibody: Does specificity for 22k GH appropriate for biological heterogeneity

• The IRR 87/518 IGF-1 is not rhIGF-1 (70aa) but Met-1 rhIGF-1 (71aa)
• Is of low purity (44%) and assigned a protein content higher than thatdetermined by QAAA
• Protein content assigned by consensus estimates in IGF-1 RIA’s from 9laboratories
• Protein content not verified by physico-chemical analysis
IGF-1 Standards and Assay AccuracyQuarmby et al JCEM 1998; 83:1211

HPLC Analysis of WHO IGF-1 87/518
Quarmby et al JCEM 1998; 83:1211
The First International Reference Reagent for IGF-I

Improving Assay Comparability
Standardisation and Harmonisation

Consensus Statement on the Standardization andEvaluation of Growth Hormone and Insulin-like
Growth Factor AssaysClinical Chemistry 57:4:555–559 (2011)
David R. Clemmons,1* on behalf of the conference participantsGH Research SocietyIGF SocietyInternational Federation of Clinical Chemisty
Contributors to the Consensus Statement:Alecia Algeciras-Schimnich, Margherita Banci, Gerhard Baumann, Robert Baxter, Martin Bidlingmaier,Beverly Biller, David E. Bruns, Felipe Casanueva, Phillippe Chanson, Jens Christiansen, PeterClayton, David Clemmons, Pinchas Cohen, Cheri Deal, Andy Ellis, Robin A. Felder, Pamela Freda,Jan Frystyk, Richard Fulanetto, H. Mario Geysen, Shelia Hanna, Philip Harris, Ken K.Y. Ho, AndrewHoffman, Jeff Holly, Reiko Horikawa, Gudmundur Johnannsson, Anna-Marie Kappelgaard, SusanKirshner, David Kleinberg, John Kopchick, Derek LeRoith, Saul Malozowski, Kathy Maugh, A. WayneMeikle, Shlomo Melmed, Pharis Mohideen, Clement Olivier, Bernhard Saller, Rudolf Schemer, AkiraShimatsu, Christian Strasburger, Catharine M. Sturgeon, Mario Thevis, Michael Thorner, PeterTrainer, Yi Tsong, Mary Lee Vance, Gwen Wark, and Ingrid Zegers.
Queensland

• Calibration against a single universally accepted• Define specificities of the antibodies• Standardise preanalytical conditions• Matrix calibrators mimic human serum• Participation in an external quality assessment program that uses
commutable materials• Global advisory group to facilitate the exchange of proficiency
testing/external quality assessment information• Meaningful normative data
General Requirements forImproving Assay Comparability

GH
Calibration against WHO IRP 98/574 (recombinant 22K)Use recombinant GH in calibratorsReport concentrations in mass units - ug/L
IGF-I
Calibration against WHO Second IRP 02/254 (recombinant IGF-I)Use recombinant GH in calibratorsReport concentrations in mass units – ug/L or nmol/L
What can be Standardised?

Adopting Common GH Standard
A Nationwide Attempt to Standardize Growth Hormone AssaysTanaka et al Horm Res 2005;64: 6-11
Study Committee of the Foundation for Growth Science,Japan reported that:
Variation (CV) between GH measurements of commonsamples by different methods fell from 35% to 18%when rhGH was used as standards.

Harmonization of growth hormone measurementswith different immunoassays by data adjustment.Muller et al Clin Chem Lab Med 2011;49:1135
Assay comparison of 312 samples (GH 5-10 ug/L) from short children
•AutoDELFIA (PerkinElmer)•BC-IRMA (Beckman-Coulter),•ELISA (Mediagnost)•IMMULITE 2000 (Siemens)•iSYS (IDS)•Liaison (DiaSorin),•UniCel DxI 800 Access (BeckmanCoulter)•"In house"-RIA (Tübingen)
Method CV (%)Straight sample comparison 24.3Linear regression 13.2Conversion factor (assay mean/all method mean) 12.6Quartile transformation 11.4
Data adjustment can be used to reduce variability and improvecomparability between assays for diagnostic application

Reference Intervals for IGF-I From Birth to SenescenceJ Clin Endocrinol Metab, 2014, 99(5):1712–1721
iSYS, Immunodianostic SystemCalibrated against IRS 02/254> 15000 subjects from Europe, Canada and US

Bring together key stakeholders: Professional organisations,manufacturers, laboratory service providers, NATA, to agree there is aproblem and a need for a solution
RCPA and AACB-appointed working group to include harmonisation inexisting QAPs
Accelerate harmonisation programs including establishment ofcommutable reference samples necessary to achieve this
Formulate procedures for implementation after validation
Participation in and application of harmonisation procedures a necessarycondition of accreditation
Establishing Assay Utility for Australia

For laboratory-service providers• Select only IRP-calibrate kits with using recombinant standards• Report in mass units• Report harmonisation-adjusted values• Provide validatedy reference ranges
For RCPA and AACB and associated professional bodies• Designate an assay for reference benchmarking• Establish commutable reference samples to provide equivalence
between methods through harmonisation/QAPs• Develop stringent standards for reference range reporting• Engage NATA to implement recommendations for achieving
standardisation and harmonisation through accredation
Establishing Assay Utility for Clinicians

Acknowledgment
• Lyn Boscato, St. Vincent’s Hospital, Sydney
• Martin Bidlingmaier, Munich

Calibrators are a Black Box
• What standards
• Have they been calibrated against IRPs
• What is the matrix
• BP content