Embed Size (px)
Citation preview
1
The Pediatric Infectious Disease Journal Publish Ahead of Print
DOI: 10.1097/INF.0000000000002015
Performance of Tuberculin Skin Tests and Interferon-γ Release Assays in
Children Younger Than 5 years
Eneritz Velasco-Arnaiza,b
, MD, Antoni Soriano-Arandesc, MD, PhD, Irene Latorre
d,
PhD, Neus Altetc, MD, PhD, José Domínguez
d, PhD, Clàudia Fortuny
a,b,e,f, MD, PhD,
Manuel Monsonísg, MD,
Marc Tebruegge
h,i,j,k*, MD, MRCPCH, DTM&H, MSc, PhD,
and Antoni Noguera-Juliana,b,e,
f*, MD, PhD
Address correspondence to (and address for reprints): Antoni NOGUERA-
JULIAN, MD, PhD, Passeig de Sant Joan de Déu 2, 08950 Esplugues de Llobregat,
Barcelona (Spain), e-mail address: [email protected], Phone number: +34
93 280 40 00; fax number: +34 93 203 39 59
Abbreviated title: TST and IGRA in Children Younger Than 5 Years
Running head: TST and IGRA in Young Children
Affiliations: aMalalties Infeccioses i Resposta Inflamatòria Sistèmica en Pediatria.
Unitat d´Infeccions, Servei de Pediatria. Institut de Recerca Pediàtrica Hospital Sant
Joan de Déu; Barcelona, Spain. bDepartament de Pediatria, Universitat de Barcelona;
Barcelona, Spain. cInstitut Català de la Salut. Unitat de Tuberculosi Hospital
Universitari Vall d’Hebrón-Drassanes. Barcelona, Spain. dInstitut d’Investigació
Germans Trias i Pujol. CIBER Enfermedades Respiratorias. Universitat Autònoma de
Barcelona. Badalona, Spain. eCIBER de Epidemiología y Salud Pública (Ciberesp,
Spain). fRed de Investigación Transalacional en Infectología Pediátrica (RITIP, Spain).
gServei de Microbiologia. Hospital Sant Joan de Déu. Barcelona, Spain.
hAcademic Unit
of Clinical and Experimental Sciences, Faculty of Medicine & Global Health Research
Institute, University of Southampton, Southampton, United Kingdom. iDepartment of
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
2
Paediatric Infectious Diseases & Immunology, Evelina London Children’s Hospital,
Guy’s and St. Thomas’ NHS Foundation Trust, London, UK, United Kingdom. jGreat
Ormond Street Hospital Institute of Child Health, University College London, London,
UK. kDepartment of Paediatrics, The University of Melbourne, Parkville, Australia.
*Both authors share credit for senior authorship.
Conflicts of Interest and Source of Funding:
Dr. Tebruegge has received QuantiFERON-TB Gold assays at reduced cost for related
research projects from the manufacturer (Cellestis/Qiagen). The manufacturer had no
influence on the study design, data interpretation, writing of the manuscript or decision
to submit the data for publication. The remaining authors have no potential conflicts of
interest to disclose.
Dr. Domínguez is funded by the Miguel Servet program of the Instituto de Salud Carlos
III (Spain). This research was partially supported by different grants from the Instituto
de Salud Carlos III (PI 13/01546, PI 13/01740 and ICI14/00228), integrated in the Plan
Nacional de I+D+I and co-funded by the ISCIII-Subdirección General de Evaluación
and the Fondo Europeo de Desarrollo Regional (FEDER). Dr. Tebruegge was supported
by a Clinical Lectureship provided by the UK National Institute for Health Research and
funding provided by the Technology Strategy Board/Innovate U.K.
Key words: Bacillus Calmette-Guérin vaccine; infant; latent tuberculosis infection;
non-tuberculous mycobacteria; tuberculosis
Acknowledgements
The authors thank the patients and their families for kindly agreeing to take part in this
study.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
3
ABSTRACT
Background :Available data to assess the optimal diagnostic approach in infants and
pre-school children at risk of tuberculosis (TB) are limited.
Methods: We conducted a prospective observational study in children younger than 5
years undergoing assessment with both tuberculin skin tests (TST) and QuantiFERON-
TB Gold In-Tube® (QFT-GIT) assays at two tertiary TB Units in Barcelona, Spain.
Results: 383 children were included. One of 304 participants considered uninfected
developed active TB during follow-up (median [IQR]: 47 [30;48] months), compared
with none of 40 participants with latent TB infection (follow-up since completion of
anti-TB treatment: 42 [32;45] months). Overall test agreement between TST and QFT-
GIT was moderate (κ=0.551), but very good in children screened after TB contact
(κ=0.801) and in BCG-unvaccinated children (κ=0.816). Discordant results (16.8%, all
TST+/QFT-GIT negative) were mainly observed in new-entrant screening and in BCG-
vaccinated children. Children with indeterminate QFT-GIT results were on average
younger than those with determinate results (median age: 12 versus 30 months;
p<0.001). The sensitivity of TSTs and QFT-GIT assays in children with confirmed
active TB was 100% (95%CI: 79.4-100%) and 93.7% (95%CI: 69.8-99.8%),
respectively. In patients with latent TB infection or active TB there was no correlation
between age and antigen-stimulated interferon-gamma responses (r=-0.044, p=0.714).
Conclusions: In young BCG-unvaccinated children with recent TB contact a dual
testing strategy using TST and QFT-GIT in parallel may not be necessary. However,
TST+/QFT-GIT negative discordance is common, and it remains uncertain if this
constellation indicates TB infection or not. In active TB, QFT-GIT assays do not
perform better than TSTs.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
4
Introduction
Children younger than 5 years infected with Mycobacterium tuberculosis (MTB) are at
greater risk of progression to active tuberculosis (TB) and developing severe and
disseminated forms of TB than are adults. In infants the rate of progression is up to 40-
50% in the first 2 years after primary infection.1-3
In the absence of a gold standard, the diagnosis of latent tuberculosis infection (LTBI)
in infants and toddlers remains challenging, because of the limitations of current
immune-based diagnostic tests, the in vivo tuberculin skin test (TST) and ex vivo
interferon-gamma (IFN-γ) release assays (IGRAs).4,5
Moreover, the non-specific
clinical presentation of active TB and the comparatively low diagnostic yield of
microbiological investigations in this age group commonly result in delays in
establishing the diagnosis of active TB.2,6
Commercially available IGRAs detect circulating T-cells that produce IFN-γ in
response to stimulation with MTB-specific antigens that are absent from all Bacillus
Calmette-Guérin (BCG) vaccine strains and from most non-tuberculous mycobacteria
(NTM).3,7
Both TSTs and IGRAs indicate host sensitization to mycobacterial antigens
by detecting cell-mediated immune responses, which are critical in preventing
progression to active TB.8 The physiological immaturity of the immune system of
infants and toddlers not only results in a reduced ability to contain MTB infection (i.e.,
prevent progression),9 but may also result in impaired diagnostic accuracy of TSTs and
IGRAs.10,11
In many industrialized countries IGRAs have largely replaced TSTs as the main TB
screening tool in adults.12-14
The existing evidence regarding the optimal diagnostic
approach for children younger than 5 years at risk of LTBI is limited. Recent U.S.,
Canadian and European guidelines recommend the preferential use of TSTs irrespective
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
5
of BCG vaccination status in this age group, and consider IGRAs as a complementary
tool to improve sensitivity and specificity.3,10,12-14
The Spanish Society of Pediatric
Infectious Diseases also recommends using TSTs as the first line investigation in
children younger than 5 years after TB contact.15
In those with a negative TST result,
performing an IGRA test is recommended. In patients with a positive TST result, IGRA
testing is considered unnecessary unless there is a history of prior BCG vaccination.
Recent shortages of purified protein derivative (the test substance used for TSTs) have
led to changes in TB screening practices, increasing the need for more robust data on
IGRAs in young children.16
The aim of this study was to evaluate the performance of TSTs and QuantiFERON-TB
Gold In-Tube (QFT-GIT) assays in the diagnostic evaluation of LTBI and active TB in
previously healthy children younger than 5 years.
Materials and methods
Study population
We performed a prospective observational study of children younger than 5 years at risk
of TB undergoing assessment at one of two tertiary Pediatric TB Units, the Drassanes-
Vall d’Hebrón (DVH) Unit in Barcelona City or the Hospital Sant Joan de Déu (SJD) in
Regió Sanitària Barcelona Sud. Both units are located in Catalonia, Spain and are
jointly covering a population of more than 2,9 million inhabitants, of which 15.8% are
younger than 15 years.17
In Catalonia, the incidence of TB gradually decreased from
21.6/100,000 in 2004 to 16.6/100,000 in 2014. In 2014 the TB incidence in children
aged 0 to 4 years was 12.4/100,000.17
BCG vaccination is not part of the routine
immunization program in Catalonia.
Children were eligible for participation if they were assessed for LTBI (either in the
context of contact tracing or as part of new entrant screening) or were investigated for
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
6
suspected active TB, and underwent both TST and QFT-GIT testing simultaneously.
Children with a previous diagnosis of LTBI or active TB, chronic medical conditions
(including HIV infection) and/or receiving immunosuppressive therapy (including
corticosteroids) were excluded from participation. The study commenced at DVH in
January 2005 and at SJD in February 2012, and concluded in July 2015. The study was
approved by the institutional ethics review boards of both units. Written informed
consent was obtained from the parents/guardians of each participant.
Demographic characteristics (age, gender, country of birth, family origin, BCG
vaccination history and presence of BCG scar) were recorded on a standardized data
collection sheet. Participants were classified as BCG-vaccinated if they had a visible
scar in the deltoid region and/or a positive vaccination history. In addition, the primary
reason for performing the assessment was categorized as follows: a) clinical and/or
radiological suspicion of active TB, b) contact tracing following contact with a TB
index case, or c) new-entrant screening in immigrants and international adoptees from
high TB prevalence countries.
TST and IGRA testing
TSTs were performed by intradermal injection of 0.1 ml (2TU) of purified protein
derivative RT23 (Tuberkulin PPD RT23 SSI, Statens Serum Institut, Copenhagen,
Denmark), with results read after 48-72 hours. The cut-offs for a positive TST result
were defined according to national guidelines as follows: ≥5 mm of induration in
children assessed for clinically and/or radiologically suspected active TB and in children
assessed following TB contact, and ≥10 mm in children undergoing new-entrant
screening.15
QFT-GIT (Cellestis/Qiagen, Carnegie, Australia) assays were performed in
a fully-accredited routine diagnostic laboratory at each centre and interpreted according
to manufacturer's instructions.18
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
7
Case definitions and follow-up
The diagnosis of active TB was made on the basis of epidemiological, clinical,
radiological and microbiological findings according to consensus criteria described
elsewhere,19
independent of TST and QFT-GIT results. Active TB cases were classified
as a) definite, microbiologically-confirmed cases when MTB was detected by culture
(Lowenstein-Jensen or liquid Middlebrook 7H9+OADC media) or molecular analysis
(AMPLICOR MTB-Test, Roche Molecular Systems, NJ, U.S.), and b) probable, non-
microbiologically-confirmed cases.
In children assessed following contact with a TB index case, LTBI was defined as the
absence of clinical and radiological signs of active TB in combination with a positive
TST and/or QFT-GIT result, independent of the BCG vaccination status.15
In accordance with national guidelines, in BCG-vaccinated children undergoing new-
entrant screening a positive TST result in combination with a negative QFT-GIT result
was interpreted as being the result of BCG vaccination, and the child was considered
uninfected. In the absence of BCG vaccination, a positive TST and/or QFT-GIT result
was considered to be evidence for LTBI.15
In both units children who undergo TB screening are routinely followed up clinically
every 3 to 6 months for at least 2 years. Repeat TB testing or radiological investigations
are not done routinely, but are performed if patients develop symptoms or signs
suggestive of active TB.
Statistical methods
Statistical analyses were carried out using SPSS version 21.0 (IBM Corp., Armonk, NY,
U.S.). Categorical variables are reported as proportions with 95% confidence intervals,
and continuous variables as medians with interquartile ranges (IQRs). Chi-square tests
and Fisher’s exact tests were used to compare qualitative variables, and Mann-Whitney
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
8
U and Kruskal-Wallis tests for quantitative variables. Confidence intervals around
proportions were calculated with the ‘exact’ method. Spearman's Rho test was used to
analyze correlations between test results. Statistical significance was defined as a p-
value <0.05.
Total percentage agreement and Cohen's kappa coefficient (κ) with standard error (SE)
were used to quantify concordance between TST and QFT-GIT results; indeterminate
QFT-GIT results were excluded from this particular analysis. Strength of agreement was
defined as poor (κ≤0.2), fair (0.2<κ≤0.4), moderate (0.4<κ≤0.6), good (0.6<κ≤0.8) and
very good (κ>0.8). Sensitivity estimates of TST and QFT-GIT were based exclusively
on active TB cases.
Results
A total of 383 children were recruited into the study, comprising 207 at DVH and 176 at
SJD. The participants’ demographics, the reason for their assessment, and TST and
QFT-GIT results are summarized in Table 1. At assessment, the age distribution of the
cohort was: 0-6 months, n=22; 6-12 months, n=32; 12-24 months, n=84; 24-36 months,
n=94; 36-48 months, n=88; and 48-60 months, n=63.
Children vaccinated with BCG were on average older than those without a history of
BCG vaccination (median [IQR]: 37 [24;49] vs. 28 [16;40] months, p<0.001), and
mainly underwent assessment because of new entrant screening (66/97, 68.0%). BCG-
vaccinated children were diagnosed with LTBI more frequently than those without a
history of BCG vaccination (23/100, 23.0% vs. 16/269, 5.9%, p<0.001; BCG status
unknown in 14 cases).
A total of 304 children were classified as uninfected according to the study definitions.
In this subgroup the median follow-up period was 47 months (IQR: 30;48). In 7/304
participants (2.3%) the follow-up period was 12-24 months at the end of the study
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
9
period (none followed up for less than one year). One patient (0.3%) in this subgroup
developed active TB during follow-up - a Pakistani boy initially assessed at 16 months
of age as part of new entrant screening. At that time the QFT-GIT result was negative
and the TST induration was 8 mm, which was attributed to prior BCG vaccination. Two
years later he presented with symptoms and radiological findings consistent with
intrathoracic TB (TST induration: 15mm; QFT-GIT not performed), but cultures were
negative. The only additional risk factor for TB identified between the two assessments
was a 2-month visit to Pakistan. The child fully recovered with 6 months of anti-TB
treatment.
All children diagnosed with LTBI (n=40) received chemoprophylaxis (isoniazid and
rifampicin for 3 months, n=28; or 6-9 months of isoniazid monotherapy, n=12) as per
national guidelines.15
None of these patients had significant drug-related adverse events
or developed active TB during the follow-up period (median [IQR] follow-up since
completion of anti-TB treatment: 42 [32;45] months).
Thirty-nine patients were diagnosed with active TB (n=32 intrathoracic disease; n=16
microbiologically-confirmed; all confirmed cases had fully drug-susceptible strains of
MTB). All children responded to standard anti-TB treatment (2-month induction phase
with three drugs until March 2009, four-drug regimen since then, followed by isoniazid
and rifampicin for a minimum of 4 months).15
The distribution and concordance between TST and QFT-GIT results according to the
reason for assessment, the BCG vaccination status and the final diagnosis are shown in
Table 2; complete TST and QTF-GIT results are shown in (Table Supplemental Digital
Content 1, http://links.lww.com/INF/D72). Overall, agreement between tests was
moderate (83.2%, κ=0.551). However, in children tested as part of contact tracing and in
children without a history of BCG vaccination the concordance was higher and the test
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
10
agreement very good (94.4%, κ=0.801 and 94.6%, κ=0.816, respectively).
Discordance between TST and QFT-GIT results was observed in 62/369 participants
(16.8%; excludes n=14 with indeterminate QFT-GIT test results); all had a TST
positive/QFT-GIT negative (TST+/QFT-GIT-) result constellation. Discordant results
were mainly observed among BCG-vaccinated children (47/62, 75.8%; BCG status
unknown in one patient), in whom agreement between tests was poor (κ=0.190). Most
of these patients (47/62, 75.8%) were classified as uninfected according to the study
definitions. Among the 14 BCG-unvaccinated patients with discordant results the final
diagnoses were: NTM lymphadenitis (n=9, culture-confirmed in 4 cases; all recovered
fully without anti-TB treatment), LTBI (n=4) and probable active TB (n=1). The
diagnosis in the latter, who was investigated after recent TB contact, was based on a
positive TST (7mm induration) and hilar lymphadenopathy in combination with
pulmonary nodules on chest computer tomography imaging.
Of the 39 cases with active TB, 30 had concordantly positive TST and QFT-GIT results,
while five had concordantly negative results. Three cases had a TST+/QFT-GIT-
discordant result constellation; one case had a positive TST result and an indeterminate
QFT-GIT result. All concordantly negative and all discordant results occurred in
patients with probable disease. The five children with concordantly negative results all
had symptoms and radiological findings consistent with active TB, and responded
clinically to anti-TB treatment. In microbiologically-confirmed cases (n=16) TST
results were universally positive, and 15 cases had a positive QFT-GIT result; one had
an indeterminate QFT-GIT result (Table 2 and Table 3, Supplemental Digital Content 1,
http://links.lww.com/INF/D72). Therefore, the sensitivities of TSTs and QFT-GIT
assays in children with confirmed active TB were 100% (95%CI: 79.4-100%) and
93.7% (95%CI: 69.8-99.8%; p=0.388), and in children with confirmed or probable
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
11
active TB combined 87.2% (95%CI: 72.6-95.7%) and 77.0% (95%CI: 60.7-88.9%;
p=0.221), respectively.
Indeterminate QFT-GIT results occurred in 14/383 (3.6%) children and universally were
due to inadequate IFN-γ responses in the positive control sample. Children with
indeterminate QFT-GIT results were significantly younger than those with determinate
(i.e. positive or negative) results [median age (IQR): 12 (6;19) vs. 30 (18;42) months,
p<0.001]. QFT-GIT indeterminate results were more common in children aged <2 years
(8.7%) than in older ones (0.8%; p<0.001).
In participants with LTBI and active TB the diameter of TST induration was similar
(median[IQR]: 14[10;17] vs. 15[10;18] mm, respectively; p=0.581). Also, the
background-corrected antigen-stimulated IFN-γ responses in the QFT-GIT assay did not
differ significantly between those two groups (median[IQR]: 1.37[0.20;10.72] vs.
4.96[1.26;10.50] IU/mL, respectively; p=0.241).
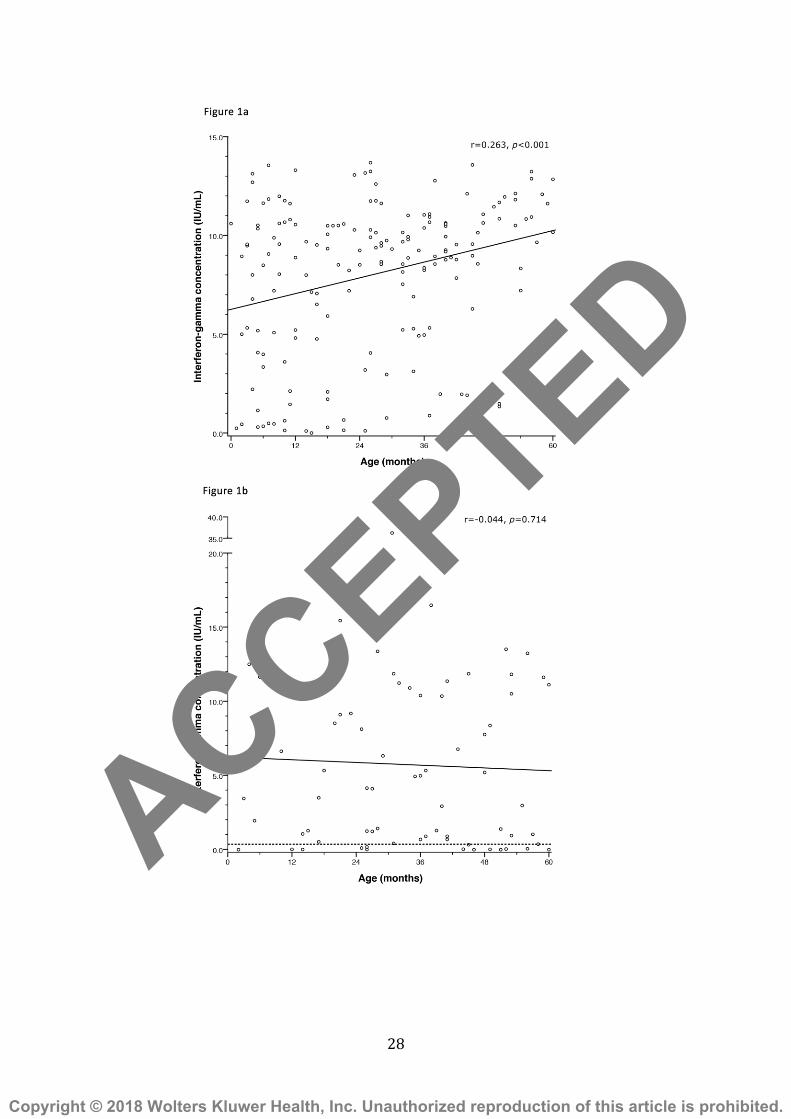
In the whole cohort there was a positive correlation between the diameter of the TST
induration and the magnitude of background-corrected antigen-stimulated IFN-γ
responses in the QFT-GIT assay (r=0.601, p<0.001). A positive correlation was also
observed between age and the diameter of TST induration (r=0.187, p<0.001).
Furthermore, there was a positive correlation between age and background-corrected
mitogen control responses in the QFT-GIT assay (r=0.263, p<0.001; Figure 1a). In
contrast, in children diagnosed with LTBI or active TB, background-corrected antigen-
stimulated IFN-γ responses were age-independent (r=-0.044, p=0.714; Figure 1b).
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
12
Discussion
Most international guidelines on the management of children with suspected TB
highlight that IGRAs may perform worse in young children compared to adults, but also
acknowledge that the data to support this view remain relatively limited.10,12-14
A
growing number of studies have assessed the performance of IGRAs in children,
including seven meta-analyses.20-26
However, the interpretation of the findings of these
meta-analyses is complex because of the large heterogeneity of the studies included
(background TB prevalence rates, variations in participants’ ages, and varying
proportions of immunocompromised participants) and also methodological differences
(varying TST cut-offs and the range of microbiological investigations employed).
Importantly, our study is one of the largest studies specifically evaluating the
performance of TSTs and QFT-GIT assays in children younger than 5 years in a low-
prevalence setting to date.
Overall, 79.4% of children in our cohort were classified as uninfected. The observation
that only one (0.3%; 118.4 cases per 100,000 patient-years) of these children developed
active TB during a median follow-up period of 47 months is reassuring as the period of
greatest risk of progression to disease is within the first 2 years after primary
infection.1,4,27
In our cohort, the test agreement between TSTs and IGRAs was good in non-BCG-
vaccinated children and in children undergoing contact screening, which is consistent
with the findings reported by other pediatric studies in low TB burden countries.28-30
These results suggest that a dual immunodiagnostic testing strategy (i.e., use of both
tests simultaneously), an approach used by many pediatric specialists,5 may not be
necessary in these particular patient populations. The proportion of indeterminate IGRA
results (3.6%) in our cohort was relatively small compared to other pediatric studies,
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
13
which have typically observed indeterminate IGRA results in >5-10% of the study
population.30-35
In keeping with other pediatric studies, a significant proportion (16.8%) of our study
populations had discordance between TST and IGRA results.36-38
All of these
participants had a TST+/QFT-GIT- result constellation. In the absence of a gold
standard for LTBI, it remains uncertain whether individuals with discordant TST and
IGRA results are TB-infected or TB-uninfected. Since TST+/IGRA- discordance is
more commonly observed in BCG-vaccinated children, some authors have argued that
this constellation reflects false-positive TST results caused by immune sensitisation
induced by the BCG vaccine. However, data from a large meta-analysis that included
more than 240,000 children immunised with BCG in the neonatal period suggest that
only 8.5% of vaccinees become TST-positive as a result of BCG vaccination.39
In
addition, the obvious confounder is that most children who are BCG-vaccinated are
from high TB burden countries or born to high-risk populations, meaning their TB
exposure risk is generally greater than that of BCG-unvaccinated children. Notably,
almost a quarter of the children with TST+/QFT-GIT- discordance in our study had not
been vaccinated with BCG, and consequently their positive TST result cannot be
attributed to vaccine-induced immune responses. It has been postulated that in some
cases TST+/IGRA- discordance may reflect false-positive TST results caused by
exposure to NTM; some evidence for this has been provided by a study that used an ex-
vivo NTM-sensitin ELISPOT assay.40
Interestingly, in our study some non-BCG-
vaccinated children with TST+/IGRA- discordance had microbiologically-confirmed
NTM lymphadenitis. However, compelling data from a recently published study using
detailed immunological analyses suggest that children with TST+/IGRA- discordance
are a heterogeneous group comprising both TB-infected and TB-uninfected
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

14
individuals.41
Considering these uncertainties, most experts recommend to treat children
with risk factors for TB and discordant TST/IGRA results with chemoprophylaxis,
particularly as adverse events related to chemoprophylaxis are rare in childhood.5
We found no significant differences in TST indurations or antigen-stimulated IFN-γ
responses in the QFT-GIT assay between LTBI and active TB cases, confirming
previous observations that neither TSTs nor QFT-GITs can be used to discriminate
between LTBI and active TB.11,34,37,42
Also, our data confirm that QFT-GIT assays do
not have higher sensitivity than TSTs in children with active TB, which aligns with
previously published observations.29,34,35,43
We found no correlation between age and the magnitude of antigen-stimulated IFN-γ
responses in QFT-GIT assays in children with LTBI or active TB. This finding is
surprising considering existing data suggesting that T-cell-mediated immune responses
are less robust in young children because of incomplete immune maturation.44,45
Previous studies have highlighted that phytohaemagglutinin-induced IFN-γ (positive
control) responses in the QFT-GIT assay are significantly lower in young children than
in adults, in part contributing to the high proportions of indeterminate IGRA results in
children.30,31
Some authors have therefore argued that age-specific cut-offs should be
used for positive control responses, or suggested the use of alternative control
stimulants.30,31,36
In our cohort, we observed a positive correlation between age and
positive control responses, and found that indeterminate results were more common in
younger patients, universally as a result of inadequate positive control responses.
Therefore, while age adjustment is likely needed for the evaluation of positive control
responses, our data suggest that such adjustment may not be required for antigen-
stimulated IFN-γ responses. However, we can not rule out with certainty that the
absence of a correlation between age and antigen-stimulated IFN-γ responses was due to
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
15
the relatively narrow age spectrum of our cohort.
Our study has a number of limitations in common with all previous studies investigating
IGRAs in children, namely the lack of a gold standard for LTBI, and the absence of
microbiological confirmation in a substantial proportion of active TB cases. Also, our
study did not include a control group of healthy children without known risk factors for
TB, and non-immigrant children were not routinely tested for HIV. However, the
prevalence of HIV infection in children and adolescents in Spain is estimated to be
below 5 per 100,000.46
Also, except for age, other factors known to be associated with
indeterminate QTF-GIT results, such as malnutrition and co-existing helminth
infections were not specifically investigated.47,48
Finally, it remains uncertain whether
our results can be extrapolated to the T-SPOT®.TB (Oxford/Immunotec, UK) or the
QuantiFERON®-TB Gold Plus assays (Cellestis/Qiagen, Australia).
Our study adds significantly to the knowledge base regarding the performance of TSTs
and IGRAs in infants and pre-school children in a low TB prevalence setting. In
children without prior BCG vaccination and those screened for LTBI as part of contact
investigations, there was very good agreement between both tests; in these patient
groups, a dual immunodiagnostic testing strategy may therefore not be necessary.
Similar to previous pediatric studies, a considerable proportion of the study population
had TST+/QFT-GIT- discordance, and it currently remains uncertain whether these
children are TB-infected or TB-uninfected. Although indeterminate QFT-GIT results
were relatively uncommon compared to other pediatric studies, we found that those
results occurred more commonly in children at the lower end of the age spectrum. QFT-
GIT assays did not have higher sensitivity than TSTs in children with probable and
confirmed active TB, highlighting that IGRAs should not replace TSTs as a first-line
adjunctive test in children with suspected active TB.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

16
References
1 Marais BJ, Gie RP, Schaaf HS, et al. The natural history of childhood intra-thoracic
tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J
Tuberc Lung Dis. 2004;8:392-402.
2 Newton SM, Brent AJ, Anderson S, Whittaker E, Kampmann B. Paediatric
tuberculosis. Lancet Infect Dis. 2008;8:498-510.
3 Starke JR; American Academy of Pediatrics Committee On Infectious Diseases.
Interferon-γ release assays for diagnosis of tuberculosis infection and disease in
children. Pediatrics. 2014;134:e1763-773.
4 Ritz N, Curtis N. Novel concepts in the epidemiology, diagnosis and prevention of
childhood tuberculosis. Swiss Med Wkly. 2014;144:w14000.
5 Tebruegge M, Ritz N, Curtis N, Shingadia D. Diagnostic tests for childhood
tuberculosis: past imperfect, present tense and future perfect? Pediatr Infect Dis J.
2015;34:1014-1019.
6 Pérez-Porcuna TM, Ascaso C, Ogusku MM, et al. Evaluation of new strategies for
the diagnosis of tuberculosis among pediatric contacts of tuberculosis patients.
Pediatr Infect Dis J. 2012;31:e141-146.
7 Lalvani A, Millington KA. T cell-based diagnosis of childhood tuberculosis
infection. Curr Opin Infect Dis. 2007;20:264-271.
8 Mack U, Migliori GB, Sester M, et al. LTBI: latent tuberculosis infection or lasting
immune responses to M. tuberculosis? A TBNET consensus statement. Eur Respir
J. 2009;33:956-973.
9 Vanden Driessche K, Persson A, Marais BJ, Fink PJ, Urdahl KB. Immune
vulnerability of infants to tuberculosis. Clin Dev Immunol. 2013;2013:781320.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
17
10 Mazurek GH, Jereb J, Vernon A, Lobue P, Goldberg S, Castro K. Updated
guidelines for using interferon gamma release assays to detect Mycobacterium
tuberculosis infection - United States, 2010. MMWR Recomm Rep. 2010;59(RR-
5):1-25.
11 Altet-Gómez N, De Souza-Galvão M, Latorre I, et al. Diagnosing TB infection in
children: analysis of discordances using in vitro tests and the tuberculin skin test.
Eur Respir J. 2011;37:1166-1174.
12 Menzies D. Canadian TB standards 7th edition. Canadian Thoracic Society,
Canadian Lung Association and Public Health Agency of Canada, February 2014.
Available from: http://www.respiratoryguidelines.ca/tb-standards-2013.
13 National Institute for Health and Clinical Excellence. Tuberculosis. NICE
guideline. Available from: https://www.nice.org.uk/guidance/ng33.
14 American Academy of Pediatrics. Tuberculosis. In: Kimberlin DW, Brady MT,
Jackson MA, Long SS, eds. Red Book: 2015 Report of the Committee on Infectious
Diseases. 30th ed. Elk Grove Village, IL: American Academy of Pediatrics 2015:
805-831.
15 Moreno-Pérez D, Andrés Martín A, Altet Gómez N, et al. Diagnosis of tuberculosis
in pediatrics. Consensus document of the Spanish Society of Pediatric Infectology
(SEIP) and the Spanish Society of Pediatric Pneumology (SENP). An Pediatr
(Barc). 2010;73:143.e1-143.14.
16 Tebruegge M, Buonsenso D, Brinkmann F, et al. European shortage of purified
protein derivative and its impact on tuberculosis screening practices. Int J Tuberc
Lung Dis. 2016;20:1293-1299.
17 Rodés Monegal A, López Espinilla M, García Lebrón M. [Epidemiological
situation and trends of tuberculosis in Catalonia; 2014 Annual Report. Prevention
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
18
and control of tuberculosis in Catalonia]. Barcelona: Agencia de Salut Pública de
Catalunya. Departament de Salut; January 2016. Available from:
http://canalsalut.gencat.cat/web/.content/home_canal_salut/professionals/temes_de_
salut/tuberculosi/documents/arxius/informe_anual_tuberculosi_2014.pdf.
18 QuantiFERON®-TB Gold (In-Tube Method) Package Insert. August 2006.
Cellestis/Qiagen, Australia. Available from:
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials
/MedicalDevices/MedicalDevicesAdvisoryCommittee/MicrobiologyDevicesPanel/
UCM260551.pdf.
19 Graham SM, Ahmed T, Amanullah F, et al. Evaluation of tuberculosis diagnostics
in children: 1. Proposed clinical case definitions for classification of intrathoracic
tuberculosis disease. Consensus from an expert panel. J Infect Dis. 2012;205(Suppl.
2):S199-208.
20 Mandalakas AM, Detjen AK, Hesseling AC, Benedetti A, Menzies D. Interferon-
gamma release assays and childhood tuberculosis: systematic review and meta-
analysis. Int J Tuberc Lung Dis. 2011;15:1018-1032.
21 Menzies D, Pai M, Comstock G. Meta-analysis: new tests for the diagnosis of latent
tuberculosis infection: areas of uncertainty and recommendations for research. Ann
Intern Med. 2007;146:340–354.
22 Machingaidze S, Wiysonge CS, Gonzalez-Angulo Y, et al. The utility of an
interferon gamma release assay for diagnosis of latent tuberculosis infection and
disease in children: a systematic review and meta-analysis. Pediatr Infect Dis J.
2011;30:694-700.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
19
23 Sun L, Xiao J, Miao Q, et al. Interferon gamma release assay in diagnosis of
pediatric tuberculosis: a meta-analysis. FEMS Immunol Med Microbiol.
2011;63:165-173.
24 Chiappini E, Accetta G, Bonsignori F, et al. Interferon-γ release assays for the
diagnosis of Mycobacterium tuberculosis infection in children: a systematic review
and meta-analysis. Int J Immunopathol Pharmacol. 2012;25:557-564.
25 Sollai S, Galli L, de Martino M, Chiappini E. Systematic review and meta-analysis
on the utility of Interferon-gamma release assays for the diagnosis of
Mycobacterium tuberculosis infection in children: a 2013 update. BMC Infect Dis.
2014;14(Suppl. 1):S6.
26 Laurenti P, Raponi M, de Waure C, Marino M, Ricciardi W, Damiani G.
Performance of interferon-γ release assays in the diagnosis of confirmed active
tuberculosis in immunocompetent children: a new systematic review and meta-
analysis. BMC Infect Dis. 2016;16:131.
27 Perez-Velez C, Marais B. Tuberculosis in children. N Engl J Med. 2012;367:348-
361.
28 Méndez-Echevarría A, González-Muñoz M, Mellado MJ, et al. Interferon-γ release
assay for the diagnosis of tuberculosis in children. Arch Dis Child. 2012;97:514-
516.
29 Chiappini, Bonsignori, Mazzantini, et al. Interferon-gamma release assay sensitivity
in children younger than 5 years is insufficient to replace the use of tuberculin skin
test in Western countries. Pediatr Infect Dis J. 2014;33:1291-1293.
30 Connell TG, Tebruegge M, Ritz N, Bryant PA, Leslie D, Curtis N. Indeterminate
interferon-gamma release assay results in children. Pediatr Infect Dis J.
2010;29:285-286.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
20
31 Tebruegge M, de Graaf H, Sukhtankar P, et al. Extremes of age are associated with
indeterminate QuantiFERON-TB Gold assay results. J Clin Microbiol.
2014;52:2694-2697.
32 Haustein T, Ridout DA, Hartley JC, et al. The likelihood of an indeterminate test
result from a whole-blood interferon-gamma release assay for the diagnosis of
Mycobacterium tuberculosis infection in children correlates with age and immune
status. Pediatr Infect Dis J. 2009;28:669-673.
33 Bergamini BM, Losi M, Vaienti F, et al. Performance of commercial blood tests for
the diagnosis of latent tuberculosis infection in children and adolescents. Pediatrics.
2009;123:e419-424.
34 Kampmann B, Whittaker E, Williams A, et al. Interferon-gamma release assays do
not identify more children with active tuberculosis than the tuberculin skin test. Eur
Respir J. 2009;33:1374-1382.
35 Bamford ARJ, Crook AM, Clark JE, et al. Comparison of interferon-γ release
assays and tuberculin skin test in predicting active tuberculosis (TB) in children in
the UK: a paediatric TB network study. Arch Dis Child. 2010;95:180–186.
36 Lighter J, Rigaud M, Eduardo R, Peng CH, Pollack H. Latent tuberculosis
diagnosis in children by using the QuantiFERON-TB Gold In-Tube test. Pediatrics.
2009;123:30-37.
37 Connell TG, Ritz N, Paxton GA, Buttery JP, Curtis N, Ranganathan. A three-way
comparison of tuberculin skin testing, QuantiFERON-TB Gold and T-SPOT.TB in
children. PLoS One. 2008;3:e2624.
38 Tsolia MN, Mavrikou M, Critselis E, et al. Whole blood interferon-γ release assay
is a useful tool for the diagnosis of tuberculosis infection particularly among Bacille
Calmette Guèrin-vaccinated children. Pediatr Infect Dis J. 2010;29:1137-1140.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
21
39 Farhat M, Greenaway C, Pai M, Menzies D. False-positive tuberculin skin tests:
what is the absolute effect of BCG and non-tuberculous mycobacteria? Int J Tuberc
Lung Dis. 2006;10:1192-1204.
40 Latorre I, De Souza-Galvão M, Ruiz-Manzano J, et al. Evaluating the non-
tuberculous mycobacteria effect in the tuberculosis infection diagnosis. Eur Respir
J. 2010;35:338-342.
41 Tebruegge M, Dutta B, Donath S, et al. Mycobacteria-specific cytokine responses
detect tuberculosis infection and distinguish latent from active tuberculosis. Am J
Respir Crit Care Med. 2015;192:485-499.
42 Latorre I, De Souza-Galvão M, Ruiz-Manzano J, et al. Quantitative evaluation of T-
cell response after specific antigen stimulation in active and latent tuberculosis
infection in adults and children. Diagn Microbiol Infect Dis. 2009;65:236-246.
43 Detjen AK, Keil T, Roll S, et al. Interferon-gamma release assays improve the
diagnosis of tuberculosis and nontuberculous mycobacterial disease in children in a
country with a low incidence of tuberculosis. Clin Infect Dis. 2007;45:322-328.
44 Dowling DJ, Levy O. Ontogeny of early life immunity. Trends Immunol.
2014;35:299-310.
45 Goenka A, Kollmann TR. Development of immunity in early life. J Infect.
2015;71(Suppl. 1):S112-120.
46 Área de Vigilancia de VIH y Comportamientos de Riesgo. Vigilancia
Epidemiológica del VIH y sida en España: Sistema de Información sobre Nuevos
Diagnósticos de VIH y Registro Nacional de Casos de Sida. Plan Nacional sobre el
Sida - S.G. de Promoción de la Salud y Epidemiología / Centro Nacional de
Epidemiología - ISCIII. Madrid; Nov 2016. Available from:
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
22
https://www.msssi.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/vigilancia
/InformeVIH_SIDA_2016.pdf.
47 Thomas TA, Mondal D, Noor Z, et al. Malnutrition and helminth infection affect
performance of an interferon-gamma release assay. Pediatrics. 2010;126:e1522-
1529.
48 Banfield S, Pascoe E, Thambiran A, Siafarikas A, Burgner D. Factors associated
with the performance of a blood-based interferon-γ release assay in diagnosing
tuberculosis. PLoS One. 2012;7:e38556.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
23
Figure legends
Figure 1. Correlation between age and IFN-γ concentrations.
Correlation between age and (1a) background-corrected IFN-γ concentration in the
mitogen-stimulated (positive control) sample of the QFT-GIT assay in 173 study
participants in whom quantitative data were available, and (1b) background-corrected
IFN-γ concentration in the antigen-stimulated sample in the 72 participants diagnosed
with LTBI or active TB, with fitted regression line; the dotted line represents the QFT-
GIT cut-off for positivity (≥0.35 IU/mL). The values shown are Spearman’s correlation
coefficients (r) and their corresponding p-value.
List of Supplemental Digital Content
- Table 3, which has been submitted as a .pdf file.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
24
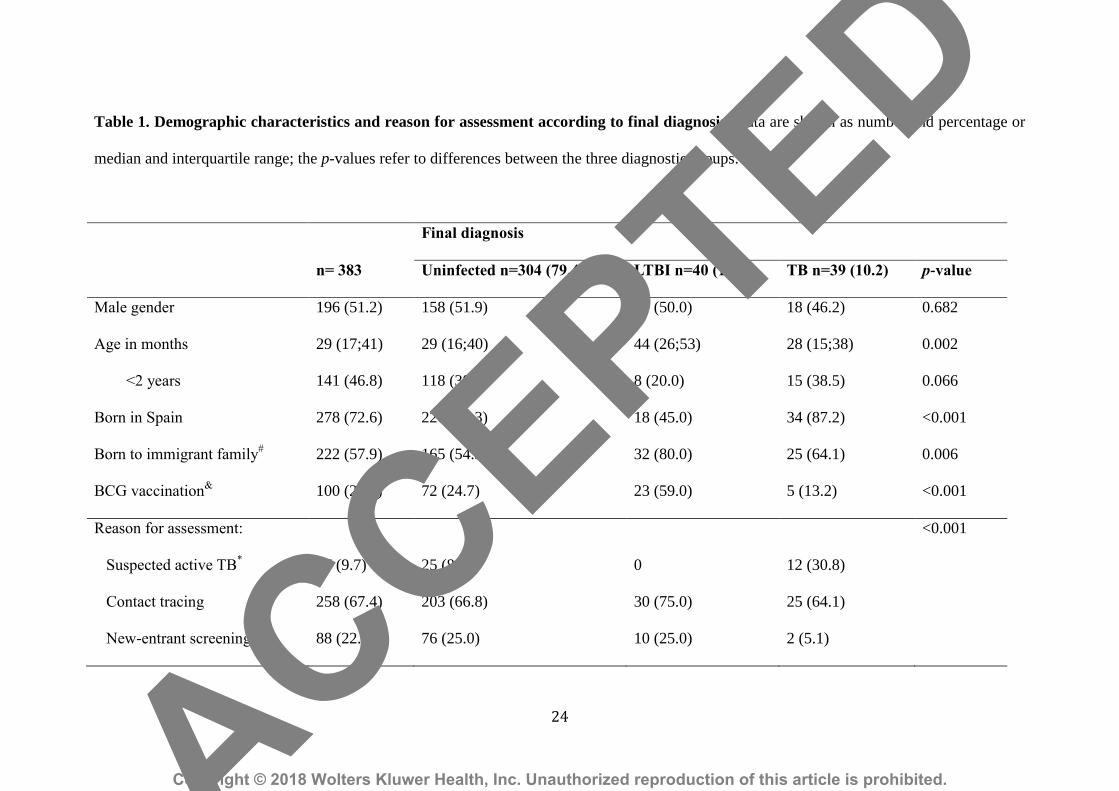
Table 1. Demographic characteristics and reason for assessment according to final diagnosis. Data are shown as number and percentage or
median and interquartile range; the p-values refer to differences between the three diagnostic groups.
Final diagnosis
n= 383 Uninfected n=304 (79.4) LTBI n=40 (10.4) TB n=39 (10.2) p-value
Male gender
Age in months
<2 years
Born in Spain
Born to immigrant family#
BCG vaccination&
196 (51.2)
29 (17;41)
141 (46.8)
278 (72.6)
222 (57.9)
100 (27.1)
158 (51.9)
29 (16;40)
118 (38.8)
226 (74.3)
165 (54.3)
72 (24.7)
20 (50.0)
44 (26;53)
8 (20.0)
18 (45.0)
32 (80.0)
23 (59.0)
18 (46.2)
28 (15;38)
15 (38.5)
34 (87.2)
25 (64.1)
5 (13.2)
0.682
0.002
0.066
<0.001
0.006
<0.001
Reason for assessment:
Suspected active TB*
Contact tracing
New-entrant screening
37 (9.7)
258 (67.4)
88 (22.9)
25 (8.2)
203 (66.8)
76 (25.0)
0
30 (75.0)
10 (25.0)
12 (30.8)
25 (64.1)
2 (5.1)
<0.001
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
25
#Families’ origins: Spain, n=150 (39.2%); other European countries, n=16 (4.2%); South America, n=61 (15.9%); Africa, n=59 (15.4%); and
Asia, n=97 (25.3%).
&BCG vaccination status was known in 369 patients overall (n=292, n=39 and n=38 patients classified as uninfected, LTBI and TB, respectively).
*Clinically or radiologically suspected active TB.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
26
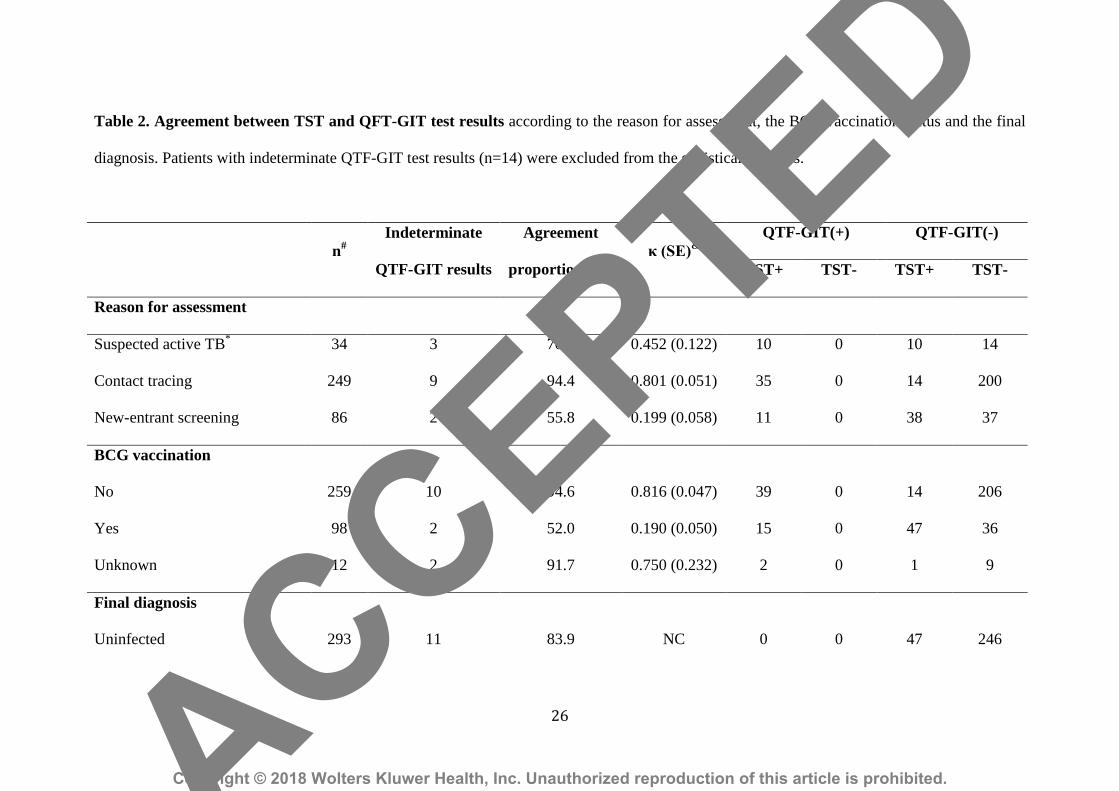
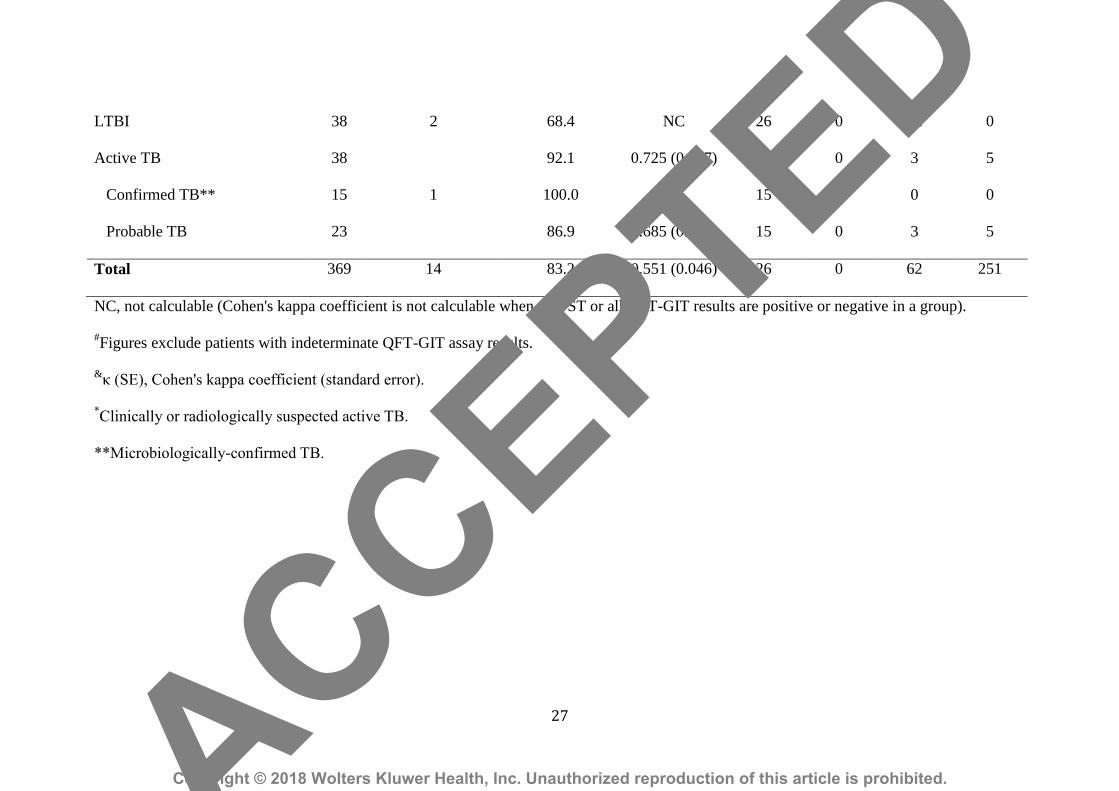
Table 2. Agreement between TST and QFT-GIT test results according to the reason for assessment, the BCG vaccination status and the final
diagnosis. Patients with indeterminate QTF-GIT test results (n=14) were excluded from the statistical analyses.
n#
Indeterminate
QTF-GIT results
Agreement
proportion (%)
κ (SE)&
QTF-GIT(+) QTF-GIT(-)
TST+ TST- TST+ TST-
Reason for assessment
Suspected active TB*
34 3 70.6 0.452 (0.122) 10 0 10 14
Contact tracing 249 9 94.4 0.801 (0.051) 35 0 14 200
New-entrant screening 86 2 55.8 0.199 (0.058) 11 0 38 37
BCG vaccination
No 259 10 94.6 0.816 (0.047) 39 0 14 206
Yes 98 2 52.0 0.190 (0.050) 15 0 47 36
Unknown 12 2 91.7 0.750 (0.232) 2 0 1 9
Final diagnosis
Uninfected 293 11 83.9 NC 0 0 47 246
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
27
LTBI 38 2 68.4 NC 26 0 12 0
Active TB 38 92.1 0.725 (0.147) 30 0 3 5
Confirmed TB** 15 1 100.0 NC 15 0 0 0
Probable TB 23 86.9 0.685 (0.161) 15 0 3 5
Total 369 14 83.2 0.551 (0.046) 26 0 62 251
NC, not calculable (Cohen's kappa coefficient is not calculable when all TST or all QFT-GIT results are positive or negative in a group).
#Figures exclude patients with indeterminate QFT-GIT assay results.
&κ (SE), Cohen's kappa coefficient (standard error).
*Clinically or radiologically suspected active TB.
**Microbiologically-confirmed TB.
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
28
ACCEPTED
Copyright © 2018 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.





























