Embed Size (px)
Citation preview

The Ob-Gyn’s Key Role in Influenza Prevention
Originally presented on Wednesday, October 22, 2014
Learning Objectives
By the end of the webinar participants will be able to : • Understand the rationale for influenza vaccination
as well as the indications and contraindications • Understand the burden of influenza disease in the
general adult population and among pregnant women • Communicate the safety data for vaccination during
pregnancy • Understand the indications for pneumococcal
vaccine
Vaccines are not just for children…
• Adult vaccination saves lives!• Each year in the United States, ~ 60,000 adults die from
vaccine preventable diseases or their complications• Pneumonia and influenza together are the 7th leading
cause of death in the United States
Routine adult vaccine recommendations are based on recommendations from the Advisory Committee on
Immunization Practices (ACIP)• Visit ACOG’s www.immunizationforwomen.org for adult
and childhood/adolescent immunization schedules

What is Influenza? Influenza is NOT a cold
Influenza is far MORE SEVERE than a cold
Influenza, or “the flu” is a highly contagious viral infection of the respiratory tract
• Symptoms develop quickly after infection (1 to 4 days), and usually include fever, headache, extreme fatigue, cough, sore throat, runny or stuffy nose, and muscle aches • Nausea, vomiting, diarrhea are common in children
• An infected person can expect to be sick for 7 to 10 days

Flu Season Flu season usually begins in October, and can run through May; • Peak activity is typically expected around January or February• Timing, severity, and length of the season varies year to year*
• Influenza vaccine is available starting in mid August/ September • Vaccination should begin as soon as vaccine is available – no need to delay
Conditions associated with severe influenza illness
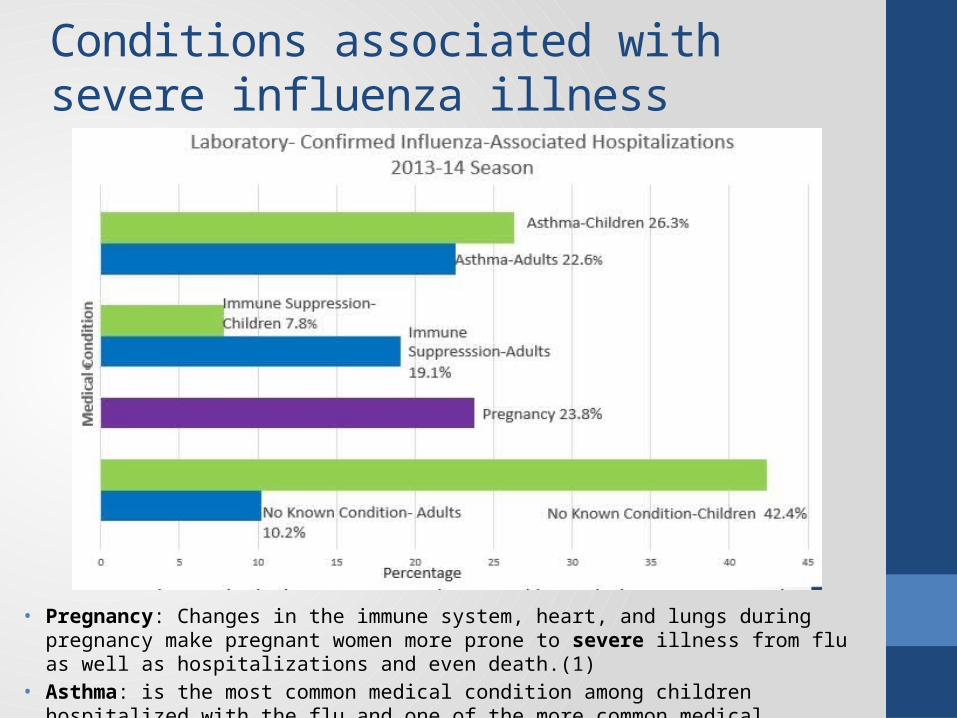
• Pregnancy: Changes in the immune system, heart, and lungs during pregnancy make pregnant women more prone to severe illness from flu as well as hospitalizations and even death.(1)
• Asthma: is the most common medical condition among children hospitalized with the flu and one of the more common medical conditions among hospitalized adults (2)
Influenza and Pregnancy
• 1918: Mortality associated with infection during latter part of pregnancy ~50-61%1 (pneumonia)
• 1957: 50% of women of childbearing age who died of influenza were pregnant; 10% of all influenza deaths that season were in PW (most in latter half of pregnancy)2
• Since 2005 – H5N1:• Six affected pregnant women, 4 did not survive, 2 survivors had
spontaneous abortions3
• Post-mortem studies suggest possible mother to fetus transmission via placenta 4,5
• Interpandemic case reports of complications since 1950’s – mostly healthy women in later stages of pregnancy 6
1. Harris. JAMA 1919;14:978 / 2. Freeman and Barno, Am J Ob Gyn 1959;78:1172 / 3. Abdel-Ghafer et al., NEJM 2008;358: 261 / 4. Gu et al., Lancet 2007;370:1137/ 5. Ng and To, Lancet 2007; 370:1106 / 6. Neuzil et al Inf Dis Clin N Am 2001;15:123
• PW were at high risk to be hospitalized, admitted to the ICU (4x), require mechanical ventilation, and die* from influenza, particularly if in 2-3rd trimester of gestation or with underlying conditions (asthma).
• 5% of all reported 2009 H1N1 influenza deaths in the U.S. were pregnant women, while only approximately 1% of the population was estimated to be pregnant.
• The median age of mothers who died: 25 years (14 - 43 yr).
• Severe illness in the post-partum period and increased rate of premature birth (30.2%) also documented
• Delayed diagnosis and treatment increased risk of death
2009 Influenza A H1N1 and Pregnancy
Louie, JK, et al. NEJM 2010, 362:27-35; Newsome K, et al. MMWR, 2011;60(35):1193-96*All cause maternal mortality California 19.3/100,000; USA 13.3/100,000 – most related to obstetrical factorsInfluenza associated mortality 4.3/100,000
Cost of Influenza: by the numbers5 to 20 Percentage of US residents who get the flu every year
200,000 People hospitalized from flu-related complications each year
$87.1 billion Annual loss to US economy due to influenza and its repercussions
$16.3 billion Annual toll on businesses due to influenza
70 million Workdays missed by Americans last year due to the flu
Between 3,000 and 49,000 Flu-related deaths in America each year
http://theweek.com/article/index/234770/the-cost-of-getting-the-flu-by-the-numbers
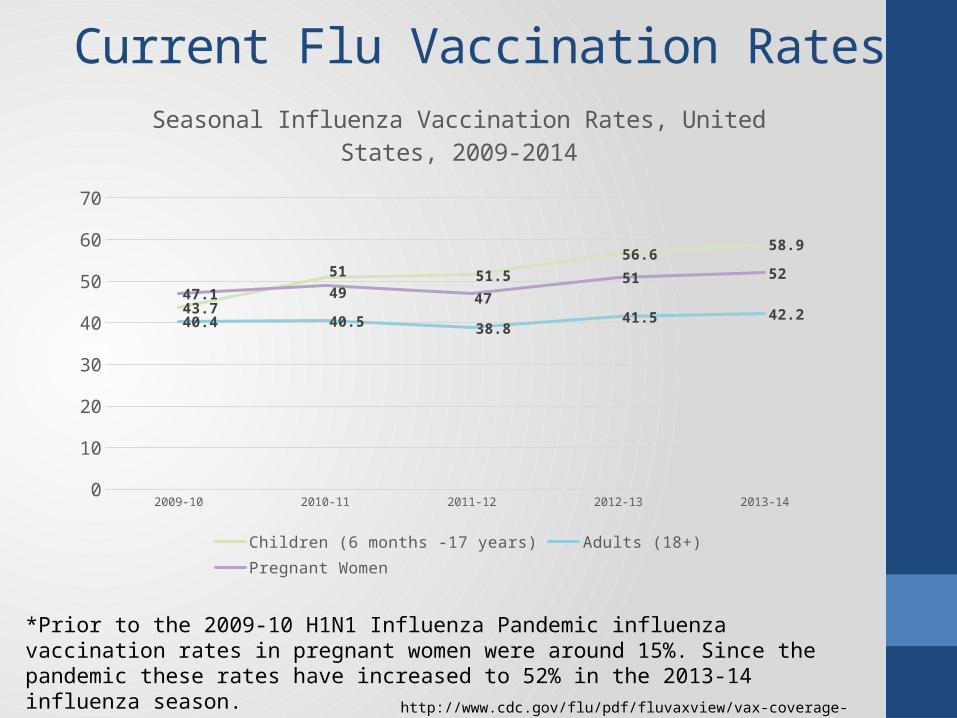
Current Flu Vaccination Rates
http://www.cdc.gov/flu/pdf/fluvaxview/vax-coverage-1314estimates.pdf
*Prior to the 2009-10 H1N1 Influenza Pandemic influenza vaccination rates in pregnant women were around 15%. Since the pandemic these rates have increased to 52% in the 2013-14 influenza season.
2009-10 2010-11 2011-12 2012-13 2013-140
10
20
30
40
50
60
70
43.7
51 51.5
56.658.9
40.4 40.538.8
41.5 42.2
47.1 49 47
51 52
Seasonal Influenza Vaccination Rates, United States, 2009-2014
Children (6 months -17 years) Adults (18+) Pregnant Women
Flu Vaccine Formulations
Flu vaccine options available: Influenza inactivated, intramuscular (IM)
- Quadrivalent- Trivalent
Influenza inactivated, intradermal Cell-based influenza vaccines Nasal spray (contraindicated in pregnancy)
2014-2015 U.S. licensed influenza vaccine formulations Trivalent influenza vaccines will contain:• hemagglutinin (HA) derived from an A/California/7/2009
(H1N1)-like virus • A/Texas/50/2012 (H3N2)-like virus • B/Massachusetts/2/2012-like (Yamagata lineage) virus.
Quadrivalent influenza vaccines will contain the above antigens, and also: • B/Brisbane/60/2008-like (Victoria lineage) virus
2014-2015 U.S.-licensed influenza vaccines will contain the same vaccine virus strains as those in the 2013–14 vaccine.

The Centers for Disease Control and Prevention (CDC) and ACOG recommends routine annual influenza vaccination for all
persons aged 6 months and older who do not have contraindications.
• Vaccination should occur before the onset of influenza activity in the community
• Health care providers should offer vaccination as soon as it becomes available
• Vaccination should be offered as long as influenza viruses are circulating i.e. October through May
• Persons with a history of egg allergy who have experienced only hives after exposure to egg should receive influenza vaccine.
Influenza Vaccination Recommendations
Source: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6332a3.htm#Groups_Recommended_Vaccination_Timing_Vaccination
Influenza Vaccination Recommendations:Pregnant Women
• CO 608: Influenza vaccination is an essential part of prenatal and preconconception care
• Pregnant women have increased morbidity and mortality from influenza
• Neonates also have increased morbidity and mortality from influenza and cannot be vaccinated until 6 months
• Keeping mom healthy during pregnancy protects fetus from early delivery

Influenza Vaccination Recommendations:Pregnant Women cont’d
Influenza vaccination is recommended for all pregnant women regardless of trimester
• Pregnant women should receive the inactivated vaccine and NOT the nasal spray, which is a live vaccine• Pregnant women can receive the trivalent or the
quadrivalent vaccine
• The Flu shot is OK to have while breastfeeding
• The Flu shot has been shown to protect both the mother and her baby (up to 6 months old) from flu

Influenza Vaccination Recommendations:Pregnant Women cont’d
Children younger than 6 months old cannot receive the flu vaccine – protecting mom helps protect baby:• Maternal antibodies cross the placenta and protect newborns (1)
• Vulnerable newborns/young infants are protected by vaccinating family members and caretakers
• Everyone (e.g. siblings, grandparents and babysitters) who will be around the baby should be vaccinated, ideally, before the baby is born
• Encourage extended family members and friends to get vaccinated
• Ensure anyone holding the baby washes their hands first

Inactivated Influenza Vaccine: Effectiveness in Mother and Child
Infants• Maternal influenza
vaccine reduced proven influenza illness in infants by 65%
• 29% reduction in any respiratory illness
• 42% reduction in clinic visits
Mothers• Maternal influenza
vaccine reduced respiratory illness with fever by 36%
• Fewer clinic visits
Zaman, NEJM, 2008

Maternal Inactivated Influenza Vaccine: Effectiveness in infants

The Ob-Gyn’s Role
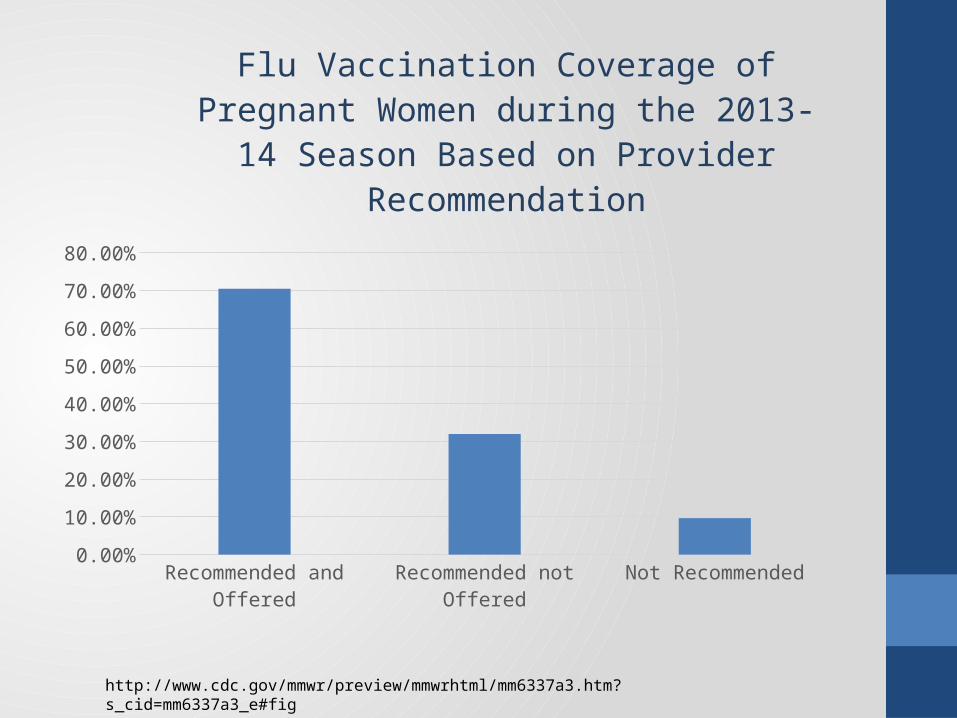
• Studies continue to show a provider recommendation is the most influential factor in a patient’s decision to receive an immunization1 • Ob Gyns have a long standing role of providing ‐ ‐
primary and preventive care to women and are a major source of ambulatory care for women, accounting for 44% of preventive care visits for women over age 182
• Pregnant women see their ob-gyn regularly throughout the course of their prenatal and postpartum care allowing for multiple opportunities to vaccinate. 1. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6337a3.htm?s_cid=mm6337a3_e#fig
2. Stormo AR, Saraiya M, Hing E, Henderson JT, Sawaya GF. Women’s Clinical Preventive Services in the United States: Who Is Doing What?. JAMA Intern Med. Published online July 07, 2014. doi:10.1001/jamainternmed.2014.3003.
Recommended and O
ffered
Recommended not O
ffered
Not Reco
mmended0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
Flu Vaccination Coverage of Pregnant Women during the 2013-14 Season Based on
Provider Recommendation
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6337a3.htm?s_cid=mm6337a3_e#fig

Protect their infant from influenza
Protect themselves from influenza
Clinician recommended the influenza vaccine
0 5 10 15 20 25 30 35
Most Common Reasons among for Receiving the Influenza Vaccine in the 2013-14 Season
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6337a3.htm?s_cid=mm6337a3_e#fig

Health Care Personnel: Be the Example
• Make sure all staff members are vaccinated • 75.2% coverage rate for HCP for 2013-14
season, similar to coverage of 72.0% in the 2012-13 season. (1)
• Coverage was highest among HCP working in settings with flu vaccination requirements 97.8%.(1)
• Make sure you and your family are vaccinated • Educate entire staff
Safety of influenza vaccineHow is it monitored ? • Vaccine Adverse Event Report System (VAERS) is a
national program, jointly managed by CDC and FDA, which monitors the safety of all vaccines licensed in the United States. Anyone can file a VAERS report• Vaccine Safety Datalink (VSD) is a vaccine safety system
used to both monitor and assess adverse events following vaccination • Vaccines and Medications in Pregnancy Surveillance
System (VAMPSS) study

Influenza Vaccine Safety in Recent studies
Observational studies:
• VAERS ~ 2 million pregnant women vaccinated 2000-031
• VAERS ~11.8 million vaccinated from 1990 to 20092 • VAERS H1N1 vaccinations 2009-102
ALL: No increased risk of adverse events or pregnancy outcomes vs. background rates
1. Pool V and Iskander J. Am J Obstet Gynecol 2006;194:1200; 2. Moro et al. Am J Obstet Gynecol 2010; 203:1.e1-e7 3. Moro et al. Am J Obstet Gynecol 2011; 205:43e1-7

Summary of recent safety studies flu vaccineStudy Vaccinated PW ControlMunoz 2005 225 TIV 826 unvax. PW No increase AE/OB
complicationsTavares 2011* 267
ASO3/AH1N1pdmnone < expected rate OB
complicationsHeikkinen 2012* 2,295
MF59/AH1N1pdm2,2,13 unvax. PW No increase AE; Sig
lower gest. diabetes
Oppermann 2012* 323 ASO3/AH1N1 pdm
1,329 unvax. PW No increase AE
Conlin 2013 10,376 A/H1N1 exposed PW
7,560 PW given TIV No difference in OB complications
Kallan 2013 18,612 ASO3 A/H1N1pdm
136,914 and 83,298 unvax. PW
No increase AE
Kharbanda 2013 74,292 TIV 144,597 unvac PW No increase AERubinstein 2013 7,293
MF59 AH1N1pdm23,195 unvac PW No increase AE
* Prospective studies. The others were Retrospective with matched cohort

Vaccination is Safer than Influenza during Pregnancy• Norwegian National Registries study • 113,331 pregnancies in 2009-2010• 54% of women were vaccinated (2nd-3rd trim. Pandemrix ASO3)• 492 Fetal deaths – 4.3 per 1000 births (outside pandemic 4.1)• Vaccination during pregnancy substantially reduced (70%) the
risk of an influenza diagnosis in pregnant women (Adj. hazard ratio 0.30; 95% CI, 0.25-0.34)
• Among pregnant women with influenza, the risk of fetal death was increased (Ajd hazard ratio, 1.91; 95% CI 1.07-3.41)
• The risk of fetal death was reduced with vaccination during pregnancy (not sig: Adj hazard ratio, 0.88; 95% CI 0.66-1.17)
• Among live births: no association with preterm delivery, LBW, low Apgar
Haberg et al NEJM (2013)
Common side effects
Possible mild side effects of the flu shot include:
Soreness RednessSwelling at injection siteFainting
Mainly in adolescents:HeadachesFeverNausea
Possible mild side effects of the nasal spray include: Runny nose
WheezingHeadacheVomitingMuscle achesFever
Serious side effects
Serious side effects are extremely rare and usually begin within a few minutes to a few hours after receiving the shot, they include:
If any unusual condition occurs following vaccination, seek medical attention right away. Ask your doctor, nurse, or health department to report a possible reaction by filing a Vaccine Adverse Event Reporting System (VAERS) form. Or you can file this report yourself through the VAERS website. You may call 1-800-822-7967 to receive a copy of the VAERS form. VAERS does not provide medical advice.
- Difficulty breathing- Hoarseness- Hives- Paleness- Swelling around the eyes or lips
- Weakness- Racing heart- Dizziness- Behavior changes- High fever

Pregnant Women experiencing flu-like symptoms should be treated early and liberally
Pregnant women who are ill during the influenza season should be treated with Oseltamivir presumptively regardless of vaccination status
Do not wait for test results to start antiviral treatment
Algorithm can be found at immunizationforwomen.org

Common MythsMyth 1: I got the shot last year I don’t need it this year.Response: Every year flu vaccines are made specifically to fight the strains of the virus that are predicted to be the most prevalent that season. This means that the vaccines can be slightly different from year to year and in order to be best protected you need a flu shot every year
Myth 2: I’ll get sick from the vaccineResponse: Because the flu vaccine is made with a killed or very weakened virus you can not get the flu from flu vaccine.
Myth 3: Flu vaccine causes autismResponse: Many studies have been conducted reviewing mercury (thimerosal), influenza vaccines and autism. No study has ever shown a positive relationship between influenza vaccine, mercury and subsequent autism diagnosis. Most flu vaccines don’t contain preservatives.

Common Myths cont’d
Myth 4: I’m healthy and I never get the flu, so I don’t need it Response: Even healthy adults can become severely ill from the flu. The flu vaccine is recommended for everyone 6 months and older.
Myth 5: I can’t get the vaccinate in the first trimester of pregnancyResponse: The vaccine has proven to be safe in all trimesters. Since 2004 the CDC and ACOG have recommended influenza vaccination during any trimester.
Myth 6: The flu vaccine will cause birth defects or miscarriage Response: Flu vaccines have been given to millions of pregnant women over decades. No relationship has been shown between influenza vaccination and birth defects and miscarriage.

Integrating into practice
• Practical recommendations: • Give recommendation for flu
immunization to patients• Talk to moms about immunizing
their families• Uses tools scripts and toolkits
found at www.immunizationforwomen.org
Provider responsibilities
• Patient vaccine records are kept up to date• Vaccine logic in EHR—may not reflect ob-gyn
needs• Specific order vs. standing order• VIS (Vaccine Information Statement) forms
Provider responsibilities cont’d
• VAERS (Vaccine Adverse Event Reporting System)• Recording—in chart. State IIS—requirements vary by
state• Report all vaccines administered to your state vaccine
registry. Useful for verifying immunization history where vaccines may have been administered in other settings and avoiding unnecessary duplication of vaccines. Contact state/local health department • State Registry Contacts:
http://www.cdc.gov/vaccines/programs/iis/contacts-registry-staff.html
Business Practice• Reimbursement • Vaccine purchasing resource• VFC (Vaccines for Children) • Vaccine registries
More information about business practice can be found:• at immunizationforwomen.org • By watching the On-Demand webinar: ACOG
Immunization & Clinical Strategies for Ob-Gyn Practices
Pneumococcal Disease• Invasive disease from Streptococcus pneumoniae
(pneumococcus) is a major cause of illness and death in the general population• Pneumococcal vaccination is recommended for persons >
65, immunosuppressed individuals, as well as immune competent individuals with certain underlying medical conditions including:• Smokers• Asthmatics• Diabetics

Pneumococcal Disease cont’d• Immune competent adults should receive the
pneumococcal polysaccharide vaccine (PPSV23) • Immune compromised adults should receive the
pneumococcal conjugate vaccine (PCV13) as well as PPSV23• Providers should make every effort to vaccinate medically
high-risk women before they become pregnant• If pregnant women have never been vaccinated:• Asthmatics, diabetics, and smokers should receive
PPSV23 during pregnancy• Women with immune deficiencies or asplenia should
receive PCV13 followed by PPSV23

Additional Vaccination Opportunities for Obstetricians and Gynecologists
Influenza vaccine for all women including those who are pregnant
Tdap vaccine for all adults who have not been vaccinated and all women during each pregnancy
Pneumococcal vaccine for high risk women including those who are pregnant
Hepatitis B vaccine for all at risk women including those who are pregnant
MMR vaccine for women who were not previously vaccinated. Should give before or after pregnancy
Varicella vaccine for women who were not previously vaccinated or have not had chickenpox. Should give before or after pregnancy
HPV vaccine for girls and women ages 9-26. Not recommended during pregnancy
Graphic courtesy of the National Foundation for Infectious Diseases.


Conclusions
All persons 6 months and older should receive influenza immunization every year
Pregnant women are at increased risk of complications for influenza infection
Influenza immunization during pregnancy protects pregnant women and their babies
Influenza vaccines are safe and effective Ob-Gyns have a responsibility to integrate influenza
immunization into routine practice

ResourcesACOG Immunization for Women : About Influenza
ACOG Committee Opinion 608 Influenza Vaccination in Pregnancy (2014) http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Influenza-Vaccination-During-Pregnancy
CDC: http://www.cdc.gov/flu/
HHS:http://www.flu.gov/

ACOG’s Immunization Department
Immunizationforwomen.orgImmunization Program: [email protected]
Debra Hawks, MPH, Senior Director Practice Activities, Obstetrics, & Immunization
Sarah Patterson Carroll, MPH, Immunization [email protected]
Valerie Echeveste, Immunization Program [email protected]
Megan McReynolds, Director Obstetrics Practice Bulletins, Immunization, and [email protected]





























