Embed Size (px)
Citation preview

12/8/2015
1
The Next Big Thing: Transitions in Care
December 8, 20151:30 pm– 2:45pm
#IHI27FORUM
Marlene Bober – VP, Acute Enterprise Care Management
Tina Esposito – VP, Center for Health Information Services
Advocate Health Care
Session Objectives
Examine one organization’s data on transitions in care
Review an empirically driven model for guiding care transitions
Discuss impending considerations around transitions in care
2
#IHI27FORUM
12/8/2015
2
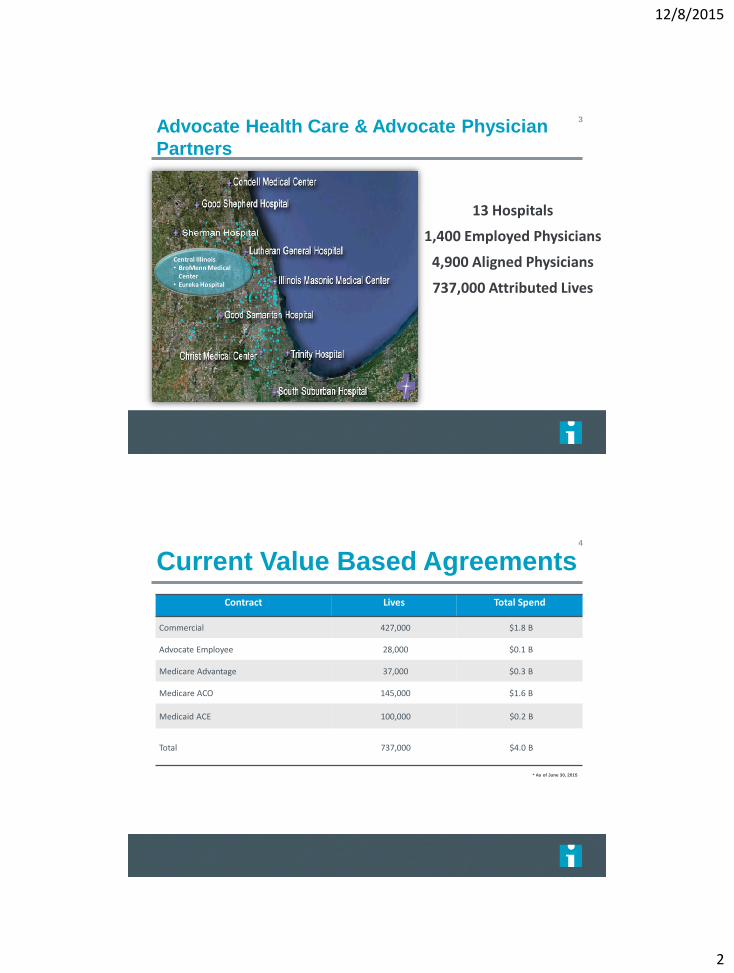
Advocate Health Care & Advocate Physician
Partners
3
13 Hospitals
1,400 Employed Physicians
4,900 Aligned Physicians
737,000 Attributed Lives
Current Value Based Agreements
Contract Lives Total Spend
Commercial 427,000 $1.8 B
Advocate Employee 28,000 $0.1 B
Medicare Advantage 37,000 $0.3 B
Medicare ACO 145,000 $1.6 B
Medicaid ACE 100,000 $0.2 B
Total 737,000 $4.0 B
* As of June 30, 2015
4
12/8/2015
3
5
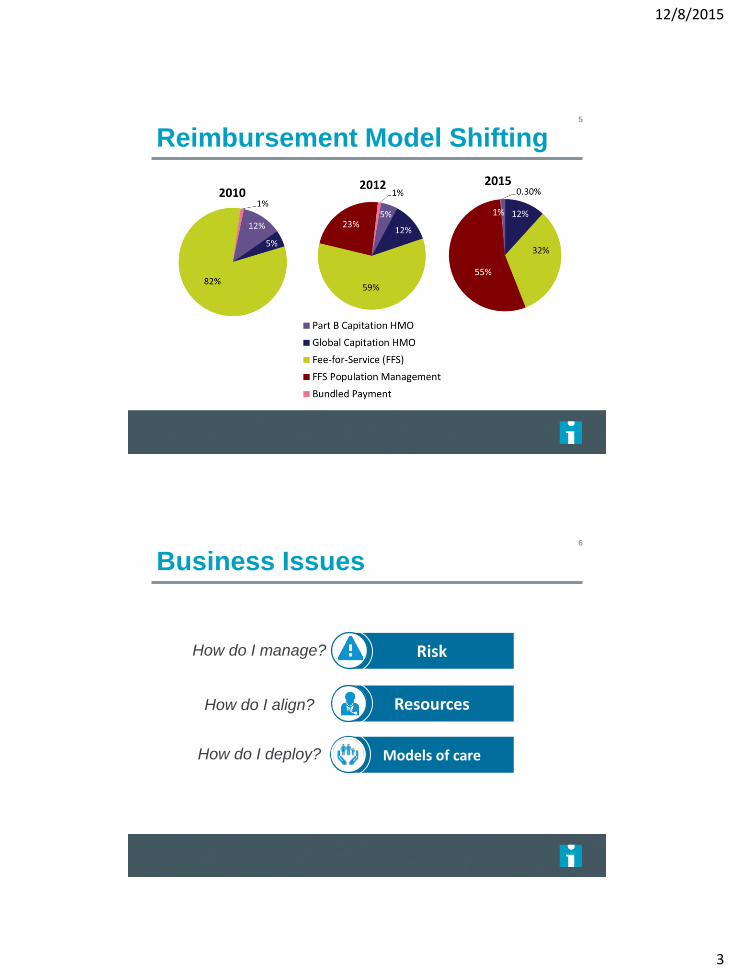
Reimbursement Model Shifting
6
Business Issues
Resources
Risk
Models of care
How do I manage?
How do I align?
How do I deploy?
12/8/2015
4
7
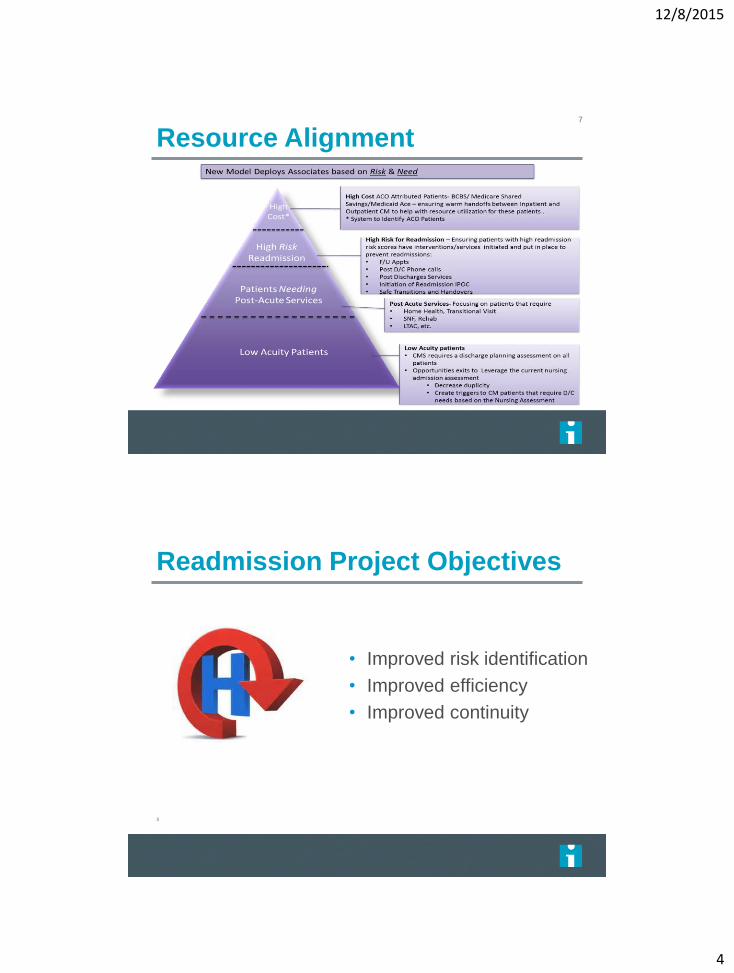
Resource Alignment
Readmission Project Objectives
8
• Improved risk identification
• Improved efficiency
• Improved continuity

12/8/2015
5
Readmission Model Results9
Readmission Workflow Improvements
Data/Model
Ability to leverage more clinical data
Real time data updates
Workflow
Automated and continuous
calculation (every 2 hours)
Embedded into a care manager
workflow
Before
After
12/8/2015
6
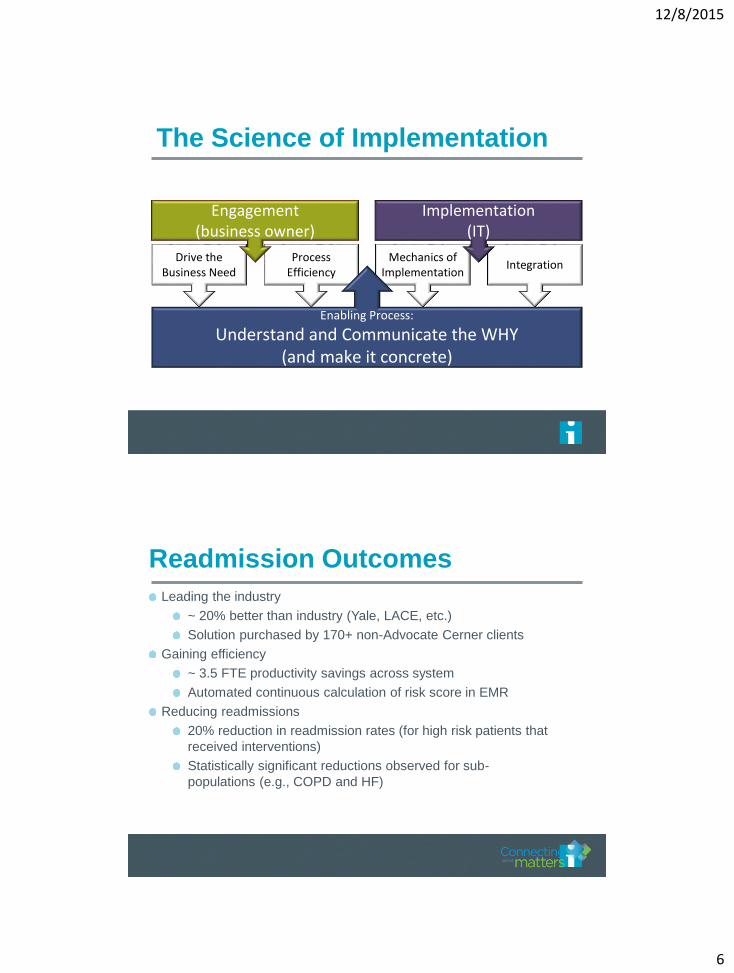
The Science of Implementation
Drive the Business Need
IntegrationMechanics of
ImplementationProcess
Efficiency
Engagement (business owner)
Implementation (IT)
Enabling Process:
Understand and Communicate the WHY (and make it concrete)
Readmission Outcomes
Leading the industry
~ 20% better than industry (Yale, LACE, etc.)
Solution purchased by 170+ non-Advocate Cerner clients
Gaining efficiency
~ 3.5 FTE productivity savings across system
Automated continuous calculation of risk score in EMR
Reducing readmissions
20% reduction in readmission rates (for high risk patients that
received interventions)
Statistically significant reductions observed for sub-
populations (e.g., COPD and HF)

12/8/2015
7
Where is the Most Appropriate Location for Our
Patients?
13
Hospital
Skilled Nursing
Assisted Living
Home Care
Retail Pharmacy
Behavioral Health
Rehab
?
P14
Note: In general, acute spinal cord and brain injury patients and complex stroke are most appropriate for acute inpatient rehab*Patient meets criteria based on applicable Milliman guidelines. Refer to Post-Acute Service Availability Grid; Home Care patients must meet home-bound status** Transition program offered by Home Health Services: check with your site for availability and specific patient inclusion criteria. The readmission risk tool should be used in conjunction with sound clinical judgment when used to help determine post acute care setting and/or intensity. The expected probability of readmission increases with an increase in score, but for any individual patient, other factors (i.e. literacy, social, financial) may impact whether or not the patient actually is actually readmitted

12/8/2015
8
15
Model Overview
HomeHome health
Skilled nursing facility
Acute inpatient
rehab
Acute long-
term care
Risk of medical instability
Intensity of services
Find patients with similar clinical profiles
Identify where this patient type is most successful (lower actual
readmission rate)
Quantify the recommendation’s impact on readmission risk
Acute Transitions of Care (ATOC) Model Results16
12/8/2015
9
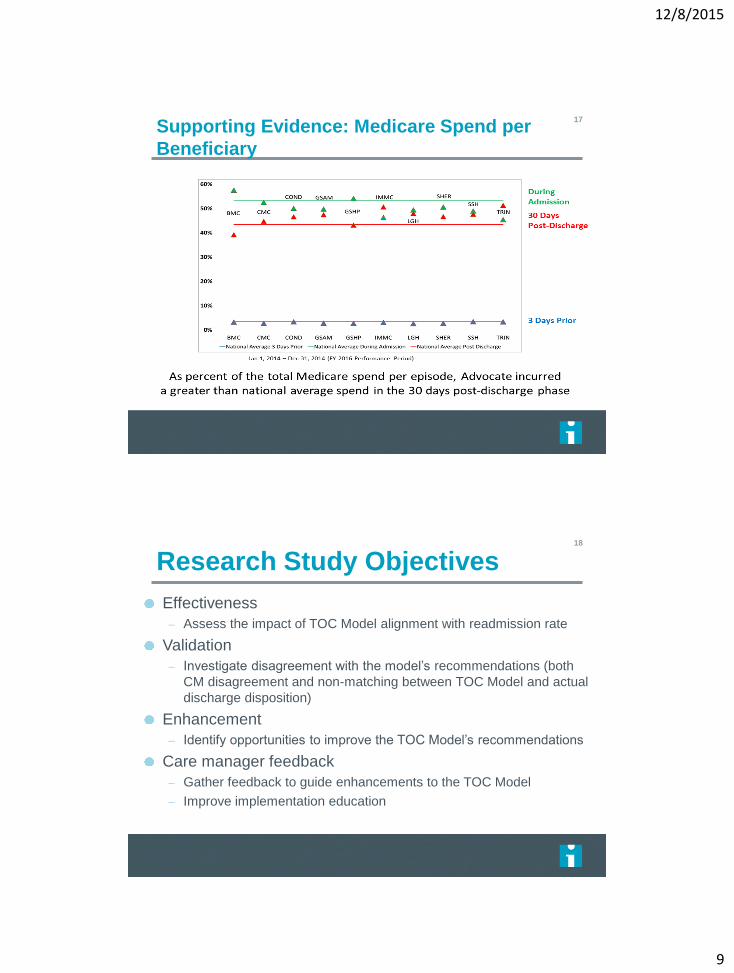
Supporting Evidence: Medicare Spend per
Beneficiary
17
18
Research Study Objectives
Effectiveness
– Assess the impact of TOC Model alignment with readmission rate
Validation
– Investigate disagreement with the model’s recommendations (both
CM disagreement and non-matching between TOC Model and actual
discharge disposition)
Enhancement
– Identify opportunities to improve the TOC Model’s recommendations
Care manager feedback
– Gather feedback to guide enhancements to the TOC Model
– Improve implementation education
12/8/2015
10
19
ATOC Pilot Results
Prospective effectiveness trial (form of a randomized
controlled trial)
Time period: Oct 2014 – Jan 2015
Preliminary findings:
– Indication that alignment between the actual discharge disposition
and the ATOC model is associated with lower rates of readmission.
Bridging the Gap with Transitions
12/8/2015
11
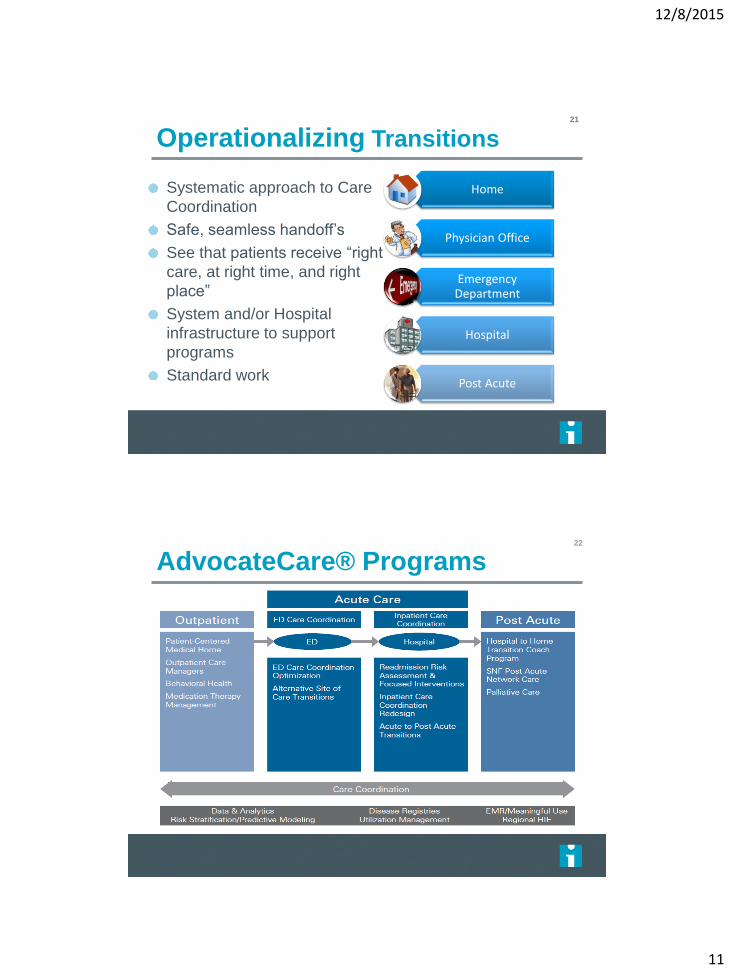
Operationalizing Transitions
Home
Physician Office
Emergency Department
Hospital
Post Acute
21
Systematic approach to Care
Coordination
Safe, seamless handoff’s
See that patients receive “right
care, at right time, and right
place”
System and/or Hospital
infrastructure to support
programs
Standard work
22
AdvocateCare® Programs

12/8/2015
12
Acute Care Focus23
ED care coordination optimization
Inpatient care coordination redesign
Readmission Risk Assessment and Prevention
Post acute transitions
Advocate’s Standard Model24
Role Clarity & Accountabilities
Org Structure & Operational Oversight
Care Coordination Activities
Transitioning with Referring Provider / PCP
Patient Family Engagement

12/8/2015
13
ED Care Coordination25
Goal - to identify best practices of ED care
coordination in all of Advocate hospitals and agree
upon a standard approach of evidence-based
practices to:
– Prevent unnecessary admissions
– Avoid readmissions
– Ensure appropriate utilization of resources
– Improved collaboration with the ED Physicians and
nurses on awareness of alternatives to admission
when appropriate
ED Care Coordination Optimization Outcome26
Implementation of a standard set of practices for ED
care coordination at all Advocate hospitals i.e.
– ED Care Manager Orientation Checklist
– ED Care Manager Competency
– ED Workflow Diagram
– Referral and Handover Process
– ED Care Coordination FAQ’s
Implementation of key metrics to track performance
Patient Education - “Care Options”
12/8/2015
14
Importance of Transition Handoff’s
Key Tenets of Cross-Continuum Care
Management
28
The Care
Manager with
the patient is the
responsible
Care Manager
Perfect Handoffs
Are expected Technology would
make this much
more efficient and
reliable
12/8/2015
15
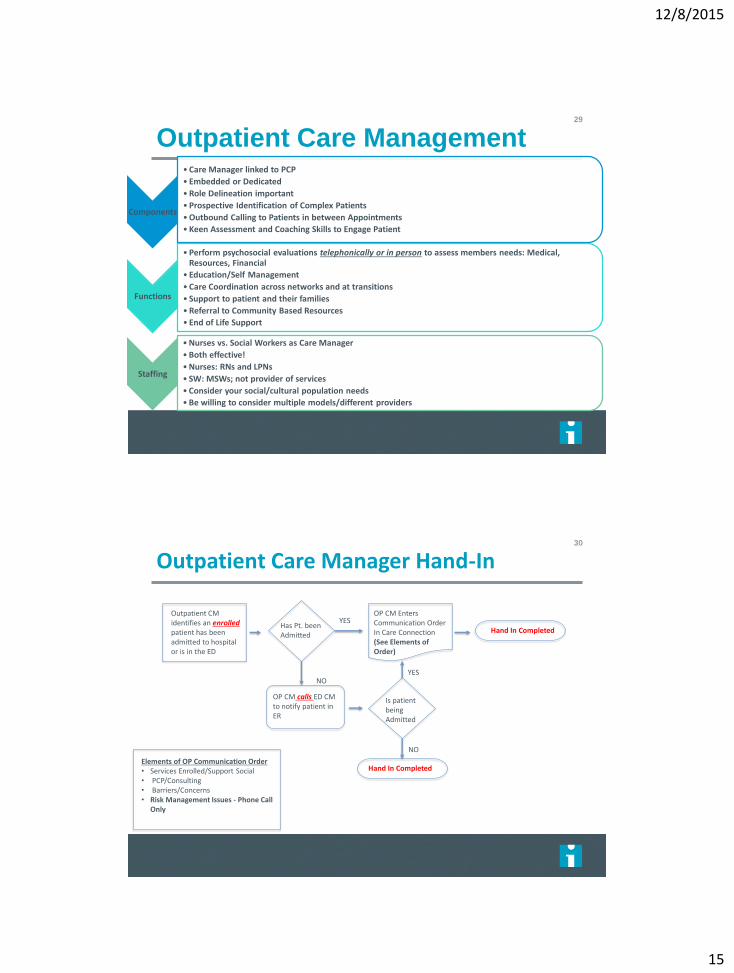
Outpatient Care Management29
Components
• Care Manager linked to PCP
• Embedded or Dedicated
• Role Delineation important
• Prospective Identification of Complex Patients
• Outbound Calling to Patients in between Appointments
• Keen Assessment and Coaching Skills to Engage Patient
Functions
• Perform psychosocial evaluations telephonically or in person to assess members needs: Medical, Resources, Financial
• Education/Self Management
• Care Coordination across networks and at transitions
• Support to patient and their families
• Referral to Community Based Resources
• End of Life Support
Staffing
• Nurses vs. Social Workers as Care Manager
• Both effective!
• Nurses: RNs and LPNs
• SW: MSWs; not provider of services
• Consider your social/cultural population needs
• Be willing to consider multiple models/different providers
30
Outpatient Care Manager Hand-In
OP CM Enters Communication Order In Care Connection (See Elements of Order)
Outpatient CM identifies an enrolledpatient has been admitted to hospital or is in the ED
Has Pt. been Admitted
Elements of OP Communication Order • Services Enrolled/Support Social• PCP/Consulting• Barriers/Concerns • Risk Management Issues - Phone Call
Only
YESHand In Completed
OP CM calls ED CM to notify patient in ER
NO
Is patient being Admitted
Hand In Completed
YESNO
12/8/2015
16
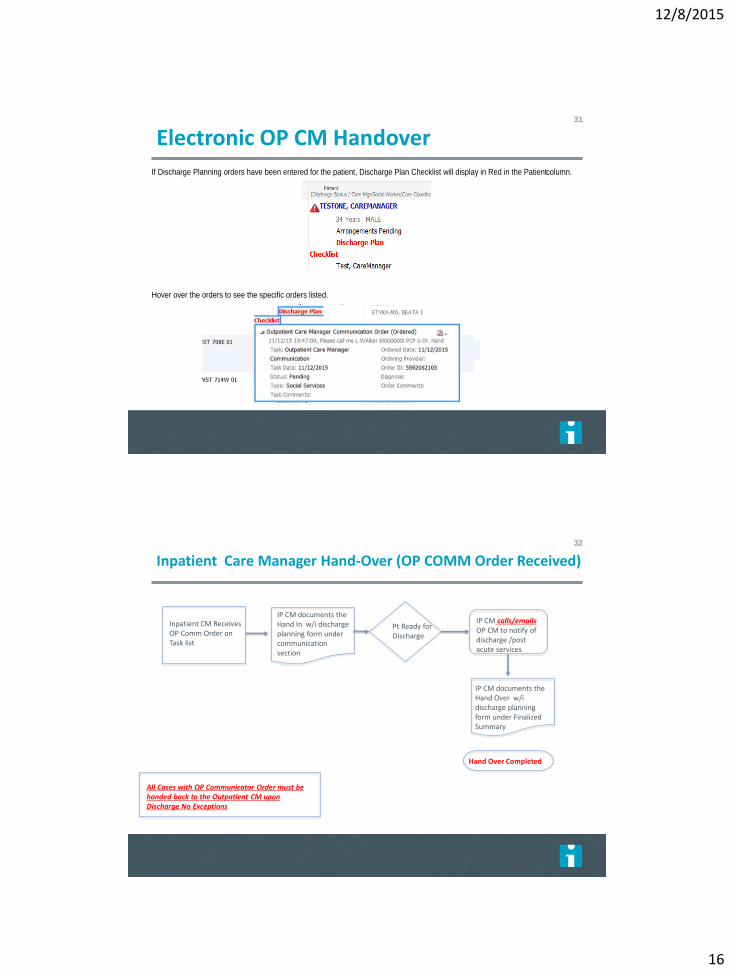
Electronic OP CM Handover31
If Discharge Planning orders have been entered for the patient, Discharge Plan Checklist will display in Red in the Patient column.
Hover over the orders to see the specific orders listed.
Inpatient Care Manager Hand-Over (OP COMM Order Received)
32
IP CM documents the Hand In w/i discharge planning form under communication section
Inpatient CM Receives OP Comm Order on Task list
Pt Ready for Discharge
All Cases with OP Communicator Order must be handed back to the Outpatient CM upon Discharge No Exceptions
Hand Over Completed
IP CM calls/emails OP CM to notify of discharge /post acute services
IP CM documents the Hand Over w/i discharge planning form under Finalized Summary

12/8/2015
17
Post Acute Standards33
• Standard Criteria to determine appropriate post-acute care
• Standard data elements for referral to post-acute care
• Standard workflow using ECIN for transition management
• Standard process for offering upfront home care choice to patients
Process Deliverables
• Quick reference grid and decision algorithm for appropriate post-acute care
• Pre-define data elements for referral through ECIN
• ECIN Implementation for post-acute transitions and referral management
Tool Deliverables
34
Post Acute Services Availability by Program or Location
Program / Services HomeTransition
Program*
Home
Health
SNF/
SubacuteAcute Inpatient Rehab LTACH
Risk of medical instability
CLINICAL SERVICES
Physician Care OP OP OP1-3x/week (first visit within
72 hours)Daily Daily
Nursing Care NoneOne visit & up to 3 phone
calls1-3 visits/week
~2-3 RN/LPN ~2-3 CNA
hours/day
~4-6 Rehab RN ~2-3 PCA
hours/day~5 RN ~3-5 CNA hours/day
Therapy OP OPAs needed, intermittent up
to 7 days/weekUp to 2.5 hours/weekday 3+ hours/ weekday required Up to 5x/ week
SPECIALTY SERVICES
Dialysis OP OP OP OP or In-house In-house In-house
Infusion NA NA
IV meds parenteral & enteral
nutrition/
hydration**
IV meds parenteral & enteral
nutrition/
hydration
IV meds parenteral & enteral
nutrition/
hydration
IV meds parenteral & enteral
nutrition/
hydration
Ventilator NA NA NASite specific (typically
chronic)NA
In-house (primarily intent to
wean)
Complex Wound Care OP Wound Program OP Wound Program Home Wound Care Site specific In-house In-house
Other Considerations (to aid in communicating to patient/family about long term plan of care)
Anticipated Discharge
LocationNA NA NA Home w/ skilled services Home w/ skilled services IRF/SNF
Anticipated LOS (Post-
Acute)NA NA 2 days - 6 weeks 14-28 days 7-21 days 21-45 days
* Transition program offered by Advocate at Home: check with your site for availability and specific patient inclusion criteria
** Highly dependent on payor and specific benefits - validate coverage on a case-by-case basis
LOWER HIGHER

12/8/2015
18
Post Acute Business Model35
Post Acute
NetworkInfusion
RT/HME
Hospice
Home Care
Palliative Care Transition
Program
SNF
LTACH
IP
Rehab
Business to Business Model
Same referral flow
Similar goals to improve delivery of
care:
– quality
– readmissions
– reduce cost of care
– manage continuum leakage
Tools for managing care/offering
different levels of care
Centralized oversight / strategic
alignment
AHHSin place
“Build” / partner
The SNF Care Model36
The SNF Care Model is currently in place as a nationally
recognized model of APN/Physician SNF Rounding
Team
1-2 Physician FTE
1 APN FTECapability to manage SNF
ADC
* Physician visits 1x per week, APN 5x’s per week
12/8/2015
19
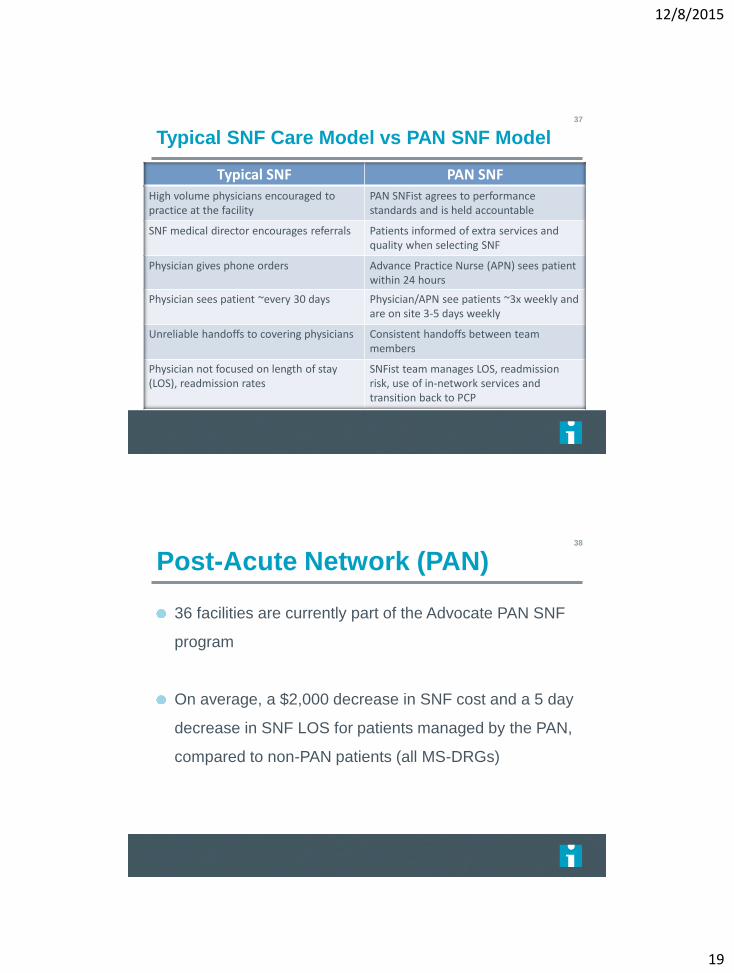
Typical SNF Care Model vs PAN SNF Model37
Typical SNF PAN SNF
High volume physicians encouraged to practice at the facility
PAN SNFist agrees to performance standards and is held accountable
SNF medical director encourages referrals Patients informed of extra services and quality when selecting SNF
Physician gives phone orders Advance Practice Nurse (APN) sees patient within 24 hours
Physician sees patient ~every 30 days Physician/APN see patients ~3x weekly and are on site 3-5 days weekly
Unreliable handoffs to covering physicians Consistent handoffs between team members
Physician not focused on length of stay (LOS), readmission rates
SNFist team manages LOS, readmission risk, use of in-network services and transition back to PCP
Post-Acute Network (PAN)38
36 facilities are currently part of the Advocate PAN SNF
program
On average, a $2,000 decrease in SNF cost and a 5 day
decrease in SNF LOS for patients managed by the PAN,
compared to non-PAN patients (all MS-DRGs)
12/8/2015
20
39
AdvocateCare® Programs Across the Continuum





























