Embed Size (px)
Citation preview

®
A P R O G R A M O F H E A L I N G F O R A L C O H O L A N D D R U G U S E D I S O R D E R S
DIRECTORY OF SERVICESAddiction Medicine Consultationand Evaluation Services (AMCES)
202 S. Park StreetMadison, Wisconsin 53715
(Ph) 608-267-6291(Fax) 608-267-6687
• Addiction Medicine Consultation and Evaluation
• Information and Referral• Chemical Dependency Assessment
• Emergency Services• Medical Inpatient Detoxification
• Nursing Evaluation• Referral Services
Outpatient Services and Adolescent Program
1015 Gammon LaneMadison, Wisconsin 53719
(Ph) 608-271-4144(Fax) 608-271-3457
• Assessment and Referral Service• Adolescent Intensive Outpatient Program
• Adult Intensive Outpatient Program • Adult Day Treatment
• Individual, Group, and Family Counseling for Chemical Dependency
and for Family Members• Chemical Awareness Programs
Inpatient ServicesUnit 1 East
202 S. Park StreetMadison, Wisconsin 53715
(Ph) 608-267-5330(Fax) 608-267-5334
• Adult Inpatient Rehabilitation Services
1A P R O G R A M O F H E A L I N G F O R A L C O H O L A N D D R U G U S E D I S O R D E R S
The Mission of NewStart is to provide a comprehensivenetwork of treatment, education, and referral services forpersons with alcohol or other substance use disorders, andothers affected by the patient’s substance use.
IN THIS ISSUE…Directory of Services ..........................................1NewStart’s Scope of Treatment .............................1NewStart Counseling Strategies Expanding .............1Fifth Annual Recovery Rally .................................2NewStart to Participate in National StudySponsored by Texas Christian University ................2Limitations on Buprenorphine Lightened................3“Light” at the End of the Addiction Tunnel forQuad/Graphics Employees and Family Members ......3Marijuana: Health Benefits? .............................4-5Clinical Tips Regarding Use of Urine Drug Tests .......6NewStart Retreat ...............................................6Staff Profile: Sue Klein-Kennedy, MS, CADCIII ........72005 Professional of the Year Award......................7Coerced Treatment..........................................8-9NewStart Physicians Receive ASAM Certification....10
NEWSTART’S SCOPE OF TREATMENTNewStart is the sole remaining hospital-
based treatment program for alcohol and druguse disorders in South-Central Wisconsin.NewStart continues to offer a full continuumof services including outpatient, intensiveoutpatient, and full-day treatment;detoxification; and inpatient rehabilitationservices. NewStart remains one of the fewlocal providers which accepts fee-for-serviceMedical Assistance patients. NewStartcounseling staff are all certified to provideaddiction treatment services through theWisconsin Certification Board, and all areMasters-prepared. In our current two-physician model of care, 24-hour coverage isavailable for emergency room and hospitalconsults and inpatient coverage while allowingfor consistent availability of physician servicesin our outpatient clinic every week.
NEWSTART COUNSELING STRATEGIESEXPANDINGJennifer Schoff
Competency in alcohol and drug counsel-ing requires that we learn new skills andrefresh existing skills for treatment of sub-stance use disorders. That is why NewStartstaff is currently focusing staff developmentefforts on Cognitive Behavioral Therapy (CBT),specifically Cognitive Behavioral Therapy ofSubstance Abuse (Beck, et al, 1993). In theseweeks of training, the staff is reviewing eachchapter, discussing techniques, and how CBTis helpful in therapeutic settings. AlthoughNewStart’s alcohol and drug counselors havebeen using the CBT techniques, it has been alearning experience to discuss specific tech-niques as a group. This has given the coun-selors the opportunity to hone their skills formore effective practice and share skills/ideaswith their colleagues.
What is CBT? The underlying theme to CBTis that our feeling and thoughts relate to ouractions. The focus is then changing ourthoughts in order to have more control overactions. The goal is to slow down our reactionsso that we make healthier decisions, like notusing alcohol or drugs. Our core beliefs lead toemotions, which lead to addictive beliefs,which lead to addictive behaviors. With CBT,we are able to change our core beliefs, whichlead to different emotions, leading healthydecisions, like not using substances.
CBT is one more tool in the tool belt of ourcounselors. CBT is used in conjunction withother treatment techniques, such as 12-Stepfacilitation. Using the techniques in CBT, weare teaching our clients more ways to remainabstinent, become more productive citizensand improve relationships.
VOLUME XXV FALL 2005

FIFTH ANNUAL RECOVERY RALLY September is National Recovery Month,
when thousands of Americans and theirfamilies and communities celebrate recov-ery from alcohol and other drug abuse.In Wisconsin, we are celebrating witha Recovery Rally at the State Capitol inMadison, Saturday, September 17, 11:00 a.m.to 2:00 p.m.
This is Wisconsin’s Fifth AnnualRecovery Rally which emphasizes how thecommunities can heal through celebrationof recovery from substance abuse— “Healing the Wisconsin Community:Celebrating Recovery from Alcohol andOther Drug Abuse.”
Organized by the Wisconsin Associationon Alcohol and Other Drug Abuse and theAlliance for Recovery Advocates, the 2005Recovery Rally includes music and dancefrom some of Wisconsin’s diverse commu-nities. The Rally presents special perform-ances by the Madison Community GospelChoir, Wolf River Singers, United RefugeeServices of Wisconsin Sunshine Dancers,Jazz Works, Tiawanaku Bolivian DanceGroup, and the Kalaanjali School of Danceand Music with Bharatanatyam ClassicalIndian dance. Speakers at the Rally includeRacine County Executive and WAAODABoard Member William McReynolds, DaneCounty Executive Kathleen Falk, CentroHispano Executive Director and WAAODABoard Member Peter Muñoz, Mark Sandersof the Great Lakes Addiction TechnologyTransfer Center, and others.
The goal of our Recovery Rally is toincrease awareness throughout the stateof the terrible, tragic toll of substance abuseon Wisconsin communities, families, andproductive citizens. Wisconsin still leadsthe nation in the per capita consumptionalcohol beverages and women drinkingwhile pregnant, and ranks high in otherindicators of substance abuse. Alcoholand other drug abuse has a staggeringeconomic impact on Wisconsin, too—almost$5 billion per year.
But the Recovery Rally celebrates hopeand resolve: Recovery happens every day!
In conjunction with the 2005 RecoveryRally, we are sponsoring a 5K (3-mile) walk,starting at the Camp Randall Stadium at8:30 a.m. and arriving at the West Wing ofthe State Capitol in time for the Rally. Thetheme of the 2005 Recovery Rally Walk is,“You don’t have to run, you can walk forrecovery!” WAAODA President Steve Tatewill lead the Walk for Recovery to theState Capitol.
More than 570 people from 34 Wisconsincities and three other states attended the2004 Rally. Rally organizers WAAODA andAFRA reported that at least 24 for-profit busi-nesses provided sponsorships and donationsin support of recovery from substance abuse.
The 2005 Recovery Rally will attracthundreds to enjoy the music and dance andcelebrate recovery from alcohol and otherdrug abuse. Participation of those who arein recovery and their family members andfriends will offer proof that recovery worksand that recovery happens every day.
For more information, please contact: WAAODA, Inc.6601 Grand Teton Plaza, Suite AMadison, WI 53719Phone: (608) 276-3400; 1-800-787-9979Fax: (608) 276-3402E-mail: [email protected]: www.waaoda.org
NEWSTART TO PARTICIPATE INNATIONAL STUDY SPONSORED BYTEXAS CHRISTIAN UNIVERSITY
The study sponsored by TCU focuses ondeveloping an assessment and informationsystem for drug abuse treatment providersthat will monitor organizational attributesand program resources, and link these fac-tors to client performance and programchanges over time. It uses a program change
model as a conceptual framework for get-ting the system incorporated into practice.The sample consists of 100 outpatient drug-free community-based treatment providers.Our primary goal is to develop reliableinstruments that can measure and providefeedback on program resources and organi-zational dynamics (along with aggregatedclient data) for the purpose of clinical man-agement in real world community settingswhere the majority of substance abuse treat-ment occurs. The specific aims of this pro-posed project are to – (1) develop a set offield instruments and procedures (i.e., theOrganizational and Resource Assessments,ORA) that treatment programs are willingto implement and use; (2) demonstrate thefeasibility and utility of these assessmentsin a sample of 100 outpatient drug freetreatment providers from two regions in theU.S.; (3) monitor organizational changesover time and relate them to client-levelindicators of program effectiveness; (4) planand evaluate a training protocol for programdirectors on how to use ORA informationsystems for improving program managementand functioning; and (5) study the processof program change and the long-rangeimplementation of this new technology.
The TCU study hopes to examine a num-ber of different hypotheses. They are:
a. better program functioning will beassociated with a higher level ofservices, better training resources,lower staff turnover, accreditations,and a stable organizational climate.
b. better program functioning will beassociated with higher staff levels,lower staff/client ratios, higher edu-cation and certification levels amongstaff, and higher levels of revenues.
c. better program functioning will beassociated with staff who are growth-oriented and have high levels ofinfluence, efficacy, and adaptability,and an organizational climate thathas a clear mission, strong communi-cation, high staff cohesion, and arechange-oriented.
d. better program functioning will beassociated with adoption of new tech-nologies, especially those involvingevidence-based clinical strategies andcounseling approaches.
The first subject pool consists of treat-ment program staff and the second is the
N e w S t a r t V o l u m e X X V • F a l l 2 0 0 5 2

Guest Article:
“Light” at the End of theAddiction Tunnel forQuad/Graphics Employeesand Family MembersBill Arnold, CADC III, CCS II, ICADC
Most people in Wisconsin obtain health insurancethrough their employer. But even insured personsare often ‘under-insured’ or even uninsured foraddiction services. One Wisconsin employer handlesthe health care needs of its employees differently: itdoesn’t buy insurance, but has developed its ownhealth care delivery system, hiring primary carephysicians, nurses, and behavioral health profes-sionals to work in company-owned facilities, sup-plementing company-operated clinics with localproviders as necessary. NewStart is pleased thatQuad/Graphics accepted our invitation to ‘sharetheir story’ in our Newsletter.
Quad/Graphics is the largest privatelyheld printing company in the western hemi-sphere, with 12,000 employees and annualsales of over two billion dollars. Its head-quarters are in Sussex, Wisconsin.
In 1990 Quad/Graphics initiated the firstof three benchmark experiments, the open-ing of the first onsite medical clinic in aQuad/Graphics production plant. The clinicsare managed and run by Quad/Graphicsemployees and perform services rangingfrom routine prenatal exams to minor surgi-cal procedures. Ultimately, two more med-ical clinics opened in other plants inWisconsin and one in our Saratoga Springs,New York plant. Including employees anddependents, health care services are offeredfor over 21,000 ‘covered lives’.
It was in 1991 that we pioneered ouronsite alcohol and drug treatment program.Consistent with the mission of the medicalclinics—to promote comprehensive well-ness—establishing the recovery programwas a natural next step for our company. Bybringing AODA treatment in-house, wewould know exactly what kind of servicesour employees were getting. Quad/GraphicsAODA Counseling Services is a WisconsinState Certified all inclusive outpatientAODA treatment program. The program was,and continues to be, far more successfulthan we ever envisioned. The quality of ourservices has also been recognized by others:Quad/Med LLC AODA Counseling Serviceswas presented with The Meta House Sub-
A P R O G R A M O F H E A L I N G F O R A L C O H O L A N D D R U G U S E D I S O R D E R S 3
client pool. The staff pool will includeprogram directors, financial officers, andclinical staff (counselors). The first sub-ject pool will be asked to complete a sur-vey. This survey will measureorganizational structure, capacity, pro-gram outcomes, revenues, costs, staffbackground, motivation, attitudes.
TCU hypothesizes that there is a con-nection between the organization of thetreatment center and the effectiveness intreatment. NewStart is excited to be apartof this nationwide study and looks for-ward to examining the results.
LIMITATIONS ON BUPRENORPHINELIGHTENED
Since the federal Center for SubstanceAbuse Treatment and the DEA implement-ed office-based treatment of opioid addic-tion with buprenorphine in 2003 (inresponse to Congress’ Drug AddictionTreatment Act of 2002, DATA), medicalgroup practices have been limited toadmitting a census 30 patients at a giventime for buprenorphine treatment. Thismeant that solo practices could treat 30patients; a two-person group like the New-Start physicians could treat 30 patients;or a 1000-physician group like the MayoClinic could treat 30 patients. This didn’tseem logical or fair to many persons inthe addiction treatment field, but it wasthe law, and we’ve followed it.
NewStart has been treating selectedpatients using Suboxone brand ofbuprenorphine since the spring of 2003;over 60 patients have been started on Sub-oxone for detoxification or maintenancetreatment. Twenty-nine patients are cur-rently in ongoing outpatient treatment.
But August 3, President Bush signedlegislation that had worked its waythrough Congress, to take away the 30-patients-per-group-practice ceiling. Now,each ‘qualified physician’ can treat up to30 patients with this treatment method.So NewStart’s two physicians will gradu-ally raise our census of Suboxone patientsto 60. Patients are still selected carefullyand must agree to detailed treatment con-tracts. Drs. Miller and Powell are pleasedto be able to offer this treatment when itis indicated, and are delighted thatrestrictions on total patient census arenot as burdensome as they have been forthe last two years.
stance Abuse Awareness Award for Corpo-rate Leadership in 1999.
Our goal is to make addiction recoveryas easy to access as possible. An employeecalls me directly to schedule an intake ses-sion. There is NO CHARGE for any individ-ual or group counseling and NO LIMIT onthe number of sessions.
Our third experiment was the most chal-lenging. I was meeting with one of the VicePresidents shortly after starting up theAlcohol and Drug Treatment Program. Heasked me if I ever thought it would be agood idea to have volunteers who had gonethrough the Quad/Graphics Recovery Pro-gram wear a patch on their uniform as con-tact people in the workforce for otheremployees who wanted to get into recovery.(All employees wear uniforms atQuad/Graphics, including the CEO and Pres-ident). I initially rejected the idea becausewe are very conscientious about the impor-tance of confidentiality particularly becauseour services are onsite. After many days ofreview, I asked some of the clients whom Ihad worked with previously at Quad/Graph-ics if they would be interested in a volun-teer program of wearing a patch on theiruniform, signifying the “unspoken advo-cates of recovery” for employees, so therecould be an avenue to get quick and compre-hensive treatment.
As it turns out, the group decided that apatch of a lighthouse—signifying hope anddirection—would be appropriate for theirvolunteer services. Currently there are over140 employees who have signed on to thevolunteer program, and we are representedin all of our major printing plants in thecountry. Any Quad/Graphics employee instable recovery, no matter where they wentto treatment, can apply to be a “lighthouse”volunteer; and when approached by anoth-er employee, the conversation is bound byconfidentiality—even I don’t know aboutit if the employee decides not to accessservices at that time.
Our goal at Quad/Graphics is “to get sub-stance abuse and recovery out of the closet”,out of darkness and into light. Our employ-ees know that is okay and desirable to getthe help you need to overcome substanceuse issues and still work at Quad/Graphics.
Bill Arnold, CADC III, CCS II, ICADC, is the Direc-tor, Manager, and Founder of The Quad/Med LLCSubstance Abuse Counseling Services, and founderof the Friends Of Recovery “Lighthouse Patch”Volunteer Program at Quad/Graphics.

Marijuana: Health Benefits?Michael M. Miller, M.D.,MeriterHospital NewStart Medical Director
© 2005 Meriter Hospital
Permission is granted to reprint this publication without alter-ations for general patient use: You must cite Meriter Hospitalas the copyright holder, along with the title and year of publica-tion, followed with the words “Reprinted with permission.”
Third in a three-part series on marijuana.
Dr. Miller addressed Marijuana’s health effects in
the Fall 2004 NewStart Newsletter.
“Drugs Kill.” It’s a phrase we’ve heardmany times. Alcohol and other “rewarding”drugs certainly have the potential to pro-duce health problems, even death, due toeffects of intoxication, overdose or chronicuse. Marijuana is not a lethal drug, how-ever, and marijuana addiction—while itcan lead to significant impairments infunctioning—does not result in mortalitylike many other “drugs of abuse.”
“Drugs Heal.” That’s a sign that couldhang outside of pharmacies. Many kindsof medications act on the body to changefunctioning or to abort or reverse thecourse of illness. Significant debate inpopular, even political circles—not justin scientific and medical circles—centerson whether, and to what extent, marijuanaor active ingredients in the marijuanaplant (or chemicals synthesized in a labthat are similar to the chemicals inmarijuana) have effects that are beneficialto human health.
Marijuana’s effects are well known:relaxation, euphoria, blood pressure andpulse changes, changes in blood vessels andappetite, changes in perception (especiallytime perception), etc. However, someeffects of marijuana may prove to be sobeneficial that chemicals from marijuanamay be useful as medications some day.In fact, there are already some benefitsso well established that the active ingre-dient in cannabis (the marijuana plant),delta-9-THC, is available in an oral capsuleform, called dronabinol (the trade name is Marinol).
Many health claims have been madeabout marijuana or chemicals similar toTHC called cannabinoids. But scientificresearch has confirmed safety and efficacyonly to the extent that the Federal Food andDrug Administration has approved Marinolfor two indications. One, to treat nausea incancer chemotherapy patients who have notresponded to other medications used tocontrol nausea and vomiting. And two, tostimulate appetite in patients who have
branes, the cell changes its functioning,resulting in changes in emotional, motor,perceptual, cognitive or overall behavioralfunctioning. There are three well-knowncannabinoid receptors: CB1, CB2, and CB3.What is also known is that there are natu-rally occurring chemicals in the humanbody that attach to these cannabinoidreceptors. Anandamide is the name of oneof the endogenous chemicals, made by thehuman body, that acts on cannabinoidreceptors.
What is the role of endogenous cannabi-noids? The best available knowledge is thatthey affect inflammation and the abilityof other naturally occurring chemicals,called prostaglandins, to produce an anti-inflammatory response in general. CB1receptors are located in regions of the brainthat control mood, motor control, memoryformation, regulation of food intake andcentral control of cardiovascular and repro-ductive functioning. CB1 receptors are alsopresent in areas that control processingof pain information. CB2 receptors seemconcentrated in areas that influence theimmune response, and in reproductiveglands. Another identified receptor is theCB3 receptor. It is thought that pharmaceu-tical companies have, in their development“pipelines,” synthetic products that serveas both agonists and antagonists to CB1, CB2and CB3 receptors. Current research willdetermine what happens when you agonize(turn on) or antagonize (turn off) one or acombination of these CB receptors.
So there are legitimate medical questionsabout the use of cannabinoids as analgesics,as they have the ability to directly affectthe body’s ability to produce and interpretinformation about pain. It is also knownthat cannabinoids can potentate the painrelieving actions of opioid analgesics.
Here is what research has shown so far.Five milligrams of medicinal THC is equiva-lent to 30 milligrams of codeine as a painreliever. Ten milligrams of medicinal THCis equivalent to 60 milligrams of codeine.Twenty milligrams of medicinal THC hasthe potency of 120 milligrams of codeine.However, even when given in this oral,medicinal form, patients experience sideeffects to the higher doses of pharmaceu-
N e w S t a r t V o l u m e X X V • F a l l 2 0 0 5 4
been wasting away from AIDS, to help themregain weight. There are many otherindications for which delta-9-THC has beenalleged to be beneficial—to treat spasticityin patients with multiple sclerosis, to lowerintraocular pressure in patients with glau-coma, etc. However, the FDA has not foundconvincing evidence from research studiesto grant the manufacturer of Marinol theauthority to state that these conditions arean approved indication for this medication.In England, there is no pharmaceutical THCavailable, but drug companies are licensedto market nabilone, a synthetic cannabinoid.
What has been discovered the last 25years is that the reason delta-9-THC has aneffect on the brain is that there are braincell receptors that respond to THC. Thus,when THC comes into contact with thesespecialized regions on nerve cell mem-

tical THC, including sedation, confusion,dizziness, uncoordination, slurred speech,disorientation, disconnected thoughts,impaired memory, blurred vision and drymouth. The 20-milligram dose of oral THCis tolerated by few patients in clinicaltrials. The 10-milligram dose is somewhatbetter tolerated, but has clearly moreadverse effects than when people take a 60-milligram dose of codeine. The five-milligram dose of THC is well tolerated,and does not change consciousness orbehavior in ways patients find uncomfort-able. Note, however, that five milligramsof THC has a pain-killing potency equalto only 30 milligrams of codeine. Mostpatients with significant pain conditionscertainly need a higher dose of opiateanalgesic than that.
There are several groups of patients forwhom it was hoped that cannabinoidsmight prove to be effective analgesics: indi-viduals with neuropathic pain (peripheralnerves themselves are injured), patientswith cancer pain and patients with painfrom AIDS. The problem is that it has notbeen shown that pharmaceutical cannabi-noid has the power to block pain in thesepatients effectively without producingundesirable side effects.
The medical question is, are thereconditions for which pharmaceuticalcannabinoids will be beneficial?Researchers are looking into alternativedelivery systems for cannabinoids—suchas nasal sprays and inhalers—which mightoffer better ways to deliver the drug to thebloodstream and the brain. Still, there’sthe question of side effects.
The political question, however, iswhether smoked marijuana has medicinalbenefits to the extent it should beapproved as a medicine, thus made legalfor “patients.” The political debate, wellpublicized in the media, is whether medicalmarijuana should be legalized in variousstates. What has happened is that when thequestion is put to referendums, citizensalmost always vote in significant majoritiesin favor of “legalizing medical marijuana.”
The reason people vote this way is fairlyobvious. The question is posed as, “if some-
thing isn’t really harmful (the assumptionis that marijuana is a benign agent), andthere are patients who are really suffering(such as AIDS patients), would you want tomake it okay for them to smoke this benignproduct and get benefits, rather than beingthrown in jail?” Of course, the compassion-ate side of voters says “yes” to such issues.
Physician organizations don’t agree,because they look to the medical evidence.The American Medical Association and theAmerican Society of Addiction Medicinepositions on this question are explicit. Theseorganizations support that well-supervisedbiomedical research—clinical trials—beconducted to answer questions about thebenefit/risk ratio of using smoked mari-juana to treat various medical conditions.
include acute adverse effects (bothersomedry mouth, blurry vision, palpitations andanxiety or other psychiatric phenomenon)and the potential chronic effects of smok-ing. Finally, research is pretty clear nowthat the amount of analgesic effect one canget from smoked marijuana does not exceedthe analgesic potency of 30 milligrams ofcodeine. So there is not much true benefitto be derived, despite the acute and poten-tial chronic adverse effects.
This sort of medical information rarelyenters the public (“media”) or politicaldebate. In Wisconsin, the chairman of theAssembly Health Committee has introduceda medical marijuana bill. This bill, likemost around the country, is well intended.The problem is that there is no medical evi-dence to show that smoked marijuana hasbenefits to a sufficient degree to warrantits use given its side effects and the poten-tial for harmful outcomes from long-termuse—not the least of which is the fact thatprobably 10 percent of marijuana users dodevelop addiction with long-term use.
The question of whether drugs should belegalized in America is a complex one. Com-pared to other countries, the United Stateshas stringent laws and harsh penaltieswith respect to euphoria-producing chemi-cals. In some countries, such as Mexico,opioid analgesics are available over thecounter, without a prescription.
“Medical marijuana” proponents areleading the debate about whether using andpossessing marijuana should be decriminal-ized. Some proponents of “medical marijua-na,” such as National Organization for theReform of Marijuana Laws (NORML) clearlybelieve that this is a health issue, but many“medical marijuana” proponents havebroader political agendas, and are usingefforts to decriminalize marijuana for“medical use” as a subterfuge—a way to getthe public gradually comfortable with theidea of overall decriminalization. Legaliza-tion arguments should be analyzed on theirown merits—but current biomedical evi-dence does not support the “medical argu-ment” as a compelling one for legislativeaction to decriminalize marijuana.
A P R O G R A M O F H E A L I N G F O R A L C O H O L A N D D R U G U S E D I S O R D E R S 5
To date, no published study shows that
smoked marijuana provides clear-cut bene-
fits for any of the conditions for which
Marinol is currently approved.
Of course, in calculating a benefit/risk
ratio, one has to factor in the negative
health effects of delivering marijuana to
the body via smoking. On one hand, deliver-
ing a predictable dose via the smoked route
is challenging. On the other hand, smoke
itself contains harmful chemicals, including
carbon monoxide and carcinogens. Use of
smoked marijuana has limitations that

• Yes, poppy seed muffins can produce urinedrug tests positive for ‘opiates’. One way torule-out a false-positive is that, whenpoppy seeds have caused the positive test,the ratio of morphine to codeine is greaterthan 5:1. (To get this kind of quantitativeand specific information, more expensiveand time-consuming GC/MS confirmatorytesting is required. Call the laboratory ifthe quantitation is necessary.
• Another thing to watch for: somehydrocodone (the active ingredient inVicodin) is metabolized into hydromoro-phone (the active ingredient in Dilaudid).So a urine ‘positive’ for hydromorphonemight be explained by the fact that thepatient has taken hydrocodone.
• Methadone is included in several of thenew GML panels; but if one is using a dif-ferent lab, and one is interested in author-ized or unauthorized use of this compound,one has to be sure that the drug testordered has methadone in its contents.
• Physicians Plus and other Wisconsinhealth insurers are required to considerlab tests, including urine drug tests, to be‘medical care’, and thus the costs of testingdo not count against the limited insurancebenefits for inpatient/outpatient mentalhealth or addiction care. So any primarycare physician or behavioral healthcareprovider can order a urine drug test, and itwon’t come out of the ‘behavioral health’benefits. But this is not the case for all payors,e.g., ERISA-exempt plans, so you may needto check with the patient’s carrier, espe-cially for the more expensive tests.
There are many options for using urineto detect recent drug use. It is important toremember that confirmation of the factthere has been recent substance use by nomeans confirms that a patient has addic-tion or another substance use disorder.
NEWSTART RETREATMichael Gerst, MSW, CADC III, CAPSW
NewStart staff participated in a retreaton June 8th, 2005. NewStart is a multi-leveled AODA/mental health treatmentfacility that draws on the talents of manydisciplines to complete its work. A retreatgives NewStart the time to stop evaluateand find more effective and patient orien-tated methods of operations.
N e w S t a r t V o l u m e X X V • F a l l 2 0 0 5 6
CLINICAL TIPS REGARDING USE OFURINE DRUG TESTS
In the last issue of the NewStart Newsletter,we introduced the newly formatted urinedrug test panels, and urine drug test reportslips, that had been constructed for clinicalsettings by Meriter’s General Medical Labo-ratories (GML). In this issue, we providesome helpful tips on how best to interpreturine drug tests in clinical practice.
• Many people have questions about testingfor THC, the active ingredient in mari-juana. Over-the-counter ‘kits’ will haveadequate specificity for THC, but thedetection thresholds may be rather high,and only qualitative ‘answers’ can begleaned from these inexpensive testingmethods. GML reports a ‘positive’ resultin a clinical test for a THC level of 20 orgreater. But a specific advantage of panelsordered through GML (or, a single-drug testrequest for THC) is that GML quantifiesTHC and also quantifies the creatininelevel in the urine, then calculates aTHC/creatinine ratio. It is this ratio thatcan be trended over time to see if apatient’s THC levels are rising or falling.Normal dilutional effects (diet, illness) canaffect the urine, as can conscious attemptsby the patient to overhydrate themselves.Use of these THC/creatinine ratios hasproven very helpful in NewStart whenreviewing sequential test results.
• Some benzodiazepines are hard to detectusing even GC/MS methodologies. If a doc-tor is concerned about unauthorized useof a sedative/hypnotic, and the patientneeds treatment with a benzodiazepinefor a medical/psychiatric condition, onestrategy is to prescribe clonazepam orlorazepam, for many urine drug tests willread ‘negative’; then if the urine drug testreturns ‘positive’, it is a fair assumptionthat the person has used a compound notauthorized for their use. If clonazepamand/or lorazepam testing is required callthe laboratory or order a panel thatincludes them.
• One needs to be quite careful in interpret-ing results of urine drug tests for opioidanalgesics. Most drug tests comply withthe federal Department of Transportationrequirement to test for ‘opiates’, not‘opioids’. ‘Opiates’ refers to the naturalproducts derived from the opium poppy:codeine (which is a pro-drug, exerting its
effects after its metabolism into morphine),morphine, and heroin, which is diacetyl-morphine. So a patient could be prescribed,or could be illicitly taking/snorting/shooting,a synthetic or semi-synthetic ‘opioid’ such asmeperidine (Demerol), oxycodone (Percocet),hydrocodone (Vicodin), hydromorphone(Dilaudid), or methadone (Dolophine), andthe drug test report would give the result“Negative”. This reality can be turned intoan advantage by a physician: if a doctor isconcerned about unauthorized use of a nar-cotic analgesic, and the patient needs treat-ment with such a pain-killer, one strategyis to prescribe one of these agents other thancodeine or morphine; then if the urine drugtest returns ‘positive’, it is a fair assumptionthat the person has used codeine, morphineor heroin, which are not metabolic break-down products of the synthetic opioids.
• Based on the above discussion, it’s impor-tant to not come to a hasty conclusion thata patient is non-compliant with (or divert-ing) the opioid one has prescribe for painrelief, just because the drug test result is‘negative’; make sure that the compoundyou’re trying to detect is part of the con-tents of the drug test panel you ordered.The new GML panels make it far easier forthe physician to order the test that willgive the information he/she is looking for.
• A side comment: codeine does requiremetabolism by the cytochrome p450isoenzyme 2D6 in the liver, for it to beconverted into the active analgesic mor-phine. About 10 percent of the populationlacks this metabolic enzyme. So a patientprescribed higher and higher doses ofcodeine who says ‘Doctor, this isn’t work-ing’, may be right!
• Note that codeine and heroin (diacetyl-morphine) are both metabolized to mor-phine; but it doesn’t go in the otherdirection. So a patient authorized to takecodeine will have codeine and morphinereported ‘positive’ on comprehensive drugtest panels that use GC/MS methods, and apatient using heroin will have morphinereported ‘positive’ (6-mono-acetyl-mor-phine is the first break-down product ofheroin, and detecting it in the urine isconfirmatory for heroin use, but it lingersin the body only a few hours, so usually isnot detected). But a patient using heroin orMS Contin who has a urine positive forcodeine, has obtained that codeine fromanother source!

This year the retreat had two aims: oneto evaluate progress on action plans of 2005and to plan for new action plans for 2006.
Newstart decided on three action plansfor 2005. They were
• improve customer service,
• improve handoffs between levels of care,and
• improve communications betweenUtilization Review and therapists.
Reviewing the action plans for 2005substantial improvements were made in:
• NewStart has improved customer services,as evidenced by improvement in customerservices scores. In general NewStart scoresextremely well with customer satisfaction,however one score was bothersome. Afterreflecting on our practice we made someadjustments. As a result the patientsatisfaction score went from 47 percentsatisfaction to 94 percent satisfaction.
• Improving communications betweenUtilization Review and therapists asevidenced by substantial decrease in thenumber of unauthorized charges.
• NewStart improved handoffs betweenlevels of care by creating check lists forRN and therapists to follow.
Looking to the future the action plans for2006 include:
Patient Satisfaction
• Patient Satisfaction Questionnaires willinclude items regarding satisfaction withprogram elements such as small groupexperience, individual sessions, familyprogramming, and patient education con-tent (lectures, videos); make changes inprogramming based on survey results.
Clinical Outcomes
• Reduce variation in clinical approach
• Standardize patient education contentacross services
• Better cataloging of Patient Educationmaterials
• Resource Book of group activities thatclinicians could draw from
• Review curriculum of IOP: patient activities
• Twelve Step Facilitation and standardiz-ing expectations
NewStart will continue to hold retreatson a yearly basis to review our program-ming and examine our practice guidelines.NewStart recognizes the need to reflect onour practice so that we will provide thebest possible treatment for our patients.
A P R O G R A M O F H E A L I N G F O R A L C O H O L A N D D R U G U S E D I S O R D E R S 7
STAFF PROFILE: SUE KLEIN-KENNEDY, MS, CADCIIISue started working for Meriter Hospital as a recreational therapist on a part-time basis until she
graduated from College. Sue worked for Tellurian for approximately 3 years until she came to APEC(Alcohol Prevention and Education of Madison General Hospital) in 1977. Sue then worked for theAPEC/NewStart Satellite clinic in Mount Horeb for 20 years doing general outpatient alcohol and drugtreatment until she moved to the Gammon Lane clinic in 2002.
Q. How and why did you get into this work?A. “I was a recreational therapist at Madison General Hospital and they kept bugging
me to be a counselor—I did the rec. therapy consultations. Originally, I didn’t want tobe a counselor anymore because I like rec. therapy so much. Actually, I really wanted tocoach women’s college sports. It wasn’t planned at all and I haven’t gotten out yet. I likehelping people and seeing them change and I like the people I work with. I love the flex-ibility that I am given in my job at NewStart.”
Q. What is the therapist role in all addiction therapy?A. “To help them discover who they are and what is stopping them from becoming
happy with who they are. To help them develop the healthy skills to find who they are.To role model healthy, assertive communication, caring and support, and teach themhow to trust themselves. Also learn how to have fun again.”
Q. What style of therapy do you use?A. “I use an eclectic mix of therapy techniques—CBT (Cognitive Behavioral Therapy),
EMDR (Eye Movement Desensitization and Reprogramming)... a little but of everything.I think that I am fairly unrigid and go a long way with people. I like to have people topick their goals and have a say in their treatment.”
Q. How did you get into this work?A. “I took job at Tellurian and learned about alcohol and drug treatment. I then took
a job at APEC/NewStart again and the rest is history.”
Q. What keeps you going in the business?A. “Seeing people change…becoming happy and healthy people.”
Sue is an integral member of the NewStart team. She is involved in assessments forpotential patients, individual therapy, couples therapy, and several continuing caregroups, including two women’s only continuing care groups.
NewStart Medical Director Michael M. Miller, M.D., FASAM, is presented the Wisconsin Association on Alcohol and Other DrugAbuse’s 2005 Professional of the Year Award by Lawrence S. Brown, Jr., MD, MPH, FASAM, Medical Director of Addiction
Research and Treatment Corporation of Brooklyn, NY. at the 39th Annual WAAODA Conference on May 10th. Dr. Brown is Imme-diate Past President of the American Society of Addiction Medicine. Dr. Miller is President-Elect of ASAM.
COERCED TREATMENT
The only requirement for membership inAA is ‘a desire to stop drinking.’ A substanceuser’s internal motivation to change theirbehavior is an important variable in treat-ment outcome. Reliable methods exist toassess a person’s motivational level (such asthe University of Rhode Island ChangeAssessment), and clinical methods havebeen developed to enhance a person’s moti-vation and move them along the continuumof motivation to change as described by Pro-chaska and diClemente (the authors of theURICA). MET, or Motivation EnhancementTreatment, was one of the three approachesused in the famous NIAAA study ProjectMATCH. Researchers from Texas ChristianUniversity have shown that while ‘intra-treatment factors’ are very important ineventual outcome (what happens to patientsduring treatment), ‘pre-treatment factors’are also important, and proactive efforts tomotivate them to enter treatment, as wellas to engage them so they don’t depart earlyfrom treatment, are critical as well.
So what about the corollary to this: if aperson ‘isn’t ready’, doesn’t have the inter-nal motivation, isn’t contemplating quittinguse, is treatment worthwhile? The answer,from the literature, is a clear-cut ‘Yes’.
Much is known about so-called ‘coercedtreatment.’ ‘Coersion’ can take many forms.At the extreme, there is the civil commit-ment process, in which a court determines
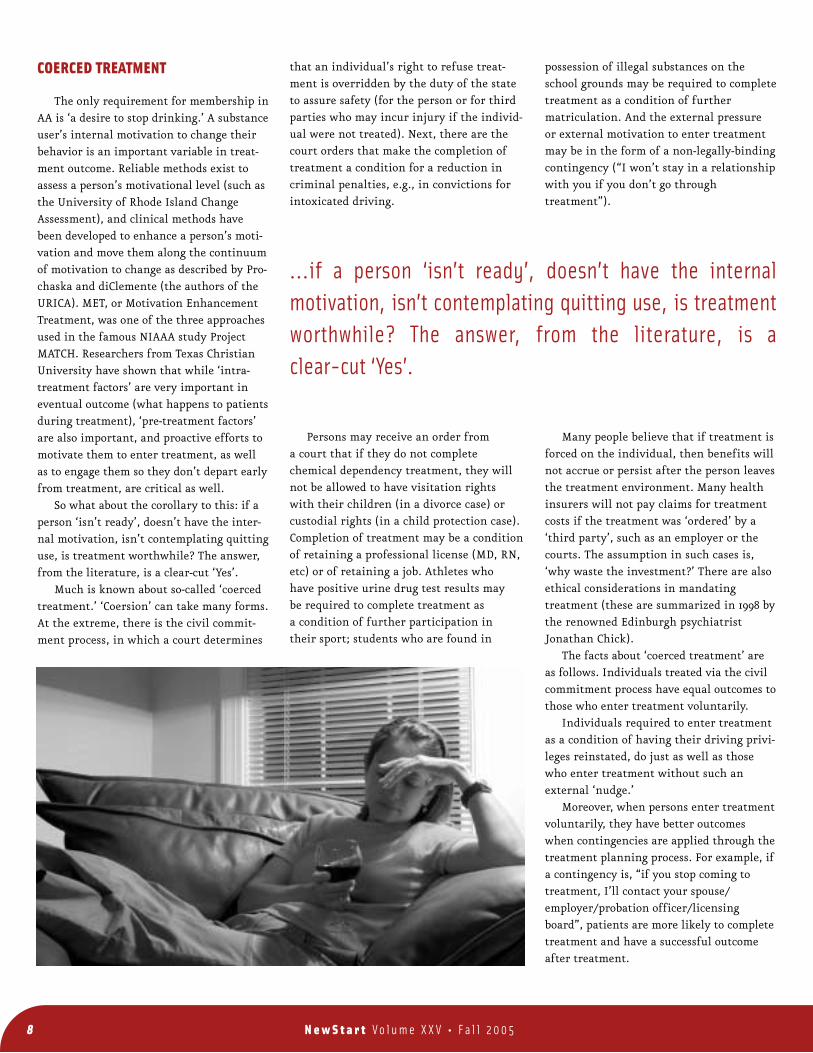
possession of illegal substances on theschool grounds may be required to completetreatment as a condition of furthermatriculation. And the external pressureor external motivation to enter treatmentmay be in the form of a non-legally-bindingcontingency (“I won’t stay in a relationshipwith you if you don’t go throughtreatment”).
Many people believe that if treatment isforced on the individual, then benefits willnot accrue or persist after the person leavesthe treatment environment. Many healthinsurers will not pay claims for treatmentcosts if the treatment was ‘ordered’ by a‘third party’, such as an employer or thecourts. The assumption in such cases is,‘why waste the investment?’ There are alsoethical considerations in mandatingtreatment (these are summarized in 1998 bythe renowned Edinburgh psychiatristJonathan Chick).
The facts about ‘coerced treatment’ areas follows. Individuals treated via the civilcommitment process have equal outcomes tothose who enter treatment voluntarily.
Individuals required to enter treatmentas a condition of having their driving privi-leges reinstated, do just as well as thosewho enter treatment without such anexternal ‘nudge.’
Moreover, when persons enter treatmentvoluntarily, they have better outcomeswhen contingencies are applied through thetreatment planning process. For example, ifa contingency is, “if you stop coming totreatment, I’ll contact your spouse/employer/probation officer/licensingboard”, patients are more likely to complete treatment and have a successful outcomeafter treatment.
that an individual’s right to refuse treat-ment is overridden by the duty of the stateto assure safety (for the person or for thirdparties who may incur injury if the individ-ual were not treated). Next, there are thecourt orders that make the completion oftreatment a condition for a reduction incriminal penalties, e.g., in convictions forintoxicated driving.
Persons may receive an order froma court that if they do not completechemical dependency treatment, they willnot be allowed to have visitation rightswith their children (in a divorce case) orcustodial rights (in a child protection case).Completion of treatment may be a conditionof retaining a professional license (MD, RN,etc) or of retaining a job. Athletes whohave positive urine drug test results maybe required to complete treatment asa condition of further participation intheir sport; students who are found in
…if a person ‘isn’t ready’, doesn’t have the internalmotivation, isn’t contemplating quitting use, is treatmentworthwhile? The answer, from the literature, is a clear-cut ‘Yes’.
N e w S t a r t V o l u m e X X V • F a l l 2 0 0 5 8

(averaging 500 days after treatment entry)the health-related quality of life scores ona standardized questionnaire were betterfor the committed-and-treated group thanfor other cohorts of alcoholics post-treat-ment. Moreover, viewing their treatmentretrospectively, a majority of those who hadundergone civil commitment believed it hadbeen justified and that the treatment hadbeen useful. These authors described civilcommitment of these alcohol patients ashaving been a ‘life-saving’ intervention.
One hypothesis to explain why ‘coerced’patients do as well as ‘non-coerced’ patientsis the notion that no treatment for addictionis 100% voluntary. Persons with addictionare universally ambivalent about their ill-ness: there are aspects of their substance use
that they view as positive, and other aspectsthey recognize as negative. Through the nat-ural processes of defense mechanisms andcognitive reframing (combined with possibleconstitutional differences in the way theirfrontal lobes make judgments to ascribe‘value’ to the rewards and punishments thatcome from substance use), substance addictsunder-value the negative aspects of use andover-value the positive aspects of use. Theymay want to cease (possibly to make othersaround them happier) but they still want tobe able to use (though maybe in a less out-of-control manner). Their ambivalence aboutwhether or not to cease use, and whether ornot to enter treatment, gets resolved on theside of entering treatment, largely due toexternal pressures they perceive in theirlives. These pressures may be more subtle (agradual withdrawal of affection from a lifepartner) or may be more overt (a summonsfrom a deputy). But everyone who enters
treatment for addiction has experiencedsome sort of ‘nudge.’ The most recent studyin the literature on this topic (2004)assessed motivational level in patientscoerced by the legal system compared tonon-coerced outpatients, and discoveredthat it was the coerced cohort that—afteraddiction severity and prior treatment werecontrolled for—had higher readiness forchange at treatment entry. Maybe they per-ceived that they had more to lose by notchanging their behavior patterns. One trendthat emerged from many of these studies isthat outcome doesn’t depend as much onthe degree of coercion at treatment entry asit depends on the amount of support onehas after treatment.
Wisconsin Statutes do provide for theinvoluntary treatment of persons with alco-holism. If an individual has a pattern ofheavy drinking and a pattern of lifeimpairments due to drinking, and it can bedemonstrated that it would be dangerous orlife-threatening to the patient, or to others,for them to continue drinking, and if theyhave refused voluntary treatment, then apetition can be signed by three adults andsubmitted to the probate court in the coun-ty of the individual’s residence. This israrely necessary, but our experience is com-parable to that reported in the literature.Persons with severe medical problems dueto their drinking, and inadequate socialsupports for sobriety, can be committed bythe courts, and can have good outcomesafter involuntary treatment.
Gallant DM et al. Quarterly Journal of Studieson Alcohol 29:77-83 (1968)
Rosenberg CM and Liftik J. Journal of Studies onAlcohol 37:58-65 (1976)
Vogler et al. Journal of Community Psychology4:357-61 (1976)
Moberg DP et al. International Journal of theAddictions 17:549-67 (1982)
Hoffmann NG et al. Journal of Studies onAlcohol 48:591-94 (1987)
Watson, CG et al. Journal of Clinical Psychology44:573-81 (1988)
Brizer DA, Maslansky R, and Galanter M.American Journal of Drug and Alcohol Abuse16:269-64 (1990)
Chick J. Alcohol & Alcoholism. 33:20-25 (1998)
Bourquin-Tieche D, et al. European AddictionResearch 7:48-55 (2001)
Gregoire TK, Burke AC. Journal of SubstanceAbuse Treatment 26:337-43 (2004).
Scientific literature confirming thisextends over four decades. Gallant etal.(1968) found that parolees required toattend outpatient treatment had betterclinic attendance and lower rates of crimi-nal offenses than voluntary patients in thesame clinic. As far back as 1976, it wasreported that retention in outpatient treat-ment in Boston was far greater for personsmandated to treatment after a drunkendriving than for voluntary clinic patients.Marc Galanter’s group in New York City(1990) published similar results: treatmentretention (not dropping out) was identicalin voluntary outpatients and those coercedby a public assistance agency. Vogler et al.reported (1976) no differences in one-yearoutcome for patients in a 17-week treatment
program between legal system referralsand self-referrals. Paul Moberg of the UW-Madison (1982) studied inpatients referredby their employers and found that theinvolvement of the employer in the referralhad a positive influence on outcome at 9months, and that coercion by the employerhad no detrimental effect. Hoffmann et al.(1987) found that outcomes were no differ-ent between inpatients forced into treat-ment in the wake of a drunk drivingconviction and voluntary inpatients. Per-sons committed or coerced to enter a VAinpatient service had comparable outcomesto voluntary admits, and trends suggestedbetter outcomes for the former group (Wat-son et al., 1988). A more recent study of res-idential patients in Switzerland (2001)found that while the civil commitmentpatients had greater severity-of-illness atadmission based on bio-psycho-socialcomplications of their use, at follow-up
Persons with severe medical problems due to theirdrinking, and inadequate social supports for sobriety, canbe committed by the courts, and can have good outcomesafter involuntary treatment.
A P R O G R A M O F H E A L I N G F O R A L C O H O L A N D D R U G U S E D I S O R D E R S 9

The American Society of Addiction Medicine recentlyannounced that NewStart Physicians Ian Powell, M.D., andRandy Brown, M.D., passed the ASAM Certification Examina-tion in December 2004. ASAM certification is considered ‘thegold standard’ of physician expertise in the diagnosis andtreatment of substance related disorders, and is required byseveral states as a requirement for being a medical directorof a treatment program. It is recognized by many managedcare firms, the federal TriCare program, and many states(including Wisconsin) as an indicator of physician quality.Over 3500 physicians have become ASAM-certified since theinception of the certification program in 1986. NewStartMedical Director Michael Miller, M.D., certified in 1986 andrecertified in 1994, also passed his ASAM Recertificationexam in 2004, as well as his recertification exam in Addic-tion Psychiatry.
NewStartMeriter Hospital202 S. Park St.Madison, WI 53715(608) 267-6291www.meriter.com
Nonprofit Org.U.S. Postage
PAIDMadison, WI
Permit No. 1181
®
NEWSTART PHYSICIANS RECEIVE ASAM CERTIFICATION
NewStart Medical Director Michael M. Miller, M.D., FASAM,FAPA, ASAM President-Elect, is presented his Recertification Cer-tificate by Elizabeth F. Howell, M.D., FASAM, ASAM President.











![[XLS]secure2.vermonttreasurer.govsecure2.vermonttreasurer.gov/legacywebsite/www... · Web viewGGB GR0128010676 HELLENIC REPUBLIC BOND STEP CPN 24/FEB/2023 EUR 1 HELLENIC REP C Q67383GN5](https://img.dokumen.tips/doc/110x75/5b0451247f8b9a89208d6e18/xls-viewggb-gr0128010676-hellenic-republic-bond-step-cpn-24feb2023-eur-1-hellenic.jpg)