Embed Size (px)
Citation preview

2018Vol.4 No.4:15
Research Article
DOI: 10.21767/2469-2980.100065
Journal of Orthodontics & Endodontics ISSN 2469-2980
iMedPub Journalswww.imedpub.com
1© Under License of Creative Commons Attribution 3.0 License | This article is available in: http://orthodontics-endodontics.imedpub.com
Dejan Ćetković1, Vera Todorović2,3,4, Slobodan Marinković5*, Harun Hodžić5, Mirza Oruč6 and Jelena Boljanović7
1 InstituteofAnatomy,FacultyofDentalMedicine,UniversityofBelgrade,11000Belgrade,Serbia
2 DepartmentofBasicandPreclinicalStudies,FacultyofDentistry,26000Pančevo,UniversityofBusinessAcademy,NoviSad,Serbia
3 DepartrmentofHistologyandEmbriology,FacultyofMedicine,UniversityofZenica,72000Zenica,BosniaandHerzegovina
4 DepartmentofNursing,FacultyofMedicine,UniversityofZenica,72000Zenica,BosniaandHerzegovina
5 DepartmentofNeuroanatomy,FacultyofMedicine,InstituteofAnatomy,UniversityofBelgrade,11000Belgrade,Serbia
6 DepartmentofSurgery,FacultyofMedicine,UniversityofZenica,72000Zenica,BosniaandHerzegovina
7 FacultyofSpecialEducationandRehabilitation,UniversityofBelgrade,11000Belgrade,Serbia
*Corresponding author: Dr.SlobodanMarinković
DepartmentofNeuroanatomy,FacultyofMedicine,InstituteofAnatomy,UniversityofBelgrade,11000Belgrade,Serbia.
Tel: 00381644866829
Citation:ĆetkovićD,TodorovićV, MarinkovićS,HodžićH,OručM,etal.(2018)TheMaxillaryNeurovascularCanalsastheBasisfortheLocalAnesthesiaEfficacy.JOrthodEndodVol.4No.4:15
The Maxillary Neurovascular Canals as the Basis for the Local Anesthesia Efficacy
AbstractIt is not known the way in which a local anesthetic, following the AnteriorMiddleSuperiorAlveolar(AMSA)anesthesia,reachesthesuperiordentalplexus.Consequently,theaimofthestudywastoexaminethepossiblerouteofdiffusionof a local anesthetic from the anterior lateral palatal injection to the superiordentalplexus.Thepalatalandalveolarregionsof48drymaxillaewereexaminedand6autopsyspecimensofthesameregionwerepreparedforhistologicalandimmunohistochemicalanalysis.Thestudyrevealedpalatalandalveolarprocessopenings inall thespecimens.Theyaverage6.3 innumberclosetothecentralincisor,5.2tothelateralincisor,3.7tothecanine,3.8tothe1stpremolar,and3.9tothe2ndpremolar.Themicroscopicstructureoftheepithelium,laminapropria,submucous layer, arteries and nerves, periosteum, and cortical and spongiousbonewasdescribedindetail.Theneurovascularporesandcanalshadadiameteroftheiropeningof90.28–1,230.62µm(mean,893.62µm).Theinitialpartofthecanalsvariedindiameterbetween523.42µmand903.04µm(mean,622.93µm).Thecanalspenetratedthecorticalboneandusuallyterminatedinthespongiousbone towards the alveolar process. They contained a larger artery or severalsmallerarteries,someveins,afewtinynerves,collagenfiberstypeI,andsmallcollectionsofthefattycells.Theneurovascularcanalsandtheporesmostlikelyrepresentaroutefordiffusionofananestheticfromthelateralpalatalregiontothesuperiordentalplexus.
Keywords: Neurovascular canals; Maxilla; Anterior teeth; Anatomy; Histology;Localanesthesia
Received: November07,2018; Accepted: December12,2018; Published: December19,2018
IntroductionOneoftheproceduresindentistryistheAMSA(AnteriorMiddleSuperiorAlveolar) anesthesia, a relativelynew local anesthetictechnique, which has been introduced to achieve the pulpalanesthesiaofthemaxillaryanteriorteeth,andthesurroundingtissues,byasingleinjectionofcertainanestheticagent[1-9].Thelocalanesthetic,appliedintothelateralpalatalregionatthelevelbetweenthe1stand2ndpremolar,mustdiffuseallthewayfromtheinjectionsitetotheanteriorandmiddlepartofthesuperiordentalplexus,locatedjustabovethemaxillaryteethroots,andtoinhibittherethenociceptiveneurotransmissionalongitsdental(pulpal),andgingivalandosseoustwigs[10-13].
However, therearenoprecisedata incontemporary literaturewhich couldexplain inwhichwayananesthetic canpenetratethe osseous palatine and alveolar processes of the maxilla,

2018Vol.4 No.4:15
2
ARCHIVOS DE MEDICINAISSN 1698-9465
Journal of Orthodontics & Endodontics ISSN 2469-2980
This article is available in: http://orthodontics-endodontics.imedpub.com
especially their cortical bone which virtually does not allow aliquid resorption [13].Theonlypossibility is thatananestheticuses the neurovascular (nutritive) bony canals to reach thementionedpartsofthesuperiordentalplexuswithintheupperportionof thealveolarprocessof themaxilla [3,11,12].Toourknowledge,theanatomicandhistologicalexaminationofthesecanalshasneverbeenperformed.
Accordingly,theaimofourstudywastofindthosecanalsclosetothesiteoftheanestheticinjectionandtheadjacentregion,toexamine in detail their distribution, structure and contents, aswellastoperformcertainmorphometricstudy.
Materials and MethodsThis studyhas twodomains,ananatomic,andahistochemicalandimmunohistochemicalexamination.
Anatomic observation Weexamined48drymaxillaefromthecollectionoftheInstituteof Anatomy, Faculty ofMedicine in Belgrade, with permissionof the Institute authorities. In those specimens, the osseousporesandforaminawereinspectedatthe levelofthe incisors,thecanines,andthe1stand2ndpremolarsbyusingmagnifyingglasses (×2and×4).Theywereexaminedfromthe levelof thegreater palatine groove toward the sockets of thementionedmaxillaryanteriorteeth.Thelocationandnumberofthesebonyopeningsweredetermined.Thelargestforaminaweremeasuredby using a digital caliper (Mitutoyo, Kawasaki, Japan). Theminimum,maximumandmeanvalueswerecounted.
Histochemical processing and stainingSix specimens of themaxillary region,which included palatineprocess, alveolar process, palatal mucosa and submucosa,alveolarmucosaandgingiva,weretakenduringroutineautopsyfrom3malesand3femalesagedbetween54and68years(mean,59years).ThiswasapprovedbytheauthoritiesoftheInstituteof Pathology, Faculty ofMedicine in Belgrade, and the EthicalCommitteeoftheClinicalCenterofSerbiainBelgrade.Wewereallowedtouseonlytheunendentousportionsofthemaxillaandsurroundingtissues.Eachspecimenwascutoutfromthemaxillaby means of a dentist electric drill. Two transverse (coronal)incisionsintheoralcavityweremadeanteriorandposteriortothe1stand2ndpremolars,tothelevelofthemiddlepartofthealveolarprocess,i.e.justlateraltoitspalataine(lingual)corticalplate.Then,asagittalsectionwasplacedthroughthemedialpartofthehardpalate,andanotheronethroughthealveolarprocess.Eachcutoffspecimenmeasured11×19mmonaverage.
Tissue samples were fixed in buffered 10% formaldehydesolution (pH 7.5) for 48 h, decalcified in a solution ofethylenediaminetetraacetic acid disodium salt -EDTA [5.5 g,distilledwater90ml,and10mLformaldehyde(37/40%stock)]for3weeks,andfinallyroutinelyprocessedtotheparaffinblocks.Thesampleswerepreparedfortheopticmicroscopyaccordingtothepreviouslydescribedprotocol[14].Semithinserialsections(6μmthick)werecutonarotatoryLeicaRM2255microtome(LeicaMicro-Systems, Reuil-Malmaison, France), and then adhered
to “Super frost” microscopic slides (Menzel-Glaser, Germany).Tissuesectionswerestainedwithhematoxylinandeosin(H&E)andAzantrichromestain(BioOptica,Code04-001802).
Microscopic and morphometric analyses were performed onOlympus BX-41 light microscope, and microphotographs weretaken with Olympus XC50 digital camera, using the Cell SensEntrysoftware(Olympus,Tokyo,Japan).
Immunohistochemical stainingThe immunohistochemical (IHC) method was used for theidentification of collagen type I and laminin antigens, whichwere prepared according to a standard technique [15]. Aftertissue deparaffinization and rehydration, antigen retrieval wasperformed by incubating the tissue sections in 0.01M citratebuffer(pH6.0)inamicrowaveovenfor20minutes.Endogenousperoxidase activity was blocked with 0.3% hydrogen peroxideinmethanol for 10minutes at room temperature. Thereafter,tissue sections were incubated with anti-collagen I (ab34710,Abcam;diluted1:100withDakoantibodydiluent,CodeS0809)or anti-laminin (ab11575, Abcam; diluted 1:400 with Dakoantibodydiluent,CodeS0809)antibodies.Theincubationofthetissuesampleswithprimaryantibodieswasperformedovernightat 4°C. The sections were subsequently treated by applyingthe commercial UltraVision/DAB staining kit (ThermoScientificLabVision TL-060-HD). Antigen-antibody complexes werevisualizedwith3,3’-diamino-benzidine(DAB)substratesolution.The sections were counterstained with Mayer's hematoxylin.Negativecontrolswereperformedontissuesectionsusing thesamemethodology,butwiththeomissionofprimaryantibody.
ResultsThe anatomic examination was first performed, and then thehistochemicalandtheIHCanalysisofthepost-mortemspecimensofthelateralmaxillaryregion.
Anatomic examinationThe anatomic study was undertaken in the lateral palatineregion,i.e.justlateraltothegreaterpalatinegroove,aswellasinthemesialportionofthealveolarprocess(Figure 1).Bothareaswerelocatedattheleveloftheanteriorteeth,thatis,thecentralandlateral incisors,andthecanine,aswellasthe1thand2ndpremolars,wheretheanestheticiscommonlyappliedindentalpractice.
The examination revealed 1102 total number of the bonyopenings in 48drymaxillae. Theywerepresented at the levelofthecorrespondingteeth,wheretheyrangedfrom1to10innumber (Table 1).Mostof theobservedopeningswere small,less than 1 mm in diameter. In two cases, however, a largerforamenwasobservedwhichmeasured1.7mmand2.3mminsize,respectively(Figure 1).Someoftheopeningsweremoreorlessdistantamongthemselves,whilstsomeothersweregroupedatthelevelofcertainteeth(Figure 1).
General histological remarks The 827 obtained slices of the lateral palate and the superior

2018Vol.4 No.4:15
ARCHIVOS DE MEDICINAISSN 1698-9465
3© Under License of Creative Commons Attribution 3.0 License
Journal of Orthodontics & Endodontics ISSN 2469-2980
partofthealveolarprocess,withsurroundingsofttissues(Figure 2), were carefully analyzed. The examination first comprisedthe mucous membrane and gingiva, including the epitheliumandthepalatalsubmucouslayer,aswellastheperiosteum,thebonytissue,andtheneurovascularcanalsandtheosseouspores(Figures 2 and 3).
The alveolar gingiva was covered with a stratified squamousepithelium,which is either fullyorpartially keratinized (Figure 3).Theepitheliumrangedbetween408.03µmand443.35µm(mean,430.02µm)inthickness.Thesubepitheliallayerwasmadeupofadenseirregularconnectivetissue,withalargenumberofthecollagenfiberbundles.Theentiregingivavariedinthicknessfrom1,593.18µmto1,799.62µm,withameanvalueof1,712.85µm(i.e.about1.7mm).
Thealveolarboneshowedasuperficialcortical(compact) layercomposedofafewparallellamellae.Itsdeeperandmuchlargerpartwasmadeupofthespongybonewithcertainspiculesandbranchingtrabeculaebuiltbysomeirregularlamellae(Figure 3). Theintertrabecularspacescontainedfatcells,smallnumberof
collagenfibers,asmallamountoftheredbonemarrow,andtinybloodvesselsandnervessporadically.
Thepalatalmucosa (Figure 4)was also coveredby a stratifiedsquamous epithelium, which was either ortokeratinized orparakeratinized.Itrangedinthicknessfrom536.13µmto612.75µm(592.26µmonaverage).Thethicknessoftheentiremucousmembrane,includingboththeepitheliumandthesubepitheliallayer, varied between 2,267.55 µm to 3,148.24 µm (mean,2,875.26µm, i.e.about2.87mm).Thesubepithelial layer,thatis, the lamina propria, contained densely packed bundles ofcollagenfibers(Figure 4).
Inferior aspect of the bony palate and the right andleftalveolarprocesses.Notemolarteeth(1),premolarteeth (2), canine tooth (3), lateral and central incisors(4),incisivefossa(5),medianpalatinesuture(6),socketforthe2nd premolar (7), transversepalatalsuture(8),greater palatine foramen (9), horizontal plate of thepalatine bone (10), palatine process of the maxilla(11),lesserpalatineforamen(12),andgreaterpalatinegroove(13).Alsonotea largerpalatal foramen(largerarrow),severalsmallforamina(smallerarrows),andanopening(arrowhead)closetotheincisivefossaandthecentralincisor.
Figure 1
Level of location Number: range (mean)Centralincisor 1-10(6.3)Lateralincisor 1-9(5.2)
Canine 1-9(3.7)Firstpremolar 1-7(3.8)
Secondpremolar 1-7(3.9)
Table 1 Thelocationandnumberoftheneurovascularopenings.
Transverse (coronal) section of the left lateral palatalregion (1) and the upper part of the alveolarmucousmembrane (4), submucous layer with minor salivaryglands,arteriesandnerves(5),andspongiousbone(6).Alsonotethenasalmucosaabovethemedialpartofthepalatineprocess.(×2,Azantrichromestaining).
Figure 2
Transverse section of the gingiva (1) and themucosa(2)ofthealveolarprocesswithitsspongiousbone(3).Notegingivalepithelium(4),epitheliumofthealveolarmucosa (5), and small pores of the alveolar bone(arrows).(×4,H&Estaining).
Figure 3

2018Vol.4 No.4:15
4
ARCHIVOS DE MEDICINAISSN 1698-9465
Journal of Orthodontics & Endodontics ISSN 2469-2980
This article is available in: http://orthodontics-endodontics.imedpub.com
Thesubmucouslayercontainedcollagenfibersaswell,butalsothefattissue,salivaryglands(Figure 2),bloodvessels,andnerves(Figure 4).Thecollagenfiberswerepresentthroughoutthislayerinasmalleror largeramount.Thesmalleror largercollectionsofthefatcells(adipocytes)wererandomlyarrangedwithinthesubmucouslayeramongthecollagenfiberbundles,andaroundthebloodvesselsandnerves(Figure 4).Theyshowedatypicalappearance:roundorpolygonalinshape,withalucentcytoplasmandsmall,darkandelongatednucleusattheperiphery.
Theminor salivary glandswere presentwithin the submucouslayeratthelevelofthe1stand2ndpremolars(Figure 2).Theirmaincellscontainedsmallsecretorygranulesandadarknucleuslocatedintheirbasalpart.Thecone-shapedandtightlypackedcellswereorientedtowardthecentralpartofeachacinus.
The blood vesselswere abundantwithin the submucous layer(Figure 4).Thearteriesweremoreoftenseenthantheveins,andthey represented the branches of the greater palatine artery.Theirwallconsistedoftheintima,media,andadventitialcoats,withaclearlyvisibleinternalelasticlamina.
Thenervesof smalleror larger sizewereobservedamong thecollagenbundlesandoftenclosetothebloodvessels(Figure 4). They contained densely packed axons with the Schwann cellssurroundedby theperineurium.All of themwerebranches ofthegreaterpalatinenerve.
The palatine process showed the periosteum, and the cortical
andspongybone(Figure 5).Theperiosteumpresentedasathinconnectivelayercoveringthesurfaceofthepalatineprocess.Itcontaineddenselypackedcollagenbundleswitharelativelylargenumber of the smaller blood vessels (Figure 4). The periosteumrangedinthicknessfrom87.59µmto121.67µm(mean,106.69µm).
The cortical bone comprised the most superficial layer of thepalatineprocess,towhichtheperiosteumwasattached(Figures 4 and 5).Itconsistedofonlyafewparallelosseouslamellae(Figure 5). Just above that thin layer, the osteons were located closeto each other (Figure 5). Theywere formed by the concentriclamellae, ranging in number from 4 to 12 (7.14 on average).The lamellae contained the osteocytes embeddedwithin theirlacunae. A Haversian canal was present in the center of eachosteon(Figure 5).Theosteonsvariedinsizebetween311.02µmto869.16µm(mean,667.80µm).TheHaversiancanalsrangedindiameterfrom114.23µmto347.82µm(231.23µmonaverage).Theymainlycontainedsmallbloodvesselsandtinynerves.Afterdecalcification, the concentric lamellae of Haversian osteonsmoderatelyexpressedcollagentypeI.
Neurovascular canals Weexaminedfirstsomesmallopeningsofthecorticalboneofthealveolarandpalatineprocesses,andthentrueosseouscanalsinhistologicalslices.
Theuppermesialpartofthealveolarprocessofeachhistologicalspecimen containedbetween3 and6 pores (mean, 4.2). Theywereisolatedorgrouped,inthelattercasecomprisingsometimes3or4oftheminamicroscopicfield(Figure 3).Someofthepores
Palatal epithelium (1) and the subepithelial collagenfibers (2). Note fat cells (3), cortical bone of thepalatine process (4), the submucous palatal arteries(larger arrows) and nerves (smaller arrows). Alsonoteameasuringbar in the leftbottomcorner. (Azantrichromestaining).
Figure 4
Transverse section of the osteons with the Haversiancanals(1),aswellastheperiosteum(2).(Azantrichromestaining).
Figure 5

2018Vol.4 No.4:15
ARCHIVOS DE MEDICINAISSN 1698-9465
5© Under License of Creative Commons Attribution 3.0 License
Journal of Orthodontics & Endodontics ISSN 2469-2980
were closed, i.e. they were like small depressions within theouterpartofthecorticalbone.Theremainingpores,however,wereopen,thatis,theycontinuedthroughthewholethicknessof the compact bone, and ended soon in the intertrabecularspacesofthespongybone(Figure 6).Theporescontainedsmallarteriesand/ortinynervesaccompaniedbyjustafewcollagenfibersor,quitetheopposite,byalargernumberofthecollagenbundles (Figure 6). As regards the typical, long neurovascularcanals,theywerevirtuallynotobservedintheupperpartofthealveolarprocess.
Ontheotherhand,theporeswererarelyseenwithinthelateralpart of the palatine process, usually 1 or 2 per a specimen.However,thetypicalneurovascularcanalswerepresentinallthecases(Figure 7).Theyrangedinnumberfrom3to6(mean,3.8)atthelevelofthe1stand2ndpremolars.Thecanalsweremostoften obliquely oriented (Figure 7). After passing through thecortical bone, some of them continued through the spongiosaof the palatine process close to the alveolar process, wherethey sometimes had a slightly tortuous course (Figure 8). In somecases,themaincanalgaverisetooneortwosmallersidebranches when entering the cortical bone. In other instances,each canal divided into 2 or 3 terminal branches (secondarycanals)withinthecompactorthespongybone.
The openings of the neurovascular canals ranged in size from90.28µm to1,230.62µm (mean,893.62µm). The initialpartsofthecanalsvariedindiameterbetween523.42µmand903.04µm(622.93µmonaverage).Eachcanal containeda fewsmall
arteries,oronelargerandseveralsmallerarteries,andtheveinsoccasionally.Largerarterieswithincanalsweredividedsoonintosmallerarteries,someofwhichenteredasecondarycanal.Thenerves represented the twigsof the larger submucosalnerves.Thereweresporadicallysmallclustersofthefatcellswithinthecanals,aswellascertainamountofcollagenfibers(Figures 7 and 8).
In order to determine the expression of main type of thecollagen, that is, collagen type I, in the bone and surroundingsofttissues,aswellaswhether thosefibersarepresent in the
A typical neurovascular canal (1) within the palatineprocess (2).Noteperiosteum(3),andbranchesof thegreaterpalatineartery(4).(Azantrichromestaining).
Figure 7
Aneurovascularcanal(1)withanobliquesinusoidcoursethroughthepalatineprocess.Notethespongiousbone(2) and the submucous layer (3). (×4, Azan trichromestaining).
Figure 8
Two pores (1 and 2) of the alveolar process, whichcontain collagen fibers and small vessels. Note thelamina propria of the gingiva (3). (Azan trichromestaining).
Figure 6

2018Vol.4 No.4:15
ARCHIVOS DE MEDICINAISSN 1698-9465
6© Under License of Creative Commons Attribution 3.0 License
Journal of Orthodontics & Endodontics ISSN 2469-2980
accompanyinggreaterpalatinearterycourseslateraltothenerve[18-20]. Its branches supply thewholehardpalate, themesialpartofthealveolarprocessand,afterenteringthenasopalatineforamen,the inferiorandanteriorpartofthenasalseptum,aswellastheanteriorportionoftheinferiornasalmeatus[11].
Weexaminedthebonyopeningsbetweenthegreaterpalatinegrooveandthemesialpartof thealveolarprocessat the levelof theanteriormaxillaryteeth (Figure 1).Therearenoreportsin literature regarding the number, size and arrangement oftheopenings.OnlyBerkovitz[11]mentionedthat“Thepalatineprocessdisplaysnumerousvascularforamina…”
Thebonyopeningsobservedinourspecimens(Figure 1)transmitthe twigs of thementioned greater palatine nerve and artery(Figures 6-10).Inaddition,weobservedinsomeofourspecimensone or several openings between the nasopalatine fossa andthecentral incisor(Figure 1),whichobviouslytransmitscertainnasopalatinenervetwigs.This is inagreementwiththefindingthatthenasopalatinenervemayassistintheinnervationofthecentral incisor,whichexplainsafailure intheanteriorsuperioralveolarnerveblock in somepatientsat this level [11,21],andwhichissimilartoadoubleinnervationofthemandibularincisors[11,21,22].
Immunohistochemical reaction against collagen typeI.Notealargeamountofcollagenfibers(1)toenteraneurovascularcanal(2)andtosurroundasmallartery(3),aswellascompactbone(4)ofthepalatineprocesswithcollagenexpressionaroundtheosteocyteswithindecalcifiedbonematrix.(IHCstainingforcollagentypeI).
Figure 9
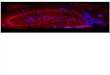
neurovascular canals, we performed the IHC examination forcollagentypeI.TheIHCreactionwasmoderateinthedecalcifiedbonematrix,andverystronginthemucosallaminapropriaandthe submucous layer, the periosteum, and the neurovascularcanalsthemselves(Figure 9).WealsousedtheIHCforlaminininourspecimens,primarilyforabettervisualizationofconnectivetissueinvestmentsofthenerves,andthusthenervesthemselves,passingalongtheneurovascularcanal(Figure 10).ThestrongestlamininIHCreactionwasobservedinthearterialwalls,especiallywithintheadventitialand,partially,themediacoat,aswellasintheconnectivetissueinvestmentsofthenerves(Figure 10).
The anatomic results will be considered first, and then thehistologicalandIHCfindings,aswellastheclinicalsignificanceoftheobtainedfacts.
DiscussionAnatomic aspectAnanestheticisappliedatthelevelofthe1stand2ndpremolars,closetothegreaterpalatinegroovewhichcontainsthenerveandthearteryofthesamename,thebranchesofwhichruntowardthemaxillaryanterior teeth [1,3,8].Thegreaterpalatinenervesupplies about three quarters of the hard palate [16,17]. The
Immunohistochemical reaction against laminin. Aneurovascularcanal(1)withitscontentsdividesintotwosmallercanals(2).Noteastrongreactioninthearterialwalls(3)andintheconnectivetissueinvestmentsofthenerves(4).(IHCstainingforlaminin).
Figure 10

2018Vol.4 No.4:15
7
ARCHIVOS DE MEDICINAISSN 1698-9465
Journal of Orthodontics & Endodontics ISSN 2469-2980
This article is available in: http://orthodontics-endodontics.imedpub.com
Asregards thebonyopenings themselves, theywereobservedat the level of each maxillary anterior tooth (Table 1). Theyweremostnumerousclosetothecentralandlateralincisors.Inadditiontothesesmallopenings,wenoticedintwospecimensalargeforamenandacanalatthelevelofthe1stpremolar(Figure 1).Itseemstobesimilartothevariableretromolarforameninthe mandible [23-25], which transmits certain neurovascularelementsforanadditionalsupplyofthemandibular3rdmolar.Suchopeningsandcanalsinourspecimensmostlikelyconducttheneurovascularcomponentsaswell.
Histological aspectThemasticatorymucosa comprises the gingiva, aswell as themucousmembraneofthehardpalateandtheupperpartofthealveolarprocess(Figures 3 and 4)[26,27].
The gingiva consists of the squamous ortokeratinized orparakeratinized epithelium and lamina propria, whilst thesubmucous layer doesnot exist (Figure 3). The laminapropriacontains a dense irregular connectivetissue (Figures 3 and 6),i.e.a largenumberof thecollagen Ifiberbundles [11,26].Ourexaminationshowedthattheepitheliallininghadameanvalueof 0.43 mm in thickness, whilst the whole mucosa measuredabout1.7mmonaverage.Someclinicianstakefromthissiteafreegingival graftandapply it arounddental implants [19,28].Theregionofthealveolarprocessabovethegingivaiscoveredwithamucousmembrane(Figure 3).
The palatal mucosa contains the epithelium, lamina propria,and submucous layer [26,29-32]. The whole palatal mucosa(Figure 4)inourspecimensaveraged2.87mminthicknessatthelevelofthepremolars.Otherauthorsobtainedsimilarorlargervalues,i.e.2.25-3.55mm[18,19,31,33,34].Thedifferencesweredue to various sites of measurement, the age of individuals,and the applied techniques: a direct probe, ultrasonic device,computerized tomography (CT), cone-beam CT (CBCT), orhistologicalmethods[27,31-35].
Thepalatalepithelium(Figure 4)isalsoasquamousortokeratinizedorparakeratinizedlining,withanaveragedthicknessof0.59mminthelateralpartofourspecimens.Accordingtootherauthors,theepitheliumvaried in thicknessbetween0.31mmand0.38mm[29].Somediscrepanciesaremostlikelyduetodifferentageofpatientsandvariouspalatalsitesofmeasurement.
Thementionedlaminapropria(Figure 4)consistsofthepapillaryand reticular layers [26,29,31]. The papillary layer, connectedwith the epithelium, comprises high columns (Figure 4) whichcontainnumerouscapillaryloops.Thereticularlayerconsistsofthickbundlesofcollagenfibers.Yuetal.[31]foundoutthatthethicknessofboththeepitheliumandthelaminapropriawas1.28mmonaverage.Ontheotherhand,Choetal.[29]obtainedtheaveragethicknessofthelaminapropriaitselfof1.08mmatthelevelofthe1stpremolar.
Sincethelaminapropriacontainsdensecollagenbundlesandalotofbloodvessels,itisoftenusedasadonorsiteforautogenous
subepithelial connective tissue grafts in periodontal therapy,thatis,foratoothrootcoverageaftersofttissuerecession,forthetreatmentofsomemucogingivaldefects,orforapplicationaround dental implants [31,36-40] Some of the mentionedauthors histologically confirmed the benefit of such a grafting[37,38].
As noticed in our study and other reports [26,29,31], thesubmucouslayerofthepalatalmucosacontainsclustersofthefatcells,i.e.adipocytes(Figure 4),minorpalatalsalivaryglands(Figure 2),bundlesofcollagenfibers,bloodvessels,andnerves(Figures 4 and 7).Becauseofsuchacomposition,thislayerisnotsuitableforgraftinginperiodontalsurgery[32].
Theperiosteumisathinconnectiveandvascularlayercoveringthe surfaceof the corticalboneof thepalateand thealveolarprocess(Figures 4, 5 and 7).Itwasconnectedtotheunderlyingcortical bone by small bundles of the collagen fibers. Theperiosteumingeneralcontainsanouterlayerofdensecollagenbundles,andaninnerlayeroftheosteoprogenitorcells[26].Wefounda largernumberofbloodvesselswithintheperiosteum,someofwhichenteredthecorticalboneviatheneurovascularcanals.
The periosteum grafts can also be used in oral surgery, forexample in the cleftpalate repair [41]. Suchgrafts,due to thepresence of the mentioned osteoprogenitor cells, can inducethe palatal or alveolar bone regeneration, but also the socketpreservationaroundthedentalimplants[41-43].
As regards the bone structure of the palatine and alveolarprocesses, it has alreadybeendescribedby certain authors tosome extent, butwithout anymeasurement data [11,26]. Themedial part of the palatine process is mainly formed by thecompactbonytissuewiththeHaversianosteons(Figure 2).Thesurfaceofthealveolarprocessisbuiltbytwocorticalplates,thelingual(orpalatine)andthebuccal(orfacial)one.However,mostofthealveolarprocess,aswellasthelateralpartofthepalatineprocess, contained a typical spongy bonewith trabeculae andtheintertrabecularspacesfilledwithfatcells,redbonemarrowsporadically,andbloodvesselsandnerves.
Neurovascular canalsInspiteofusingseveralkeywordsinvariouscombinations,wecouldnotfind inPubMedanyarticleon thehistologyof thesecanalswithinthepalatineoralveolarprocesses.Thereareonlyseveral articles regarding the canals for the superior alveolarnervesandvessels,includingthecanalissinuosus,butonlywithinthewallsofthemaxillarysinus.Theywereexaminedanatomicalyandradiologicaly,andnoneofthemhistologically[44-47].Afewotherarticlesweredevotedtothevascularalveolarcanalsofthemandible,includingthementionedvariableretromolarforamenand canal,whichwere examined by CT, CBCT, or bymagneticresonanceimaging(MRI)[23-25].
The poreswe found in the alveolar process of themaxilla areactuallysmallneurovascularcanalswhichwere,however,muchshorter than thosewithin the palatineprocesses. They usually

2018Vol.4 No.4:15
ARCHIVOS DE MEDICINAISSN 1698-9465
8© Under License of Creative Commons Attribution 3.0 License
Journal of Orthodontics & Endodontics ISSN 2469-2980
contained a larger number of small arteries, tiny nerves andcollagenbundles.Theypenetratedthecorticalbone,enteredthespongy bone, and coursedmost likely toward the sockets (i.e.dentalalveoli)ofthemaxillarypremolars,canineandincisors.
From1 to 7 of the neurovascular canalswere revealedwithinthepalatineprocessat the levelof the1stand2ndpremolarsin our specimens. They usually contained a few small arteries(or one larger and several smaller ones), veins occasionally,tinynerves, certainamountof collagenfibers, andoften smallclusters of the fat cells. Each canal in serial sections startedfirst as a small depression of the cortical bone, filled with acontents,likeadepressionoftheperiosteumandcorticalbone.In thesubsequent sections,eachcanalwasseen tobe formedgradually.Itpassedfirstthroughthecortical(compact)bone,andthenobliquelythroughthespongyboneofthelateralpartofthepalatine process (Figures 7 and 8). The palatal trabeculae andtheintertrabecularspacescommunicatedwiththespongyboneofthesuperiorpartofthealveolarprocess(Figure 2).Someofthecanalslocatedmedially,i.e.towardthepalatalraphe,passedonlythroughthethickcorticalboneandobviouslysuppliedonlythecompactpartofthepalatineprocessinthatarea.
Thenutrientcanalscontainedcertainvascularandneuraltwigswhich mainly originate from the greater palatine artery andnerve,andsporadicallyfromthenasopalatinenerve[11,16,21].Theyalsohousea smallnumberof theadipocytesandcertainamountofcollagenfiberstypeI.Toourknowledge,theimmunereactionagainstthecollagenIhasneverbeenperformedinthisregion.Itwasasimilarcasewiththelaminin,whichisoneofthecomponents of the extracellular matrix and the basal lamina,alongwithfibronectin,collagenIII,andotherelements[15,26].Thestrongestreactionwasobservedinthearterialwallsandtheconnectiveinvestmentofthenerves.
As regards thenerves themselves,Russeletal. [48] confirmedthepresenceofthecalcitoningen-relatedpeptideaxons,i.e.theCGRP-positivenervefibers,withinsomesuperioralveolarnerves.Thesefibersareinvovledinnociception,butalsoinregulationoftheadjacentbloodvessels[48].
Asalreadymentioned,certainlocalanesthetic(usuallyLidocaine,Mepivacaine,orArticaine)duringtheAMSAanesthesiaisinjectedintothelateralpalate,thatis,closetothe1stand2ndpremolars[1-4,6-10,13].
Theanteriorandmiddle superioralveolarnerves,whose twigsareblockedbytheAMSAanesthesia,arisefromtheinfraorbitalnerve [17,49-51]. The former originateswithin the infraorbitalcanal and continues inferiorly along the canalis sinuosus andacross the anterior wall of the maxillary sinus. It participatesin formationoftheanteriorpartof thesuperiordentalplexus,and innervates the incisors and canine teeth, as well as thesurroundingtissues [49]. Its nasal branch supplies thewalls oftheinferiornasalcavity[17].
The middle superior alveolar nerve, which can be singular,duplicated, triplicated or absent, arise from the infraorbitalnerveinitsgroove,andcoursesinferiorlyandanteriorlyacross
thelateralwallofthemaxillarysinus[17].Itsterminalbranches,whichassistinformationofthementioneddentalplexus,mainlyinnervate thepremolar teeth,and sometimes themesiobuccalrootofthe1stmolar[9,49].
As regards the greater palatine nerve [16,17], it leaves theforamen of the same name and continues, together with thegreaterpalatinearteryandvein,alongthecorrespondinggrooveinthelateralpalatalregion(Figure 1).Thebranchesofthenervesupplythestructuresoftheposteriorthreequartersofthehardpalate,includingthepalatineprocess,butalsothemesialpartofthealveolarprocess[17].Therestofthehardpalateisinnervatedbythetwigsofthenasopalatinenerve.Sincetheinjectionoftheanestheticisveryclosetothegreaterpalatinegroove,greatcareshouldbetakenduringtheproceduretoavoidadamagetothegreaterpalatinearteryandnerve.
Theanestheticisinjected,inanamountoflessthan2mL,intothepalatinemucosa[9].Diffusionabilitydepends,amongothers,onchemicalstructureofananestheticandthestructureoftheinvolved tissue [13]. The injected anesthetic easely diffusesamongthecollagenbundlesofthepalatalmucosa(Figures 4 and 7).Itcanalsoeaselypenetratethemembranesandbodiesofthepresent cells, sincemost of the applied anesthetics are highlyliposolublesubstances[13].
An anesthetic passes then through the periosteum and alongthelooseconnectivetissuewithintheneurovascular(nutritive)canalsofthepalatineprocess,andthencontinuesthroughthespongybone in its lateralpart (Figures 2 and 8). Similarly, theanestheticalsodiffuseseasilythroughtheporesofthealveolarbone(Figures 3 and 6).Inthisway,theanestheticblocksfirstthepalatalandalveolarbranchesofthegreaterpalatinenerve,andthenreachesthesuperiordentalplexuswhere ithasthesameeffect.
ConclusionThe neurovascular canals with small blood vessels, nerves,collagenfibers,andadipocytesarepresentinboththealveolarandpalatineprocessesofthemaxilla.Theymostlikelyrepresentthehistologicalbasisfordiffusionofa localanesthetic injectedintothelateralpalatineregion.
DeclarationsEthicsapprovalandconsenttoparticipate.
This study was performed in accordance with the Declarationof Helsinki and carried out with the approval of The EthicsCommitteeoftheClinicalCenterofSerbia.
Availability of Data and MaterialsThedatasetsusedand/oranalyzedduringthecurrentstudyareavailablefromthecorrespondingauthorsonreasonablerequest.
Authors’ ContributionsTherolesoftheauthorswere:DĆ,VT,andSMcontributedtothe

2018Vol.4 No.4:15
9
ARCHIVOS DE MEDICINAISSN 1698-9465
Journal of Orthodontics & Endodontics ISSN 2469-2980
This article is available in: http://orthodontics-endodontics.imedpub.com
References1 Acharya AB, Banakar C, Rodrigues SV, Nagpal S, Bhadbhade S, et
al. (2010)Anteriormiddlesuperioralveolar injectioniseffectiveinprovidinganesthesiaextendingtothelaststandingmolarinmaxillaryperiodontalsurgery.JPeriodontol81:1174-1179.
2 CorbettIP,JaberAA,WhitworthJM,MeechanJG(2010)Acomparisonoftheanteriormiddlesuperioralveolarnerveblockandinfraorbitalnerve block for anesthesia ofmaxillary anterior teeth. J AmDentAssoc141:1442-1448.
3 FriedmanM,HochmanM(1998)TheAMSAinjection:Anewconceptfor localanesthesiaofmaxillaryteethusingacomputer-controlledinjectionsystem. QuintessenceInt29:297-303.
4 FriedmanMJ, HochmanMN (2001)UsingAMSA and P-ASAnerveblocksforestheticrestorativedentistry.GenDent49:506-511.
5 Fukayama H, Yoshikawa F, Kohase H, Umino M, Suzuki N (2003)Efficacyofanteriorandmiddlesuperioralveolar(AMSA)anesthesiausinganewinjectionsystem:theWand.QuintessenceInt34:537-541.
6 Lee S, Reader A, Nusstein J, BeckM,Weaver J (2004) Anestheticefficacyof theanteriormiddle superior alveolar (AMSA) injection.AnesthProg51:80-89.
7 Shirmohammadi A, Faramarzi M, Lafzi A, Kashefimehr A, MalekS (2012) Comparisonof pain intensity of anteriormiddle superioralveolarinjectionwithinfiltrationanesthetictechniqueinmaxillaryperiodontalsurgery.JPeriodonImplantSci42:45-49.
8 ShokranehA, FarhadiN, SaatchiM,NavaeiH, YaghmaeiM (2016)Effect of three different injection sites on the success of anteriormiddle superior alveolar nerve block with 3% mepivacaine: Arandomizedcontrolledtrial.JContempDentPract17:130-135.
9 TolentinoLS,BarbisanSouzaAB,GirardiAA,RomitoGA,AraújoMG(2015) The anesthetic effect of anterior middle superior alveolartechnique(AMSA).AnesthProg62:153-158.
10 WaldmanSD(2002)Theroleofneuralblockadeinmanagementofcommonpainsyndromes.In:Painmanagement:apracticalguideforclinicians(WeinerRS6thEdn).BocaRaton,CRCPress,pp:449-474.
11 BerkovitzBKB(2016)Oralcavity.In:(StandringSEds)Gray’sanatomy.Theanatomicalbasisofclinicalpractice(41stEdn).London,ElsevierLimited,pp:507-533.
12 FehrenbachMJ,HerringSW(2009)Anatomyoftheheadandneck(3rdEdn).SaintLouis,SaundersElsevier.
13 Katzung BG, White PF (2009) Local anesthetics. In: Katzung BG,Masters SB, Trevor AJ (eds) Basic and clinical pharmacology (11th Edn).NewYork,McGrawHillMedical,Lange,pp:439-450.
14 CollisGM(2008)Bone.In:BancroftJD,GambleM(eds)Theoryandpracticeofhistological techniques (5thEdn).Philadelphia,ChurchillLivingstone,Elsevier,pp:269-301.
15 MillerKD(2008) Immunocytochemical techniques. In:BancroftJD,GambleM(eds)Theoryandpracticeofhistologicaltechniques(5th Edn).Philadelphia,ChurchillLivingstone,Elsevier,pp:421-464.
16 HafeezNS, GanapathyS, SondekoppamR, JohnsonM, MerrifieldP,
et al. (2015)Anatomicalvariationsofthegreaterpalatinenerve inthegreaterpalatinecanal.JCanDentAssoc 81: 14.
17 HolmesS(2016)Faceandscalp.In:StandringS(ed)Gray’sanatomy.Theanatomicalbasisofclinicalpractice(41stEdn).London,ElsevierLimited,pp:475-506.
18 KimDH,WonSY,BaeJH,JungUW,ParkDS,etal.(2014)Topographyofthegreaterpalatinearteryandthepalatalvaultforvarioustypesofperiodontalplasticsurgery.ClinAnat27:578-584.
19 Klosek SK, Rungruang T (2009) Anatomical study of the greaterpalatine artery and related structures of the palatal vault:considerationsforpalateasthesubepithelialconnectivetissuegraftdonorsite.SurgRadiolAnat31:245-250.
20 YuSK,LeeMH,ParkBS,JeonYH,ChungYY,etal.(2014)Topographicalrelationship of the greater palatine artery and the palatal spine.Significanceforperiodontalsurgery.JClinPeriodontol41:908-913.
21 MeyerTN,LemosLL,NascimentoCN,LellisWR(2007)Effectivenessof nasopalatine nerve block for anesthesia of maxillary centralincisors after failure of the anterior superior alveolar nerve blocktechnique.BrazDentJ18:69-73.
22 Pereira-MacielP,Tavares-de-SousaE,Oliveira-SalesMA(2015)Themandibular incisive canal and its anatomical relationships:A conebeamcomputed tomography study.MedOral PatolOral Cir Bucal 20:723-728.
23 Capote TS, Gonçalves Mde A, Campos JÁ (2015)Retromolar canal associated with age, side, sex,bifidmandibularcanal,andaccessorymentalforameninpanoramicradiographsofBrazilians.AnatResInt2015:1-8.
24 Muinelo-Lorenzo J, Suárez-Quintanilla JA, Fernández-Alonso A,Marsillas-RascadoS,Suárez-CunqueiroMM(2014)Descriptivestudyofthebifidmandibularcanalsandretromolarforamina:conebeamCTvspanoramicradiography.DentomaxillofacRadiol43:20140090.
25 Sedlacik J,KutznerD,KhokaleA,SchulzeD,Fiehler J,etal. (2016)Optimized 14 + 1 receive coil array and position system for 3Dhigh-resolution MRI of dental and maxillomandibular structures.DentomaxillofacRadiol45:20150177.
26 Gartner LP, Hiatt JL (2001) Color Textbook of Histology (2nd Edn).Philadelphia, W. B. Saunders Company. An Imprint of ElsevierScience.
27 Yaman D, Aksu S, Dişçi R, Demirel K (2014) Thickness of palatalmucosa and its relationship with different parameters in Turkishsubjects.IntJMedSci11:1009-1014.
28 Bengazi F, Lang NP, CaropreseM, Urbizo Velez J, Favero V, et al.(2015)Dimensionalchanges insofttissuesarounddental implantsfollowingfreegingivalgraftion:anexperimentalstudyindogs.ClinOralImplantsRes26:176-182.
29 ChoKH,YuSK,LeeMH,LeeDS,KimHJ(2013)Histologicalassessmentofthepalatalmucosaandgreaterpalatinearterywithreferencetosubepithelialconnectivetissuegrafting.AnatomyCellBiol46:171-176.
30 ReiserGM,BrunoJF,MaharPE,LarkinLH(1996)Thesubepithelialconnective tissue graft palatal donor site anatomic considerationsforsurgeons.IntJPeriodonticsRestorativeDent16:130-137.
conceptionanddesignofthestudy,analysisandinterpretationofdata.
DĆ,VT,andSMwrotethepaper,VT,HH,MO,andJBcontributed
tothehistologicalexamination,andHH,MO,andJBhavecriticallyreadandeditedthepaper.
Allauthorshavereadandapprovedthefinalmanuscript.

2018Vol.4 No.4:15
ARCHIVOS DE MEDICINAISSN 1698-9465
10© Under License of Creative Commons Attribution 3.0 License
Journal of Orthodontics & Endodontics ISSN 2469-2980
31 Yu SK, Lee BH, Lee MH, Cho KH, Kim DK, et al. (2013)Histomorphometricanalysisof thepalatalmucosaassociatedwithperiodontalplasticsurgeryoncadavers.SurgRadiolAnat35:463-469.
32 Yu SK, LeeMH, Kim CS, Kim DK, Kim HJ (2014) Thickness of thepalatalmasticatorymucosawithreferencetoautogenousgrafting:acadavericandhistologicstudy.IntJPeriodonticsRestorativeDent34:115-121.
33 RameshKSV,SwethaP,KrishnanV,MythiliR,RamaKrishnaA,etal.(2014)Assessmentofthicknessofpalatalmasticatorymucosaandmaximumgraftdimensionsatpalatalvaultassociatedwithageandgender–aclinicalstudy.JClinDiagnRes8:ZC09-ZC13.
34 Wara-aswapati N, Pitiphat W, Chandrahpo N, RattanayatikulC, Karimbux N (2001) Thickness of palatal masticatory mucosaassociatedwithage.JPeriodontol72:1407-1412.
35 SongJE,UmYJ,KimCS,ChoiSH,ChoKS,etal.(2008)Thicknessofposterior palatal masticatory mucosa: the use of computerizedtomography.JPeriodontol79:406-412.
36 UenoD,SekiguchiR,MoritaM,JayawardenaA,ShinpoS,etal.(2014)PalatalmucosalmeasurementsinaJapanesepopulationusingcone-beamcomputedtomography.JEsthetRestorDent26:48-58.
37 Goldstein M, Boyan BD, Cochran DL, Schwartz Z (2001) Humanhistologyofnewattachmentafterrootcoverageusingsubepithelialconnectivetissuegraft.JClinPeriodontol28:657-662.
38 Majzoub Z, Landi L, Grusovin MG, Cordioli G (2001) Histology ofconnectivetissuegraft.Acasereport.JPeriodontol72:1607-1615.
39 Monnet-CortiV,SantiniA,GliseJM,Fouque-DeruelleC,DillierFL,etal. (2006)Connectivetissuegraft for gingival recession treatment:assesmentofthemaximumgraftdimensionsatthepalatalvaultasadonorsite.JPeriodontol77:899-902.
40 Zuhr O, Bäumer D, HürzelerM (2014) The addition of soft tissuereplacement grafts inplasticperiodontaland implant surgery:criticalelementsindesignandexecution.JClinPeriodontol 41:S123-142.
41 Barutca SA, Aksan T, Uscetin I, Sahin D, AkanM (2014) Effects ofpalatinebonedenudationrepairwithperiostealgraftonmaxillary
growth:anexperimentalstudyinrats.JCraniomaxillofacSurg42:e1-7.
42 Kermani H, Tabrizi R (2015) Periosteal transposition flapfor graft coverage and ridge preservation in the aesthetic zone. JCraniofacSurg 26:1967-1968.
43 Mouraret S, VonKaeppler E, BardetC,HunterDJ, ChaussainC, etal.(2014)Thepotentialforverticalboneregenerationviamaxillaryperiostealelevation.JClinPeriodontol41:1170-1177.
44 Apostolakis D, Bissoon AK (2014) Radiographic evaluation of thesuperior alveolar canal: measurements of its diameter and ofits position in relation to the maxillary sinus floor: a cone beamcomputerizedtomographystudy.ClinOralImplRes25:553-559.
45 Jung J, Yim JH, Kwon YD, Al-Nawas B, Kim GT, et al. (2011) Aradiographicstudyof thepositionandprevalenceof themaxillaryarterial endosseous anastomosis using cone beam computedtomography.IntJOralMaxillofacImplants26:1273-1278.
46 Mardinger O, Abba M, Hirshberg A, Schwartz-Arad D (2007)Prevalence, diameter and course of the maxillary intraosseousvascular canal with relation to sinus augmentation procedure: aradiographicstudy.IntJOralMaxillofacSurg36:735-738.
47 Sato I,KawaiT,YoshidaS,MiwaY, ImuraK,etal (2010)Observingthebonycanalstructureofthehumanmaxillarysinus inJapanesecadaversusingconebeamCT.OkajimasFoliaAnatJpn87:123-128.
48 RusselFA,KingR,SmillieSJ,KodjiX,BrainSD(2014)Calcitoningene-related peptide: physiology and pathophysiology. Physiol Rev 94:1099-1142.
49 Yenisey M (2009) Comparison of the pain levels of computercontrolledandconventionalanesthesiatechniquesinprosthodontictreatment.JApplOralSci17:414-420.
50 HeasmanPA(1984)Clinicalanatomyofthesuperioralveolarnerves.BrJOralMaxillofacSurg22:439-447.
51 Somayaji KS, RaoMK (2012) Anatomy and clinical applications ofthe maxillarynerve indentistry:aliteraturereview.DentUpdate 39:727-730.