Embed Size (px)
Citation preview

The Healing of Below-Knee Amputations
A Comparison of Soft and Plaster Dressings
William H. Baker, MD,’ Iowa City, Iowa Robert W. Barnes, MD, Iowa City, Iowa Donald G. Shurr, LPT, Iowa City, Iowa
Plaster dressings for below-knee amputations have been increasingly used by both vascular and ortho- pedic surgeons. These dressings are alleged to pro- mote healing by immobilizing the incision and con- trolling edema of the stump (I]; However, some surgeons who deny that wound healing and rehabil- itation are facilitated still prefer a soft dressing.
Cohen et al [2] obtained eventual healing in 97.3 per cent of thirty-eight below-knee amputations treated with a soft dressing compared with 66.7 per cent of nine amputations treated with a rigid dressing.
To resolve whether plaster or soft dressings fa- vorably influenced healing of below-knee amputa- tion, the present prospective randomized study was initiated. In addition, a subgroup of amputees was evaluated for length of hospitalization and rehabili- tation.
Material and Methods
All patients who were candidates for below-knee am- putation for ischemic indications at the University of Iowa Hospitals and the Iowa City Veterans Administration Hospital were randomly allocated preoperatively into a soft or plaster dressing group. All patients were evaluated and operated on by a vascular service under the supervision of one of the surgeon authors.
Preoperatively, all patients underwent a standard his- tory, physical examination, and routine laboratory evalu- ation. Arteriograms were obtained only if any reconstruc- tive surgery was contemplated. Segmental arterial pres- sures were obtained irregularly. Any patient with warm, noninfected, neurologically intact skin at the proposed
Fran the Division of Tthxaclc and Cardbvascular Surgery. Department of .Sur@sry. University of bwa kk@tals md Veterans Administration Hospital. Iowa City, Iowa.
Rqrlnt requests shwld be addressed to Rob& W. Bemes. M). Divkiar OlThaac(ctUld cardiovascular Strgw. lkrhmralty Hospitals. bwa CHy, bwa 52242.
* Present sddres.9: Department of Sqpry. Loyola Medical Center, Maywood. Illinois 60153.
incision site, and a functional knee joint, underwent below-knee amputation.
Operations were performed under either regional or general anesthesia. A long posterior myocutaneous flap was used exclusively. The tibia was transected 4 to 6 inches distal to the knee joint and the fibula was transected ap- proximately 1 cm proximal to that level. Bleeding was meticulously controlled so that drains were never used. The posterior flap fascia was sutured to the anterior tibial periosteum and fascia with 310 chromic catgut. Myodesis was not performed. The skin was closed with interrupted sutures of wire or nylon.
Patients in the soft dressing group had a bulky, soft dressing held in place with a self-adherent gauze bandage and a compression wrap of elastic bandage. A posterior splint was used to maintain the knee in extension in some patients.
Patients in the rigid dressing group had the dressing applied by a certified prosthetist. The wound was covered with fine mesh silk and surrounded with fluffed lamb’s wool held in place by a snug fitting Lycra@ spandex stocking. With cephalic traction applied to the stocking, relief pads of orthopedic felt were glued to either side of the tibia and over the patella. A graded pressure cast was ap- plied using 4 inch rolls of elastic plaster and covered with regular plaster. A strap was incorporated into the cast and attached to a waist belt to maintain cephalic traction. The plaster around the patella was removed to allow for pat&u motion. A pylon was not added to the plaster dressing at this time.
Postoperatively, the soft dressings were changed as needed by the ward physicians. The plaster dressings were not changed for ten to fourteen days unless clinically in- dicated for possible infection. Sutures usually were re- moved at fourteen to twenty-one days. If the wound was healed at this time, primary healing was said to occur. If the wound was not healed at this time but eventually healed, secondary healing was said to occur. Nonhealing wounds required a higher level of amputation.
At the University Hospitals, all patients were evaluated by the physical therapists either preoperatively or early in
716 l’ho American Journal of Surgery

the postoperative period. The patient was judged to be rehabilitatable (independent with a walking aid) or non- rehabilitatable. Rehabilitatable patients started physical therapy within two to three days of the amputation and were walking on one leg with the aid of a walker at the time of’ discharge from the hospital. After an interval of two to six weeks the patients were readmitted, a pylon was added to the plaster dressing, and gait training was started. Usually patients were discharged home after seven to ten days of gait training.
Results
Fifty-one patients selected for below-knee am- putation between 1973 and 1975 were randomized into a soft dressing (24 patients) or plaster dressing (27 patients) group. The average age of the patients in the plaster dressing group was 65.3 years (range, 43 to 86 years) and in the soft dressing group 63.2 years (range, 41 to 76 years). Thirty-nine patients (21 plaster dressing, 18 soft dressing group) had skin necrosis as an indication for amputation and twelve (6 in each group) had incapacitating ischemic rest pain. Six patients had failure of a minor amputation and thirteen had had unsuccessful vascular recon- struction. Thirty-three patients (16 plaster dressing, 17 soft dressing) (65 per cent) were diabetic. Eleven patients had had previous lumbar sympathectomy. All patients had absent pedal pulses, thirty-four (18 plaster dressing, 16 soft dressing) (67 per cent) did not have a popliteal pulse, and three (all in the plaster dressing group) (6 per cent) had an absent femoral pulse. There were no operative deaths (30 days) in this series.
Healing. Of the fifty-one incisions, thirty-two (62.7 per cent) healed primarily, eleven (21.6 per cent) healed secondarily, and eight (15.7 per cent) failed to heal at the below-knee level but subsequent above-knee incisions healed successfully.
Eighteen of twenty-seven below-knee amputations (66.6 per cent) with plaster dressing healed primarily, five (18.5 per cent) healed secondarily, and four (14.8 per cent) required above-knee amputation. Fourteen of twenty-four below-knee amputations (58.3 per cent) with soft dressing healed primarily, six (25.0 per cent) healed secondarily, and four (16.7 per cent) required above-knee amputation. In all, 85.2 per cent of the bwenty-seven amputations with plaster dressing healed and 83.3 per cent of the twenty-four amputations with soft dressing healed. The differ- ences in the results between the total group, the plaster dressing group, and the soft dressing group are not statistically significant..
Thirty-four of the fifty-one patients did not have a popliteal pulse on physical examination. None-
Below-Knee Amputations
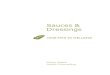
PLASTER DRESSING
SOFT DRESSING
PRIMARY HEALING
*P<o.oI
SECONDARY FAILURE HEALING
Figure 1. Initial hospitalization time after amputation.
theless, the below-knee amputations of twenty-five of these patients (74 per cent) eventually healed. Amputation incision healed in all seventeen of the patients with popliteal pulse and in only one of the three patients with absent femoral pulse.
Twenty-seven of the thirty-three diabetic patients (81.8 per cent) had eventual healing of their below- knee amputation, compared with sixteen of eighteen nondiabetic patients (89 per cent) who had healing (p >0.5).
Length of Hospitalization. Twenty-four patients (13 plaster dressing, 11 soft dressing) at the Univer- sity Hospitals were separately evaluated for length of hospital stay. The twenty-seven patients from the Veterans Administration Hospital were excluded from both this analysis as well as the rehabilitation time analysis because of different patient motiva- tions, discharge and dispo\it ion problems, and physical therapy philosophrc ,_
Six patients had wountl:: I II;I~ Ilc,;llcd primarily in a plaster dressing and stay(bc I i II I II ,,%l)ital an average of 7.3 days after amput.ation (range, 3 to 10 days). (Figure 1.) MO s patients started physical therapy on t post amputation day 1. At one week the plaster dressing was removed, the wound inspected, and the plaster reapplied. Patients were discharged as soon as they were judged to be ambulatory with a walker in the home. One agile patient who lived nearby was discharged prior to wound inspection on post am- putation day 3. One patient with one arm required hospitalization until she was independent with a special walker (35 days) and is excluded from sta- tistical analysis. Three patients had wounds that healed secondarily. They were hospitalized twenty-
vollmw 133, Jum 1977 717

Baker, Barnes, and Shurr
one, twenty-six, and seventy-one days post ampu- tation (average, 39 days). Three patients required above-knee amputations despite protracted efforts to save the knee joint and were hospitalized an av- erage of forty-three days.
The six patients with wounds healing primarily with a soft dressing had an average hospital stay of 14.7 days (p <0.05). The two patients with wounds healing secondarily stayed twenty-two and twenty- eight days, whereas three patients requiring above- knee amputation stayed an average of 35.6 days.
Rehabilitation Time. The time interval between the operation and the beginning of gait training in patients with incisions healing primarily was evalu- ated in the two groups at the University Hospital. Patients with a plaster dressing started gait training 29.6 days post amputation and those with a soft dressing 35.5 days post amputation (p <0.05). Pa- tients with incisions healing secondarily were not evaluated because of additional factors influencing their time of beginning training.
Comments
Despite the advent of successful arterial surgery, certain patients still require amputation to control ischemic pain and gangrene. These patients have a limited life expectancy, and prompt rehabilitation is necessary to restore them to their usual place in society. Amputation should relieve pain and is the initial step toward ambulation with a prosthesis.
Our overall healing rate of 84.3 per cent is not quite as good as the 90 per cent achieved by other series of below-knee amputations covered with a rigid dress- ing [2,3,4]. Neither is it as good as the 97 per cent healing rate achieved by Cohen et al (21 using a soft dressing. This discrepancy in healing rates may be due to either different technics of below-knee am- putation or to different patient selection.
Since the completion of the present study our criteria for below-knee amputation have been al- tered. Patients without a detectable Doppler velocity signal in the popliteal artery are not offered below- knee amputation, but above-knee amputation is done primarily. This is based on a recent report in which below-knee amputations of five of five patients without an audible popliteal artery velocity signal failed to heal [5].
In this series the plaster dressing was applied by a certified prosthetist in an attempt to avoid im- proper casting. Plaster dressings that fit either too loosely or too tightly will lead to an increased mor- bidity. A loosely applied cast will allow for swelling and defeat the purpose of the dressing. When the
edema subsides, the stump will be loose within the plaster and thus be traumatized. A tight cast or an improperly relieved cast will lead to anterior tibia1 or patellar skin necrosis.
It was our initial supposition that the recently improved healing rates of below-knee amputations were not due to dressing technics but to the use of a long posterior myocutaneous flap technic instead of the equal skin flap technic. The posterior flap is al- leged to have a better blood supply, and thus, skin healing is improved. Unfortunately, the posterior skin flap technic was introduced at the same time as the rigid dressing, making the assessment of the relative importance of each technic difficult. The present study shows equal healing rates of below- knee amputations using a long posterior flap re- gardless of the type of dressing used, substantiating that neither dressing is superior.
Interestingly, the plaster dressing significantly shortened the hospitalization time of the amputees. In addition, the rehabilitation of patients with wounds that healed primarily in plaster started sooner. The reason for this is speculative. However, the patients with soft dressings almost uniformly had some stump edema despite wrapping with an elastic bandage. The physician therefore did not discharge the patient until he was reasonably sure that the wound would heal. The persistence of this edema postponed the beginning of gait training.
For these reasons, we now customarily use a plaster dressing.
Summary
To evaluate the effect of wound dressing upon wound healing, fifty-one patients undergoing below-knee amputation using a long posterior myo- cutaneous flap technic were randomly allocated into a soft or plaster dressing group. Neither wound dressing technic proved superior, as wounds healed in 85.2 per cent of the plaster dressing group and 83.3 per cent of the soft dressing group.
References
1. hhre w: Below-knee amputatkxl for vascular insufficiency. Bull FrosthetRes 10-12: 15,1969.
2. c&en SI, wdman ID, Salzman EW, w4iw DJ: Tha delete&us effect of immediate postoperative prosthesis in below-knee amputations for ischemic disease. Surgery 76: 992, 1974.
3. Condon RE. John FN: Immediate postoperative prosthesis in vascular amputation. Ann Surg 170: 435. 1969.
4. Burgess EM. Romano RL. Zettl JH, S&rock RD Jr: Amputation of the leg for peripheral vascular insufficiency. J Bone Joint slug53: 874.1971.
5. Barnes RW, Shanik GD. Slaymaker EE: An index in tteallng of below knee amputation: leg blood pressure by Doppler ul- trasound. Surgety79: 13, 1976.
718 lha Amarlcan Jcurnal cl Sugary