Embed Size (px)
DESCRIPTION
The GOUT C. T. Allred, M.D. 2/4/10. Clinical Syndromes. Acute gouty arthritis – the first episode. Usually preceded by hyperuricemia for years First MTP joint (podagra - 50%), other foot joint, ankle or knee in 30% of first time cases. - PowerPoint PPT Presentation
Citation preview

The GOUTC. T. Allred, M.D.
2/4/10

Clinical Syndromes
• Acute gouty arthritis – the first episode.– Usually preceded by hyperuricemia for years– First MTP joint (podagra - 50%), other foot
joint, ankle or knee in 30% of first time cases.– Usually monoarticular (80%) with first case.
Can be polyarticular in recurrent cases.– First episode is frequently excruciating
building up over several hours, to the point a person cannot stand to have a sheet touching.

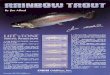
Acute gout
• The redness is sometimes shiny, sometimes dull.
• Warm. • Very tender to touch.

Acute gout
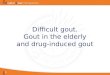
• Other common areas of affliction.

Acute gout

Acute gout


Gout risk factors
• “Classic” – an obese,hypertensive man, age 30 to 50, frequent imbiber of alcohol (especially beer)

Gout risk factors• Women = men over age
65.• Trauma to joint.• Hospitalization for
anything. (20% of gout sufferers will have an attack in hospital.)
• Diet high in meat and fish.
• Chronic renal insufficiency.

Gout risk factors
• Medications:– Diuretics – thiazides and furosamide.– Nicotinic acid (niacin).– Aspirin.– Cyclosporine (gengraf, neoral).– Ehtambutol.– Pyrazinamide.– Levodopa.

Gout Dx.
• Pt. may be febrile.• WBC may be elevated.• ESR 50 to 80 range.• CRP elevated.• Uric acid may be normal 20 to 40% of the
time at the time of the attack.• Definitive dx. – intracellular monosodium
urate crystals in synovial fluid.

Definitive dx. – intracellular monosodium urate crystals in
synovial fluid.


Gout – presumtive dx. without arthrocentesis
• A classic history of one or more episodes on monoarticular arthritis followed by periods completely free of symptoms.
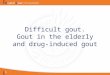
• Max. inflamation within 24 hours.• Rapid resolution with colchicine tx.• Podagra.• Hyperuricemia.• Subcortical bone cysts apparent on x ray.

Differential dx.
• Septic joint.• Pseudogout – calcium pyrophosphate
dihydrate crystal arthropathy. Usually knee or wrist.
• Reactive arthritis.• For polyarticular arthritis, RA, SLE,
psoriatic, etc.• Always consider the background info.

X ray in gout

Treatment of acute gout
• Colchicine 1.2 mg stat, then .6 mg q 2 hours until relief or 6 mg.– Problem is virtually everyone gets N/V and/or
diarrhea after about 3 doses.– If it works, suggestive but not diagnostic of
gout.– Other serious problems – renal and hepatic
injury, CNS dysfunction, neuromyopathy especially in elderly or those with decreased renal or liver function.

Treatment of acute gout
• NSAIDs:– Indocin 50 mg q 6 to 8 hours x 24 to 48 hours,
then decrease to 25 tid x 3 to 5 days.• Works well. Highest risk of GI bleed of NSAIDs.
– Ibuprofen 800 mg q 8 hours x 24 to 48 hours, then 400 to 600 tid x 3 to 5 days.
– Naprosyn 750 mg first dose, then 250 tid x 2 days, then bid x 3 days.
– Almost any other NSAID will work if high enough doses. Start early!!!!!

Treatment of acute gout
• NSAIDs– The usual problem is renal insufficiency,
hypertension, heart failure, ulcers or bleeding that keeps one from utilizing.
– Again start early.

Treatment of acute gout
• Corticosteroids– Prednisone 40 to 60 per day x 2 to 3 days,
then taper over 3 to 7 days.– Triamcinolone 40 to 60 mg IM x 1.– Intra-articular injection, dose dependent on
the joint.• Have to make sure you have the diagnosis before
injecting.

Hyperuricemia
• Treat when gout 2 to 3 x per year.• Asymptomatic and uric acid > 12.• Tophaceous gout.• Gout and any history of kidney stones.• Gout with renal insufficiency.• Acute uric acid nephropathy.

Hyperuricemia tx.• Most patients are underexcreters – 85%.• Those pts could be treated with uricosuric drugs
– probenecid and sulfinpyrazone.– Probenecid is well tolerated.
• Can’t use if kidney stones, renal insufficiency.• Some drug interactions.• Need to produce at least 1500 ml urine per day.• Start at 250 mg bid increasing to 1000 mg 2 to 3 x/d over
several weeks.• Target is < 6 uric acid level.• Need a 24 hour urine for uric acid to demonstrate not an
overproducer.

Hyperuricemia tx.• Xanthine oxidase inhibitors:
– Allopurinol• Start at 100 mg/d for 2 weeks and increase by 100 mg bid
every two weeks until at 300 mg/d.• Increase dose thereafter to achieve uric acid < 6.• Adjust dose for creatine clearance less than 80 ml/mim.• Drug interactions – cyclophosphamide, azathioprine,
mercaptopurine. Increase incidence of rash with ampicillin.• Problems: 3 to 5% develop rash, leukopenia,
thrombocytopenia, diarrhea, and drug fever. – 1 in 1000 will develop allopurinol hypersensitivity syndrome –
rash, fever, hepatitis, eosinophilia, acute renal failure with up to 25% mortality.

Hyperuricemia tx.
• Xanthine oxidase inhibitors:– Febuxostat (Urolic)
• A new drug.• Same drug interactions.• Expensive compared to allopurinol.• Start at 40 mg/d, increase to 80 if not at goal in 2
to 4 weeks.• Monitor LFTs “periodically.”• Increased incidence of CV events compared to
allopurinol.

Hyperuricemia tx.
• Colchicine prophylaxis– .6 mg 1 to 2 x/d depending on creatine
clearance. Don’t use if less than 10 and take q 2-3 days if 10 to 20.
– Use the first 3 to 6 months when instituting uric acid lowering therapy.
• Rasburicase (elitek) – IV med to be used to prevent tumor lysis
syndrome.